tUnidad de Cardiología Infantil y Hemodinámica Infantil, Servicios de Pediatría y Cardiología, Complexo Hospitalario Universitario A Coruña, A Coruña, Spain
uSección de Hemodinámica, Servicio de Cardiología, Hospital Universitario Virgen de las Nieves, Granada, Spain
vServicio de Cardiología, Hospital General Universitario Gregorio Marañón, Madrid, Spain
wServicio de Cardiología, Hospital Universitario San Rafael, Madrid, Spain
xSección de Cardiología Pediátrica, Hospital Regional Universitario de Málaga, Málaga, Spain
RESUMEN
Introduction and objectives: The Interventional Cardiology Association of the Spanish Society of Cardiology (ACI-SEC) and the Interventional Working Group of the Spanish Society of Pediatric Cardiology (GTH-SECPCC) present their 2023 annual activity report.
Methods: Participation was open to all Spanish centers with cath labs and interventional programs for congenital heart disease. Data was collected online and analyzed by an external company, and members from the ACI-SEC and the GTH-SECPCC.
Results: A total of 19 centers participated (15 public and 4 private). Interventional data on adult congenital diseases was contributed to the Registry of Hemodynamics and Interventional Cardiology of the ACI-SEC in 2023 by another 114 hospitals and, then, added to the analysis. A total of 1127 diagnostic studies (1.2% less than 2022) and 3856 interventional cardiac catheterizations (53.7% more than 2022) were registered, 2439 of which (65%) were performed on patients older than 18 years. The most widely performed procedures were foramen ovale closure (1498 cases), atrial septal defect closure (700 cases), transcatheter closure of the patent ductus arteriosus (344 cases) and aortic coarctation (221 cases). The most significant volume increment of cases was associated with ventricular septal defect closure (181%), foramen ovale closure (87%), and aortic coarctation (75%). Interventional procedures were considered successful in 98.3% of the cases, with rates of major procedural complication and in-hospital mortality of 1% and 0.05%, respectively.
Conclusions: We present the fourth Spanish cardiac catheterization in congenital heart diseases registry with data from 2023. We observed a significant rise in interventional procedures, notably ventricular septal defect and patent foramen ovale closures. Most interventional techniques continue to demonstrate excellent safety and efficacy outcomes.
Introducción y objetivos: La Asociación de Cardiología Intervencionista de la Sociedad Española de Cardiología (ACI-SEC) y el Grupo de Trabajo de Hemodinámica de la Sociedad Española de Cardiología Pediátrica y Cardiopatías Congénitas (GTH-SECPCC) presentan su informe anual de actividad hemodinámica en cardiopatías congénitas correspondiente al año 2023.
Métodos: Se invitó a participar a los centros españoles con laboratorio de hemodinámica y actividad intervencionista en cardiopatías congénitas. La recogida de datos fue telemática y su análisis lo realizó una empresa externa junto con miembros de la ACI-SEC y el GTH-SECPCC.
Resultados: Participaron en el registro 19 centros (15 públicos y 4 privados). Se incorporaron al análisis los datos de intervencionismo en cardiopatías congénitas del adulto aportados por otros 114 hospitales al Registro de Hemodinámica y Cardiología Intervencionista de la ACI-SEC del año 2023. Se registraron 1.127 estudios diagnósticos (1,2% menos que en 2022) y 3.856 cateterismos intervencionistas (53,7% más que en 2022), de los que 2.439 (65%) se realizaron en mayores de 18 años. Las técnicas más frecuentes fueron los cierres de foramen oval (1.498 casos), de comunicación interauricular (700 casos) y de ductus arterioso (344 casos), y la coartación de aorta (221 casos). Respecto al año anterior, se incrementaron significativamente las técnicas de cierre de comunicación interventricular (181%), cierre de foramen oval (87%) y coartación de aorta (75%). La tasa de éxito en los procedimientos intervencionistas fue del 98,3%, con una tasa de complicaciones mayores del 1% y una mortalidad intrahospitalaria del 0,05%.
Conclusiones: Se presenta el informe del Registro español de intervencionismo en cardiopatías congénitas del año 2023. Se ha comunicado un aumento muy significativo de los procedimientos terapéuticos, destacando el incremento en los cierres de comunicación interventricular y de foramen oval. Todas las técnicas intervencionistas han mostrado excelentes datos de seguridad y eficacia.
Palabras clave:Cardiopatías congénitas.Cateterismo cardiaco.Cierre de comunicación interventricular.Implante percutáneo de válvula aórtica.
INTRODUCTION
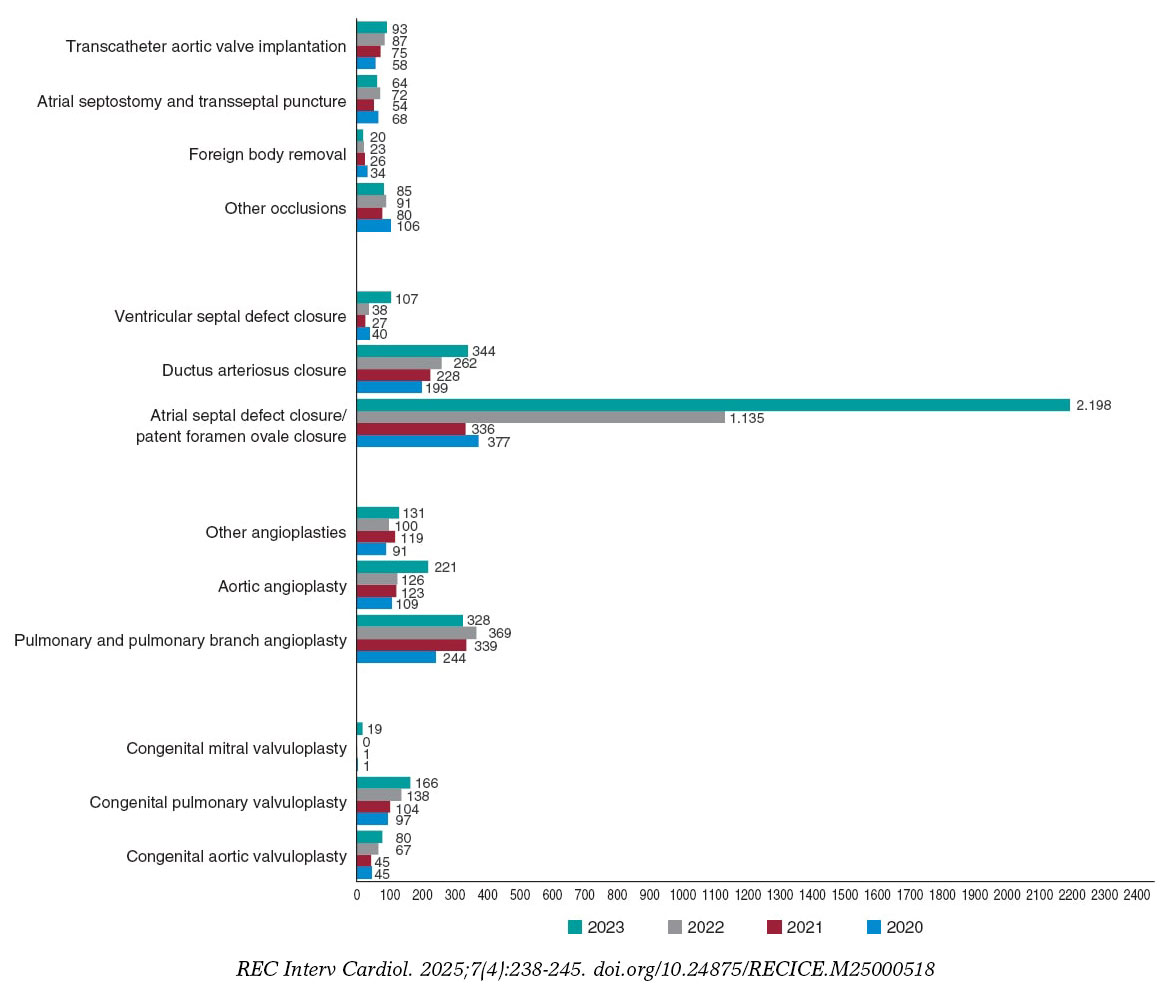
Over the past 5 years, the collaboration between the Interventional Cardiology Association of the Spanish Society of Cardiology (ACI-SEC) and the Interventional Working Group of the Spanish Society of Pediatric Cardiology (GTH-SECPCC) has led to the consolidation of the Spanish cardiac catheterization in congenital heart diseases registry, substantiated thus far by the publication of its first 3 reports on the activities conducted in 2020,1 2021,2 and 20223 (figure 1). The first 2 reports demonstrated that the number of centers participating in the registry, although highly representative of pediatric activity, did not accurately reflect the activity of adult congenital heart disease conducted in Spain.4,5,6 Therefore, the analysis of the current report presented in this article, on the activity conducted in 2023, has incorporated—same as in the previous report—the interventional activity in congenital heart disease from the Registry of Hemodynamics and Interventional Cardiology of the ACI-SEC for that same year.7 This methodology has proven to more reliably quantify hemodynamic procedures in congenital heart disease across all age groups. The findings from this edition were presented on June 14, 2024, at the ACI-SEC Congress held in Las Palmas de Gran Canaria (Canary Islands, Spain).
Figure 1. Comparison of the number of interventional procedures in 2020, 2021, 2022, and 2023.
METHODS
Data come from an annually updated, retrospective, voluntary, and non-audited registry. The inclusion of interventional data on congenital heart disease from the Registry of Hemodynamics and Interventional Cardiology of the ACI-SEC was possible due to the harmonization of questionnaires between the 2 registries conducted the previous year, which continued to undergo improvements.
All hospitals already participating in the Registry of Hemodynamics and Interventional Cardiology of the ACI-SEC, and all hospitals represented in the GTH-SECPCC, were asked to participate. Data was collected through an electronic database managed by an external company (pInvestiga España), which analyzed the registry results and compared them with those from previous years in collaboration with members of the GTH-SECPCC and the ACI-SEC board. Discrepant or particularly noteworthy data were cleaned and verified with the responsible investigator.
Due to the methodological characteristics of the study and the fact that it is only an activity registry, both the approval from the ethics committee and the processing of informed consent were deemed unnecessary.
RESULTS
Resources and infrastructure
A total of 19 hospitals participated (3 less than in 2021), of which 15 belong to the public health care system and 4 to the private sector (table 1 of the supplementary data). In addition, the analysis incorporated data on adult congenital heart disease interventions from another 114 hospitals (15 more than in 2022) included in the 2023 Registry of Hemodynamics and Interventional Cardiology of the ACI-SEC (table 2 of the supplementary data).
Table 1. Number of interventional procedures and distribution by age groups
Variable
Fetal
< 1 month
1 month to 1 year
1-18 years
> 18 years
Total
Interventional procedures
4 (0.1)
165 (4.2)
281 (7.2)
967 (25)
2439 (63.2)
3856
Congenital aortic valvuloplasty
2 (2.5)
18 (22.5)
16 (20.0)
24 (30.0)
20 (25.0)
80
Congenital pulmonary valvuloplasty
2 (1.2)
43 (25.9)
44 (26.5)
19 (11.4)
58 (34.9)
166
Congenital mitral valvuloplasty
–
0
0
1 (5.2)
18 (94.7)
19
Pulmonary angioplasty
–
13 (12.0)
8 (7.4)
63 (58.3)
24 (22.2)
108
Pulmonary branch angioplasty
–
5 (2.2)
48 (21.8)
109 (49.5)
58 (26.3)
220
Aortic coarctation
–
7 (3.1)
34 (15.3)
69 (31.2)
111 (50.2)
221
Other angioplasties
–
28 (21.3)
17 (12.9)
63 (48.0)
23 (17.5)
131
Patent foramen ovale closure
–
0
0
12 (0.8)
1486 (99.1)
1498
Atrial septal defect closure
–
0
7 (1.0)a
238 (34.0)
455 (65.0)
700
Ductus arteriosus closure
15 (4.3)b
20 (5.8)b
38 (11.1)b
208 (60.4)
63 (18.3)
344
Ventricular septal defect closure
–
0
9 (9.6)
58 (62.3)
40 (37.9)
107
Other occlusions
–
2 (2.3)
17 (20.0)
45 (52.9)
21 (24.7)
85
Foreign body removal
–
1 (5.0)
3 (15.0)
15 (75.0)
1 (5.0)
20
Atrial septostomy and transseptal puncture
0
48 (75.0)
5 (7.8)
9 (14.0)
2 (3.1)
64
Transcatheter aortic valve implantation
–
0
0
34 (36.5)c
59 (63.4)
93
Data are expressed as no. (%).
a In this case, < 1 month and 1 month to 1 year are not collected separately, so the value corresponds to < 1 year.
bFor ductus arteriosus closure, the groups are premature (fetal), < 6 months (< 1 month) and 6 months to 1 year (1 month to 1 year).
cCollected as < 18 years, so the value corresponds to < 18 years.
Table 2. Number of interventional catheterizations in patients > 18 years and distribution according to origin registry
Interventional procedures
> 18 years
Total
RICCa
RHCIb
Congenital aortic valvuloplasty
20
1 (5.0)
19 (95.0)
Congenital pulmonary valvuloplasty
58
22 (37.9)
36 (62.0)
Congenital mitral valvuloplasty
18
1 (5.5)
17 (94.5)
Pulmonary angioplasty
24
24 (100.0)
0 (0.0)
Pulmonary branch angioplasty
58
30 (51.7)
28 (48.3)
Aortic coarctation
111
29 (26.1)
82 (73.8)
Other angioplasties
23
23 (100.0)
0 (0.0)
Patent foramen ovale closure
1486
149 (10.0)
1337 (90.0)
Atrial septal defect closure
455
53 (11.6)
402 (88.4)
Ductus arteriosus closure
63
3 (4.7)
60 (95.2)
Ventricular septal defect closure
40
5 (12.5)
35 (87.5)
Other occlusions
21
21 (100.0)
0 (0.0)
Foreign body removal
1
1 (100.0)
0 (0.0)
Atrial septostomy and transseptal puncture
2
2 (100.0)
0 (0.0)
Transcatheter aortic valve implantation
59
59 (100.0)
0 (0.0)
Total
2439
423 (17.3)
2016 (82.7)
RHCI, Registry of Hemodynamics and Interventional Cardiology of the ACI-SEC; RICC, Spanish cardiac catheterization in congenital heart diseases registry of the ACI-SEC.
Data are expressed as no (%).
aData provided by the 19 centers participating to the 2023 Interventional Cardiology in Congenital Heart Diseases Registry of the ACI-SEC and the GTH-SECPCC.
bData provided by 96 centers to the 2023 Registry of Hemodynamics and Interventional Cardiology of the ACI-SEC.
A total of 38 cath labs performing interventional procedures in congenital heart disease were registered, 7 of which (18.4%) only deal with pediatric procedures; 9 are equipped with biplane systems and 8 implement rotational angiography. The median number of monthly days dedicated to congenital heart disease interventions per hospital was 7 (range, 3–18) vs 6 days in 2022. Thirteen centers (68.4%) provide 24-hour emergency interventional care, including services for pediatric patients.
Regarding medical staff, a total of 68 interventional cardiologists were dedicated to this activity, including 36 (52.9%) specialized in adult interventions and 32 (47.1%) in pediatric interventions.
Diagnostic procedures
A total of 1127 diagnostic studies were recorded, representing a 1.2% decrease compared with the previous year. The age distribution was as follows: 27 (2.4%) were performed in infants younger than 1 month, 95 (8.4%) in children aged 1 month to 1 year, 548 (48.6%) in patients aged 1–18 years, and 457 (40.6%) in patients older than 18 years.
A total of 70 procedures (6.5%) were categorized as emergencies. Regarding morbidity, there were 5 cases (0.4%) of severe complications: 2 vascular events, 1 arrhythmia with severe hemodynamic instability and cardiorespiratory arrest, 1 anaphylactic reaction, and 1 neurological event. There were no procedural deaths.
Interventional procedures
Reported activity increased by 53.7% compared with the previous year for a total of 3856 therapeutic catheterizations registered and categorized into 15 different groups. Their case distribution and age breakdown are shown in table 1. Of the 2439 procedures (63.2%) performed in patients older than 18 years, 2016 (82.7%) came from data added from the Registry of Hemodynamics and Interventional Cardiology of the ACI-SEC (table 2).
A total of 195 cardiac catheterizations were categorized as emergencies (10.9% of all procedures for which this information was available). The volume of interventional procedures per center was as follows: 7 hospitals (36.8%) recorded > 150 cardiac catheterizations; 3 hospitals (15.7%) between 75 and 150 procedures, and 9 (47.3%) < 75 procedures. The overall effectiveness reported for the different interventional techniques was 97.9%, with most procedures showing success rates exceeding 95% (table 3).
Table 3. Summary of reported efficacy of interventional procedures
Interventional procedures
n
n with success or ineffectiveness data
Success
Ineffective
Congenital aortic valvuloplasty
80
65 (81.2)
59 (90.7)
6 (9.2)
Congenital pulmonary valvuloplasty
166
133 (80.1)
129 (96.9)
2 (1.5)
Congenital mitral valvuloplasty
19
19 (100)
18 (94.7)
1 (5.3)
Pulmonary angioplasty
108
89 (82.4)
81 (91.0)
8 (8.9)
Pulmonary branch angioplasty
220
193 (87.7)
181 (93.7)
12 (6.2)
Aortic coarctation
221
139 (62.8)
131 (94.2)
8 (5.7)
Other angioplasties
131
131 (100)
128 (96.9)
4 (3.0)
Patent foramen ovale closure
700
547 (78.4)
539 (98.5)
8 (1.4)
Atrial septal defect closure
1498
1188 (79.3)
1182 (99.4)
6 (0.5)
Ductus arteriosus closure
344
251 (72.9)
249 (99.2)
3 (1.1)
Ventricular septal defect closure
107
81 (75.7)
78 (96.2)
3 (3.7)
Other occlusions
85
85 (100)
85 (100.0)
0 (0.0)
Foreign body removal
20
20 (100)
20 (100.0)
0 (0.0)
Atrial septostomy and transseptal puncture
64
64 (100)
63 (98.4)
1 (1.5)
Transcatheter aortic valve implantation
93
92 (98.9)
91 (98.9)
1 (1.1)
Total
3856
3084 (79.9)
3034 (98.3)
63 (2.0)
Data are expressed as no (%).
Percentage of success or ineffectiveness based on the number of procedures with available data.
Transcatheter valvuloplasties
A total of 80 aortic valvuloplasties were reported for congenital aortic stenosis, reflecting a 19.4% increase from 2022. Two of these procedures were performed in fetuses. Sixty cases (75%) involved patients younger than 18 years, and in 77% of procedures, the dilation was performed on native, previously untreated valves.
A total of 166 pulmonary valvuloplasties were performed, marking a 20% increase from 2022. This included 2 fetal catheterizations. Technical details were available for 143 cases, of which 115 (80.4%) involved native valves—15 of them (10%) imperforate. In 8 cases (5.5%), the procedure was combined with ductal stent implantation.
Mitral valvuloplasty was reported in 19 cases, only 1 of which was performed in a patient younger than 18 years.
Transcatheter angioplasties
A total of 108 right ventricular outflow tract dilations were recorded, which is a 20% decrease compared with 2022. Technical and anatomical data were reported for 89 procedures (82.4%); 55% involved angioplasty of native tracts, and the remaining 45%, angioplasty of surgical conduits. Conventional balloon dilation was performed in 52% of cases, and stent implantation in 48%.
Pulmonary branch angioplasty accounted for 196 procedures (a 16% decrease compared with 2022). In 95% of cases, proximal branches were dilated, while peripheral arteries (lobar-segmental) accounted for the remaining 5%. Stent implantation was used in 52% of catheterizations, conventional balloon dilation in 46%, and cutting balloon dilation in 2%.
A total of 221 aortic coarctation procedures were reported (a 75% increase compared with 2022). Anatomical data were available for 139 procedures (62.8%), most of which (64%) were reinterventions. The site of dilation was the aortic arch/isthmus in all but 5 cases (4 abdominal aorta dilations and 1 ascending aorta dilation). The technique used included conventional balloon dilation in 28%, uncovered stent implantation in 26%, covered stent implantation in 32%, and repeat dilation of a previously implanted stent in 12%.
Finally, a total of 131 catheterizations were reported under the “other angioplasties” category, representing a 31% increase compared with the previous year, among them, 29 ductus arteriosus dilations and 7 surgical fistula dilations. Stent implantation was associated with 72% of these procedures.
Shunt closures and other occlusion procedures
A total of 1498 patent foramen ovale closures were reported (a 112% increase compared with 2022), of which 1337 (90%) came from the Registry of Hemodynamics and Interventional Cardiology of the ACI-SEC (table 2). Adults accounted for 99.1% of all patients undergoing this procedure.
Atrial septal defect (ASD) closures saw a substantial increase, reaching 700 procedures. This represents a 62% rise compared with 2022. Among the defects classified, 67% were complex, with the rest being simple. Guidance data were provided in 351 (50.1%) cases: transesophageal echocardiography was used in 82% procedures, angiographic balloon sizing in 15.9%, and intracardiac echocardiography in 1.9%.
A total of 344 ductus arteriosus closures were performed. Patients aged 1–18 years accounted for 65.6% of these procedures, while premature infants represented 4.7%, with 15 cases reported (compared with 9.2% in 2022). Anterograde venous access was used in 63% of closures. Occluder devices were used in 81% of cases and controlled-release coils in the remaining ones.
There were 107 ventricular septal defect (VSD) closures, a 181% increase compared with the previous year. Anatomical substrate data were provided in 73 cases (68.2%): 54 (73.9%) perimembranous, 14 (19.1%) muscular, and 5 (6.8%) postoperative. Occluder devices were used in 93% of cases, and coils in the remaining ones. Two devices were implanted via hybrid approach and the rest (97.2%) via transcatheter approach.
A total of 85 cardiac catheterizations were included under the “other occlusion procedures” category. Closure of systemic-to-pulmonary collaterals accounted for 70% of these cases, and venous collateral occlusion for 14%. The most widely used materials were occluder devices (46.3%), followed by coils (34.1%) and particles either alone or in combination with other materials (18.2%).
Atrial septostomy
A total of 64 procedures were reported (an 11.1% decrease compared with the previous year). Regarding imaging support, echocardiography was used in 16.5% of cases, fluoroscopy in 26.1%, and a combination of both imaging modalities in 57.4%. Fifty-two (81%) of these were balloon atrial septostomies (Rashkind). Additionally, 5 procedures were performed with radiofrequency septal perforation, 9 with needle perforation, and 8 with septal stent implantation.
Transcatheter valve implantation
A total of 93 procedures were reported, of which 51 (54.8%) were performed in adults. All procedures were performed via transcatheter approach, except for 1 case which required hybrid implantation. The pulmonary position was the most widely used (95.6%), with 4 valves being implanted in the tricuspid position. The anatomical substrates for pulmonary valve implantation were the native right ventricular outflow tract in 54 cases (58%), surgical conduits in 23 cases (24.7%), and valve-in-valve procedures in 16 cases (17.2%).
Complications
Morbidity and mortality data were available for 3738 interventional procedures. A total of 40 serious adverse events were reported (table 4), including 2 deaths, resulting in a major complication rate of 1.07% and a mortality rate of 0.05%. The categories with the highest morbidity were mitral and aortic valvuloplasties (5.2% and 4.8%, respectively), atrial septostomy (4.6%), and VSD closure (3.4%). The most frequent complications were device embolizations, reported in 12 cases (30% of all complications): 8 in ASD and foramen ovale closures, 2 in ductus arteriosus closures, 1 stent in vascular angioplasty, and 1 in pulmonary valve implantation. In 3 ASD closures and 1 valve implantation, surgical retrieval of the embolized prosthesis was required; the rest were resolved via transcatheter approach. A total of 8 serious arrhythmia events occurred, including 1 cardiac arrest which required extracorporeal membrane oxygenation. Furthermore, there were 7 cases of vascular complications.
Table 4. Distribution of major complications and reported deaths across different interventional procedures
Variable
n
Major complications
Deaths
Congenital aortic valvuloplasty
80a (62)
3 (4.8) – 1 severe aortic regurgitation – 1 CPR-ECMO – 1 death
3 (2.1) – 1 severe tricuspid regurgitation – 1 embolization requiring surgery – 1 death
1 (1,0)
Total
3856 (3738)
40 (1.07)
2 (0.05)
CPR-ECMO, cardiopulmonary arrest with need for extracorporeal membrane oxygenator; NS, not specified.
aData are expressed as no (%).
bPercentages calculated from 62 reported cases.
cPercentages calculated from 133 reported cases.
dPercentages calculated from 89 reported cases.
ePercentages calculated from 193 reported cases.
fPercentages calculated from 86 reported cases.
DISCUSSION
The most significant finding of this report is the considerable increase in recorded interventional procedures (3856), representing a 53.7% rise compared with 2022. The most notable increases were observed in VSD closures (181%), patent foramen ovale closures (112%), and interventions for aortic coarctation (75%). Another remarkable observation is that 62% (55% in 2022 and 31% in 2021) of all reported procedures were performed in patients older than 18 years, confirming the growing volume of procedures in this age group. This trend likely reflects the broader expansion of structural heart procedures in Spain.7 Of note, as in the previous report, data from 114 hospitals (99 in 2022) reporting adult congenital heart disease procedures to the 2023 Registry of Hemodynamics and Interventional Cardiology of the ACI-SEC were included in the analysis. Comparisons with prior reports must be interpreted considering this methodology.
Nonetheless, most interventional categories recorded (10 out of 15) still concentrate the largest number of patients in the pediatric population (table 1). Additionally, fetal intervention activity remains minimal in Spain, with only 4 cases reported (2 aortic and 2 pulmonary valvuloplasties), despite evidence supporting their value and efficacy across multiple prenatal scenarios.8
Reported success rates for the different interventional techniques yield an overall success rate of 98.3% (97.6% in 2022) and a mortality rate of 0.05% (0.2% in 2021). Although the voluntary and unaudited design of the registry could limit the strength of these findings, they remain the best reported to date and are consistent with most international studies.9,10 Similarly, the 1% rate of serious adverse events is the lowest recorded so far (1.4% in 2022). Device embolization remains the most frequent complication, accounting for 30% of all cases by arrhythmias (20%) and vascular complications (17.5%) in 2023. Recent national studies have validated the usefulness of specific methodologies to assess expected risk of complications across different techniques and various clinical scenarios.11 Their application could enhance the quality of information produced by these results and is expected to be incorporated in coming years.
Regarding valvuloplasties, the most notable development was the reporting of 19 mitral valve dilations—a category that had been nearly absent from previous reports. This technique, in use for more than 40 years in adult interventional cardiology, has significantly evolved with the integration of 3D imaging modalities for patient selection and procedural guidance.12 Aortic and pulmonary valvuloplasties continue to rise (19% and 20%, respectively), mostly in the pediatric setting, reaffirming their role as first-line options for congenital valve stenosis in our environment. Of particular note within pulmonary valvuloplasties is the treatment of 15 cases of imperforate pulmonary valves. A transjugular approach might simplify such procedures, as recently demonstrated by a national group.13
In the angioplasty category, the most striking observation is the rise in reported cases of aortic coarctation (75% increase compared with 2022); 50.2% of the 221 cases were reported in patients older than 18 years. Dilations of the aortic arch and isthmus continue to account for most cases, with covered stent implantation increasingly established as the preferred approach in this anatomical setting. The use of this technique in pediatric patients is also on the rise, driven by the availability of covered stents with lower delivery profiles, now applied to other congenital anatomical contexts too.14
Interatrial septal defect closures (patent foramen ovale and ASD) are the highest-volume procedures in the registry, accounting for 57% of all cardiac catheterizations (38%, patent foramen ovale closure; 19%, ASD closure). Inclusion of patent foramen ovale closure in this registry, and its categorization as a congenital heart disease, is essential to maintain consistent criteria and comparability with previous reports, especially given its massive growth in adult interventional procedures.7 While double-disc devices remain the most widely used with the largest cumulative experience, the emergence of suture-based devices has expanded transcatheter treatment options, offering an attractive alternative in selected patients.15 Furthermore, ASD closure experienced significant growth this year (62% more compared with 2022). Up to 33% of cases with anatomical data were categorized as complex, which along with an excellent safety (1.5% complication rate) and efficacy (97.5%) profile confirm the maturity of this technique in Spain.
Ductus arteriosus closure remains a predominantly pediatric technique (87% of cases in patients younger than 18 years). However, a significant decline was reported in premature neonates, who represented only 4.7% of cases this year (9.4% in 2022). This slowdown in adopting transcatheter options for neonates contrasts with continued international studies validating it over surgery.16
VSD closure showed the greatest growth among procedures (181%), with notable progress across all age groups. Safety and efficacy results continue to improve, with a rate of major complications reduced to 3.4% (compared with 18% in 2021 and 5.2% in 2022) and a success rate of 96.2% (compared with 77.3% in 2021 and 96.7% in 2022). Occluder devices were used in 93% of cases. These results confirm a paradigm shift for the technique in Spain, driven by the introduction of new closure devices and technical modifications that facilitate the approach.17,18
Transcatheter aortic valve implantation increased slightly by 6.8%. Notably, 63.4% of these procedures were performed in patients older than 18 years, highlighting the growth of this technique in adult congenital heart diseases. As in previous reports, most were pulmonary valve implantations, with only 4 implantations being performed in the tricuspid position (2 in 2022). A major innovation in Spain is the availability of new self-expandable valve designs that broaden anatomical applicability—especially relevant for the 58% of patients with a native pulmonary tract.19,20
Limitations
The design of the registry (retrospective, voluntary, unaudited) may weaken the robustness of its findings. Expanding the information collected on certain key techniques would improve report quality and should be considered in future editions.
CONCLUSIONS
The significant increase in the volume of interventional procedures recorded compared with previous years, along with the rise in the number of participant centers, is the primary finding of this report. This growth is accompanied by continued improvements in the safety and efficacy data of most techniques. The most prominent increases were observed in VSD closures, interatrial shunt closures, and aortic coarctation procedures. The data obtained offer a realistic representation of interventional activity in congenital heart disease across all age groups in Spain.
An increase in participant centers and continued registry updates will enhance the quality and reliability of the information generated, reinforcing the relevance and usefulness of the registry.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
Due to the methodological characteristics of the study and its design as a procedural activity registry, approval from the ethics committee or processing of informed consent were both deemed unnecessary. The nature of the work precludes the consideration of sex and gender variables, and therefore, SAGER guidelines were not followed.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence tools were used.
AUTHORS’ CONTRIBUTIONS
All authors made substantial contributions to data collection, and to the critical review and approval of the final version of the manuscript. F. Ballesteros Tejerizo and F. Coserría Sánchez drafted the manuscript.
CONFLICTS OF INTEREST
S. Ojeda Pineda is an Associate Editor of REC: Interventional Cardiology, and R. Sanz-Ruiz is a Section Editor of REC: Interventional Cardiology. In both cases, the journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. The remaining authors declared no conflicts of interest whatsoever.
ACKNOWLEDGMENTS
To all the members of the Interventional Working Group of the SECPCC and the ACI-SEC who collaborated on this project from the beginning, and especially to the successive boards of directors of the ACI-SEC, which have consistently provided decisive support for the creation, growth, and consolidation of the Spanish cardiac catheterization in congenital heart diseases registry.
SUPPLEMENTARY DATA
WHAT IS KNOWN ABOUT THIS TOPIC?
The Spanish cardiac catheterization in congenital heart diseases registry provides a nationwide annual report on the activity conducted in this field of cardiology, covering procedures performed across all age groups.
The existence of this report ensures insight into the adoption and evolution of interventional techniques, as well as their outcomes.
The information generated is of great value to professionals involved in this field of cardiology, as well as to patients and their families.
WHAT DOES THIS STUDY ADD?
This report is the consolidation of the registry goal to provide realistic data on interventional activity in patients of all ages.
A very significant increase in interventional procedures was reported in 2023, with the most notable growth observed in ventricular septal defect closure, patent foramen ovale closure, and aortic coarctation.
Foramen ovale, atrial septal defect, and ductus arteriosus closures remain the procedures with the highest volumes.
Device embolizations and arrhythmias led the list of procedural adverse events this year.
REFERENCES
1. Ballesteros Tejerizo F, Coserría Sánchez F, Romaguera R, et al. Spanish cardiac catheterization in congenital heart diseases registry. First Official Report from ACI-SEC and GTH-SECPCC (2020). REC Interv Cardiol. 2022;4:173-180.
2. Ballesteros Tejerizo F, Coserría Sánchez F, Freixa X, et al. Spanish cardiac catheterization in congenital heart diseases registry. Second official report from the ACI-SEC and the GTH-SECPCC (2021). REC Interv Cardiol. 2023;5:185-192.
3. Ballesteros Tejerizo F, Coserría Sánchez F, Jurado-Román A, et al. Spanish cardiac catheterization in congenital heart diseases registry. Third official report from the ACI-SEC and the GTH-SECPCC (2022). REC Interv Cardiol. 2024;6:182-190.
4. Romaguera R, Ojeda S, Cruz-González I, Moreno R. Spanish Cardiac Catheterization and Coronary Intervention Registry. 30th Official Report of the Interventional Cardiology Association of the Spanish Society of Cardiology (1990-2020) in the year of the COVID-19 pandemic. Rev Esp Cardiol.2021;74:1096-1106.
5. Freixa X, Jurado-Roman A, Cid B, et al. Spanish cardiac catheterization and coronary intervention registry. 31st official report of the Interventional Cardiology Association of the Spanish Society of Cardiology (1990-2021). Rev Esp Cardiol. 2022;75:1040-1049.
6. Jurado-Román A, Freixa X, Cid B, Cruz-González I. Spanish cardiac catheterization and coronary intervention registry. 32nd official report of the Interventional Cardiology Association of the Spanish Society of Cardiology (1990-2022). Rev Esp Cardiol.2023;76:1021-1031.
7. Bastante T, Arzamendi D, Martin-Moreiras J, et al. Spanish cardiac catheterization and coronary intervention registry. 33rd official report of the Interventional Cardiology Association of the Spanish Society of Cardiology (1990-2023). Rev Esp Cardiol. 2024;77:936-946.
8. Yilmaz Furtun B, Morris SA. Catheter-Based Fetal Cardiac Interventions. J Cardiovasc Dev Dis. 2024;11:167.
9. Kevin D, Wei Du, Fleming GA, et al. Validation and refinement of the catheterization RISK score for pediatrics (CRISP score):An analysis from the congenital cardiac interventional study consortium. Catheter Cardiovasc Interv.2019;93:97-104.
10. Quinn BP, Ye M, Gauvreau K, et al. Procedural Risk in Congenital Cardiac Catheterization (PREDIC3T). J Am Heart Assoc.2022;11:022832.
11. Éden Santos P, Ballesteros F, Rodríguez A, Zunzunegui JL. Use of a pediatric risk score for cardiac catheterization in a Spanish population with congenital heart disease. REC Interv Cardiol. 2024;6:20-24.
12. Turi ZG. The 40th Anniversary of Percutaneous Balloon Valvuloplasty for Mitral Stenosis:Current Status. Struct Heart. 2022;6:100087.
13. Figueras Coll M, Fidalgo García A, MartíAguasca G, Betrián Blasco P. Neonatal transcatheter pulmonary valve perforation. Evolution from transfemoral to transjugular approach. REC Interv Cardiol. 2023;5:129-135.
14. Rebonato M, Pilati M, Milani SM, et al. BeGraft Aortic Stents:A European Multi-Centre Experience Reporting Acute Safety and Efficacy Outcomes for the Treatment of Vessel Stenosis in Congenital Heart Diseases. J Cardiovasc Dev Dis.2024;11:192.
16. Arriaga-Redondo M, Rodríguez-Sánchez de la Blanca A, Zunzunegui JL, et al. Impact of catheterized ductal closure on renal and cerebral oximetry in premature neonates. Eur J Pediatr. 2024;183:2753-2761.
17. Álvarez-Fuente M, Carrasco JI, Insa B, et al. Percutaneous closure of ventricular septal defect with the KONAR-MF device. REC Interv Cardiol.2022;4:181-185.
18. Rasines Rodríguez A, Aristoy Zabaleta MM, Abelleira Pardeiro, et al. Retrograde closure of perimembranous ventricular septal defects. A paradigm shift. REC Interv Cardiol. 2023;5:73-75.
19. Álvarez-Fuente M, Toledano M, Hernández I, et al. Initial experience with the new percutaneous pulmonary self-expandable Venus P-valve. REC Interv Cardiol. 2023;5:263-269.
20. Salas-Mera D, Abelleira Pardeiro C, Balbacid Domingo E, et al. The PULSTA valve in native right ventricular outflow tract:initial experience in 3 Spanish hospitals. REC Interv Cardiol. 2024;6:89-96.
aServicio de Cardiología, Hospital Universitario de La Princesa, Instituto de Investigación Sanitaria de La Princesa (IIS-IP), Universidad Autónoma de Madrid, Spain
bCentro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain