
Article
Ischemic heart disease and acute cardiac care
REC Interv Cardiol. 2019;1:21-25
Access to side branches with a sharply angulated origin: usefulness of a specific wire for chronic occlusions
Acceso a ramas laterales con origen muy angulado: utilidad de una guía específica de oclusión crónica
Servicio de Cardiología, Hospital de Cabueñes, Gijón, Asturias, España
Abstract
Introduction and objectives: To describe the efficacy of the BIOSS LIM C dedicated sirolimus-eluting stent to treat coronary bifurcation lesions, and impact on the bifurcation angle and carina through quantitative coronary angiography.
Methods: Observational prospective study including 124 patients with bifurcation lesions treated with a BIOSS LIM C dedicated sirolimus-eluting stent excluding restenotic lesions and those without main vessel involvement.
Results: The stent was successfully deployed in 121 patients (97.6%) while in 18 (14.5%) double stenting was used. The quantitative coronary analysis has shown proper stent expansion with a mean residual stenosis of 18% in the proximal segment, nearly 0% in the distal segment, and 21% in the side branch. The angiographic results of double stenting showed higher mean diameters (2.12 ± 0.30 vs 1.60 ± 0.42; P < .001), and lower residual stenosis (18.36 ± 9.94 vs 28.49 ± 14.19%, P < .01). Distortion imposed on the bifurcation angulation was minimal with an absolute reduction of 5 degrees (52.8 ± 18.4 vs 47.5 ± 17.2; P = .001).
Conclusions: The dedicated BIOSS LIM C stent has had a very high success rate to treat coronary bifurcation lesions. Angiographic results are good with a remarkably low impact on the native bifurcation angulation, and excellent results from double stenting. We think this can be a very useful device to treat coronary bifurcation lesions with the advantage of easing out the bailout deployment of a second stent into the side branch.
Keywords: Dedicated stent. Bifurcation lesion. BIOSS LIM C sirolimus-eluting stent.
RESUMEN
Introducción y objetivos: El estudio EPIC03-BIOSS se llevó a cabo para describir la eficacia del stent farmacoactivo dedicado BIOSS LIM C en el tratamiento de las lesiones en bifurcación, así como la modificación inducida sobre la lesión en bifurcación por angiografía cuantitativa automatizada.
Métodos: Estudio observacional prospectivo en el que se incluyeron 124 pacientes con lesión en bifurcación tratados con stent farmacoactivo BIOSS LIM C, excluidas las lesiones por reestenosis y aquellas en las que no había afección del vaso principal.
Resultados: El stent se implantó con éxito en 121 pacientes (97,6%); en 18 (14,5%) se utilizó una técnica de 2 stents. El análisis por angiografía cuantitativa automatizada mostró una estenosis residual media del 18% en el segmento proximal, de prácticamente el 0% en el segmento distal y del 21% en la rama lateral. Los resultados angiográficos para la técnica de doble stent muestran unos diámetros (2,12 ± 0,30 frente a 1,60 ± 0,42 mm; p < 0,001) y estenosis residuales (18,36 ± 9,94 frente a 28,49 ± 14,19%; p < 0,01) significativamente mejores. La distorsión sobre la angulación nativa del vaso resultó mínima, con una reducción absoluta de unos 5° (52,8 ± 18,4 frente a 47,5 ± 17,2°; p = 0,001).
Conclusiones: El stent BIOSS LIM C consigue una elevada tasa de éxito para el tratamiento de las lesiones en bifurcación. Los resultados angiográficos son buenos, destacando la escasa distorsión sobre la angulación nativa del vaso y los excelentes resultados. Consideramos que puede ser un buen dispositivo para el tratamiento de las bifurcaciones, la ventaja de poder facilitar la implantación no prevista de un segundo stent.
Palabras clave: Stent dedicado. Lesión en bifurcación. Stent liberador de sirolimus BIOSS LIM C.
Abbreviations
MB: main branch; OCT: optical coherence tomography; POT: proximal optimization technique; QCA: quantitative coronary angiography: SB: side branch.
INTRODUCTION
Percutaneous treatment of coronary bifurcation lesions can represent up to 20% of all coronary lesions treated.1 The definition of bifurcation lesion given by the European Bifurcation Club2 includes those that effect a relevant side branch (SB) whether by its angiographic diameter or the myocardium at risk associated with such SB.
The pseudo-fractal anatomy of coronary bifurcation lesions3 involves a significant caliber difference between proximal and distal segments. The study of the structural limits of tubular stents has favored the development of treatment techniques4,5 designed to optimize implantation in an anatomy that is not completely cylindrical with good angiographic and clinical results.6-10 Also, a progressive escalated strategy has been agreed based on parameters of damage to the SB from the provisional stenting technique to the complex double stenting one.
Although specific platforms have been designed to treat coronary bifurcation lesions, these have been limited for expert operator use only. On the one hand, dedicated stents can be categorized into stents designed to treat the main vessel by securing proper access to the SB, (Nile Croco & Pax, Minvasys, France, the Multi-Link Frontier, Abbott Vascular Devices, United States or the TAXUS Petal, Boston Scientific, United States). On the other hand, stents designed to treat the SB first to later complete the main branch (MB) with a tubular stent (Tryton Side Branch stent, Tryton Medical, United States; Sideguard, Cappella Inc, United States). However, because of the discrete results reported or their complexity, they have not become entirely popular.
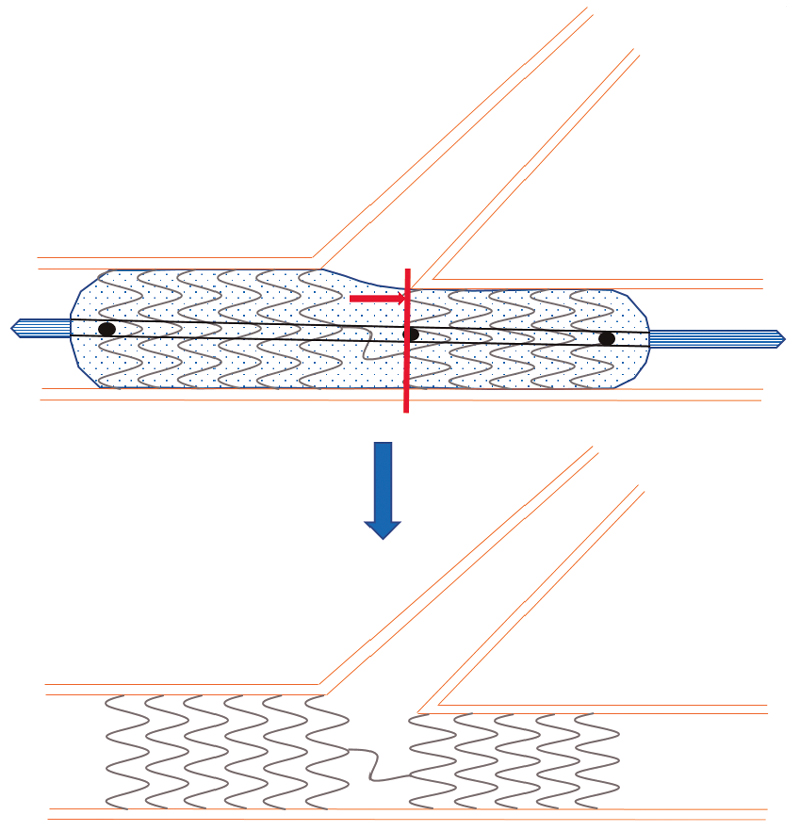
The BIOSS LIM C stent11 (Balton, Poland) is a 70 µm ultra-thin-strut chrome-cobalt platform with a sirolimus-eluting biodegradable polymer of polylactic acid. It is a dedicated stent for bifurcations that consists of 2 segments of different size linked by 2 long connective struts (figure 1). Goal is to keep the pseudo-fractal correlation between the proximal and distal portions of the SB and facilitate the technique to access the SB or the provisional stenting technique. Former studies have given good results with successful implantation rates of 100%, and target lesion revascularization rates from 6.8% to 9.8%.12-14

Figure 1. Image of the BIOSS stent design. Note the structure in 2 bodies with central space for the side branch.
The objective of this study is to describe immediate angiographic results assessed through quantitative coronary angiography (QCA) in terms of deformation of the lesion native angulation and expansion, especially at the level of the polygon of confluence and at the origin of the side branch.
METHODS
Patients
This is a prospective, multicenter registry started by independent investigators that included patients with ischemic heart disease referred for percutaneous coronary revascularization of a bifurcated lesion considered as a lesion with distal branches with a minimum diameter of 2 mm.
Patients with lesions damaging the bifurcation on the SB only were excluded. Also, patients with restenosis, complete total coronary occlusions, a contraindication for dual antiplatelet therapy, cardiogenic shock, minors or patients who gave their express rejection to be included.
Study was conducted according to the Declaration of Helsinki and the study protocol was approved by the different ethics committees of participant centers. The specific written informed consent was obtained from all the patients included in the study.
Procedure
Stenting was performed following the implantation recommendations of every device (figure 2) by implanting and performing the final control in the angiographic view with better deployment of bifurcation. Anticoagulation with sodium heparin or low-molecular weight heparin was administered according to the usual standards of every cath lab. Specific treatment of each coronary bifurcation lesion was left to the operator’s criterion. Predilatation of both branches, the provisional stenting technique or the early double stenting technique were allowed whenever, at least, 1 dedicated stent from the study was used.
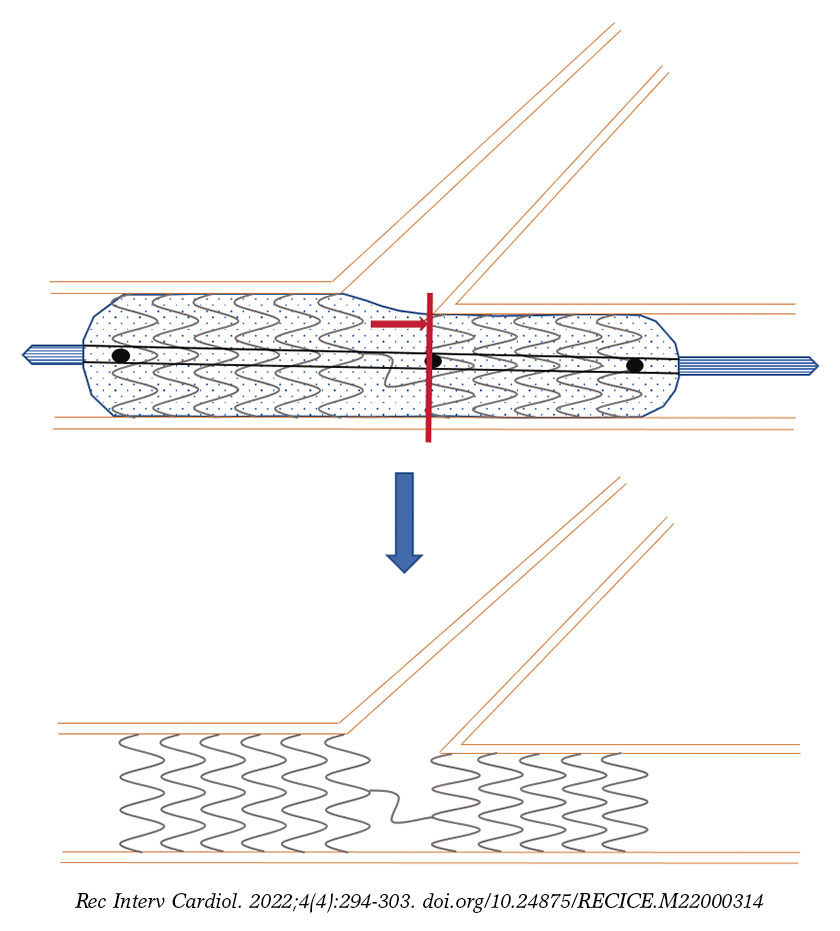
Figure 2. Scheme of the positioning of the BIOSS stent for correct implantation. Central marker needs to be adjusted to the carina of bifurcation, and the ostium of the distal main branch.
Procedural success was defined as the implantation of a BIOSS LIM C stent into the bifurcation lesion with residual stenosis on visual estimate < 30% in the MB and 50% in the SB.
Clinical follow-up
Telephone or on-site follow-up was conducted at 30 days and 12 months. Patients were surveyed on adverse cardiovascular events of death, myocardial infarction, stroke, stent thrombosis, need for new revascularization or bleeding.
Angiographic analysis
Angiographic analysis was conducted independently by an imaging lab (BARCICORE-Lab, Spain) using a specific dedicated software for bifurcations (QAngio XA 7.3, The Netherlands) with which all angiographic measurements were acquired including the measurements of bifurcation angulation. Two analysts selected the images before and after implantation without the intracoronary guidewire and in the same view (< 10º of difference). Angiographic analysis was conducted in end-diastole following the lab internal protocols.
Software used allows us to measure the 3 segments of a bifurcation simultaneously (proximal MB, distal MB, and SB) and obtain individual results from all the segments including the polygon of confluence of bifurcation. All analyses were conducted taking the proximal and distal borders of the stent deployed as the reference framework. When the double stenting technique was used, the distal border of the stent implanted into the SB was used as the analysis distal limit. In case of single-stent implantation, only the proximal 5 mm of the SB were used. Figure 3 shows an example of angiographic analysis.
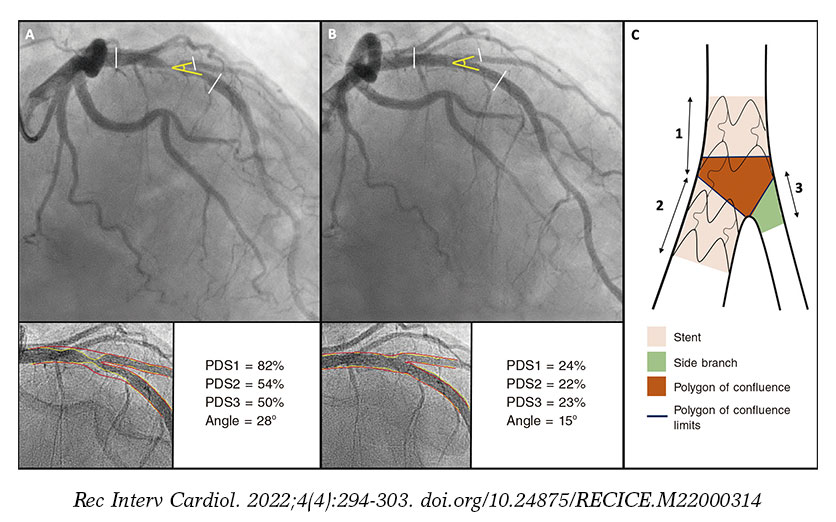
Figure 3. Quantitative coronary angiography showing the percentage diameter stenosis (PDS) at the proximal main vessel (1), distal main vessel (2), and 5 mm proximal to the side branch (3) before (A) and after the procedure (B). Also, it measures changes to the bifurcation angle between the distal branches. Image C shows the limits of each segment (1, 2, and 3), and the borders of the polygon of confluence.
Statistical analysis
All quantitative data are expressed as mean ± standard deviation (SD) while qualitative data are expressed as number (percentage). For the quantitative angiographic analysis (QCA) between angiographic values before and after implantation, Student t test was used for paired data (quantitative data) while the McNemar test (qualitative data) was used when appropriate. For comparison purposes between the cohorts treated with provisional stenting and double stenting, Student t test or the Mann-Whitney U test (quantitative data) were used. Also, the chi-square test or Fisher’s exact test (qualitative data) were used, when appropriate. P values ≤ .05 were considered statistically significant. Statistical analyses were conducted using the statistical software package SPSS version 20.
RESULTS
Baseline clinical data
From August 2018 through February 2021 a total of 124 patients were included in the study (figure 4). The demographic data of patients are shown on table 1. We should mention the rates of patients with diabetes [26.9% (32/124)], and acute coronary syndrome [52,8% (66/124)], 12,8% (16/124) of whom had ongoing ST-segment elevation. No significant differences were reported in the baseline clinical characteristics between the single-stent and the double stenting cohorts.
Table 1. Description of population
| Total | |
|---|---|
| Baseline demographics | 124 |
| Feminine sex | 23 (18.47%) |
| Age | 65.48 (11.09) |
| Arterial hypertension | 79 (63.2%) |
| Dyslipidemia | 72 (57.6%) |
| Diabetes Mellitus | 32 (25.6%) |
| On insulin | 8 (6.4%) |
| Current smoker | 39 (31.2%) |
| Chronic kidney disease | 10 (8%) |
| Peripheral vasculopathy | 8 (6.4%) |
| Baseline treatment | |
| Acetylsalicylic acid | 81 (64.8%) |
| Clopidogrel | 34 (27.2%) |
| Ticagrelor | 18 (14.4%) |
| Prasugrel | 2 (0.6%) |
| Oral anticoagulant drugs | 9 (7.2%) |
| Vitamin K inhibitor | 1 (0.8%) |
| Direct-acting oral anticoagulants | 8 (6.4%) |
| Indication | |
| Stable angina | 37 (29.6%) |
| Silent ischemia | 12 (9.6%) |
| Ventricular dysfunction | 3 (2.4%) |
| STEACS | 6 (4.8%) |
| NSTEACS/unstable angina | 16 (12.8%) |
| NSTEACS/myocardial infarction | 34 (27.2%) |
| STEACS | 16 (12.8%) |
| AMI | 25 (20%) |
| Previous CABG | 4 (3.2%) |
| Previous PCI | 29 (23.2%) |
| Ejection fraction (%) | 54.31 (12.29) |
| Atrial fibrillation | 9 (7.2%) |
| Heart failure | 16 (12.8%) |
|
AMI, acute myocardial infarction; CABG, coronary artery bypass graft; NSTEACS, non-ST-segment elevation acute coronary syndrome; PCI, percutaneous coronary intervention; STEACS, ST-segment elevation acute coronary syndrome. |
|
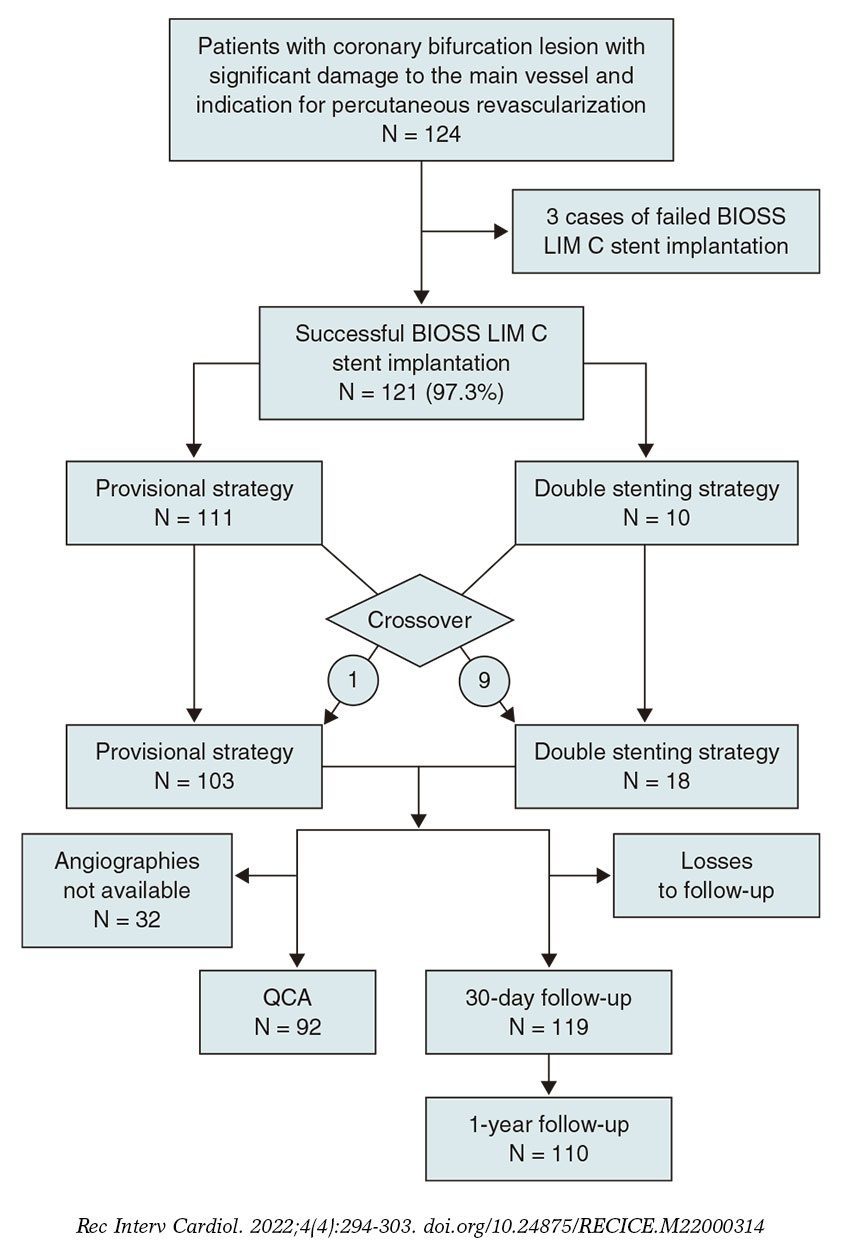
Figure 4. Flowchart of the EPIC03-BIOSS study. QCA, quantitative coronary angiography.
Angiographic and procedural data
Angiographic and procedural data are shown on table 2 and table 3. Most procedures were performed via radial access (120, 96.8%) and the angiography revealed the presence of 3-vessel coronary artery disease in 19 patients (15.3%). In 10 cases (8%) the target lesion was found in the left main coronary artery. Regarding complexity, in 55 cases (44.3%) the lesions treated fell into the B2/C categories of the American Heart Association/American College of Cardiology while 32 lesions (25.8%) were categorized as moderate or severe.
Table 2. Angiographic data on visual estimate
| Total | Provisional | Complex | P | |
|---|---|---|---|---|
| Radial access | 120 (96%) | 110 (97.3%) | 10 (90.9%) | .314 |
| LMCA lesion | 11 (8.8%) | 10 (8.8%) | 1 (9.1%) | .830 |
| Proximal LAD | 77 (61.6%) | 71 (62.8%) | 6 (54.5%) | .746 |
| Coronary artery disease | .524 | |||
| 1 vessel | 55 (44%) | 51 (46.4%) | 4 (36.4%) | |
| 2 vessels | 47 (37.6%) | 43 (39.1%) | 4 (36.4%) | |
| 3 vessels | 19 (15.2%) | 16 (14.5%) | 3 (27.3%) | |
| Right dominance | 109 (87.2%) | 99 (87.6%) | 10 (90.9%) | .773 |
| Damaged bifurcation | .693 | |||
| LMCA-LAD/LCX | 10 (8%) | 8 (7.3%) | 2 (18.2%) | |
| LAD/Diagonal | 71 (56.8%) | 53 (57.5%) | 4 (54.6%) | |
| LCX/OMA | 28 (22.4%) | 25 (22.2%) | 3 (27.3%) | |
| RCA/PL | 15 (12.0%) | 15 (13.2%) | 0 (0%) | |
| Medina classification | .001 | |||
| 100 | 8 (6.4%) | 8 (7.3%) | 0 (0%) | |
| 010 | 18 (14.4%) | 18 (15.9%) | 0 (0%) | |
| 001 | 0 (0%) | 0 (0%) | 0 (0%) | |
| 110 | 38 (30.4%) | 38 (33.6%) | 0 (0%) | |
| 101 | 5 (4%) | 5 (4.4%) | 0 (0%) | |
| 011 | 10 (8%) | 6 (5.3%) | 4 (36.4%) | |
| 111 | 44 (35.2%) | 38 (33.6%) | 6 (54.5%) | |
| True | 59 (47.2%) | 49 (43.3%) | 10 (100%) | |
| Calcification (moderate or severe) | 32 (25.6%) | 28 (24.8%) | 4 (36.4%) | .542 |
| Proximal tortuosity | 25 (20%) | 20 (17.7%) | 5 (45.5%) | .04 |
| Thrombus | 15 (20%) | 14 (12.4%) | 1 (0.9%) | 1.000 |
| Type of lesion | .362 | |||
| A | 3 (2.4%) | 3 (2.7%) | 0 (0%) | |
| B1 | 37 (29.6%) | 31 (27.4%) | 6 (54.5%) | |
| B2 | 45 (36%) | 43 (38.1%) | 2 (18.2%) | |
| C | 10 (8%) | 10 (8.8%) | 0 (0.0%) | |
|
LAD, left anterior descending coronary artery; LCX, left circumflex artery; LMCA, left main coronary artery; OMA, obtuse marginal artery; PL, posterolateral; RCA, right coronary artery. |
||||
Table 3. Procedural description and follow-up
| Total | Provisional | Complex | P | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Procedure | 124 | 106 (85.5%) | 18 (14.5%) | |||||||
| Early strategy | 124 | 113 (90.4%) | 11 (9.6%) | |||||||
| Guide catheter | .289 | |||||||||
| 6-Fr | 113 (90.4%) | 104 (92%) | 9 (81.8%) | |||||||
| 7-Fr | 10 (8%) | 8 (7.1%) | 2 (18.2%) | |||||||
| 8-Fr | 1 (0.8%) | 1 (0.9%) | 0 (0%) | |||||||
| SB predilatation | 100 (80%) | 90 (79.6%) | 10 (90.9%) | .690 | ||||||
| Rotational atherectomy | 0 (0%) | 0 (0%) | 0 | 1.000 | ||||||
| Stenting | 121 (97.6%) | 111 (98.2%) | 10 (90.9%) | .314 | ||||||
| Length of stent | 19.73 (3.23) | 19.57 (3.21) | 21.45 (3.04) | .064 | ||||||
| POT | 33 (26.6%) | 30 (26.5%) | 3 (27.3%) | .800 | ||||||
| SB dilatation | 47 (37.9%) | 43 (38.1%) | 4 (36.4%) | .449 | ||||||
| Kissing after stenting the MB | 21 (44.7%) | 21 (48.8%) | 0 (0%) | |||||||
| SB dilatation only | 26 (55.3%) | 22 (51.2%) | 4 (100%) | |||||||
| Additional stenting | 17 (13.7%) | 16 (14.2%) | 1 (9.1%) | |||||||
| Stent into the SB | 18 (14.5%) | 9 (8%) | 9 (81.8%) | .000 | ||||||
| Kissing after stenting the SB | 16 (88.9%) | 7 (77.8%) | 9 (100%) | |||||||
| Imaging modalities | 11 (8.9%) | 8 (7.1%) | 3 (27.3%) | .023 | ||||||
| IVUS | 9 (7.3%) | 7 (6.2%) | 2 (18.2%) | |||||||
| OCT | 2 (1.6%) | 1 (0.9%) | 1 (9.1%) | |||||||
| Complications | 1 (0.8%) | 1 (0.9%) | 0 | |||||||
| Occlusion of the SB | 1 (0.8%) | 1 (0.9%) | 0 (0%) | |||||||
| Success (lack of stenosis ≥ 50%) | 114 (91.2%) | 104 (92%) | 10 (90.9%) | .338 | ||||||
| TIMI-flow grade at MB | .638 | |||||||||
| 3 | 114 (91.9%) | 103 (91.2%) | 11 (100%) | |||||||
| 2 | 0 (0%) | 0 (0%) | 0 (0%) | |||||||
| 1 | 3 (2.4%) | 3 (2.7%) | 0 (0%) | |||||||
| TIMI-flow grade at SB | .638 | |||||||||
| 3 | 114 (91.9%) | 103 (91.2%) | 11 (100%) | |||||||
| 2 | 0 (0%) | 0 (0%) | 0 (0%) | |||||||
| 1 | 3 (2.4%) | 3 (2.7%) | 0 (0%) | |||||||
| MB stenosis | 3.27% (6.14) | 3.24% (6.25) | 3.57% (4.76) | .892 | ||||||
| SB stenosis | 14.74% (19.94) | 15.55% (20.45) | 4.29% (4.5) | .211 | ||||||
| ≥ 50% stenosis of MB | 0 (0%) | 0 (0%) | 0 (0%) | 1.000 | ||||||
| ≥ 50% stenosis of SB | 7 (7.1%) | 7 (7.7%) | 0 (0%) | .585 | ||||||
| ≥ 30% stenosis of SB | 22 (22.4%) | 22 (24.2%) | 0 (0%) | .158 | ||||||
| 12-month follow-up | 110 (88.7%) | 92 (86.8%) | 18 (100%) | |||||||
| Death | 0 (0%) | 0 (0%) | 0 (0%) | |||||||
| Stent related AMI | 2 (1.8%) | 1 (1.1%) | 1 (5.5%) | .223 | ||||||
| Re-PCI | 6 (5.4%) | 5 (5.4%) | 1 (5.5%) | .555 | ||||||
| Thrombosis | 1 (0.9%) | 0 (0%) | 1 (5.5%) | .115 | ||||||
|
AMI, acute myocardial infarction; IVUS, intravascular ultrasound; OCT optical coherence tomography; POT, proximal optimization therapy; Re-PCI, re-percutaneous coronary intervention; SB, side branch; MB, main branch; TIMI, Thrombolysis in Myocardial Infarction. |
||||||||||
When we analyzed the differences between the cohorts treated with the provisional stenting technique and the double stenting one (table 2 and table 3) we saw that in the latter the rate of true bifurcations, proximal tortuosity, and use of imaging modalities was significantly higher.
During the procedure (table 3) the BIOSS LIM C stent was successfully implanted in 121 patients (97.6%). In the 3 cases when the stent was not implanted, the lesions showed moderate or severe calcification and proximal tortuosity. One case out of the 121 treated with stenting became complicated with SB occlusion following a dissection that could not be revascularized. In 30 (26.5%) out of the 113 cases (90.4%) where the early provisional stenting strategy was used, the POT (proximal optimization technique) was used. In 43 (38.1%) it was necessary to dilate the SB through kissing-balloon or simple dilatation (table 3). Finally, in 9 cases (7.2%) initially treated with the single-stent strategy, a second stent was needed in the SB. The double stenting strategy was initially adopted in 11 patients (9.6%). However, after SB dilatation and stent implantation into the MB the implantation of a second stent was deemed as unnecessary in 2 of them (18.2%). Therefore, 18 patients (14.5%) were eventually treated with the double stenting technique. The rates of predilatation, rotational atherectomy, use of POT, and successful implantation were similar in both cohorts.
Quantitative angiography of bifurcation
The angiographic images of 92 patients were available (table 4). Mean residual stenosis of 18% was seen in the proximal segment and nearly 0% in the MB distal segment. In the SB, the postoperative mean residual stenosis was 21% with significant residual stenosis in 5% of all patients treated with the provisional stenting technique.
Table 4. Quantitative coronary angiography of bifurcation in the entire cohort. Comparison between simple and double stent
| N = 92 lesions | Entire population (N = 92) | 1-stent technique (N = 75) | 2-stent technique (N = 17) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Pre | Post | P | Pre | Post | P | Pre | Post | P |
| Minimum lumen diameter, mm | 0.97 ± 0.48 | 1.70 ± 0.44 | < .001 | 0.99 ± 0.48 | 1.60 ± 0.42 | < .001 | 0.85 ± 0.47 | 2.12 ± 0.30 | < .001 |
| Maximum percentage diameter stenosis, % | 62.78 ± 17.70 | 26.62 ± 14.03 | < .001 | 61.63 ± 17.92 | 28.49 ± 14.19 | < .001 | 67.86 ± 16.25 | 18.36 ± 9.94 | < .001 |
| Carinal angle, degrees (º) | 52.8 ± 18.4 | 47.5 ± 17.2 | .001 | 52.3 ± 13.4 | 46.4 ± 18.1 | .002 | 55.3 ± 13.3 | 51.9 ± 12.5 | .161 |
| Proximal main branch | |||||||||
| Length, mm | 11.15 ± 5.28 | 10.86 ± 5.22 | .154 | 11.56 ± 5.59 | 11.21 ± 5.53 | .155 | 9.06 ± 2.50 | 8.97 ± 2.69 | .776 |
| Reference lumen diameter, mm | 3.83 ± 1.13 | 3.88 ± 0.80 | .674 | 3.65 ± 0.98 | 3.84 ± 0.71 | .089 | 4.75 ± 1.42 | 4.10 ± 1.12 | .066 |
| Minimum lumen diameter, mm | 1.63 ± 0.85 | 2.96 ± 0.62 | < .001 | 1.60 ± 0.77 | 2.85 ± 0.46 | < .001 | 1.78 ± 1.15 | 3.50 ± 0.93 | < .001 |
| Percentage diameter stenosis, % | 55.36 ± 20.81 | 18.09 ± 10.34 | < .001 | 54.12 ± 20.78 | 19.44 ± 10.01 | < .001 | 61.16 ± 20.58 | 11.77 ± 9.78 | < .001 |
| Binary stenosis (SD ≥ 50%), N (%) | 58 (63.0) | 0 | < .001 | 45 (60.0) | 0 | < .001 | 13 (76.5) | 0 | < .001 |
| Distal main branch (BIOSS) | |||||||||
| Length, mm | 10.35 ± 5.36 | 9.96 ± 5.46 | .190 | 10.61 ± 5.69 | 10.28 ± 5.76 | .105 | 9.13 ± 3.24 | 8.66 ± 3.43 | .082 |
| Reference lumen diameter, mm | 2.33 ± 0.45 | 2.34 ± 0.42 | .797 | 2.29 ± 0.45 | 2.32 ± 0.42 | .547 | 2.49 ± 0.39 | 2.42 ± 0.40 | .409 |
| Minimum lumen diameter, mm | 1.19 ± 0.56 | 2.28 ± 0.36 | < .001 | 1.24 ± 0.56 | 2.27 ± 0.37 | < .001 | 0.99 ± 0.53 | 2.34 ± 0.30 | < .001 |
| Percentage diameter stenosis, % | 48.43 ± 23.07 | 0.12 ± 15.00 | < .001 | 46.67 ± 22.98 | -0.62 ± 15.06 | < .001 | 60.61 ± 19.77 | 3.40 ± 14.74 | < .001 |
| Binary stenosis (SD ≥ 50%), N (%) | 43 (46.7) | 0 | < .001 | 31 (41.3) | 0 | < .001 | 12 (70.6) | 0 | < .001 |
| Side branch | |||||||||
| Length, mm | 6.32 ± 3.81 | 6.27 ± 3.47 | .689 | 5.20 ± 0.99 | 5.21 ± 0.89 | .905 | 11.58 ± 6.88 | 11.25 ± 6.08 | .549 |
| Reference lumen diameter, mm | 2.18 ± 0.48 | 2.22 ± 0.49 | .199 | 2.12 ± 0.46 | 2.16 ± 0.42 | .268 | 2.42 ± 0.51 | 2.49 ± 0.71 | .536 |
| Minimum lumen diameter, mm | 1.41 ± 0.64 | 1.75 ± 0.52 | < .001 | 1.46 ± 0.57 | 1.62 ± 0.43 | .022 | 1.19 ± 0.88 | 2.31 ± 0.50 | < .001 |
| Percentage diameter stenosis, % | 34.16 ± 27.52 | 20.94 ± 19.14 | < .001 | 30.06 ± 25.34 | 24.35 ± 17.13 | .070 | 52.24 ± 30.19 | 5.88 ± 20.77 | < .001 |
| Binary stenosis (SD ≥ 50%), N (%) | 22 (23.9) | 5 (5.4) | < .001 | 13 (17.3) | 5 (6.6) | .044 | 9 (52.9) | 0 | < .001 |
|
PDS, percentage diameter stenosis. |
|||||||||
Comparing patients treated with the single-stent technique or the double stenting technique (table 4) revealed that, at proximal segment level, expansion results are better with the double stenting technique with residual stenosis of 11% (vs 19% with the single-stent) although starting from greater baseline reference diameters (3.65 ± 0.98 vs 4.75 ± 1.42). The double stenting technique showed excellent results on the SB with a significantly greater minimum lumen diameter (2.31 ± 0.50 vs 1.62 ± 0.43, P = .01), and minimum residual stenosis of 5.9% (vs 24.3% with the provisional stenting technique) with special attention to the lack of stenosis > 50%. Results were similar in the distal segment.
Quantitative angiography of the polygon of confluence
At the polygon of confluence (table 5) results show residual stenoses of 17.15% ± 10.96% at the polygon core, and 19.21% ± 20.56% for the ostium of the SB. When the provisional stenting and double stenting techniques were compared (table 5), data from the QCA show better minimum lumen diameters for the double stenting technique in the bifurcation core and the ostium of the SB, and almost identical for the ostium of the distal segment.
Table 5. Quantitative coronary angiography. Polygon of confluence. Comparative between simple and double stent
| N = 92 lesions | Provisional technique (N = 75) | Double stenting technique (N = 17) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | P | Pre | Post | P | Pre | Post | P | |
| Bifurcation core | |||||||||
| Reference lumen diameter, mm | 4.04 ± 1.13 | 3.97 ± 0.80 | .531 | 3.83 ± 0.97 | 3.88 ± 0.69 | .618 | 4.82 ± 1.34 | 4.35 ± 1.10 | .095 |
| Minimum lumen diameter, mm | 2.09 ± 0.94 | 3.28 ± 0.78 | < .001 | 1.87 ± 0.72 | 2.93 ± 0.49 | < .001 | 2.25 ± 0.98 | 3.63 ± 0.90 | < .001 |
| Percentage diameter stenosis, % | 48.49 ± 17.94 | 17.15 ± 10.96 | < .001 | 47.57 ± 18.23 | 18.76 ± 10.68 | < .001 | 52.39 ± 15.70 | 10.31 ± 9.63 | < .001 |
| Binary stenosis (SD ≥ 50%), N (%) | 46 (50.0) | 0 | < .001 | 35 (46.7) | 0 | < .001 | 11 (64.7) | 0 | .001 |
| Distal main branch ostium (BIOSS) | |||||||||
| Reference lumen diameter, mm | 2.34 ± 0.45 | 2.35 ± 0.43 | .842 | 2.29 ± 0.45 | 2.32 ± 0.42 | .544 | 2.55 ± 0.40 | 2.48 ± 0.43 | .406 |
| Minimum lumen diameter, mm | 1.38 ± 0.53 | 2.40 ± 0.37 | < .001 | 1.40 ± 0.50 | 2.39 ± 0.36 | < .001 | 1.32 ± 0.67 | 2.45 ± 0.41 | < .001 |
| Percentage diameter stenosis, % | 40.59 ± 21.36 | -3.67 ± 15.54 | < .001 | 38.61 ± 20.61 | -4.57 ± 15.76 | < .001 | 48.95 ± 23.07 | 0.13 ± 14.37 | < .001 |
| Binary stenosis (SD ≥ 50%), N (%) | 34 (37.0) | 0 | < .001 | 23 (30.7) | 0 | < .001 | 11 (64.7) | 0 | .001 |
| Side branch ostium | |||||||||
| Reference lumen diameter, mm | 2.21 ± 0.50 | 2.24 ± 0.51 | .280 | 2.14 ± 0.46 | 2.17 ± 0.41 | .375 | 2.51 ± 0.56 | 2.57 ± 0.72 | .553 |
| Minimum lumen diameter, mm | 1.56 ± 0.52 | 1.80 ± 0.55 | < .001 | 1.58 ± 0.47 | 1.65 ± 0.45 | .219 | 1.47 ± 0.71 | 2.40 ± 0.52 | < .001 |
| Percentage diameter stenosis, % | 28.21 ± 21.77 | 19.21 ± 20.56 | .004 | 24.91 ± 20.30 | 23.13 ± 17.97 | .501 | 42.19 ± 22.82 | 2.58 ± 22.99 | < .001 |
| Binary stenosis (SD ≥ 50%), N (%) | 16 (17.4) | 5 (5.4) | .012 | 9 (12.0) | 5 (6.7) | .267 | 7 (41.2) | 0 | .016 |
|
PDS, percentage diameter stenosis. |
|||||||||
Bifurcation angle (table 4) showed a slight change after stenting with a statistically significant reduction from 52.8 ± 18.4 º down to 47.5 ± 17.2º (P = .001). In the double stenting cohort, angulation modification was similar—in absolute terms—with a reduction of some 4º. However, this difference was not statistically significant (table 4). No significant correlation between the degree of angulation modification and the SB residual stenosis was reported (P = .86).
Clinical outcomes
Only 1 procedural complication was reported consisting of the occlusion of the SB in a patient treated with the provisional stenting technique that could not be solved. No major clinical events, cases of stent thrombosis or target lesion revascularization were reported at 30 days.
One year after implantation, 110 patients (88.7%) were contacted. A case of definitive device thrombosis (0.91%) was reported at 1-year follow-up especially in a case of double stenting treated with primary angioplasty. This case added to other 5 cases of new target lesion revascularization due to restenosis (4.54%) reveal a 12-month rate of target lesion failure of 5.45%. Two of these restenoses were found in the ostium of the SB and the remaining 3 were in the main vessel. No deaths and 3 infarctions (2.72%) were reported all of them associated with the device in relation to stent thrombosis and, in the other 2 cases, due to restenosis with minimum mobilization of troponin.
DISCUSSION
The study main findings are: a) the BIOSS LIM C dedicated stent has a high rate of success at 30 days in patients with complex coronary bifurcation lesions; b) such device is basically used with the provisional stenting strategy and is associated with a very reduced need for stenting in the SB; c) immediate angiographic outcomes show the proper behavior from the stent in the 3 bifurcation segments, as well as in the polygon of confluence where the contact surface between the stent and the artery is minimum.
Demographic data confirm that this is a non-selected population with a prevalence of risk factors, comorbidities, heart disease, and anatomical characteristics of the lesions we see in the routine clinical practice of any cath lab these days.
The device had a high rate of implantation success that was consistent with the easiness of its design being successfully implanted in > 97% of the cases. Success rate is similar to that reported in most studies with tubular stents used in bifurcations, something unreported in previous series of dedicated stents (Axxess, Frontier, and Nile studies). For example, the Frontier stent15 had a rate of restenosis of nearly 29.9%. The Nile stent16,17 was successfully used in tortuous arteries and distal segments with acceptable results with a rate of target lesion revascularization of 8.4%. However, it required distribution of angiographic stenosis focused on the carina. The self-expandable Axxess stent18 showed favorable results with a 1-year rare of cardiovascular events and restenosis of 7.7% and 6.4%, respectively. Nonetheless, it only treated the polygon of confluence and the segment immediately proximal to the ostia of the branches. Also, it was limited to certain angles and lengths needing, on many occasions, the use of additional stents.
In 14.5% of the cases, the double stenting technique was used. This is a dedicated stent in such a way that, when crossing the SB, the lack of struts in the polygon of confluence facilitates its advance without requiring previous opening. Results from the study support just how easy it is to use it with the double stenting technique. In all the cases where it was used, a second stent was successfully implanted into the SB. In 6 (66%) out of the 9 cases where the double stenting strategy was planned, the SB stent was directly implanted without dilatation. This data, though very limited, could signal a possible advantage of the BIOSS LIM C dedicated stent to facilitate access of a second stent to the SB when necessary. On the other hand, angiographic results after implantation are particularly remarkable for the double stenting technique: both the minimum lumen diameters and the residual stenosis of the proximal segments and the SB are better compared to those seen in the cohort where the provisional stenting technique was used.
If procedural data are analyzed, something that calls our attention is the SB predilatation in 47 cases where the SB was not damaged significantly. The protocol did not define the obligation to predilate the SB. According to the investigator’s criterion in each case, the observation of a lesion that did not reach a 50% stenosis was still considered to pose risk of carina displacement.
Another aspect we should mention is the strikingly low use of the POT reported in 33 cases (26%), and similarly in both cohorts. On this regard, we should mention that the device is designed with a proximal segment of a greater caliber in such a way that with simple inflation this proximal postdilatation is already incorporated. The POLBOS I19 and II14 clinical trials showed that the use of POT improved the rate of target lesion revascularization. Also, a tendency towards less late lumen loss was reported. However, POT was used at a rate of 37%, which is similar to that of our cohort.
One of the main study endpoints was to assess the potential disadvantage of design in 2 stent segments. This design provides a space for the polygon of confluence—of 0.9 mm to 1.5 mm—between both segments linked by 2 connectors. In this space, the metal-to-artery ratio is significantly lower, which may contribute to a relatively systematic underexpansion.
Results of the provisional cohort on the polygon of confluence show that mean residual stenosis is 19% at the core of the polygon and 23% in the ostium of the SB. These data suggest a certain impact in the angiographic results of this relative lack of scaffold between both segments that we believe could be the cause for a certain degree of underexpansion at the polygon of confluence.
Another study primary endpoint was to see the degree of damage in the bifurcation native angulation. Godino et al.20 analyzed changes to the bifurcation angle after angioplasty using the 1 or 2-stent technique in a cohort of 215 patients. They described a mean reduction of around 10º of the angle in the left main coronary artery, and 7º in the remaining bifurcations with the double stenting technique. However, with the provisional stenting technique no significant differences were reported. In our study, the results seen in the overall population show a statistically significant change—although not very relevant numerically—of the bifurcation angle that went from 53º to 47º. Contrary to what was reported by Godino et al.20, in our study, in the 2-stent cohort, changes to the bifurcation angle were not significant with mean reductions of 3º. However, in the provisional stenting cohort, a significant reduction of the angle was seen of 6º. In any case, we consider that this just has simple statistical significance; it seems very unlikely that a 5º variation of the bifurcation angle can be seen through visual estimate, and much less that any clinical disadvantages can occur.
Overall, the follow-up results were good and consistent with what was described in former studies.14,19 There was a significant loss of cases for the QCA since 92 cases were available only. Another study limitation is that regarding the analysis of the double stenting technique. Although the QCA data suggest good results for the double stenting technique, the study was not designed to draw comparisons between the provisional and the double stenting techniques. Also, the information collected is limited, and the number of patients treated with the double stenting technique is not enough to reach any conclusions.
An additional limitation we would like to mention is the low use of imaging modalities. Probably in coronary bifurcation lesions its systematic use can be beneficial.
In conclusion, we believe that this study conducted at several centers with different operators reveals how relatively easy it is to use the BIOSS LIM C stent to treat coronary bifurcation lesions. We’re pretty sure this is significant enough to simplify the double stenting approach where the scarce distortion overlapping the bifurcation native angulation called our attention. On the other hand, the weak spot would be the feeble metal scaffold that remains in the polygon of confluence probably due to a certain degree of underexpansion. However, the good clinical outcomes reported at 1-year follow-up are indicative that such design is not really a problem.
Limitations
This was a prospective observational study, which means that any comparisons among the routine techniques used to treat coronary bifurcation lesions can be limited. The informed consent from all the patients was not obtained. Although information from 88% of the cohort was obtained, losses to follow-up were slightly higher than they should have been.
CONCLUSIONS
The BIOSS LIM C dedicated stent works well to treat coronary bifurcation lesions. Angiographically, the stent has a space at the polygon of confluence to facilitate access to the SB. This is associated with a lower metal-to-artery ratio conditioning residual stenosis of around 20%. However, such residual stenosis does not necessarily trigger more events at 1 year and, at the end, this carinal design allows easy access to the SB in case a second stent would be needed and with excellent results. Finally, the stent-induced distortion on the angle of the carina is limited, around 5º.
FUNDING
The study was funded with a graft from Fundación EPIC, which was unconditionally funded by the LOGSA group.
AUTHORS’ CONTRIBUTIONS
As the study lead co-investigators, B. García del Blanco, and A. Pérez de Prado drafted the protocol, managed funds, directed the project, recruited the patients, wrote part of the article, and made their contributions to the overall drafting of the article. J. Gómez-Lara conducted the angiographic analysis at the core lab, the statistical analysis, drafted part of the article, and made his contributions to the article overall draft. I. In his capacity of sub-investigator, Otaegui Irurueta recruited patients by performing procedures and protocol follow-ups, entered the data required in the data curation notebook, depurated and finalized the data entered in the database, was involved in statistical analysis, drafted part of the article, participated in the article overall draft by compiling all the sections drafted from the remaining authors, and responded to the corrections requested by reviewers. M.A. Carmona Ramírez dealt with all regulatory actions needed to start the study and include the different participant centers both with the Spanish Agency of Medicines and Medical Devices and the different centers and ethics committees. As study sub-investigators, the remaining authors recruited patients, performed the procedures and follow-ups according to protocol, filled out the data curation notebook, and responded to all the questions asked.
CONFLICTS OF INTEREST
A. Pérez de Prado is an associate editor of REC: Interventional Cardiology; the journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. He has received research grants from the following research sponsors (Fundación EPIC): Abbott, Biosensors, Biotronik, Bristol-Myers-Squibb, Boston Scientific, Cardiva, iVascular, Shockwave Ltd, Terumo, Volcano Philips; also, fees for his theoretical or practical proctoring for Braun, Boston Scientific, and Terumo. The remaining authors declared no conflicts of interest whatsoever.
WHAT IS KNOWN ABOUT THE TOPIC?
- Dedicated stents facilitate better adaptation to fractal anatomy of coronary bifurcation lesions with less bifurcation angle distortion and access to the side branch. The BIOSS LIM C stent has shown favorable results in randomized clinical trials compared to second-generation tubular stents.
WHAT DOES THIS STUDY ADD?
- In this study, the angiographic pattern of coronary bifurcation lesions with the implantation of BIOSS LIM C dedicated stent is shown. Also, it shows the feasibility of its systematic use—with a high rate of success and scarce damage to bifurcation angulation—can have. Residual underexpansion at the polygon of confluence is acceptable for the provisional stenting technique despite a reduced metal-to-artery ratio, and excellent for the double stenting technique.
REFERENCES
1. Ojeda S, Romaguera R, Cruz-González I, Moreno R. Spanish Cardiac Catheterization and Coronary Intervention Registry. 29th Official Report of the Interventional Cardiology Association of the Spanish Society of Cardiology (1990-2019). Rev Esp Cardiol. 2020;73:927-936.
2. Burzotta F, Lassen JF, Lefèbre T, et al. Percutaneous coronary intervention for bifurcation coronary lesions: the 15th consensus document from the European Bifurcation Club. EuroIntervention. 2021;16:1307-1317.
3. Huo Y, Kassab GS. Scaling laws of coronary circulation in health and disease. J Biomech. 2016;49:2531-2539.
4. Foin N, Sen S, Allegria E, et al. Maximal expansion capacity with current DES platforms: a critical factor for stent selection in the treatment of left main bifurcations? EuroIntervention. 2013;8:1315-1325.
5. Finet G, Derimay F, Motreff P, et al. Comparative Analysis of Sequential Proximal Optimizing Technique Versus Kissing Balloon Inflation Technique in Provisional Bifurcation Stenting: Fractal Coronary Bifurcation Bench Test. JACC Cardiovasc Interv. 2015;8:1308-1317.
6. Maeng M, Hom NR, Erglis A, et al. Long-term results after simple versus complex stenting of coronary artery bifurcation lesions: Nordic Bifurcation Study 5-year follow-up results. J Am Coll Cardiol. 2013;62:30-34.
7. Hildick-Smith D, Behan MW, Lassen JF, et al. The EBC TWO Study (European Bifurcation Coronary TWO): A Randomized Comparison of Provisional T-Stenting Versus a Systematic 2 Stent Culotte Strategy in Large Caliber True Bifurcations. Circ Cardiovasc Interv. 2016;9:e003643.
8. Ferenc M, Gick M, Kienzle R-P, et al. Randomized trial on routine vs. provisional T-stenting in the treatment of de novo coronary bifurcation lesions. Eur Heart J. 2008;29:2859.
9. Ferenc M, Ayoub M, Büttner HJ, et al. Long-term outcomes of routine versus provisional T-stenting for de novo coronary bifurcation lesions: five-year results of the Bifurcations Bad Krozingen I study. EuroIntervention. 2015;11:856-859.
10. Erglis A, Kumsars I, Niemelä M, et al. Randomized comparison of coronary bifurcation stenting with the crush versus the culotte technique using sirolimus eluting stents: the Nordic stent technique study. Circ Cardiovasc Interv. 2009;2:27-34.
11. Gil RJ, Bil J, Kern A, Pawłowski T. First-in-man study of dedicated bifurcation cobalt-chromium sirolimus-eluting stent BIOSS LIM C® - Three-month results. Kardiol Pol. 2018;76:464-470.
12. Gil RJ, Bil J, Grundeken MJ, et al. Long-term effectiveness and safety of the sirolimus-eluting BiOSS LIM® dedicated bifurcation stent in the treatment of distal left main stenosis: an international registry. EuroIntervention. 2016;12:1246-1254.
13. Gil RJ, Bil J, Vassiliev D, Garcia LAI. First-in-man study of dedicated bifurcation sirolimus-eluting stent: 12-month results of BiOSS LIM® Registry. J Interv Cardiol. 2015;28:51-60.
14. Gil RJ, Bil J, Grundeken MJ, et al. Regular drug-eluting stents versus the dedicated coronary bifurcation sirolimus-eluting BiOSS LIM® stent: the randomised, multicentre, open-label, controlled POLBOS II trial. EuroIntervention. 2016;12:e1404-e1412.
15. Lefèvre T, Ormiston J, Guagliumi G, et al. The Frontier stent registry: safety and feasibility of a novel dedicated stent for the treatment of bifurcation coronary artery lesions. J Am Coll Cardiol. 2005;46:592-598.
16. Costa RA, Abizaid A, Abizaid AS, et al. Procedural and early clinical outcomes of patients with de novo coronary bifurcation lesions treated with the novel Nile PAX dedicated bifurcation polymer-free paclitaxel coated stents: results from the prospective, multicentre, non-randomised BIPAX clinical trial. EuroIntervention. 2012;7:1301-1309.
17. TCT-50: Complex Coronary Bifurcation Lesions Treated with the Novel Polymer-Free Dedicated Bifurcation Paclitaxel-Eluting Stent (Nile Pax): 9-Month Clinical and Angiographic Results of the Prospective, Multicenter BIPAX Clinical Trial. J Am Coll Cardiol. 2011;58:B15.
18. Verheye S, Agostoni P, Dubois CL, et al. 9-Month clinical, angiographic, and intravascular ultrasound results of a prospective evaluation of the Axxess self-expanding biolimus A9-eluting stent in coronary bifurcation lesions: the DIVERGE (Drug-Eluting Stent Intervention for Treating Side Branches Effectively) study. J Am Coll Cardiol. 2009;53:1031-1039.
19. Gil RJ, Bil J, Džavík V, et al. Regular Drug-Eluting Stent vs Dedicated Coronary Bifurcation BiOSS Expert Stent: Multicenter Open-Label Randomized Controlled POLBOS I Trial. Can J Cardiol. 2015;31:671-678.
20. Godino C, Al-Lamee R, C La Rosa C, et al. Coronary left main and non-left main bifurcation angles: how are the angles modified by different bifurcation stenting techniques? J Interv Cardiol. 2010;23:382-393.
ABSTRACT
Introduction and objectives: The need for complete coronary artery revascularization after acute coronary syndrome in diabetic patients with multivessel coronary artery disease was discussed, even more so if they reflect the routine clinical practice (“real world”). Therefore, the objective of this study is to analyze cardiovascular complications in diabetics with and without complete revascularization included in clinical trials and in the routine clinical practice.
Methods: This was a single-center retrospective study of diabetic patients with multivessel coronary artery disease. We analyzed 733 diabetic patients: 299 (40.8%) with compatible criteria to be included in clinical trials, and 434 real-world patients (59.2%).
Results: Real-world patients make up 59.2% of the sample. They are characterized by a higher percentage of risk factors, older mean age, and more comorbidities. Diabetics with multivessel coronary artery disease included in the trials have a lower risk of overall mortality (HR, 0.30; 95%CI, 0.16-0.57; P < .001), cardiac death (HR, 0.33; 95%CI, 0.15-0.71; P = .03), and major adverse cardiovascular events (HR, 0.58; 95%CI, 0.38-0.86; P = .008). On the other hand, receiving complete revascularization reduces the risk of cardiac death (HR, 0.32; 95%CI, 0.13-0.83; P = .019), and major adverse cardiovascular events (HR, 0.50; 95%CI, 0.29-0.89; P = .017) in real-world diabetic patients.
Conclusions: It is suggested that fully revascularizing real-world patients would improve survival prognosis. In addition, diabetics included in clinical trials present fewer complications compared to those not included.
Keywords: Diabetes. Revascularization. Real world. Multivessel coronary artery disease.
RESUMEN
Introducción y objetivos: Se debate la necesidad de realizar revascularización coronaria completa tras un síndrome coronario agudo en pacientes diabéticos con enfermedad coronaria multivaso, y más aún si estos son reflejo de los pacientes de la práctica clínica habitual (mundo real). Por ello, el objetivo de este trabajo es analizar las complicaciones cardiovasculares en pacientes diabéticos con y sin revascularización completa incluibles en ensayos clínicos como de la práctica clínica habitual.
Métodos: Estudio unicéntrico retrospectivo de pacientes diabéticos con enfermedad coronaria multivaso. Se analizaron 733 pacientes diabéticos: 299 (40,8%) con criterios compatibles de inclusión de ensayos clínicos y 434 (59,2%) del mundo real.
Resultados: Los pacientes del mundo real constituyen el 59,2% de la muestra. Se caracterizan por presentar mayor porcentaje de factores de riesgo, mayor edad media y comorbilidad. Los diabéticos con enfermedad coronaria multivaso incluibles en ensayos tienen menor riesgo de mortalidad total (HR = 0,30; IC95%, 0,16-0,57; p < 0,001), de mortalidad de causa cardiaca (HR = 0,33; IC95%, 0,15-0,71; p = 0,03) y de sufrir eventos cardiovasculares adversos mayores (HR = 0,58; IC95%, 0,38-0,86; p = 0,008). Por otro lado, recibir revascularización completa desciende el riesgo de mortalidad de causa cardiaca (HR = 0,32; IC95%, 0,13-0,83; p = 0,019) y de eventos cardiacos adversos mayores (HR = 0,50; IC95%, 0,29-0,89; p = 0,017) en los pacientes diabéticos del mundo real.
Conclusiones: Se sugiere que revascularizar completamente a los pacientes del mundo real mejoraría el pronóstico en cuanto a supervivencia. Asimismo, los diabéticos incluibles en ensayos clínicos presentan menos complicaciones que los diabéticos no incluibles.
Palabras clave: Diabetes. Revascularización. Mundo real. Enfermedad coronaria multivaso.
Abbreviations
CR: complete revascularization. IR: incomplete revascularization. MACCE: major adverse cardiovascular and cerebrovascular events. MACE: major adverse cardiovascular events. MCAD: multivessel coronary artery disease.
INTRODUCTION
Cardiovascular diseases—the most prominent of which is ischemic heart disease (IHD)—are a problem of global health and responsible for 1 out of every 3 premature deaths worldwide.1 In Spain, IHD is thought to increase health spending and morbidity due to the ageing of the population, and the greater number of survivors.2
Diabetes mellitus is closely associated with ischemic heart disease. It makes patients—most of them elderly patients—have a very high cardiovascular risk.3 Hypoglycemia and hyperinsulinemia are both associated with a higher risk of developing multivessel coronary artery disease (MCAD).4 In the long-term, this leads to a grim prognosis and more cardiovascular death in these diabetic patients.5
Due to the high incidence rate of MCAD, several studies have been conducted to see what type of revascularization is the most suitable one for the profile of these patients. It has been suggested that anatomic complete revascularization (CR) is associated with a lower rate of major adverse cardiovascular events (MACE)—a composite endpoint of death, non-fatal myocardial infarction, and need for new revascularization—compared to anatomic incomplete revascularization (IR).6 As a matter of fact, it has been reported that the risk of MACE increases significantly when performing IR with minimal residual disease in coronary vessels.7 Therefore, the treatment recommended is to perform anatomic CR. When this is not feasible, functional CR—currently widely used—is advised.
On the one hand, in patients with stable angina refractory to conservative treatment or non-ST-segment elevation acute coronary syndrome (NSTEACS), single-stage CR is advised through surgical coronary revascularization or percutaneous coronary intervention.8 On the other hand, in patients with ST-segment elevation acute coronary syndrome (STEACS) staged CR has been suggested by treating, first of all, the culprit coronary artery causing the clinical signs, and then the remaining stenotic arteries.9 However, in the routine clinical practice, it has been observed that patients with greater comorbidities and worse prognosis are often treated with IR, which worsens even more their clinical evolution since the survival associated with cardiac death, and MACE is lower.10
However, one of the main problems we face is passing scientific knowledge from clinical trials on to the routine clinical practice. It has been reported that most of the patients from cardiology units meet some of the exclusion criteria posed by these clinical trials. Such patients are highly heterogeneous, older, and have several cardiovascular risk factors and concomitant diseases, which worsens their prognosis. Therefore, the findings from clinical trials should be used with caution in the overall population.11,12
Thus, the objective of this study was to analyze whether there are significant differences regarding mortality and cardiovascular events between patients treated with CR or IR, which is why patients with clinical trial inclusion criteria and patients with characteristics from the routine clinical practice (real world) were included.
METHODS
This was a retrospective, single-center study that used data anonymization and included 733 diabetic patients with MCAD treated with coronary angiography from January 1, 2012 through December 31, 2014. Participants were divided into 2 groups based on whether or not they met the FREEDOM clinical trial inclusion criteria.13 In this study, those who met these criteria were considered participants eligible for clinical trials while the rest (the non-eligible ones) were categorized as patients from the routine clinical practice or real-world patients.
Due to data anonymization, it was not necessary to request any approval from the ethics committee since it had already been obtained by Chueca González et al.10 who used the same patient selection. The different informed consents authorize us to treat data to conduct this study.
Study population
Patients over 18 years old with an indication for revascularization—both percutaneous coronary intervention and surgery—due to acute coronary syndromes (STEACS, NSTEACS or unstable angina), refractory stable angina, refractory heart failure, valvular heart disease, cardiac arrest, new revascularization or cardiogenic shock were included in the study Patients with previous cardiac surgeries due to coronary artery disease and valvular heart disease, as well as patients with valvular heart diseases plus a surgical indication were excluded from the study.
The following were categorized as real-world patients (non-FREEDOM): those with STEACS within the 72 previous hours, those with a past medical history of percutaneous transluminal angioplasty, stroke or major bleeding within the previous 6 months, those with functional class III or IV according to the New York Heart Association, in-stent restenosis, known dementia or dependency, at least moderate, according to the Barthel index, and finally those with an extracardiac disease (chronic obstructive pulmonary disease, hepatopathies, chronic kidney disease) bringing survival under 5 years. All the criteria developed have been described previously.10
Definitions
When coronary angiography was performed, patients were considered diabetic if they had already been diagnosed as such in their health record or if they were on hypoglycemic treatments like diet, oral antidiabetic drugs or insulin.
MCAD consists of the existence of ≥ 70% luminal stenosis in 2 or more epicardial vessels covering, at least, 2 or more different coronary artery territories. Also, such lesions are prone to revascularization via angioplasty and surgery according to the clinical practice guidelines and the criterion of interventional cardiologists and cardiac surgeons.
Coronary lesions were treated with anatomic CR. Epicardial vessels > 2 mm in caliber with > 70% stenosis were treated regardless of whether the areas compromised were viable or necrotic.
The indication to perform the coronary angiography was given based on the patient’s clinical course that led to his admission. Acute coronary syndromes with and without ST-segment elevation according to the third universal definition of infarction were included.14 Also, this test was performed on other diseases like unstable angina, refractory stable angina to medical treatment, and other (decompensated heart failure, cardiogenic shock, cardiac arrest, ventricular arrhythmias).
Left ventricular ejection fraction was categorized as dichotomic with values ≥ 40% or < 40%.
To assess the stage of kidney failure the glomerular filtration rate was estimated using the CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) equation. It was defined as reduced with glomerular filtration rates < 45 mL/min/1.73 m3, which is consistent with stage 3B chronic kidney disease.
Regarding the variables that should be measure at the follow-up, events such as death, non-fatal myocardial infarction, and new revascularization were categorized as MACE. On the other hand, major adverse cardiovascular and cerebrovascular events (MACCE) were considered a composite endpoint of death, non-fatal myocardial infarction, new revascularization, and stroke.
Statistical analysis
All statistical analyses were conducted using the statistical software package SPSS version 21.0 for Windows. Quantitative variables were studied using the Student t test for independent samples, and expressed as mean ± standard deviation. Cualitative variables were compared using the chi-square test and expressed as percentages and absolute numbers. Also, the odds ratios (OR) were obtained too. Multivariate analysis was conducted through survival analysis using Cox regression method. Also, survival charts and hazard ratios (HR) with their corresponding 95% confidence intervals were obtained for the significant covariables of the univariate analysis. P values ≤ .05 were considered statistically significant.
RESULTS
A total of 733 diabetic patients met the inclusion criteria to participate in the study. A total of 299 of these patients (40.8%) had criteria that were compatible with the clinical trials, and 434 (59.2%) with the real world. The presence of CR was less common in both groups compared to participants treated with IR. Among the patients in whom CR was achieved, this type of revascularization turned out to be more common in those with criteria from the FREEDOM trial (43.5%).
Patients’ baseline characteristics
Multiple parameters collected at admission were analyzed to perform coronary angiography (table 1).
Table 1. Patients’ baseline characteristics based on compliance of the FREEDOM criteria
| Total | CR in patients from CT | IR in patients from CT | P | Total | CR in patients from the RCP | IR in patients from the RCP | P | |
|---|---|---|---|---|---|---|---|---|
| N | 40.8 (299) | 43.5% (130) | 56.5% (169) | < .001 | 59.2% (434) | 28.3% (123) | 71.7% (311) | < .001 |
| Age | 66.2 ± 9 | 64.1 ± 9.1 | 68 ± 8.4 | < .001 | 69.8 ± 9.6 | 67.5 ± 9.9 | 70.7 ± 9.3 | .002 |
| + 80 years | 6 (18) | 16.7 (3) | 83.3 (15) | .10 | 15.4 (67) | 17.9 (12) | 82.1 (55) | .364 |
| Woman | 30.1 (90) | 40 (36) | 60 (54) | .45 | 31.1 (135) | 28.1 (38) | 71.9 (97) | .95 |
| 3 vessels | 44.8 (134) | 30.6 (41) | 69.4 (93) | < .001 | 54.6 (171) | 35.3 (30) | 61.8 (141) | < .001 |
| Indication | .42 | .01 | ||||||
| STEACS | 2(6) | 16.7 (1) | 83.3 (5) | 32.5 (141) | 39 (55) | 61 (86) | ||
| NSTEACS | 35.5 (106) | 40.6 (43) | 59.4 (63) | 32 (139) | 19.4 (27) | 80.6 (112) | ||
| Unstable angina | 28.4 (85) | 47.1 (40) | 52.9 (45) | 15.7 (57) | 27.9 (19) | 72.1 (49) | ||
| Stable angina | 28.1 (84) | 47.6 (40) | 52.4 (44) | 13.1 (57) | 29.8 (17) | 70.2 (40) | ||
| LVEF < 40% | 14.4 (43) | 32.6 (14) | 67.4 (29) | .14 | 29.8 (129) | 21. (28) | 78.3 (101) | .048 |
| Hypertension | 84.3 (252) | 42.9 (108) | 57.1 (144) | .63 | 84.1 (365) | 26 (95) | 74 (270) | .046 |
| Dyslipidemia | 66.9 (200) | 45 (90) | 55 (110) | .46 | 61.1 (265) | 25.7 (68) | 74.3 (197) | .127 |
| Obesity | 28.1 (84) | 52.4 (44) | 47.6 (40) | .07 | 27.9 (121) | 27.3 (33) | 72.7 (88) | .813 |
| Tobacco use history | 46.5 (139) | 51.1 (71) | 48.9 (68) | .019 | 43.5 (189) | 29.1 (55) | 70.9 (134) | .078 |
| Treatment of DM | 43.5 (130) | 56.5 (169) | .67 | 28.3 (123) | 71.7 (311) | .83 | ||
| Diet | 7.7 (23) | 52.2 (12) | 47.8 (11) | 31.8 (7) | 68.2 (15) | |||
| Oral antidiabetic drugs | 65.9 (197) | 43.1 (85) | 56.9 (112) | 27.3 (73) | 72.7 (194) | |||
| Insulin | 26.4 (79) | 41.8 (33) | 58.2 (46) | 29.7 (43) | 70.3 (102) | |||
| Previous infarction | 12.7 (38) | 28.9 (11) | 71.1 (27) | .053 | 17.3 (75) | 32 (24) | 68 (51) | .439 |
| Heart failure | 4.3 (13) | 23.1 (3) | 76.9 (10) | .129 | 9.2 (40) | 7.5 (3) | 92.5 (37) | .002 |
| Peripheral arterial disease | 8.4 (25) | 32 (8) | 68 (17) | .227 | 13.8 (60) | 15 (9) | 85 (51) | .014 |
| Stroke | 6.4 (19) | 31.6 (6) | 68.4 (13) | .28 | 9.4 (41) | 22 (9) | 78 (32) | .34 |
| COPD | 13.7 (41) | 46.3 (19) | 53.7 (22) | .691 | 18.7 (81) | 21 (17) | 79 (64) | .103 |
| GFR < 45 | 7.4 (22) | 18.2 (4) | 81.8 (18) | .013 | 13.8 (60) | 16.7 (10) | 83.3 (50) | .031 |
| Previous PCI | 17.1 (51) | 35.3 (18) | 64.7 (33) | .195 | 22.1 (96) | 25 (24) | 75 (72) | .41 |
| EuroSCORE II | 2.27±2.27 | 1.84 ± 1.62 | 2.59 ± 2.63 | .004 | 7.57 ± 11.2 | 5.71 ± 7.98 | 8.39 ± 12.24 | .025 |
|
COPD, chronic obstructive pulmonary disease; CR, complete revascularization; CT, clinical trials; DM, diabetes mellitus; GFR, glomerular filtration rate; IR, incomplete revascularization; LVEF, left ventricular ejection fraction; NSTEACS, non-ST-segment elevation acute coronary syndrome; PCI, percutaneous coronary intervention; RCP, routine clinical practice; STEACS, ST-segment elevation acute coronary syndrome. Data are expressed as no. (%). |
||||||||
Differences were found when patients were compared based on their clinical characteristics (patients from clinical trials and from the real world) and type of revascularization received. The most significant differences were found in real-world patients. On the one hand, mean age (69.8 years) was older with more patients > 80 years compared to the group with clinical trial criteria (mean, 66.2 years). On the other hand, in this group there was a higher incidence rate of coronary artery disease with damage to 3 vessels (54.6%) compared to patients from clinical trials (44.8%). Regarding the indication of coronary angiography, a higher rate of acute coronary syndromes—both STEACS and NSTEACS—in such subgroup was reported. They were eventually treated with IR (61% and 80.6%; P < .001) more often. However, patients with characteristics from clinical trials had NSTEACS, and unstable and stable angina as the main indications for coronary angiography. In these patients, CR was achieved more often compared to real-world diabetics.
Major events at 30-day and 35-month follow-up
When it comes to patients with clinical trial inclusion criteria, achieving CR suggested the occurrence of fewer major events—both overall mortality and cardiovascular system-related mortality—especially at 35-month follow-up without any significant differences being reported (table 2).
Table 2. Major events at 30-day and 35-month follow-up in patients with criteria from the FREEDOM clinical trial
| Event | 30 days | P | 35 months | P | ||
|---|---|---|---|---|---|---|
| CR | IR | CR | IR | |||
| Mortality | 0.4 (1) | 0.4 (1) | .863 | 2.8 (5) | 6.7 (12) | .285 |
| Cardiac death | 0 | 0.4 (1) | .375 | 1.1 (2) | 4.5 (8) | .154 |
| Acute myocardial infarction | 0.4 (1) | 0.7 (2) | .715 | 2.4 (4) | 5.4 (9) | .359 |
| Stroke | 0 | 0.7 (2) | .209 | 1.2 (2) | 1.9 (3) | .883 |
| MACE | 0.7 (2) | 1.5 (4) | .601 | 9.7 (19) | 17.9 (35) | .348 |
| MACCE | 0.7 (2) | 2.2 (6) | .277 | 11.2 (22) | 18.9 (37) | .451 |
|
CR, complete revascularization; IR, incomplete revascularization; MACE, major adverse cardiovascular events (death, non-fatal myocardial infarction, and need for new revascularization); MACCE, major adverse cardiovascular and cerebrovascular events (death, non-fatal myocardial infarction, need for new revascularization and stroke). Data are expressed as no. (%). |
||||||
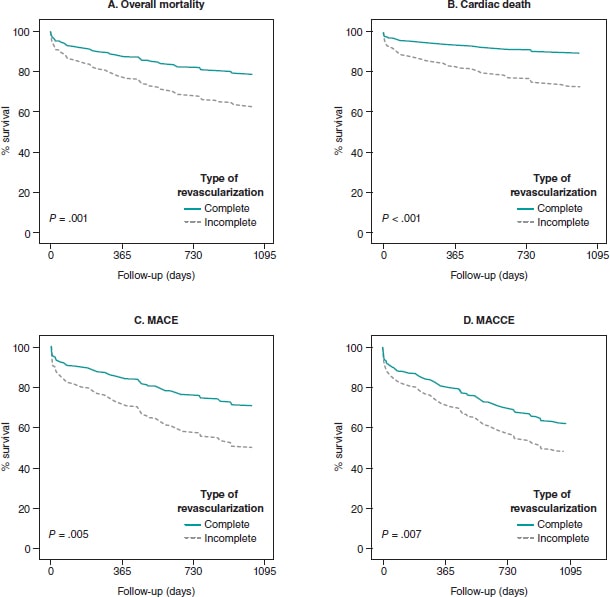
The same tendency was seen in real-world patients. Therefore, CR reduced the risk of overall mortality (OR, 0.84; 95%CI, 0.74-0.95; P = .006), cardiac death (OR, 0.81; 95%CI, 0.73-0.91; P = .002), and MACE (OR, 0.84; 95%CI, 0.74-0.96; P = .012) at 35-month follow-up (table 3). In the survival analysis, the same tendency was found in the said subgroup of participants at 35-month follow-up. CR reduced the risk of cardiac death (HR, 0.35; 95%CI, 0.13-0.90; P = .029), and MACE (HR, 0.5; 95%CI, 0.28-0.89; P = .019). Similarly, EuroSCORE-II > 5 increased the risk of cardiac death (HR, 2.74; 95%CI, 1.11-6.75; P = .028). Finally, a higher risk of MACE (HR, 2.08; 95%CI, 1.03-4.23; P = .042), and MACCE (HR, 2.36; 95%CI, 1.13-4.95; P = .023) was reported (figure 1).
Table 3. Major events at 30-day and 35-month follow-up in patients from the routine clinical practice
| Event | 30 days | P | 35 months | P | ||
|---|---|---|---|---|---|---|
| CR | IR | CR | IR | |||
| Mortality | 1.8 (6) | 8.5 (29) | .257 | 5.5 (14) | 38.4 (98) | .006 |
| Cardiac death | 1.5 (5) | 8.1 (27) | .195 | 3.2 (8) | 31.2 (78) | .002 |
| Acute myocardial infarction | 0.7 (3) | 1.7 (7) | .911 | 7.7 (21) | 17.2 (47) | .626 |
| Stroke | 0 | 0.3 (1) | .522 | 1.5 (3) | 4.9 (10) | .650 |
| MACE | 1.7 (5) | 7.9 (24) | .225 | 6.5 (15) | 40 (92) | .012 |
| MACCE | 1.7 (5) | 7.9 (24) | .225 | 8.3% (19) | 41.3 (95) | .089 |
|
CR, complete revascularization; IR, incomplete revascularization; MACE, major adverse cardiovascular events (death, non-fatal myocardial infarction, and need for new revascularization; MACCE, major adverse cardiovascular and cerebrovascular events (death, non-fatal myocardial infarction, need for new revascularization and stroke).Data are expressed as no. (%). |
||||||
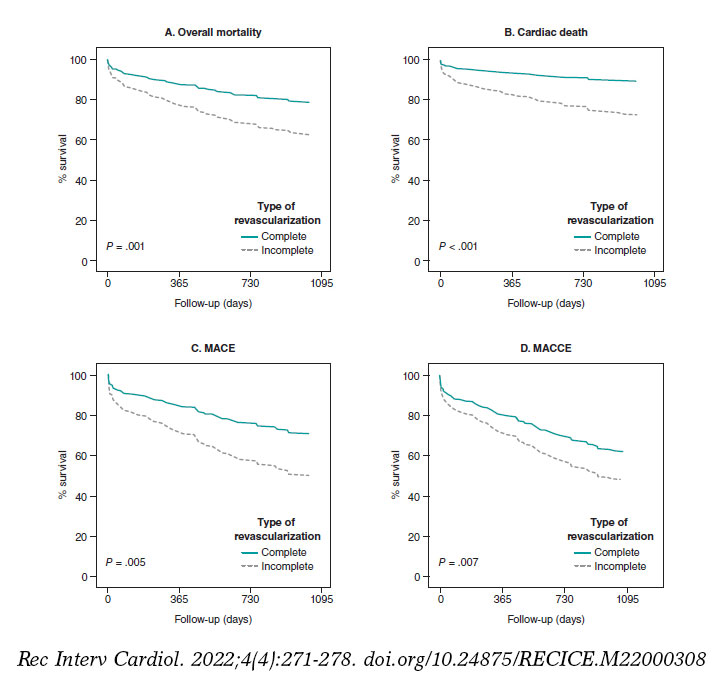
Figure 1. Evolution of survival in diabetic patients from the routine clinical practice with multivessel coronary artery disease. MACE, major adverse cardiovascular events (death, non-fatal myocardial infarction, and need for new revascularization); MACCE, major adverse cardiovascular and cerebrovascular events (death, non-fatal myocardial infarction, need for new revascularization and stroke).
When survival was analyzed in the 4 groups of patients (figure 2), those with FREEDOM clinical trial inclusion criteria had a lower risk of overall mortality (HR, 0.30; 95%CI, 0.16-0.57; P < .001), cardiac death (HR, 0.33; 95%CI, 0.15-0.71; P = .03), MACE (HR, 0.58; 95%CI, 0.38-0.86; P = .008), and MACCE (HR, 0.59; 95%CI, 0.40-0.89; P = .01). On the one hand, achieving CR lowered the risk of cardiac death (HR, 0.32; 95%CI, 0.13-0.83; P = .019), and MACE (HR, 0.50; 95%CI, 0.29-0.89; P = .017). On the other hand, EuroSCORE > 5 when coronary angiography was performed was associated with higher rates of overall mortality (HR, 2.16; 95%CI, 1.06-4.41; P = .034), cardiac death (HR, 3.48; 95%CI, 1.49-8.16; P = .004), MACE (HR, 2.18; 95%CI, 1.26-3.78; P = .005), and MACCE (HR, 2; 95%CI, 1.18-3.40; P = .011). It was reported that if the patient had heart failure, this increased the risk of MACE (HR, 2.44; 95%CI, 1.25-4.74; P = .009), and MACCE (HR, 2.77; 95%CI, 1.39-5.53; P = .004). On the remaining variables, a lower overall mortality rate was confirmed if the patient was a non-smoker (HR, 0.46; 95%CI, 0.24-0.89; P = .02), and a higher risk of MACCE was reported if he had hypertension (HR, 1.50; 95%CI, 1.01-2.24; P = .049) or 3-vessel disease (HR, 1.44; 95%CI, 1.06-1.97; P = .022).
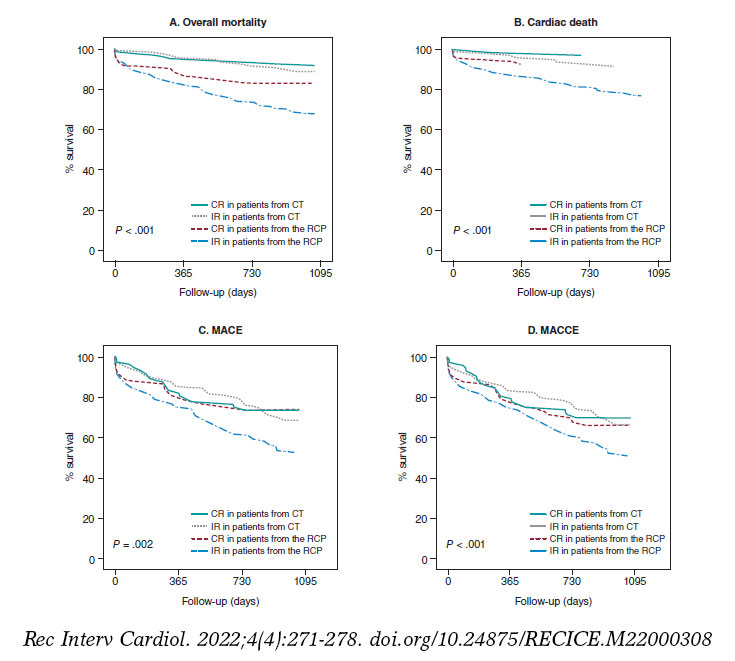
Figure 2. Evolution of survival in diabetic patients con multivessel coronary artery disease. CT, clinical trials; CR, complete revascularization; IR, incomplete revascularization; MACCE, major adverse cardiovascular and cerebrovascular events (death, non-fatal myocardial infarction, need for new revascularization and stroke); MACE, major adverse cardiovascular events (death, non-fatal myocardial infarction, and need for new revascularization); RCP, routine clinical practice.
Type of procedure received
Regarding the therapies received, we found a higher rate of percutaneous coronary interventions (80.8%) performed in all the study subgroups. Real-world patients were treated with coronary artery bypass graft more often compared to patients from clinical trials. Finally, conservative treatment was more common (9%) in real-world patients with IR (table 4).
Table 4. Type of procedures performed per group of patients
| Treatment | CR in patients from CT | IR in patients from CT | CR in patients from the RCP | IR in patients from the RCP | Total |
|---|---|---|---|---|---|
| Conservative | 0 | 4.1 (7) | 0 | 9 (28) | 4.8 (35) |
| PCI | 78.5 (102) | 87 (147) | 76.4 (94) | 80.1 (249) | 80.8 (592) |
| CABG | 21.5 (28) | 8.9 (15) | 23.6 (29) | 10.9 (34) | 14.5 (106) |
|
CABG, coronary artery bypass graft; CR, complete revascularization; CT, clinical trials; IR, incomplete revascularization; PCI, percutaneous coronary intervention; RCP, routine clinical practice.Data are expressed as no. (%). |
|||||
DISCUSSION
The main conclusions of this study are: a) although patients potentially eligible for clinical trials receive CR more often no significant differences have been found regarding survival or adverse cardiovascular events; b) real-world patients are treated with IR more often. In these patients, less mortality has been suggested, both overall and cardiac, as well as fewer MACE at 35-month follow-up have been reported if CR is achieved; c) patients with FREEDOM clinical trial criteria have higher survival rates compared to real-world diabetics; d) most patients are treated with percutaneous coronary intervention.
One of the main problems when analyzing the repercussions of CR is the lack of clinical trials with patients similar to those found in the routine clinical practice or the real word. This complicates the extrapolation of results to the overall population since, in most studies, homogeneous participants can be found often with a better clinical profile.11,12 This reality would explain why CR does not improve the survival rate of such patients who are younger and have fewer comorbidities and cardiovascular risk factors, while in diabetics from the routine clinical practice CR does provide improvements because these are older patients with more MCAD and comorbidities (reduced ejection fraction, arterial hypertension, heart failure, peripheral arterial disease, and chronic kidney disease with, at least, a 3B stage). However, the current scientific evidence available recommends performing a therapeutic effort to achieve CR. It has been suggested that it improves survival in both overall mortality and cardiac death in real-world patients, and avoids IR that is an independent predictor of mortality (HR, 2.46; 95%CI, 1.46-4.13; P = .001).10 On the other hand, The Complete Trial9 confirmed less cardiac death and fewer new reinfarctions (HR, 0.74; 95%CI, 0.60-0.91; P = .004) when CR was performed in patients with STEACS compared to patients in whom only the culprit vessel was treated. Finally, a recent metanalysis confirmed that CR also reduces the overall mortality rate (RR, 0.73; 95%CI, 0.66-0.81), the need for new revascularizations (RR, 0.77; 95%CI, 0.66-0.88), and the occurrence of new myocardial infarctions (RR, 0.74; 95%CI, 0.64-0.85).15
In the first place, this study included diabetic patients who would not be eligible for clinical trials because they are a too heterogeneous population whose characteristics and comorbidities resemble those of real-world patients too much. Secondly, the study deals with a discussed topic these days because cardiovascular diseases, ischemic heart disease among them, are the leading cause of death in developed countries. Diabetes is especially associated with it most often leading to MCAD. Therefore, it is necessary to assess whether CR provides benefits regarding survival always focusing on the patient and his clinical-functional status because, at times, there is controversy on whether to treat all lesions or only the culprit lesions causing the problem.
Finally, if CR provides the benefits suggested in this and other studies, it could improve the survival of diabetic patients and their quality of life and that of their relatives. Also, it would reduce the health spending and the years of life lost or the disability-adjusted years of life by reducing mortality, the need for reinterventions to treat new infarctions and strokes, as well as the need for new revascularizations.
Limitations
This study was conducted from a statistical analysis of a database already used by Chueca González et al.10. It was a retrospective, single-center registry, which limits the possibilities of establishing causality and extrapolating the results to the overall population. Similarly, since the population was designed for a different study, statistical power was probably lost since the size of the sample and the characteristics of the participants included are different from the ones a study like the present one would require.
Another aspect we should mention is the technology of the stents currently used compared to those used during this study recruitment process. Since they appeared, different types and generations of stents associated with different antiproliferative drugs have been manufactured. This has improved secondary survival and minimized the occurrence of in-stent stenosis. Therefore, the study results could be different compared to those obtained today.
Finally, the definitions of CR vary based on the study. Some recommend it in the presence of > 50% occlusions of luminal diameter. Others with occlusions > 70%. In some cases, only coronary vessels with minimum diameters of 2 mm are considered. In other cases, these diameters need to be 1.5 mm. Specifically, this study only considered vessels with stenosis > 70% with minimum calibers of 2 mm.
CONCLUSIONS
This study suggests that diabetics eligible for clinical trials have fewer complications compared to non-eligible diabetic patients. Also, this suggests that real-world diabetics have worse prognosis in case of MCAD. Under this circumstance, it is suggested that achieving CR would improve their long-term survival.
In conclusion, further studies, and clinical trials including real-world patients are advised. Also, they would need to include updated diagnostic criteria and new therapeutic techniques—both pharmacological and interventional—to obtain new evidence to guide us on the therapeutic effort needed to treat patients who require coronary artery revascularization whether through angioplasty or surgery.
FUNDING
This study was funded by the Cardiovascular Biomedical Research Center Network (CB16/11/00360), Instituto de Salud Carlos III. Also, it has been co-funded by the European Regional Development Fund.
The statistical analysis of this manuscript was funded by the Chair of Advanced Therapies in Cardiovascular Diseases at Universidad de Málaga, Spain (CIF Q-2918001-E).
AUTHORS’ CONTRIBUTIONS
F. Puyol-Ruiz: study design, data curation, and drafting of the manuscript. M. Jiménez-Navarro: study design, data curation, and critical review of the manuscript. EM. Chueca-González, F. Carrasco-Chinchilla, J. L. López-Benítez, J. H. Alonso-Briales, J. M. Melero- Tejedor, and J. M. Hernández-García: data curation.
CONFLICTS OF INTEREST
None reported.
ACKNOWLEDGEMENTS
We wish to thank María Jiménez Salva for her constant support and collaboration while drafting this manuscript.
WHAT IS KNOWN ABOUT THE TOPIC?
- Due to the ageing of the population, health spending and morbidity due to ischemic heart disease and diabetes are expected to grow.
- Diabetes increases the number of cases of MCAD, which is associated with a worse prognosis.
- Results from clinical trials should be applied to real-world patients with caution.
WHAT DOES THIS STUDY ADD?
- More than half of diabetic patients with MCAD had exclusion criteria to participate in the FREEDOM clinical trial
- Real-world diabetics have a worse prognosis against MCAD.
- Anatomic CR reduces the risk of cardiac death and MACE at 35-month follow-up.
- More studies and clinical trials are needed with real-world patients.
REFERENCES
1. Roth GA, Mensah GA, Johnson CO, et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J Am Coll Cardiol. 2020;76:2982-3021.
2. Dégano IR, Elosua R, Marrugat J. Epidemiología del síndrome coronario agudo en España: estimación del número de casos y la tendencia de 2005 a 2049. Rev Esp Cardiol. 2013;66:472-481.
3. Ruiz-García A, Arranz-Martínez E, García-Álvarez JC, et al. Prevalence of diabetes mellitus in Spanish primary care setting and its association with cardiovascular risk factors and cardiovascular diseases. SIMETAP-DM study. Clin Investig Arterioscler. 2020;32:15-26.
4. Adeva-Andany MM, Funcasta-Calderón R, Fernández-Fernández C, Ameneiros-Rodríguez E, Domínguez-Montero A. Subclinical vascular disease in patients with diabetes is associated with insulin resistance. Diabetes Metab Syndr Clin Res Rev. 2019;13:2198-2206.
5. Burgess S, Juergens CP, Yang W, et al. Cardiac mortality, diabetes mellitus, and multivessel disease in ST elevation myocardial infarction. Int J Cardiol. 2021;323:13-18.
6. Hosoyama K, Maeda K, Saiki Y. What does complete revascularization mean in 2021? – Definitions, implications, and biases. Curr Opin Cardiol. 2021;36:748-754.
7. Burgess SN, French JK, Nguyen TL, et al. The impact of incomplete revascularization on early and late outcomes in ST-elevation myocardial infarction. Am Heart J. 2018;205:31-41.
8. Gaba P, Gersh BJ, Ali ZA, Moses JW, Stone GW. Complete versus incomplete coronary revascularization: definitions, assessment and outcomes. Nat Rev Cardiol. 2021;18:155-168.
9. Mehta SR, Wood DA, Storey RF, et al. Complete Revascularization with Multivessel PCI for Myocardial Infarction. N Engl J Med. 2019;381:1411-1421.
10. Chueca González EM, Carrasco Chinchilla F, López Benítez JL, et al. Enfermedad coronaria multivaso en el paciente diabético en la vida real: ¿eficacia o efectividad? REC CardioClinics. 2019;54:81-90.
11. Wasilewski J, Polon´ski L, Lekston A, et al. Who is eligible for randomized trials? A comparison between the exclusion criteria defined by the ISCHEMIA trial and 3102 real-world patients with stable coronary artery disease undergoing stent implantation in a single cardiology center. Trials. 2015;16:1-7.
12. Laursen PN, Holmvang L, Lønborg J, et al. Comparison between patients included in randomized controlled trials of ischemic heart disease and real-world data. A nationwide study. Am Heart J. 2018;204:128-138.
13. Goel SS, Shishehbor MH. Strategies for multivessel revascularization in patients with diabetes. Cardiol Rev. 2013;29:2375-2384.
14. Thygesen K, Alpert JS, Jaffe AS, et al. Documento de consenso de expertos. Tercera definición universal del infarto de miocardio. Rev Esp Cardiol. 2013;66:1-15.
15. Zimarino M, Ricci F, Romanello M, Di Nicola M, Corazzini A, De Caterina R. Complete myocardial revascularization confers a larger clinical benefit when performed with state-of-the-art techniques in high-risk patients with multivessel coronary artery disease: A meta-analysis of randomized and observational studies. Catheter Cardiovasc Interv. 2016;87:3-12.
ABSTRACT
Introduction and objectives: When using radial access established as the approach of choice to perform coronary angiographies it is important to avoid radial spasm as it is the leading cause of access failure. This study aims to determine whether a topical anesthetic cream reduces the rate of radial spasm, as well as the increased gain with the use of different vasodilators.
Methods: Randomized, double-blind, and single-center clinical trial. Patients will be randomized to receive the anesthetic cream vs placebo, and 4 types of different vasodilator cocktails will be used in each group. The presence—or not—of radial spam and caliper gain will be analyzed.
Conclusions: Demonstrating the efficacy of the anesthetic cream, and different vasodilators to reduce radial spam would have a significant clinical impact, and justify its systematic use when performing coronary angiographies.
Registered at The Spanish Agency of Medicines and Medical Devices (AEMPS) EudraCT number: 2017-000321-12.
Keywords: Radial spasm. Anesthetic cream. Vasodilators. Coronary angiography. Luminal diameter.
RESUMEN
Introducción y objetivos: Con el abordaje radial establecido como técnica de elección para la coronariografía, es importante evitar el espasmo radial como principal causa de fallo en el acceso intravascular. En este estudio se pretende demostrar si la anestesia tópica en crema disminuye la incidencia de espasmo radial, así como conocer la ganancia de calibre con el uso de diferentes vasodilatadores.
Métodos: Ensayo clínico aleatorizado doble ciego en un solo centro. Los pacientes se aleatorizarán para recibir crema anestésica o placebo, y se utilizarán 4 tipos de cócteles vasodilatadores en cada grupo. Se analizará la presencia o no de espasmo radial y la ganancia de calibre como objetivos primarios.
Conclusiones: La demostración de la eficacia de la crema anestésica y de los diferentes vasodilatadores en la disminución del espasmo radial tendría un impacto clínico importante y justificaría su uso sistemático en la coronariografía.
Registrado en la Agencia Española de Medicamentos y Productos Sanitarios (AEMPS) con n.º EudraCT: 2017-000321-12.
Palabras clave: Espasmo radial. Crema anestésica. Vasodilatadores. Coronariografía. Diámetro luminal.
Abbreviations
MLD: mean luminal diameter. RS: radial spasm. TA: topical anesthesia.
INTRODUCTION
Radial approach for cardiac catheterizations has become the most widely used across the world. In Spain it represents up to 75% of all the procedures performed and, in some centers, up to 91.1%.1 Compared to traditional femoral approach, this access has clearly proven its superiority from the safety standpoint of the procedures.2
Arterial canalization failure is often due to radial spasm (RS), and it can occur in up to 10% of all attempts. Also, it is associated with feminine sex, young age, low weight3 or deficits of certain enzymes that act on the endothelium.4 The special histological characteristics of this artery—with a high density of alpha-adrenergic receptors and smooth muscle cells—make it more prone to spasm.5
On the other hand, pain during lumbar puncture contributes to arterial canalization failure due to a higher frequency of appearance of spasm, vasovagal reaction with hypotension and discomfort for patient and operator, and the patient’s possible hemodynamic instability. Similarly, several patients complain of discomfort. As a matter of fact, the arterial puncture is described by many patients as the main moment of discomfort.5
Former studies have reported on the greater success achieved with isolated punctures for arterial gas analysis in the radial artery with the use of anesthesia injected around the puncture site. Also, more comfort and less pain have been reported by the patients.6 However, for many professionals injected anesthesia is ill-advised due to the pain caused by the injection. Also, because there are times that pain leads discomfort, and eventually RS.7 Despite of all this, the use of injected anesthesia is a common thing in procedures performed via radial access.
On the other hand, in the pediatric population as well as in different anatomical locations or in skin surgery, the use of topical anesthesia (TA) in the form of gel, cream or ointment has proven to minimize the pain associated with venous or arterial punctures, and some procedures too.8 The use of this type of anesthetic agents has not been properly studied in the cardiac catheterization setting. However, it could minimize the rate of RS, reduce pain when using this access, and improve the patient’s perception.
Together with TA, the use of different vasodilator drug combinations with unfractionated heparin (the so-called «radial cocktail»)—after successful arterial access—has proven to reduce the rates or arterial spasm and radial occlusion after the procedure.9-12 In particular drugs like verapamil, nitroglycerin, nitroprusside, nicorandil, isosorbide dinitrate or phentolamine in different doses have been compared with one another and also with placebo with heterogeneous results with arterial spams having been reported in 4% to 12% of the cases. Verapamil in doses of 5 mg and nitroglycerin 200 µg have yielded the best results so far. However, to this date, no comparison studies between the 2 drugs at these doses have ever been drawn or randomized for this matter.13 Therefore, it has not been fully established which is the best drug combination to prevent spasm and radial occlusion.
At our center, the current radial puncture procedure includes the use of injected anesthesia around the puncture site plus a cocktail of 5000 IU of unfractionated heparin, and 2.5 mg of verapamil. The rate of RS in our cath lab is around 10% of all punctures performed. In some patients, other drugs commonly available in our setting are often used—at the operator’s criterion—like nitroprusside, nitroglycerin or high doses of verapamil.
The objective of this study is to demonstrate whether the administration of topical anesthesia reduces the rate of RS and improves the patient’s perception regardless of the vasodilator used. Also, to compare arterial caliber gain with different vasodilators.
METHODS
Study design
Double-blind randomized clinical trial conducted at a single center to analyze the rate of RS in patients treated with TA in cream with lidocaine 25 mg/g + prilocaine 25 mg/g (Emla) in topical solution compared to placebo, as well as the effect of vasodilators (table 1) (verapamil 2.5 mg or 5 mg, nitroglycerin 200 µg, nitroprusside 150 µg) in the arterial caliber while attempting vascular access to perform diagnostic transradial cardiac catheterization.
Table 1. Inclusion and exclusion criteria of the E-RADIAL study
| Composition of the radial cocktail | Type of dilution |
|---|---|
| Cocktail #1 (verapamil 2.5 mg): | 12.5 mg of verapamil are diluted in 95 mL of FSS at 0.9%. A total of 20 mL are loaded in the syringe and fully administered. |
| Cocktail #2 (verapamil 5 mg): | 25 mg of verapamil are diluted in 90 mL of FSS at 0.9%. A total of 20 mL are loaded in the syringe and fully administered. |
| Cocktail #3 (nitroglycerin 0.2 mg): | 5 mg of nitroglycerin are diluted in 95 mL of FSS at 0.9%. A total of 4 mL of this solution are loaded in a 20 mL-syringe that is completed with FSS at 0.9%. The entire load of the syringe is administered. |
| Cocktail #4 (nitroprusside 0.150 mg): | 50 mg are diluted in 10 mL of FSS at 0.9% followed by the extraction of 1 mL of this solution that is diluted again in 100 mL of FSS at 0.9%. A total of 3 mL of the latter solution are loaded in a 20 mL-syringe that is completed with FSS at 0.9%. The entire load of the syringe is administered. |
|
FSS, physiological saline solution. |
|
Study population
The study will be conducted entirely at Unidad de Hemodinámica y Cardiología Intervencionista of Complejo Hospitalario Universitario de Albacete, Spain. All consecutive patients treated with diagnostic cardiac catheterization via radial access from November 2020 until completing the sample estimated will be included. Patients will need to meet the inclusion criteria and none of the exclusion ones (table 2).
Table 2. Inclusion and exclusion criteria of the E-RADIAL study
| Inclusion criteria | Exclusion criteria |
|---|---|
| Age > 18 years | Allergy or intolerance to any of the drugs used in the study. |
| Informed consent signing | Baseline systolic arterial blood pressure < 90 mmHg. |
| Elective diagnostic cardiac catheterization with intended radial access |
Impossibility to understand the study or give the corresponding informed consent. |
| Introductor 5 French |
Ethical aspects
The study has been approved by the center ethics committee, and a favorable resolution was obtained. The study has been registered by Agencia Española de Medicamentos y Productos Sanitarios (AEMPS) with registration No. EudraCT: 2017-000321-12. The study will observe the principles established in the Declaration of Helsinki. Also, written informed consent will be obtained from all the patients before joining the study.
Study endpoints
Primary endpoints
– Study the rate of RS using a topical anesthetic cream before radial puncture.
– Study radial artery caliber gain using different vasodilators.
Secondary endpoints
– Study the rate of radial-radial, and radial-femoral crossing with each strategy.
– Study the rate of vasovagal reactions requiring treatment in each group.
– Study parameters associated with pain during radial artery canalization using pain assessment analogue scales.
– Subjective assessment of pain and comfort by the patient using pain assessment analogue scales, and dedicated tests.
– Subjective assessment of the difficulty involved in the puncture and perception of RS by the operator using dedicated tests.
Study development
The administration of TA/placebo plus cocktail (table 1) will be fully randomized (figure 1). Both the patient and the treating interventional cardiology will be blind to the group they’ll be assigned to. If certain circumstances or complications occur, and if deemed necessary, the chain of secrecy can be broken only if investigators abide, and only under strict clinical judgement.
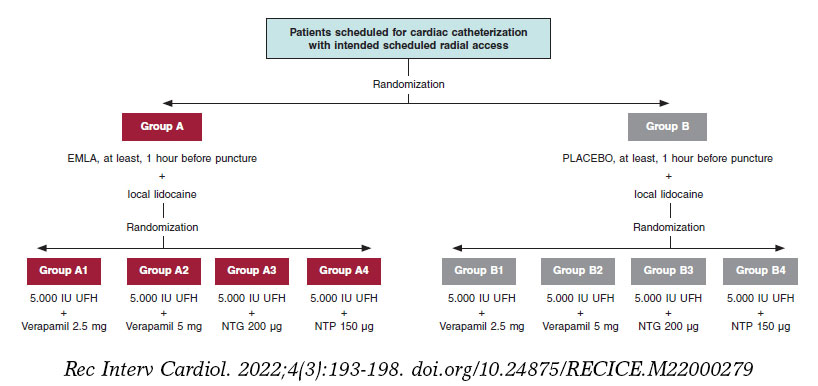
Figure 1. Flowchart of patients from the E-RADIAL study. NTG, nitroglycerin; NTP, nitroprusside; UFH, unfractionated heparin.
Placebo with cream of similar color, consistency, and characteristics to Emla will be prepared, and they both will be marked with letters A (Emla) and B (placebo). Both placebo and the TA will be prepared by personnel from the hospital pharmacy unit. The nursing team in charge of the patients while waiting for cardiac catheterization at the cath lab will randomize each patient, and the only blind element of the study. TA or placebo will be administered in both wrists and, at least, 1 hour before the procedure.
Prior to puncture, 25 mg of subcutaneous local anesthesia will be injected into the puncture area (mepivacaine at 2%). Another 1-2 minutes will need to pass before it starts to work.
Different cocktails (table 1) will be prepared at the dilution often used at Complejo Hospitalario Universitario de Albacete cath lab in 100 mL-jars of physiological saline solution (NaCl at 0.9%). Each jar will be marked with an alphanumeric code and its content will remain blind to everyone but the nursing team in charge of randomization.
Variable quantification during puncture
After monitoring the patient, arterial blood pressure will be determined invasively, as well as the baseline heart rate before administering the cocktail that will be used just after the introduction of hydrophilic guidewire (Radiofocus 5-Fr, Terumo, Japan). Similarly, arterial blood pressure will be recorded 2 minutes after the cocktail administration, as well as the maximum heart rate during puncture.
All vagal data that can occur and any other complications associated with access will be written down. The crossing rate to other accesses will also be studied prioritizing homolateral (cubital, distal radial) or contralateral access. Unless the operator specifies otherwise, femoral access will be set aside as the third go-to option.
Radial spasm determination and caliber gain quantification
RS will be defined as yes/no—both qualitative and dichotomically—and considered as sudden, transient, and abrupt narrowing of the radial artery during puncture. It will be clinically determined by, at least, 1 of the following events: loss of pulse during puncture, pain in the upper limb during catheter manipulation or entrapment. Its presence can also be determined through the angiography if spasm is seen during contrast injection.
Caliber gain will be determined through quantitative analysis of the radial artery luminogram. Therefore, an angiography will be immediately performed after the insertion of the introducer sheath plus another one 2 minutes after the injection of the antispasmodic cocktail. The radial artery caliber will be measured in the segment located between the tip of the arterial introducer sheath—2 cm away from it—and the location where it meets the humeral artery. Measurements will be acquired through computerized quantitative analysis (Xcelera, Philips, United States) after previous calibration of the arterial introducer sheath in the same segment before and after the cocktail injection to determine the mean luminal diameter (MLD).
Caliber gain will be estimated in percentage according to the following formula:
Caliber gain =  × 100
× 100
Postoperative patient assessment
The patient will be asked to give his opinion on the radial puncture through the pain qualitative analogue scale, and the comfort scale consisting of 4 questions (annex of the supplementary data).
Similarly, the interventional cardiologist will give his evaluation through a survey including 2 questions (annex of the supplementary data), the difficulties found while performing the puncture, and how the procedure was accomplished via the access used.
Statistical analysis
The analysis will be conducted using the SPSS statistical software package for Windows v 21.0.
In descriptive statistics frequencies and percentages will be used to express discrete variables while mean, median, mode, standard deviation, and ranges will be used to express continuous variables. The rate of spams and other study components will be described through frequencies and percentages. The statistical analysis of the main variables will be conducted by intention-to-treat analysis. The chi-square test will be used to study differences among proportions while the continuous variables will be analyzed using the Student t test if normally distributed or else non-parametric tests if not normally distributed. In the presence of non-homogeneous distribution of confounding variables between the groups that will be analyzed, a logistic regression analysis will be conducted that should collect those clinically significant and non-homogeneously distributed parameters.
It is our will to conduct an intermediate analysis after which the study will move on or not (existence of a significant difference in the primary endpoint of RS > 7,5% between both groups).
Estimate of the sample size
According to former studies, it is estimated that the proportion of patients who will have RS in the control group will be 10%3,5 being the criterion of clinical effectiveness the reduction of this percentage off by 50%, which is why it will be necessary to have a minimum sample of 668 patients.
This volume of patients will allow us to confirm the statistical significance of the variations described in radial artery vasodilation with different types of vasodilators.
DISCUSSION
Currently, the arterial approach via radial access is used in 91.1%1 of all diagnostic and therapeutic coronary angiographies performed. In particular, the rates of bleeding complications have dropped thus contributing to the patients’ comfort. This access has facilitated the implementation of safe coronary angiography and outpatient angioplasty programs even in complex settings.14-16
Hand in hand with this and assuming pain hypothesis and adrenergic discharge are caused by puncture and risk factors for RS, different strategies have come up to contribute to the proper administration of anesthesia promoting patients’ comfort, and looking to reduce the rate of RS. As it happens in other places, at our center the use of subcutaneously injected anesthesia is the common practice since the direct correlation between less RS and proper anesthetic release in the punction area has already been confirmed.5 This study paves the way for a possible change in the routine clinical practice that could be associated—or not—with TA in cream pharmaceutical form. The medical literature includes different and very heterogeneous studies that, whether randomized or not, have tried to assess the utility of this type of creams. However, all of them include small samples (usually less than 100 patients), which makes it difficult to extrapolate the results.
We have a few examples of injected anesthesia vs a composite of TA plus injected anesthesia with favorable results from the latter.17,18 As far as we know, the heterogeneity of designs, and the small sample sizes make us question studies like these.
Although subcutaneous anesthesia—often with lidocaine—has proven to improve pain at the puncture site and reduce the rate of RS compared to TA there is a huge controversy regarding the active principles and drug combination that should be used, the specific action times of these drugs or which are the best pharmaceutical forms. However, it seems that the cream/ointment formulation, and the lidocaine/prilocaine combination (Emla type) yield the best results of all.18
Assuming that this type of formulation is the most widely studied and looking to achieve an adequate design with a representative sample, the E-RADIAL trial (Effectiveness in preventing radial spasm of different vasodilators and topic local anesthesia during transradial cardiac catheterization) has just been started. Although it is not the first trial to propose this hypothesis, it is the first one indeed to confirm it on a double-blind randomized clinical trial and compare it to different radial cocktails and a wide sample size.
This vasolidator comparison is a particularly new approach of our trial. There is some controversy on the use, or not, of such drugs: although some centers in our country do not use vasodilators on a routine basis, it seems to be proven that, overall, its use promotes arterial dilatation and, therefore, the navigability of catheters with lower rates of spasm.9,13 Currently, no such thing as head-on comparisons of cocktails have been drawn in trials to assess their efficacy and safety profile.19 Therefore, we designed our study taking into consideration that a comparison can be drawn among these different drugs in quantitative terms using MLD gain.
Although not part of our study primary endpoints we assume that—with radial access clearly established in the routine clinical practice of cath labs—the operator’s experience, his learning curve or even the rotating fellow/resident’s learning curve can have an impact on the rate of success of puncture, RS, as well as on other complications. This can be an interesting aspect we could discuss. As far as we know both in the current medical literature and good practice recommendations regarding the radial access20—although with limitations depending on the study analyzed—it seems reasonable to assume that the threshold to overtake the learning curve would be at around 30-5021 cases for conventional diagnostic coronary angiography, and > 100-200 cases for complex coronary anatomies22,23 or even in the ST-segment elevation acute coronary syndrome setting. In the E-RADIAL study, all operators widely exceed the number of cases recommended for this curve in diagnostic coronary angiography. Even so, while collecting data for the E-RADIAL we’ll have the possibility to know the identity of the operator who will perform the puncture, his years of experience using radial access, and whether a resident or a novel interventional cardiology (< 2 years of experience) was involved. Also, we will try to know descriptively the rate of puncture success, and whether any RS differences or other complications occurred.
The design of this clinical trial used 4 types of radial cocktail (table 1) from the ones most widely used ones in today’s clinical practice. However, this is also a controversial issue. On the one hand, some centers don’t use vasodilators systematically after radial puncture. On the other hand, choosing one over the other at the cath labs where they’re used is often based on the good clinical results obtained empirically in the routine clinical practice. Unlike the use of heparin to prevent radial occlusion, evidence is scarce regarding benefits from vasodilators, and no homogeneous head-on comparisons have been drawn among different drug cocktails. Verapamil in doses of 5 mg, and nitroglycerin in doses of 200 µg have yielded the best results so far. However, to this date, they have never been compared to one another at these doses or in a randomized way.13 Certain clinical features of the patients can turn the use of these cocktails into a controversial issue. As an example of this, in patients with very severe left ventricular dysfunction or severe aortic stenosis the use of these drugs can trigger significant adverse reactions, mainly hypotension or significant hemodynamic changes. Although, in theory, overall, these drugs are contraindicated in these clinical settings, the dose used, slow infusion, and other factors like the patients’ clinical stability, the existence—or not—of associated heart failure or different comorbidities can turn the use of these drugs into a safe practice. In its design the E-RADIAL study includes a head-on comparison of cocktails and some of the aforementioned drugs and doses. Therefore, it is an opportunity to know what the clinical implication of these drugs really is regarding adverse events.
One of the possible weaknesses or aspects that should be discussed in this trial is pain assessment and quantification. A reproducible design was attempted while assuming the difficulties posed by individual subjectivity. Therefore, following in the footsteps of former studies and registries, we decided to use the most standardized method available to this date in the medical literature: analogue scales.
Another possible weakness or cofounding factor in the study design is the systematic use of sodium heparin via arterial access as standard prevention against radial occlusion.20 According to the drug label24 the heparin-induced cardiac tamponade solution is often an acid solution with a pH between 5.0 and 7.5. The mean arterial pH is between the traditional values of 7.35 and 7.45, and could be partially altered when in contact with heparin solutions thus favoring, through different mechanisms, the development of RS, something not clearly established to this date. To solve this possible bias, the IV—not intraarterial use—of heparin was selected. Although evidence is certainly scarce and heterogeneous the IV use of heparin does not seem to increase the rate of radial occlusion, which is more associated with the heparin dose used and factors like compression time, type of material or size of the radial introducer sheath used that are well established as predictors of radial occlusion.25,26
CONCLUSIONS
The E-RADIAL study is the first randomized clinical trial to assess, on the one hand, the implications of less RS due to topical anesthesia and, on the other, arterial caliber gain with the use of different vasodilators.
FUNDING
None whatsoever.
AUTHORS’ CONTRIBUTIONS
J. J. Portero-Portaz: idea, methodology, validation, formal analysis, drafting of the original project; J. G. Córdoba-Soriano: idea, methodology, review and edition of the manuscript; A. Gutiérrez-Díez: idea, methodology, validation, formal analysis, review and edition of the manuscript; A. Gallardo-López, and D. Melehi El-Assali: idea, methodology, review and edition of the manuscript; L. Expósito-Calamardo, and A. Prieto-Lobato: research, review, and edition of the manuscript; E. García-Martínez, S. Ruiz-Sánchez, M. R. Ortiz Navarro, and E. Riquelme-Bravo: methodology, review, and edition of the manuscript; J. Jiménez-Mazuecos: idea, methodology, review and edition of the manuscript.
CONFLICTS OF INTEREST
Authors declared having no affiliation or participation in any organization or entity with any financial or non-financial interest in the topic at stake or in the materials discussed in this manuscript.
ACKNOWLEDGEMENTS
We wish to thank the nursing personnel of our unit for their work, dedication, and availability during the entire study.
WHAT IS KNOWN ABOUT THE TOPIC?
- RS is the leading cause of access failure in diagnostic or therapeutic coronary angiographies.
- The use of injected local anesthesia is standardized and reduces the rate of RS.
- There is no consensus on the use or non-use of vasodilators, which depends on the characteristics and routine clinical practice of each center.
WHAT DOES THIS STUDY ADD?
- The E-RADIAL study can pave the way to systematization in the use of other type of anesthesia.
- It will provide relevant information on the effectiveness of different vasodilators through head-on comparisons of the most widely used agents.
SUPPLEMENTARY DATA

REFERENCES
1. Romaguera R, Ojeda S, Cruz-González I, Moreno R. Registro Español de Hemodinámica y Cardiología Intervencionista. XXX Informe Oficial de la Asociación de Cardiología Intervencionista de la Sociedad Española de Cardiología (1990-2020) en el año de la pandemia de la COVID-19. Rev. Esp Cardiol. 2021;74:1095-1105.
2. Rao SV, Turi ZG, Wong SC, Brener SJ, Stone GW. Radial versus femoral access. J Am Coll Cardiol. 2013;62(17 Suppl):S11-20.
3. Dandekar VK, Vidovich MI, Shroff AR. Complications of transradial catheterization. Cardiovasc Revasc Med. 2012;13:39-50.
4. Kocayigit I, Cakar MA, Kahyaog˘lu B, Aksoy MNM, Tatli E, Akdemir R. The relationship between serum asymmetric dimethylarginine levels and radial artery spasm. Anatol J Cardiol. 2020;23:228-232.
5. Ho HH, Jafary FH, Ong PJ. Radial artery spasm during transradial cardiac catheterization and percutaneous coronary intervention: incidence, predisposing factors, prevention, and management. Cardiovasc Revasc Med. 2012;
13:193-195.
6. Hudson TL, Dukes SF, Reilly K. Use of local anesthesia for arterial punctures. Am J Crit Care. 2006;15:595-599.
7. France JE, Beech FJ, Jakeman N, Benger JR. Anaesthesia for arterial puncture in the emergency department: a randomized trial of subcutaneous lidocaine, ethyl chloride or nothing. Eur J Emerg Med. 2008;15:218-220.
8. Tran NQ, Pretto JJ, Worsnop CJ. A randomized controlled trial of the effectiveness of topical amethocaine in reducing pain during arterial puncture. Chest. 2002;122:1357-1360.
9. Boyer N, Beyer A, Gupta V, et al. The effects of intra-arterial vasodilators on radial artery size and spasm: implications for contemporary use of trans-radial access for coronary angiography and percutaneous coronary intervention. Cardiovasc Revasc Med. 2013;14:321-324.
10. Ruiz-Salmerón RJ, Mora R, Vélez-Gimón M, et al. Espasmo radial en el cateterismo cardíaco transradial. Análisis de los factores asociados con su aparición y de sus consecuencias tras el procedimiento. Rev Esp Cardiol. 2005;58:504-511.
11. Majure DT, Hallaux M, Yeghiazarians Y, Boyle AJ. Topical nitroglycerin and lidocaine locally vasodilate the radial artery without affecting systemic blood pressure: a dose-finding phase I study. J Crit Care. 2012;27:532.e9-13.
12. Beyer AT, Ng R, Singh A, et al. Topical nitroglycerin and lidocaine to dilate the radial artery prior to transradial cardiac catheterization: a randomized, placebo-controlled, double-blind clinical trial: the PRE-DILATE Study. Int J Cardiol. 2013;168:2575-2578.
13. Kwok CS, Rashid M, Fraser D, Nolan J, Mamas M. Intra-arterial vasodilators to prevent radial artery spasm: a systematic review and pooled analysis of clinical studies. Cardiovasc Revasc Med. 2015;16:484-490.
14. Córdoba-Soriano JG, Rivera-Juárez A, Gutiérrez-Díez A, et al. The Feasibility and Safety of Ambulatory Percutaneous Coronary Interventions in Complex Lesions. Cardiovasc Revasc Med. 2019;20:875-882.
15. Córdoba-Soriano JG, Jiménez-Mazuecos J, Rivera Juárez A, et al. Safety and Feasibility of Outpatient Percutaneous Coronary Intervention in Selected Patients: A Spanish Multicenter Registry. Rev Esp Cardiol. 2017;70:535-542.
16. Gallego-Sánchez G, Gallardo-López A, Córdoba-Soriano JG, et al. Safety of transradial diagnostic cardiac catheterization in patients under oral anticoagulant therapy. J Cardiol. 2017;69:561-564.
17. Tatlı E, Adem Yılmaztepe M, Gökhan Vural M, et al. Cutaneous analgesia before transradial access for coronary intervention to prevent radial artery spasm. Perfusion. 2018;33:110-114.
18. Youn YJ, Kim WT, Lee JW, et al. Eutectic mixture of local anesthesia cream can reduce both the radial pain and sympathetic response during transradial coronary angiography. Korean Circ J. 2011;41:726-732.
19. Shehab A, Bhagavathula AS, Kaes AA, et al. Effect of Vasodilatory Medications on Blood Pressure in Patients Undergoing Transradial Coronary Angiography: A Comparative Study. Heart Views. 2020;21:75-79.
20. Shroff AR, Gulati R, Drachman DE, et al. SCAI expert consensus statement update on best practices for transradial angiography and intervention. Catheter Cardiovasc Interv. 2020;95:245-252.
21. Hess CN, Peterson ED, Neely ML, et al. The learning curve for transradial percutaneous coronary intervention among operators in the United States: a study from the National Cardiovascular Data Registry. Circulation. 2014;
129:2277-2286.
22. Azzalini L, Ly HQ. Letter by Azzalini and Ly regarding article, “The learning curve for transradial percutaneous coronary intervention among operators in the United States: a study from the National Cardiovascular Data Registry”. Circulation. 2015;131:e357.
23. Hamon M, Pristipino C, Di Mario C, et al. European Association of Percutaneous Cardiovascular Interventions; Working Group on Acute Cardiac Care of the European Society of Cardiology; Working Group on Thrombosis on the European Society of Cardiology. Consensus document on the radial approach in percutaneous cardiovascular interventions: position paper by the European Association of Percutaneous Cardiovascular Interventions and Working Groups on Acute Cardiac Care** and Thrombosis of the European Society of Cardiology.EuroIntervention. 2013; 8:1242–1251.
24. Ficha técnica de la heparina sódica. Agencia Española de Medicamentos y Productos Sanitarios. Available online: https://cima.aemps.es/cima/dochtml/ft/56029/FT_56029.html. Accessed 20 Nov 2021.
25. Pancholy SB. Comparison of the effect of intra-arterial versus intravenous heparin on radial artery occlusion after transradial catheterization. Am J Cardiol. 2009;104:1083-1085.
26. Rashid M, Kwok CS, Pancholy S, et al. Radial Artery Occlusion After Transradial Interventions: A Systematic Review and Meta-Analysis. J Am Heart Assoc. 201625;5:e002686.
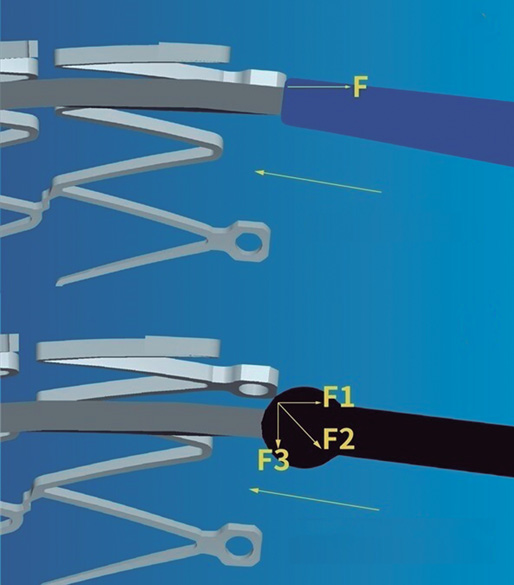
ABSTRACT
Introduction and objectives: Noncompliant balloon postdilatation of coronary stents improves clinical results. Regular noncompliant balloons (RegNC) have less crossability and a tapered-tip that can complicate successful stent postdilatation. The mechanical conditions of a new spherical tip non-compliant balloon (SphNC) could facilitate stent postdilatation. We tried to evaluate the effectiveness of a new SphNC in the routine percutaneous coronary intervention (PCI) practice.
Methods: Prospective multicenter technical registry to assess the effectiveness of a new SphNC for stent postdilatation with 2 study arms: use of SphNC as the first choice or as the secondary choice after RegNC failure. The primary endpoint was technical success defined as advancing the SphNC across the stent segment. Secondary endpoints were angiographic success defined as technical success and residual stenosis < 30% with final TIMI grade-3 flow, and procedural success defined as angiographic success without mechanical stent complications or any perioperative major adverse cardiovascular events.
Results: The SphNC was used in 263 lesions (177 lesions as first choice, and 86 after RegNC failure) in 250 procedures. The use of the complex technique to advance the SphNC was low (9.9%). Technical, angiographic, and procedural success rates were 98.9%, 98.3%, and 98.3%, respectively, as the first choice, and 98.8%, 97.7%, and 96.5%, respectively, after RegNC failure. SphNC had similar size (3.39 mm ± 0.6 mm vs 3.34 mm ± 0.6 mm; P = nonsignificant), and shorter lengths (11 mm ± 2 mm vs 12 mm ± 3 mm; P = .005) compared to RegNC. No stent-related mechanical complications were reported.
Conclusions: SphNC for coronary stent postdilatation in the routine PCI clinical practice has a very high technical success rate as the first choice (98.9%), as well as in cases of RegNC failure (98.8% with low complex technique requirements, and a safe profile).
Keywords: Complex PCI. Stent postdilatation. Tapered-tip balloon. Spherical tip balloon.
RESUMEN
Introducción y objetivos: La posdilatación de stents coronarios con balones no distensibles mejora los resultados clínicos. Los balones no distensibles normales (RegNC) presentan peor navegabilidad y tienen una punta cónica que puede dificultar la posdilatación exitosa. Las condiciones mecánicas de un nuevo balón no distensible con punta esférica (EsfNC) podrían facilitar la posdilatación del stent. Evaluamos la efectividad del EsfNC en la posdilatación coronaria para la intervención coronaria percutánea en la práctica clínica habitual.
Métodos: Registro técnico prospectivo y multicéntrico para evaluar la efectividad de un nuevo EsfNC en posdilatación coronaria, con 2 grupos de estudio: uso de EsfNC como primera opción o uso de EsfNC ante el fracaso de RegNC. El evento primario fue el éxito técnico, definido como conseguir avanzar el EsfNC hasta el segmento que posdilatar dentro del stent. Los eventos secundarios fueron el éxito angiográfico, definido como éxito técnico junto con estenosis residual < 30% con flujo final TIMI 3, y el éxito del procedimiento, definido como éxito angiográfico sin complicación mecánica del stent ni eventos cardiovasculares mayores periprocedimiento.
Resultados: Se usó EsfNC en 263 lesiones (en 177 como primera opción y en 86 tras el fracaso de RegNC), en 250 procedimientos. Se usaron técnicas complejas para avanzar el EsfNC en el 9,9% de los procedimientos. Los porcentajes de éxito técnico, angiográfico y de procedimiento fueron del 98,9%, el 98,3% y el 98,3% como primera opción, y del 98,8%, el 97,7% y el 96,5% tras fracaso de RegNC, respectivamente. Los EsfNC tuvieron similar calibre (3,39 ± 0,6 frente a 3,34 ± 0,6 mm; p = no significativo) y longitud más corta (11 ± 2 frente a 12 ± 3 mm; p = 0,005) que los RegNC. No se comunicaron complicaciones mecánicas del stent.
Conclusiones: La posdilatación coronaria con EsfNC para la intervención coronaria percutánea en la práctica clínica habitual muestra un porcentaje muy alto de éxito técnico, tanto en primera opción (98,9%) como en casos de fracaso de RegNC (98,8%), con baja necesidad de técnicas complejas y buen perfil de seguridad.
Palabras clave: Intervención coronaria percutánea compleja. Posdilatación coronaria. Balón no distensible. Balón no distensible punta esférica.
Abbreviations
NC: noncompliant balloon. PCI: percutaneous coronary intervention. RegNC: regular noncompliant balloon. SphNC: spherical tip noncompliant balloon.
INTRODUCTION
Optimal stenting is crucial in the long-term clinical outcomes while proper stent expansion and apposition reduce the risk of thrombosis and restenosis.1 Coronary stent postdilatation increases luminal area while reducing stent strut malapposition.2,3
Unlike semicompliant balloons, noncompliant (NC) balloon postdilatation allows uniform dilatation at higher pressures, which reduces the risk of damage to the vessel wall (edge dissection or coronary perforation),4 and is associated with greater stent expansion and a lower rate of target lesion revascularization.5 Therefore, postdilatation using NC balloons is a common strategy to increase the luminal area of underexpanded stents or increase the stent proximal caliber in long lesions or in bifurcation techniques like the proximal optimization technique (POT) or the conventional kissing-balloon technique in a safe and predictable way.6,7
The navigability of NC balloons is more limited, a significant setback in cases of coronary tortuosity, calcified lesions or proximal stent edge malapposition. Regular noncompliant balloons (RegNC) include a cone-shaped tip that can collide with the struts or with the proximal stent edge, thus conditioning a force vector opposed to the push force that can potentially interfere with its advancement (figure 1A), and eventually lead to mechanical stent failure in cases of inadequate coaxiality. In these cases, the use of complex techniques (buddy-wire, buddy-balloon, anchoring...) or specific devices (guide catheter extension systems) are often needed to advance the balloon, which increases the cost of the procedure.
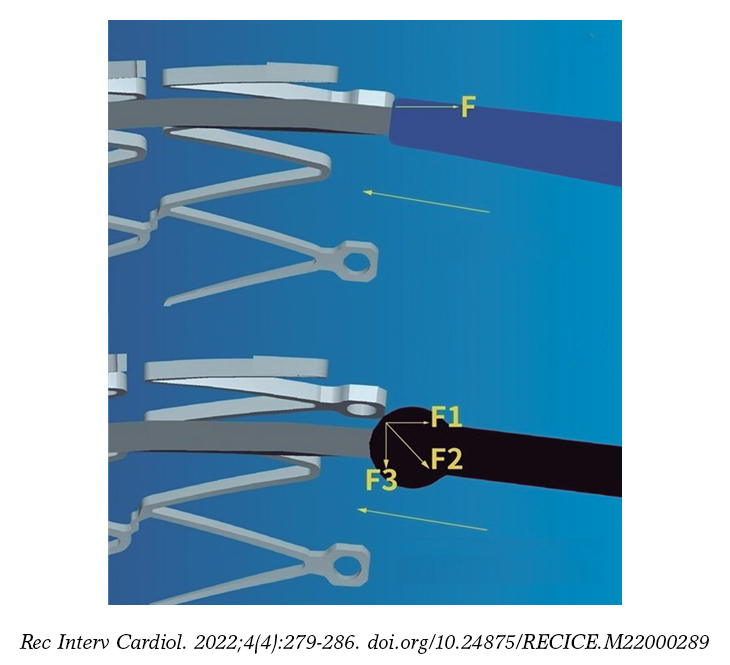
Figure 1. A: the cone-shaped tip of a regular noncompliant balloon can collide with the stent struts thus conditioning a force (F) vector opposed to the push force that can potentially interfere with its advancement. B: the spherical tip contributes to decomposing and reducing the resistance force vector opposed to the push vector, thus facilitating the balloon advancement towards the inside of the stent. Courtesy of APT Medical, China.
The cone-shaped tip has been replaced by a spherical tip in a new NC balloon (NC Conqueror Spherical tip, APT Medical, China) (SphNC). Despite its greater crossing profile (0.039 in), the spherical tip contributes to decomposing and reducing the resistance force vector opposed to the push vector (figure 1B), facilitating the advancement of the balloon until reaching the inside of the stent and the post-dilatable segment.

Figure 2. Actual appearance of the spherical tip noncompliant balloon used in the study. Courtesy of APT Medical, China.
Our objective is to assess the effectiveness of this new SphNC in coronary postdilatation during percutaneous coronary intervention (PCI) in the routine clinical practice.
METHODS
The RECONQUISTHA trial is a prospective and multicenter technical registry conducted in 16 high volume PCI-capable centers (> 500 PCIs/year)8 designed to assess the effectiveness of SphNC in coronary postdilatation during PCI in the routine clinical practice. Since it is a technical registry that used no personal or clinical data on a device approved with CE marking no ethics committee approval or informed consent forms were required.
Inclusion and exclusion criteria
The only inclusion criterion was the indication for coronary postdilatation with the SphNC according to the operator (long, calcified, ostial lesion, bifurcation and angiographic or stent balloon underexpansion). The exclusion criteria were the use of a ≤ 5-Fr guide catheter, vessel size < 2mm or > 5mm, jailed branch postdilatation without previous opening of the stent struts of the main vessel towards such branch or finding 1 of the following scenarios before postdilatation: mechanical stent failure, stent edge dissection ≥ C, coronary perforation or TIMI grade ≤ 2 flow in the main vessel or lateral branch.
Procedure
All lesions were treated with stenting according to the operator’s criterion and according to the routine clinical practice (arterial access, guide catheter caliber, predilatation or plaque modification, and intracoronary imaging). Also, they should be treated with standard antithrombotic treatment (dual antiplatelet therapy with acetylsalicylic acid, and P2Y12 receptor inhibitors prior to the PCI plus weight-adjusted unfractionated heparin at doses of 100 IU/kg with further boluses to achieve activated coagulation times between 250 s and 300 s).
The use of the SphNC was considered in 2 different clinical settings that categorized the lesions into 2 study groups: use of SphNC as first-line treatment, and use of SphNC as a second choice after failed RegNC advancement. Complex techniques like the buddy-wire, buddy-balloon, anchoring or guide catheter extension system were allowed to advance both the RegNC and the SphNC. In cases where the second choice after failed RegNCn advancement was used despite the use of a complex technique, the same complex technique with the SphNC was advised too.
The spherical tip noncompliant balloon
The NC Conqueror Spherical tip balloon (APT Medical, China) is a rapid exchange balloon catheter for percutaneous coronary interventions that is compatible with a 0.014 in intracoronary guidewire. This device has a distinctive tungsten radiopaque spherical tip (0.039 in crossing profile) designed to minimize resistance while advancing the balloon towards the inside of the stent (figure 2). It is available in calibers ranging from 2 mm to 5 mm in intervals of 0.25 mm to 0.5 mm, and lengths of 6 mm, 8 mm, 12 mm, 15 mm, 20 mm, and 30 mm. Nominal pressure stands at 12 atm, and rated pressure burst at around 20 atm (18 atm in 4.5 mm to 5 mm calibers). The device has the CE marking.
Definition of endpoints
The study primary endpoint was technical success defined as the successful advancement of the SphNC until reaching the stent post-dilatable segment. Secondary endpoints were angiographic success—defined as technical success with residual stenosis < 30% with final TIMI grade-3 flow—and procedural success defined as angiographic success without mechanical stent failure or perioperative major adverse cardiovascular events like myocardial infarction—based on the criteria established by the Academic Research Consortium [ARC]-29—stroke, coronary perforation, need for emergency heart surgery or death.
The hypothesis was to consider the study positive if technical success was achieved in > 80% of the lesions regarding the use of the SphNC as the go-to option (according to data published on technical success rates with postdilatation balloons10), and in > 30% regarding the use of the SphNC after failed RegNC advancement (random criterion based on the success of the new balloon in 1 out of 3 cases of failed RegNC advancement).
Data curation
The characteristics of the lesion and the PCI, the indication for postdilatation, any information on the devices used, and quantitative and procedural angiographic results were collected prospectively. Data was introduced in an anonymized electronic database specifically designed for the purpose of the study. Lesions were categorized based on the classification established by the American College of Cardiology and the American Heart Association (ACC/AHA).11 Coronary calcification was defined as moderate whenever coronary radiopacities would be found prior to the injection of contrast or severe whenever these radiopacities would damage both sides of the arterial lumen.12 Coronary tortuosity was defined as moderate if ≥ 3 consecutive curvatures between 45° and 90° were found during diastole or severe if any previous curvatures between 90° and 180° would be found or that encompassed the lesion.13 Angulation inside the lesion was measured as the angle between the start and the end of stenosis. The presence of ostial stenosis > 50% in the branch lateral to the lesion or the need to place the protection guidewire in the lateral branch was considered bifurcation. The stent suboptimal expansion was defined as residual stenosis ≥ 10% on the coronary quantitative angiography after the PCI. Residual stenosis ≥ 30% was considered stent underexpansion (the use of intracoronary imaging was not mandatory). Mechanical stent failure was defined as longitudinal stent deformation or fracture. The patients’ personal or clinical data were not collected.
Statistical analysis
In each of the study groups the overall and individual data were analyzed (SphNC as the go-to option, and as the second choice after failed RegNC advancement). Data was expressed as percentages regarding the categorical variables or as mean and standard deviation regarding the continuous ones. Categorical variables were compared using the chi-square test (or Fisher’s exact test when appropriate). Continuous variables were compared using the Student t test. P values < .05 were considered statistically significant.
RESULTS
From February through June 2021, the SphNC was used in 263 lesions (in 177 lesions as the go-to option, and in 86 lesions after failed RegNC advancement) in a total of 250 procedures. All the lesions were treated with state-of-the-art drug-eluting stents. The characteristics of the lesions and the PCIs, and the immediate angiographic results—both overall and with the use of the SphNC as the first choice or after failed RegNC advancement—are shown on table 1 and table 2. A total of 9.9% of the lesions required complex techniques to move the SphNC forward. Lesions in the failed RegNC group were more unfavorable with a lower rate of direct stenting, greater tortuosity and angulation inside the lesion, more need for cutting balloon during predilatation, shorter SphNC length, and a higher rate of angiographic data of suboptimal stent expansion.
Table 1. Characteristics of the lesions
| Total (N = 263) |
SphNC as the go-to option (N = 177) |
SphNC after failed RegNC (N = 86) |
P* | Total (N = 263) |
SphNC as the go-to option (N = 177) |
SphNC after failed RegNC (N = 86) |
P* | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Target vessel | .27 | AHA classification | .1 | ||||||||
| LAD | 40.7% (107) | 41.8% (74) | 38.4% (33) | A | 2.7% (7) | 4% (7) | 0% (0) | ||||
| LCx | 20.5% (54) | 17.5% (31) | 26.7% (23) | B1 | 23.6% (62) | 26% (46) | 18.6% (16) | ||||
| RCA | 30% (79) | 31.1% (55) | 27.9% (24) | B2 | 45.2% (119) | 44.1% (78) | 47.7% (41) | ||||
| LMCA | 7.6% (20) | 8.5% (15) | 5.8% (5) | C | 26.4% (57) | 26% (46) | 33.7% (29) | ||||
| CABG | 1.2% (3) | 1.1% (2) | 1.2% (1) | Baseline TIMI flow | .65 | ||||||
| Location | .98 | 0 | 21.7% (57) | 20.9% (37) | 23.3% (20) | ||||||
| Proximal | 42.6% (112) | 42.9% (76) | 41.9% (36) | 1 | 1.1% (3) | 1.7% (3) | 0% (0) | ||||
| Medial | 43.3% (114) | 42.9% (76) | 44.2% (38) | 2 | 8.4% (22) | 8.5% (15) | 8.1% (7) | ||||
| Distal | 14.1% (37) | 14.1% (25) | 12% (12) | 3 | 68.8% (181) | 68.9% (122) | 68.6% (59) | ||||
| Calcification | .54 | Bifurcation | 29.7% (78) | 27.7% (49) | 33.7% (29) | .31 | |||||
| Moderate | 39.5% (104) | 41.2% (73) | 36% (31) | 2 stents | 7.6% (20) | 5.6% (10) | 11.6% (10) | .16 | |||
| Severe | 18.6% (49) | 16.9% (30) | 22.1% (19) | Ostial | 11.1% (24) | 13% (23) | 8.1% (7) | .24 | |||
| Tortuosity | <.001 | CTO | 5.7% (15) | 7.9% (14) | 1.2% (1) | .03 | |||||
| Moderate | 35.7% (94) | 35% (62) | 37.2% (32) | STEMI | 16.3% (43) | 13.6% (24) | 22.1% (19) | .08 | |||
| Severe | 6.1% (16) | 1.7% (3) | 15.1% (13) | Lesion on the QCA | |||||||
| Lesion angulation | <.001 | MLD (mm) | 1.01 ± 1.04 | 1.05 ± 1.06 | 0.9 ± 1 | .27 | |||||
| <30 ° | 62.4% (164) | 70.1% (124) | 46.5% (40) | VRD (mm) | 3.34 ± 0.62 | 3.3 ± 0.59 | 3.44 ± 0.65 | .09 | |||
| 30º-70 ° | 30.8% (81) | 26% (46) | 40.7% (35) | Percent diameter stenosis (%) | 83 ± 17 | 82 ± 17 | 84 ± 16 | .48 | |||
| > 70 ° | 6.8% (18) | 4% (7) | 12.8% (11) | Stenotic area (%) | 88 ± 13 | 87 ± 14 | 89 ± 12 | .13 | |||
|
AHA, American Heart Association; CABG, coronary artery bypass graft; CTO, chronic total coronary occlusion; LAD, left anterior descending coronary artery; LCx, left circumflex artery; LMCA, left main coronary artery; MLD, minimal lumen diameter; QCA, quantitative coronary angiography; RCA, right coronary artery; RegNC, cone-shaped tip regular noncompliant balloon; SphNC, spherical tip noncompliant balloon; STEMI, ST-segment elevation myocardial infarction; TIMI, Thrombolysis in Myocardial Infarction; VRD, vessel reference diameter. * P between SphNC groups as the go-to option, and SphNC after failed RegNC. |
|||||||||||
Table 2. Characteristics of percutaneous coronary intervention and angiographic outcomes
| Total (N = 263) |
SphNC as the go-to option (N = 177) |
SphNC after failed RegNC (N = 86) |
P* | Total (N = 263) |
SphNC as the go-to option (N = 177) |
SphNC after failed RegNC (N = 86) |
P* | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Plaque modification | Kissing balloon | 1.9% (5) | 2.3% (4) | 1.2% (1) | ||||||
| Noncompliant balloon | 44.9% (118) | 47.5% (84) | 39.5% (34) | .45 | Other | 1.5% (4) | 1.1% (2) | 2.3% (2) | ||
| Scoring balloon | 12.5% (33) | 9% (16) | 19.8% (17) | .14 | SphNC | |||||
| Cutting balloon | 4.9% (13) | 2.3% (4) | 10.5% (9) | .01 | Caliber (mm) | 3.36 ± 0.55 | 3.34 ± 0.53 | 3.39 ± 0.6 | .5 | |
| Lithotripsy balloon | 1.9% (5) | 1.7% (3) | 2.3% (2) | .66 | Length (mm) | 12 ± 3 | 13 ± 2 | 11 ± 2 | <.001 | |
| Rotational atherectomy | 1.9% (5) | 1.1% (2) | 3.5% (3) | .33 | Atm | 18 ± 3 | 18 ± 2 | 18 ± 3 | .09 | |
| Direct stenting | 14.1% (37) | 16.9% (30) | 8.1% (7) | .05 | Complex technique | .52 | ||||
| Stent | Guide catheter extension system | 7.6% (20) | 7.9% (14) | 7% (6) | ||||||
| Caliber (mm) | 3.07 ± 0.52 | 3.04 ± 0.49 | 3.12 ± 0.57 | .3 | Buddy-wire | 1.9% (5) | 1.1% (2) | 3.5% (3) | ||
| Length (mm) | 27 ± 11 | 27 ± 10 | 27 ± 11 | .95 | Anchoring | 0.4% (1) | 0.6% (1) | 0% (0) | ||
| Atm | 14 ± 2 | 15 ± 2 | 14 ± 2 | .02 | Intracoronary imaging | 9.5% (27) | 9.1% (16) | 10.4% (9) | .51 | |
| Number of stents in the lesion | .47 | QCA after PCI | ||||||||
| 1 | 81.4% (214) | 81.4% (144) | 81.4% (70) | MLD (mm) | 3.23 ± 0.58 | 3.19 ± 0.56 | 3.29 ± 0.61 | .21 | ||
| 2 | 13.7% (36) | 12.4% (22) | 16.3% (14) | Percent diameter stenosis (%) | 4 ± 5 | 3 ± 5 | 4 ± 5 | .18 | ||
| 3 | 5% (13) | 6.2% (11) | 2.3% (2) | Stenotic area (%) | 6 ± 8 | 5 ± 8 | 7 ± 8 | .05 | ||
| Overall stent length (mm) | 32 ± 18 | 32 ± 18 | 32 ± 16 | .96 | Stent expansion | .03 | ||||
| Postdilatation indication | .29 | Optimal | 97.7% (257) | 99.4% (176) | 94.2% (81) | |||||
| Long lesion | 39.9% (105) | 44.6% (79) | 30.2% (26) | Suboptimal | 1.9% (5) | 0.6% (1) | 4.7% (4) | |||
| Suboptimal expansion | 30.8% (81) | 28.2% (50) | 36% (31) | Underexpansion | 0.4% (1) | 0% (0) | 1.2% (1) | |||
| POT | 16% (42) | 13% (23) | 22.1% (19) | Final TIMI grade-3 flow | 99.6% (262) | 99.4% (176) | 100% (86) | 1 | ||
| Calcified lesion | 6.8% (18) | 7.3% (13) | 5.8% (5) | |||||||
| Aorto-ostial lesion | 3% (8) | 3.4% (6) | 2.3% (2) | |||||||
|
Atm, balloon inflation atmospheres; MLD, minimal lumen diameter; PCI, percutaneous coronary intervention; POT, proximal optimization technique in bifurcation; QCA, quantitative coronary angiography; RegNC, cone-shaped tip regular noncompliant balloon; SphNC, spherical tip noncompliant balloon; TIMI, Thrombolysis in Myocardial Infarction. * P between SphNC groups as the go-to option, and SphNC after failed RegNC. |
||||||||||
The overall rates of technical, angiographic, and procedural success were very high and similar between both groups (table 3).
Table 3. Rates of primary and secondary endpoints
| Total (N = 63) | SphNC as the go-top option (N = 177) | SphNC after failed RegNC (N = 86) | P* | |
|---|---|---|---|---|
| Primary endpoint | ||||
| Technical success | 98.9% (260) | 98.9% (175) | 98.8% (85) | 1 |
| Secondary endpoint | ||||
| Angiographic success | 98.1% (258) | 98.3% (174) | 97.7% (84) | .66 |
| Procedural success | 97.7% (257) | 98.3% (174) | 96.5% (83) | .33 |
| Mechanical stent failure | 0% (0) | 0% (0) | 0% (0) | N/A |
| Perioperative complications | 0.4% (1) | 0% (0) | 1.2% (1) | .32 |
|
N/A, non-applicable; RegNC: cone-shaped tip regular noncompliant balloon; SphNC, spherical tip noncompliant balloon. * P between SphNC groups as the go-to option, and SphNC after failed RegNC. |
||||
The rate of technical success in the same lesion where the RegNC had failed was very high (98.8%): only 1 SphNC failed too (figure 3). The SphNC and the RegNC had a similar mean caliber (3.39 ± 0.6 mm vs 3.34 ± 0.6 mm; P = .06) while the SphNC had a shorter mean length (11 ± 2 mm vs 12 ± 3 mm; P = .005). The length of the SphNC was shorter, similar or longer in 36%, 46.5%, and 17.5% of the lesions, respectively. The same complex techniques were used to advance the RegNC and the SphNC in 7 lesions (the guide catheter extension system and the buddy-wire technique were used in 6 and 1 cases, respectively). The buddy-wire technique was used in 2 lesions to advance the SphNC, but not previously with the RegNC. In 1 lesion where the RegNC could not be advanced despite anchoring, the SphNC was moved forward without the need for a complex technique. Both the RegNC and the SphNC had been previously used on 3 and 9 occasions, respectively for predilatation purposes.
The description of failed primary and secondary endpoints with the SphNC is shown on table 4. In 2 of the 3 cases without technical success regarding the SphNC, a shorter RegNC was eventually advanced. No instances of mechanical stent failure were reported. One proximal fracture of the catheter hypotube was reported due to excessive resistance during push in 1 SphNC. Nonetheless, the device could be retrieved uneventfully. Only 1 major adverse cardiovascular event was reported: 1 distal branch perforation due to an angioplasty guidewire unrelated with the use of the SphNC that occurred while unsuccessfully trying to advance the RegNC. However, according to the definitions of the study protocol, it was adjudicated as lack of procedural success.
Table 4. Description of cases of failed spherical tip noncompliant balloon
| Case of failed SphNC | Failed event | Use of SphNC | Postdilatation indication | Success of other NC balloons | Complex technique | Complication |
|---|---|---|---|---|---|---|
| Lesion #46 | Technical success | Go-to option | Suboptimal expansion | Yes | No | No |
| Lesion #71 | Technical success | Go-to option | Long lesion | No | No | No |
| Lesion #83 | Technical success | Failed RegNC | POT | Yes | No | Hypotube rupture |
| Lesion #84 | Angiographic success (QCA) | Failed RegNC | Suboptimal expansion | N/A | Guide catheter extension system | No |
| Lesion #224 | Angiographic success (TIMI flow) | Go-to option | Suboptimal expansion | N/A | No | No |
| Lesion #258 | Procedural success | Failed RegNC | POT | N/A | No | Coronary perforation |
|
NA, non-applicable; POT, proximal optimization technique in bifurcation; QCA, quantitative coronary angiography; RegNC, cone-shaped tip regular noncompliant balloon; SphNC, spherical tip noncompliant balloon; TIMI, Thrombolysis in Myocardial Infarction. |
||||||
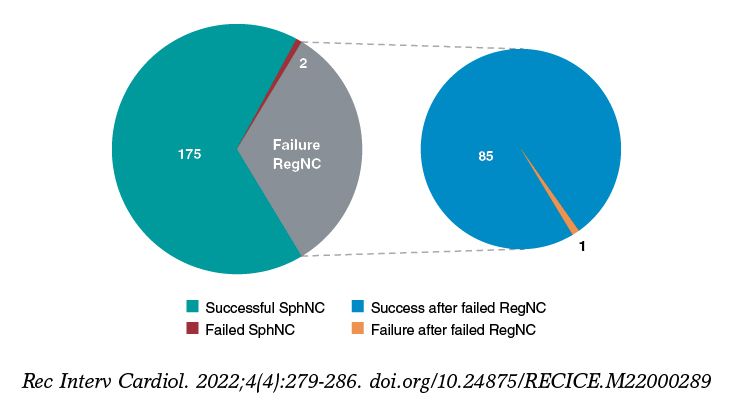
Figure 3. Overall technical success and failure of the spherical tip noncompliant balloon (SphNC), as well as in cases of failed regular noncompliant balloon (RegNC); section chart on the right.
DISCUSSION
As far as we know, it is the first time that a clinical trial—the REPIC02-RECONQUISTHA—reports on the most extensive experience using SphNC for coronary stent postdilatation. The registry included 16 high volume PCI-capable centers and collected data from 263 lesions where SphNCs were used at the operator’s discretion both as the go-to and second choice after failed RegNC advancement in the same lesion. Based on the initial hypothesis, the study can be considered positive; findings can be summarized as follows: a) very high rates of technical, angiographic and procedural success defined, respectively, as the capacity to move forward towards the inside of the stent and reach an adequate expansion without mechanical stent failure or periprocedural complications; b) very high rates of technical, angiographic and procedural success in the same lesions where the RegNC failed; and c) lower need for complex techniques to achieve technical success.
Over the last few years, the arrival of new techniques and modern devices has facilitated the performance of successful PCIs on more complex lesions in the routine clinical practice. Although the operators were not specifically encouraged to include complex lesions in the study, our data show this reality where over 70% of the lesions were type B2/C, and nearly 50% showed significant calcification, tortuosity or angulation inside the lesion. These characteristics reduce the success of the PCI14,15 and can eventually lead to stent malapposition16 and underexpansion17 or difficulties advancing the devices until reaching such stents, which means that the availability of effective and safe postdilatation balloons is essential to perform successful PCIs.
There is no data in the medical literature to compare or discuss our findings. Our study can be considered positive as it exceeded 80% of the success anticipated in the initial hypothesis. Despite the complexity of the lesions reported, the overall and subgroup outcomes of use of the SphNCs as the go-to option are nothing new since they can be expected in the assessment of any NC balloons (rate of success and proper stent expansion > 90%)10 since it is rare to find difficulties or impossibilities if complex techniques are used to advance these devices. However, these maneuvers can lead to severe complications like mechanical stent deformation.18,19 The lack of mechanical stent failure in our series places the SphNC as an effective and safe device for coronary postdilatation.
After the first 200 procedures, the percentage of cases where the SphNC was used in lesions where the RegNC would have failed was low. Since focus was on assessing the SphNC performance in this context, only inclusions in this subgroup were allowed later on. As already mentioned, the rate of RegNC failure is rare, and the rhythm of inclusion of the next 50 procedures was a slower. We designed this study group considering that the sequential use of a SphNC in the same lesion where a RegNC had failed would show the potential benefit of this new device. The SphNC achieved technical success in 98.8% of the lesions in this subgroup and validated its superiority in the exact same lesions where the RegNC had failed, which can be considered the most valuable piece of information from our study. The mean SphNC length was shorter compared to the RegNC (a 1 mm difference, which is statistically significant due to similar and narrow standard deviations, yet of uncertain practical significance). However, the operators used SphNCs and RegNCs of similar length in most of the lesions. In this study subgroup, lesions were more unfavorable, which may explain the rate of failure with RegNCs, the discretely low rate of angiographic and procedural success reported, and the presence of the complications described (fracture of the SphNC hypotube or coronary perforation).
It has been reported that the tortuosity and angulation seen until the lesion are predictors of failed PCI or perioperative complications.14,15,20 In our series, their prevalence was high—around 40%—and up to 50% in lesions where the RegNC failed. Several complex techniques for the management of these anatomies have been described,21 but they increase procedural time and cost. Eddin et al.22 determined that tortuosity and angulation were the main predictors for the use of a guide catheter extension system. Also, angulations > 45° proximal to the lesion predict its use with a 73% sensitivity and a 74% specificity. In different series, tortuosity and angulation justify the use of a guide catheter extension system in 22% to 43% of the cases.18 Despite the significant tortuosity and angulation of our series, the need for a guide catheter extension system or any other kind of complex technique to advance the SphNC was low (< 8% and 10% respectively), which is why this device emerges as a useful tool in the coronary tortuosity setting with potential to reduce procedural costs.
The study design was moderately ambitious since we hypothesized that if the SphNC were successful in 1 out of 3 lesions where the RegNC had failed this outcome would have been good enough for the new device. The fact that it exceeded the success rate of 30% proposed in the hypothesis makes us think of the results as positive. To better understand these outcomes, 5 videos have been provided as supplementary data including examples of failed RegNCs and succesful SphNCs in the same lesion.
Limitations
Despite its prospective design, the study has several limitations. The indication of postdilatation with SphNC based only on the operator’s criterion may have conditioned selection biases, thus preventing the inclusion of very unfavorable lesions. The study design does not allow us to assess the superiority of the SphNC over the RegNC regarding the lower need for complex techniques, mechanical stent failure or better angiographic and procedural outcomes. The use of intracoronary imaging was low, and a more comprehensive assessment of stent expansion with imaging techniques could have changed the data of the PCI final outcomes and, consequently, the secondary endpoints. The SphNC recrossing after first inflation was anecdotal and is, therefore, ill-advised. We should mention that our results cannot be extrapolated to coronary predilatation because the device has not been tested prior to stenting. Finally, the lack of follow-up to monitor the patients’ clinical course does not allow us to assess the clinical impact derived from the use of SphNC.
CONCLUSIONS
Coronary postdilatation with the SphNC during PCI in the routine clinical practice has a very high rate of technical success both as first choice (98.9%), and in cases of failed RegNC advancement (98.8%) with a lower need for complex techniques, and a good safety profile.
FUNDING
RECONQUISTHA is an investigator-initiated trial promoted and developed by Fundación EPIC, Spain as the clinical research organization sponsored by IZASA Medical, Spain. All the authors received research grants for their participation in the study.
AUTHORS’ CONTRIBUTIONS
J. A. Linares Vicente: design, data curation, analysis, and interpretation, and manuscript drafting. A. Pérez de Prado, and J. R. Rumoroso Cuevas: design, data curation, manuscript drafting, and critical review of its content. K. García San Román, F. Lozano Ruiz-Póveda, G. Veiga Fernández, A. Gómez Menchero, G. Moreno Terribas, G. Miñana Escrivà, J. Sánchez Gila, C. Arellano Serrano, G. Martín Cáceres, P. Bazal Chacón, P. Martín Lorenzo, F. Rebollal Leal, and J. Moreu Burgos: data curation, critical review of the content of the manuscript, and final approval.
CONFLICTS OF INTEREST
A. Pérez de Prado is an associate editor of REC: Interventional Cardiology; the journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. J. A. Linares has received lecture fees from IZASA Medical, Spain.
WHAT IS KNOWN ABOUT THE TOPIC?
- Coronary stent postdilatation with NC balloons is associated with better clinical outcomes. The complexity of PCIs in the routine clinical practice is on the rise. The navigability of RegNCs is limited, and their cone-shaped tip can complicate moving forward inside of the stent. Therefore, success could be limited in in complex lesions.
WHAT DOES THIS STUDY ADD?
- In the routine clinical practice, coronary postdilatation using SphNC while performing a PCI has a very high rate of technical success even in complex clinical settings where the RegNC has failed (especially in coronary tortuosity), a lower need for complex techniques, and a good safety profile. Therefore, it could be considered as the go-to option for coronary postdilatation when performing complex PCIs.
SUPPLEMENTARY DATA
Vídeo 1. Linares Vicente J.A. DOI: 10.24875/RECICE.M22000289
Vídeo 2. Linares Vicente J.A. DOI: 10.24875/RECICE.M22000289
Vídeo 3. Linares Vicente J.A. DOI: 10.24875/RECICE.M22000289
Vídeo 4. Linares Vicente J.A. DOI: 10.24875/RECICE.M22000289
Vídeo 5. Linares Vicente J.A. DOI: 10.24875/RECICE.M22000289
REFERENCES
1. Takano Y, Yeatman LA, Higgins JR, et al. Optimizing stent expansion with new stent delivery systems. J Am Coll Cardiol. 2001;38:1622-1627.
2. Romagnoli E, Sangiorgi GM, Cosgrave J, Guillet E, Colombo A. Drug-Eluting Stenting. The Case for Post-Dilation. JACC: Cardiovasc Interv. 2008;
1:22-31.
3. Brodie BR, Cooper C, Jones M, Fitzgerald P, Cummins F. Is adjunctive balloon postdilatation necessary after coronary stent deployment? Final results from the POSTIT trial. Catheter Cardiovasc Interv. 2003;59:184-192.
4. Seth A, Gupta S, Singh VP, Kumar V. Expert Opinion: Optimising stent deployment in contemporary practice: The role of intracoronary imaging and non-compliant balloons. Interv Cardiol. 2017;12:81-84.
5. Pasceri V, Pelliccia F, Pristipino C, et al. Clinical effects of routine postdilatation of drug-eluting stents. Catheter Cardiovasc Interv. 2014;83:898-904.
6. Mylotte D, Hovasse T, Ziani A, et al. Non-compliant balloons for final kissing inflation in coronary bifurcation lesions treated with provisional side branch stenting: A pilot study. EuroIntervention. 2012;7:1162-1169.
7. Park TK, Lee JH, Song YB, et al. Impact of non-compliant balloons on long-term clinical outcomes in coronary bifurcation lesions: Results from the COBIS (COronary BIfurcation Stent) II registry. EuroIntervention. 2016;12:456-464.
8. Moreno R, Ojeda S, Romaguera R, et al. Actualización de las recomendaciones sobre requisitos y equipamiento en cardiología intervencionista. REC Interv Cardiol. 2021;3:33-44.
9. Garcia-Garcia HM, McFadden EP, Farb A, et al. Standardized End Point Definitions for Coronary Intervention Trials: The Academic Research Consortium-2 Consensus Document. Circulation. 2018;137:2635-2650.
10. Secco GG, Buettner A, Parisi R, et al. Clinical Experience with Very High-Pressure Dilatation for Resistant Coronary Lesions. Cardiovasc Revasc Med. 2019;20:1083-1087.
11. Ryan TJ, Faxon DP, Gunnar RM, et al. Guidelines for percutaneous transluminal coronary angioplasty. A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcommittee on Percutaneous Transluminal Coronary Angioplasty). Circulation. 1988;78:486-502.
12. Madhavan MV, Tarigopula M, Mintz GS, Maehara A, Stone GW, Généreux P. Coronary Artery Calcification. J Am Coll Cardiol. 2014;63:1703-1714.
13. Jakob M, Spasojevic D, Krogmann ON, Wiher H, Hug R, Hess OM. Tortuosity of coronary arteries in chronic pressure and volume overload. Cathet Cardiovasc Diag. 1996;38:25-31.
14. Ellis SG, Vandormael MG, Cowley MJ, et al. Coronary morphologic and clinical determinants of procedural outcome with angioplasty for multivessel coronary disease. Implications for patient selection. Multivessel Angioplasty Prognosis Study Group. Circulation. 1990;82:1193-1202.
15. Moushmoush B, Kramer B, Hsieh AM, Klein LW. Does the AHA/ACC task force grading system predict outcome in multivessel coronary angioplasty? Cathet Cardiovasc Diag. 1992;27:97-105.
16. Wang B, Mintz GS, Witzenbichler B, et al. Predictors and Long‐Term Clinical Impact of Acute Stent Malapposition: An Assessment of Dual Antiplatelet Therapy With Drug‐Eluting Stents (ADAPT‐DES) Intravascular Ultrasound Substudy. J Am Heart Assoc. 2016;5:e004438.
17. Komaki S, Ishii M, Ikebe S, et al. Association between coronary artery calcium score and stent expansion in percutaneous coronary intervention. Int J Cardiol. 2021;334:31-36.
18. Fabris E, Kennedy MW, di Mario C, et al. Guide extension, unmissable tool in the armamentarium of modern interventional cardiology. A comprehensive review. Int J Cardiol. 2016;222:141-147.
19. Arnous S, Shakhshir N, Wiper A, et al. Incidence and mechanisms of longitudinal stent deformation associated with Biomatrix, Resolute, Element, and Xience stents: Angiographic and case-by-case review of 1,800 PCIs. Catheter Cardiovasc Interv. 2015;86:1002-11.
20. Ellis SG, Topol EJ. Results of percutaneous transluminal coronary angioplasty of high-risk angulated stenoses. Am J Cardiol. 1990;66:932-7.
21. Saeed B, Banerjee S, Brilakis ES. Percutaneous Coronary Intervention in Tortuous Coronary Arteries: Associated Complications and Strategies to Improve Success. J Interv Cardiol. 2008;21:504-511.
22. Eddin MJ, Armstrong EJ, Javed U, Rogers JH. Transradial interventions with the GuideLiner catheter: Role of proximal vessel angulation. Cardiovasc Revasc Med. 2013;14:275-279.

ABSTRACT
Introduction and objectives: Systemic coronary artery embolism is one of the mechanisms of acute myocardial infarction of nonatherosclerotic origin. However, the epidemiological, clinical, and angiographic profile of this entity has not been properly established yet. Our objective was to describe the clinical characteristics, angiographic features, and prognosis of acute coronary syndromes (ACS) due to systemic embolism (ACS-E), compare them to those due to coronary atherosclerosis (ACS-A), and identify predictive clinical factors of ACS-E.
Methods: All consecutive patients with ACS—admitted to a tertiary hospital from 2003 through 2018—were classified as ACS-E (n = 40) or ACS-A (n = 4989), and prospectively recruited on a multipurpose database.
Results: Patients with ACS-E were younger (27.5% vs 9.6% were < 45 years old, P < .001), more often women (42.5% vs 22.5%, P = .003), and had higher rates of atrial fibrillation (AF) (40.0% vs 5.3%, P < .001), previous stroke (15.0% vs 3.6%, P < .001), active neoplasms (17.5% vs 6.9%, P =.009), and previous valvular surgery (12.5% vs 0.5%, P < .001). Also, a higher proportion of them were on warfarin (27.5% vs 2.9%, P < .001). The most frequent culprit vessel was the left anterior descending coronary artery in both groups. A percutaneous coronary intervention was attempted in all patients with ACS-A, and in 75.0% of those with ACS-E (P < .001) being successful in 99.1% and 80.0%, respectively. The in-hospital all-cause mortality rate was 15.0% regarding ACS-E, and 4.0% in the control group (P < .001). A multivariate analysis was performed to study the independent predictors of ACS-E, identify AF, previous valvular surgery, and active neoplasms, younger age, and female sex.
Conclusions: ACS-E and ACS-A have different clinical and angiographic characteristics. Atrial fibrillation, previous valvular surgery, active neoplasms, younger age, and female sex were all independent predictors of ACS-E.
Keywords: Coronary artery embolism. Atrial fibrillation. Acute coronary syndrome. Myocardial infarction.
RESUMEN
Introducción y objetivos: La embolia coronaria de origen sistémico representa uno de los mecanismos de infarto agudo de miocardio de causa no aterosclerótica. Sin embargo, el perfil epidemiológico, clínico y angiográfico de esta entidad no ha sido aún bien definido. Nuestro objetivo fue describir las características clínicas y angiográficas y el pronóstico de los síndromes coronarios agudos (SCA) de origen embólico (SCA-E), compararlos con aquellos debidos a aterosclerosis (SCA-A) e identificar predictores clínicos de SCA-E.
Métodos: Todos los pacientes con SCA atendidos en un hospital terciario entre 2003 y 2018 se clasificaron en SCA-E (n = 40) o SCA-A (n = 4.989) e incluidos de forma prospectiva en un registro multipropósito.
Resultados: Entre los pacientes con SCA-E existía mayor proporción de jóvenes (27,5 frente a 9,6% tenían menos de 45 años, p < 0,001), mujeres (42,5 frente a 22,5%, p = 0,003), fibrilación auricular (FA) (40,0 frente a 5,3%, p < 0,001), neoplasias activas (17,5 frente a 6,9%, p = 0,009), cirugía valvular previa (12,5 frente a 0,5%, p < 0,001) y una mayor proporción de los mismos se encontraba en tratamiento con warfarina (27,5 frente a 2,9%, p < 0,001). El vaso responsable con mayor frecuencia fue la descendente anterior en ambos grupos. En todos los pacientes con SCA-A se llevó a cabo una intervención coronaria percutánea, frente al 75,0% de los pacientes con SCA-E (p < 0,001), la cual se completó con éxito en el 99,1% y el 80,0% de los casos, respectivamente. La mortalidad por todas las causas en el grupo de SCA-E fue del 15,0% frente al 4,0% en el grupo control (p < 0,001). Se llevó a cabo un análisis multivariante para estudiar predictores independientes de SCA-E, identificando la FA, la cirugía valvular previa, la presencia de una neoplasia activa, una menor edad y el sexo femenino.
Conclusiones: Los SCA-E y los SCA-A presentan características clínicas y angiográficas diferentes. La FA, la cirugía valvular previa, la presencia de una neoplasia activa, ser más joven y el sexo femenino son predictores independientes de SCA-E.
Palabras clave: Embolia coronaria. Fibrilacion auricular. Sindrome coronario agudo. Infarto de miocardio.
Abbreviations
ACS: acute coronary syndrome. ACS-A: acute coronary syndrome due to atherosclerosis. ACS-E: acute coronary syndrome due to systemic embolism. AF: atrial fibrillation. AMI: acute myocardial infarction. STEMI: ST-segment elevation myocardial infarction.
INTRODUCTION
Systemic coronary artery embolism is one of the mechanisms of acute myocardial infarction (AMI) of non-atherosclerotic origin and represents 3% to 14% of all acute coronary syndromes (ACS) reported, according to angiographic and autopsy studies. However, the real prevalence of this entity remains unknown due to the uncertainty of its diagnosis in the acute setting.1,2
Atrial fibrillation (AF), cardiomyopathies, valvular heart disease, malignancies, and infective endocarditis have previously been associated with ACS due to systemic embolism (ACS-E).1,3 Nevertheless, the epidemiological, clinical, and angiographic profile of this entity has not been properly established yet.
Our objective was to describe the clinical characteristics, angiographic features, therapeutic management, and prognosis of ACS-E, compare it to ACS due to coronary atherosclerosis (ACS-A), and identify predictive clinical factors of ACS-E.
METHODS
Study population
All consecutive patients with ACS—admitted to a tertiary hospital from January 2003 through December 2018—were evaluated, classified as ACS-E or ACS-A, and prospectively recruited on a multipurpose database. The protocol was approved by the local ethics committee (internal code 22/137-E), and patients’ informed consent was waived because it involved only the analysis of data obtained during standard clinical practice.
AMI was defined as elevated cardiac troponin levels (myocardial injury) with clinical evidence of acute myocardial ischemia including symptoms, new ischemic electrocardiographic changes, development of pathological Q waves on the electrocardiogram, new regional wall motion abnormalities in a pattern consistent with ischemic aetiology, and/or angiographic identification of a coronary thrombus.4 All patients underwent a thorough diagnostic work-up including detailed clinical histories and physical examinations, serial electrocardiograms, blood tests, transthoracic echocardiographies, and invasive coronary angiographies. Intracoronary imaging techniques like optical coherence tomography or intravascular ultrasound were left to the operator’s discretion.
Diagnosis of ACS-E was achieved according to the angiographic evidence of coronary artery thrombosis without atherosclerotic components, concomitant multi-site coronary artery embolism or concomitant systemic embolization excluding left ventricular thrombus due to AMI.1 Only emboli of principal coronary arteries were considered. Patients with the following angiographic findings were systematically excluded: a) presence of atherosclerosis at culprit lesion level, b) evidence of > 25% coronary artery stenosis outside the culprit lesion, c) plaque rupture or coronary erosion at culprit lesion level found on the intravascular imaging, d) coronary artery ectasia, and e) other causes of non-atherosclerotic AMI (vasospasm, spontaneous coronary artery dissection).
Angiographic evaluation of the culprit site was performed by 2 expert operators with an intention to rule out a) the presence of thrombus (defined as noncalcified filling defect outlined by contrast media), b) presence of angiographic stenosis, and c) signs of atherosclerosis (eg, vessel wall calcification). The rest of the angiogram was assessed looking for angiographic stenosis or atherosclerosis.
Clinical events
Epidemiological data, clinical features, angiographic characteristics, management, and outcomes were prospectively collected as patients were recruited and retrospectively analysed. The long-term follow-up of ACS-E was performed by monitoring any recurrences of systemic emboli (including cardiogenic stroke), and the occurrence of major adverse cardiovascular and cerebrovascular events including cardiac death, myocardial infarction, new percutaneous coronary intervention (PCI), hospitalization due to heart failure or stroke more than 30 days after admission due to ACS-E.
In the present study, we first performed a detailed description of the episodes of ACS-E followed by a comparison to ACS-A to identify clinical peculiarities, and predictors.
Statistical analysis
Quantitative variables were expressed as median and interquartile range [IQR] or mean and standard deviation. The assessment of normality and equality of variances for continuous data was performed using the Shapiro-Wilk test and the Levene test, respectively. Thereafter, continuous variables were compared using the Student t test, the Fisher-Pittman permutation test or the median test when appropriate. Categorical variables were expressed as frequencies and percentages.
Variables in which statistically significant differences were seen in the univariate model and those clinically relevant were introduced in a multivariate analysis using stepwise logistic regression to identify clinical predictors of ACS-E.
All tests were 2-sided, and differences were considered statistically significant with P values < .05. Statistical analyses were performed using Stata/IC12.1 statistical software package (StataCorp, College Station, Texas, United States).
RESULTS
During the study period, a total of 5029 patients with ACS were included. After applying the previously described diagnostic criteria, 40 patients (0.8%) were classified as ACS-E and 4989 (99.2%) as ACS-A.
Acute coronary syndrome due to systemic embolism population
Regarding patients with ACS-E, 17 were women (42.5%), and the population’s mean age was 60.3 years old. A total of 2 patients (5.0%) had a past medical history of exertional angina, 4 (10.0%) carried a prosthetic valve, and 2 (5.0%) and 1 (2.5%) had non-corrected severe mitral regurgitation, and severe aortic stenosis, respectively. The mean left ventricular ejection fraction was 55.0% ± 12.3%, and 16 patients (40.0%) had any form of AF. Also, 1 patient (2.5%) was diagnosed with infective endocarditis in the aortic valve right after being admitted due to ACS. Regarding other medical conditions, 7 patients (17.5%) had active neoplasms, and 3 (7.5%) chronic kidney disease. Information associated with other baseline characteristics is shown on table 1 of the supplementary data.
Table 1. Baseline epidemiological and clinical characteristics
| ACS-A N = 4989 | ACS-E N = 40 | P | |
|---|---|---|---|
| Age (years) | 63.0 ± 13.4 | 60.3 ± 18.7 | .129 |
| Age < 45 years | 480 (9.6) | 11 (27.5) | < .001 |
| Age > 80 years | 559 (11.2) | 9 (22.5) | .025 |
| Female sex | 1120 (22.5) | 17 (42.5) | .003 |
| Diabetes | 1087 (21.8) | 4 (10.0) | .070 |
| Hypertension | 2632 (52.8) | 16 (40.0) | .108 |
| Dyslipidemia | 2192 (43.9) | 11 (27.5) | .037 |
| Smoking | 3101 (62.2) | 22 (55.0) | .353 |
| BMI | 27.6 ± 4.1 | 27.1 ± 4.2 | .424 |
| Chronic kidney failure | 239 (4.8) | 3 (7.5) | .425 |
| Peripheral vascular disease | 241 (4.8) | 1 (2.5) | .493 |
| Stroke | 181 (3.6) | 6 (15.0) | < .001 |
| Active neoplasm | 343 (6.9) | 7 (17.5) | .009 |
| AF | 262 (5.3) | 16 (40.0) | < .001 |
| Treatment with warfarin | 143 (2.9) | 11 (27.5) | < .001 |
| Previous valvular surgery | 25 (0.5) | 5 (12.5) | < .001 |
| Past medical history of angina | 1698 (34.0) | 2 (5.0) | < .001 |
|
ACS-A, acute coronary syndrome due to atherosclerosis; ACS-E, acute coronary syndrome due to systemic embolism; AF, atrial fibrillation; BMI, body mass index; NSTEMI, non-ST-elevation acute myocardial infarction; STEMI, ST-segment elevation myocardial infarction. |
|||
A total of 32 patients (80.0%) had ST-segment elevation myocardial infarction (STEMI) 3 of whom received fibrinolytic therapy, undergoing bailout PCI in 2 of the cases. A total of 28 patients (70.0%) underwent a primary PCI and the remaining 12 (30.0%) were catheterized in another scenario. The most frequent culprit vessel was the left anterior descending coronary artery (LAD) that accounted for 13 (32.5%) of the cases followed by the right coronary artery (n = 10; 25.0%), and the left circumflex artery (n = 9; 22.5%). Besides, the proximal (n = 12; 30.0%) and medium (n = 12; 30.0%) segments of the vessels were the ones most often compromised (table 2 of the supplementary data).
| ACS-A N = 4989 | ACS-E N = 40 | P | |
|---|---|---|---|
| Culprit lesions | |||
| LMCA | 113 (2.3%) | 1 (2.5%) | .921 |
| LAD | 2274 (45.6%) | 15 (37.5%) | .108 |
| Cx | 1064 (21.3%) | 11 (27.5%) | .344 |
| RCA | 1902 (38.1%) | 10 (25.0%) | .125 |
| Number of vessels with moderate lesions (> 50%) | 1.6 ± 0.0 | 0.8 ± 0.1 | < .001 |
| Number of vessels with severe lesions (> 70%) | 1.3 ± 0.0 | 0.8 ± 0.1 | < .001 |
|
ACS-A, acute coronary syndrome due to atherosclerosis; ACS-E, acute coronary syndrome due to systemic embolism; Cx, circumflex coronary artery; LAD, left anterior descending coronary artery; LMCA, left main coronary artery; PCI, percutaneous coronary intervention; RCA, right coronary artery. |
|||
On the coronary angiography, 25 patients (62.5%) showed TIMI grade-0 flow (Thrombolysis in Myocardial Infarction) before crossing the wire. Twenty-nine cases (72.5%) received thrombus aspiration therapy and 7 underwent balloon angioplasty. None of the patients were treated with stenting, but TIMI grade-3 flow was observed in 32 cases (77.5%) after the PCI (table 3 of the supplementary data). Regarding intracoronary imaging during the PCI, pre- and postoperative optical coherence tomography and intravascular ultrasound were performed in 3 (7.5%) and 1 (2.5%) patients, respectively. Antithrombotic treatment at presentation and after PCI is shown on table 4 of the supplementary data.
Table 3. Complications during PCI, hospitalization, and follow-up in patients with ACS-E
| During PCI | |
| Cardiac arrest | 3 (7.5) |
| Slow flow/no reflow | 8 (20.0) |
| Perforation | 1 (2.5) |
| Embolizationa | 15 (37.5) |
| Coronary dissection | 0 (0) |
| Coronary perforation | 1 (2.5) |
| Cardiac tamponade | 0 (0) |
| During admission | |
| Vascular complicationsb | 2 (5.0) |
| Heart failure | 12 (30.0) |
| Arrhythmic complicationsc | 7 (17.5) |
| Extracardiac complicationsd | 9 (22.5) |
| Death | 6 (15.0) |
| At the follow-up | |
| MACCE | 13 (38.2) |
| AMI | 4 (11.8) |
| New PCI | 2 (5.9) |
| Stroke | 2 (5.9) |
| Hospitalization | 11 (32.4) |
| Heart failure | 11 (32.4) |
| NYHA | |
| I | 24 (70.6) |
| II | 6 (17.6) |
| III | 1 (2.9) |
| IV | 4 (11.8) |
| Systemic embolism | 0 (0) |
| Pulmonary embolism | 1 (2.9) |
| Deathe | 12 (35.3) |
|
AMI, acute myocardial infarction; PCI, Percutaneous coronary intervention; MACCE, major adverse cardiovascular and cerebrovascular events; NYHA, New York Heart Association Functional Classification. a In 2 cases, embolization of thrombotic material reached a different vessel from the culprit one. b 1 case of femoral pseudoaneurysm and radial pseudoaneurysm, respectively were treated with conservative measures. c 4 cases of bradyarrhythmia and 3 cases of tachyarrhythmia. d 8 cases of infection and 1 case of stroke coexisting with subarachnoid haemorrhage. e Due to heart failure in 5 cases, ventricular arrythmia in the AMI setting in 1 case and multiorgan failure due to advanced pulmonary neoplasm in a different case. In the remaining the patients, the cause of death could not be identified. |
|
Table 4. Multivariate analysis to identify clinical predictors of acute coronary syndrome due to systemic embolism
| Variables* | Adjusted OR (95%CI) | P |
|---|---|---|
| Age (years) | 0.95 (0.92-0.97) | < .001 |
| Female sex | 2.80 (1.37-5.65) | .007 |
| Dyslipidemia | 0.45 (0.22-0.93) | .024 |
| Active neoplasm | 3.37 (1.33-8.54) | .019 |
| Previous valvular surgery | 4.28 (1.19-15.5) | .038 |
| Past medical history of angina | 0.17 (0.05-0.55) | < .001 |
| AF | 16.10 (7.23-35.9) | < .001 |
|
95%CI, 95% confidence interval; AF, atrial fibrillation; OR, odds ratio. * Variables from the univariate model introduced in the analysis included: age, female sex, diabetes, dyslipidemia, stroke, active neoplasm, previous valvular surgery, past medical history of angina, AF, and chronic treatment with oral anticoagulants. |
||
Comparison between acute coronary syndrome due to systemic embolism and acute coronary syndrome due to atherosclerosis
Baseline characteristics
Compared to ACS-A, there was a significantly higher proportion of patients under 45 and over 80 years old in the ACS-E group. Besides, a higher proportion of women was observed (42.5% vs 22.5%; P = .003). Among these patients, cardiovascular risk factors were less prevalent compared to those with ACS-A, although statistically significant differences were only seen regarding dyslipidemia. A significantly higher proportion of patients with ACS-E had active neoplasms, AF, previous strokes, and had undergone heart valve surgery. Also, 27.5% of the patients from the ACS-E group were on warfarin (P < .001) at presentation whereas the patients with ACS-A often had a past medical history of angina (34.0% vs 5.0%; P < .001). The inter-group differences regarding other medical conditions are also shown on table 1.
Clinical and angiographic characteristics and outcomes
Regarding the episode of ACS, no differences were seen regarding the presentation as STEMI between both groups (ACS-E, 80.0% vs ACS-A, 67.0%; P = .082). However, patients with ACS-A showed significantly longer times between the diagnosis of ACS and the performance of a coronary angiography (1.16 ± 0.8 hours vs 0.81 ± 0.5 hours; P = .003). No differences were seen regarding the rate of cardiogenic shock.
The presence of other moderate or severe stenoses, apart from the culprit one, was significantly more frequent among patients with ACS-A (table 2). PCI was attempted in all the patients with ACS-A and in 75.0% of those with ACS-E (P < .001) being successful in 99.1% and 80.0%, respectively. Conversely, adjuvant treatment with GP IIb/IIIa inhibitors was used in 55.0% of the patients with ACS-E and 36.0% of the patients from the ACS-A group (P = .020).
Complications during PCI and hospitalization in the ACS-E group are shown on table 3 including death that occurred in 5 patients (12.5%) due to heart failure/cardiogenic shock and anoxic encephalopathy after cardiac arrest in another case. A control coronary angiography was performed in 14 cases (40.0%) with persistence of culprit vessel compromise in 2 (14.3%). The median follow-up after the episode was 5.8 ± 4.8 years. Three days after emergency thrombus aspiration due to acute LAD occlusion, a 51-year-old woman with acute myeloid leukemia presented a recurrent ACS-E with new compromise of both the LAD and a marginal branch. No recurrent emboli in other systemic territories were identified in any of the cases. However, major adverse cardiovascular and cerebrovascular events at the follow-up occurred in 13 patients with ACS-E (38.2%) while death occurred in 12 patients (35.3%) being attributed to cardiac causes in 6 cases (50.0%) (table 3). The overall major adverse cardiovascular and cerebrovascular events-free survival during hospitalization and at the follow-up was estimated using Kaplan-Meier curves (figure 1).
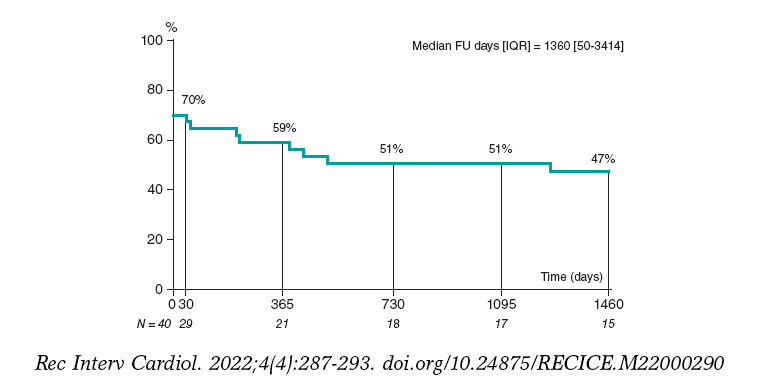
Figure 1. MACCE-free survival during admission and at the 4-year follow-up in patients with ACS-E. ACS-E, acute coronary syndrome due to systemic embolism, FU, follow-up; IQR, interquartile range; MACCE, major adverse cardiovascular and cerebrovascular events.
The in-hospital all-cause mortality rate was 15.0% in the ACS-E group and 4.0% in the control group (P < .001).
Predictors of acute coronary syndrome due to systemic embolism
To determine the clinical predictors of ACS-E, a multivariate analysis was performed including those variables with statistically significant differences in the univariate model and those considered clinically relevant. Therefore, younger age, female sex, an active neoplasm, previous heart valve surgery, and a past medical history of AF were identified as independent predictive factors for ACS-E (table 4, figure 2).
Figure 2. Independent clinical predictors of ACS-E. ACS-E, acute coronary syndrome due to systemic embolism.
DISCUSSION
The main findings of our study include a) the prevalence of ACS-E in patients admitted due to AMI was low (0.8%); b) the in-hospital mortality rate was higher among patients with ACS-E as compared to ACS of atherosclerotic origin; and c) being younger, female sex, an active neoplasm, previous heart valve surgery, and AF were identified as ACS-E predictors.
Systemic coronary artery embolism is one of the underlying mechanisms of AMI of non-atherosclerotic cause.4 First autopsy studies reported a prevalence of coronary emboli in patients with AMI of 13%5 although subsequent studies conducted at the clinical setting described a frequency of around 3%.1 The low prevalence seen in our series (0.8%) may be associated with strict diagnostic criteria excluding patients with coronary artery stenosis > 25% outside the culprit lesion, and emboli due to secondary coronary arteries. However, the real occurrence of ACS-E remains unknown since the early presentation can be indistinguishable from an ACS-A.6
Also, the limited rate of coronary artery emboli reported compared to other vascular territories may also be associated with intrinsic anatomical and physiological characteristics like aortic caliber differences, the acute angle at which the coronary arteries originate at the sinus of Valsalva,7 and the position of the coronary ostia behind the valve cusps during systole.3,8
Although some series comparing ACS-A and ACS-E have not described gender differences when focusing on STEMI,2 in our study, the proportion of women was significantly higher among ACS-E (43% vs 22%; P = .003). Similarly, Shibata et al. reported rates of 40% vs 29% (P = .087).1 Besides, according to the aforementioned authors, a lower prevalence of traditional cardiovascular risk factors was seen within the embolic group of our cohort, although statistically significant differences were only noticed regarding dyslipidemia (27.5% vs 43.9%; P = .037).
Regarding the compromise of coronary arteries, the LAD was the most commonly affected vessel in both the ACS-E and the ACS-A (table 3). Similarly, a previous autopsy study had shown that coronary emboli are up to 4 times more common in the LAD compared to the right coronary artery, and in the LAD compared to the the left circumflex artery.5 Also, in a recent systematic review including 129 case reports and case series of coronary emboli, Lacey et al. described that the LAD was the most frequently affected vessel (45.3%).6 However, such differences in the distribution of culprit coronary vessels may be explained by bias associated with the fact that arteries with larger territories are more likely to be involved in autopsies1 and case reports.
On the interventional treatment used, in our study, 30 patients (75.0%) from the ACS-E group underwent thrombus aspiration followed by balloon angioplasty in 8 cases. None of the patients from this group were treated with stenting. Similarly, Shibata et al. performed initial thrombus aspiration in 96.6% of embolic patients undergoing PCI followed by balloon angioplasty in 14.3% of the cases and stenting in 17.9%.1 Thrombus aspiration has proven to be a feasible option to treat AMI with angiographic evidence of thrombus including cases associated with coronary emboli.9 However, these devices may be less useful to aspirate large thrombi due to the smaller diameter of the lumen of the inner catheter.10 Besides, in specific situations like small arteries or distal coronary occlusions, simple wire manipulation added to antithrombotic drugs (including glycoprotein IIb/IIIa inhibitors, which were more frequently used in the ACS-E group) may be the preferred option to achieve reperfusion.2
At the follow-up after an episode of ACS-E (5.8 ± 4.8 years) in our series, the major adverse cardiovascular and cerebrovascular events occurred in 37.1% of the patients. However, no recurrences of systemic emboli were documented in accordance with other previous series.2 The in-hospital all-cause mortality rate was significantly higher among patients with ACS-E (15% vs 4%; P < .001) mainly due to cardiovascular causes. Shibata et al. reported no differences in the 30-day mortality rate, but significantly higher cardiovascular and all-cause mortality rates in ACS-E compared to ACS-A.1 Similarly, Popovic et al. observed that 64% of all deaths reported at the follow-up after an episode of STEMI due to coronary embolism were due to cardiac causes.2
Finally, after multivariate analysis, AF, previous heart valve surgery, active neoplasm, female sex, and younger age were identified as clinical predictors of ACS-E. AF has been described as the most frequent condition predisposing to coronary artery embolism being present in 40.0% of ACS-E in our study and in up to 73% in other current series.1,3 However, early studies reported that valvular heart disease, especially rheumatic, and infective endocarditis represented the most common causes of coronary artery embolism.5,11 This disparity may be associated with the advances made in antibiotic therapy implementation over the last few decades, and the remarkable increase of AF prevalence parallel to the gradual aging of the population.1,2,12,13 Furthermore, it has been reported that the risk of AMI associated with AF is significantly higher in women14,15 and patients without coronary artery disease.15-18
On the other hand, it is fully recognized that patients with active neoplasms are at a significantly higher risk of developing thrombotic events, both venous and arterial.19 The pathogenesis of cancer-associated coagulopathy is complex including a multifactorial interaction among the patient’s comorbidities, the specific malignancy, and treatment with several chemotherapeutic agents or immunomodulatory drugs that often lead to hypercoagulability, platelet activation, and endothelial injury.20 Besides, it has also been described that malignancy is associated with a higher risk of developing AF following interactions at the pathophysiological level.21,22 In our series, 17.5% of the patients presented active neoplasms in accordance with Popovic et al.2 who reported a prevalence of 15.1% notably higher than the one reported by Shibata et al.1 and Lacey et al.6 of 10% and 1.4%, respectively.
Limitations
The present study presents several limitations. First, being a retrospective study may have resulted in a certain degree of bias. Secondly, applying strict diagnostic criteria which excluded patients with ≥ 25% coronary artery stenosis outside the culprit lesion may have omitted cases of ACS-E in patients with concomitant coronary artery disease. Thirdly, in contrast with all previous reports on this matter, only emboli of major coronary arteries were considered, which possibly resulted in a lower number of ACS-E being diagnosed. Finally, including patients over a long period of time may explain some differences in treatment modalities, and the low use of intracoronary imaging seen in our series.
CONCLUSIONS
ACS-E and ACS-A have different clinical and angiographic characteristics. Female sex, younger age, past medical history of active neoplasms, previous valvular surgery, and AF were all independent predictors of ACS-E. Patients with ACS-E had a higher in-hospital mortality rate mainly due to cardiovascular causes.
FUNDING
None whatsoever.
AUTHORS’ CONTRIBUTIONS
All authors contributed to the study conception and design. Material preparation and data collection were prepared by A. Jerónimo, A. Travieso, A. McInerney, B. Hennessey, and L. Marroquín. Statistical analysis was conducted by A. Jerónimo, M.J. Pérez- Vyzcaino, and N. Gonzalo. The manuscript first draft was written by A. Jerónimo, and N. Gonzalo, and all authors commented on previous versions of the manuscript. All authors read and approved the manuscript final version.
CONFLICTS OF INTEREST
None reported.
WHAT IS KNOWN ABOUT THE TOPIC?
- According to angiographic studies and autopsies, systemic coronary artery embolism is representative of 3% to 14% of all ACSs. However, the real prevalence of this entity remains unknown due to uncertainty of its diagnosis in the acute setting. AF, infective endocarditis, valvular heart disease, and malignancies have been associated with ACS-E, but the clinical and angiographic profile of this entity has not been properly established to this date.
WHAT DOES THIS STUDY ADD?
- Our study describes the epidemiological, clinical, and angiographic characteristics of patients with ACS-E comparing them to ACS-A and admitted to a single centre during the same period of time. On this regard, patients with ACS-E were younger compared to those with ACS-A, female in a higher proportion, and more often had AF, previous stroke, previous valvular surgery, and active neoplasms. The left anterior descending coronary artery was the most common culprit vessel in both groups, but patients with ACS-A presented with a significantly higher proportion of other significant stenoses. On the therapeutic approach regarding the PCI, thrombus aspiration was the most frequent strategy in ACS-E without stenting in any of the cases. Besides, the in-hospital all-cause mortality rate was significantly higher among patients with ACS-E mainly due to cardiovascular causes. A younger age, female sex, active neoplasms, previous valvular surgery, and a past medical history of AF were identified as independent clinical predictors of ACS-E.
SUPPLEMENTARY DATA
REFERENCES
1. Shibata T, Kawakami S, Noguchi T, et al. Prevalence, Clinical Features, and Prognosis of Acute Myocardial Infarction Attributable to Coronary Artery Embolism. Circulation. 2015;132:241–250.
2. Popovic B, Agrinier N, Bouchahda N, et al. Coronary Embolism Among ST-Segment-Elevation Myocardial Infarction Patients:Mechanisms and Manegement. Circ Cardiovasc Interv. 2018;11:e005587.
3. Kolodgie FD, Virmani R, Finn A V, Romero ME. Embolic Myocardial Infarction as a Consequence of Atrial Fibrillation:A Prevailing Disease of the Future. Circulation. 2015;132:223–226.
4. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40:237-269.
5. Prizel KR, Hutchins GM, Bulkley BH. Coronary artery embolism and myocardial infarction. Ann Intern Med. 1978;88:155-161.
6. Lacey MJ, Raza S, Rehman H, Puri R, Bhatt DL, Kalra A. Coronary embolism:A systematic review. Cardiovasc Revasc Med. 2020;21:367-374.
7. Cheng JT, Cahill WJ, Foley EF. Coronary embolism. J Am Med Assoc. 1953;153:211-213.
8. Cheng TO. Coronary embolism. Int J Cardiol. 2009;136:1-3.
9. Kotooka N, Otsuka Y, Yasuda S, Morii I, Kawamura A, Miyazaki S. Three cases of acute myocardial infarction due to coronary embolism:treatment using a thrombus aspiration device. Jpn Heart J. 2004;45:861-866.
10. Stoel MG, von Birgelen C, Zijlstra F. Aspiration of embolized thrombus during primary percutaneous coronary intervention. Catheter Cardiovasc Interv. 2009;73:781-786.
11. Charles RG, Epstein EJ. Diagnosis of coronary embolism:A review. J R Soc Med. 1983;76:863-869.
12. Roxas CJ, Weekes AJ. Acute myocardial infarction caused by coronary embolism from infective endocarditis. J Emerg Med. 2011;40:509-514.
13. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS):The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42:373-498.
14. Soliman EZ, Safford MM, Muntner P, et al. Atrial fibrillation and the risk of myocardial infarction. JAMA Intern Med. 2014;174:107-114.
15. Emdin CA, Wong CX, Hsiao AJ, et al. Atrial fibrillation as risk factor for cardiovascular disease and death in women compared with men:systematic review and meta-analysis of cohort studies. BMJ. 2016;532:h7013.
16. Ruddox V, Sandven I, Munkhaugen J et al. Atrial fibrillation and the risk for myocardial infarction, all-cause mortality and heart failure:A systematic review and meta-analysis. Eur J Prev Cardiol. 2017;24:1555-1566.
17. Guo XY, Li N, Du X, et al. Atrial fibrillation is associated with an increased risk of myocardial infarction:insights from a meta-analysis. Atherosclerosis. 2016;254:1–7.
18. Bayturan O, Puri R, Tuzcu EM, et al. Atrial fibrillation, progression of coronary atherosclerosis and myocardial infarction. Eur J Prev Cardiol. 2017;24:373–381.
19. Falanga A, Schieppati F, Russo D. Cancer Tissue Procoagulant Mechanisms and the Hypercoagulable State of Patients with Cancer. Semin Thromb Hemost. 2015;41:756-764.
20. Aronson D, Brenner B. Arterial thrombosis and cancer. Thromb Res. 2018;164 Suppl 1:S23-S28.
21. Liu F, Xu Z, Luo J, et al. Effectiveness and Safety of DOACs vs. VKAs in AF Patients With Cancer:Evidence From Randomized Clinical Trials and Observational Studies. Front Cardiovasc Med. 20215;8:766377.
22. Chu G, Versteeg HH, Verschoor AJ, et al. Atrial fibrillation and cancer - An unexplored field in cardiovascular oncology. Blood Rev. 2019;35:59-67.
- Incidence, morbidity and mortality, and management of acute coronary syndrome during the time of COVID-19 lockdown
- Selective serotonin reuptake inhibitors and bleeding risk after PCI. A propensity score matching study
- Clinical follow-up of long nontapered sirolimus-eluting coronary stent in real-world patients with de novo lesions. The Billar registry
- Stent-grafts versus drug-eluting stents in arterial aneurysms, insights from the International Coronary Artery Aneurysm Registry (CAAR)







Interviews

An interview with Bruno Scheller
aServicio de Cardiología, Hospital Universitario de La Princesa, Instituto de Investigación Sanitaria de La Princesa (IIS-IP), Universidad Autónoma de Madrid, Spain
bCentro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain




