

Article
Ischemic heart disease and acute cardiac care
REC Interv Cardiol. 2019;1:21-25
Access to side branches with a sharply angulated origin: usefulness of a specific wire for chronic occlusions
Acceso a ramas laterales con origen muy angulado: utilidad de una guía específica de oclusión crónica
Servicio de Cardiología, Hospital de Cabueñes, Gijón, Asturias, España
ABSTRACT
Introduction and objectives: According to the recommendations of the latest clinical practice guidelines, non-ST-elevation acute myocardial infarction (NSTEMI) patients should undergo an invasive coronary angiography. However, the best moment to perform this coronary angiography has not been stablished yet. Our main objective was to see if performing an early angiography (within the first 24 h) in NSTEMI patients was associated with better prognosis compared to delayed angiography (beyond the first 24 h).
Methods: From January 2014 to June 2016, 447 consecutive patients were admitted to the acute cardiac care unit of a tertiary hospital with a diagnosis of NSTEMI. They all underwent catheterization. We classified them into 3 groups depending on the moment when the coronary angiography was performed (within the first 24 h after diagnosis, 24 h to 72 h later, and > 72 h after diagnosis).
Results: Coronary angiography was performed within the first 24 h in 285 patients (63.8%). There were no differences among the groups regarding gender, distribution of cardiovascular risk factors, past medical history of coronary disease or presence of other comorbidities. We found no differences among the 3 groups in variables with known prognostic impact. The cardiovascular events and 1-year mortality at follow-up were similar among the 3 groups.
Conclusions: In our study, in the whole spectrum of NSTEMI, early coronary angiography (within the first 24 h) did not show any clinical benefits regarding survival or fewer major adverse cardiovascular events.
Keywords: Acute coronary syndrome. GRACE score. Early angiography. Prognosis. Mortality.
RESUMEN
Introducción y objetivos: Las guías clínicas recomiendan la realización de una coronariografía en los pacientes con infarto agudo de miocardio sin elevación del segmento ST (IAMSEST). Sin embargo, no está claramente establecido el mejor momento para hacerla. Por ello, el objetivo del presente trabajo fue analizar si practicar un cateterismo precoz (durante las primeras 24 h) se relaciona con un mejor pronóstico, en comparación con hacerlo de manera diferida (más allá de las 24 h).
Métodos: De enero de 2014 a junio de 2016 ingresaron en la unidad de cuidados agudos cardiológicos de un hospital terciario 447 pacientes consecutivos con diagnóstico de IAMSEST a los que se hizo una coronariografía. Se clasificó de forma retrospectiva a los pacientes en 3 grupos en función del momento de realización del cateterismo: durante las primeras 24 h, entre las 24 y las 72 h tras el diagnóstico, y después de las primeras 72 h.
Resultados: El cateterismo se llevó a cabo en las primeras 24 h en 285 pacientes (63,8%). No se identificaron diferencias entre los grupos en cuanto a sexo, prevalencia de factores de riesgo cardiovascular ni presencia de comorbilidad. Tampoco se encontraron diferencias en las variables pronósticas analizadas ni en la mortalidad. En el seguimiento a los 12 meses, la incidencia de eventos cardiovasculares y la mortalidad fueron similares entre los grupos.
Conclusiones: En el presente estudio, la realización de una coronariografía precoz (en las primeras 24 h) a los pacientes ingresados por IAMSEST no mostró beneficio clínico en términos de supervivencia o reducción de eventos cardiovasculares.
Palabras clave: Síndrome coronario agudo. GRACE score. Cateterismo precoz. Pronóstico. Mortalidad.
Abbreviations: CA: coronary angiography. NSTEMI: non-ST-elevation acute myocardial infarction.
INTRODUCTION
Coronary angiography (CA) is a key step in treatment of patients with non-ST-elevation acute myocardial infarction (NSTEMI). CA reduces mortality and the rates of new cardiovascular adverse events compared to the conservative approach.1,2 Therefore, the current European clinical practice guidelines on the management of NSTEMI recommend an invasive strategy to treat these patients.1
The appropriate time to perform the CA in NSTEMI patients is still under discussion. Early CA (within the first 24 h after diagnosis) is still recommended in patients with high-risk NSTEMI defined as a GRACE score > 140. However, the potential benefit of this approach has not been completely established yet.3
The objective of our study was to assess the prognostic impact of an early CA (within the first 24 h after diagnosis) in patients NSTEMI compared to a delayed CA strategy (after 24 h).
METHODS
This is a retrospective, observational cohort study. From January 2014 to June 2016, data from 447 patients with NSTEMI admitted to a tertiary referral hospital who underwent an invasive coronary angiography were consecutively collected.
NSTEMI was defined according to the guidelines and all patients were treated following the recommendations established by these guidelines.1
Data from all the cases were included prospectively in a continuous multipurpose database. The collection of data included detailed past clinical histories, physical examinations, pulse oximetry measures, 12-lead electrocardiograms, continuous electrocardiogram monitoring, blood tests, echocardiographies, and CAs. The Global Registry of Acute Coronary Events (GRACE) and Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early implementation of the ACC/AHA guidelines (CRUSADE) scores were calculated for each patient.1
Patients were classified into 3 groups according to the time to CA (figure 1): catheterization within the first 24 h after diagnosis (group 1, n = 285 patients), 24 h to 72 h later (group 2, n = 102 patients) and after 72 h (group 3, n = 60 patients). The decision on when to perform the CA was made by the treating physician in each case. After being discharged from the hospital, the 12-month follow-up of patients was performed in a dedicated clinic.
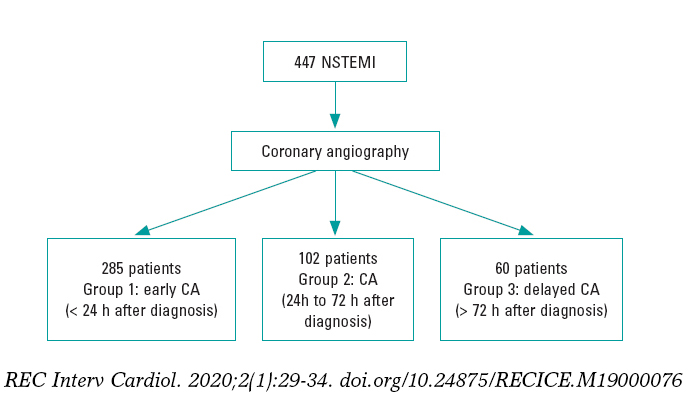
Figure 1. Flowchart. CA, coronary angiography; NSTEMI, non-ST-elevation acute myocardial infarction.
The primary endpoints of our study were mortality and major adverse cardiovascular events (stroke, new acute coronary syndrome, new revascularization) during hospitalization and depending on the time to CA in patients with NSTEMI. The secondary endpoints were mortality and the rate of major cardiovascular events at the 1-year follow-up, and bleeding events according to the BARC criteria.4 We also analyzed the antiplatelet treatment prescribed at discharge and its correlation with MACE at follow-up.
Statistical analysis
Continuous variables are described as mean and standard deviation or median and interquartile range [IQR] when appropriate. The Kolmogorov-Smirnov test was used to assess the variables normal distribution. Regarding quantitative variables, the groups were compared using the 2-tailed Student t test or the Mann-Whitney U test when necessary. Categorical variables were expressed as frequency and percentage, and compared using the chi-square test or Fisher’s exact test when appropriate. No variable had losses > 15%.
A multivariate logistic regression analysis was performed to assess the potential impact of the CA timing on in-hospital mortality. The model included all variables that were statistically significant in the univariate analysis regarding mortality and time to CA. Adjusted odds ratios (OR) with 95% confidence intervals (95%CI) were calculated for each variable. Regarding the secondary endpoint of 1-year mortality, a Cox regression analysis was performed to assess any potential prognostic factors.
All tests were 2-tailed and the differences were considered statistically significant with P values < .05. The statistical analysis was performed using the statistical software package IBM SPSS Statistics V 22.0.
RESULTS
Table 1 shows the baseline characteristics of the patient population. Patients in group 1 were younger (66.5 ± 13.5 years vs 71.1 ± 12.7 years in group 2, and 70.7 13.5) in group 3, P = .016). There were no gender differences among the groups (P = .565). The cardiovascular risk factors, previous coronary artery disease (P = .314), and presence of other comorbidities were similar among the groups (table 1).
Table 1. Baseline characteristics among the 3 study groups and antiplatelet therapy at discharge
| Group 1 (n = 285) | Group 2 (n = 102) | Group 3 (n = 60) | P | |
|---|---|---|---|---|
| Age (years) | 66.5 (13.5) | 70.7 (13.5) | 71.1 (12.7) | .016 |
| Sex (male) | 78.9% | 80.2% | 73.3% | .565 |
| Diabetes | 34.9% | 37.6% | 35.0% | .880 |
| Hypercholesterolemia | 63.4% | 54.5% | 55.9% | .195 |
| Hypertension | 71.1% | 71.3% | 73.3% | .942 |
| GRACE score | 157 (44.9) | 161 (45.7) | 170 (39.6) | .041 |
| CRUSADE score | 32.8 | 34.8 | 36.4 | .251 |
| GFR | 72 | 69.8 | 66 | .118 |
| Peak CK levels | 659.9 | 479.4 | 590 | .623 |
| LVEF at discharge | 49.6 | 54.2 | 52 | .229 |
| Killip class | .604 | |||
| I | 194 (71.3%) | 75 (72.7%) | 37 (62.7%) | |
| II | 32 (11.8%) | 15 (15.2%) | 9 (15.3%) | |
| III | 23 (8.5%) | 7 (7.1%) | 8 (13.6%) | |
| IV | 23 (8.5%) | 5 (5.1%) | 5 (8.5%) | |
| Mechanical ventilation | 29 (10.7%) | 6 (6.1%) | 5 (8.3%) | .636 |
| Number of vessels with severe stenosis | .488 | |||
| 1 | 133 (46.8%) | 45 (44.6%) | 23 (38.6%) | |
| 2 | 77 (27.1%) | 23 (22.8%) | 22 (36.7%) | |
| 3 | 68 (23.9%) | 29 (28.7%) | 14 (23.3%) | |
| Successful revascularization | 211 (89.8%) | 70 (92.1%) | 42 (91.3%) | .930 |
| Antiplatelet therapy at discharge | ||||
| Ticagrelor | 154 (54%) | 52 (50.9%) | 29 (48.3%) | .154 |
| Clopidogrel | 105 (36.8%) | 40 (39.2%) | 24 (40%) | .358 |
| Prasugrel | 26 (9.2%) | 10 (9.9%) | 7 (11.7%) | .469 |
|
CK, creatine kinase; GFR, glomerular filtration rate; LVEF, left ventricular ejection fraction. Group 1: coronary angiography within the first 24 h after diagnosis; group 2: 24 h to 72 h later; group 3: coronary angiography > 72 h after diagnosis. |
||||
A CA was performed within the first 24 h in 285 patients (63.8%). Surprisingly, we noticed that the patients from group 1 showed lower GRACE scores [157.67 (44.9) points vs 170 (39.5) points in group 3, (P = .041)] and similar CRUSADE scores compared to the other 2 groups (P = .251).
There were no significant differences among the groups in the Killip class at admission (table 1). The left ventricular ejection fraction and the peak values of cardiac biomarkers were similar among the groups. The presence of multivessel disease was similarly in the 3 study groups (table 1). There were no significant differences in the primary endpoint among the 3 study groups (table 2). During hospitalization, strokes and bleeding events occurred similarly in the 3 groups (table 2). It is important to emphasize here the low rate of bleeding events (5 patients with BARC 2 and 2 patients with BARC 3 events in group 1, and 3 patients with BARC 2 and 2 patients with BARC 3 events in groups 2 and 3, with no fatal events). At the 1-year follow-up, cardiovascular adverse events and 1-year mortality were similar among the 3 groups (table 2).
Table 2. In-hospital and follow-up rate of adverse events and mortality (expressed as percentage) among the 3 groups
| Group 1 (n = 285) | Group 2 (n = 102) | Group 3 (n = 60) | P | |
|---|---|---|---|---|
| In-hospital events | ||||
| Heart failure | 74 (25.9%) | 26 (25.4%) | 21 (36%) | .246 |
| Non-fatal AMI | 3 (1%) | 4 (3.9%) | 3 (6%) | .371 |
| Acute kidney injury | 47 (16.5%) | 18 (17.6%) | 15 (25%) | .334 |
| Stroke | 3 (1%) | 2 (1.9%) | 2 (3.3%) | .548 |
| Bleeding events | 20 (7%) | 6 (5.8%) | 6 (10%) | .213 |
| In-hospital mortality | 19 (6.6%) | 7 (6.8%) | 2 (3.4%) | .358 |
| Events at the 1-year follow-up | ||||
| Death | 17 (5.9%) | 5 (4.9%) | 5 (8.3%) | .114 |
| Stroke | 3 (1.05%) | 3 (2.9%) | 1 (1.6%) | .271 |
| Major bleeding | 7 (2.45%) | 6 (5.8%) | 4 (6.6%) | .427 |
| Myocardial infarction | 16 (5.6%) | 5 (4.9%) | 4 (6.6%) | .907 |
|
AMI, acute myocardial infarction. Group 1: coronary angiography within the first 24 h after diagnosis; group 2: 24 h to 72 h later; group 3: coronary angiography > 72 h after diagnosis. |
||||
Regarding medical treatment at discharge, a similar percentage of patients received clopidogrel, prasugrel and ticagrelor in the 3 study groups (table 1). In our cohort, antiplatelet therapy was not associated with differences in the rate of major adverse cardiovascular events and mortality at the 12-month follow-up.
The multivariate logistic regression analysis performed to predict mortality revealed that hypertension, Killip class IV at admission, left ventricular ejection fraction, and myocardial damage (defined as peak creatine kinase levels) were independently associated with higher in-hospital mortality rates. The time to CA was not an independent predictor of in-hospital mortality after the multivariate adjustment (table 3).
Table 3. Multivariate logistic regression analysis to predict in-hospital mortality
| Variable | Odds ratio (95%CI) | P |
|---|---|---|
| CA after 72 h | reference | |
| CA within the first 24 h | 0.98 (0.26-3.74) | .978 |
| CA 24 h to 72 h later | 1.33 (0.28-6.24) | .716 |
| Hypertension | 6.25 (1.09-33.3) | .04 |
| Age (per year) | 1.03 (0.98-1.08) | .292 |
| Successful revascularization | 0.51 (0.12-2.21) | .371 |
| Peak CK levels (per pg/mL) | 1.00 (1.00-1.01) | .010 |
| LVEF | 0.93 (0.90-0.97) | < .001 |
| Killip class at admission | ||
| I | reference | .026 |
| II | 3.39 (0.98-11.75) | .054 |
| III | 3.24 (0.92-11.36) | .067 |
| IV | 15.34 (2.19-107.58) | .006 |
|
95%CI, 95% confidence interval; CA, coronary angiography; CK, creatine kinase; LVEF, left ventricular ejection fraction. |
||
Regarding 1-year mortality, the Cox regression analysis showed similar results. The time to CA was non-significant in the multivariate analysis. Hypertension, age, left ventricular ejection fraction, and Killip class at admission were independently associated with higher mortality rates at 1 year (table 4).
Table 4. Multivariate Cox regression analysis to predict 1-year mortality
| Variable | Hazard ratio (95%CI) | P |
|---|---|---|
| CA after 72 h | reference | |
| CA within the first 24 h | 0.96 (0.46-2.03) | .919 |
| CA 24 h to 72 h later | 0.82 (0.33-2.07) | .677 |
| Hypertension | 3.64 (1.30-10.3) | .014 |
| Age (per year) | 1.04 (1.01-1.07) | .022 |
| Successful revascularization | 0.94 (0.41-2.13) | .876 |
| Peak CK levels (per pg/mL) | 1.00 (1.00-1.01) | .198 |
| LVEF | 0.96 (0.94-0.98) | < .001 |
| Killip class at admission | ||
| I | reference | |
| II | 2.83 (1.32-6.08) | .008 |
| III | 2.78 (1.27-6.09) | .010 |
| IV | 2.91 (0.83-10.2) | .096 |
|
95%CI, 95% confidence interval; CA, coronary angiography; CK, creatine kinase; LVEF, left ventricular ejection fraction. |
||
DISCUSSION
Our study included a large cohort of 447 consecutive patients with NSTEMI that were retrospectively analyzed. Our results showed that early CAs (defined as a CA performed within the first 24 h after diagnosis) in NSTEMI patients did not improve the prognosis of this cohort of patients compared to delayed CAs. No differences were seen among the 3 groups regarding the time to CA in the in-hospital cardiovascular adverse event rate, mortality rate or at the 12-month follow-up either.
Early CA, within the first 24 h after diagnosis, is currently recommended by the clinical practice guidelines for the management of patients with NSTEMI. However, this recommendation is based on the results of relatively old clinical trials and a meta-analysis.4-8 Several recent trials have explored the prognostic impact of the CA timing on NSTEMI patients in order to find stronger evidence in this clinical setting.9,10
The results of the TIMACS study (Timing of Intervention in Acute Coronary Syndromes) showed that an early CA was associated with a reduction in the composite endpoint of death, myocardial infarction or refractory ischemia compared to a delayed CA strategy.11
A retrospective cohort study that included 19 704 propensity scorematched patients hospitalized with a first acute coronary syndrome conducted between January 1, 2005 and December 31, 2011 showed that the use of an early invasive treatment strategy was associated with a lower risk for cardiovascular mortality and re-hospitalization due to myocardial infarction compared to a conservative invasive approach.12 However, it is important to emphasize the retrospective nature of this study and the fact that patients were followed for 60 days only.
However, a meta-analysis that combined data from 83 229 patients did not show any significant differences regarding mortality, myocardial infarction or major bleeding events between the 2 strategies.13
Another meta-analysis that included 8 randomized controlled trials (n = 5324 patients) with a median follow-up of 180 days [180-360] and compared an early invasive group of NSTEMI patients to a delayed strategy showed that the early invasive strategy did not reduce mortality in all NSTEMI patients including high risk patients with GRACE score > 140 points.14
Similarly, a recent meta-analysis that combined the results of 10 clinical trials did not find any differences in mortality, myocardial infarction or major bleedings among NSTEMI patients based on the CA timing. Nevertheless, the early CA strategy was associated with less recurrent angina and shorter hospital stays.15
The LIPSIA-NSTEMI study randomized patients with NSTEMI to undergo CA within the first 2 h after randomization (immediate CA strategy), 10 h to 48 h after randomization (early CA), and the so-called “selectively invasive” arm, in which patients initially received medical treatment without showing any differences in the infarct size among the 3 study groups.16
A recent randomized controlled trial conducted by a Kofoed et al., the VERDICT trial, included a total of 2147 patients of which 1075 were allocated to very early invasive evaluation (within the first 12 h after diagnosis), and 1072 to receive standard invasive care (CA 61.6 h after randomization).17 The primary endpoint was a composite of all-cause mortality, nonfatal recurrent myocardial infarction, refractory myocardial ischemia-related hospital admission or heart failure-related hospital admission. In this trial, the very early invasive coronary evaluation strategy did not improve overall the long-term clinical outcome compared to the invasive strategy performed within 2 to 3 days in patients with non-ST-segment elevation acute coronary syndrome. However, in patients with the highest risk, the very early invasive therapy improved long-term outcomes17 which is consistent with the results shown by the TIMACS trial.
Despite all these data, there is still controversy on what the best timing is to perform a CA in patients with NSTEMI.
An important limitation of previous studies is heterogeneity in the definition of early and late CA, and the differences seen in the primary endpoints.4-14 The lack of uniform criteria makes it difficult to compare the results. The definition of NSTEMI has changed over time. Thus, old clinical trials used a different criterion for the definition of NSTEMI and included different patients from those of current studies. We should try to identify what patients with the highest risk would benefit from an early invasive strategy. In this sense, previous studies did not use risk grading systems to classify patients. However, in our study we calculated the ischemic and bleeding risks of all patients. As our objective was to assess the potential benefit of an early invasive strategy among NSTEMI patients, the GRACE risk score was estimated in the entire study population. However, despite the high ischemic risk of our patients, no significant differences were found between the 2 strategies (early or delayed CA) regarding mortality or adverse events.
Limitations
Our study has several limitations that should be considered when interpreting the results. Although we included a large number of NSTEMI patients with a collection of high quality data, this is an observational, retrospective, single center study with the limitations of this type of study. Besides, the current clinical practice guidelines recommend the PRECISE-DAPT score to assess bleeding risk in this clinical setting. In our study bleeding risk at admission was classified according to CRUSADE score.
CONCLUSIONS
The results of our study show that the early CA strategy did not improve prognosis or reduce mortality in NSTEMI patients. However, larger studies are still needed to clarify which group of patients may benefit from early CA strategies.
CONFLICTS OF INTEREST
None declared.
WHAT IS KNOWN ABOUT THE TOPIC?
- Early CA is recommended by the current clinical practice guidelines in patients with a high-risk suffering from non-ST-elevation acute myocardial infarctions.
- To this day, clinical trials and meta-analyses show contradictory results without clear prognostic differences between the early CA strategy and delayed catheterization.
WHAT DOES THIS STUDY ADD?
- A large cohort of consecutive NSTEMI patients was retrospectively studied. We assessed in-hospital progression and cardiovascular events and mortality at the 1-year follow-up.
- The results of our study show that the early CA strategy did not imporive prognosis or reduced mortality in NSTEMI patients.
- No differences among the 3 groups were seen based on the CA timing regarding cardiovascular adverse events and mortality during the hospital stay or at the 12-month follow-up.
- No differences among the 3 groups were seen based on the CA timing regarding cardiovascular adverse events and mortality during the hospital stay and at the 12-month follow-up.
REFERENCES
1. Roffi M, Patrono C, Collet JP, et al. 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation:Task Force for the Management of Acute Coronary Syndromes in Patients Presenting Without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37:267-315.
2. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes:executive summary:a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130:2354-2394.
3. Reuter PG, Rouchy C, Cattan S, et al. Early invasive strategy in high-risk acute coronary syndrome without ST-segment elevation. The Sisca randomized trial. Int J Cardiol. 2015;182:414-418.
4. Vranckx P, White HD, Huang Z, et al. Validation of BARC Bleeding Criteria in Patients With Acute Coronary Syndromes:The TRACER Trial. J Am Coll Cardiol. 2016;67:2135-2144.
5. Montalescot G, Cayla G, Collet JP, et al. ABOARD Investigators. Immediate vs delayed intervention for acute coronary syndromes:a randomized clinical trial. JAMA.2009;302:947-954.
6. De Winter RJ, Windhausen F, Cornel JH, et al. Early invasive versus selectively invasive management for acute coronary syndromes. N Engl J Med.2005;353:1095-1104.
7. Hirsch A, Windhausen F, Tijssen JG, et al. Long-term outcome after an early invasive versus selective invasive treatment strategy in patients with non-ST-elevation acute coronary syndrome and elevated cardiac troponin T (the ICTUS trial):a follow-up study. Lancet.2007;369:827-835.
8. O'Donoghue M, Boden WE, Braunwald E, et al. Early invasive vs conservative treatment strategies in women and men with unstable angina and non- ST-segment elevation myocardial infarction:a meta-analysis. JAMA. 2008;300:71-80.
9. Badings EA, The SH, Dambrink JH, el al. Early or late intervention in high-risk non-ST-elevation acute coronary syndromes:results of the ELISA-3 trial. EuroIntervention.2013;9:54-61.
10. Milosevic A, Vasiljevic-Pokrajcic Z, Milasinovic D, et al. Immediate Versus Delayed Invasive Intervention for Non-STEMI Patients:The RIDDLE-NSTEMI Study. JACC Cardiovasc Interv.2016;9:541-549.
11. Mehta SR, Granger CB, Boden WE, et al. Early versus delayed invasive intervention in acute coronary syndromes. N Engl J Med. 2009;360:2165-2175.
12. Hansen KW, Sorensen R, Madsen M, et al. Effectiveness of an early versus a conservative invasive treatment strategy in acute coronary syndromes:a nationwide cohort study. Ann Intern Med. 2015;163:737-746.
13. Navarese EP, Gurbel PA, Andreotti F, et al. Optimal timing of coronary invasive strategy in non-ST-segment elevation acute coronary syndromes:a systematic review and meta-analysis. Ann Intern Med. 2013;158:261-270.
14. Jobs A, Mehta SR, Montalescot G, et al. Optimal timing of an invasive strategy in patients with non-ST-elevation acute coronary syndrome:a meta-analysis of randomized trials. Lancet.2017;390:737-746.
15. Bonello l, Laine M, Puymirat E, et al. Timing of Coronary Invasive Strategy in Non-ST-Segment Elevation Acute Coronary Syndromes and Clinical Outcomes:An Updated Meta-Analysis. JACC Cardiovasc Interv. 2016;9:2267-2276.
16. Thiele H, Rach J, Klein N, et al. Optimal timing of invasive angiography in stable non-ST-elevation myocardial infarction:the Leipzig Immediate versus early and late PercutaneouS coronary Intervention triAl in NSTEMI (LIPSIA-NSTEMI Trial). Eur Heart J. 2012;33:2035-2043.
17. Kofoed KF, Kelbæk H, Hansen PR, et al. Early Versus Standard Care Invasive Examination and Treatment of Patients With Non-ST-Segment Elevation Acute Coronary Syndrome. Circulation. 2018;138:2741-2750.
ABSTRACT
Introduction and objectives: The strategy of the percutaneous treatment of patients with multivessel disease associated with chronic total coronary occlusion (CTO) lesions is not well defined. Also, the functional significance of lesions located in the collateral donor artery has not been fully addressed. Using the fractional flow reserve (FFR) the objective was to evaluate the amount of ischemia related to the angiographically intermediate stenosis of collateral donor vessels before and immediately after successful percutaneous coronary intervention (PCI) of a CTO. Also, to assess any changes operated in the amount of ischemia using cardiovascular magnetic resonance imaging prior to the PCI and at 1-month follow-up.
Methods: Prospective pilot study including 14 patients with stable angina and a CTO receiving collateral circulation from a blood vessel with intermediate stenosis (50%-70% diameter stenosis measured using quantitative angiography). In order to indicate recanalization by PCI all patients were referred for magnetic resonance assessment of the presence of myocardial viability.
Results: Seven (50%) of the 14 patients included showed FFR values ≤ 0.80 before the PCI. FFR measures of the donor artery significantly increased after the revascularization of the CTO (0.75 [0.73-0.78] vs 0.83 [0.81-0.84]; P = .017). Eventually, only 3 patients showed hemodynamically significant FFR values after the recanalization of CTO requiring further revascularization. There was a tendency towards a reduction of the number of ischemic segments (2.5 [0-4] vs 0 [0-0.25]; P = .066) assessed using magnetic resonance imaging before and after the PCI. No major adverse cardiovascular events were reported at the 2-year follow-up.
Conclusions: Our data suggest that FFR measurements in intermediate stenoses of collateral donor vessels of a CTO may be misleading. Therefore, the strategy of focusing primarily on the revascularization of the CTO and then on the assessment of the intermediate lesion in a collateral donor vessel may be recommended.
Keywords: Chronic total coronary occlusion. Collateral donor vessel. Fractional flow reserve. Cardiovascular magnetic resonance imaging.
RESUMEN
Introducción y objetivos: La estrategia de tratamiento percutáneo de los pacientes con enfermedad multivaso y oclusión total crónica (OTC) no está bien definida. La importancia funcional de las lesiones localizadas en arterias donantes de colaterales no se ha abordado por completo. Nuestro objetivo fue evaluar mediante reserva fraccional de flujo (RFF) la cantidad de isquemia dependiente de una lesión angiográfica intermedia en un vaso donante de colaterales antes y después de la recanalización de la OTC, y valorar el cambio en la cantidad de isquemia por resonancia magnética cardiaca (RMC) antes y 1 mes después de la recanalización.
Métodos: Estudio piloto prospectivo en 14 pacientes con angina estable y una OTC que recibía circulación colateral de un vaso con una estenosis intermedia (50-70% por angiografía coronaria cuantitativa). Para indicar la revascularización, todos los pacientes presentaban viabilidad miocárdica por RMC.
Resultados: De los 14 pacientes, 7 (50%) evidenciaron una RFF ≤ 0,80 antes de la recanalización. Los valores medios de RFF de la arteria donante aumentaron significativamente tras la revascularización de la OTC (0,75 [0,73-0,78] frente a 0,83 [0,81-0,84]; p = 0,017). Solo 3 pacientes mostraron valores de RFF hemodinámicamente significativos después de la recanalización de una OTC que requirió revascularización adicional. Hubo una tendencia hacia una reducción del número de segmentos isquémicos (2,5 [0-4] frente a 0 [0-0,25]; p = 0,066) evaluados por RMC antes y después del intervencionismo. No se observaron eventos cardiacos adversos mayores durante el seguimiento de 2 años.
Conclusiones: Las mediciones de RFF en estenosis intermedias de vasos donantes de colaterales de una OTC pueden ser engañosas. En estos casos podría plantearse la estrategia de centrarse primero en la revascularización de la OTC y después en la evaluación de la lesión intermedia del vaso donante.
Palabras clave: Oclusión total crónica. Reserva fraccional de flujo. Resonancia magnética cardiaca. Vaso colateral donante.
Abreviaturas: CMR: cardiovascular magnetic resonance imaging. CTO: chronic total coronary occlusion. FFR: fractional flow reserve. PCI: percutaneous coronary intervention.
INTRODUCTION
The prevalence of chronic total coronary occlusions (CTO) is around 16% to 52% in patients with significant coronary artery disease on the angiography.1 In the presence of a CTO, collateral blood supply is often enought to maintain resting perfusion and contractility in the collateral-dependent myocardium.2 Restoration of antegrade flow by the percutaneous coronary intervention (PCI) of a CTO is associated with a rapid reduction in the collateral supply received in the treated vessel.3
Randomized trials support the use of fractional flow reserve (FFR) to guide the PCI with an established treatment threshold of ≤ 0.8.4-8 Although the FFR is reported to be independent of hemodynamic changes,9 it is intimately related to total coronary flow through a stenosis, which in turn is related to perfused myocardial mass.10 In keeping with this, there have been several reports of normalization of FFR values from collateral donor vessel after successful recanalization of a CTO.11 By removing nutrient flow to the collateralized territory by CTO recanalization, the collateral network almost immediately increased its resistance, thus favoring flow to the donor territory during maximal hyperemia.12
In patients with Rentrop grade-2 or grade-3 collateral flow, the FFR value of the donor artery increased at least 0.10 after revascularization of the recipient artery. However, the FFR value did not change significantly in patients with Rentrop grade-0 or grade-1 collateral flow following revascularization. This suggests that well-developed collateral circulation might overestimate the FFR value in the donor artery with mild stenosis.13
The assessment of myocardial-perfusion through cardiovascular magnetic resonance imaging (CMR) is a noninvasive imaging modality for the detection of coronary artery disease with a high degree of concordance with the FFR for ischemia detection.14-16 Also, the CMR has emerged as robust and reproducible method to assess the ischemia and viability of the myocardium related to the CTO.17-19 The MR-INFORM trial showed that in patients with stable angina and risk factors for coronary artery disease, the CMR of myocardial perfusion was associated with a lower incidence of coronary revascularization compared to the FFR and was noninferior to the FFR regarding major adverse cardiovascular events (all-cause mortality, non-fatal myocardial infarction or target-vessel revascularization) at 12 months.20 However, it is uncertain whether opening a CTO can modify the amount of ischemia related to an angiographically intermediate lesion of the collateral donor vessel. It could also be possible to diagnose microvascular dysfunction using CMR.21
Therefore, in this pilot study, using the FFR we assessed changes in the amount of ischemia related to the angiographically intermediate stenosis of collateral donor vessel before and immediately after the successful PCI of a CTO. We also tried to determine any changes in the amount of ischemia using the CMR prior to the PCI and 1 month after recanalization.
METHODS
In this prospective pilot study, we included patients with stable angina and CTO with collateralization of the distal vascular bed, and collateral donor vessel with a single angiographically intermediate lesion (50%-70% diameter stenosis by quantitative coronary angiography). In order to indicate recanalization through PCI all patients were referred for CMR evaluation to assess the presence of myocardial viability. During the procedure, the FFR of the donor vessel was measured before the PCI of the CTO (figure 1). Only with FFR values ≤ 0.80, the measure was reassessed after the procedure (figure 2). A second CMR was performed 1 month after the index PCI. All patients gave their informed consent, the local ethics committee approved the study, and all procedures were performed in accordance with the Helsinki Declaration. The study population was clinically followed for 2 years. The rate of major adverse cardiovascular events was established. This was defined as a composite of all-cause mortality, non-fatal acute myocardial infarction (AMI), clinically-driven target vessel revascularization or rehospitalization due to unstable or progressive angina according to Braunwald Unstable Angina Classification. The exclusion criteria were: prior IAM; failed recanalization of the CTO, inability to obtain signed written informed consents; severity of valvular heart disease; acutely decompensated chronic heart failure; asthma or obstructive sleep apnea; high risk of bleeding; known hypersensitivity or contraindication to aspirin; nursing subjects; patients with pacemakers/implantable cardioverter- defibrillators.
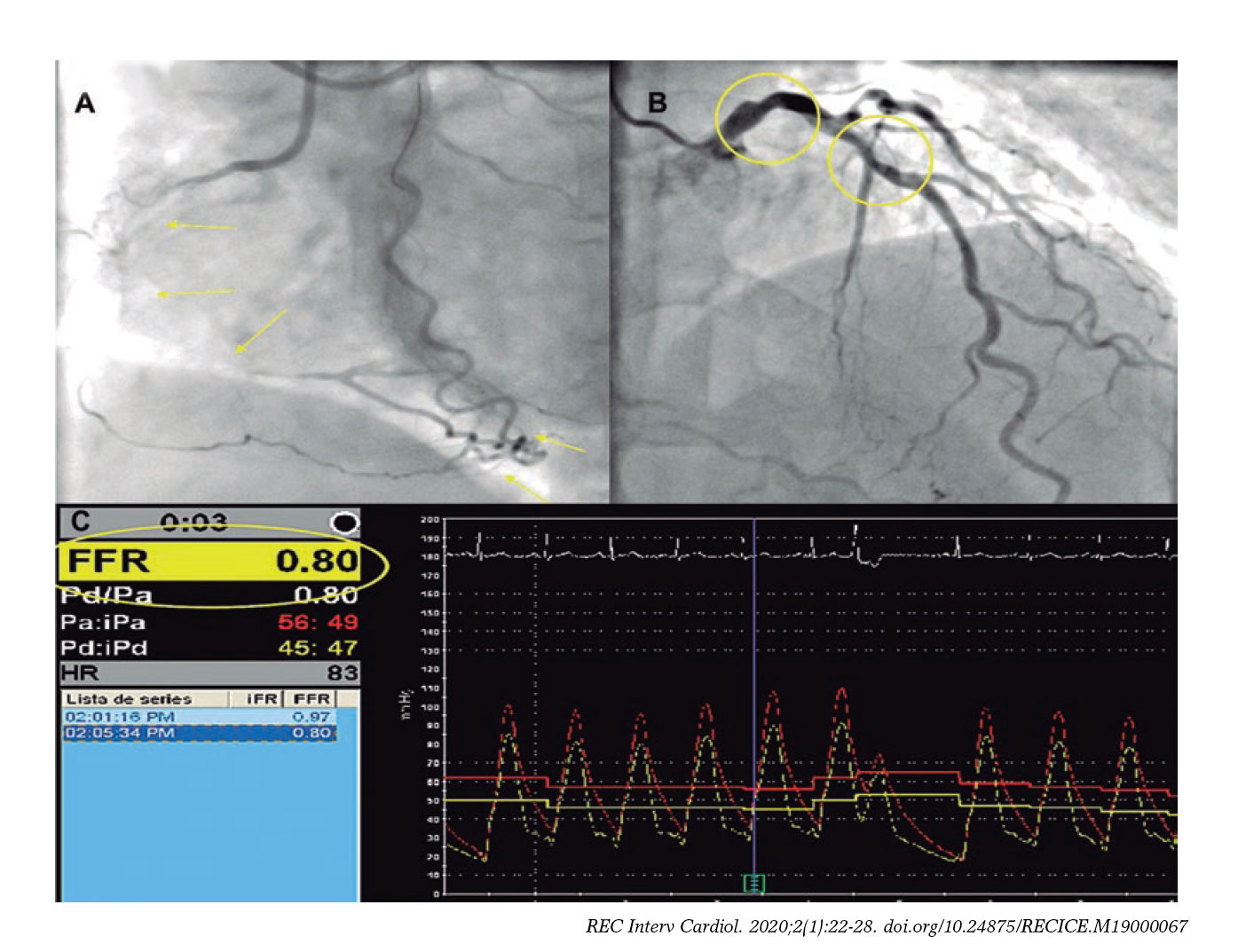
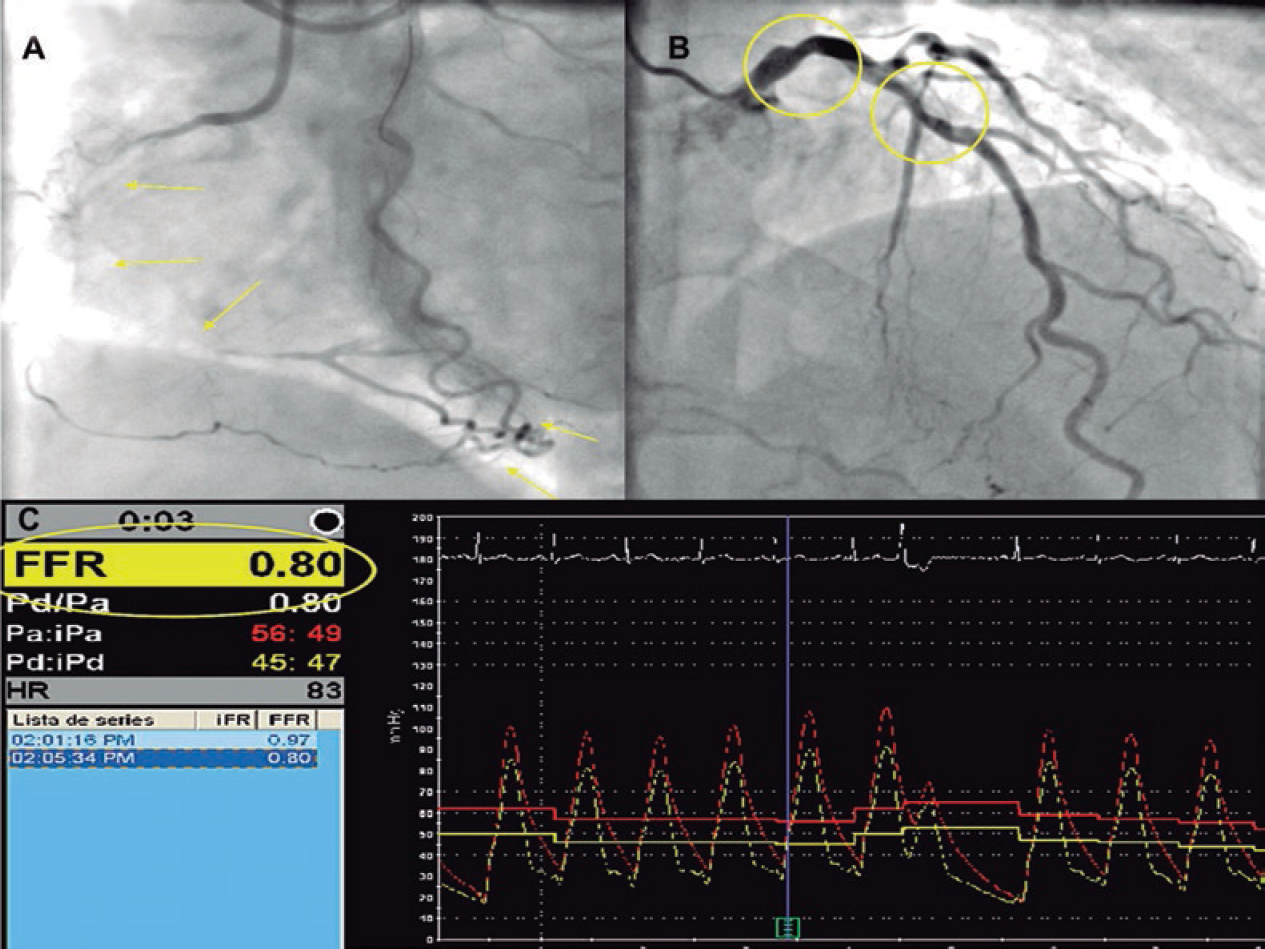
Figure 1. Example of chronic total coronary occlusion (CTO) of right coronary artery (panel A, yellow arrows) with collateralization of distal vascular bed, and left main and left anterior descendent artery (LAD) as the collateral donor vessel shows an angiographically intermediate lesion (panel B, yellow circles). During the procedure, the fractional flow reserve (FFR) of the donor vessel was measured before the percutaneous coronary intervention of the CTO (panel C).
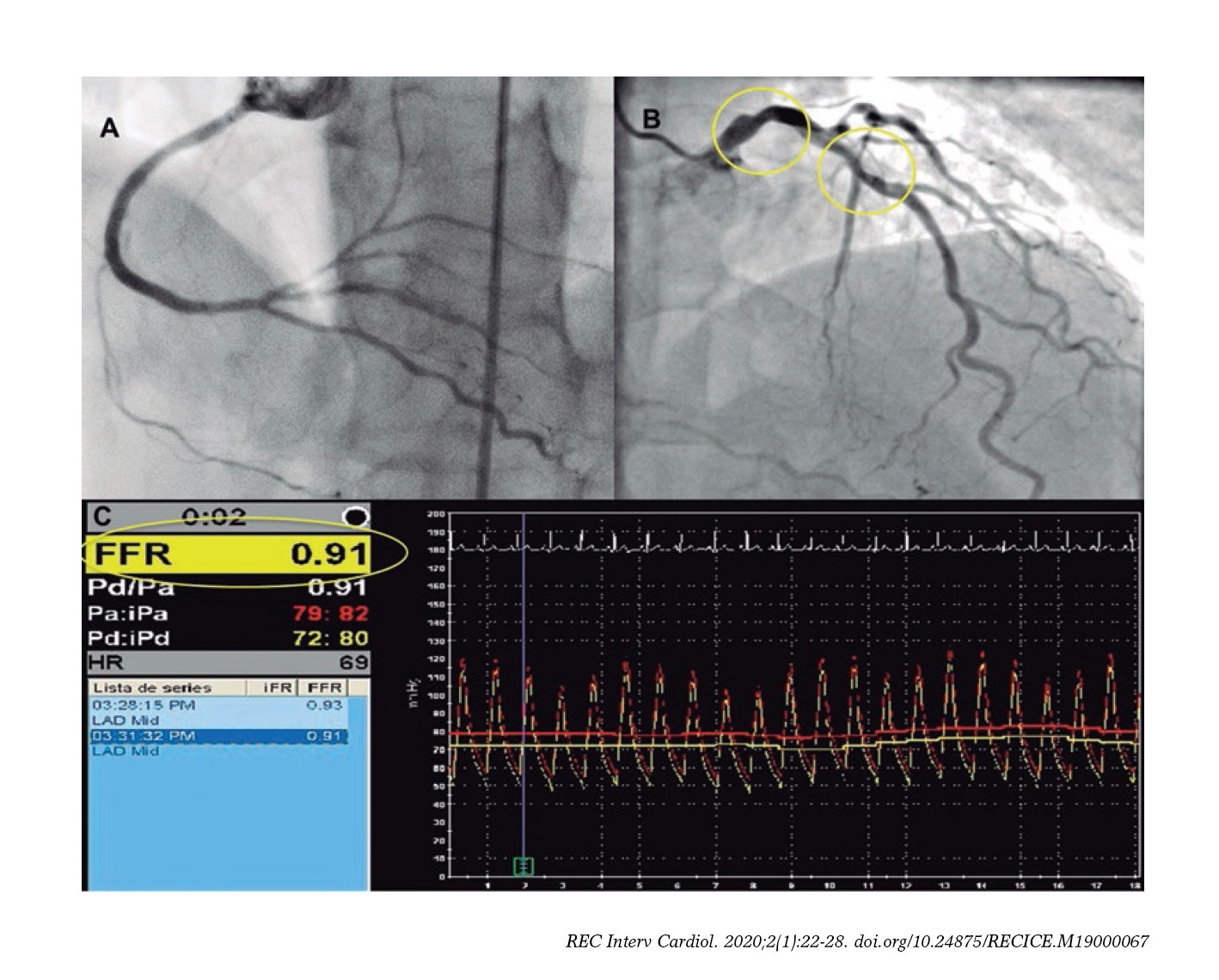
Figure 2. Example of the recanalization of chronic total coronary occlusion (CTO) of the right coronary artery (panel A) with left anterior descendent artery (LAD) as the collateral donor vessel shows an angiographically intermediate lesion (panel B, yellow circles). Panel C: after the CTO repermeabilization, the fractional flow reserve (FFR) value of the LAD increased (FFR value = 0.91).
The percutaneous coronary intervention
The PCI was performed using bilateral femoral artery access and 7-Fr sheaths and guide catheters. Anticoagulation was achieved with 100 U/Kg of unfractionated heparin to maintain activated clotting times of 250-300 msec. All the procedures on the CTO were performed using the antegrade wire escalation technique. All patients were treated with drug-eluting stent implantation. The J-CTO score was calculated for each CTO lesion and assessed taking the following parameters into consideration: occlusion length, stump morphology, presence of calcification, presence of tortuosity and prior attempt to open the CTO.22 Collateral flow was graded in accordance with Rentrop collateral flow classification.23 Procedural success was defined as achievement of residual post-PCI stenosis < 30% in the target lesion associated with TIMI grade-3 flow without mortality, IAM or new lesion revascularization during the index hospitalization.
Assessment using fractional flow reserve
To measure FFR in the intermediate coronary lesions a 0.014-inch pressure-monitoring guidewire (Prime Wire Volcano Therapeutics, Inc, Rancho Cordova, CA, United States) was used. After calibration of both the aortic and wire pressures, the FFR wire was advanced until the tip of the guiding catheter. Equalization of both pressures was performed. Then, the wire was advanced and positioned distally at least 15 mm from the stenotic lesion followed by the administration of 0.2 mg of nitroglycerin to avoid any form of epicardial vasoconstriction. Maximal hyperemia was induced through the IV infusion of adenosine (180 µg/kg/min). After reaching the steady state we measured the FFR as the ratio between mean distal coronary pressure and mean aortic pressure. Values < 0.80 were considered significant from the hemodynamical standpoint. After FFR measurement and under maximal hyperemia, the pressure wire was pulled back until the sensor was close to the tip of the guiding catheter to make sure that no drift had occurred.
Cardiovascular magnetic resonance imaging
All CMR studies were performed using a General Electric Signa HDxt 1.5-T scanner equipped with an 8-channel coil and cardiac-dedicated software. Perfusion studies were conducted using a gradient-echo turbo-field sequence prescribed in the left ventricular short-axis orientation, at the basal, mid-ventricular and apical levels after 4 min of IV administration of adenosine (Atepo-din) at a dose of 180 µg/kg/min and simultaneous administration of 0.1 mmol/kg of gadobutrol (Gadovist, Bayer Hispania) at a 5 mL/s rate. The functional and volumetric assessment of the left ventricle (LV) was conducted using the conventional Steady State Free Precession (SSFP) cine sequence, prescribed in sequential short-axis slices, and encompassing the entire LV and the 2-, 3-, and 4-chamber views. The typical temporal and in-plane spatial resolution of these images was 40 ms and 1.4 × 1.4 mm, respectively. Rest perfusion images were obtained at least 10 min after the stress perfusion study using the same sequence, location, and contrast injection protocol. Ten minutes after administering the dose of gadolinium for the rest perfusion study, late gadolinium-enhanced images were obtained using a segmented inversion-recovery spoiled gradient echo sequence in the same location and identical spatial resolution as the cine images. To calculate left ventricular ejection fraction (LVEF), the LV mass and left ventricular end-systolic and end-diastolic volumes, the endocardial and epicardial borders were manually traced at end-systole and end-diastole in the cine short-axis images using a dedicated software package (ReportCard, GE). The regional wall motion analysis was performed by visual grading of the cine images according to the 17-segment model proposed by the American Heart Association.17 The pre- and post-PCI image analysis was conducted by 2 independent experienced operators masked to the patient’s coronary anatomy and the PCI results; the disparities in their evaluation were resolved by consensus with a third independent operator. The appropriate allocation between the involved myocardial segments and the correspondent coronary anatomy in each case was evaluated according to previously reported criteria.18
Statistical analysis
The distribution of continuous variables was assessed by visual inspection of frequency histograms and using the Shapiro–Wilk test. Continuous variables were expressed as mean ± standard deviation (SD) or median with interquartile range (IQR) when they followed a normal or non-normal distribution, respectively. The continuous variables were compared using the unpaired Student t test or Mann–Whitney U test and the categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate. Correlations between variables were conducted using the Pearson test. The software SPSS 17.0 (SPSS Italy, Florence, Italy) was used for statistical analyses.
RESULTS
We screened 23 patients with stable angina and CTO with collateralization of distal vascular bed, and collateral donor vessel with angiographically intermediate lesion. We excluded 9 patients who showed some exclusion criteria. Fourteen patients were finally included in the study (figure 3). The clinical characteristics and angiographic details are shown on table 1. Seven intermediate lesions (50%) of the collateral donor vessels showed FFR values ≤ 0.80 before the recanalization of the CTO. On average, FFR measures significantly increased after CTO revascularization (0.75 [0.73-0.78] vs 0.83 [0.81-0.84]; P = .017) (table 2 and figure 4). Four patients normalized their FFR values, while in the other 3 the FFR remained hemodynamically significant and required subsequent PCI. There was a tendency towards a reduction of the number of ischemic segments assessed through CMR before and after the recanalization of the CTO (2.5 [0-4] vs 0 [0-0.25]; P = .066). No differences were found in other parameters including the number of hypokinetic segments, left ventricular ejection fraction, left ventricular end-diastolic and end-systolic volumes; left ventricular mass; and necrotic mass before and after the PCI (table 2). In addition, the number of ischemic segments did not significantly correlate with the FFR values before or after PCI (R2 = -0.31, P = .328; R2 = -0.68, P = .20, respectively). Finally, no major adverse cardiovascular events were reported during the 2-year follow-up.
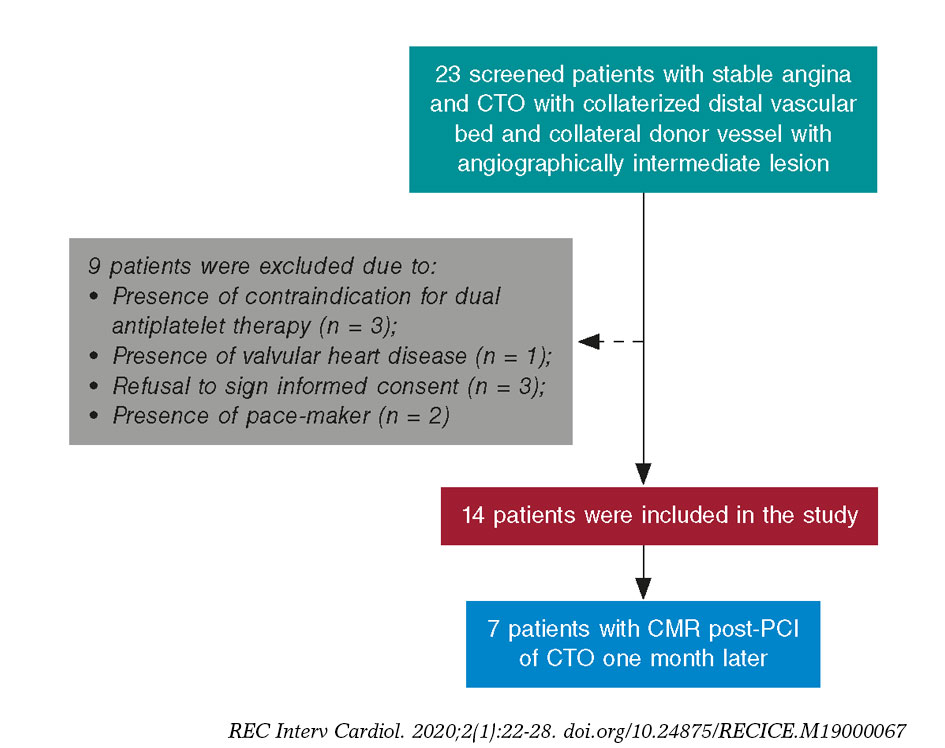
Figure 3. We screened 23 patients with stable angina and chronic total occlusion (CTO) with collateralization of distal vascular bed, and collateral donor vessel with angiographically intermediate lesion; 9 of them were excluded after meeting the exclusion criteria. In particular, 3 contraindications for dual antiplatelet therapy, 1 valvular heart disease requiring surgery, 3 refusals to sign the informed consent, and 3 pacemakers. CMR, cardiovascular magnetic resonance; PCI, percutaneous coronary intervention.
Table 1. Clinical and angiographic characteristics
| Clinical characteristics | Patients (n = 14) |
|---|---|
| Age, years | 67.44 ± 12.9 |
| Male | 12 (85) |
| Hypertension | 6 (42.8) |
| Smoking | 2 (14.3) |
| Hyperlipidemia | 10 (71.4) |
| Diabetes Mellitus | 5 (35.7) |
| Renal failure | 2 (14.3) |
| Prior CABG | 1 (7.1) |
| Medical treatment | |
| Beta-blockers | 5 (35.7) |
| Calcium antagonist | 2 (14.3) |
| ACE inhibitor | 4 (28.5) |
| Statins | 10 (71.4) |
| Angiographic characteristics | |
| CTO vessel | |
| LAD | 2 (14.3) |
| LCX | 1 (7.1) |
| RCA | 11 (78.6) |
| Calcification | 7 (50%) |
| Bending > 45 degrees | 2 (14.3) |
| Tapered | 8 (57.1) |
| Occlusion length, mm | 24.6 [6-43.3] |
| Rentrop > 1 | 13 (92.8) |
| J-CTO score > 2 | 3 (21.4) |
| Collateral donor vessel | |
| LAD | 7 (50) |
| LCX | 4 (28.6) |
| RCA | 3 (21.4) |
| Stenosis degree | 52 [50-55] |
|
Data are expressed as n (%), mean ± standard deviation or median [interquartile range]. ACE, angiotensin converting enzyme; CABG, coronary artery bypass grafting; CTO, chronic total occlusion; IQR, interquartile range; JCTO, Japanese CTO; LAD, left anterior descending artery; LCX, left circumflex artery; RCA, right coronary artery. |
|
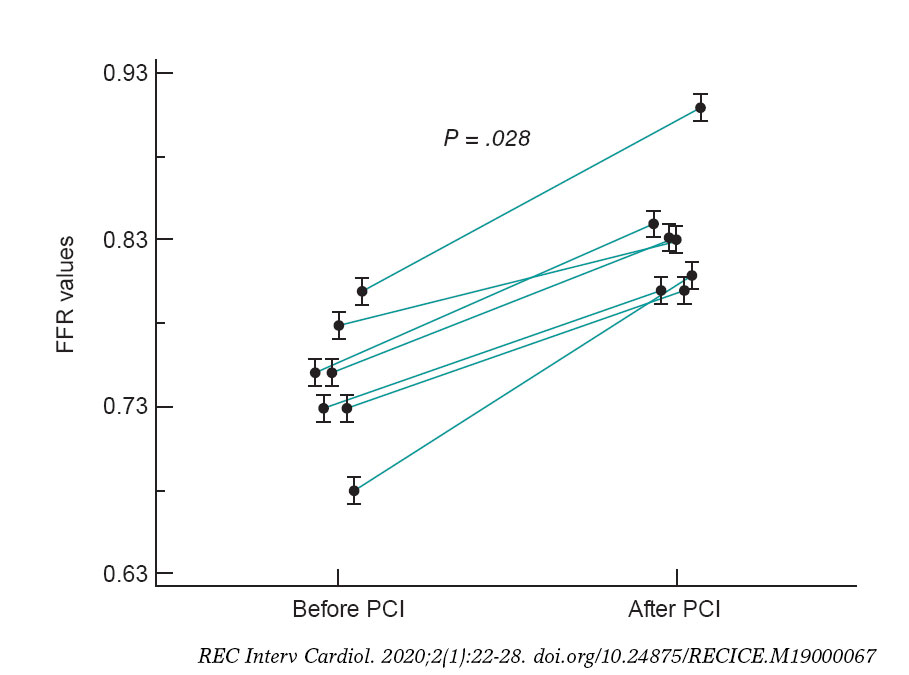
Figure 4. Fractional flow reserve (FFR) values of 7 angiographically intermediate lesions in the collateral donor vessels before and after the percutaneous coronary intervention (PCI) of a chronic total coronary occlusion.
Table 2. FFR and CMR measures in the study population
| Before PCI (n = 7) | After PCI (n = 7) | P | |
|---|---|---|---|
| Pd/Pa | 0.93 (0.88-0.96) | 0.91 (0.89-0.93) | 1.00 |
| FFR | 0.75 (0.73-0.78) | 0.83 (0.81-0.84) | .017 |
| IS | 2.5 (0.0-4.0) | 0.0 (0.0-0.25) | .066 |
| HS | 1.0 (0.0-4.75) | 0.0 (0.0-0.50) | .15 |
| LVEF, % | 60.5 (55.0-63.25) | 63.5 (54.0-65.25) | .41 |
| LVEDV, ml | 111.3 (102.7-451.1) | 109.0 (100.6-139.2) | .50 |
| LVESV, ml | 41.1 (38.6-65.17) | 38.9 (35.2-81.4) | .49 |
| LV mass, gr | 83.4 (56.4-92.1) | 88.5 (69.1-110.2) | .50 |
| NM, gr | 0.83 (0.3-2.3) | 0.92 (0.4-1.5) | 1.0 |
|
CMR, cardiovascular magnetic resonance imaging; FFR, fractional flow reserve; HS, hypokinetic segments; IS, ischemic segments; LV, left ventricular; LVEDV, left ventricular end-diastolic volume; LVEF, left ventricular ejection fraction; LVESV, left ventricular end-systolic volume; NM, necrotic mass; Pd/Pa: resting distal coronary pressure to aortic pressure ratio; PCI, percutaneous coronary intervention. Data expressed as median (interquartile range). |
|||
DISCUSSION
These are the main findings of the study: a) functional assessment of intermediate lesions located in the collateral donor artery showed significantly lower FFR values than it would have in the absence of collateralized CTOs; b) after the recanalization of the CTO, the FFR values of the collateral donor artery normalized in most of patients; c) the amount of ischemia assessed through CMR used to decrease after successful CTO recanalization; d) no major adverse cardiovascular events were reported in our population at the long-term follow-up.
The FFR is a method used to assess the functional significance of coronary stenosis while taking in account the following parameters: severity of stenosis, myocardial territory and viability, and collateral perfusion.19 Results from the FAME trial showed that FFR-guided PCI was superior to the angiography-guided PCI at 1 and 2 years in terms of death or AMI and AMI alone.5,11 In the FAME 2 trial, the FFR-guided PCI reduced the rate of major adverse cardiovascular events compared to medical therapy alone.6 To this day, physiology has been proposed to outline which stenoses should be treated in the context of multivessel disease.24 However, there is uncertainty around what the waiting time is before performing an accurate pressure wire assessment of donor arteries after the successful recanalization of a CTO. Several studies have shown that full collateral regression does not happen immediately after the successful revascularization of a CTO.3 During embryonic development, collaterals derive either from capillary sprouting or pre-existing arteriolar connections.25 Collateral growth occurs through 2 major processes: arteriogenesis and angiogenesis. The former, stimulated by physical forces, consists of the growth, positive remodeling, and expansion of preexisting collateral vessels. The latter, induced by hypoxia, is the de novo growth of new capillaries by sprouting or intussusception from pre-existing vessels.26 Although once established, coronary collaterals are believed to persist and can be re-recruited, this process does not happen immediately. Well-developed collateral vessels close when the pressure gradient across the collateral network disappears. Also, the time needed to reopen the closed collaterals after reestablishing the pressure gradient seems to be directly related to the time interval between coronary occlusions.27 Recently, Mohdnazri et al. have showed that the successful recanalization of a right coronary artery CTO resulted in a modest but statistically significant and immediate increase of instantaneous wave-free ratio (iFR) in the predominant donor vessel following the recanalization of the CTO. At 4 months, both the FFR and the iFR showed significant improvement compared to pre-PCI values together with a concomitant reduction of collateral function.28 Ladwiniec et al. showed that the recanalization of a CTO resulted in a modest FFR increase of the predominant collateral donor vessel associated with a reduced coronary flow, of a similar magnitude at baseline and maximal hyperemia.29 Few patients of our study did not show this improvement. The persistence of non-angiographically visible collateral circulation, the presence of microcirculation dysfunction and type of prior collateral circulation grade,30 and distal embolization or myonecrosis following PCI recanalization may be potential causes of this lack of improvement. In this regard, in a recent study, measurements repeated shortly after the PCI of a CTO showed transient procedural-related changes like microvascular dysfunction secondary to distal embolization, catecholamine release, left ventricular stunning or hyperemic stimulus related to side-branch occlusion.29
Our data suggest that in the setting of CTOs and an angiographically intermediate lesion of the collateral donor vessel, it seems like the FFR measurement may be misleading. Therefore, it seems advisable to postpone the assessment of intermediate stenoses until achieving the successful recanalization of the associated CTO. This approach should avoid overtreating patients who only require the revascularization of their CTOs. On the contrary, if the recanalization of the CTO fails, treating the intermediate stenosis in the donor artery may be necesary to reduce ischemia in this territory. It also still is a good practice to try to re-open the CTO prior to performing any interventions on the donor vessel, due to the risk of extensive acute ischemia in case of troublesome PCIs.
Moreover, we did not find any correlations between the amount of ischemia assessed through CMR and the FFR values before or after the PCI. As far as we know, this is the first comparison between CMR and FFR assessment of an angiographically intermediate lesion in a collateral donor vessel related a CTO. Former studies have suggested that the CMR underestimates or that the FFR overestimates the number of ischemic segments in multi-vessel disease.31-32 This discrepancy seems to highlight the poor accuracy of the FFR method in the presence of collaterals involving territories that are from the target lesion to be assessed.
Finally, after treating the patients according to the FFR measures obtained after the PCI of a CTO, no major adverse cardiovascular events were detected at the 2-year follow-up.
Limitations
Several limitations should be acknowledged. First, due to the small size of the sample our findings should be, at best, hypothesis- generating findings. Secondly, we only used FFR as hyperemic index; other indices (eg. iFR, IMR, etc.) were not assessed. Similarly, we could not assess the influence of microcirculation through CMR or hyperemic microvascular resistance. Third, we did not assess whether collateral circulation originated from a segment proximal or distal to the target stenosis under study. Fourth, in patients with negative FFR before the recanalization of their CTO we did not repeat the FFR after the PCI. Finally, no follow-up CMRs were performed in patients with negative FFR prior to recanalization.
CONCLUSIONS
The FFR assessment of intermediate stenoses in a collateral donor vessel of a CTO may overestimate the severity of the lesion by increasing the territory at risk. Therefore, the strategy of first focusing on the revascularization of the CTO and then re-assess the intermediate lesion in a collateral donor vessel may be recommended to overcome this pitfall.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare.
WHAT IS KNOWN ABOUT THE TOPIC?
- In patients with CTOs, collateral circulation supplied by donor vessels is often seen.
- The progression of atherosclerosis in donor vessels may compromise the coronary circulation of several territories.
- Angiography is not a reliable technique to assess the hemodynamic compromise of an intermediate lesion located in a vessel that provides collateral circulation to a chronically-occluded vessel.
WHAT DOES THIS STUDY ADD?
- Patients with positive FFR of donor vessels before the recanalization of a CTO may show significant increases of FFR values (even normalization in most of them too) after successful revascularization of the CTO.
- Also, the revascularization of the CTO may lead to a reduction in the number of ischemic segments assessed through CMR before and after the PCI of the CTO.
- These findings support the strategy of recanalizing the CTO first and then performing the functional assessment of donor artery with intermediate lesions.
REFERENCES
1. Fefer P, Knudtson ML, Cheema AN, et al. Current perspectives on coronary chronic total occlusions:the Canadian Multicenter Chronic Total Occlusions Registry. J Am Coll Cardiol. 2012;59:991-997.
2. Hoebers L, Claessen B, Dangas G, et al. Contemporary overview and clinical perspectives of chronic total occlusions. Nat Rev Cardiol. 2014; 11:458-469.
3. Fujita M, Sasayama, S. Reappraisal of functional importance of coronary collateral circulation. Cardiology. 2010;117:246-252.
4. Bech GJ, De Bruyne B, Pijls NH, et al. Fractional flow reserve to determine the appropriateness of angioplasty in moderate coronary stenosis:a randomized trial. Circulation. 2001;103:2928-2934.
5. Tonino PA, De Bruyne B, Pijls NH, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360:213-224.
6. De Bruyne B, Pijls NH, Kalesan B, et al. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. N Engl J Med. 2012; 367:991-1001.
7. Adjedj J, De Bruyne B, Flore V, et al. Significance of intermediate values of fractional flow reverse in patients with coronary artery disease. Circulation. 2016;133:502-508.
8. Pijls NH, Fearon WF, Tonino PA, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention in patients with multivessel coronary artery disease:2-year follow-up of the FAME (Fractional Flow Reserve Versus Angiography for Multivessel Evaluation) study. J Am Coll Cardiol. 2010;56:177-184.
9. Pijls NH, van Son JA, Kirkeeide RL, De Bruyne B, Gould KL. Experimental basis of determining maximum coronary, myocardial, and collateral blood flow by pressure measurements for assessing functional stenosis severity before and after percutaneous transluminal coronary angioplasty. Circulation. 1993;87:1354-1367.
10. Christou MA, Siontis GC, Katritsis DG, Ioannidis JP. Meta-analysis of fractional flow reserve versus quantitative coronary angiography and noninvasive imaging for evaluation of myocardial ischemia. Am J Cardiol 2007;99:450-456.
11. Sachdeva R, Uretsky BF. The effect of CTO recanalization on FFR of the donor artery, Catheter Cardiovasc Interv. 2011;77:367-369.
12. Sachdeva R, Agrawal M, Flynn SE, et al. Reversal of Ischemia of Donor Artery Myocardium After Recanalization of a Chronic Total Occlusion. Catheter Cardiovasc Interv. 2013;82:E453-E458.
13. Tigen K, Durmus E, Sari I. Recanalization of a Total Occlusion With Marked Retrograde Collateral Supply:Impact of Collateral Circulation on Fractional Flow Reserve Measurements of Donor Artery. J Invasive Cardiol. 2014;26:E70-E75.
14. Greenwood JP, Maredia N, Younger JF, et al. Cardiovascular magnetic resonance and single-photon emission computed tomography for diagnosis of coronary heart disease (CEMARC):a prospective trial. Lancet. 2012;379:453-460.
15. Watkins S, McGeoch R, Lyne J, et al. Validation of magnetic resonance myocardial perfusion imaging with fractional flow reserve for the detection of significant coronary heart disease. Circulation. 2009;120:2207-2213.
16. Takx RAP, Blomberg BA, El Aidi H, et al. Diagnostic accuracy of stress myocardial perfusion imaging compared to inva- sive coronary angiography with fractional flow reserve meta-analysis. Circ Cardiovasc Imaging. 2015;8:e002666-e6.
17. Cerqueira MD, Weissman NJ, Dilsizian V, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation. 2002;105:539-542.
18. Ortiz-Pe?rez JT, Rodri?guez J, Meyers SN, Lee DC, Davidson C, Wu E. Correspondence between the 17-segment model and coronary arterial anatomy using contrast-enhanced cardiac magnetic resonance imaging. J Am Coll Cardiol Img. 2008;1:282-293.
19. Christou MA, Siontis GC, Katritsis DG, Ioannidis JP. Meta-analysis of fractional flow reserve versus quantitative coronary angiography and noninvasive imaging for evaluation of myocardial ischemia. Am J Cardiol. 2007;99:450-456.
20. Nagel E, Greenwood JP, McCann GP, et al. Magnetic Resonance Perfusion or Fractional Flow Reserve in Coronary Disease. N Engl J Med. 2019;380:2418-2428.
21. Liu A, Wijesurendra RS, Liu JM, et al. Diagnosis of Microvascular An-gina Using Cardiac Magnetic Resonance. J Am Coll Cardiol. 2018;71:969-979.
22. Morino Y, Abe M, Morimoto T, et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes:the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. 2011; 4:213-221.
23. Rentrop KP, Cohen M, Blanke H, Phillips RA. Changes in collateral channel filling immediately after controlled coronary artery occlusion by an angioplasty balloon in human subjects. J Am Coll Cardiol. 1985;5:587-592.
24. Escaned J, Banning A, Farooq V, et al. Rationale and design of the SYNTAX II trial evaluating the short to long-term outcomes of state-of-the-art percutaneous coronary revascularisation in patients with de novo three-vessel disease. EuroIntervention. 2016;12:e224-e234.
25. Werner GS. The role of coronary collaterals in chronic total occlusions. Curr Cardiol Rev. 2014;10:57-64.
26. Zimarino M, D'Andreamatteo M, Waksman R, et al. The dynamics of the coronary collateral circulation . Nat Rev Cardiol. 2014;1:191-197.
27. Zimarino M, Ausiello A, Contegiacomo G, et al. Rapid decline of collateral circulation increases susceptibility to myocardial ischemia:the trade-off of successful percutaneous recanalization of chronic total occlusions. J Am Coll Cardiol. 2006;48:59-65.
28. Mohdnazri SR, Karamasis GV, Al-Janabi F, et al. The impact of coronary chronic total occlusion percutaneous coronary intervention upon donor vessel fractional flow reserve and instantaneous wave-free ratio:Implications for physiology-guided PCI in patients with CTO. Catheter Cardiovasc Interv. 2018;92:E139-148.
29. Ladwiniec A, Cunnington MS, Rossington J, et al. Collateral Donor Artery Physiology and the Influence of a Chronic Total Occlusion on Fractional Flow Reserve. Circ Cardiovasc Interv. 2015;8:e002219.
30. Brugaletta S, Martin-Yuste V, PadróT, et al. Endothelial and smooth muscle cells dysfunction distal to recanalized chronic total coronary occlusions and the relationship with the collateral connection grade. JACC Cardiovasc Interv. 2012;5:170-178.
31. Hussain ST, Chiribiri A, Morton G, et al. Perfusion cardiovascular magnetic resonance and fractional flow reserve in patients with angiographic multi-vessel coronary artery disease. J Cardiovasc Magn Reson. 2016;18:44.
32. Cardona M, Martín V, Prat-Gonzalez S, et al. Benefits of chronic total coronary occlusion percutaneous intervention in patients with heart failure and reduced ejection fraction:insights from a cardiovascular magnetic resonance study. J Cardiovasc Magn Reson. 2016;18:78.
ABSTRACT
Introduction and objectives: After the results of several randomized trials, routine thrombus aspiration (TA) has remained out of the spotlight after not improving the prognosis of patients with ST-segment elevation myocardial infarction and even increasing their complications. The goal here was to assess the impact of selective TA during primary percutaneous coronary intervention (pPCI), its safety and clinical benefits at 1-year follow-up.
Methods: The TAPER registry (efficacy and safety of selective Thrombus Aspiration in Real clinical Practice) retrospectively included patients with ST-segment elevation myocardial infarction treated with pPCI. The clinical and procedural characteristics and the composite endpoint of cardiovascular mortality, non-fatal myocardial infarction, stent thrombosis, target lesion revascularization or stroke were evaluated after at 1-year follow-up.
Results: 687 patients (76.9% males, 64 ± 12 years) were analyzed. The TA was performed in 40.3% of cases (in 89.9% as the initial strategy and in 10.1% as the bailout strategy) and it was successful in 93.8% of them. The most important predictor of TA use was a higher initial Thrombolysis in Myocardial Infarction (TIMI) thrombus grade (OR, 3.2; 95%CI, 2.5-3.9; P < .0001). TA achieved a significant improvement of TIMI-flow (2.4 points) and a significant reduction of the TIMI thrombus grade (2.6 points). At 1-year follow-up, no stroke was observed in the TA-group and the rate of the composite endpoint (cardiovascular mortality, non-fatal myocardial infarction, stent thrombosis, target lesion revascularization or stroke) was similar in both groups (TA-group 8% vs non-TA-group 5.7%; P = .24).
Conclusions: Selective TA is frequently used in the current clinical practice with a high success rate and a low rate of associated complications. It significantly reduces thrombotic burden and improves coronary flow. At 1-year follow-up, a similar rate of adverse events was observed regardless of the use of TA.
Keywords: Thrombus aspiration. Primary PCI. STEMI.
RESUMEN
Introducción y objetivos: Tras los resultados de varios estudios aleatorizados, la tromboaspiración (TA) sistemática ha sido relegada a un segundo plano por no mejorar el pronóstico de los pacientes con infarto agudo de miocardio con elevación del segmento ST e incluso aumentar sus complicaciones. El objetivo de este trabajo fue evaluar el impacto de la TA selectiva durante la angioplastia primaria (ICPp), su seguridad y sus beneficios clínicos tras 1 año de seguimiento.
Métodos: El registro TAPER (eficacia y seguridad de la tromboaspiración selectiva en la práctica clínica real) incluyó retrospectivamente pacientes con infarto de miocardio con elevación del segmento ST tratados con ICPp. Se evaluaron las características clínicas y de los procedimientos, así como la presentación del evento combinado de muerte cardiovascular, infarto de miocardio no fatal, trombosis de stent, necesidad de revascularización de la lesión tratada o ictus tras 1 año de seguimiento.
Resultados: Se analizaron 687 pacientes (76,9% varones, 64 ± 12 años). La TA se realizó en el 40,3% de los casos (89,9% como estrategia inicial y 10,1% como rescate) y fue exitosa en el 93,8%. El predictor más importante de uso de TA fue un alto grado de trombo inicial según la escala TIMI (Thrombolysis in Myocardial Infarction) (odds ratio = 3,2; intervalo de confianza del 95%, 2,5-3,9; p < 0,0001). La TA consiguió una mejora significativa del flujo de 2,4 puntos en la escala TIMI de flujo y una reducción significativa del grado de trombo de 2,6 puntos en la escala TIMI de trombo. En 1 año de seguimiento no se observó ningún ictus en el grupo de TA y la tasa del evento combinado fue similar en ambos grupos (grupo de TA 8% y grupo de no-TA 5,7%; p = 0,24).
Conclusiones: La TA selectiva se usa con frecuencia en la práctica clínica actual, con una alta tasa de éxito y pocas complicaciones asociadas. La TA selectiva reduce significativamente la carga de trombo y mejora el flujo coronario. Tras 1 año de seguimiento, se observó una tasa similar de eventos adversos en los pacientes a quienes se realizó ICPp con independencia del uso de TA.
Palabras clave: Tromboaspiracion. Angioplastia primaria. IAMCEST.
Abreviaturas: Abbreviations pPCI: primary percutaneous coronary intervention. TA: thrombus aspiration.
INTRODUCTION
Primary percutaneous coronary intervention (pPCI) is the preferred treatment for the management of ST-segment elevation myocardial infarction.1 However, one of its limitations is the possibility of distal embolization of thrombus and failure to restore flow at the microvascular level, which is associated with a significantly higher mortality rate.2 Thrombus aspiration (TA) was thought to be a simple method to remove thrombus before stent deployment, thereby reducing distal embolization and improving outcomes.3
After the promising results of the TAPAS trial,4,5 TA was included in the routine practice and was probably overused.6 However, the results from the TASTE8 and TOTAL9 clinical trials have brought uncertainty to the clinical benefits of TA. Additionally, possible harm from an increased risk of stroke has been suggested.9 Subsequently, guidelines have downgraded the indication for routine TA from IIa10-12 to III,13,14 resulting in a progressive reduction in the use of TA (figure 1).4,7,9,15
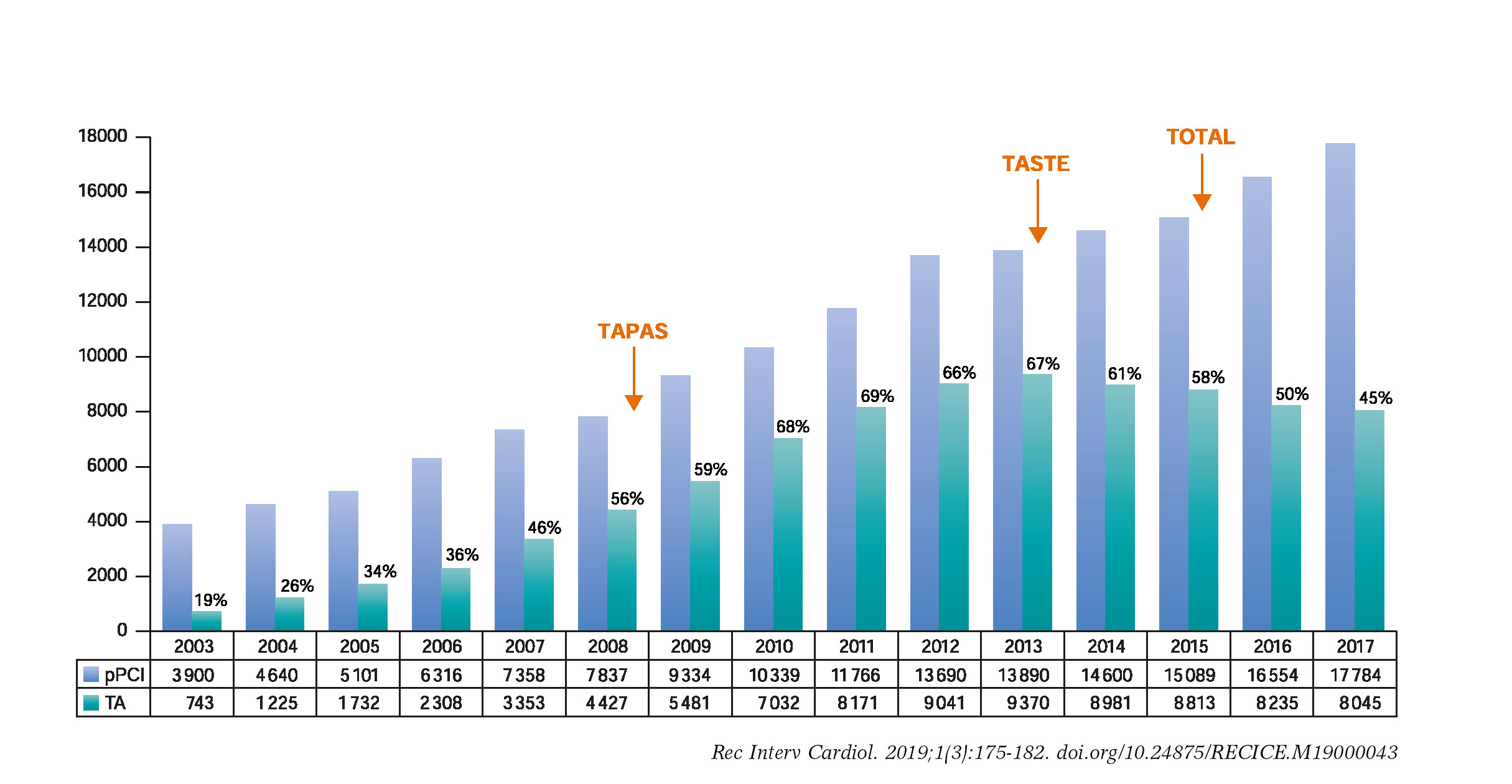
Figure 1. Evolution of pPCI and TA over the last 15 years: Evolution of primary percutaneous coronary intervention and TA in Spain over the last 15 years15 in relation to the publication of the main TA trials.4,7,9 pPCI, primary percutaneous coronary intervention; TA, thrombus aspiration.
In addition to the fact that the above-mentioned clinical trials may not reflect the actual clinical practice,6 we should be consider that these recommendations apply for routine TA and not for selective TA, where the operator performs the technique in cases where the expected benefit is higher. Although selective TA may be more indicative of the common practice, we do not have actual data on its application. For this reason, we designed the TAPER registry (efficacy and safety of selective Thrombus Aspiration in Real clinical Practice) in an attempt to analyze the procedural advantages of selective TA during pPCI, its safety and clinical benefit at 1-year of follow-up.
METHODS
Patients and study design
The TAPER registry retrospectively included patients with ST-segment elevation myocardial infarction treated with pPCI in 4 high-volume centres of different countries (A, B, C, D) on a 24/7 program. These centers serve communities of 615 000, 400 000, 450 000, and 350 000 people, respectively.
Consecutive patients with ST-segment elevation myocardial infarction who were referred to undergo pPCI within 12 hours after symptoms onset in the period between January 2015 and December 2016 were included. Those who had received fibrinolytic therapy were not eligible.
We excluded those patients who did not have an evident culprit coronary lesion, those who presented with cardiac arrest and those who were lost to follow-up. Patients with contraindications to antiplatelet therapy were also excluded (figure 2).
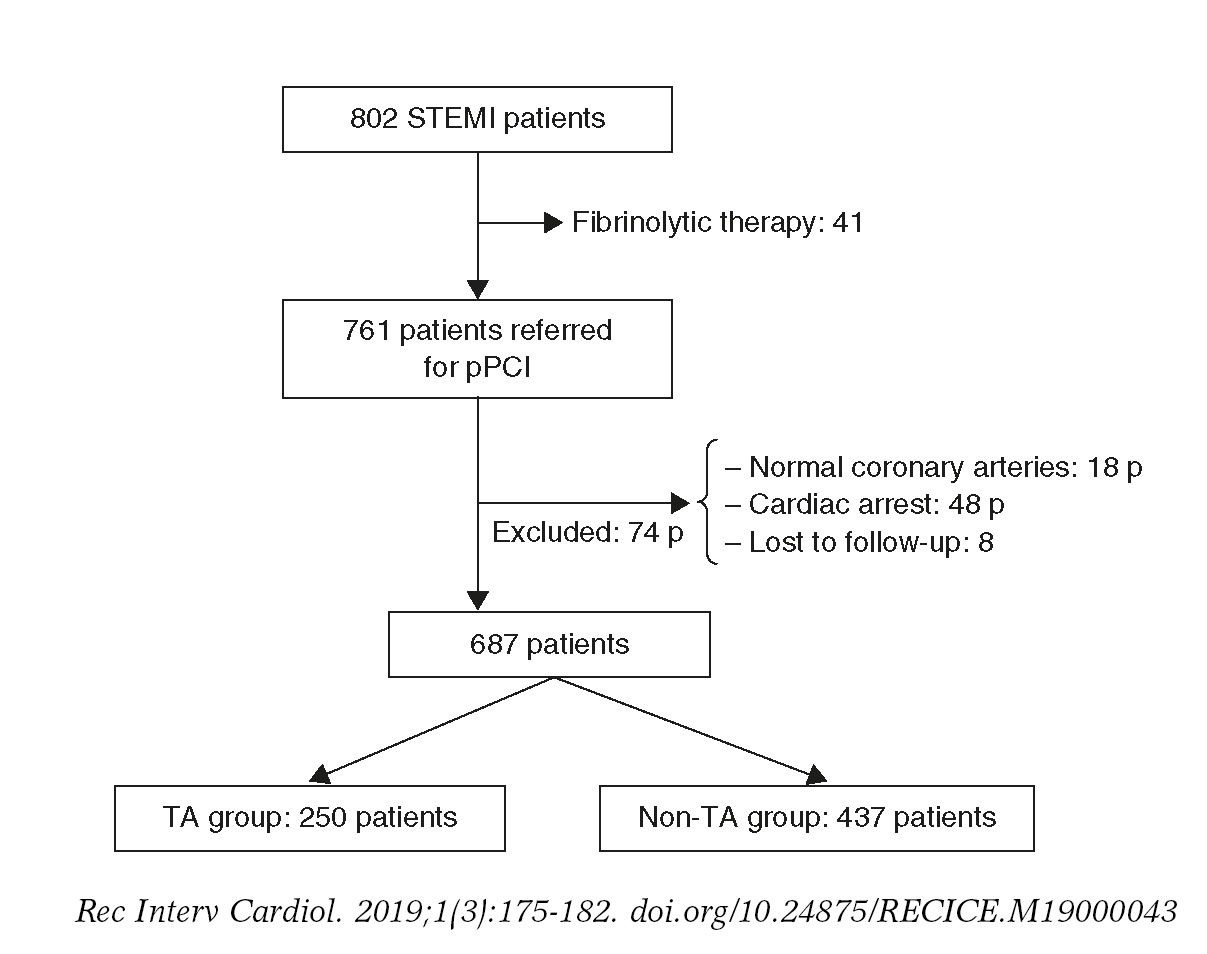
Figure 2. Study flowchart. P, patients; pPCI, primary percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction; TA, thrombus aspiration.
The TA group was defined as those patients in whom the TA was performed as an initial strategy and non-TA group as those patients in whom the TA was not performed or it was performed as a bailout strategy after balloon dilatation or stent implantation.
Both the clinical and procedural characteristics were analyzed and a combined endpoint of cardiovascular mortality, non-fatal myocardial infarction related to the treated lesion, stent thrombosis, target lesion revascularization or stroke was evaluated at 1-year follow-up.
Study procedures
Patients received antiplatelet and anticoagulant treatment according to the clinical practice guidelines.16 The addition of IIb/IIIa glycoprotein inhibitors was left to the discretion of the operator. The use of TA and other technical details of the pPCI were left at the discretion of the interventional cardiologist. TA was performed using a standard technique.9
Angiographic assessment
The angiographic analysis was performed by 4 experienced interventional cardiologists. After defining the culprit lesion in the initial coronary angiogram, the distal flow of the culprit vessel was assessed using the Thrombolysis in Myocardial Infarction (TIMI) grade score.17 Once the culprit lesion had been crossed with a coronary guidewire, the thrombotic burden was defined according to the TIMI-thrombus scale.18 Both the TIMI-flow scale and the TIMI-thrombus scale were reassessed after the TA. The presence of no-reflow phenomenon and thrombus distal embolization were also evaluated.
Follow-up and clinical endpoints definitions
The follow-up of the patients was carried out through telephone calls and in-hospital clinical records of the visits to the cardiology department after the initial admission.
The occurrence of major acute cardiovascular events (MACE) [cardiovascular mortality, myocardial infarction related to the treated lesion, stent thrombosis or need for revascularization of the treated lesion or stroke] at 1-year follow-up was established as the primary endpoint. The secondary endpoints were the independent analysis of each individual event of the composite endpoint.
All deaths were considered cardiac unless another specific cause was documented. Myocardial infarction was defined following the actual recommendations19 and only those related to the treated lesion, whether periprocedural or at follow-up, were taken into consideration. Target lesion revascularization or stent thrombosis was defined according to the Academic Research Consortium criteria.20
The angiographic success was defined as final TIMI 3 distal flow with less than 20% of vessel stenosis and no immediate mechanical complications. TA was considered successful if an improvement of TIMI-flow ≥ 1 grades or a reduction of TIMI-thrombus scale ≥ 1 grades were achieved, without any immediate complications related to the technique.
Statistical analysis
Quantitative variables following a normal distribution were expressed as mean ± standard deviation. Those that did not follow were described by the median [range]. Qualitative variables were expressed as absolute and relative frequencies of their categories.
P levels < .05 were considered statistically significant and the 95% confidence interval (95%CI) of the target analysis variables was estimated. When it comes to the bivariate analysis, the Student t test or the non-parametric Mann-Whitney U test were used for mean comparison purposes and the chi-square test or Fisher’s exact test were used to compare qualitative variables.
For the multivariate analysis, logistic regression was used. Variables were considered as potential predictors of risk in the multivariate model when they showed a statistically significant association in the univariate analysis. The SPSS statistical package software version 20 (Armonk, NY: IBM Corp), was used for calculations.
RESULTS
Out of the 761 patients initially screened, 74 were excluded (18 patients did not have any evident culprit coronary lesions, 48 patients presented with cardiac arrest, and 8 patients were lost to follow-up). The remaining 687 patients (64.1 ± 12.2 years; 76.9% male) were finally analyzed. The baseline characteristics are shown on table 1.
Table 1. Baseline characteristics
| TA group N = 250 | Non-TA group N = 437 | P | |
|---|---|---|---|
| Age (y) | 63.6 ± 12.6 | 64.4 ± 12.1 | .46 |
| Male | 208 (83.2%) | 320 (73.2%) | .003 |
| BMI | 27.2 ± 6.4 | 26.6 ± 5.8 | .23 |
| Current smoker | 105 (42%) | 140 (32%) | .012 |
| Diabetes mellitus | 44 (17.6%) | 80 (18.3%) | .86 |
| Dyslipidemia | 74 (29.6%) | 103 (23.6%) | .07 |
| Hypertension | 114 (45.6%) | 195 (44.6%) | .68 |
| LVEF | 48.7 ± 10.7 | 49.7 ± 10.4 | .27 |
| Previous PCI | 27 (10.8%) | 37 (8.5%) | .29 |
| Previous CABG | 3 (1.2%) | 5 (1.1%) | .93 |
| Chronic kidney disease | 13 (5.2%) | 13 (2.9%) | .14 |
|
BMI, body mass index; CABG, coronary artery bypass grafting; LVEF, left ventricle ejection fraction; PCI, percutaneous coronary intervention; TA, thrombus aspiration. Data are expressed as no. (%) or mean ± standard deviation. |
|||
Procedural characteristics
In the overall cohort, the culprit lesion was more frequently located at the left anterior descending coronary artery (45.6%), followed by the right coronary artery (36.9%). Forty-eitgh-point-one per cent of patients had multivessel disease. The initial TIMI-flow was 0-1 in 72.7% of cases and the TIMI-thrombus grade was ≥ 3 in 61.6% of the cases.
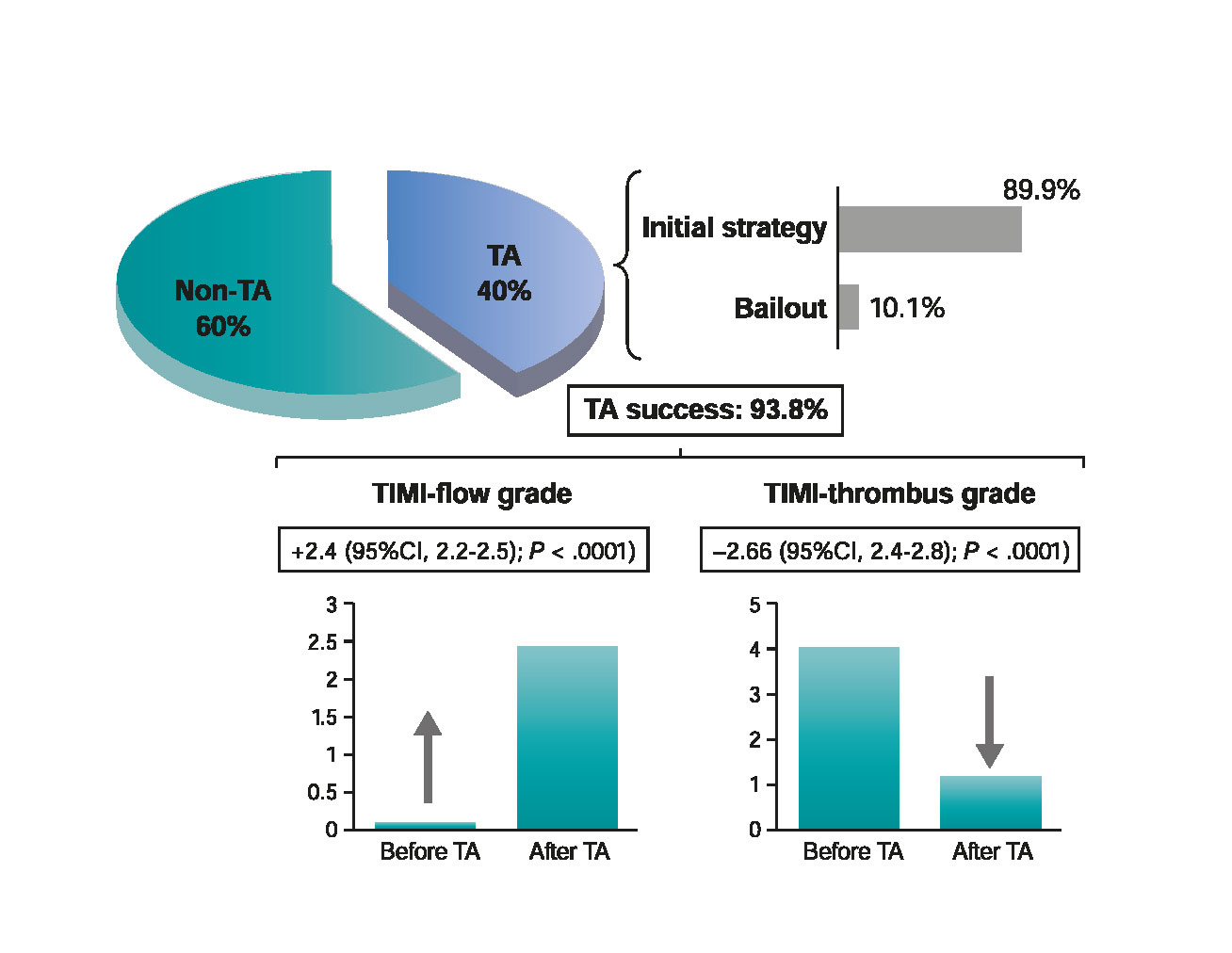
The TA was performed in 40.3% of cases. In 89.9%, the TA was the initial strategy after crossing the culprit lesion with the coronary guidewire, whereas in 10.1% of the cases it was performed as a bailout strategy (figure 3). Procedural characteristics are shown on table 2.
Table 2. Angiographic and procedural characteristics
| TA group n = 250 | Non-TA group n = 437 | P | |
|---|---|---|---|
| Culprit artery | .01 | ||
| LM | 5 (2%) | 2 (0.5%) | |
| LAD | 98 (39.2%) | 209 (47.8%) | |
| LCx | 30 (12%) | 71 (16.2%) | |
| RCA | 114 (45.6%) | 148 (33.8%) | |
| Other | 3 (1.2%) | 1 (0.2%) | |
| Multivessel disease | 107 (42.8%) | 221 (50.6%) | .08 |
| P2Y12 inhibitor | < .0001 | ||
| Clopidogrel | 185 (74%) | 272 (62.2%) | |
| Prasugrel | 15 (6%) | 29 (6.6%) | |
| Ticagrelor | 37 (14.8%) | 119 (27.2%) | |
| Anticoagulation | .69 | ||
| UFH | 245 (96%) | 433 (99%) | |
| Bivalirudin | 2 (0.8%) | 2 (0.45%) | |
| Enoxaparin | 0 (0%) | 1 (0.22%) | |
| Glycoprotein IIb/IIIa inhibitor | .13 | ||
| Abciximab | 91 (36.4%) | 120 (27.5%) | |
| Eptifibatide | 15 (6%) | 18 (4.1%) | |
| Ventricular assist device | 11 (4.4%) | 12 (2.7%) | .24 |
| Initial TIMI-flow | 0.3 ± 0.8 | 1.1 ± 1.3 | < .0001 |
| Initial TIMI-flow 0-1 | 228 (91.2%) | 271 (62%) | < .0001 |
| Initial TIMI-thrombus grade | 4.8 ± 0.9 | 2.5 ± 1.4 | < .0001 |
| Initial TIMI-thrombus grade ≥ 3 | 233 (93.2%) | 191 (43.7%) | < .0001 |
| Initial stent thrombosis (as culprit lesion) | 14 (5.6%) | 7 (1.6%) | .004 |
| Bifurcation (at the culprit lesion) | 62 (24.8%) | 108 (24.7%) | .8 |
| DTB time (minutes) | 101 ± 55 | 102 ± 83 | .8 |
| TA device | |||
| Medtronic Export | 134 (53.6%) | NA | |
| Terumo Eliminate | 96 (38.4%) | NA | |
| Hexacath Recover | 20 (8%) | NA | |
| Direct stenting | 178 (71.2%) | 144 (32.9%) | < .0001 |
| Type of stent | .04 | ||
| Bare metal | 80 (32%) | 108 (24.7%) | |
| Drug-eluting | 170 (68%) | 329 (75.3%) | |
| Stent length (mm) | 29 ± 13.8 | 27.8 ± 14.8 | .29 |
| Stent diameter (mm) | 3.3 ± 0.7 | 3.4 ± 2.2 | .8 |
| Post-dilatation | 43 (17.2%) | 82 (18.8%) | .47 |
| No reflow | 24 (9.6%) | 31 (7.1%) | .24 |
| Distal embolization | 4 (1.6%) | 7 (1.6%) | .97 |
| Angiographic success | 238 (95.2%) | 404 (92.4%) | .16 |
|
DTB, door-to-balloon time; LAD, left anterior descending coronary artery; LCx, left circumflex artery; LM, left main coronary artery; RCA, right coronary artery; TA, thrombus aspiration; TIMI, Thrombolysis in Myocardial Infarction. Data are expressed as no. (%) or mean ± standard deviation. |
|||
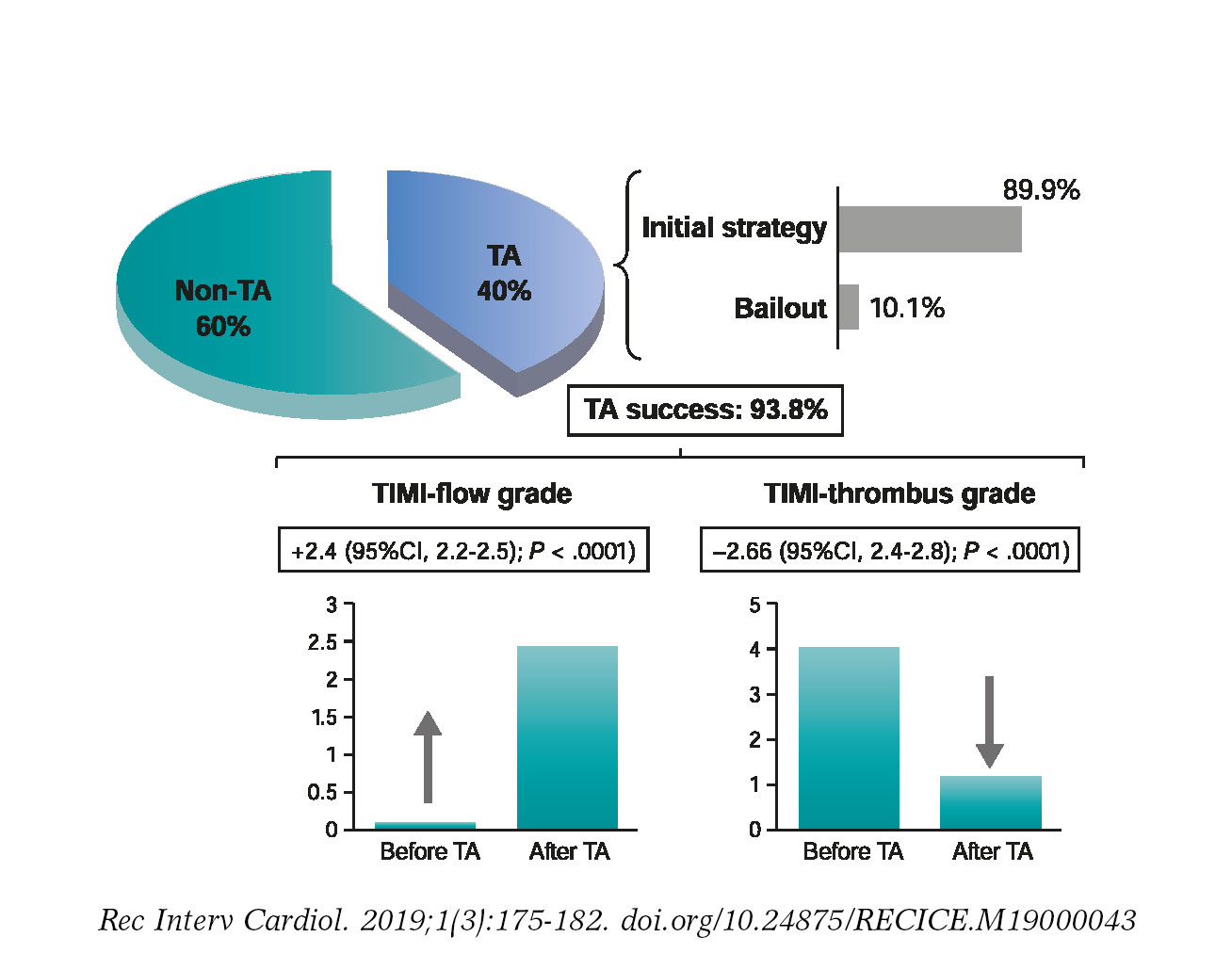
Figure 3. Selective TA performance and beneficial effects during primary percutaneous coronary intervention. Percentage of cases in which TA was used (as an initial or bailout strategy) and TA success rate by improving TIMI-flow or TIMI-thrombus grade. TA, thrombus aspiration; TIMI, Thrombolysis in Myocardial Infarction.
Predictors of use of thrombus aspiration
There were significant differences in the use of TA rates among the different centers (A = 63.7%; B = 32.9%; C = 16.9%; D = 15.7%; P < .0001). The TA was more frequently used as the initial strategy in male patients (40.9% vs 26.4%; P = .003), in current smokers (47.7% vs 36.1%; P = .012), and when the culprit lesion was the thrombosis of a former stent (66.7% vs 36%; P = .004). The rate of TA was also different when it comes to the culprit artery (left anterior descending coronary artery, 31.9%; left circumflex coronary artery, 29.7%; right coronary artery, 43.5%; P = .01). Also, the patients from the non-TA group were treated more often with ticagrelor or prasugrel compared to clopidogrel (P < .0001) and received more frequently drug-eluting stents (TA group, 68% vs non-TA group, 75.3%; P = .04). In the patients from the TA-group, the initial TIMI-flow was significantly lower (0.3 ± 0.8 vs 1.1 ± 1.3; P < .0001) and the initial TIMI-thrombus grade was higher (4.3 ± 0.9 vs 2.5 ± 1.4; P < .0001).
In the multivariate analysis, we included those variables that showed a statistically significant association with TA in the univariate analysis: gender, current smoking habit, culprit artery, P2Y12 inhibitor, initial TIMI-flow, initial TIMI-thrombus grade, initial stent thrombosis (as culprit lesion), center and type of stent. The strongest independent predictor for the use of TA as the initial strategy was a higher initial TIMI-thrombus grade (odds ratio [OR], 3.2; 95%CI, 2.5-3.9; P < .0001). The performance of the pPCI in center A (OR, 20.7; 95%CI, 10-42.5; P < .0001) or B (OR, 3.3; 95%CI, 1.4-7.5; P = .005) was also an independent predictor of TA (compared to center D; the center where the TA was less frequently used). Culprit lesions located at the right coronary artery [OR, 2; 95%CI, 1.008-3.9; P = .047] were also identified as predictors for the use of TA as the initial strategy.
Angiographic results after thrombus aspiration
When TA was performed as initial strategy, a significant improvement of TIMI-flow (2.4; 95%CI, 2.2-2.5; P < .0001) and a significant reduction of TIMI-thrombus grade [2.6; 95%CI, 2.4-2.8; P < .0001] were observed (figure 3). There were no significant differences between both groups in the occurrence of no-reflow phenomenon or distal embolization. The rate of direct stenting was twice as frequent in the TA group. Similarly, the rate of procedural success was high and similar in both groups (TA group, 95.2% vs non-TA group, 92.4%; P = .16) (table 2).
Adverse events at follow-up
After a 1-year follow-up, there were no significant differences in terms of the overall rate of MACE between both groups (TA group, 8% vs non-TA group, 5.7%; P = .24). Also, no differences were seen in any of the individual adverse events: cardiovascular mortality (TA group, 5.2% vs non-TA group, 3.9%, P = .38), myocardial infarction (TA group, 2.4% vs non-TA group, 3.4%; P = .47), stent thrombo- sis (TA group, 2.4% vs non-TA group, 2.3%, P = .9) or target lesion revascularization (TA group, 4.4% vs non-TA group, 4.8%; P = .85). The incidence of cerebral ischemic events was similar in both groups (TA group, 0.4% vs non-TA group, 0.46%; P = .92). One patient only was diagnosed with transient ischemic attack in the TA group that occurred > 30 days after the pPCI. None of the patients of this group suffered a stroke during follow-up. In the non-TA group, two pati- ents suffered a stroke (one was a ischemic stroke 24 hours after the pPCI and the other one was a hemorrhagic stroke that occurred 3 months after the procedure in a patient treated with triple therapy due to atrial fibrillation). There were no differences in the rate of MACE during the first 24 hours after pPCI (TA group, 1.2% vs non-TA group, 1.4%; P = .88) or at the 1-month follow-up (TA group, 3.6% vs non-TA group, 3.9%; P = .9) (figure 4).
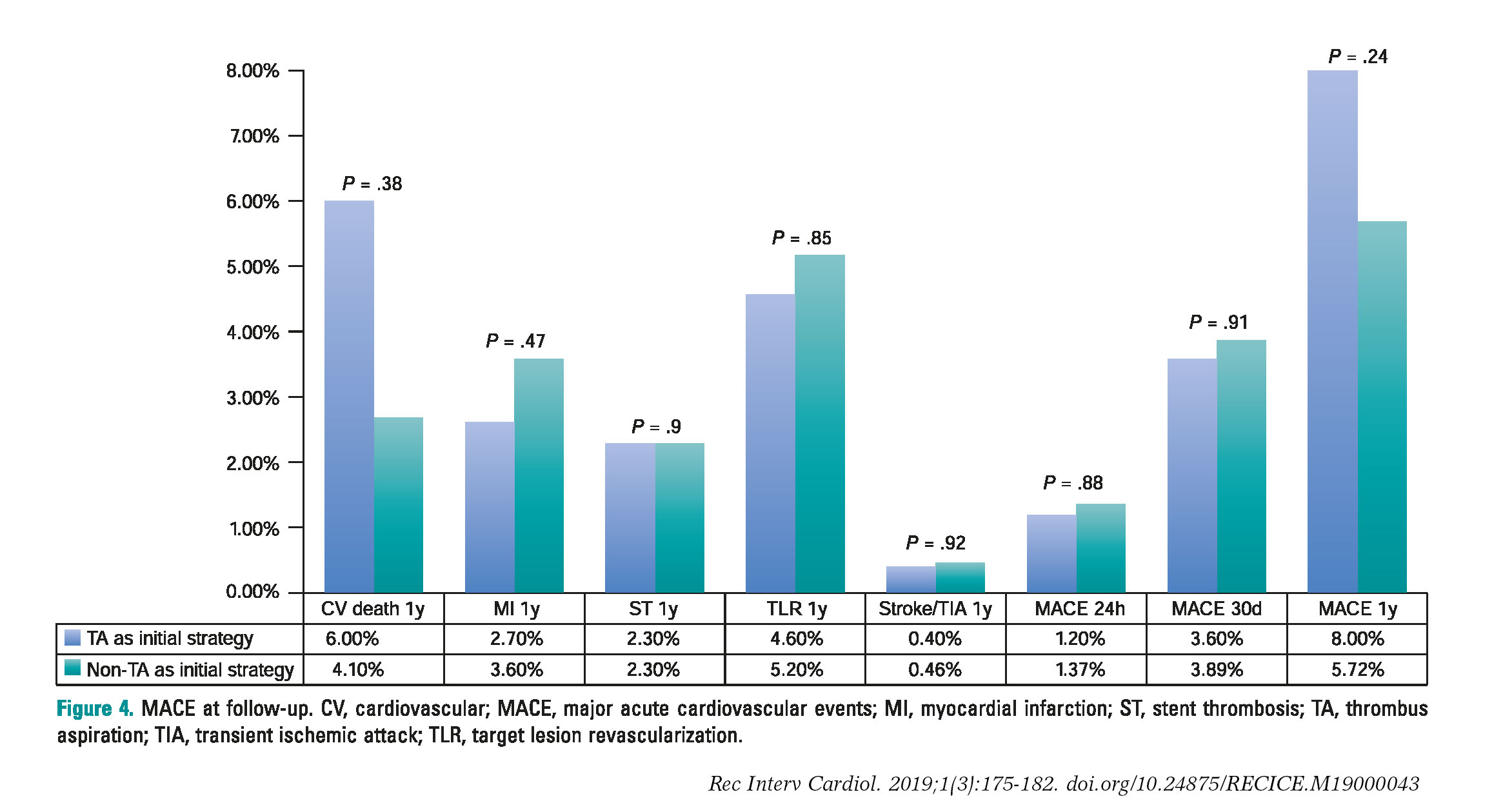
Figure 4. MACE at follow-up. CV, cardiovascular; MACE, major acute cardiovascular events; MI, myocardial infarction; ST, stent thrombosis; TA, thrombus aspiration; TIA, transient ischemic attack; TLR, target lesion revascularization.
DISCUSSION
The main findings of this study are: a) TA is frequently used during pPCI (40.3%), mainly as an initial strategy, with significant differences between the different centers; b) A higher initial TIMI-thrombus grade is the most important predictor for the use of TA; c) TA has a high technical success rate, leading to a significant reduction of the thrombus burden and an improvement of TIMI-flow, facilitating pPCI by allowing more frequently direct stenting; d) TA was not associated with higher rates of cerebrovascular events; and e) The TA was not associated with any differences in the occurrence of MACE during acute phase or at the 1-year follow-up.
The present study analyzes the efficacy and safety of selective TA in the real clinical practice. And this is remarkable for 2 reasons: the most important TA studies4,7,9 assessed the routine use of this technique. Performing routine TAs during pPCI is not the standard in clinical practice, where TA is selectively performed in scenarios where it is expected that this technique will be more effective. Also, some of these trials may have a non-negligible sample selection bias6,7,9 that may not reflect the actual clinical practice. In our study, the average rate of TA use was around 40.3%. This rate was similar in other nationwide registries.15 The most important predictor for the use of TA was a high initial thrombotic burden.
A key finding of this registry is that TA is effective when it comes to facilitating the pPCI. Unlike other studies, we specifically described thrombotic burden reductions and coronary flow improvements after the TA which, in our opinion, are the most representative effects of the utility of this technique. TA success was achieved in 93.8% of the cases. Since this was not a randomized study, it is not easy to analyze the reduction of no-reflow or the rate of distal embolization with TA. This is so because while trying to reflect real practice TA was used at the discretion of the operator and consequently the TA-group had a higher initial thrombus grade (approximately twice as much) compared to the non-TA group (table 2). It is precisely in patients with a higher thrombotic burden where we can expect higher no-reflow or distal embolization rates. However, probably due to this initial TA that allowed significant reductions of the TIMI-thrombus grade, there were no differences in the rates of no-reflow or distal embolization with the non-TA group that had a lower initial thrombus grade.
Also, patients who underwent TA as an initial strategy had a more than two-fold increase in the rate of direct-stenting compared to those treated conventionally. Beyond the potential economic benefit, direct stenting could be associated with clinical benefits.21
As our study suggests it is possible that the greatest benefit of TA occurs when performed selectively in patients with a higher thrombotic burden. This idea has been suggested in a meta-analysis including the most important TA studies.3 These results must be interpreted with caution since a significant percentage of patients who underwent routine TA did not have significant thrombotic loads. In the TAPAS trial, angiographic thrombi were not observed in 51.4% of cases,4 which also happened in 35% of patients included in the TASTE trial.7 The TOTAL study showed that in up to 90% of patients the thrombus scale ≥ 3.9 Nevertheless, the thrombotic burden was assessed before crossing the culprit lesion with the coronary guidewire which probably lead to overestimating the TIMI-thrombus scale18 as 65% of patients showed TIMI 0 flow. In our own opinion this limits the conclusions drawn from this trial and subsequent subanalyses.22
Beyond the effectiveness of TA, our results support the safety of the technique. The TOTAL study9 described a slight increase in the rate of TA-related strokes. This fact was not consistent with previous trials and ignited and ongoing controversy that still goes on. In our study, there were no significant differences in the stroke rate between both groups. These data are similar to those from the TASTE7,8 or INFUSE-AMI trial.23 On this regard, TA-related strokes would initially be of ischemic nature, appear during the procedure, and would be evident during the first 24 hours. It is unlikely that hemorrhagic or ischemic strokes occurring > 24 hours after the procedure would have anything to do with this technique.24 In the TOTAL trial,9 the rate of ischemic strokes during the first 48 hours after the procedure was low and did not significantly differ between arms. Also, in the on-treatment and per-protocol analyses the rate of all-cause stroke at 30 days was no significantly different between groups.
Similar to the TA trials most recently published,7,9 we did not find a significant prognostic benefit associated with TA during the acute phase or at the 1-year follow-up. Despite having repeatedly demonstrated that TA improves reperfusion parameters,4,9 the lack of an association with any prognostic benefits somehow makes sense. First because it is unlikely that a technical tool, designed to facilitate pPCI, can reduce mortality. Secondly, because the low rate of events described (reported in our cohort as in previous studies) make it difficult for an individual therapy to prove significant reductions of mortality rate. Finally, because mortality depends on many more factors that were not analyzed in our study or in these trials.25
Limitations
This is a retrospective, observational study, with the natural limitations of this design. The exclusion of patients who had a cardiac arrest or underwent bailout PCIs may be indicative of selection bias.
The quantification of thrombotic load according to the previously validated TIMI-thrombus scale may not be accurate due to the design of this tool. We have maintained this classification because it is the most widely used in this setting. However, the degree of thrombus before the TA was assessed after crossing the culprit lesion with the angioplasty guidewire in order to reduce the number of cases with initial TIMI-flow = 0 in which it is impossible to assess the initial TIMI-thrombus grade.
We decided to define TA success when achieving improvements of TIMI-flow grade ≥ 1 or reductions of TIMI-thrombus scale grades ≥ 1 without any immediate complications associated with the technique. However, other parameters of microvascular reperfusion such as the ST-segment elevation resolution or the myocardial blush grade were not measured.
The angiographic coronary flow data are not described after the alternative strategy to perform TA in the non-TA group. This can be a limitation since the immediate results cannot be compared to the TA group. Also, the angiographic analysis was not conducted by an independent core-lab that would have added validity to the results.
The high heterogeneity of the operators involved may have influenced the results seen due to their individual preferences in relation to TA. However, we believe that this may play a favorable role in the external validation of our findings.
CONCLUSIONS
Despite being recently discredited, TA is frequently used in current clinical practice during the pPCI, basically as an initial strategy. A higher initial TIMI-thrombus grade is the most important predictor for the use of selective TA. Selective TA facilitate pPCI by reducing thrombotic burden and improving coronary flow. Selective TA is not associated with with a reduction of MACE neither during the acute phase or at the 1-year follow-up. There is no association of TA with a higher stroke rate.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
WHAT IS KNOWN ABOUT THE TOPIC?
- Following the results of several randomized trials, routine TA has remained out of the spotlight after not improving the prognosis of patients with ST-segment elevation myocardial infarction and even increasing their complications.
- Although selective TA may reflect better common practice, we do not have enough data on its implementation.
WHAT DOES THIS STUDY ADD?
- Selective TA is still frequently used in current clinical practice during pPCI, mainly as an initial strategy.
- A higher initial TIMI-thrombus grade is the most important predictor for the use of TA.
- It facilitates pPCI by reducing thrombotic burden and improving coronary flow.
- Selective TA is not associated with a reduction of MACE at 1-year follow-up. There is no association between TA and a higher stroke rate.
REFERENCES
1. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction:a quantitative review of 23 randomised trials. Lancet. 2003;361:13-20.
2. Henriques JP, Zijlstra F, Ottervanger JP, et al. Incidence and clinical significance of distal embolization during primary angioplasty for acute myocardial infarction. Eur Heart J. 2002;23:1112-1117.
3. Jolly SS, James S, Dzavik V, et al. Thrombus Aspiration in ST-Segment-Elevation Myocardial Infarction:An Individual Patient Meta-Analysis:Thrombectomy Trialists Collaboration. Circulation. 2017;135:143-152.
4. Svilaas T, Vlaar PJ, van der Horst IC, et al. Thrombus aspiration during primary percutaneous coronary intervention. N Engl J Med. 2008;358:557-567.
5. Vlaar PJ, Svilaas T, van der Horst IC, et al. Cardiac death and reinfarction after 1 year in the Thrombus Aspiration during Percutaneous coronary intervention in Acute myocardial infarction Study (TAPAS):a 1-year follow-up study. Lancet. 2008;371:1915-1920.
6. Jurado-Roman A, Sanchez-Perez I, Lozano-Ruiz-Poveda F. Letter by Jurado-Roman et al Regarding Article, “Thrombus Aspiration in ST-Segment-Elevation Myocardial Infarction:An Individual Patient Meta-Analysis:Thrombectomy Trialists Collaboration“. Circulation. 2017;135:e1099-e1100.
7. Frobert O, Lagerqvist B, Olivecrona GK, et al. Thrombus aspiration during ST-segment elevation myocardial infarction. N Engl J Med. 2013;369:1587-1597.
8. Lagerqvist B, Frobert O, Olivecrona GK, et al. Outcomes 1 year after thrombus aspiration for myocardial infarction. N Engl J Med. 2014;371:1111-1120.
9. Jolly SS, Cairns JA, Yusuf S, et al.;for the TOTAL Investigators. Randomized trial of primary PCI with or without routine manual thrombectomy. N Engl J Med. 2015;372:1389-1398.
10. Wijns W, Kolh P, Danchin N, et al.;Task Force on Myocardial Revascularization of the European Society (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS), European Association for Percutaneous Cardiovascular Interventions (EAPCI). Guidelines on myocardial revascularization. Eur Heart J. 2010;31:2501-2555.
11. O'Gara PT, Kushner FG, Ascheim DD, et al.;American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction:a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:e362-425.
12. Levine GN, Bates ER, Blankenship JC, et al.;American College of Cardiology Foundation;American Heart Association Task Force on Practice Guidelines;Society for Cardiovascular Angiography and Interventions. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011;58:e44-122.
13. Neumann FJ, Sousa-Uva M, Ahlsson A, et al.;Group ESCSD. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40:87-165.
14. Levine GN, Bates ER, Blankenship JC, et al. 2015 ACC/AHA/SCAI Focused Update on Primary Percutaneous Coronary Intervention for Patients With ST-Elevation Myocardial Infarction:An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention and the 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction. J Am Coll Cardiol. 2016;67:1235-1250.
15. Cid Álvarez AB, Rodríguez Leor O, Moreno R, Pérez de Prado A. Spanish Cardiac Catheterization and Coronary Intervention Registry. 27th Official Report of the Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology (1990-2017). Rev Esp Cardiol. 2018;71:1036-1046.
16. Windecker S, Kolh P, Alfonso F, et al.;Authors/Task Force members. 2014 ESC/EACTS Guidelines on myocardial revascularization:The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014;35:2541-2619.
17. Chesebro JH, Knatterud G, Roberts R, et al. Thrombolysis in Myocardial Infarction (TIMI) Trial, Phase I:A comparison between intravenous tissue plasminogen activator and intravenous streptokinase. Clinical findings through hospital discharge. Circulation. 1987;76:142-154.
18. Sianos G, Papafaklis MI, Serruys PW. Angiographic thrombus burden classification in patients with ST-segment elevation myocardial infarction treated with percutaneous coronary intervention. J Invasive Cardiol. 2010;22:6B-14B.
19. Thygesen K, Alpert JS, Jaffe AS, et al.;ESC Committee for Practice Guidelines (CPG). Third universal definition of myocardial infarction. Eur Heart J. 2012;33:2551-2567.
20. Cutlip DE, Windecker S, Mehran R, et al. Academic Research Consortium. Clinical end points in coronary stent trials:a case for standardized definitions. Circulation. 2007;115:2344-2351.
21. Mahmoud KD, Jolly SS, James S, et al. Clinical impact of direct stenting and interaction with thrombus aspiration in patients with ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention:Thrombectomy Trialists Collaboration. Eur Heart J. 2018;39:2472-2479.
22. Jolly SS, Cairns JA, Lavi S, et al.;TOTAL Investigators. Thrombus Aspiration in Patients With High Thrombus Burden in the TOTAL Trial. J Am Coll Cardiol. 2018;72:1589-1596.
23. Stone GW, Maehara A, Witzenbichler B, et al.;INFUSE-AMI Investigators. Intracoronary abciximab and aspiration thrombectomy in patients with large anterior myocardial infarction:the INFUSE-AMI randomized trial. JAMA. 2012;307:1817-1826.
24. Sabate M, Brugaletta S. Thrombectomy and Stroke:Guilty or Innocent Bystander?J Am Coll Cardiol. 2018;72:1597-1599.
25. Spitzer E, Heg D, Stefanini GG, et al. Aspiration Thrombectomy for Treatment of ST-segment Elevation Myocardial Infarction:a Meta-analysis of 26 Randomized Trials in 11,943 Patients. Rev Esp Cardiol. 2015;68:746-752.
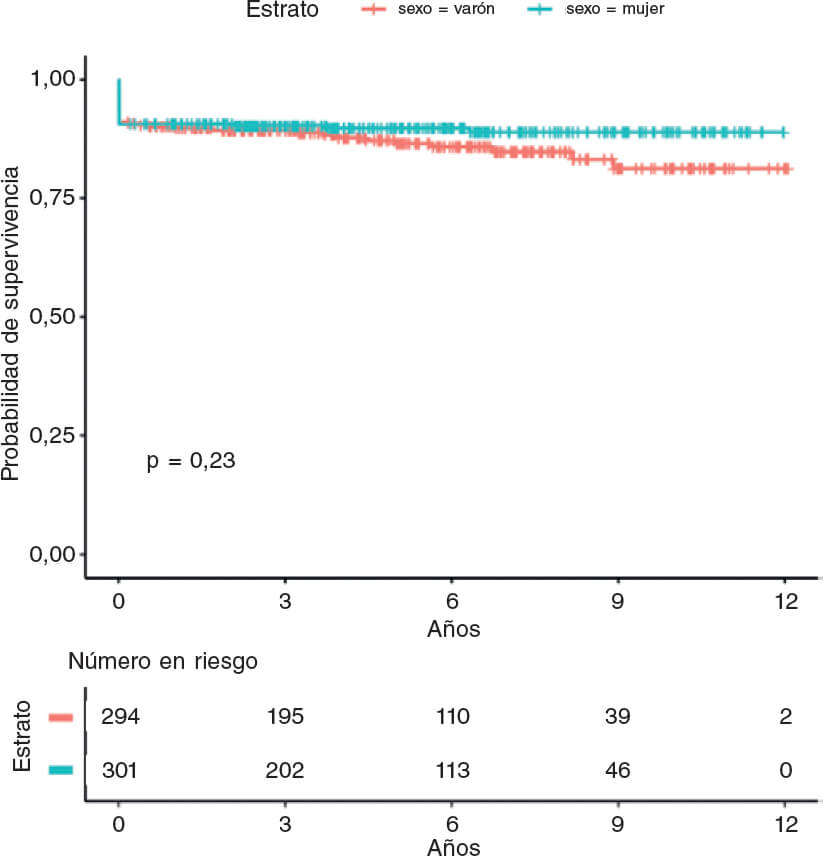
ABSTRACT
Introduction and objectives: Female sex is believed to be a significant risk factor for mortality among patients with ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary interventions (pPCI).
Methods: We collected data on all consecutive STEMI patients treated with pPCI within 12 hours and compared the males vs the females. The primary endpoint was long-term mortality one month after hospital discharge. The secondary endpoint was 30-days mortality.
Results: From March 2006 to December 2016, 1981 patients underwent pPCI at our hospital, 484 (24.4%) were females. Compared with men, women were older (mean age 71.3 ± 11.6 vs 62.9 ± 11.8 years, P < .001), less smokers (26.7% vs 72.7%; P < .001), more diabetic (28.0% vs 22.3%; P < .002), more hypertensive (69.6% vs 61.3%; P < .001), presented more often with shock at baseline (13.2% vs 9.0%; P = .006), had longer symptoms-to-balloon time frames (5.36 ± 3.97 vs 4.47 ± 3.67 hours; P < .001). Also, women were less likely to receive glycoprotein IIb-IIIa inhibitors (59.5% vs 71.4%; P < .001) and stents (79.5% vs 86.6%; P = .01). During the 30-day and long-term follow-up (mean 4.9 ± 3.2 years) the female sex was associated with a higher mortality rate (8.9% vs 4.0%, P < .001 and 23.8% vs 18.4%, P = .01, respectively). After propensity score matching, 379 men and 379 women were selected. Female sex continued to be associated with a higher death rate at 30 days (9.5% vs 5.5%; P = .039) but not in the long term among survivors (25.6% vs 21.4%; P = .170).
Conclusions: Compared to men, women with STEMI undergoing pPCI had higher 30-day mortality rates. However, among survivors, the long-term mortality rate was similar. Even if residual confounding cannot be ruled out, this difference in the outcomes may be partially explained by biological sex-related differences.
Keywords: ST-segment elevation myocardial infarction. Primary angioplasty. Sex differences. Outcomes.
RESUMEN
Introducción y objetivos: El sexo femenino se considera un importante factor de riesgo de mortalidad en el infarto agudo de miocardio con elevación del segmento ST (IAMCEST) tratado con intervención coronaria percutánea primaria (ICPp).
Métodos: Se analizó a todos los pacientes consecutivos con IAMCEST tratados con ICPp dentro de las primeras 12 horas, y se compararon varones y mujeres. El objetivo principal fue la mortalidad a largo plazo en los supervivientes después del primer mes del alta, y el objetivo secundario fue la mortalidad a los 30 días.
Resultados: Desde marzo de 2006 hasta diciembre de 2016 se trató con ICPp 1.981 a pacientes, de los cuales 484 (24,4%) eran mujeres. En comparación con los varones, las mujeres tenían mayor edad (edad media 71,3 ± 11,6 frente a 62,9 ± 11,8 años, p < 0,001) y la frecuencia de fumadoras era más baja (26,7 frente a 72,7%; p < 0,001), mientras que era más alta la frecuencia de diabetes (28,0 frente a 22,3%; p < 0,002), hipertensión arterial (69.6 frente a 61,3%, p < 0,001) y shock al ingreso (13,2 frente a 9,0%; p = 0,006), y más largo el tiempo desde el comienzo de los síntomas hasta la intervención con balón (5,36 ± 3,97 frente a 4,47 ± 3,67 horas; p < 0,001). Además, la frecuencia de tratamiento con inhibidores de la glucoproteína IIb-IIIa (59,5 frente a 71,4%; p < 0,001) y stent (79,5 frente a 86,6%, p = 0,01) fue inferior. Tanto a los 30 días como a largo plazo (media 4,9 ± 3,2 años), el sexo femenino se asoció con una mortalidad más alta (8,9 frente a 4,0%, p < 0,001, y 23,8 frente a 18,4%, p = 0,01, respectivamente). Se seleccionaron 379 mujeres y 379 varones emparejados por puntuación de propensión. Se mantuvo la asociación entre sexo femenino y mayor mortalidad a los 30 días (9,5 frente a 5,5%; p = 0,039), pero no a largo plazo (25,6 frente a 21,4%; p = 0,170).
Conclusiones: En comparación con los varones, las mujeres con IAMCEST tratadas con ICPp tuvieron mayor mortalidad a los 30 días. Sin embargo, entre los supervivientes, la mortalidad a largo plazo fue similar. Aunque no puede descartarse el efecto de variables residuales de confusión, las diferencias en el pronóstico podrían explicarse en parte por diferencias biológicas relacionadas con el sexo.
Palabras clave: Infarto agudo de miocardio con elevacion del segmento ST. Angioplastia primaria. Diferencias por sexo. Pronostico.
Abreviaturas
pPCI: primary percutaneous coronary interventions. STEMI: ST-segment elevation myocardial infarction.INTRODUCTION
Primary percutaneous coronary interventions (pPCI) have proven superior to fibrinolytic therapy for the management of patients with ST-segment elevation myocardial infarction (STEMI)1-3 becoming the treatment of choice in this field.4 However, the question of whether there are any prognostic differences between women and men is still under discussion. Yet despite the fact that in recent studies women exhibit higher mortality rates,5 it is not clear if these differences are associated with worse risk profiles or with a sex-related frailty. Indeed, some studies have not shown any significant relationships between sex and mortality in STEMI, even after adjusting for age and other risk factors.6 Actually, only a limited number of studies have described medium or long-term mortality outcomes and differences in the inclusion criteria (ie, the entire acute coronary syndrome spectrum or only the STEMI subset) and in the therapeutic strategies (ie, medical or interventional) might explain these different findings. The goal of this large, single-center registry was to assess whether in consecutive patients with STEMI undergoing pPCI there were any differences between men and women in the clinical, angiographic, procedural characteristics, and clinical outcome at 30 days or in the long-term.
METHODS
All consecutive patients admitted to our center between January 2006 and December 2016 with a diagnosis STEMI treated with pPCI within 12 hours of symptom onset were recruited. The baseline features (age, sex, burden of cardiovascular risk factors, time from symptoms onset to balloon) were collected along with the procedural characteristics (target vessel, site and type of lesion, pharmacological treatment, thrombus aspiration, type of stent). All interventions were performed following the actual standards of PCI, and the treatment choice was left at the discretion of the operator who performed the procedure. All patients were routinely treated with aspirin (325 mg upon arrival, and then 100 mg daily indefinitely), and an IV bolus of unfractionated heparin (5000 IU). The use of bivalirudin (0.75 mg/kg and 1.75 mg/kg/h at least to the end of the procedure), or unfractionated heparin (100 U/kg or 60 U/kg if abciximab was used) or abciximab was left at the operator’s discretion. When used, the infusion of abciximab was extended for another 12 hours after the procedure. A loading dose of clopidogrel (600 mg), prasugrel (60 mg), or ticagrelor (180 mg) was administered before or immediately after the PCI, unless patients were already on chronic maintenance therapy, and then followed by a maintenance dose of clopidogrel (75 mg once a day), prasugrel (10 mg once a day), or ticagrelor (90 mg twice a day) for 12 months when possible. Repeated revascularization was only performed in the presence of symptom recurrence or proven ischemia related to the treated lesion.
Data on the 30-day follow-up were available for all patients at our center database. Information beyond the first month was collected through outpatient visits, telephone calls or by reviewing any available medical records to obtain the longer follow-up for each patient. All data were entered into a dedicated database.
The men vs women outcomes before and after the propensity score matching were compared. The primary endpoint was long-term mortality after hospital discharge. The secondary endpoint was 30-day mortality rate, 30-day and long-term Bleeding Academic Research Consortium bleeding type ≥ 2.7 Long-term events were evaluated starting from day 31 after discharge until the longer available follow-up. The rate of procedural efficiency (defined a Thrombolysis in Myocardial Infarction [TIMI] III grade flow and residual stenosis < 30%) and ST-segment resolution of more than 50% 60–90 minutes after the PCI was also collected and reported.
Statistical analysis
Quantitative variables were expressed as mean ± standard deviation or median (Q1-Q3), according to the normality of their distribution. Qualitative variables were expressed as frequencies and percentages. The Fisher’s exact test or the chi-square test were used for qualitative variables while the Student’s t test or the Mann-Whitney U test were used for quantitative variables as appropriate. Survival data were represented and analyzed using the Kaplan-Meier curves and the Cox regression analysis. All statistical tests were 2-sided. Results were considered significant if P values < .05. Given the baseline differences between female and male patients and in order to reduce selection bias, we used propensity score matching. The logistic regression model was used based on the baseline and peri-percutaneous coronary intervention characteristics. Thus, P values < .20 were defined to include the selected variables in the final model. The selected variables were age, smoking habit, hypertension, dyslipidemia, diabetes mellitus type 2, obesity, severe chronic renal failure, shock at presentation, cardiac resuscitation at presentation, ejection fraction < 35%, anterior wall myocardial infarct location, femoral access, use of bivalirudin, use of glycoprotein IIb-IIIa inhibitors, percutaneous transluminal coronary angioplasty on the left main coronary artery, use of counterpulsation, thrombectomy, use of drug-eluting stents and total ischemic time. Using these covariates, propensity score was calculated for each patient. Each female patient was matched using 1:1 nearest neighbor matching with a patient from the control group (male) with the same propensity score. The maximum difference (caliper) in the match propensity scores was < 0.15. The standardized mean differences were estimated before and after the matching and balance between both matched cohorts was assessed using the Hotelling T-squared test. Using this technique, 2 comparable groups of 379 patients each were obtained for final analysis. All standardized mean differences after matching were below 10%. Calibration was tested using the Hosmer-Lermeshow test and accuracy was assessed using the area under the ROC curve. Statistical analyses were performed using SPSS 21 statistical software package (IBM software). Propensity score matching was performed using the MatchIt package of R software (version 3.0.2).
RESULTS
From March 2006 to December 2016, among the 1981 patients who underwent pPCIs at our hospital, 484 (24.4%) were females (table 1). Compared to men, women were older (mean age 71.3 ± 11.6 vs 62.9 ± 11.8 years; P < .001), there were fewer female smokers (26.7% vs 72.7%; P < .001), they were more diabetic (28.0% vs 22.3%; P < .002), more hypertensive (69.6% vs 61.3%; P < .001), and they presented more frequently with cardiogenic shock at admission (13.2% vs 9.0%; P= .006). They also had longer symptoms-to-balloon time (5.36 ± 3.97 vs 4.47 ± 3.67 hours; P < .001) and lower left ventricular ejection fractions (46.8 ± 10% vs 48.5 ± 10%; P = .007). Also, as shown on table 2, women were less likely to be treated with glycoprotein IIb-IIIa inhibitors (59.5% vs 71.4%; P < .001), thrombus aspiration devices (48.3% vs 58.0%, P < .001) and stents (79.5% vs 86.6%; P = .01). Procedural efficiency and ST-resolution were significant lower in the female cohort (93.0 vs. 97.1%, P < .001 and 60.0 vs 65.8%, P = .033, respectively, and table 3).
| Raw | Matched | ||||||
|---|---|---|---|---|---|---|---|
| Overall (n = 1981) | Female (n = 484; 24.4%) | Male (n = 1497; 75.6%) | P | Female (n = 379) | Male (n = 379) | P | |
| Age | 65.0 ± 12.3 | 71.3 ± 11.6 | 62.9 ± 11.8 | < .001 | 68.5 ± 11.9 | 69.2 ± 11.6 | .43 |
| Age > 80 years | 262 (13.2) | 134 (27.7) | 128 (8.6) | < .001 | 69 (18.2) | 75 (19.8) | .58 |
| Diabetes mellitusa | 469 (23.7) | 135 (27.9) | 334 (22.3) | .002 | 63 (16.6) | 74 (19.5) | .29 |
| Hypertensionb | 1254 (63.3) | 337 (69.6) | 917 (61.3) | .001 | 227 (59.9) | 240 (63.3) | .33 |
| Dyslipidemiac | 742 (37.5) | 182 (37.6) | 560 (37.4) | .93 | 134 (35.4) | 142 (37.5) | .54 |
| Obesityd | 307 (15.5) | 113 (23.3) | 194 (13.0) | < .001 | 64 (16.9) | 66 (17.4) | .85 |
| Chronic kidney failuree | 53 (2.7) | 17 (3.5) | 36 (2.4) | .19 | 23 (6.1) | 23 (6.1) | 1.00 |
| Smoking (current or former smoker) | 1217 (61.4) | 129 (26.7) | 1088 (72.7) | < .001 | 129 (34.0) | 129 (34.0) | 1.00 |
| Cardiogenic shock at presentation | 198 (10.0) | 64 (13.2) | 134 (9.0) | .006 | 56 (14.8) | 43 (11.3) | .16 |
| Oral intubation | 116 (5.9) | 31 (6.4) | 85 (5.7) | .56 | 26 (6.9) | 23 (6.1) | .66 |
| Cardiac resuscitation at presentation | 21 (1.1) | 8 (1.7) | 13 (0.9) | .14 | 7 (1.8) | 8 (2.1) | .79 |
| Left ventricular ejection fraction (%) | 48.4 ± 10.0 | 46.8 ± 10.0 | 48.5 ± 10.0 | .007 | 47.5 ± 9.4 | 47.3 ± 9.6 | .83 |
| Left ventricular ejection fraction < 35% | 202 (10.2) | 69 (14.3) | 133 (8.9) | .001 | 43 (11.3) | 44 (11.6) | .91 |
| Total ischemia time | 4.7 ± 3.8 | 5.4 ± 4.0 | 4.5 ± 3.7 | < .001 | 4.4 ± 3.7 | 4.6 ± 4.0 | .13 |
| Anterior wall infarct location | 877 (44.3) | 217 (44.8) | 660 (44.1) | .82 | 165 (43.5) | 165 (43.5) | 1.00 |
|
a American Heart Association Guidelines definition. |
|||||||
Table 2. Angiographic and periprocedural features
| Raw | Matched | ||||||
|---|---|---|---|---|---|---|---|
| Overall (n = 1981) | Female (n = 484; 24.4%) | Male (n = 1497; 75.6%) | P | Female (n = 379) | Male (n = 379) | P | |
| Multivessel disease | 1055 (53.3) | 259 (53.5) | 796 (53.2) | .90 | 194 (51.2) | 195 (51.5) | .94 |
| Graft disease | 6 (0.3) | 2 (0.4) | 4 (0.3) | .62 | 1 (0.3) | 2 (0.5) | .56 |
| Radial access | 371 (18.7) | 82 (16.9) | 289 (19.3) | .25 | 58 (15.3) | 57 (15.0) | .92 |
| Use of GP IIb-IIIa | 1357 (68.5) | 288 (59.5) | 1069 (71.4) | < .001 | 251 (66.2) | 242 (63.9) | .49 |
| Bivalirudin | 210 (10.6) | 61 (12.6) | 149 (9.9) | .12 | 35 (9.2) | 45 (11.9) | .24 |
| Multivessel PCI | 93 (4.7) | 25 (5.2) | 68 (4.5) | .57 | 20 (5.3) | 18 (4.7) | .74 |
| PCI on left main coronary artery | 64 (3.2) | 17 (3.5) | 47 (3.1) | .69 | 13 (3.4) | 13 (3.4) | 1.00 |
| Aortic counterpulsation | 251 (12.7) | 69 (14.3) | 182 (12.2) | .23 | 57 (15.0) | 49 (12.9) | .40 |
| Thrombus aspiration | 1102 (55.6) | 234 (48.3) | 868 (58.0) | < .001 | 203 (53.6) | 193 (50.9) | .47 |
| Stent implantation | 1682 (84.9) | 385 (79.5) | 1297 (86.6) | .01 | 314 (82.9) | 318 (83.9) | .58 |
| Drug-eluting stent implantation | 832 (42.0) | 194 (40.0) | 658 (43.9) | .09 | 148 (39.0) | 152 (40.1) | .77 |
|
Values are expressed as mean ± standard deviation or frequencies (percentages). |
|||||||
| Raw | Matched | ||||||
|---|---|---|---|---|---|---|---|
| Overall (n = 1981) | Female (n = 484; 24.4%) | Male (n = 1497; 75.6%) | P | Female (n = 379) | Male (n = 379) | P | |
| Procedural efficacy | 1903 (96.1) | 450 (93.0) | 1453 (97.1) | < .001 | 342 (90.2) | 358 (94.4) | .039 |
| ST-segment resolution > 50% | 1086 (64.4) | 243 (60.0) | 843 (65.8) | .033 | 180 (47.5) | 205 (54.1) | .07 |
| 30-day BARC bleeding type ≥ 2 | 27 (2.1) | 22 (4.5) | 21 (1.4) | .002 | 16 (4.2) | 6 (1.6) | .007 |
| Long-term BARC bleeding type ≥ 2 | 41 (2.1) | 21 (4.3) | 20 (1.3) | < .001 | 13 (3.4) | 7 (1.8) | .257 |
| 30-day mortality rate | 103 (5.2) | 43 (8.9) | 60 (4.0) | < .001 | 36 (9.5) | 21 (5.5) | .039 |
| Overall mortality at long-term follow-up | 390 (19.7) | 115 (23.8) | 275 (18.4) | .01 | 97 (25.6) | 81 (21.4) | .170 |
|
Values are expressed as frequencies (percentages). |
|||||||
At the 30-day and long-term follow-up (mean 4.9 ± 3.2 years, completed in 1634, 82.5% patients) the female sex was associated with a higher mortality rate (8.9% vs 4.0%, P < .001 and 23.8% vs 18.4%, P = .01, respectively) and a higher rate of major bleedings at 30 days (4.5% vs 1.4%; P = .002).
After propensity score matching, 379 men and 379 women were selected. The baseline and peri-procedural characteristics of the propensity-matched pairs were identical (table 1, table 2, figure 1, figure 2, and table 1 and table 2 of the supplementary data). In this cohort, female sex continued to be associated with a lower procedural efficiency (94.4% vs 90.2%; P = .039) and a higher rate of major bleedings and death at 30 days (9.5% vs 5.5%, P = .039 and 4.2% vs 1.6%, P = .007). Conversely, in the matched cohort no significant differences were found in the long-term mortality rate among survivors (25.6% vs 21.4%, P = .170, table 3; and log-rank P = .23, figure 3). The multiple Cox regression analysis revealed that age (hazard ratio [HR], 1.09; (1.06 – 1.12); P < .001), cardiogenic shock at presentation (HR, 6.82 (3.84 – 12.12); P < .001), the left ventricular ejection fraction < 35% (HR, 1.98 (1.11 – 3.54); P = .022) and procedural efficacy (HR, 0.46 (0.23 – 0.89); P = .022) have an effect on mortality when included together with female sex (HR, 0.68 (0.42 – 1.09); P = .106), which is not significant as stated before (table 4).
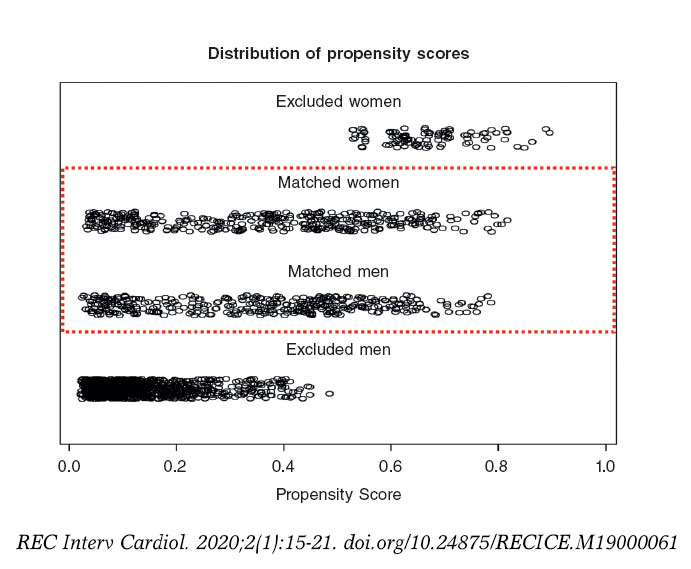
Figure 1. Distribution of propensity scores. Propensity score goes between 0 and 1 and several variables are included in its estimation. It serves as a tool for measuring the similarities among patients. Therefore, matched female and male patients show similar distributions of propensity scores and a wide range, covering all types of patients. Unmatched propensity score units lay on opposite extremes, as expected.
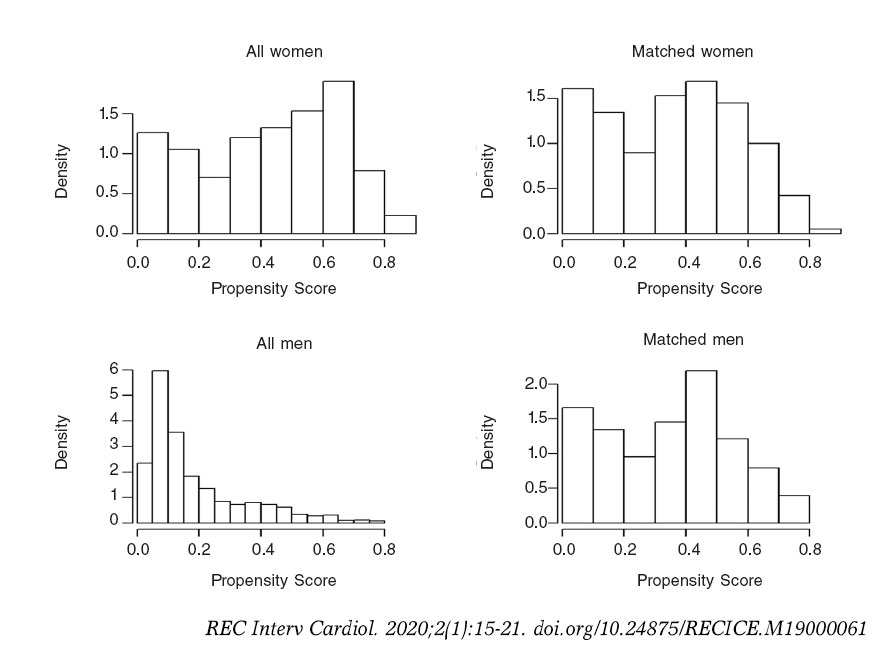
Figure 2. Distribution of propensity score before and after the matching.
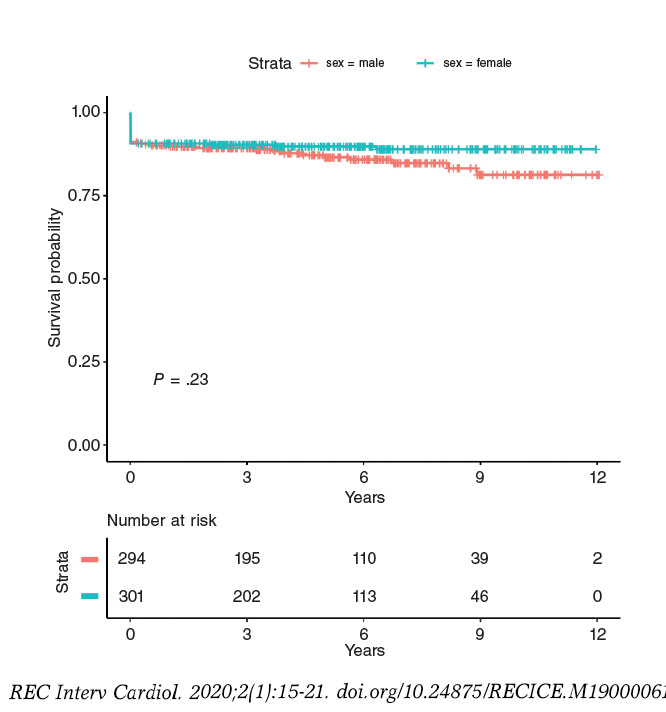
Figure 3. Kaplan-Meier curve for long-term mortality based on sex. There is no difference on the long-term mortality rate between female and male patients in the matched population.
Table 4. Multiple regression analysis
| HR (95%CI) | P | |
|---|---|---|
| Female sex | 0.68 (0.42 – 1.09) | .106 |
| Age | 1.09 (1.06 – 1.12) | < .001 |
| Cardiogenic shock at presentation | 6.82 (3.84 – 12.12) | < .001 |
| Left ventricular ejection fraction < 35% | 1.98 (1.11 – 3.54) | .022 |
| Procedural efficacy | 0.46 (0.23 – 0.89) | .022 |
|
Cox proportional hazard model for overall mortality at long term follow-up. |
||
Main outcome analysis was performed based on a 2-time period (2006-2010 and 2011-2016) without underlining any differences among the groups (table 2 of the supplementary data).
DISCUSSION
Our large single-center registry showed that in a high PCI volume center, women admitted with STEMI undergoing pPCI have a higher 30-day and long-term mortality rate compared to men. This difference persists after propensity score adjustment regarding the 30-day mortality.
A drop in cardiovascular mortality has been observed over the last few decades, but cardiovascular disease is still the leading cause of mortality in women worldwide. Cardiovascular mortality remains higher in women compared to men.5 So far, the reasons of this difference have been mainly justified by the higher prevalence of traditional risk factors (higher mean age, hypertension, diabetes, and renal failure) in the female cohort.6 Also, women who experience myocardial infarction often present with atypical symptoms like dyspnea, fatigue, nausea/vomiting and atypical chest pain, which can lead to delayed diagnosis and treatment.8 Another factor associated with a higher mortality rate to be taken into account is represented by bleeding and mechanical complications, more common in women compared to men.9-11 Our study confirmed all these data: in our population, women were significantly older, with more traditional risk factors (except for smoking), longer ischemic time frames and higher-risk presentations. Also, they had a significantly higher rate of bleeding and mechanical complications.
After propensity score adjustment, out study showed that female sex was independently associated with 30-day but not long-term mortality. These findings are similar to those of a recent large meta-analysis led by Conrotto et al.,12 that included 98 778 patients (73 559 men and 25 219 women) and could be explained, at least in part, by the different pathophysiology of coronary disease in women: the rupture of the plaque surface, the leading cause of coronary occlusion in men, happens only in around 50% of women,13 the remaining percentage being represented by the erosion of the plaque,14 coronary spasm leading to thrombus generation,15 and spontaneous coronary artery dissection.16 Particularly spontaneous coronary artery dissection seems to play an important role in younger women (< 60 years of age) and is associated with a high rate of major adverse cardiac events.17 Therefore, these findings may explain why, in our population, women had lower rate of thrombus aspiration, use glycoprotein IIb-IIIa inhibitors, and stent implantation, which in turn may justify, along with the clinical features, the lower procedural success and ST-segment resolution observed in our study. These factors, associated with the higher rate of bleedings and mechanical complications and other psychological factors, like depression, more prevalent in women compared to men in the general population,18,19 may be phenotypes of a higher frailty in the female sex, and may definitely explain the worse outcomes, at least in the short-term. At long-term, other factors, like the lower in-stent restenosis rate and the resulting lower need for target vessel revascularization observed in women, and already shown in some studies,20-23 may explain the similar outcomes observed in the propensity score analysis.
Limitations
This study has some important limitations; first, even though is a retrospective analysis, it is based on a prospective and dedicated database with propensity score matched analysis. Secondly, data are derived from a single center, which limits their applicability. For example, the use of drug-eluting stents was lower than it is actually is, mainly because the time frame of the study is wide. Actually, from 2006 to 2010 the percentage of drug-eluting stents was about 15% while during the second period (2011-2016), we found 65% of cases with drug-eluting stent implantation. Finally, due to the time frame of the data collection, most procedures were performed via femoral artery access, so we can assume that radial access could have lowered the rate of access bleeding complications, but we need further randomized studies targeted at the female population before being able to validate this hypothesis. However, this is probably a representative sample of an all-comers STEMI population who undergo pPCI in the real world.
CONCLUSIONS
In conclusion, in our single-center cohort of patients and after propensity score adjustment, women with STEMI undergoing pPCI seem to have a higher 30-day mortality rate but similar long-term outcomes after discharge compared to men. Even if residual confounding cannot be ruled out, this difference in the outcomes may be partially explained by biological sex-related differences.
CONFLICT OF INTERESTS
None of the authors have declared any conflicts of interests related to the present article.
WHAT IS KNOWN ABOUT THE TOPIC?
- Women have a higher ACS-related mortality rate but there is no consensus on whether to consider female sex as a risk factor of poor outcomes. This is due to the fact that many authors explain this sex difference by the atypical onset of symptoms in women and the lower recurrence to cath. lab procedures and angioplasties performed in females. However, only a limited number of studies have reported medium or long-term mortality results and even fewer studies have had clear inclusion criteria (ie, the entire acute coronary syndrome spectrum or only the STEMI subset) or reported on the treatment strategies used.
WHAT DOES THIS STUDY ADD?
- Our large single-center registry showed that in a high PCI volume center, women admitted with STEMI to undergo pPCI have a higher rate of 30-day and long-term mortality compared to men. This difference persisted even after propensity score adjustment on the the 30-day mortality, which may be justified by the higher frailty of the female sex, which could in turn explain the worse outcomes seen, at least, in the short-term.
REFERENCES
1. Grines CL, Browne KF, Marco J, et al. A comparison of immediate angioplasty with thrombolytic therapy for acute myocardial infarction. The Primary Angioplasty in Myocardial Infarction Study Group. N Engl J Med. 1993;328:673-679.
2. Schömig A, Kastrati A, Dirschinger J, et al. Coronary stenting plus platelet glycoprotein IIb/IIIa blockade compared with tissue plasminogen activator in acute myocardial infarction. Stent versus Thrombolysis for Occluded Coronary Arteries in Patients with Acute Myocardial Infarction Study Investigators. N Engl J Med. 2000;343:385-391.
3. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction:a quantitative review of 23 randomized trials. Lancet. 2003;361:13-20.
4. Steg PG, James SK, Atar D, et al. Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC). ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2012;33:2569-2619.
5. Mozzafarian D, Benjamin EJ, Go AS, et al. On behalf of the American Heart Association Statistics Committee and Stroke Statistics subcommittee. Heart disease and stroke statistics-2015 update:a report from the American Heart Association. Circulation. 2015;131:e29-e322.
6. Otten AM, Maas AH, Ottervanger JP, et al. Is the difference in outcome between men and women treated by primary percutaneous coronary intervention age dependent?Gender difference in STEMI stratified on age. Eur Heart J Acute Cardiovasc Care. 2013;2:334-341.
7. Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding definitions for cardiovascular clinical trials:a consensus report from the Bleeding Academic Research Consortium. Circulation. 2011;123:2736-2747.
8. Wenger NK. Angina in women. Curr Cardiol Rep. 2010;12:307-314.
9. Lansky AJ, Pietras C, Costa RA, et al. Gender differences in outcomes after primary angioplasty versus primary stenting with and without abciximab for acute myocardial infarction:results of the Controlled Abciximab and Device Investigation to Lower Late Angioplasty Complications (CADILLAC) trial. Circulation. 2005;111:1611-1618.
10. Yu J, Mehran R, Grinfeld L, et al. Sex-based differences in bleeding and long term adverse events after percutaneous coronary intervention for acute myocardial infarction:three year results from the HORIZONS-AMI trial. Catheter Cardiovasc Interv. 2015;85:359-368.
11. Mehran R, Pocock SJ, Nikolsky E, et al. A risk score to predict bleeding in patients with acute coronary syndromes. J Am Coll Cardiol. 2010;55:2556-2566.
12. Conrotto F, D'Ascenzo F, Humphries KH, et al. A Meta-Analysis of Sex-Related Differences in Outcomes After Primary Percutaneous Intervention for ST-Segment Elevation Myocardial Infarction. J Intervent Cardiol. 2015;28:132-140.
13. Falk E, Nakano M, Bentzon JF, et al. Update on acute coronary syndromes:the pathologists'view. Eur Heart J. 2013;34:719-728.
14. Farb A, Burke AP, Tang AL, et al. Coronary plaque erosion without rupture into a lipid core:a frequent cause of coronary thrombosis in sudden coronary death. Circulation. 1996;93:1354-1363.
15. Kawana A, Takahashi J, Takagi Y, et al. Japanese Coronary Spasm Association. Gender differences in the clinical characteristics and outcomes of patients with vasospastic angina:a report from the Japanese Coronary Spasm Association. Circ J. 2013;77:1267-1274.
16. Vrints CJ. Spontaneous coronary artery dissection. Heart. 2010;96:801-808.
17. Tweet MS, Hayes SN, Pitta SR, et al. Clinical features, management, and prognosis of spontaneous coronary artery dissection. Circulation. 2012;126:579-588.
18. Yusuf S, Hawken S, Ounpuu S, et al. INTERHEART Study Investigators. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study):case-control study. Lancet. 2004;364:937-952.
19. Substance Abuse and Mental Health Services Administration. Results from the 2011 National Survey on Drug Use and Health:Mental Health Findings. 2012. Available at:http://www.samhsa.gov/data/sites/default/files/2011MHFDT/2k11MHFR/Web/NSDUHmhfr2011.htm. Consulted 1 Jun 2019.
20. Alfonso F, Hernández R, Bañuelos C, et al. Initial results and long-term clinical and angiographic outcome of coronary stenting in women. Am J Cardiol. 2000;86:1380-1383.
21. Mehilli J, Kastrati A, Bollwein H, et al. Gender and restenosis after coronary artery stenting. Eur Heart J. 2003;24:1523-1530
22. Presbitero P, Belli G, Zavalloni, et al. “Gender paradox“in outcome after percutaneous coronary intervention with paclitaxel eluting stents. EuroIntervention. 2008;4:345-350.
23. Regueiro A, Fernández-Rodríguez D, Brugaletta S, et al. Sex-related Impact on Clinical Outcome of Everolimus-eluting Versus Bare-metal Stents in ST-segment Myocardial Infarction. Insights From the EXAMINATION Trial.Rev Esp Cardiol. 2015;68:382-389
ABSTRACT
Introduction and objectives: This study aims to investigate if the non-invasive assessment of coronary calcium score using multislice cardiac computerized tomography (MSCT) may anticipate the need for elective rotational atherectomy (RA) during percutaneous coronary intervention.
Methods: Patients were considered eligible for the study after receiving a diagnosis of severe coronary stenosis with moderate or severely calcified plaques during index coronary angiography. Those patients underwent the Agatston coronary artery calcium (CAC) score quantification using the MSCT and then underwent percutaneous intervention. Only those lesions considered non-crossable or non-dilatable according to a pre-specified revascularization protocol were treated with RA. All operators were blinded to the MSCT results. According to the study protocol, clinical, angiographic and Agatston-related variables were included in the statistical analysis. Short and long-term outcomes were investigated in both treatment groups during follow-up.
Results: A total of 40 patients were included in the analysis: 20 underwent RA and 20 conventional percutaneous coronary interventions. Most patients were included after suffering from an acute coronary syndrome and had complex coronary anatomy (mean Syntax score, 25 points). The logistic regression analysis showed that creatinine levels and the per-lesion Agatston score were the only predictors of RA. No significant differences were observed regarding in-hospital or long-term procedural outcomes. A novel parameter, the CAC-Cre index, was found to be useful to anticipate the need for RA.
Conclusion: Coronary artery calcification analysis using the Agatston score is a simple technique that improves the non-invasive assessment of complex coronary plaques prior to percutaneous coronary intervention. The per-lesion Agatston score, serum creatinine levels, and the CAC-Cre index may become useful parameters to anticipate the need for elective RAs during percutaneous coronary intervention.
Keywords: Rotational atherectomy. Cardiac computerized tomography. Agatston. Calcium score. Calcified coronary lesions.
RESUMEN
Introducción y objetivos: El objetivo del estudio fue investigar si la evaluación no invasiva del índice de calcificación coronaria mediante tomografía computarizada cardiaca multidetector (TCMD) puede predecir la necesidad de una aterectomía rotacional (AR) electiva durante la intervención coronaria percutánea.
Métodos: Se incluyeron pacientes diagnosticados de estenosis coronaria grave con placas moderadamente o gravemente calcificadas durante la angiografía coronaria. Esos pacientes se sometieron a la cuantificación del índice de calcificación coronaria con la escala de Agatston utilizando TCMD y posteriormente a intervención percutánea. Solo fueron tratadas con AR las lesiones que se consideraba que no era posible cruzar ni dilatar, según un protocolo de revascularización prediseñado. Ninguno de los operadores conocía de antemano los resultados de la TCMD. Según el protocolo del estudio, en el análisis estadístico se incluyeron variables clínicas, angiográficas y relacionadas con la puntuación Agatston. Durante el seguimiento se estudiaron los resultados a corto y largo plazo en ambos grupos.
Resultados: Se analizaron 40 pacientes: 20 que recibieron AR y 20 con intervención coronaria percutánea convencional. La mayoría se incluyó después de un síndrome coronario agudo y tenían una anatomía coronaria compleja (puntuación media de la escala Syntax de 25 puntos). La creatinina y la puntuación de Agatston por lesión fueron los únicos factores predictivos de la AR. No se observaron diferencias significativas en el pronóstico dentro del hospital o a largo plazo. Un nuevo parámetro, el índice CAC-Cre, fue útil para predecir la necesidad de AR.
Conclusion: El análisis de la calcificación de las arterias coronarias mediante la puntuación de Agatston mejora la evaluación no invasiva de las placas coronarias complejas antes de la intervención coronaria percutánea. La puntuación de Agatston por lesión, la creatinina sérica y el índice CAC-Cre son parámetros útiles para predecir la necesidad de una AR electiva durante la intervención coronaria percutánea.
Palabras clave: Aterectomía rotacional. Tomografía computarizada cardiaca. Agatston. Índice de calcificación coronaria. Lesiones coronarias calcificadas.
Abbreviations: CAC: coronary artery calcium. MSCT: multislice cardiac computerized tomography. PCI: percutaneous coronary intervention. RA: rotational atherectomy.
INTRODUCTION
Coronary artery calcium (CAC) is a key marker of coronary artery disease and one of the most robust predictors of cardiovascular adverse events in different populations. Its prevalence increases with age and affects a large percentage of patients over 60 years of age.1
Increased life expectancy in developed countries has led interventional cardiologists to frequently face complex calcified lesions in patients undergoing percutaneous coronary interventions (PCI). This situation remains a challenging scenario due to lower success rate, higher risk of periprocedural complications and need for repeated revascularizations. Occasionally, plaque modification techniques such as rotational atherectomy (RA) are needed to obtain adequate stent expansion and apposition in severely calcified plaques, and they may improve angiographic and clinical outcomes in selected patients. However, the use of RA as a bailout technique may increase procedural time, the amount of contrast media and the incidence of procedural complications. Besides, the assessment of calcification using fluoroscopy only during the coronary angiography has significant limitations and cannot make reliable predictions on what lesions require RA during the intervention.
On the other hand, multislice cardiac computerized tomography (MSCT) improves the non-invasive assessment of coronary calcified lesions. The coronary artery calcium score analysis using MSCT has been related not only to the extension, complexity and severity of the obstructive coronary artery disease, but also to the risk of periprocedural complications after PCI.2,3
The primary objective of this study was to investigate whether accurate quantifications of CAC using MSCT may be useful to anticipate the need for RA during PCI due to calcified coronary lesions. Secondary objectives included the analysis of in-hospital and long-term outcomes.
METHODS
Study patients
Prospective, non-randomized, single-center study at a tertiary cardiac center that performs over 1100 PCI and 10-15 RA procedures per year. Between January 2011 and December 2013, patients undergoing coronary angiography who showed calcified obstructive coronary disease and were considered suitable to undergo PCI were screened to enter the study. All patients who had undergone coronary computerized tomography (CT) scans in the past, with all the inclusion criteria and without any exclusion criteria were enrolled in the present study (table 1 of the supplementary data). The exclusion criteria were: ST-segment elevation acute coronary syndrome within 7 days, previous PCI within 2 months, hemodynamic instability and total coronary occlusions. All the patients included gave their written informed consent, and the protocol was approved by the local ethics committee.
Table 1. Baseline clinical and angiographic characteristics
| RA Group | PCI Group | P | |
|---|---|---|---|
| Age | 72.4 ± 10.6 | 72.8 ± 10.2 | .91 |
| Men | 16 (80%) | 15 (75%) | .70 |
| BMI | 26.7 ± 4.8 | 26.6 ± 4.3 | .96 |
| Hypertension | 14 (70%) | 16 (80%) | .46 |
| Dyslipidemia | 12 (60%) | 17 (85%) | .07 |
| DM | 9 (45%) | 8 (40%) | .93 |
| Current smoker | 12 (60%) | 11 (55%) | .74 |
| Creatinine levels (mg/dL) | 1.64 ± 1.48 | 0.96 ± 0.23 | .05 |
| STEMI | 3 (15%) | 1 (5%) | .5 |
| NSTEMI | 10 (50%) | 10 (50%) | .5 |
| Stable angina | 7 (35%) | 9 (45%) | .5 |
| Previous MI | 4 (20%) | 1 (5%) | .25 |
| Previous PCI | 4 (20%) | 2 (10%) | .25 |
| Previous CABG | 0 (0%) | 1 (5%) | .25 |
| LM disease | 1 (5%) | 2 (10%) | .5 |
| Multivessel disease | 16 (80%) | 19 (95%) | .26 |
| EF < 50% | 2 (10%) | 6 (30%) | .28 |
| Multi-lesion PCI | 15 (75%) | 19 (95%) | .077 |
| New oral antiplatelet agents | 3 (15%) | 1 (5%) | .48 |
| SYNTAX observer A | 25.8 ± 15.7 | 24.4 ± 9.3 | .73 |
| SYNTAX observer B | 26.8 ± 17.2 | 24.4 ± 11.8 | .61 |
|
BMI, body mass index; CABG, coronary artery bypass graft surgery; DM, diabetes mellitus; EF, ejection fraction; LM, left main coronary artery; MI, myocardial infarction; NSTEMI, non-ST-segment elevation myocardial infarction; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction. |
|||
Coronary angiography
Coronary angiography was performed based on our institutional protocol and the indication for PCI was based on clinical criteria. Both the SYNTAX score4 and coronary calcification were independently evaluated by 2 different experienced interventional cardiologists using at least 2 orthogonal fluoroscopic projections. Calcification was defined as an evident density within the arterial wall, visualized in fluoroscopy as a more radiopaque area. The degree of calcification was as follows: 1) moderate: radiopacities noted only during the cardiac cycle before contrast injection; 2) severe: radiopacities noted without cardiac motion before contrast injection usually involving both sides of the arterial lumen.5
Multislice cardiac computerized tomography
The MSCT was performed after the index coronary angiography and prior to the PCI procedure. All operators performing PCI were blinded to the MSCT results. CAC and non-contrast-enhanced coronary CT angiography data sets were acquired using a 64-slice single-source CT system (Aquilion-Toshiba, Medical systems corporation, Otawa, Japan). In order to quantify coronary calcification, the Agatston score was determined using the Vitrea 2 workstation (Vital Images Inc, Plymouth, MN, United States). Collimation was 4 x 3 mm; rotation time was 250 mseg; tube voltage 120 Kv; effective tube current 300 mA. Raw data from the CT scan were reconstructed using algorithms optimized for retrospectively ECG-gated segmental reconstruction with 2 mm slices thickness and at an increment of 2 mm.
Agatston score
The extent of calcification was measured individually for each patient (total calcium score), vessel (per-vessel calcium score), and segment lesion (per-lesion calcium score). Coronary calcium was defined as any plaque of at least 3 contiguous pixels with a density > 130 Hounsfield units. Per-lesion calcium scores were estimated by multiplying the target lesion area by a density factor derived from the maximal Hounsfield units within this area, and as described by Agatston.6 The Bypass Angioplasty Revascularization Investigation (BARI) nomenclature endorsed by 2018 ESC/EACTS Guidelines on myocardial revascularization was used to describe the specific anatomical location of a given coronary lesion.7,8
PCI
According to the previously designed protocol, PCI was performed after MSCT, and all operators were blinded to the study results. Femoral access was considered the preferred artery approach, 7-8 F guiding catheters were used, and intravenous heparin was administered to maintain an activated clotting time ≥ 250 ms. All patients received dual antiplatelet therapy with aspirin and a P2Y12 inhibitor (clopidogrel, ticagrelor, or prasugrel) according to the recommendations established by the clinical practice guidelines. Hydrophilic wires were used to cross the target lesion and predilation with a semi-compliant balloon up to 16 atm (burst rupture pressure) was performed. Non-compliant balloons were not used as most of them had worse crossing profile than semi-compliant at the time of our study. A specific balloon catheter of 15-20 mm in length was selected to meet a ratio of 0.8-1 with the reference diameter vessel by visual estimation. When the balloon did not cross the lesion, it was considered non-crossable. If the ratio between the minimal balloon diameter at 16 atm and the nominal balloon diameter was less than 80%, then the lesion was considered non-dilatable. It is important to explain that currently there is not such a thing as a clear-cut definition of non-dilatable coronary lesions. All non-crossable and non-dilatable lesions underwent RA, and the remaining ones were treated with conventional PCI. Therefore, 2 groups were established, and pre-specified variables were compared (figure 1). Routine use of intravascular ultrasound (IVUS) was not performed in this study due to the difficulties experienced when crossing these types of lesions.
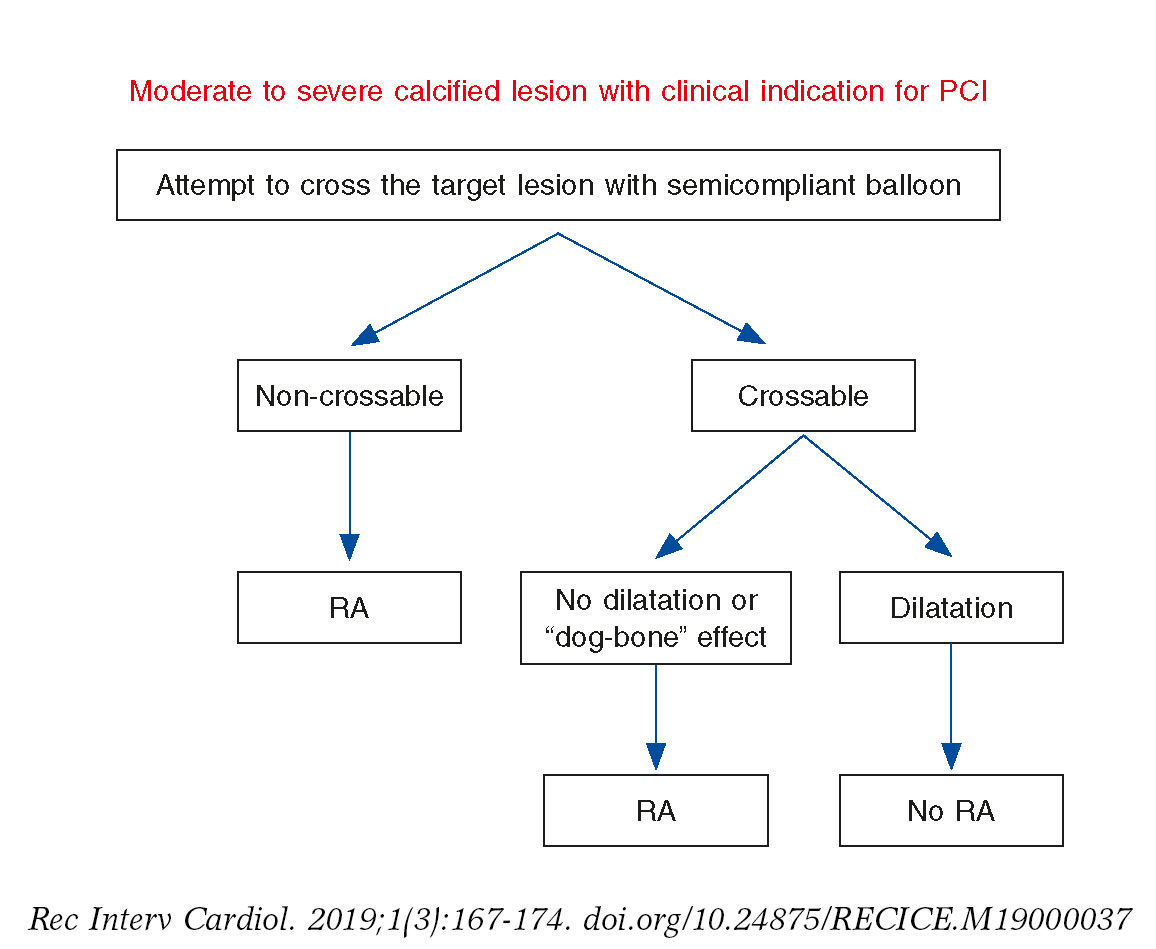
Figure 1. Study revascularization protocol. Lesions were considered non-crossable if a semicompliant dilatation balloon could not pass through them. If the ratio between the minimal balloon diameter at 16 atm and the nominal balloon diameter was less than 80%, the lesion was considered non-dilatable. All non-crossable and non-dilatable lesions underwent rotational atherectomy, and the remaining ones were treated through conventional percutaneous coronary intervention. RA, rotational atherectomy.
Rotablation was performed using the Rotablator (Boston Scientific Corporation; Natick, MA, United States) and burr sizes from 1.25-2.5 mm. The burr size was selected to reach a burr/vessel ratio of 0.7. The recommended burr speed was 165 000-200 000 rpm with each sequence being less than 15 seconds, and care was taken to prevent any drops in the rotational speed > 5000 rpm. Tem- porary pacing was used in cases of rotablation of right coronary artery and dominant left circumflex.
Angiographic success was defined as adequate release and expansion of the stent with a residual stenosis of less than 20% of the target lesion in the presence of Thrombolysis in Myocardial Infarction (TIMI) flow grade 3; non-success was defined as an non-crossable injury or loss of the stent and other complications like dissection, perforation or no reflow.
Follow-up and endpoints
Troponin I levels were obtained 8-10 hours after the intervention and an ECG was performed in all patients the day after the procedure. The primary endpoint was defined as the need to perform RA during the revascularization of target lesions. Secondary endpoints included the incidence of cardiac and non-cardiac events during the index hospitalization and long-term follow up. Follow-up data were collected by phone or using central databases. Death was defined as all-cause mortality. Myocardial infarction was defined as chest pain or other clinical data consistent with myocardial ischemia, new pathologic Q waves in 2 or more contiguous leads or elevated troponin levels 5 times the normal values after the procedure. Target vessel revascularization was defined as either repeated percutaneous or surgical revascularization of the treated vessel, and target lesion revascularization as any reintervention anywhere within the stent implanted during the index procedure, or on the 5 mm proximal or distal edges of the stents. Stent thrombosis was defined following the criteria developed by the Academic Research Consortium.9
Statistical analysis
Categorical variables were expressed as absolute and relative frequencies and compared using the Chi-square test or Fisher’s exact test. Continuous variables were expressed as mean ± standard deviation or, when not normally distributed, as median and interquartile range. The differences among the continuous variables were analyzed using the Student t-test or the Kruskal-Wallis method, respectively. The level of inter-observer agreement was assessed using the Kappa and Phi coefficients. Forward stepwise logistic regression analysis was used to select candidate variables that improved the prediction of RA during PCI, with a statistically significant P value of .05. Receiver operating characteristic (ROC) curve analysis was performed to estimate the sensibility and specificity of the different cut-off points provided by the variables obtained through logistic regression.
RESULTS
Baseline clinical and angiographic characteristics
A total of 40 patients (77.5 % male, 72 ± 10.3 years) were included in the study. The most common indications for index coronary angiography were non-ST-segment elevation acute coronary syndromes (50%) and stable angina with a positive stress test (40%).
The baseline clinical characteristics are shown in table 1. There were no significant differences in the demographic characteristics or antithrombotic regimens between both arms, although there was a trend towards a higher rate of dyslipidemia in the PCI group (P = .077) and worse renal function in the RA group (P = .05).
The Syntax score was high in both treatment groups, without any significant differences between them and a good correlation between the 2 observers (Phi coefficient 0.83, P = .001).
Multislice cardiac computerized tomography
Agatston score was over 3000 in both arms, with no statistically significant differences (P = .24). However, the per-vessel and per-lesion Agatston scores were significantly higher in the RA group (table 2).
Table 2. Coronary artery calcium analysis using Agatston score
| RA Group | PCI Group | P | |
|---|---|---|---|
| Total Agatston score | 3772.0 ± 2154.7 | 3040.4 ± 1693.8 | .240 |
| Per-vessel Agatston score | 1628.5 ± 1142.8 | 833.2 ± 466.0 | .008 |
| Per-lesion Agatston score | 864.1 ± 471.0 | 458.4 ± 360.3 | .004 |
|
PCI, percutaneous coronary intervention; RA, rotational atherectomy. |
|||
Regarding the anatomical distribution of calcium, the vessel with a higher Agatston score was the right coronary artery, showing homogeneous calcification between the proximal and distal segments. The left anterior descending artery was the second most calcified blood vessel, especially at its proximal and middle segments. The circumflex artery had the lowest Agatston score.
Procedural details and outcomes
Procedural details are shown in table 3. Percutaneous access occurred through the femoral artery in 37 patients (92.5%). In 29 patients (72.5%), the target lesion could be crossed by the dilation balloon. Among these 29 crossable lesions, 9 (31%) showed the “dog bone” effect during balloon inflation and could not be dilated. Therefore, according to the study protocol, 20 patients (50%) underwent conventional PCI and the other 20 (50%) RA.
Table 3. Angiographic and procedural characteristics
| RA Group | PCI Group | P | |
|---|---|---|---|
| Location | .17 | ||
| LMCA | 0 | 1 | |
| Proximal LAD | 10 | 6 | |
| Mid LAD | 2 | 8 | |
| Proximal LCx | 3 | 4 | |
| Proximal RCA | 2 | 1 | |
| Mid RCA | 2 | 0 | |
| Ramus Intermedius | 1 | 0 | |
| RVD (mm) | 2.96 ± 0.43 | 2.91 ± 0.26 | .68 |
| Lesion length (mm) | 44.85 ± 17.84 | 41.25 ± 24.13 | .59 |
| Diameter stenosis, % | 79.2 ± 7.9 | 73.0 ± 9.2 | .028 |
| Bifurcation | 6 (46.2%) | 7 (53.8%) | .73 |
| Maximum burr size (mm) | 1.45 ± 0.15 | ||
| No. of stents/lesion | 1.84 ± 0.60 | 2.05 ± 0.89 | .40 |
| Contrast media (mL) | 312.0 ± 96.7 | 239.0 ± 66.5 | .018 |
| Contrast-induced nephropathy | 4 | 0 | .035 |
| Dissections | 2 | 2 | .36 |
| Perforations | 1 | 0 | .56 |
| Intraprocedural major complications | 0 | 0 | > .99 |
| Angiographic success | 90% | 100% | .14 |
| Death | 0 | 0 | > .99 |
| Target vessel re-PCI | 1 | 1 | > .90 |
| Myocardial infarction | 1 | 0 | .31 |
| Access site complications | 2 | 0 | .34 |
|
LAD, left anterior descending artery; LCx, left circumflex artery; LMCA, left main coronary artery; PCI, percutaneous coronary intervention; RA, rotational atherectomy; RCA, right coronary artery; RVD, reference vessel diameter. |
|||
The mean balloon size and length was similar in both arms. Among patients undergoing RA, a single burr was used in most lesions (95%) with a mean burr size of 1.45 ± 0.15 mm. In the entire study population, the most frequently treated artery was the left anterior descending artery (65%); 32.5% of the target lesions were bifurcations; 35 patients (87.5%) had multivessel disease, and 34 (85%) required intervention in more than one major coronary artery. No differences were seen on the target lesion treated no in the number of bifurcation lesions between both groups.
Angiographic success rate was 90% in the RA arm and 100% in the PCI arm, without any significant differences between groups. Coronary dissections, perforations, and no-/slow-flow phenomena were rare and occurred equally in both groups. A significantly larger contrast volume was used in the RA group compared to conventional PCI group.
Stepwise logistic regression analysis showed that creatinine and per-lesion Agatston were the only predictors of RA. For every 0.1mg/dL increase in creatinine level, the probability of RA increased 48%. On the other hand, every 100 point increment in per-lesion Agatston score increased the probability of RA in 22%. Using the optimal cut-off value from ROC analysis (figure 2A), a per-lesion Agatston score of 383 resulted in a sensitivity of 89.5% and specificity of 60% (area under the curve, 0.79). ROC curve for serum creatinine level (figure 2B) showed a sensitivity of 75% and a specificity of 65% for an optimal cut-off point of 1.02 mg/dL (area under the curve, 0.75). Given the association of both variables with the use of RA, we created a combined index of creatinine (Cre) and per-lesion Agatston score (CAC-Cre index), obtained by multiplying the creatinine levels and the per-lesion Agatston score. The ROC analysis of CAC-Cre index (figure 2C) demonstrated better area under the curve (0.86), being 622.79 the value with the best sensitivity (78.9%) and specificity (80%).
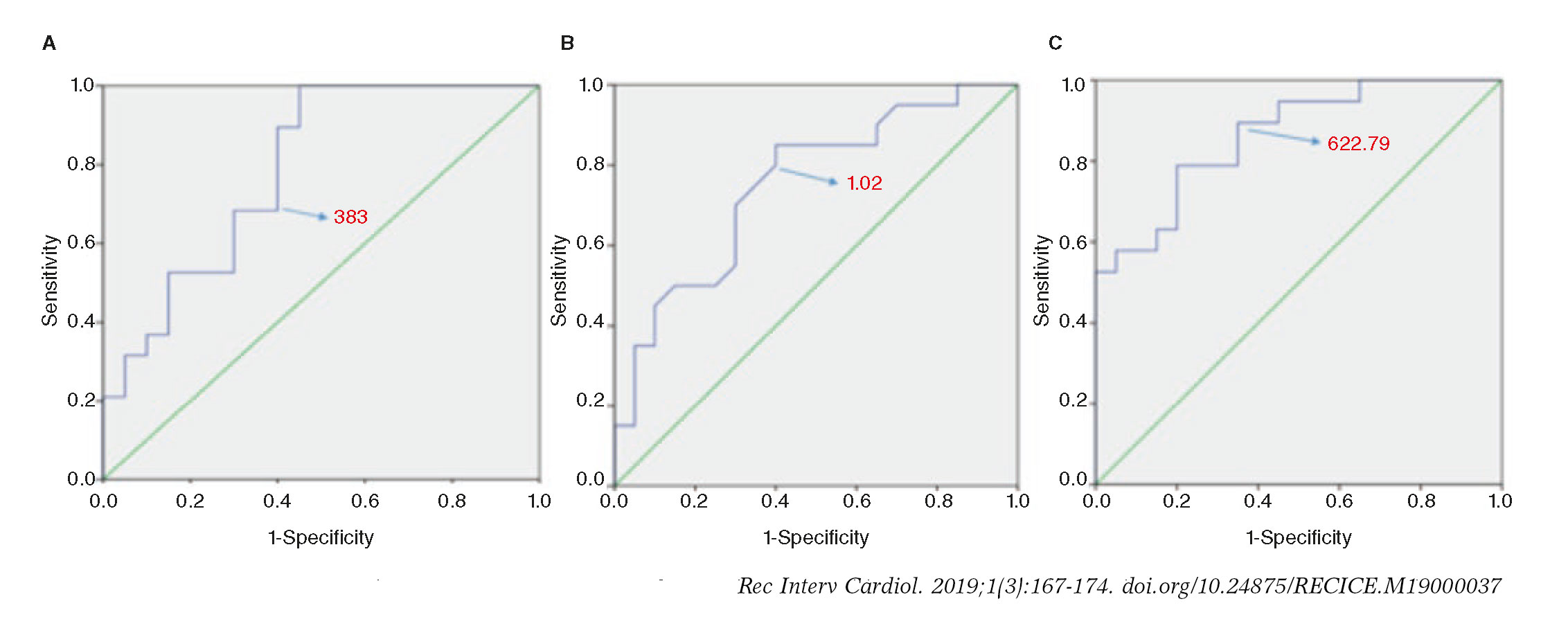
Figure 2. Receiver operating characteristic curve (ROC) for predicting rotablation based on the per-lesion Agatston score (A), the serum creatinine levels (B) and the CAC-Cre index (C). The optimal thresholds for predicting rotablation were 383 per-lesion Agatston points, creatinine levels of 1.02 mg/dL, and a 622.79 CAC-Cre index, respectively.
In-hospital outcomes and long-term follow-up
There were no deaths during hospitalization. Two patients (1 in the RA group and 1 in the PCI group) underwent target vessel revascularization during the index admission. Only 1 patient, included in the RA group, experienced a protocol-defined MI. Complications in the access site were numerically higher in the RA group, without any significant differences. One patient of the PCI group required one intra-aortic balloon pump. On the other hand, the RA group showed a higher incidence of contrast-induced nephropathy (P = .035), possibly due to worse baseline renal function.
There were no differences between the 2 treatment groups regarding major cardiac events at the end of the follow up (4.1 ± 2.2 years) (table 4); with an overall mortality of 12 patients (30%) and 7 cardiovascular deaths (58.3%). Other cardiovascular events such as myocardial infarctions, target-vessel revascularizations and non-target vessel revascularizations, were statistically not-significant. None of the baseline clinical or angiographic variables included in the analysis was associated with the occurrence of major events at follow-up.
Table 4. Major adverse cardiac events during follow-up
| RA Group | PCI Group | P | |
|---|---|---|---|
| Death | 6 (30%) | 6 (30%) | .59 |
| MI | 3 (15%) | 5 (25%) | .34 |
| TLR | 1 (5%) | 3 (15%) | .3 |
| NTLR | 4 (20%) | 5 (25%) | .5 |
|
MI, myocardial infarction; NTLR, non-target lession revascularization; PCI, percutaneous coronary intervention; RA, rotational atherectomy; TLR, target lesion revascularization. |
|||
Regarding the analysis of coronary calcium using the MSCT, a statistically significant correlation was observed between long-term mortality and the total Agatston score (P = .005).
DISCUSSION
Severe coronary artery calcification remains a major challenge in contemporary interventional cardiology. It reduces the chances of angiographic success, and significantly increases the rate of procedural complications.10 The stent underexpansion or asymmetric expansion and malapposition are frequently observed in very calcified plaques; this results in a significantly greater incidence of restenosis and stent thrombosis.11 It is in this context that RA may be useful.12,13
In order to implement the most appropriate revascularization strategy, there is a growing interest in the non-invasive assessment of complex coronary lesions that may benefit from plaque modification techniques.15,16 If we were able to anticipate what patients will require elective RA, we would not have to use this technique as a bailout strategy, thus reducing procedural time, use of contrast media, and the number of ischemic complications.
Fluoroscopy is not useful to adequately quantify coronary calcium, because of its limited sensitivity and significant intra- and interobserver variability, and it has not proven useful either to anticipate the need for RA. Intravascular ultrasound improves the assessment of coronary plaques, providing an accurate evaluation of the amount of calcium in the arterial wall.17 However, it cannot adequately characterize calcium itself, limiting its ability to anticipate the response of a given plaque to balloon catheter dilatation. Another limitation of intravascular ultrasound is the inability to cross many complex lesions with the ultrasound catheter. Although some operators use this situation as a criterion for using RA, there is no clinical evidence that supports such a practice.
In this study we have seen that the Agatston score improves the identification of patients who would benefit from a plaque modification strategy with elective RA. The Agatston score analysis is a sensitive, reproducible and widely available technique that may improve the interventional management of patients with complex coronary lesions. As far as we know, there is only another study that has tested this hypothesis, although with a different methodology. Sekimoto et al.18 studied patients with chronic stable angina who underwent non-invasive angiography and coronary calcium quantification by CT prior to cardiac catheterization. In this study, the decision to perform RA was entirely left to the discretion of the interventional cardiologist.
Our work tried to investigate the use of these parameters both in stable ischemic heart disease and patients after an acute coronary syndrome, selecting a population with significant coronary calcification and high pre-test chances to have calcified circumferential lesions,17 that may perhaps be better treated with RA as the first-line proactive therapy.
Also, our study was designed in such a way that the decision to perform RA was not left at the discretion of the operator, but dictated by the formal prospective protocol. Only non-crossable or non-dilatable lesions with a balloon catheter were treated with RA, which is strictly in accordance with the clinical practice guidelines. This strategy also limits the disparity of criteria among different operators, providing a greater consistency to the study results.
We decided not to perform CT angiography because of its limitations in adequately characterizing the degree of stenosis in patients with significant calcification and also to avoid the use of unnecessary radiation and contrast. Regarding the Agatston calcium score, we selected 3 parameters: global, per-treated vessel and per-lesion or segment. In our study that included patients with complex coronary anatomy, global Agatston values were above 3000 in both treatment arms, with no significant differences between the 2 groups. As in the Japanese study,18 significantly higher values of per-vessel and per-lesion Agatston score were observed in patients who underwent rotational atherectomy. After logistic regression analysis, only the per-lesion score turned out to be an independent predictor of the need for RA. A per-lesion Agatstson score of 383 was the optimal cut-off value determined by the ROC analysis, relatively close to that described by Sekimoto et al.18 An analytical variable, serum creatinine, also turned out to be an independent predictor of RA (chronic renal failure was also significantly higher in the AR group, indicative of a clear clinical association between chronic renal failure and the percentage of intracoronary calcium; something already confirmed in the past). However, ROC curve analysis showed that its use resulted in an optimal classification of the patients. Additionally, we combined both predictors (per-lesion Agatston and serum creatinine) to create an index that would improve the prediction of RA in our patients, being 622.79 the value with the best sensitivity and specificity rate. Therefore, the CAC-Cre index may become useful in the decision-making process at the the cath lab.
Lesion length is one of the characteristics included in the Syntax score that increases complexity during PCI. Sekimoto et al. found that the length of the lesion was significantly associated with the use of RA during the revascularization procedure. In our series, in which the decision to perform rotablation was made following a strict protocol, we found no significant correlations between lesion length and the need for RA. These results are consistent with the findings of Dill et al., who did not observe a significant benefit from routine RA compared to simple angioplasty in patients with complex coronary disease and longer lesions.19
Baseline characteristics were well balanced between both treatment arms, both clinically and in terms of the complexity reflected in the Syntax score. The population included is representative of a subset of patients with severe coronary artery disease who are eligible for PCI in contemporary cardiology centers. In this group, RA showed good angiographic results, with no significant differences between groups during follow-up. Long term incidence of major adverse cardiovascular events was high, but similar to that described by other groups in patients with a similar risk profile.20,21
LIMITATIONS
This is an observational, non-randomized protocol with the corres-ponding limitations of its specific study design. The number of patients included was small, but provided useful information to plan interventions of complex lesions. Defining a lesion as non-dilatable or non-crossable may have a significant component of operator-dependency, and currently there is not such a thing as a clear-cut definition of non-dilatable coronary lesions. Thus, our protocol was designed to be straightforward in order to follow the actual clinical practice guidelines and reduce the inter-operator variability. On the other hand, although the Agatston calcium score is a common technique used in cardiac imaging units all over the world, the per-vessel and per-lesion assessment may require additional time and experienced staff. Selection bias may occur in patients without a CT study during the recruitment period. Also, the fact that this technique is not an indication after performing a diagnostic angiography involves a low use of this technique in the routine clinical practice.
CONCLUSIONS
Coronary artery calcification analysis using Agatston coronary calcium score is a simple technique that improves the non-invasive assessment of complex coronary plaques prior to PCI. The per-lesion Agatston score and the serum creatinine levels may be useful indicators to anticipate the need for elective rotational atherectomy during PCI. A new parameter created by combining both variables, the CAC-Cre index, improved even more the prediction of RA during PCI. A prospective study is needed to validate this index.
CONFLICTS OF INTEREST
R. Moreno is associate editor of REC: Interventional Cardiology. No other conflicts of interest were declared by the authors. The journal’s editorial procedure to ensure impartial handling of the manuscript has been followed.
WHAT IS KNOWN ABOUT THE TOPIC?
- The percutaneous treatment of moderate-to-severely calcified coronary lesions remains a challenge for contemporary interventional cardiologists since choosing the wrong management strategy may lead to severe complications.
- RA is a useful technique that may improve outcomes in non-crossable or non-dilatable coronary lesions, yet its results are not optimal when used as a bailout strategy
- The MSCT-determined Agatston score is the most useful technique for the quantitative assessment of coronary calcium. There is limited information on its role as a predictive tool for the assessment of a particular coronary plaque as non-crossable or non-dilatable.
- To our knowledge, the combination of a clinical variable such as creatinine levels with a CAC variable to create an index to anticipate the need of RA has not previously been reported.
WHAT DOES THIS STUDY ADD?
- In this study we have seen that the Agatston score improves the identification of patients who would benefit from a plaque modification strategy with elective RA.
- A per-lesion Agatstson score of 383 and the serum creatinine levels are independent predictors of RA. We combined both predictors to create an index that improved the prediction of RA in our patients (CAC-Crex index), being 622.7 the value with the best sensitivity and specificity rate..
REFERENCES
1. Wexler L, Brundage B, Crouse J, et al. Coronary Artery Calcification:Pathophysiology, Epidemiology, Imaging Methods, and Clinical Implications. Circulation. 1996;94:1175-1192.
2. Wang X, Liu X, Ge H, et al. Positive association of coronary calcium detected by computed tomography coronary angiography with periprocedural myocardial infarction. PLoS One. 2013;8:8-13.
3. Généreux P, Madhavan MV, Mintz GS, et al. Relation between coronary calcium and major bleeding after percutaneous coronary intervention in acute coronary syndromes (from the Acute Catheterization and Urgent Intervention Triage Strategy and Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction Trials). Am J Cardiol. 2014;113:930-935.
4. Sianos G, Morel MA, Kappetein AP, et al. The SYNTAX score:an angiographic tool grading the complexity of coronary artery disease. EuroIntervention. 2005;1:219-27.
5. Abdel-Wahab M, Richardt G, Joachim Büttner H, et al. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions:The randomized ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) trial. JACC Cardiovasc Interv. 2013;6:10-19.
6. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990;15:827-832.
7. Alderman EL, Stadius M. The angiographic definitions of the Bypass Angioplasty Revascularization Investigation study (BARI). Coron Artery Dis. 1992;3:1189–1207.
8. Nuemann FJ, Sousa Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines of myocardial revascularization. Eur Heart J. 2019;40:86-165.
9. Mauri L, Hsieh W, Massaro JM, Ho KKL, D'Agostino R, Cutlip DE. Stent thrombosis in randomized clinical trials of drug-eluting stents. N Engl J Med. 2007;356:1020-1029.
10. Savage MP, Goldberg S, Hirshfeld JW, et al. Clinical and angiographic determinants of primary coronary angioplasty success. J Am Coll Cardiol. 1991;17:22-28.
11. Liu X, Doi H, Maehara A, et al. A Volumetric Intravascular Ultrasound Comparison of Early Drug-Eluting Stent Thrombosis Versus Restenosis. JACC Cardiovasc Interv. 2009;2:428-434.
12. Moussa I, Di Mario C, Moses J, et al. Coronary Stenting After Rotational Atherectomy in Calcified and Complex Lesions. Circulation. 1997;96:128-136.
13. Vaquerizo B, Serra A, Miranda F, et al. Aggressive plaque modification with rotational atherectomy and/or cutting balloon before drug-eluting stent implantation for the treatment of calcified coronary lesions. J Interv Cardiol. 2010;23:240-248.
14. Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation. 2011;124:e574-651.
15. Hoffmann U, Moselewski F, Nieman K, et al. Noninvasive Assessment of Plaque Morphology and Composition in Culprit and Stable Lesions in Acute Coronary Syndrome and Stable Lesions in Stable Angina by Multidetector Computed Tomography. J Am Coll Cardiol. 2006;47:1655-1662.
16. Estevez-Loureiro R, Ghione M, Kilickesmez K, Agudo P, Lindsay A, Di Mario C. The Role for Adjunctive Image in Pre-procedural Assessment and Peri-Procedural Management in Chronic Total Occlusion Recanalisation. Curr Cardiol Rev. 2014;10:120-126.
17. Tuzcu EM, Berkalp B, De Franco AC, et al. The dilemma of diagnosing coronary calcification:Angiography versus intravascular ultrasound. J Am Coll Cardiol. 1996;27:832-838.
18. Sekimoto T, Akutsu Y, Hamazaki Y, et al. Regional calcified plaque score evaluated by multidetector computed tomography for predicting the addition of rotational atherectomy during percutaneous coronary intervention. J Cardiovasc Comput Tomogr. 2016;10:221-8.
19. Dill T, Dietz U, Hamm CW, et al. A randomized comparison of balloon angioplasty versus rotational atherectomy in complex coronary lesions (COBRA study). Eur Heart J. 2000;21:1759-1766.
20. Édes IF, Ruzsa Z, SzabóG, et al. Clinical predictors of mortality following rotational atherectomy and stent implantation in high-risk patients:A single center experience. Catheter Cardiovasc Interv. 2015;86:634-641.
21. Tohamy A, Klomp M, Putter H, et al. Very Long-Term Follow-Up After Coronary Rotational Atherectomy:A Single-Center Experience. Angiology. 2016;68:519-527.
- Outcomes of percutaneous coronary intervention of chronic total occlusions in heart transplant recipients
- Safety profile of outpatient diagnostic catheterization procedures in patients under direct-acting oral anticoagulants
- 5 year-effectiveness of paclitaxel drug-eluting balloon for coronary in-stent restenosis in a real-world registry
- Intravenous regadenoson versus intracoronary adenosine for fractional flow reserve measurement







Review Articles

Interviews

An interview with Bruno Scheller
aServicio de Cardiología, Hospital Universitario de La Princesa, Instituto de Investigación Sanitaria de La Princesa (IIS-IP), Universidad Autónoma de Madrid, Spain
bCentro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain



