
A 55-year-old woman with an incomplete atrioventricular canal, who underwent repair of the mitral cleft and patch closure of the ostium primum type defect, followed by mitral bioprosthesis implantation (Carpentier PERIMOUNT 27, Edwards, United States) in adulthood. She developed episodes of left atrial flutter. Due to the inability to perform a transseptal puncture, we proceeded with retroaortic atrioventricular node ablation, resulting in iatrogenic left main coronary artery dissection, which resolved after drug-eluting stent implantation (figure 1A-D, videos S1 and S2). During follow-up, she showed signs of progressive prosthetic degeneration (figure 2A-B, videos S3 and S4), which led to transcatheter mitral valve-in-valve implantation. We performed a transseptal puncture of the severely calcified patch (figure 2C-D) using a Versacross system (Boston Scientific, United States). Then, we used a deflectable catheter to advance a high-support guidewire, which was, eventually, captured in the left ventricle, establishing a venoarterial loop. Afterwards, we performed a septostomy with an Atlas Gold 16 mm × 45 mm balloon catheter (BD, United States) and with great difficulty given the anatomical complexity, we advanced a 26-Fr DRYSEAL sheath (Gore, United States) into the left atrium through which we implanted a SAPIEN 3 Ultra 26 bioprosthesis (Edwards, United States) with a nominal +2 cm³ inflation. Good expansion was observed, with slight protrusion into the left ventricle without conflict with the outflow tract (figure 3A-D, video S5). The patient was discharged with normal prosthetic valve function, which was maintained at the 1-year follow-up (video S6). The patient signed the informed consent form.
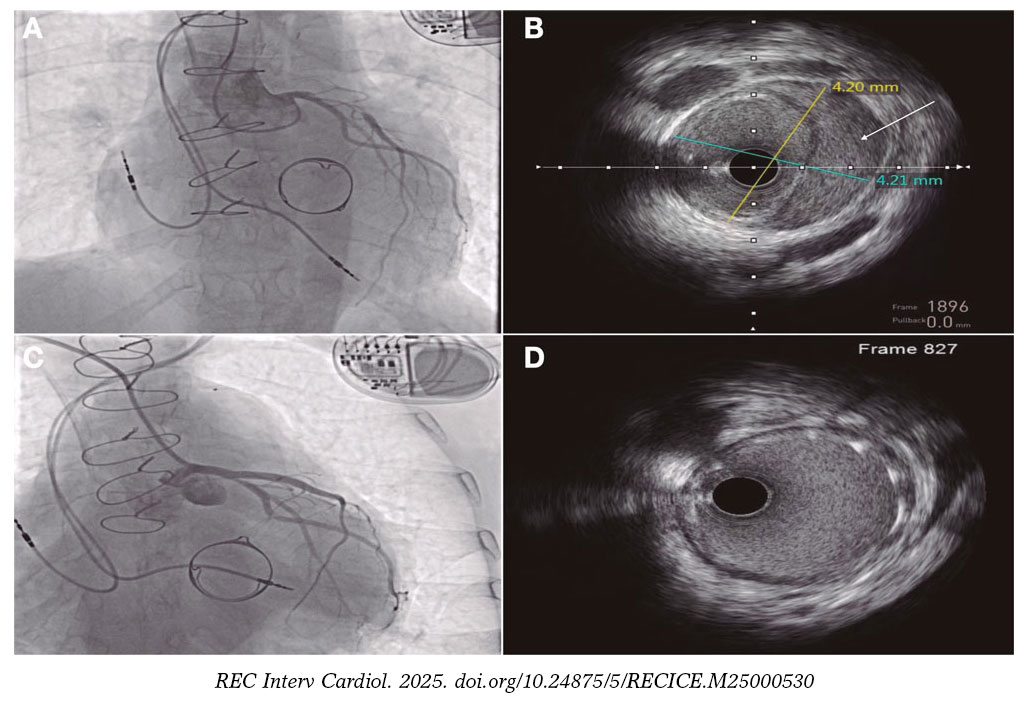
Figure 1.
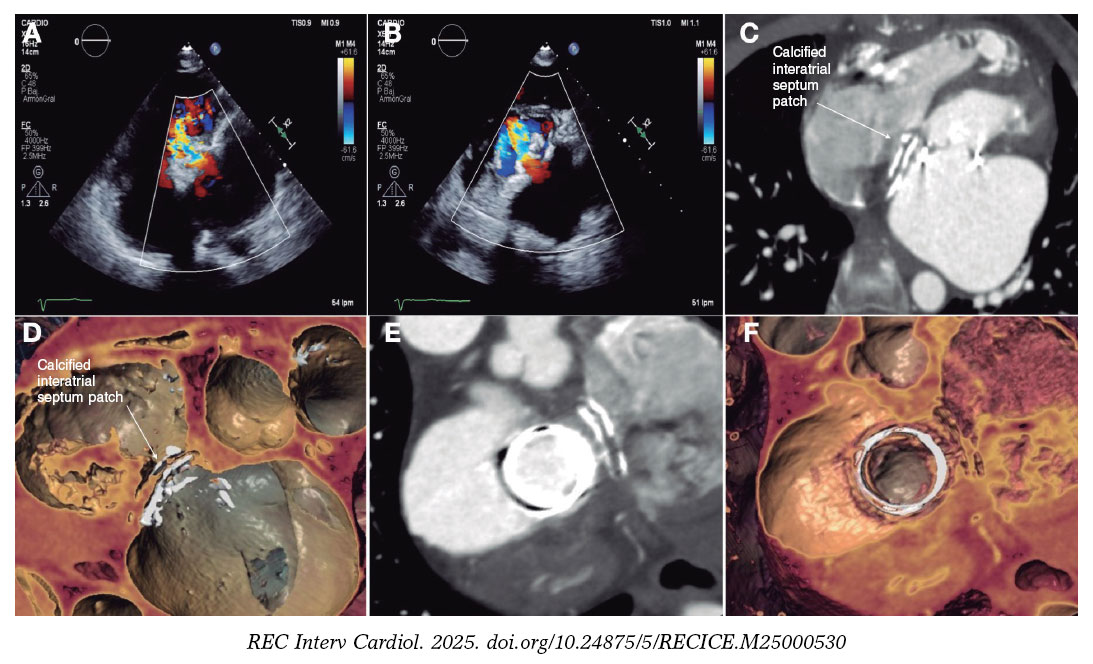
Figure 2.
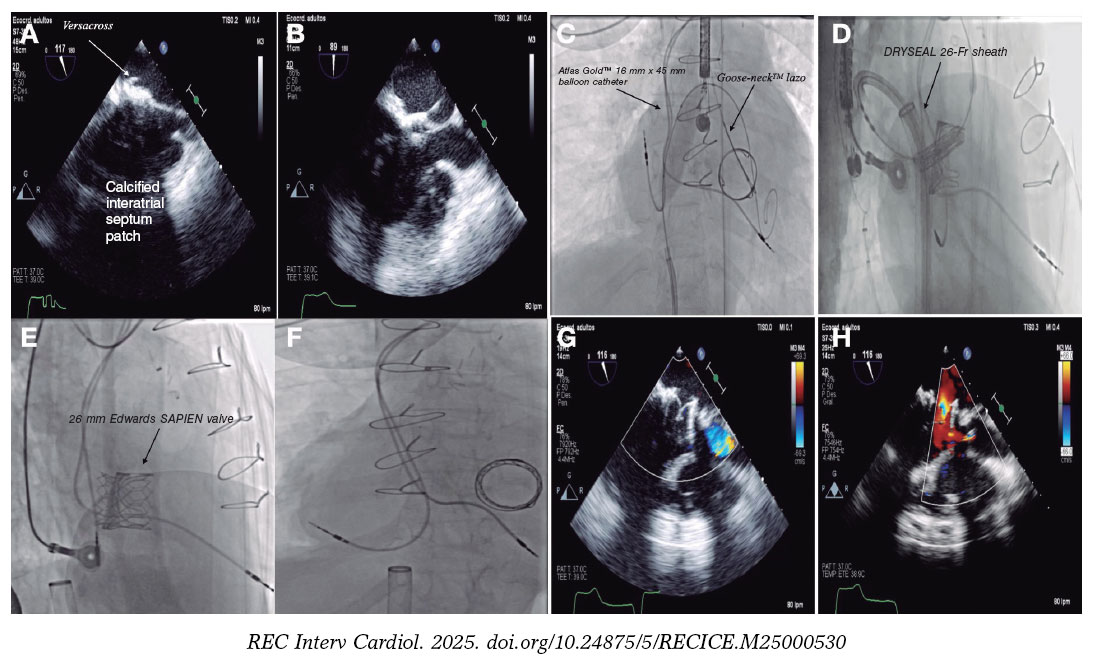
Figure 3.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
This work was accepted by our center ethics committee. Informed consent for publication of this case was obtained and has been archived. SAGER guidelines regarding potential sex/gender biases have been followed.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence was used in the preparation of this work.
AUTHORS’ CONTRIBUTIONS
All authors contributed equally to the preparation of the text.
CONFLICTS OF INTEREST
None declared.
SUPPLEMENTARY DATA
Vídeo 1. Fernández González L. DOI: 10.24875/RECICE.M25000530
Vídeo 2. Fernández González L. DOI: 10.24875/RECICE.M25000530
Vídeo 3. Fernández González L. DOI: 10.24875/RECICE.M25000530
Vídeo 4. Fernández González L. DOI: 10.24875/RECICE.M25000530
Vídeo 5. Fernández González L. DOI: 10.24875/RECICE.M25000530
Vídeo 6. Fernández González L. DOI: 10.24875/RECICE.M25000530













