

Article
Ischemic heart disease and acute cardiac care
REC Interv Cardiol. 2019;1:21-25
Access to side branches with a sharply angulated origin: usefulness of a specific wire for chronic occlusions
Acceso a ramas laterales con origen muy angulado: utilidad de una guía específica de oclusión crónica
Servicio de Cardiología, Hospital de Cabueñes, Gijón, Asturias, España
ABSTRACT
Introduction and objectives: ST-segment elevation myocardial infarction (STEMI) requires early coronary reperfusion to reduce mortality and improve prognosis. In rural areas, timely access to reperfusion therapies, including fibrinolysis or percutaneous coronary intervention (PCI) is frequently constrained by logistical and health care system-related factors.
This study aimed to identify factors associated with delays in reperfusion and those associated with mortality in patients with STEMI code activation in a mountainous European region.
Methods: This is an observational, retrospective, and quantitative study in Alt Pirineu-Aran region (Catalonia, Spain) from 2015 through 2020. Sociodemographic and geographic factors, clinical status, resource management and the treatment provided were analyzed using data from the STEMI code registry and the Catalan emergency medical system.
Results: During the study period, a total of 221 patients with STEMI code were treated in the Alt Pirineu-Aran region. Patients ranged in age from 27 to 96 years, with a mean age of 64.7 years; 72.4% were men. Of these, 47 received fibrinolytic therapy and 173 were transferred to a PCI-capable center, of whom 162 underwent PCI; in 11 cases the code was deactivated. Most patients transferred for PCI experienced delays of > 120 minutes from the diagnostic electrocardiogram. Helicopter transport improved treatment times, with the greatest benefit observed in primary transfers. The 15-day mortality rate was 8.1%.
Conclusions: Most fibrinolysis treatments and PCI were not performed within the times recommended by the European clinical practice guidelines. The study highlights the underutilization of fibrinolysis.
Keywords: ST-segment elevation myocardial infarction. Rural areas. Fibrinolysis. Percutaneous coronary intervention. Mountainous regions. Prehospital care.
RESUMEN
Introducción y objetivos: El infarto agudo de miocardio (IAM) con elevación del segmento ST requiere una reperfusión coronaria precoz para reducir la mortalidad y mejorar el pronóstico. En las zonas rurales, los tiempos de acceso a los tratamientos de reperfusión (fibrinolisis o intervención coronaria percutánea primaria [ICPp]) se ven comprometidos por aspectos logísticos y asistenciales. El objetivo de este estudio es determinar los factores asociados a los retrasos en la reperfusión y los asociados a la mortalidad en pacientes con código IAM en una región montañosa europea.
Métodos: Se realizó un estudio observacional, retrospectivo y cuantitativo en la región del Alt Pirineu-Aran, en Cataluña (España), entre 2015 y 2020. Se analizaron los factores sociodemográficos y geográficos, el estado clínico de los pacientes, la gestión de los recursos y el tratamiento realizado, utilizando los datos del registro del código IAM y del Sistema d’Emergències Mèdiques.
Resultados: Durante el periodo de estudio, 221 pacientes con código IAM fueron atendidos en el Alt Pirineu-Aran. Los pacientes tenían entre 27 y 96 años, con una media de 64,7 años, y el 72,4% eran varones. De ellos, 47 pacientes recibieron fibrinolisis como tratamiento de reperfusión y 173 fueron trasladados a un hospital con unidad de hemodinámica, donde 162 recibieron ICPp; en 11 casos se desactivó el código. La mayoría de los pacientes trasladados para ICPp experimentaron un retraso superior a 120 minutos desde el electrocardiograma diagnóstico. El uso de helicópteros mejoró los tiempos de tratamiento, especialmente en los traslados primarios. La tasa de mortalidad a los 15 días fue del 8,1%.
Conclusiones: La mayoría de las fibrinolisis y de las ICPp no se realizaron dentro de los tiempos recomendados según las guías europeas. Se evidencia una marcada infrautilización de la fibrinolisis.
Palabras clave: Infarto agudo de miocardio con elevación del segmento ST. Zonas rurales. Fibrinolisis. Intervención coronaria percutánea. Zonas montañosas. Atención prehospitalaria.
Abbreviations
AMI: acute myocardial infarction. ECG: electrocardiogram. EMS: Emergency Medical Services of Catalonia. PCI-capable center: percutaneous coronary intervention capable center. pPCI: primary percutaneous coronary intervention. STEMI: ST-segment elevation acute myocardial infarction.
INTRODUCTION
Acute myocardial infarction (AMI) is a medical emergency that requires a rapid response to minimize cardiac damage and improve patient survival. Initial recognition and early treatment based on the optimal reperfusion strategy are key to survival; however, implementing this protocol in rural and mountainous regions is a major challenge.1-4
Primary percutaneous coronary intervention (pPCI) is recommended in all cases provided it can be performed within 120 minutes (ideally in less than 90 minutes).4 If not contraindicated, fibrinolysis is the treatment of choice when this time frame cannot be guaranteed. Contraindications to fibrinolytic therapy may be classified as absolute or relative and should be evaluated on an individual basis. When fibrinolysis is contraindicated, primary angioplasty should be prioritized whenever feasible.1,4 The STEMI code in Catalonia was implemented as a regional health care network in June 2009 designed to organize the management of patients with suspected ST-segment elevation myocardial infarction (STEMI).5,6
Several authors have linked delays in reperfusion treatment to the type of infarction, the timing of symptom onset, and complications.7-9 Other studies suggest that a distance > 50 km to a PCI- capable center is associated with higher mortality rates vs early fibrinolysis.10,11 Other experiences, such as sharing patient data during prehospital care, including electrocardiograms (ECG) and the use of nighttime helicopter transfer to the PCI-capable center have been associated with shorter diagnosis-to-treatment times; however, a reduction in mortality has not been demonstrated.12 However, few studies have analyzed the factors causing delays in mountainous and hard-to-access geographic areas.
The main aim of this study was to determine the factors associated with delays in reperfusion treatment and those associated with mortality in patients treated under the STEMI code in a European mountainous area.
METHODS
Study design
We conducted an observational, retrospective, and quantitative study that included all STEMI code activations in the Alt Pirineu-Aran territory (Catalonia, Spain) from January 2015 through December 2020. The main sources of information were the STEMI code registry of the Department of Health of the Government of Catalonia5,6 and the database of the medical Emergency Medical Services (EMS) of Catalonia, which were cross-referenced to obtain a comprehensive overview. Because the data were derived from preexisting registries and analyzed anonymously, informed consent was deemed unnecessary. The study was approved by the Instituto Universitario de Investigación en Atención Primaria (IDIAP) Jordi Gol Ethics Committee, code CEIm 22/238-P. The SAGER guidelines were followed regarding potential sex and gender bias.
Study setting
Alt Pirineu-Aran is a mountainous region comprising 6 counties and represents 18% of Catalonia’s territory, yet it is home to less than 1% of its population. Population density is extremely low (12.6 inhabitants per km²), and most towns are located between 500 and 800 meters above sea level, far from a specialized hospital center.
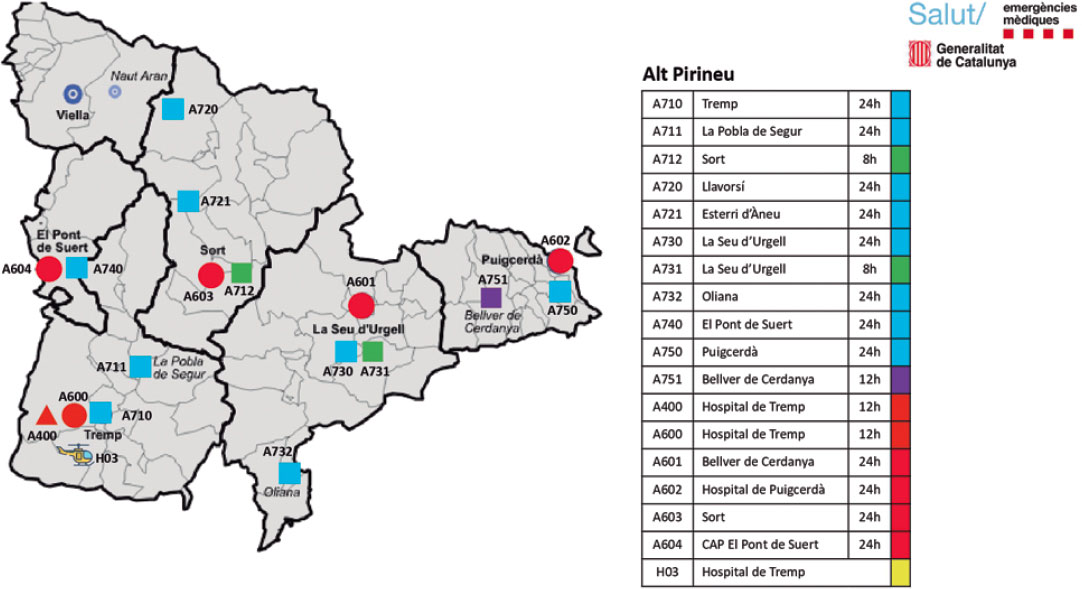
This regional health care system faces several challenges. Prehospital care is provided by the EMS, a public service that operates 24 hours per day and provides coverage throughout the entire territory. Each county is served by 1 advanced life support unit, and the region has access to 1 medicalized helicopter, 1 of the 4 operating in Catalonia. Alt Pirineu–Aran includes 4 county hospitals, all of which are non–PCI-capable centers (figure 1).
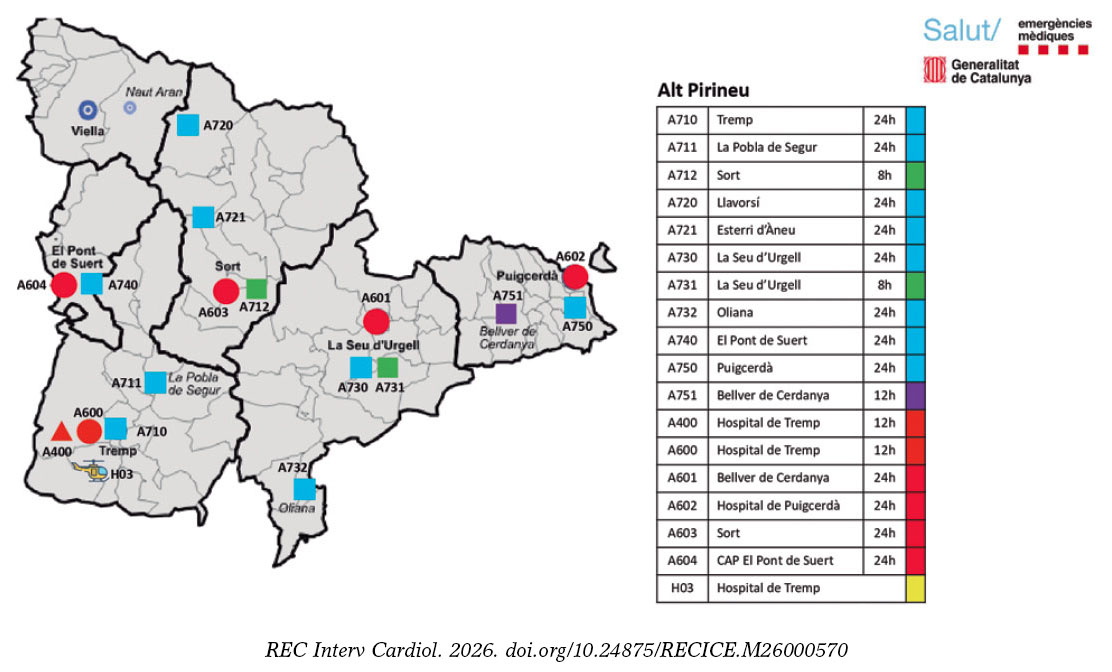
Figure 1. Alt Pirineu-Aran Health Region. H03: Tremp medicalized helicopter. H: county hospitals. Unit call signs are identified with A for Alt Pirineu; 1st number indicates the type of unit (7, basic life support; 4, advanced life support + nurse; and 6, advanced life support + physician); 2nd and 3rd numbers indicate the location of the units on the map.
Hospital Universitario Arnay de Vilanova (Lleida, Spain) serves as the reference center for pPCI for Alt Pirineu-Aran, with the exception of the Cerdanya basic health area, where STEMI code patients are transferred to centers in the Barcelona metropolitan area (table S1).
Definitions and inclusion criteria
The definitions of “delay” used in the study were more than 10 minutes for fibrinolysis administration and more than 120 minutes for pPCI, measured from the time of ECG acquisition. These criteria were established on the basis of former studies and are consistent with current European clinical practice guideline recommendations.1-4
According to EMS protocols, a 90-minute transfer threshold—from ECG acquisition to arrival at the receiving hospital—is used to allow adequate time to perform pPCI and ensure compliance with the 120-minute target. To determine whether patients had a transfer time of less than 90 minutes to a PCI-capable center, a geographic analysis based on distance and estimate travel-time maps was performed.
Patients were included if the STEMI code was activated in Alt Pirineu–Aran and they were attended by EMS during the study period, as well as those who died after prior activation of the STEMI code.
Incomplete cases or those with coding errors were excluded, as were patients transferred to Toulouse (France) from Vall d’Aran.
Study variables
The variables analyzed included demographic, clinical, and logistical data. The primary time intervals assessed were symptom onset to first medical contact, time from first medical contact to ECG, and ECG to initiation of reperfusion treatment. The type of reperfusion strategy (fibrinolysis or pPCI) was recorded as well. Other relevant variables included the location of STEMI code activation, distance to the PCI-capable center, mode of transport to the PCI-capable center (ambulance or helicopter), and type of transfer (primary: direct care and transfer by a medicalized EMS ambulance; secondary: interhospital transfer; or delayed primary: initial assessment by a primary care physician or nurse-staffed ambulance followed by transfer to a medicalized ambulance or medical helicopter). Acute-phase complications and all-cause mortality at first medical contact, and at 24 and 48 hours, and at 15 days were also recorded.
Statistical analysis
The descriptive statistical measures used were absolute and relative frequencies for qualitative variables; mean and standard deviation for quantitative variables with normal distribution; and median and interquartile range for the remaining non-normally distributed quantitative variables, according to the Shapiro-Wilk test.
We analyzed a total of 4 binary outcome variables: use of fibrinolysis as the initial treatment, delays in fibrinolysis (> 10 minutes from ECG acquisition), delays in pPCI (> 120 minutes from ECG acquisition), and mortality. Furthermore, we evaluated associations between each outcome variable and patient- and care-related characteristics using the chi-square test for qualitative variables (or Fisher’s exact test when expected frequencies were < 5), the Mann-Whitney U test for non-normally distributed quantitative variables, and the Student t test otherwise. In addition, we analyzed the importance of variables for treatment delay and mortality using the Boruta algorithm for variable selection. Only variables not rejected by this algorithm were selected for subsequent multivariable analyses to reduce the risk of overfitting. A conditional inference classification tree was constructing using a Monte Carlo test with a minimum terminal node size of 3.
All statistical analyses were performed using R statistical software (R Foundation for Statistical Computing, Austria). P values < .05 were considered statistically significant.
RESULTS
During the study period, a total of 24 125 STEMI codes were activated across Catalonia. The study analyzed 225 cases occurring in Alt Pirineu-Aran, representing less than 1% of the total. Four patients were excluded for not meeting STEMI code criteria (1 pulmonary thromboembolism, 2 coding errors, and 1 duplicate case) (figure 2).
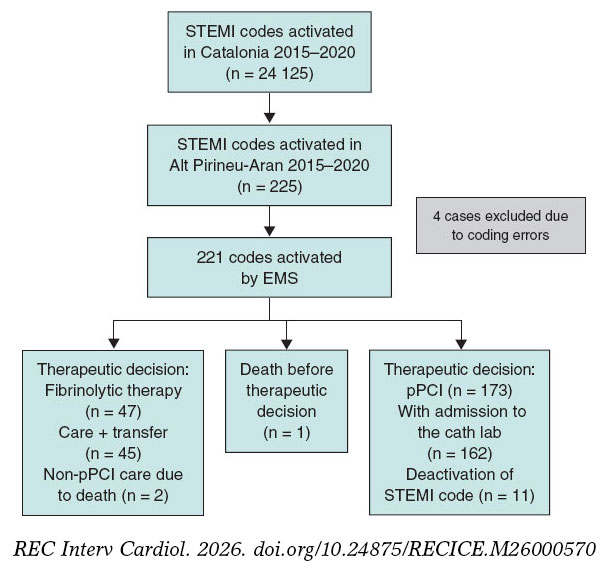
Figure 2. Flow diagram of STEMI codes. AMI, acute myocardial infarction; pPCI, primary percutaneous coronary intervention; EMS, Emergency Medical Services of Catalonia.
The mean age of the 221 included patients was 64.7 years (range, 27–96). Of these, 72.4% were men and 67.4% resided in the study area. All STEMI codes were activated after ECG acquisition at first medical contact, either at a county hospital (51.6%), by EMS at the patient’s home or in a public setting (28.9%), or at a primary care center (19.5%). The median time from first medical contact to ECG acquisition was 6 minutes, and from pain onset to ECG acquisition, 90 minutes (table 1).
Table 1. Clinical characteristics and care times of activated STEMI codes and comparison according to therapeutic decision
| Clinical and care characteristics | Total AMI (n = 221)* | No fibrinolysis (n = 173) | Fibrinolysis (n = 47) | P |
|---|---|---|---|---|
| Female sex | 61 (27.6) | 47 (27.2) | 13 (27.7) | 1 |
| Age (years) | 64.7 (13.7) | 65.7 (13.7) | 60.7 (12.7) | .023 |
| Year | .201 | |||
| 2015 | 30 (13.6) | 25 (14.5) | 5 (10.6) | |
| 2016 | 34 (15.4) | 24 (13.9) | 10 (21.3) | |
| 2017 | 27 (12.2) | 17 (9.83) | 9 (19.1) | |
| 2018 | 35 (15.8) | 27 (15.6) | 8 (17.0) | |
| 2019 | 57 (25.8) | 46 (26.6) | 11 (23.4) | |
| 2020 | 38 (17.2) | 34 (19.7) | 4 (8.51) | |
| Residents in Alt Pirineu i Aran health region | 149 (67.4) | 118 (68.2) | 30 (63.8) | .695 |
| Altitude (m) | 838 [691;1202] | 790 [659;1202] | 974 [691;1202] | .08 |
| Location of first medical contact | .01 | |||
| Primary care center | 65 (29.4) | 57 (32.9) | 8 (17.0) | |
| Home | 20 (9.05) | 18 (10.4) | 2 (4.26) | |
| County hospital | 94 (42.5) | 63 (36.4) | 30 (63.8) | |
| EMS or public setting | 42 (19.0) | 35 (20.2) | 7 (14.9) | |
| Night shift | 56 (25.3) | 34 (19.7) | 22 (46.8) | < .001 |
| Sympton onset–first medical contact time (min) | 80.0 [35.0;193] | 82.0 [39.0;210] | 60.0 [30.0;180] | .292 |
| First medical contact–ECG acquisition time (min) | 6.00 [1.00;12.0] | 6.00 [1.00;12.0] | 5.00 [2.50;12.0] | .807 |
| Sympton onset–ECG acquisition time (min) | 90.0 [45.0;216] | 91.0 [49.0;253] | 80.0 [37.5;192] | .182 |
| Estimated time to PCI-capable center (min) | 106 [93.0;112] | 105 [84.0;109] | 107 [96.0;114] | .061 |
| Estimated time to PCI-capable center ≥ 90 min | 169 (76.5) | 127 (73.4%) | 41 (87.2) | .074 |
| Distance to PCI-capable center (km) | 131 [116;143] | 131 [100;142] | 131 [127;149] | .393 |
| Type of transfer | .036 | |||
| Interhospital | 123 (55.7) | 89 (51.4) | 33 (70.2) | |
| Delayed | 71 (32.1) | 63 (36.4) | 8 (17.0) | |
| Primary | 27 (12.2) | 21 (12.1) | 6 (12.8) | |
| Mode of transport | < .001 | |||
| Ambulance | 106 (48.0) | 69 (39.9) | 36 (76.6) | |
| Helicopter | 56 (25.3) | 49 (28.3) | 7 (14.9) | |
| Ambulance + helicopter | 59 (26.7) | 55 (31.8) | 4 (8.51) | |
| Past medical history | ||||
| Hypertension | 104 (47.1) | 85 (49.1) | 18 (38.3) | .248 |
| Diabetes | 49 (22.2) | 42 (24.3) | 6 (12.8) | .135 |
| Dyslipidemia | 92 (41.6) | 69 (39.9) | 23 (48.9) | .343 |
| Smoking | 63 (28.5) | 47 (27.2) | 16 (34.0) | .458 |
| Previous AMI | 25 (11.3) | 21 (12.1) | 4 (8.51) | .663 |
| Previous pPCI | 25 (11.3) | 22 (12.7) | 3 (6.38) | .34 |
| Stroke | 16 (7.24) | 14 (8.09) | 2 (4.26) | .532 |
| Previous antiplatelet therapy | 40 (18.1) | 35 (20.2) | 5 (10.6) | .194 |
| Treatment and prehospital complications | ||||
| Shock | 8 (3.62) | 5 (2.89) | 2 (4.26) | .643 |
| Ventricular fibrillation | 6 (2.71) | 4 (2.31) | 2 (4.26) | .611 |
| Asystole | 6 (2.71) | 3 (1.73) | 2 (4.26) | .29 |
| Intubation | 7 (3.17) | 4 (2.31) | 2 (4.26) | .611 |
|
AMI, acute myocardial infarction; ECG, electrocardiogram; EMS, Emergency Medical Services of Catalonia; PCI-capable center, percutaneous coronary intervention capable center; pPCI, primary or secondary percutaneous coronary intervention. * Includes 1 patient who died without therapeutic decision. Distribution of totals, no fibrinolysis, and fibrinolysis. Values are expressed as percentage or median. Quantitative variables are expressed as mean (standard deviation) or median [25th percentile; 75th percentile]. |
||||
The incident location had a mean altitude of 838 meters and was located at distances ranging from 81 km to 257 km from the PCI-capable center (median, 131 km). Overall, 76.5% of patients were situated more than 90 minutes from the PCI-capable center (median estimate transfer time, 106 minutes). Air advanced life support was used in 52.5% of the transfers (table 1).
Differences were observed in the time from ECG acquisition to pPCI according to mode of transport (Kruskal-Wallis; P < .001). The median time was 183 minutes for ground ambulance, 138 minutes for helicopter transport, and 140 minutes for combined transport (table 1). Pairwise comparisons using the Mann–Whitney U test showed significant differences compared with ground transport after adjustment for the false discovery rate.
We observed marked variability in the annual frequency of STEMI code cases, with a particularly high number in 2019, and in the proportion of first-assistance fibrinolysis performed from a minimum of 10.5% in 2020 to a maximum of 34.6% in 2017. The number of cases attended in 2020 (the year of the COVID-19 pandemic) was slightly higher than in 2015–2017 (38 cases [17.2%]) but lower than in 2019, which recorded 57 cases (25.8%) (table 1).
Delays in treatment
In 91.5% of patients in whom the therapeutic decision was to perform fibrinolysis at first medical contact, the time between ECG acquisition and treatment exceeded the recommended threshold (> 10 minutes).
When the therapeutic decision was to perform pPCI, the time between ECG acquisition and pPCI exceeded the recommended threshold (> 120 minutes) in 79.6% of cases (table 2).
Table 2. Factors associated with delay in reperfusion treatment
| Clinical and care characteristics | Fibrinolysis (n = 47) | ≤ 10 min | > 10 min | P | pPCI (n = 162) | ≤ 120 min | > 120 min | P |
|---|---|---|---|---|---|---|---|---|
| Female sex | 13 (27.7) | 3 (75.0) | 10 (23.3) | .059 | 45 (27.8) | 6 (18.2) | 39 (30.2) | .245 |
| Age (years) | 60.7 (12.7) | 61.2 (13.8) | 60.7 (12.7) | .943 | 65.3 (13.4) | 65.3 (13.3) | 65.3 (13.5) | 1 |
| Residents in Alt Pirineu i Aran health region | 30 (63.8) | 3 (75.0) | 27 (62.8) | 1 | 109 (67.3) | 22 (66.7) | 87 (67.4) | 1 |
| Altitude (m) | 974 [691;1202] | 946 [649;1202] | 974 [691;1202] | .859 | 692 [640;1202] | 692 [524;957] | 838 [691;1202] | .079 |
| Location of first medical contact | .13 | .014 | ||||||
| Primary care center | 8 (17.0) | 2 (50.0) | 6 (14.0) | 55 (34.0) | 12 (36.4) | 43 (33.3) | ||
| Home | 2 (4.26) | 0 (0.00) | 2 (4.65) | 16 (9.88) | 5 (15.2) | 11 (8.53) | ||
| County hospital | 30 (63.8) | 1 (25.0) | 29 (67.4) | 58 (35.8) | 5 (15.2) | 53 (41.1) | ||
| EMS or public setting | 7 (14.9) | 1 (25.0) | 6 (14.0) | 33 (20.4) | 11 (33.3) | 22 (17.1) | ||
| Night shift | 22 (46.8) | 3 (75.0) | 19 (44.2) | .328 | 31 (19.1) | 1 (3.03) | 30 (23.3) | .017 |
| Symptom onset–first medical contact time (min) | 60.0 [30.0;180] | 190 [180;200] | 57.0 [28.5;152] | .047 | 82.5 [40.0;206] | 60.0 [40.0;116] | 90.0 [40.0;255] | .124 |
| First medical contact–ECG acquisition time (min) | 5.00 [2.50;12.0] | 3.00 [0.75;7.50] | 6.00 [3.00;12.0] | .421 | 6.00 [1.00;11.8] | 6.00 [1.00;10.0] | 6.00 [1.00;12.0] | .75 |
| Symptom onset–ECG acquisition time (min) | 80.0 [37.5;192] | 198 [191;202] | 60.0 [35.0;160] | .05 | 93.5 [50.0;250] | 80.0 [43.0;117] | 115 [57.0;309] | .053 |
| Time to PCI-capable center (min) | 106 (15.9) | 101 (16.2) | 106 (16.0) | .614 | 105 [82.5;110] | 97.0 [71.0;108] | 106 [94.0;111] | .309 |
| Time to PCI-capable center ≥ 90 min | 41 (87.2) | 3 (75.0) | 38 (88.4) | .432 | 118 (72.8) | 19 (57.6) | 99 (76.7) | .047 |
| Distance to PCI-capable center (km) | 131 [127;149] | 132 [123;138] | 131 [127;149] | .969 | 131 [100;143] | 123 [85.0;137] | 131 [123;143] | .085 |
| Type of transfer | .342 | .001 | ||||||
| Interhospital | 33 (70.2) | 2 (50.0) | 31 (72.1) | 83 (51.2) | 8 (24.2) | 75 (58.1) | ||
| Delayed | 8 (17.0) | 1 (25.0) | 7 (16.3) | 59 (36.4) | 18 (54.5) | 41 (31.8) | ||
| Primary | 6 (12.8) | 1 (25.0) | 5 (11.6) | 20 (12.3) | 7 (21.2) | 13 (10.1) | ||
| Mode of transport | 1 | < .001 | ||||||
| Ambulance | 36 (76.6) | 4 (100) | 32 (74.4) | 65 (40.1) | 2 (6.06) | 63 (48.8) | ||
| Helicopter | 7 (14.9) | 0 (0.00) | 7 (16.3) | 48 (29.6) | 18 (54.5) | 30 (23.3) | ||
| Ambulance + helicopter | 4 (8.51) | 0 (0.00) | 4 (9.30) | 49 (30.2) | 13 (39.4) | 36 (27.9) | ||
|
ECG, electrocardiogram; EMS, Emergency Medical Services of Catalonia; PCI-capable center, percutaneous coronary intervention capable center; pPCI, primary or secondary percutaneous coronary intervention. Values are expressed as percentage or median. Quantitative variables are expressed as mean (standard deviation) or median [25th percentile; 75th percentile]. |
||||||||
Among patients located more than 90 minutes from a PCI-capable center who did not receive fibrinolysis at first medical contact, the reason for withholding treatment was not documented in 87 cases (68.5%). Although 76.5% of patients were situated more than 90 minutes from the PCI-capable center, a substantial underuse of fibrinolytic treatment was observed. Of note, patients with a longer time interval from symptom onset to ECG acquisition were more likely to receive fibrinolytic treatment earlier.
Interhospital transfers, incidents without participation of air advanced life support, and nighttime incidents located more than 90 minutes from the PCI-capable center showed greater delays in performing pPCI. Exclusive use of ground ambulance for transfer to the PCI-capable center was associated with a 96.9% rate of delay and emerged as the primary variable in the classification tree for delay between ECG acquisition and pPCI. Among helicopter transfers, delays were more frequent in interhospital transfers (85.4%). In primary or delayed primary transfers, delays were more common when the incident location was more than 90 minutes from the PCI-capable center (65.1%) compared with locations less than 90 minutes away (23.1%) (figure 3).
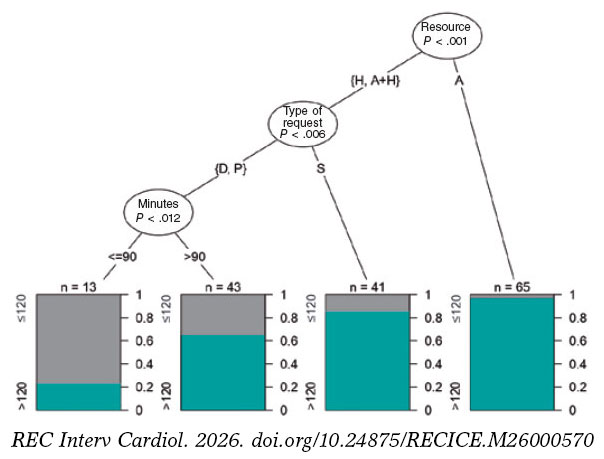
Figure 3. Classification tree for delay in primary percutaneous coronary intervention (pPCI). Three factors were significantly associated with delay: mode of transport (ambulance [A], helicopter [H], or combined use), type of activation (primary [P], delayed [D], or interhospital [S]), and estimated road travel time from the event location to the PCI-capable center in minutes (> 90 minutes < 90 minutes).
Mortality
A total of 18 patients (8.1%) died within the first 15 days. Mortality was significantly higher in patients who experienced a major event (asystole, intubation, shock, or ventricular fibrillation) within the first 24 hours. Age was significantly associated with mortality only at the 48-hour and 15-day follow-up. There were no significant differences in 15-day mortality between patients treated with fibrinolysis and those directly transferred for pPCI. Increased mortality was associated with treatment delays, particularly in the early mortality subgroup (< 24 hours); however, these differences did not reach statistical significance (table 3).
Table 3. Factors associated with mortality according to time from clinical course prior to death
| Clinical and care characteristics | Pre-PCI-capable center (n = 3) | < 24 h (n = 8) | < 48 h (n = 12) | P | ≤ 15 days (n = 18) | P |
|---|---|---|---|---|---|---|
| Female sex | 1 (33.3) | 2 (25.0) | 4 (33.3) | .741 | 6 (33.3) | .587 |
| Age (years) | 67.7 (25.7) | 69.8 (16.0) | 74.4 (15.8) | .047 | 74.1 (14.1) | .008 |
| Residents in Alt Pirineu i Aran health region | 2 (66.7) | 6 (75.0) | 9 (75.0) | .755 | 13 (72.2) | .848 |
| Altitude (m) | 974 [721;1042] | 832 [691;1014] | 691 [468;1014] | .154 | 832 [691;1136] | .625 |
| Location of first medical contact | .337 | .514 | ||||
| Primary care center | 0 (0.00) | 1 (12.5) | 1 (8.33) | 3 (16.7) | ||
| Home | 0 (0.00) | 1 (12.5) | 1 (8.33) | 1 (5.56) | ||
| County hospital | 2 (66.7) | 4 (50.0) | 7 (58.3) | 9 (50.0) | ||
| EMS or public setting | 1 (33.3) | 2 (25.0) | 3 (25.0) | 5 (27.8) | ||
| Night shift | 0 (0.00) | 1 (12.5) | 2 (16.7) | .735 | 4 (22.2) | 1 |
| Symptom onset–first medical contact time (min) | 38.0 [19.0;246] | 64.5 [22.0;488] | 41.0 [22.0;488] | .502 | 65.0 [26.2;413] | .723 |
| First medical contact–ECG acquisition time (min) | 30.0 [17.0;11 542] | 3.00 [0.00;11.2] | 1.50 [0.00;11.2] | .152 | 2.00 [0.00;24.0] | .205 |
| Symptom onset–ECG acquisition time (min) | 42.0 [36.0;11 774] | 66.5 [28.8;682] | 45.0 [30.0;682] | .543 | 81.0 [42.8;518] | .962 |
| Estimated time to PCI-capable center (min) | 96.0 [90.5;113] | 107 [95.8;107] | 96.0 [81.5;107] | .242 | 96.0 [95.0;107] | .432 |
| Estimated time to PCI-capable center ≥ 90 min | 2 (66.7) | 7 (87.5) | 8 (66.7) | .483 | 14 (77.8) | 1 |
| Distance to PCI-capable center (km) | 134 [108;149] | 131 [130;132] | 131 [85.0;131] | .15 | 131 [119;134] | .419 |
| Type of transfer | .911 | .938 | ||||
| Secondary | 2 (66.7) | 4 (50.0) | 8 (66.7) | 11 (61.1) | ||
| Delayed | 1 (33.3) | 3 (37.5) | 3 (25.0) | 5 (27.8) | ||
| Primary | 0 (0.00) | 1 (12.5) | 1 (8.33) | 2 (11.1) | ||
| Mode of transport | .508 | .734 | ||||
| Ambulance | 1 (33.3) | 3 (37.5) | 5 (41.7) | 10 (55.6) | ||
| Helicopter | 1 (33.3) | 1 (12.5) | 2 (16.7) | 3 (16.7) | ||
| Ambulance + helicopter | 1 (33.3) | 4 (50.0) | 5 (41.7) | 5 (27.8) | ||
| Fibrinolytic therapy at first medical contact | 2 (100) | 2 (28.6) | 2 (18.2) | 1 | 4 (23.5) | .764 |
| Delayed fibrinolytic therapy or pPCI | 2 (100) | 7 (100) | 10 (90.9) | .693 | 16 (94.1) | .318 |
| Past medical history | ||||||
| Hypertension | 1 (33.3) | 4 (50.0) | 7 (58.3) | .612 | 11 (61.1) | .317 |
| Diabetes | 1 (33.3) | 2 (25.0) | 3 (25.0) | .731 | 5 (27.8) | .558 |
| Dyslipidemia | 0 (0.00) | 2 (25.0) | 4 (33.3) | .765 | 7 (38.9) | 1 |
| Smoking | 0 (0.00) | 1 (12.5) | 1 (8.33) | .186 | 4 (22.2) | .731 |
| Previous AMI | 0 (0.00) | 1 (12.5) | 2 (16.7) | .631 | 3 (16.7) | .437 |
| Previous pPCI | 0 (0.00) | 1 (12.5) | 2 (16.7) | .631 | 2 (11.1) | 1 |
| Previous stroke | 0 (0.00) | 0 (0.00) | 0 (0.00) | 1 | 1 (5.56) | 1 |
| Prior antiplatelet therapy | 0 (0.00) | 0 (0.00) | 2 (16.7) | 1 | 3 (16.7) | 1 |
| Treatment and prehospital complications | ||||||
| Shock | 2 (66.7) | 3 (37.5) | 4 (33.3) | < .001 | 6 (33.3) | < .001 |
| Ventricular fibrillation | 2 (66.7) | 3 (37.5) | 3 (25.0) | .002 | 3 (16.7) | .008 |
| Asystole | 3 (100) | 5 (62.5) | 5 (41.7) | < .001 | 5 (27.8) | < .001 |
| Intubation | 3 (100) | 4 (50.0) | 4 (33.3) | < .001 | 4 (22.2) | .001 |
|
AMI, acute myocardial infarction; ECG, electrocardiogram; EMS, Emergency Medical Services of Catalonia; PCI-capable center, percutaneous coronary intervention capable center; pPCI, primary or secondary percutaneous coronary intervention. Values are expressed as percentage or median. Quantitative variables are expressed as mean (standard deviation) or median [25th percentile; 75th percentile]. |
||||||
DISCUSSION
In our study, only 20.4% of patients who underwent pPCI received treatment within 120 minutes. Only 4 of the 47 patients treated with fibrinolysis received therapy within 10 minutes.
Several studies, such as the STREAM,13 have shown that prehospital fibrinolysis followed by early pPCI may offer results similar to direct transfer for pPCI if patients are treated within the first 3 hours from symptom onset. In our analysis, we identified underuse of fibrinolytic therapy, along with insufficient documentation of the reasons for withholding treatment.
In contrast to the studies by Stopyra et al.9,14 conducted in North Carolina (United States) in which 60.5% of patients underwent pPCI within ≤ 90 minutes, only 20.4% of patients in our study achieved reperfusion within a broader threshold (< 120 minutes). These findings underscore longer treatment delays in our region and support more frequent consideration of fibrinolytic therapy.
Although Aboal et al.10,11 reported higher mortality rates associated with delayed pPCI, we did not observe a significant association in our study, despite a substantial lower proportion of patients undergoing pPCI within the target time (20.4% vs 42%). In addition, fibrinolysis was more frequently used in patients located more than 50 km from the PCI-capable center (66.7%), reflecting structural and logistical constraints specific to the Alt Pirineu-Aran region that influence treatment selection and reperfusion times.
In line with former evidence regarding mortality, the study results reinforce the clinical importance of time to care as a potential factor associated with worse prognosis, which is particularly relevant in early mortality (< 24 hours).
Compared with the study by Carol et al.,15 in which 58% of patients underwent pPCI after more than 120 minutes, our data show a substantial higher proportion (79.6%). Factors associated with delay, such as intubation, initial shock, and nighttime care, were consistent between the 2 studies; however, other variables, including left bundle branch block, were not. A notable finding of our study is that the care delivered by the EMS was associated with shorter treatment times compared with county hospitals.
Patient origin, geographic location, sex, number of resources involved, time required for therapeutic decision-making, and mode of transport influenced treatment times as well. Hakim et al.16 suggest that helicopter transport is less effective than ground transport, especially for distances of less than 50 km. In our study, 71% of patients transferred by helicopter (all located more than 50 km from the PCI-capable center) received pPCI after more than 120 minutes, which may be associated with the lack of a helipad at the reference PCI-capable center, requiring additional ground transfer, and service hours, mainly daytime during the study period. In constrast to other studies conducted during the COVID-19 pandemic,17,18 our series did not demonstrate a reduction in case volume or prolongation in alert time. However, 2020 was the year with the lowest use of fibrinolysis (4 cases, 10.5%).
Several studies indicate that delays in STEMI recognition and code activation have a direct impact on reperfusion time. One study highlights that training significantly improves these times,19 suggesting that lack of training or skills among professionals may generate delays in care and lower use of fibrinolysis. Our study shows appropriate timing in ECG acquisition and emergency recognition by teams. Delayed primary transfers included the highest percentages of patients with optimal reperfusion times (table 2).
Our findings underscore the need to review and optimize action protocols, particularly in non-PCI-capable centers and geographic areas with greater delays. It is essential to optimize professional response to suspected STEMI, improve therapeutic decision-making time, and explore innovative solutions such as triage systems and STEMI code detection with technological support, optimization of air transport, and greater coordination between PCI and non-PCI capable centers.
Limitations and strengths
This study has limitations due to the small population size in the rural areas studied, which required extending the study period to 6 years to obtain the collected sample. This extension implies that data underwent several changes in record systems (from paper to digitized format) and organizational modifications (implementation of triage in emergency departments and nighttime helicopter flights). The sample of 221 patients remains limited and may have affected the statistical power to detect significant differences between analyzed variables. Similarly, distances from the incident location and estimated average travel times under optimal conditions were used, without accounting for any potential delays due to traffic or other unforeseen factors.
CONCLUSIONS
The results of this study demonstrate the need to increase the use of fibrinolysis in areas distant from a PCI-capable center to reduce reperfusion delays. Documentation of the reasons for not performing fibrinolysis should be improved, as this limits interpretation regarding therapeutic appropriateness. Joint initial care by primary care and emergency teams, as well as delayed primary transfers, reduce reperfusion times and avoid interhospital transfers. Finally, the low number of deaths during the study period prevents multivariate analysis and only allows identification of the variables or characteristics associated with mortality described in the results.
Despite these limitations, the study provides a comprehensive analysis of variables and describes in detail how the investigated population is managed and transferred, something unprecedented in this context. In addition, cross-referencing and thorough review of 2 databases provide valuable information to assess treatment delays. Therefore, this study is a solid basis for future advances in improving STEMI code management in rural areas.
FUNDING
This study was funded by the Provincial Council of Lleida through “The strength of municipalities” project and by IRBLleida through project PP10851 of the Alt Pirineu-Aran Intramural Research Program (IREP).
ETHICAL CONSIDERATIONS
This study was approved by the IDIAP Jordi Gol Ethics Committee, code CEIm 22/238-P. The SAGER guidelines were followed regarding potential sex and gender bias.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
ChatGPT was used to improve the wording of some paragraphs of the article. After using this tool, the authors reviewed and edited the content as necessary and take full responsibility for the final version.
AUTHORS’ CONTRIBUTIONS
M. Navarra Llorens was responsible for study conception and design, overall supervision, and manuscript drafting. M. Martínez Alonso conducted the statistical analysis, interpreted the results, and critically reviewed the content. Y. Azeli was responsible for clinical analysis and critical review. S. Ferrandis Barrés collected data and contributed to the discussion and critical review. M. Canelles Seix collected data and reviewed the manuscript. L. Duch Grau participated in data collection, manuscript review, and final approval. A.M. Forradelles Rey collected data and performed critical review. M.A. Martínez Momblan supervised the project and critically reviewed the manuscript. X. Jiménez-Fàbrega supervised the project and provided intellectual contributions to the discussion. All authors approved the final text.
CONFLICTS OF INTEREST
None declared.
ACKNOWLEDGMENTS
We thank Mar Franch Casanovas and Francisco Iturbe Recasens for their collaboration in data collection, and Isidre Felip for his advice in drafting the manuscript.
WHAT IS KNOWN ABOUT THE TOPIC?
- STEMI requires early coronary reperfusion to reduce mortality and improve prognosis.
- In Catalonia, implementation of the STEMI code has optimized system response; however, in regions such as Alt Pirineu, delays have not been specifically evaluated.
WHAT DOES THIS STUDY ADD?
- This study shows significant underuse of fibrinolytic therapy, even among patients located far from a PCI-capable center. In additions, it highlights the absence of systematic documentation regarding the reasons for withholding fibrinolysis, thereby limiting the evaluation of therapeutic decision-making.
- The study demonstrates that joint initial care by primary care and emergency teams, along with delayed primary transfer, can reduce reperfusion times and avoid interhospital transfers, which are associated with longer delays.
- Similarly, it identifies the mode of transport as the main predictive variable for delay and shows that exclusive use of ground ambulance is the most critical factor.
- Although the low number of deaths prevents a robust multivariate analysis, characteristics associated with mortality are described, and the influence of delays is confirmed, reinforcing the need for adapted strategies.
SUPPLEMENTARY DATA

REFERENCES
1. Ibáñez B, James S, Agewall S, et al. ESC 2017 guidelines on the treatment of acute myocardial infarction in patients with ST segment elevation. Rev Esp Cardiol. 2017;70:1082.e1-1082.e61.
2. Steg G, James SK, Atar D, et al. ESC Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting With ST-Segment Elevation. Rev Esp Cardiol. 2013;66:53.e1-53.e46.
3. Rao SV, O'Donoghue ML, Ruel M, et al. 2025 ACC/AHA/ACEP/NAEMSP/ SCAI Guideline for the Management of Patients With Acute Coronary Syndromes:A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2025;85:2135-2237.
4. Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44:3720-3826.
5. Faixedas MT, Mauri J, Pueyo MJ. The Codi IAM registry:acute myocardial infarction code registry in Catalonia. Rev Esp Cardiol. 2022;75:291-293.
6. Instrucció04/2009, de 12 de maig. Sectoritzacióde l'atencióa les persones malaltes amb infart agut de miocardi (IAM) amb elevaciódel segment ST per tal de portar a terme l'angioplàstia primària. Available at:Error!Hyperlink reference not valid.. Accessed 20 Jan 2026.
7. Rivero F, Bastante T, Cuesta J, et al. Factors Associated With Delays in Seeking Medical Attention in Patients With ST-segment Elevation Acute Coronary Syndrome. Rev Esp Cardiol. 2016;69:279-285.
8. Berga Congost G, Valverde Bernal J, Márquez López A. Factores clínicos predictores de retraso en la actuación del código infarto. Enferm Cardiol. 2017;71:63-71.
9. Stopyra JP, Snavely AC, Ashburn NP, Supples MW, Miller CD, Mahler SA. Delayed first medical contact to reperfusion time increases mortality in rural emergency medical services patients with ST-elevation myocardial infarction. Acad Emerg Med. 2023;30:1101-1109.
10. Aboal J, Núñez M, Bosch D, Tirón C, Brugada R. Angioplastia primaria frente a fibrinolisis en pacientes alejados de un centro con hemodinámica. Emergencias. 2017;29:99-104.
11. Aboal J, Ramos R, Loma-Osorio P, et al. Factores asociados a retrasos de tiempo desde el electrocardiograma diagnóstico hasta el paso de guía en el infarto agudo de miocardio con elevación del segmento ST transferido para angioplastia primaria. Emergencias. 2021;33:195-202.
12. Brunetti ND, Dell'Anno A, Martone A, et al. Prehospital ECG transmission results in shorter door-to-wire time for STEMI patients in a remote mountainous region. Am J Emerg Med. 2020;38:252-257.
13. Van De Werf F, Ristic´AD, Averkov OV, et al. STREAM-2:Half-Dose Tenecteplase or Primary Percutaneous Coronary Intervention in Older Patients With ST-Segment-Elevation Myocardial Infarction:A Randomized, Open-Label Trial. Circulation. 2023;148:753-764.
14. Stopyra JP, Snavely AC, Ashburn NP, et al. Rural EMS STEMI Patients –Why the Delay to PCI?Prehosp Emerg Care. 2024;28:947-954.
15. Carol Ruiz A, Masip Utset J, Ariza-SoléA, et al. Predictors of primary percutaneous coronary intervention delay in cases of myocardial infarction diagnosed in hospitals without hemodynamic support systems. Emergencias. 2021;33:187-194.
16. Hakim R, Revue E, Saint Etienne C, et al. Does helicopter transport delay prehospital transfer for STEMI patients in rural areas?Findings from the CRAC France PCI registry. Eur Heart J Acute Cardiovasc Care. 2020;9:958-965.
17. Romaguera R, Ribera A, Güell-Viaplana F, Tomás-Querol C, Muñoz-Camacho JF, Agudelo V. Decrease in ST-segment elevation myocardial infarction admissions in Catalonia during the COVID-19 pandemic. Rev Esp Cardiol. 2020;73:778-780.
18. Kaddoura R, Salam AM. Thrombosis Management and Challenges in COVID-19 Patients Presenting with Acute Coronary Syndromes. Heart Views. 2020;21:195.
19. Berga Congost G, Brugaletta S, Garcimartin Cerezo P, et al. Effectiveness of a nurse training intervention in the emergency department to improve the diagnosis and treatment of stemi patients:EDUCAMI study. Heart Lung. 2025;70:305-312.
ABSTRACT
Introduction and objectives: Excimer laser coronary atherectomy (ELCA) is increasingly used in complex percutaneous coronary interventions (PCI), particularly in cases of “balloon failure,” which includes both uncrossable and undilatable coronary artery lesions. Although these 2 scenarios represent distinct technical and clinical challenges, they are usually evaluated using the same safety and efficacy endpoints. As a result, there is a lack of specific evidence on the safety and efficacy profile of ELCA in each of these situations. Furthermore, the role of intracoronary imaging in optimizing ELCA use remains insufficiently defined.
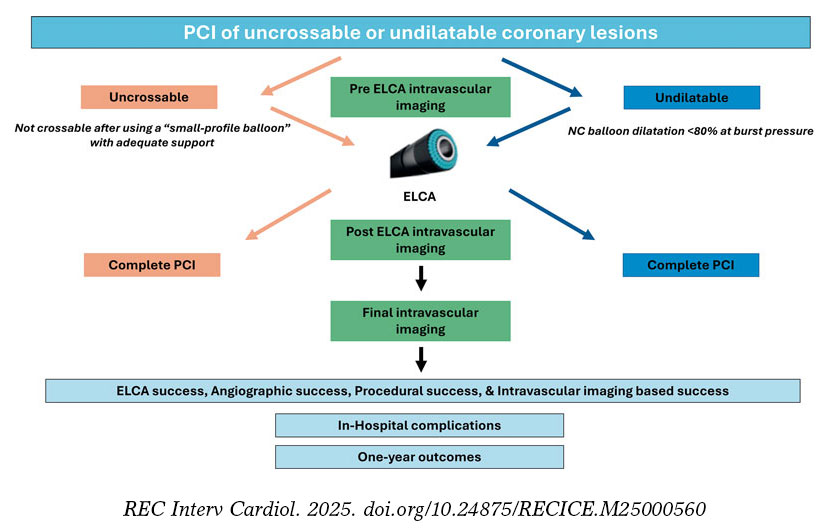
Methods: This will be an investigator-initiated, multicenter, single-arm, open-label, prospective observational study. Patients with an indication for PCI and undilatable (non-compliant balloon dilatation < 80% at burst pressure) or uncrossable (uncrossable with a “small-profile balloon” with adequate support, left to the operator’s discretion) coronary artery lesions treated with ELCA will be included. Intravascular imaging will be highly advised and analyzed in a core laboratory. Device success, angiographical success, procedural success, clinical success and related complications will be evaluated. Patients will be postoperatively followed for 1 year and clinical events will be recorded.
Conclusions: The LUDICO study will be a multicentre, prospective study of ELCA therapy in uncrossable or undilatable coronary lesions. The study aims to evaluate the safety and efficacy profile of ELCA in these lesions as well as the clinical results at the 1 year follow-up in this setting. (ClinicalTrials.gov: NCT07206082).
Keywords: Percutaneous coronary intervention. Excimer laser coronary atherectomy. Intravascular imaging. Optical coherence tomography. Complex coronary intervention.
RESUMEN
Introducción y objetivos: La aterectomía coronaria con láser de excímeros (ELCA) se utiliza cada vez más en intervenciones coronarias percutáneas (ICP) complejas, en particular en caso de «fallo del balón», que incluye tanto lesiones coronarias no cruzables como no dilatables. Aunque estos 2 escenarios representan desafíos técnicos y clínicos distintos, con frecuencia se han evaluado utilizando los mismos criterios de efectividad y seguridad. Como resultado, existe una falta de evidencia específica sobre la seguridad y la efectividad de la ELCA en cada una de estas situaciones. Además, el papel de la imagen intracoronaria en la optimización del uso de la ELCA sigue estando insuficientemente descrito.
Métodos: Se trata de un estudio observacional prospectivo, abierto, multicéntrico e iniciado por los investigadores. Se incluirán pacientes con indicación de ICP y lesiones coronarias no dilatables (dilatación con balón no distensible < 80% a presión de ruptura) o no cruzables (no cruzables con un balón de bajo perfil y adecuado soporte, a criterio del operador) tratados con ELCA. Se recomendará el uso de imagen intravascular, que se analizará en un laboratorio central. Se evaluarán el éxito del dispositivo, el éxito angiográfico, el éxito del procedimiento, el éxito clínico y las complicaciones asociadas. Se seguirá a los pacientes durante 1 año tras el procedimiento y se registrarán los eventos clínicos.
Conclusiones: El estudio LUDICO será un estudio prospectivo y multicéntrico sobre el uso de ELCA en lesiones coronarias no cruzables o no dilatables. Su objetivo es evaluar la efectividad y la seguridad de la ELCA en estas situaciones, así como los resultados clínicos durante un seguimiento de 1 año. (ClinicalTrials.gov: NCT07206082).
Palabras clave: Intervención coronaria percutánea. Aterectomía coronaria con láser de excímeros. Imagen intravascular. Tomografía de coherencia óptica. Intervención coronaria compleja.
Abbreviations
ELCA: excimer laser coronary angioplasty. IVUS: intravascular ultrasound. OCT: optical coherence tomography. PCI: percutaneous coronary intervention. RA: rotational atherectomy.
INTRODUCTION
Excimer laser coronary atherectomy (ELCA) has been applied since the 1980s in multiple anatomical and clinical settings, with several studies supporting its safety and efficacy profile.1,2 Common indications include in-stent restenoses, stent underexpansion, calcified coronary lesions, saphenous vein graft stenoses, thrombotic lesions, bifurcations, and chronic total coronary occlusions.3-14 In practice, however, ELCA is predominantly used in the setting of balloon failure–specifically uncrossable and undilatable coronary artery lesions. However, historical studies have typically applied a uniform definition of device success across both lesion types, potentially overlooking important nuances that could influence outcomes and therapeutic decision-making.
Furthermore, despite growing recognition of the value of intracoronary imaging in optimizing complex percutaneous coronary intervention (PCI),15 prior ELCA studies have largely underutilized this tool, limiting insight into the mechanisms of success or failure in balloon-resistant lesions.
The safety and efficacy profile of coronary laser in undilatable and uncrossable lesions (LUDICO) study is a real-world, observational study designed to evaluate the use of ELCA specifically in cases of balloon failure. The study has 2 primary objectives: a) to refine the definition of ELCA procedural success based on the type of balloon failure encountered—distinguishing between uncrossable and undilatable lesions—, and b) to emphasize the critical role of intracoronary imaging in guiding ELCA and interpreting procedural outcomes. By addressing these critical gaps, the study aims to provide a more precise and and clinically meaningful framework for the contemporary use of ELCA in complex coronary interventions.
METHODS
Study design and population
This is a prospective, multicentre, observational study including consecutive patients undergoing ELCA in undilatable (expansion < 80% of the distal vessel diameter after inflation of a 1:1 non-compliant balloon at 18 atm) and uncrossable coronary artery lesions (uncrossable after using a small-profile balloon with adequate support left to the operator’s discretion). At least 15 national centers will be contacted to participate in the study. Participant centers will be required to have experience with ELCA and complex PCI, with a minimum of > 5 prior ELCA cases performed. Inclusion and exclusion criteria are described in table 1. This study was conducted in full compliance with the STROBE guidelines for observational studies.16 The study protocol was registered in ClinicalTrials.gov (NCT07206082).
Table 1. Inclusion and exclusion criteria
| Inclusion criteria | Exclusion criteria |
|---|---|
| Patients > 18 | Patients with known allergies to ASA, clopidogrel, prasugrel, or ticagrelor |
| Patients with either stable coronary artery disease or acute coronary syndromes as the clinical presentation | Patients unable to provide informed consent, either personally or through a legal representative |
| Patients with severe coronary lesions (> 70% by visual estimation) in native vessels or coronary bypass grafts | Patients with clinical or hemodynamic instability defined as: sustained hypotension (SBP ≤ 90 mmHg for ≥ 30 minutes or use of pharmacological, or mechanical support to maintain an SBP ≥ 90 mmHg) or evidence of end‐organ hypoperfusion including urine output of < 30 mL/h, cool extremities, altered mental status, or serum lactate > 2.0 mmol/L |
| “Uncrossable” coronary lesions (eg, lesions that cannot be crossed with a 0.7:1 balloon after successful guidewire passage) or “Undilatable” lesions (eg, those in which balloon dilation with a 1:1 non-compliant balloon at 18 atm results in < 80% expansion relative to the distal reference vessel diameter; this group includes both de novo lesions and in-stent restenosis or underexpanded stents) |
Patients with significant comorbidities and a life expectancy of < 1 year |
ASA, acetylsalicylic acid; SBP, systolic blood pressure. |
Procedure
PCI will be performed in accordance with current clinical practice guidelines on coronary revascularization.15,17
In uncrossable lesions, following successful guidewire passage and failed balloon crossing, ELCA will be performed (as described in the following section). PCI will be completed with optional predilatation at the operator’s discretion, followed by stenting or drugcoated balloon implantation. Intravascular imaging [preferably with optical coherence tomography (OCT)] will be recommended after laser application to characterize the lesion substrate and evaluate the effect of the laser and at the end of the procedure.
In undilatable lesions, if balloon dilation is inadequate, an initial intracoronary imaging assessment will be conducted. Afterwards, laser atherectomy will be performed, followed by a second intracoronary imaging assessment to evaluate the effects of ELCA on the lesion. PCI will, then, be completed with balloon dilation and stenting or drug-coated balloon implantation, at the operator’s discretion. A third intracoronary imaging pullback will be performed to assess the final procedural outcome (figure 1).
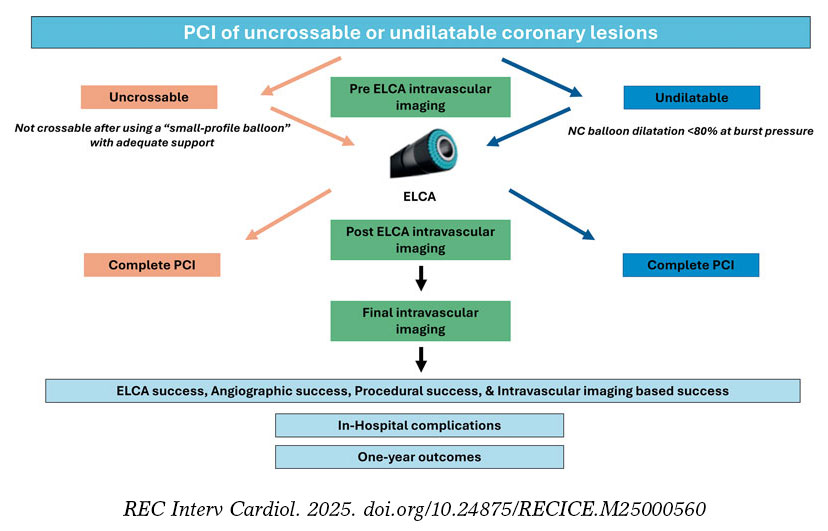
Figure 1. Central illustration. LUDICO study flowchart. ELCA, excimer laser coronary atherectomy; NC, non-compliant; PCI, percutaneous coronary intervention.
Laser atherectomy technique
ELCA procedure will be performed using the Spectranetics CVX300 (Spectranetics, United States) and the latest generation Philips Laser System Excimer (Philips, United States) System, which is based on pulsed xenon‐chlorine laser catheters capable of delivering excimer energy (wavelength, 308 nm; pulse length, 185 ns) from 30 mJ/mm2 to 80 mJ/mm2 (fluencies) at pulse repetition rates of 25 Hz to 80 Hz.
The ELCA technique will be performed according to current recommendations.18 The choice of laser catheter size will be left to the operator’s discretion, selecting among the available rapid-exchange concentric probes (0.9 mm, 1.4 mm, 1.7 mm, or 2.0 mm). The selection of fluence, and repetition rate will be left to the operator’s discretion. A saline infusion technique will be recommended, although application of laser with blood or contrast will be recommended in resistant lesions. In the event of unsuccessful initial therapy, additional plaque modification techniques may be employed at the operator’s discretion and will be thoroughly recorded and described.
Clinical definitions and follow-up
Laser success will be defined differently for uncrossable and for undilatable lesions. For the former, laser success will be defined as the ability of the laser catheter to cross the lesion. Laser success will also be considered in cases where the laser catheter cannot cross the lesion but proximal laser application permits subsequent balloon crossing. For the latter, laser success will be defined as successful balloon dilation (sized 1:1 to the vessel diameter), with adequate expansion (> 80% in 2 orthogonal projections) following laser therapy without the need for other plaque modification technique.
Angiographic success will be defined as Thrombolysis in Myocardial Infarction (TIMI) grade-3 final flow and a percent diameter stenosis < 20%. Procedural success will be defined as angiographic success without severe procedural complications (death, coronary perforation, abrupt vessel closure, flow-limiting dissection). Intracoronary imaging-based success will be defined as a stent expansion ≥ 80% (OCT or intravascular ultrasound [IVUS]) or a minimal stent area (MSA) ≥ 4.5 mm2 in OCT or ≥ 5.5 mm2 in IVUS.
Intracoronary imaging
Intracoronary imaging will aim to describe the lesion characteristics and identify potential predictors of adequate stent expansion and procedural result. Therefore, intracoronary imaging will be highly recommended and the advised imaging modality will be OCT as its better spatial resolution vs IVUS allows better tissue characterization, plaque modification assessment and visualization of stent failure etiologies.19 A baseline intracoronary imaging evaluation is recommended, when possible, to describe the lesion characteristics and identify potential predictors of ELCA success or failure. Additionally, a second intracoronary imaging run is strongly advised immediately after laser therapy. This second run aims to describe the effect of ELCA in the coronary plaque. Evaluating and characterizing changes in the coronary plaque might help guide the optimal ELCA result and allow appropriate adjustment of therapy settings (fluence, repetition rate and infusion characteristics). Finally, a postoperative intravascular imaging run is strongly recommended once the final angiographic result is achieved. All intracoronary imaging data will be analyzed by a core laboratory. In the baseline intracoronary imaging run, lesion characteristics will be described as follows: minimum lumen area (MLA), minimum and maximum lumen diameter, lesion length, calcification angle, calcification thickness. In the post-ELCA imaging run the following parameters will be evaluated: MLA, number of calcium fractures and characteristics, presence of dissection, including its angle and length. In the final imaging run, MSA, stent apposition and dissections will be described. In both OCT and IVUS assessments, a dual-reference approach will be used: the proximal and distal reference lumen diameters will be identified, and MSA will be divided by each of these diameters separately. The final stent expansion index will be calculated as the mean of the 2 resulting values. Second, the tapered mode is only available in OCT: reference lumen profile is estimated based on the distal and proximal reference frame mean diameter and side branch mean diameter in between. With stent lengths > 50 mm, the dual method is preferred. With stent lengths < 50 mm the tapered method is often used. If the dual method is used, the stent expansion percentage of both segments will be recorded with the lower value of the two measurements used for analysis. The main variables to be evaluated by intravascular imaging are summarized and graphically shown in figure 2.
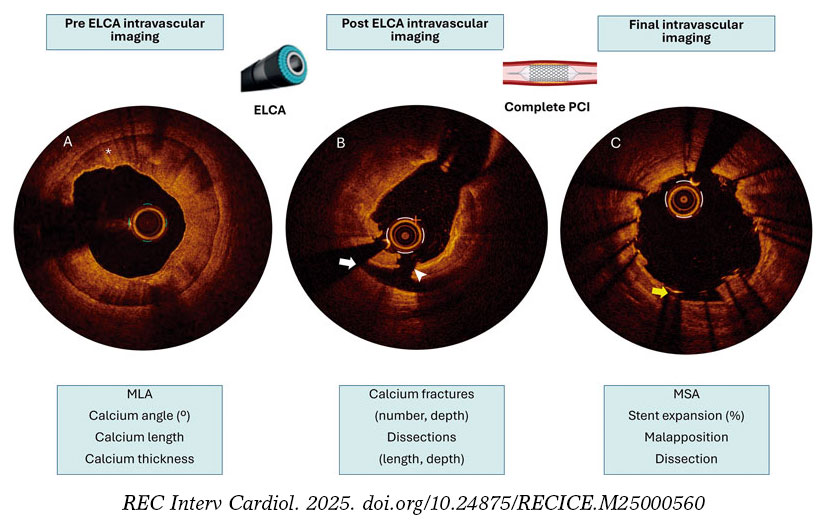
Figure 2. Example of the advised intracoronary imaging assessment in LUDICO study. A: baseline optical coherence tomography (OCT) image of a severely calcified lesion. The asterisk points to a calcium arc of 360° with a maximum thickness of 0.9 mm. B: OCT image after ELCA with contrast media. White arrow points to a dissection. The white arrowhead points to a deep calcium fracture. C: results after stenting. The yellow arrow points to a small area of malapposition. ELCA, excimer laser coronary atherectomy; MLA, minimal lumen area; MSA, minimal stent area; PCI, percutaneous coronary intervention.
Follow-up
Follow-up will be conducted at 3 different timeframes:a) after PCI; procedural success and complications will be thoroughly documented, and all patients will be evaluated for any postoperative events, such as chest pain, heart failure, bleeding, or ischemic events; b) at hospital discharge, documenting clinical status, complications and antiplatelet therapy; and c) 1 year after the index PCI; clinical events and antiplatelet therapy will be recorded.
The primary endpoint at the follow-up will be the composite endpoint of major adverse cardiovascular events, defined as the occurrence of cardiac death, target vessel-related acute myocardial infarction, target vessel revascularization, or definite/probable stent thrombosis. Secondary efficacy endpoints will include all-cause mortality, cardiac death, non-fatal myocardial infarction, target lesion revascularization, and target vessel revascularization. Secondary safety endpoints will include stroke and bleeding events (classified according to the Bleeding Academic Research Consortium [BARC] criteria). Endpoint definitions are shown in table 2.
Table 2. Procedural and clinical definitions
| Procedural definitions | |
|---|---|
| ELCA success | Uncrossable: defined as the ability of the laser catheter to cross the lesion or allow subsequent crossing with a predilatation balloon following laser application |
| Undilatable: defined as successful balloon dilation with adequate expansion following laser therapy | |
| Angiographic success | Defined adequate stent implantation and expansion, with residual stenosis < 20% and TIMI grade-3 flow, without crossover to another plaque modification technique |
| Procedural success | Angiographic success without severe procedural complications (death, coronary perforation, abrupt vessel closure, flow-limiting dissection) |
| Imaging based success | Defined as a stent expansion ≥ 80% (OCT or IVUS) or a MSA ≥ 4.5 mm2 in OCT or ≥ 5.5 mm2 in IVUS |
| Severely calcified coronary lesion | Angiographically: opacification in both sides of the artery before contrast administration |
| Intracoronary imaging: > 180° calcium arc or calcium thickness > 5 mm | |
| Clinical definitions | |
| MACE | Defined as the occurrence of cardiac death, target vessel-related acute MI, target vessel revascularization, or definite/probable stent thrombosis |
| Cardiac death | According to ARC definitions:31
|
| Non-fatal MI | Third universal definition of MI.32 In addition, procedure-related myocardial infarction—defined as a troponin elevation > 5 times the upper limit of normal in patients with previously normal troponin levels, or a ≥ 20% increase in patients with previously elevated troponin levels, along with electrocardiographic changes or new areas of myocardial necrosis detected by imaging—was included |
| Stent thrombosis | According to ARC criteria:
|
| Stroke | New neurological focal deficit with imaging confirmation and assessed by a neurologist |
| TLR | New coronary artery lesion in the previously treated coronary lesion including 5 mm proximal and distal to the implanted stent |
| TVR | New coronary artery lesion in the previously treated coronary vessel |
| Hemorrhage | According to BARC classification33 |
|
ARC, Academic Research Consortium; BARC, Bleeding Academic Research Consortium; ECG, electrocardiogram; ELCA, excimer laser coronary atherectomy; IVUS, intravascular ultrasound; MACE, major adverse cardiovascular events; MI, myocardial infarction; MSA, minimal stent area; OCT, optical coherence tomography; STEMI, ST-segment elevation myocardial infarction; TIMI, Thrombolysis in Myocardial Infarction; TLR, target lesion revascularization; TVR, target vessel revascularization. |
|
Sample size estimation
The planned sample size of 230 patients was determined based on expected device success rates reported in prior studies of ELCA for undilatable and uncrossable lesions. Assuming a conservative laser success rate of 80%, a cohort of 230 patients would yield a 95% confidence interval with a precision of approximately ± 5% (estimated range, 74.8%–85.2%), which is considered adequate for reliably estimating procedural efficacy in the routine clinical practice. Moreover, this sample size ensures sufficient statistical power to support multivariable analyses of predictors of both intraoperative and follow-up outcomes. With an anticipated 40–50 events, the study would allow the inclusion of approximately 4 to 5 covariates in multivariable regression models while maintaining acceptable model stability. Based on the expected procedural volume at each participant center and the required sample size, the recruitment period is 2 to 3 years.
Statistical analysis
Quantitative variables following a normal distribution will be expressed as mean ± standard deviation. Those not following a normal distribution will be reported using the median and minimum and maximum values. Qualitative variables will be expressed as absolute numbers and frequencies.
A significance level of 0.5 will be considered, and 95% confidence intervals will be calculated for the primary outcome variables. Normality of the data will be assessed using the Kolmogorov-Smirnov test. Based on the distribution, appropriate statistical tests will be applied to compare relevant variables. For comparisons of means, the Student t test for independent samples will be used, or the non-parametric Mann-Whitney U test in case of dichotomous qualitative variables. For comparisons involving non-dichotomous qualitative variables, ANOVA or the non-parametric Kruskal-Wallis test will be employed. For bivariate analysis of qualitative variables, the chi-square test or Fisher’s exact test will be used.
Multivariate analysis will be conducted using forward stepwise Cox regression analysis. Event-free survival curves will be constructed using the Kaplan-Meier method. Variables will be considered potential risk predictors in the multivariate model if they demonstrate a statistically significant association in the univariate analysis or show a trend toward significance. All statistical analyses will be conducted using Stata 16.1 (StataCorp, United States).
Ethical considerations
This study was conducted in full compliance with the principles outlined in the Declaration of Helsinki and with the International Council for Harmonization (ICH) Good Clinical Practice guidelines, including the most recent ICH E6 (R3) update. Before enrollment, patients or their legal representatives must be fully informed about the nature of the study and must provide written informed consent. The study protocol was approved by the Institutional Review Board at each participant center.
DISCUSSION
The LUDICO study will be a multicenter study to assess the safety, efficacy, and clinical outcomes of ELCA specifically in undilatable or uncrossable coronary artery lesions with lesion-specific endpoints and preferential use of intravascular imaging. We believe that this real-life approach will provide valuable insights into the 2 main clinical scenarios in which ELCA is currently used.
Three recent large registries confirmed ELCA to be a safe technique with an assumable rate of complications.20-22 However, these studies analyzed the overall procedural performance but failed to describe the lesion specific characteristics or intravascular imaging data. The findings of studies reporting balloon failure scenarios5,10-12,23,24 are summarized in figure 3. The LAVA multicenter registry set the main contemporary clinical indications for ELCA.12 This registry analysed ELCA use in 130 lesions and stratified them in 3 scenarios: uncrossable, undilatable and thrombotic. The LAVA and other studies analyzing ELCA has shown good performance of ELCA in balloon-failure, with lower rates of ELCA success in uncrossable vs undilatable lesions. However, one significant limitation is present in these studies: situations of balloonfailure include undilatable, uncrossable, or lesions with both components. In the routine clinical practice, these 2 situations are distinct; however, ELCA success has often been defined uniformly, potentially confounding the real efficacy of the device. Consequently, the LUDICO study aims to address this issue by specifically defining 2 endpoints based on the type of balloon failure, uncrossable or undilatable.
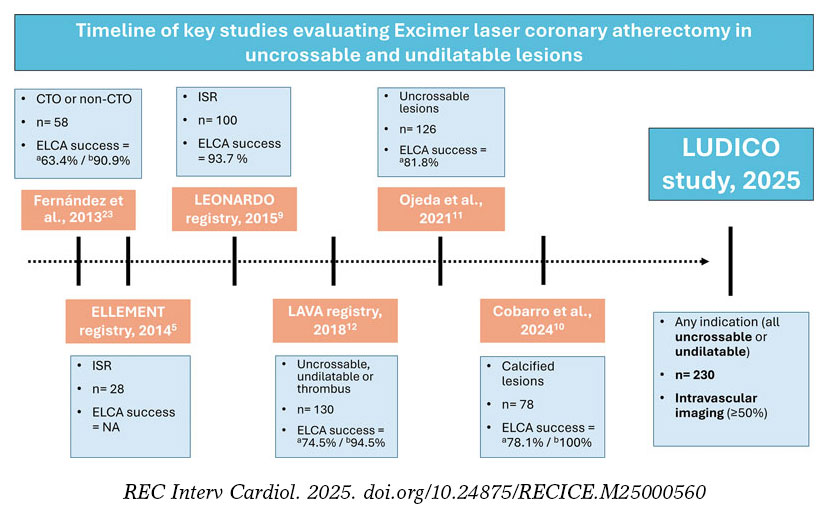
Figure 3. Timeline of key studies evaluating ELCA in uncrossable and undilatable lesions. CTO, chronic total coronary occlusion; ELCA, excimer laser coronary atherectomy; NA, not available; ISR, in-stent restenosis. a Uncrossable lesions. b Undilatable lesions.
Nonetheless, the definition of ELCA success in uncrossable lesions might be ambiguous in some cases. For instance, cases in which neither the ELCA catheter nor subsequent balloons are able to cross the lesion should not be considered procedurals failures if a microcatheter can subsequently cross and enable successful completion of the procedure using the RASER technique—a combination of ELCA and rotational atherectomy (RA). However, to simplify the endpoint, we have considered this situation a crossover to RA. In contrast, for undilatable lesions, the definition of ELCA success is less prone to interpretation; however, clearly defining what constitutes an undilatable lesion remains essential. This highlights the importance of a compliance test —that is, performing an initial balloon dilatation to objectively demonstrate that the lesion cannot be adequately expanded. Such a test is critical to identify lesions that are likely to benefit from plaque modification techniques, including ELCA. Arguably, the results of some randomized controlled trials in plaque modification devices (such as ECLIPSE25 using orbital atherectomy and ROLLERCOASTR7 using ELCA, intravascular lithotripsy and RA) may have been influenced by the absence of “compliance test”, potentially including coronary lesions in which plaque modification would not have been necessary after balloon testing, thereby reducing the differences across groups. Additionally, the recent CRATER trial showed that a total of 20.9% of patients in bailout RA group required crossover to RA because of balloon failure,26 which highlights the high frequency of this situation and underscores the importance of its prompt identification to select the most appropriate plaque modification technique such as ELCA.
RA is the most extensively studied strategy for managing uncrossable coronary lesions, supported by wide clinical experience and robust evidence.7,26,27 However, RA presents important limitations in specific scenarios where ELCA may offer clear advantages —such as in-stent restenosis or bifurcation lesions requiring side branch protection—given the risk of scaffold damage or distal embolization of debris.28 Orbital atherectomy, although less studied in uncrossable lesions,29,30 shares similar drawbacks due to its ablative mechanism. By contrast, ELCA is compatible with 6-Fr catheters, can be used over any standard guidewire, and has a less demanding learning curve.18 Of note, while RA demonstrates limited efficacy against deep calcium, ELCA can affect both superficial and deep calcification.4 Collectively, these features position ELCA as a uniquely valuable tool among plaque-modification techniques. Its capacity to safely treat in-stent restenosis, thrombotic lesions, uncrossable lesions, and bifurcations requiring side branch protection underscores advantages not readily attainable with RA or orbital atherectomy, thereby reinforcing ELCA as a superior alternative in selected complex PCI scenarios.
In conclusion, the use of intravascular imaging has been limited in most of the studies that have evaluated ELCA in balloon-failure, particularly those focused on uncrossable lesions. Additionally, none of these studies have described the findings of intravascular imaging before and after ELCA and identified potential predictors of success. In fact, the effect of ELCA in intravascular imaging remains an open question as there is a paucity of studies that have evaluated it and have been limited to in-stent restenosis.4 Therefore, one of the aims of the LUDICO study is to evaluate the effects of ELCA by intravascular imaging (preferably by OCT, due to its better spatial resolution) and identify potential predictors of ELCA success or failure and its effect on the coronary plaque. We hypothesize that recognizing potential predictors in intravascular imaging could help operators guide the procedures and identify the anatomical characteristics that best predict a favourable outcome with ELCA, thereby optimizing patient selection and procedural planning.
Limitations
First, this multicentre prospective study will be conducted in a single country, which may limit the generalizability of its findings to other settings. However, these high-volume centres, with wide experience in complex PCI comply with the international recommendations and their practice is comparable to other similar centres. Second, because of to the nonblinded study design, selection bias may have occurred, whereby certain lesions, such as extremely calcified or highly complex, were preferentially treated with alternative techniques or revascularization strategies. Additionally, there will not be a control group to assess the efficacy of the ELCA therapy vs other therapies. Finally, although intracoronary imaging will be highly recommended, we foresee that the baseline evaluation will be limited to just a few cases. In fact, by definition, uncrossable lesions will rarely have a baseline evaluation. Besides, in the event of the patient having kidney disease, OCT runs could be avoided, conducting to less OCT runs, or even to the absence of intravascular imaging.
CONCLUSIONS
The LUDICO study will be a multicenter, prospective study of ELCA therapy in uncrossable or undilatable coronary artery lesions with specific success definitions for each indication. The study aims to evaluate the safety and efficacy profile of ELCA and the clinical outcomes during the follow-up. The OCT evaluation will provide insights into the effect of ELCA in this subset of coronary lesions.
FUNDING
The LUDICO study was supported by a non-restricted grant from Biomenco.
ETHICAL CONSIDERATIONS
The study was conducted in full compliance with the principles outlined in the Declaration of Helsinki. Institutional Ethics Committee approval was obtained (institutional approval number: 5502), and all participants gave their written informed consent prior to enrolment. The confidentiality and anonymity of participants were strictly preserved throughout the study. Sex and gender considerations were addressed following the recommendations of the SAGER guidelines to ensure accurate and equitable reporting.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
Artificial intelligence assisted technologies were used exclusively to support language editing and improvement of style. No artificial intelligence tools were employed to generate, analyse, or interpret the data. The authors take full responsibility for the integrity, accuracy, and originality of the manuscript content.
AUTHORS’ CONTRIBUTIONS
A. Jurado-Román and J. Zubiaur contributed to the study equally and share first authorship. A. Jurado-Román is responsible of the study conception and design. J. Zubiaur, A. Jurado-Román, and M. Basile were involved in the draft manuscript preparation. All authors reviewed the results and approved the final version of the manuscript.
CONFLICTS OF INTEREST
R. Moreno is associate editor of REC: Interventional Cardiology; the journal’s editorial procedure to ensure impartial handling of the manuscript has been followed; moreover, he has received consulting fees and honoraria/speaker fees from Abbott vascular, Boston Scientific, Medtronic, Terumo, and Biotronik. A. Jurado-Román reported receiving consulting fees from Boston Scientific and Philips; honoraria/speaker fees from Abbott, Boston Scientific, Shockwave Medical, World Medica, and Philips; and serves as a proctor for Abbott, Boston Scientific, World Medica, and Philips. G. Galeote has received honoraria/speaker fees from Meril, Boston Scientific, Abbott SMT, and Biomenco. A. Gonzálvez-García has received honoraria from Abbott. J. Suárez de Lezo has received honoraria/ speaker fees from Abbott and Philips. F. Hidalgo has received honoraria/speaker fees from Philips. M. Basile reported receiving consulting fees and speaking fees from Iberhospitex. B. Garcia del Blanco disclosed his role as a proctor for Edwards Lifescienses and his participation on the Advisory Board of Iberhospitex. All other authors declared no conflicts of interest whatsoever.
WHAT IS KNOWN ABOUT THE TOPIC?
- ELCA has demonstrated its usefulness across several challenging lesion subsets, including in-stent restenosis, stent underexpansion, calcified plaques, saphenous vein graft disease, thrombotic lesions, bifurcations, and chronic total coronary occlusions.
- However, in real-world practice, its main indication remains balloon failure, particularly in lesions that are either uncrossable or undilatable.
- Despite this, most earlier studies applied a uniform definition of device success for these distinct scenarios, potentially missing clinically relevant nuances that may affect outcomes and guide treatment strategies.
WHAT DOES THIS STUDY ADD?
- The LUDICO study is designed as a multicenter investigation to evaluate the safety, efficacy, and clinical outcomes of ELCA specifically in undilatable or uncrossable coronary artery lesions, incorporating individualized endpoints for each subset and emphasizing the use of intravascular imaging.
- This real-world strategy is expected to yield meaningful insights into the 2 primary clinical situations in which ELCA is currently employed: uncrossable and undilatable coronary artery lesions.
REFERENCES
1. Choy DS. History of lasers in medicine. Thorac Cardiovasc Surg. 1988;36 Suppl 2:114–117.
2. Köster R, Kähler J, Brockhoff C, Münzel T, Meinertz T. Laser coronary angioplasty: history, present and future. Am J Cardiovasc Drugs. 2002;2:197–207.
3. Bilodeau L, Fretz EB, Taeymans Y, Koolen J, Taylor K, Hilton DJ. Novel use of a high-energy excimer laser catheter for calcified and complex coronary artery lesions. Catheter Cardiovasc Interv. 2004;62:155–161.
4. Lee T, Shlofmitz RA, Song L, et al. The effectiveness of excimer laser angioplasty to treat coronary in-stent restenosis with peri-stent calcium as assessed by optical coherence tomography. EuroIntervention. 2019;15:e279–288.
5. Latib A, Takagi K, Chizzola G, et al. Excimer Laser LEsion Modification to Expand Non-dilatable sTents: The ELLEMENT Registry. Cardiovasc Revasc Med. 2014;15:8–12.
6. Dörr M, Vogelgesang D, Hummel A, et al. Excimer laser thrombus elimination for prevention of distal embolization and no-reflow in patients with acute ST elevation myocardial infarction: results from the randomized LaserAMI study. Int J Cardiol. 2007;116:20–26.
7. Jurado-Román A, Gómez MA, Rivero-Santana B, et al. Rotational Atherectomy, Lithotripsy, or Laser for Calcified Coronary Stenosis. JACC: Cardiovasc Interv. 2025;18:606–618.
8. Giugliano GR, Falcone MW, Mego D, et al. A prospective multicenter registry of laser therapy for degenerated saphenous vein graft stenosis: the COronary graft Results following Atherectomy with Laser (CORAL) trial. Cardiovasc Revasc Med. 2012;13:84–89.
9. Ambrosini V, Sorropago G, Laurenzano E, et al. Early outcome of high energy Laser (Excimer) facilitated coronary angioplasty ON hARD and complex calcified and balloOn-resistant coronary lesions: LEONARDO Study. Cardiovasc Revasc Med. 2015;16:141–146.
10. Cobarro L, Jurado-Román A, Tébar-Márquez D, et al. Excimer laser coronary atherectomy in severely calcified lesions: time to bust the myth. REC Interv Cardiol. 2023;6:33–40.
11. Ojeda S, Azzalini L, Suárez de Lezo J, et al. Excimer laser coronary atherectomy for uncrossable coronary lesions. A multicenter registry. Catheter Cardiovasc Interv. 2021;98:1241–1249.
12. Karacsonyi M, Armstrong EJ, Huu Tam D, et al. Contemporary Use of Laser During Percutaneous Coronary Interventions: Insights from the Laser Veterans Affairs (LAVA) Multicenter Registry. J Invasive Cardiol. 2018;30:195–201.
13. Tomasello SD, Rochira C, Mazzapicchi A, et al. Clinical Outcomes of Percutaneous Coronary Intervention Using Excimer Laser Coronary Atherectomy for Complex Coronary Lesions: The ACCELERATE Registry. Catheter Cardiovasc Interv. 2025;106:1630–1638.
14. Basile M, Gómez-Menchero A, Rivero-Santana B, et al. Rotational Atherectomy, Lithotripsy, or Laser for Calcified Coronary Stenosis: One-Year Outcomes From the ROLLER COASTER-EPIC22 Trial. Cath Cardiovasc Interv. 2025;106:702–710.
15. Vrints C, Felicita Andreotti F, Koskinas KC, et al. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024;45:3415–3537.
16. Cuschieri S. The STROBE guidelines. Saudi J Anaesth. 2019;13(Suppl 1):S31–S34.
17. Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J Acute Cardiovasc Care. 2024;13:55–161.
18. Rawlins J, Din JN, Talwar S, O’Kane P. Coronary Intervention with the Excimer Laser: Review of the Technology and Outcome Data. Interv Cardiol. 2016;11:27–32.
19. Nagaraja V, Kalra A, Puri R. When to use intravascular ultrasound or optical coherence tomography during percutaneous coronary intervention? Cardiovasc Diag Ther. 2020;10:1429444–1421444.
20. Sintek M, Coverstone E, Bach R, et al. Excimer Laser Coronary Angioplasty in Coronary Lesions: Use and Safety From the NCDR/CATH PCI Registry. Circ Cardiovasc Interv. 2021;14:e010061.
21. Protty MB, Gallagher S, Farooq V, et al. Combined use of rotational and excimer lASER coronary atherectomy (RASER) during complex coronary angioplasty—An analysis of cases (2006–2016) from the British Cardiovascular Intervention Society database. Cath Cardiovasc Interv. 2021;97:E911–E918.
22. Hinton J, Tuffs C, Varma R, et al. An analysis of long-term clinical outcome following the use of excimer laser coronary atherectomy in a large UK PCI center. Catheter Cardiovasc Interv. 2024;104:27–33.
23. Fernandez JP, Hobson AR, McKenzie D, et al. Beyond the balloon: excimer coronary laser atherectomy used alone or in combination with rotational atherectomy in the treatment of chronic total occlusions, non-crossable and non-expansible coronary lesions. EuroIntervention. 2013;9:243–250.
24. Ambrosini V, Sorropago G, Laurenzano E, et al. Early outcome of high energy Laser (Excimer) facilitated coronary angioplasty ON hARD and complex calcified and balloOn-resistant coronary lesions: LEONARDO Study. Cardiovasc Revasc Med. 2015;16:141–146.
25. Kirtane AJ, Généreux P, Lewis B, et al. Orbital atherectomy versus balloon angioplasty before drug-eluting stent implantation in severely calcified lesions eligible for both treatment strategies (ECLIPSE): a multicentre, open-label, randomised trial. Lancet. 2025;405:1240–1251.
26. Galeote G, Zubiaur J, Jurado-Román A, et al. Coronary Rotational Atherectomy Elective Versus Bailout in Patients With Severely Calcified Lesions and Chronic Renal Failure (CRATER) Trial. Catheter Cardiovasc Interv. 2025;106:1702–1712.
27. Abdel-Wahab M, Toelg R, Byrne RA, et al. High-Speed Rotational Atherectomy Versus Modified Balloons Prior to Drug-Eluting Stent Implantation in Severely Calcified Coronary Lesions. Circ Cardiovasc Interv. 2018;11:e007415.
28. Rivero-Santana B, Galán C, Pérez-Martínez C, et al. ELLIS Study: Comparative Analysis of Excimer Laser Coronary Angioplasty and Intravascular Lithotripsy on Drug-Eluting Stent as Assessed by Scanning Electron Microscopy. Circ Cardiovasc Interv. 2024;17:e014505.
29. Helal A, Ehtisham J, Shaukat N. Overcoming Uncrossable Calcified RCA Using Orbital Atherectomy After Failure of Rotational Atherectomy. Catheter Cardiovasc Interv. 2025;105:1265–1268.
30. Bayón J, Mori-Junco RA, Jusková M, Abellas-Sequeiros M, González-Juanatey C. Feasibility and safety of orbital atherectomy in uncrossable lesions. REC: Interv Cardiol. 2025;7:269–271.
31. Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation. 2007;115:2344–2351.
32. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Eur Heart J. 2012;33:2551–2567.
33. Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium. Circulation. 2011;123:2736–2747.
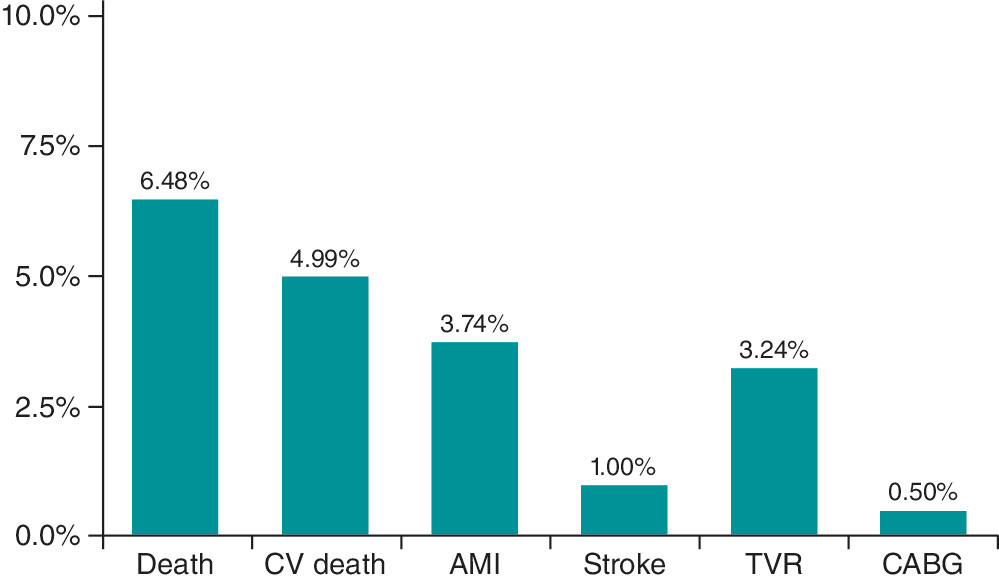
ABSTRACT
Introduction and objectives: Manual thrombectomy (MT) during primary percutaneous coronary intervention (PCI) aims to reduce thrombus burden. Our study evaluates the outcomes and predictors of successful MT.
Methods: The Hunted registry is a retrospective, single-center cohort study including patients who underwent MT during PCI using the Hunter catheter from July 2020 through February 2022. MT success was defined as an angiographic reduction to a Thrombolysis in Myocardial Infarction (TIMI) thrombus grade of ≤ 2, with clinical follow-up for major adverse cardiovascular events.
Results: Among 750 patients with acute myocardial infarction who underwent PCI, 401 (53%) received MT. The mean age of treated patients was 62 years (80% men). MT was effective in 327 patients (81.55%). Predictors of successful MT included larger vessel diameter (P < .001), high thrombus burden (TIMI grade ≥ 4 flow; P < .001), and non-circumflex target vessels (P < .001). Device-related complications occurred in 17 patients (4.3%). At follow-up, major adverse events occurred in 8.98% of patients at 1 year and in 9.97% at 2 years.
Conclusions: In patients with ST-segment elevation myocardial infarction undergoing PCI, MT with the Hunter catheter in selected cases with high thrombus burden (TIMI grade ≥ 4 flow), non-circumflex target vessels, and vessel diameters > 2.5 mm, is a safe and effective technique with a low rate of complications.
Keywords: ST-segment elevation myocardial infarction. Percutaneous coronary intervention. Manual thrombectomy. Thrombus burden.
RESUMEN
Introducción y objetivos: La trombectomía manual (TM) en la intervención coronaria percutánea primaria (ICPp) intenta reducir la carga trombótica. Este estudio evalúa los resultados y los factores predictores de éxito de la TM.
Métodos: El registro Hunted es un estudio de cohortes retrospectivo, unicéntrico, de pacientes tratados con TM en ICPp utilizando el catéter Hunter, desde julio de 2020 hasta febrero de 2022. El éxito de la TM se definió como una disminución angiográfica a grado ≤ 2 en la escala Thrombolysis in Myocardial Infarction (TIMI), con seguimiento clínico de eventos cardiovasculares adversos mayores.
Resultados: De los 750 pacientes con infarto agudo de miocardio tratados con ICPp, en 401 (53%) se realizó TM. Los pacientes tratados tenían una edad media de 62 años y el 80% eran varones. La TM fue efectiva en 327 (81,55%) pacientes. Los predictores de TM efectiva fueron un mayor diámetro del vaso (p < 0,001), una alta carga de trombo (TIMI ≥ 4; p < 0,001) y un vaso diferente de la circunfleja (p < 0,001). Se presentaron complicaciones relacionadas con el dispositivo en 17 pacientes (4,3%). En el seguimiento, el 8,98% presentaron eventos mayores a 1 año y el 9,97% a 2 años.
Conclusiones: En los pacientes con infarto de miocardio con elevación del segmento ST sometidos a ICPp, la estrategia de TM con catéter Hunter, en casos seleccionados con alta carga trombótica (escala TIMI ≥ 4), otros vasos que no fueran la circunfleja y diámetros > 2,5 mm, es una técnica eficaz y segura con una baja tasa de complicaciones.
Palabras clave: Infarto de miocardio con elevación del segmento ST. Intervención coronaria percutánea primaria. Trombectomía manual. Carga trombótica.
Abbreviations
MACE: major adverse cardiovascular events. MT: manual thrombectomy. PCI: primary coronary intervention. STEMI: ST-segment elevation myocardial infarction. TIMI: Thrombolysis in Myocardial Infarction.
INTRODUCTION
In patients with ST-segment elevation myocardial infarction (STEMI), the treatment of choice is percutaneous coronary intervention (PCI) performed within the appropriate time window and by experienced operators. PCI has been shown to reduce mortality, reinfarction, and stroke compared with fibrinolysis.1 Among other factors, this benefit may be attributed to greater epicardial reperfusion and higher TIMI (Thrombolysis in Myocardial Infarction) flow grades and myocardial blush grades achieved with PCI in the culprit artery, all of which are known to influence survival.2,3
PCI have distinctive characteristics, including the presence of a high thrombus burden and performance in patients in a markedly thrombogenic state. To reduce the local thrombus burden in the culprit artery, manual thrombectomy (MT) has been widely used during PCI to reduce thrombus load, prevent distal embolization, and improve final myocardial perfusion.3,4 Despite its initial widespread adoption, routine use of MT in all patients undergoing PCI is no longer recommended, as randomized clinical trials have not demonstrated consistent clinical benefit.3-7
MT should be reserved for patients in whom it is most likely to provide benefit. To optimize the efficacy of PCI, the American8 and European9 clinical practice guidelines recommend MT in high-risk patients with a moderate-to-high thrombus burden who present with short ischemia times. Currently, however, there are no clearly defined criteria to precisely identify patients or thrombotic lesions that would derive the greatest benefit from MT.
The aim of our study was to evaluate the results of MT performed with the Hunter catheter (IHT–Iberhospitex SA, Barcelona, Spain), which has a high extraction capacity, in selected patients with STEMI undergoing PCI, and analyze the angiographic patterns associated with successful MT in our center.
METHODS
Study design and population
The Hunted registry is a single-center, observational, retrospective study. We included all patients diagnosed with STEMI who underwent PCI and in whom MT was performed using the Hunter thrombus aspiration catheter. This device was the first-choice catheter for MT in our center during the study period. The decision to perform MT was always left to the discretion of the operator performing the PCI, following homogeneous criteria among operators, subjectively based on angiographical evidence of a large angiographically visible thrombus. MT was not recommended in coronary vessels with a diameter < 2 mm or for the extraction of chronic thrombi or atherosclerotic plaques. The study period ranged from July 2020 through February 2022. Patients in whom MT was performed using a catheter other than the Hunter device were excluded.
The primary objective of the study was to evaluate the success of thrombus aspiration during PCI in patients with STEMI. Effective MT was defined as an angiographical reduction in thrombus burden, achieving a TIMI thrombus grade ≤ 2 (thrombus dimension < 50% of the vessel diameter). Moreover, angiographic factors associated with effective MT were assessed.
Secondary objectives included describing the clinical and angiographic characteristics of the patients and evaluating major adverse cardiovascular events (MACE) during hospitalization and follow-up.
MACE were defined as a composite endpoint of cardiovascular and noncardiovascular death, stroke, and acute myocardial infarction. Two follow-up time points were established at 1 and 2 years after PCI. Total ischemia time was defined as the interval, in minutes, between symptom onset and reperfusion, defined as passage of the intracoronary guidewire, in accordance with clinical practice guidelines.
Thrombus burden was graded according to the TIMI thrombus scale,10 which includes 5 grades: grade 1, possible thrombus; grade 2, thrombus dimension < 50% of the vessel diameter; grade 3, thrombus dimension 0.5 to 2.0 vessel diameters; grade 4, thrombus dimension > 2.0 vessel diameters; and grade 5, total vessel occlusion by thrombus. Grades 4 and 5 were considered high thrombus burden.
Successful PCI was defined as achievement of TIMI grade 3 flow with residual percent diameter stenosis < 20%, without device-related complications or intraoperative MACE. For study purposes, patients were categorized into 2 groups according to whether MT was effective or not. Furthermore, these groups were compared to identify angiographic parameters that could predict MT success.
Data for the variables included in the Hunted registry were collected using a dedicated electronic case report form. Retrospective angiographic analysis was performed exclusively by 3 operators. All measures were taken to ensure confidentiality and protection of patient health record information. The study protocol fully complied with international recommendations for clinical research outlined in the Declaration of Helsinki and was approved by the hospital Ethics and Research Committee.
Characteristics of the Hunter device and aspiration technique
The Hunter thrombus aspiration catheter is a 140 cm rapid-exchange aspiration catheter compatible with a 6-Fr guiding catheter. Its tip has a slightly conical, low-profile, atraumatic design. The effective distal aspiration area measures 0.95 mm2, and it can aspirate up to 1.92 mL per second, one of the highest capacities available. The distal segment is coated with a hydrophilic surface to facilitate device navigability.
The standard thrombectomy technique used in our center consisted of advancing the Hunter catheter to a segment proximal to the culprit lesion. Aspiration was always initiated proximal to the culprit lesion. The catheter was then slowly advanced across the lesion under continuous aspiration to reach the distal segment, while continuous filling of the syringe was observed. If filling stopped, the catheter was withdrawn until aspiration resumed or removed completely if aspiration could not be reestablished. Continuous aspiration until removal from the guiding catheter was mandatory, as was thorough subsequent flushing of the guiding catheter, to prevent embolization of residual thrombotic material.
All retrieved material from the catheter and aspiration syringe was subsequently filtered using the filters provided with the device packaging. The procedure was repeated as many times as deemed necessary by the operator until the desired reduction in thrombus burden was achieved.
Statistical analysis
Qualitative variables are expressed as frequencies and percentages, and the quantitative ones as mean and standard deviation when normally distributed, and as median and interquartile range when distribution was nonnormal.
Qualitative variables were compared using the chi-square test, with odds ratios (OR) and 95% confidence intervals (95%CI) calculated. Quantitative ones were compared using the Student t test or nonparametric tests, as appropriate.
In univariate analysis, each variable was individually assessed for its association with effective MT. Variables showing a statistically significant association were included in the multivariate analysis. Multiple regression models were used to control for potential confounders and determine the independent effect of each variable on the outcome.
Survival curves were analyzed using the Kaplan–Meier method, and survival-related parameters were evaluated using Cox proportional hazards analysis. A 2-sided P value < .05 was considered statistically significant.
Statistical analyses were performed using STATA version 15 (StataCorp, United States).
RESULTS
During the study period, a total of 750 PCI were performed in patients diagnosed with STEMI. MT using the Hunter catheter was performed in 401 patients (53.47%). The clinical characteristics of the patients, STEMI features, and PCI are shown in table 1.
Table 1. Clinical characteristics of patients and procedural variables
| Clinical characteristics | (n = 401) |
|---|---|
| Age, years | 62.38 ± 12.43 |
| Male sex | 319 (80) |
| Current/former smoker | 163 (40.65) / 35 (8.73) |
| Hypertension | 207 (51.62) |
| Dyslipidemia | 186 (46.38) |
| Diabetes mellitus | 86 (21.45) |
| Kidney failure | 7 (1.75) |
| Previous stroke | 16 (3.99) |
| Peripheral vascular disease | 8 (2.00) |
| Previous AMI | 48 (11.97) |
| Previous PCI | 50 (12.47) |
| Prior CABG | 5 (1.25) |
| Infarct location | |
| Anterior | 166 (41.50) |
| Inferior | 207 (51.75) |
| Lateral | 27 (6.75) |
| Killip-Kimball classification | |
| I | 338 (84.71) |
| II | 18 (4.51) |
| III | 8 (2.01) |
| IV | 35 (8.77) |
| Procedural variables | |
| Radial access | 385 (96.01) |
| No. of diseased vessels* | |
| 1 | 233 (58.10) |
| 2 | 111 (27.68) |
| 3 | 57 (14.21) |
| Infarct-related artery | |
| Right coronary artery | 183 (45.64) |
| Left anterior descending coronary artery | 166 (41.40) |
| Left circumflex artery | 48 (11.97) |
| Venous graft | 1 (0.25) |
| Left main coronary artery | 3 (0.75) |
| No. of stents implanted | |
| 0 | 34 (8.47) |
| 1 | 288 (71.82) |
| 2 | 60 (14.96) |
| 3 | 19 (4.74) |
| Drug-eluting stent (n = 367) | 362 (98.64) |
| Total ischemic time | |
| < 90 min | 43 (10.72) |
| 91-180 min | 167 (41.65) |
| 181-270 min | 82 (20.45) |
| 271-360 min | 42 (10.47) |
| > 360 min | 67 (16.71) |
|
AMI, acute myocardial infarction; CABG, coronary artery bypass grafting; PCI, percutaneous coronary intervention. |
|
Angiographic analysis of the culprit lesion and flow in the infarct-related artery is shown in table 2. Initial TIMI grade flow in the infarct-related artery, prior to intracoronary guidewire passage was 0 in 83% of cases. A high thrombus burden was observed in 87.5% of patients, corresponding to TIMI thrombus grades 4 or 5; 53.4% had grade 5 and 34.2% had grade 4. Only 50 patients (12.5%) had a TIMI grade < 4 flow, defined as a low thrombus burden.
Table 2. Angiographic analysis of patients treated with percutaneous coronary intervention and manual thrombectomy
| Angiographic variables | |
|---|---|
| Vessel diameter | 3.25 [3.00-3.50] |
| 2.0-2.5 mm | 61 (15.21) |
| 2.6-3.0 mm | 122 (30.42) |
| 3.1-3.5 mm | 124 (30.92) |
| 3.6-4.0 mm | 66 (16.46) |
| > 4.0 mm | 28 (6.98) |
| Lesion length, mm | 16 [15-20] |
| AHA/ACC lesion type | |
| B1 | 60 (14.96) |
| B2 | 161 (40.15) |
| C | 180 (44.89) |
| Thrombus burden grade (TIMI) | |
| 1 | 1 (0.25) |
| 2 | 5 (1.25) |
| 3 | 44 (10.97) |
| 4 | 137 (34.16) |
| 5 | 214 (53.37) |
| Pre-PCI IRA TIMI flow grade | |
| 0 | 332 (82.79) |
| 1 | 18 (4.49) |
| 2 | 24 (5.98) |
| 3 | 27 (6.74) |
| Post-PCI IRA TIMI flow grade | |
| 0 | 2 (0.50); |
| 1 | 3 (0.75); |
| 2 | 10 (2.49); |
| 3 | 386 (96.26) |
|
AHA/ACC, American Heart Association/American College of Cardiology; IRA, infarct-related artery; PCI, percutaneous coronary intervention; TIMI, Thrombolysis in Myocardial Infarction. |
|
According to the predefined criteria, effective MT was achieved in 327 of 401 patients (81.5%). Thrombectomy was considered ineffective in the 6 patients who had initial TIMI thrombus grades 1 and 2. Final post-PCI coronary flow was TIMI grade < 3 flow in 15 patients (3.74%). Overall, the PCI was successful in approximately 97% of cases. Device-related complications were recorded in 17 patients (4.24%): severe arrhythmias (ventricular fibrillation or ventricular tachycardia) occurring during reperfusion in 10 patients; severe no-reflow due to distal thrombus migration that could not be successfully treated in 4 patients; and coronary dissection after passage of the MT catheter, which was successfully treated with stenting in 3 patients. There were no cases of perioperative stroke due to migration of aspirated thrombus.
Comparative analysis of angiographic factors and ischemia time between patients with effective and noneffective MT is shown in table 3. MT was effective more frequently in patients with culprit coronary vessels > 3 mm in diameter (112 [34%] vs 12 mm [16%]; P < .001) and in those with a TIMI grade ≥ 4 thrombus burden (297 [91%] vs 54 [73%]; P < .001). Among the 61 patients with vessels < 2.5 mm, MT was ineffective in 36 (59.01%) vs 38 of 340 patients (11.2%) with vessels > 2.5 mm (P < .001). There were no statistically significant differences in ischemia time in relation to MT success.
Table 3. Comparison of angiographic and procedural characteristics between patients with effective and noneffective manual thrombectomy
| Procedural variables | Effective MT (n = 327) | Noneffective MT (n = 74) | P |
|---|---|---|---|
| Infarct-related artery | .008 | ||
| Right coronary artery | 153 (46.79) | 30 (40.54) | |
| Left anterior descending coronary artery | 140 (42.81) | 26 (35.14) | |
| Left circumflex artery | 30 (9.17) | 18 (24.32) | |
| Saphenous vein graft | 1 (0.31) | – | |
| Left main coronary artery | 3 (0.92) | – | |
| AHA/ACC classification of the culprit lesion | .004 | ||
| B1 | 51 (15.60) | 9 (12.16) | |
| B2 | 142 (43.42) | 19 (25.68) | |
| C | 134 (40.98) | 46 (62.16) | |
| Reference diameter of the culprit lesion | < .001 | ||
| 2.0 mm-2.5 mm | 25 (7.65) | 36 (48.69) | |
| 2.6 mm-3.0 mm | 101 (30.89) | 21 (28.38) | |
| 3.1 mm-3.5 mm | 112 (34.25) | 12 (16.22) | |
| 3.6 mm-4.0 mm | 64 (19.57) | 2 (2.70) | |
| > 4.0 mm | 25 (7.64) | 3 (4.10) | |
| Thrombus burden grade (TIMI) | < .001 | ||
| Low thrombus burden (TIMI < 4) | 30 (9.18) | 20 (27.03) | |
| High thrombus burden (TIMI ≥ 4) | 297 (90.82) | 54 (72.97) | |
| Pre-PCI TIMI grade flow | .031 | ||
| TIMI grade 0-1 flow | 291 (88.99) | 59 (79.73) | |
| TIMI grade 2-3 flow | 36 (11.01) | 15 (20.27) | |
| Post-PCI TIMI grade flow | .61 | ||
| TIMI grade 0-1 flow | 2 (0.61) | 3 (4.05) | |
| TIMI grade 2 flow | 8 (2.45) | 1 (1.35) | |
| TIMI grade 3 flow | 317 (96.94) | 70 (94.59) | |
| Time from symptom onset to reperfusion | .79 | ||
| ≤ 90 min | 37 (11.31) | 6 (8.11) | |
| 91-180 min | 139 (42.51) | 28 (37.84) | |
| 181-270 min | 68 (20.80) | 14 (18.92) | |
| 271-360 min | 33 (10.09) | 9 (12.16) | |
| > 360 min | 50 (15.29) | 17 (22.97) | |
| Final procedural success | 317 (96.94) | 70 (94.59) | .61 |
|
AHA/ACC, American Heart Association/American College of Cardiology; MT, manual thrombectomy; PCI, percutaneous coronary intervention; TIMI, Thrombolysis in Myocardial Infarction. |
|||
The 1- and 2-year follow-up was completed in 100% of included patients. MACE occurred in 32 patients (7.98%) at 30 days, 36 patients (8.98%) at 1 year, and 40 patients (9.97%) at 2 years (table 4). Kaplan–Meier curves for event-free survival during follow-up and cardiovascular death according to effective vs noneffective MT are shown in figure 1 and figure 2, respectively. Individual components of MACE at 1 year are shown in figure 3.
Table 4. Incidence rate of the composite endpoint of major adverse cardiovascular events during follow-up
| Cardiovascular events at follow-up | n (%) |
|---|---|
| At 30 days | 32 (7.98) |
| At 1 year | 36 (8.98) |
| At 2 years | 40 (9.97) |
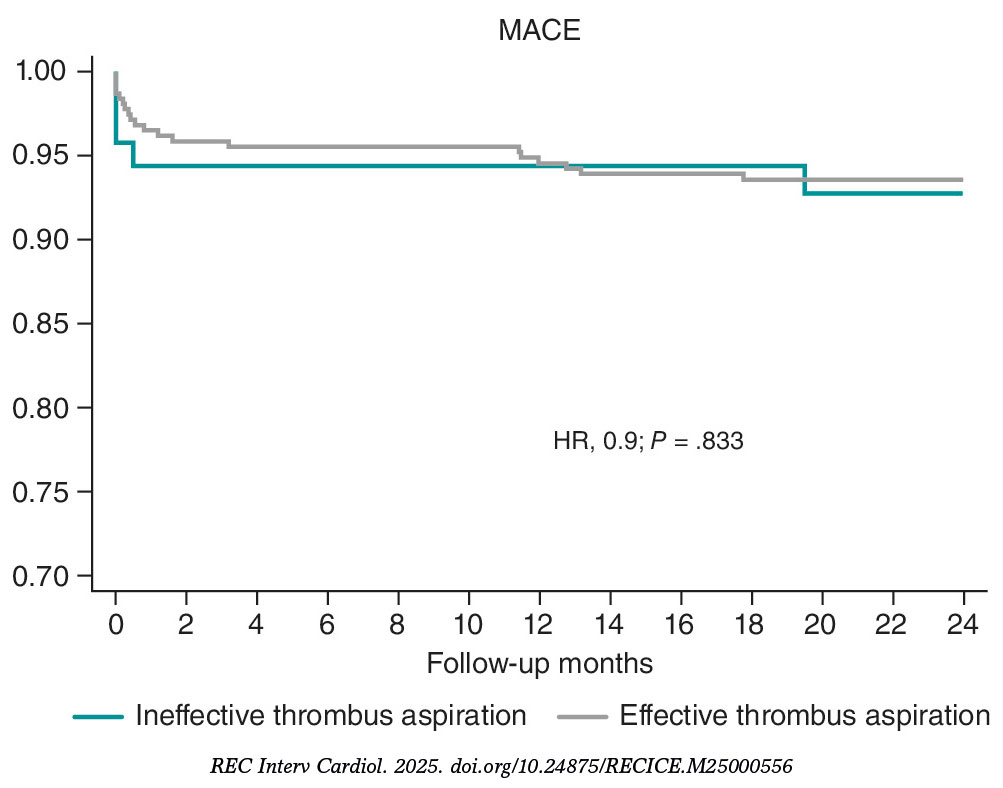
Figure 1. Kaplan–Meier curves for survival free from major adverse cardiovascular events (MACE). HR, hazard ratio.
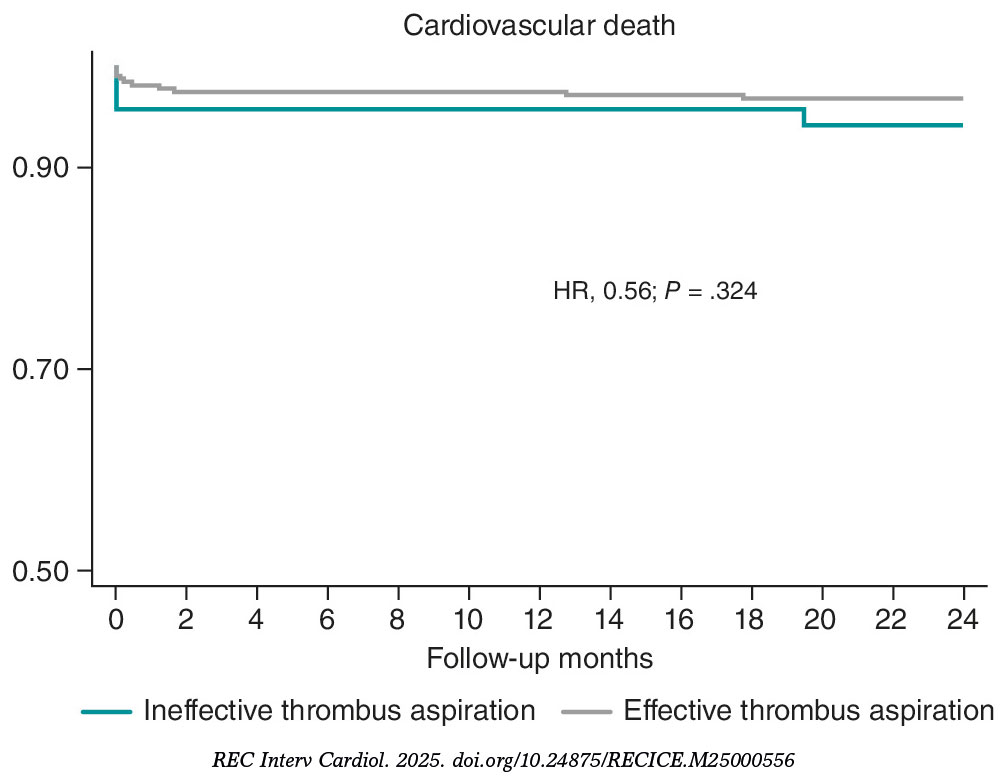
Figure 2. Kaplan–Meier survival curves for cardiovascular death. HR, hazard ratio.
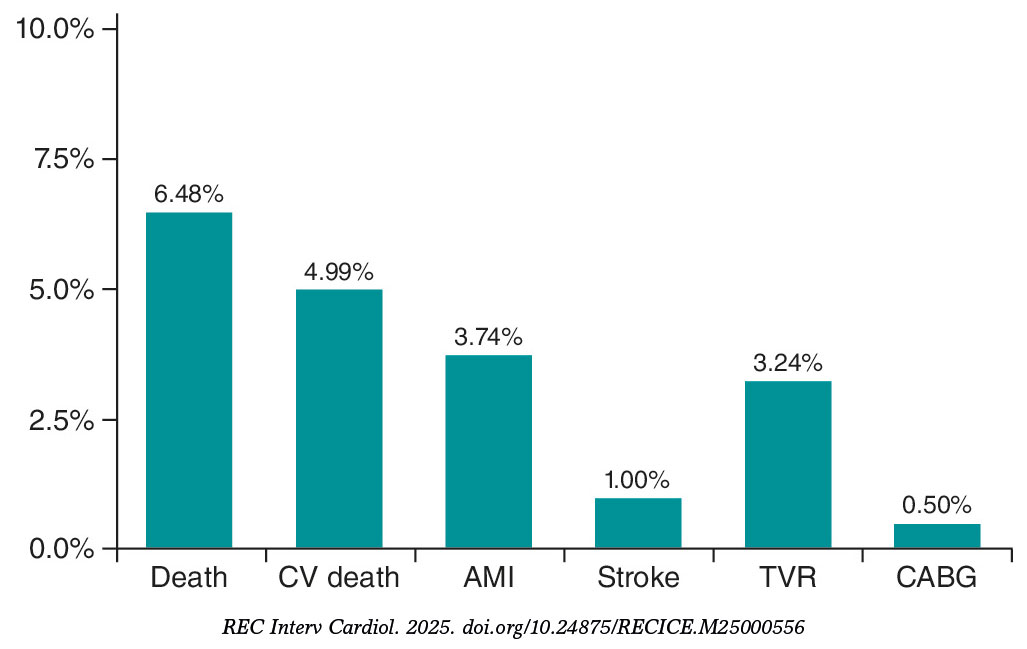
Figure 3. Individual components of major adverse cardiovascular events at the 1-year follow-up. AMI, acute myocardial infarction; CABG, coronary artery bypass grafting; CV, cardiovascular; TVR, target vessel revascularization.
DISCUSSION
In selected patients, MT using the Hunter catheter is a safe and effective strategy to reduce angiographically assessed thrombus burden during PCI.
Current clinical practice guidelines do not recommend routine MT during PCI but suggest considering it in patients with a high thrombus burden, based on individual assessment and operator experience.8,9 In our series, MT was performed in 53.5% of patients with STEMI treated with PCI, a higher proportion than reported in other countries.11-13 Only 12% of patients undergoing MT did not have a TIMI grade 4–5 thrombus burden on angiographic analysis.
In this selected population with high thrombus burden, 88% had TIMI grade ≥ 4 flow, which is similar to the 79% observed in the TOTAL trial,14 with favorable results in both cases. In contrast, only 33% of patients from the TASTE trial7 had a high thrombus burden.
A high thrombus burden appears to be a key determinant of achieving effective MT and may be associated with better clinical outcomes. In our cohort, although effective MT was achieved in 82% of cases, it was not significantly correlated with final procedural success (97% vs 95%; P = .67), likely due to the small sample size of the 2 groups. MT efficacy was higher in vessels with high thrombus burdens (TIMI grade ≥ 4 flow; P < .001), which is consistent with a meta-analysis showing less cardiovascular death in patients with STEMI undergoing PCI with MT in the high thrombus burden subgroup vs PCI alone (2.5% vs 3.2%; hazard ratio [HR], 0.81; 95%CI, 0.65–0.98; P = .03).15 These findings reinforce the concept that appropriate patient selection is crucial to benefit from MT. Moreover, the same meta-analysis reported a higher risk of stroke (0.9% vs 0.5% in the PCI-alone group),15 a complication that may be related to the TM technique used.
Strict adherence to proper technique is essential to minimize complications and maximize success. In our series, emphasis was placed on following a standardized and rigorous technique, as described in the Methods section, resulting in a low complication rate (4.3%). Many of these complications were not directly related to MT per se but rather to reperfusion, such as ventricular arrhythmias. MT-related stroke is a potential complication; in the TOTAL trial,16 the stroke rate was 0.7%, twice that observed in the PCI-alone group, whereas in the large real-world SCAAR registry, there was no increase in the incidence rate of stroke across the groups,17 which are findings more consistent with our results and possibly related to differences in MT technique.
To identify angiographic predictors of MT success, we compared the characteristics of patients with effective and noneffective MT. The former had significantly larger culprit vessel diameters; 48% of patients with noneffective MT had vessels measuring 2.5 mm. Although MT is generally discouraged in vessels < 2 mm, larger vessels may harbor greater thrombus burden and thus derive greater benefit from MT with the Hunter catheter, which has demonstrated higher in vitro aspiration capacity compared with other devices. Therefore, vessel size is a critical differentiating factor: in vessels < 2.5 mm, MT was ineffective in 59% of cases, a significantly higher proportion than the 11.2% of noneffective MT observed in larger vessels. The other major difference between groups was thrombus burden, as effective MT was achieved more frequently in patients with higher thrombus loads (TIMI grade ≥ 3 flow).15 Furthermore, this factor represents a major difference among randomized clinical trials, in which the proportion of patients with high thrombus burden varied substantially.15 More complex lesions, such as American Heart Association/American College of Cardiology type C lesions, those associated with calcification in addition to thrombus, long lesions, and left circumflex artery lesions were associated with higher rates of noneffective MT. These differences should be considered when selecting appropriate candidates for MT with the Hunter catheter, favoring patients with vessel diameters > 2.5 mm, abundant thrombus burden (TIMI grade ≥ 4 flow), and culprit arteries other than the left circumflex one.
Studies have shown that total ischemia time, which we believe may determine differences in thrombus composition,18 may influence the efficacy of thrombus aspiration.19 In our series, there were no differences between the effective and noneffective MT groups with respect to infarction duration.
When assessing whether effective MT impacted the outcome of the PCI, slightly different procedural success rates were observed: 97% for effective MT vs 95% for noneffective MT (P = .61). Statistical significance was not reached, possibly due to the small sample size. Only 4 patients experienced no-reflow that could not be resolved, with no differences across groups and without demonstrating that MT could prevent distal embolization, as suggested in former studies.17-19
Short- and long-term clinical outcomes in patients with STEMI who required MT were favorable, with a low 1-year cardiovascular death rate of 3.5%, comparable to that reported in randomized clinical trials. In the TASTE trial,7 the 30-day mortality rate was 2.4% in the MT group and 2.9% in the PCI-alone group (HR, 0.84; 95%CI, 0.70–1.01; P = .06). In the TAPAS trial,20 the 30-day all-cause mortality rate was 2.1% in the MT group vs 4.0% in the conventional PCI group, reaching statistical significance at the 1-year follow-up (P = .07). Large registries have reported mortality rates similar to those observed in our series, with 2.8% vs 3.0% in the Swedish registry21 and comparable findings in the Japanese registry.22 The overall mortality rate observed in a meta-analysis with aggregated data from published MT studies was 3.7%.15 When selecting patients with a high thrombus burden (TIMI grade ≥ 3 flow in the meta-analysis subgroup), the cardiovascular death rate was 2.5% (170 of 6872 patients) in the MT group vs 3.1% (205 of 6599 patients) in the PCI-alone group (HR, 0.8; 95%CI, 0.65–0.98; P = .03).15 Proper selection of this subgroup of patients with a high thrombus burden is, therefore, crucial to maximize the therapeutic benefit.
Limitations
As a single-center, observational, retrospective registry, this study has inherent limitations related to its design. First, because it reflects the experience of a single center—albeit with more than 15 years of experience in PCI—operator homogeneity may limit extrapolation of the results. The decision to perform MT was always left to the discretion of the operator, and no control group without MT was available for patient comparison. Because of the retrospective design of the analysis, we could not determine the cause of ineffective MT in all patients, which is why this variable could not be included in the analysis. This study should not be interpreted as an evaluation of thrombus aspiration in general, but rather as an assessment of outcomes in a selected population treated with the Hunter device; these selection criteria represent the primary contribution of this work to current scientific knowledge. The study did not incorporate systematic criteria to address sex- and gender-related variables during methodological development or result analysis. Although angiographic analysis was not performed by an independent core laboratory, it was conducted by 3 experienced analysts. In this analysis, MT success, procedural success, and baseline thrombus burden were defined using the TIMI scale.
CONCLUSIONS
In patients with STEMI undergoing PCI, selective use of MT with the Hunter catheter in cases with high thrombus burden (TIMI grade ≥ 4 flow), non-circumflex culprit vessels, and vessel diameters > 2.5 mm is a safe and effective strategy associated with a low complication rate. Further studies are needed to assess the impact of this strategy on PCI outcomes, MACE, and stroke.
FUNDING
This project was supported by IHT-Iberhospitex S.A. (Lliçà de Vall, Barcelona, Spain). As sponsor, the company collaborated in the study design but had no role in data collection, analysis, or interpretation. Manuscript preparation and the decision to submit for publication were entirely independent of the sponsor and performed by the research team.
ETHICAL CONSIDERATIONS
The study was approved by Hospital Universitari Germans Trias i Pujol Ethics Committee (Barcelona, Spain) (CEIC code: PI-22-281) and conducted in full compliance with the principles outlined in the Declaration of Helsinki. SAGER guidelines were not applied to address gender bias.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence tools were used in the preparation of this manuscript.
AUTHORS’ CONTRIBUTIONS
D.G. Borraz-Noriega: angiographic analysis, data review, and manuscript drafting. J.F. Andrés-Cordón: angiographic analysis, data review, and statistical analysis. E. Cañedo: data collection and clinical follow-up. F. Panchano-Castro: angiographic analysis and data review. M. Trichilo: data collection and clinical follow-up. V. Vilalta: data collection and critical manuscript review. O. Rodríguez-Leor: data collection and critical manuscript review. E. Fernández-Nofrerias: critical manuscript review. I. Santos-Pardo: critical manuscript review. X. Carrillo: study design, overall supervision, and manuscript drafting. All authors reviewed and approved the final version.
CONFLICTS OF INTEREST
None declared.
WHAT IS KNOWN ABOUT THIS TOPIC?
- Routine use of manual thrombectomy has not demonstrated clear benefit. Current clinical practice guidelines recommend individualized use in selected patients with high thrombus burden. Clear angiographic criteria for identifying patients most likely to benefit from thrombectomy are lacking.
WHAT DOES THIS STUDY ADD?
- The Hunted registry provides specific evidence on thrombectomy performed with the Hunter catheter during PCI.
- It identifies angiographic predictors of thrombectomy success (vessel diameter > 2.5 mm, TIMI ≥ 4 thrombus burden, non-circumflex coronary arteries).
- The Hunter catheter, with its larger effective aspiration area, along with proper technique, demonstrates a low complication rate and favorable clinical outcomes.
REFERENCES
1. Keeley EC, Boura JA, Grines CL, et al. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003;361:13-20.
2. Chesebro JH, Knatterud G, Roberts R, et al. Thrombolysis in Myocardial Infarction (TIMI) Trial, Phase I: A comparison between intravenous tissue plasminogen activator and intravenous streptokinase. Clinical findings through hospital discharge. Circulation. 1987;76:142-154.
3. Moens AL, Claeys MJ, Timmermans JP, et al. Myocardial ischemia/reperfusion-injury, a clinical view on a complex pathophysiological process. Int J Cardiol. 2005;100:179-190.
4. Bhindi R, Kajander OA, Jolly SS, et al. Culprit lesion thrombus burden after manual thrombectomy or percutaneous coronary intervention-alone in ST-segment elevation myocardial infarction: the OTC sub-study of the TOTAL trial. Eur Heart J. 2015;36:1892-1900.
5. Sim DS, Jeong MH, Ahn Y, et al. Korea Acute Myocardial Infarction Registry (KAMIR) Investigators. Manual thrombus aspiration during primary percutaneous coronary intervention: Impact of total ischemic time. J Cardiol. 2016;27:753-758.
6. Vlaar PJ, Svilaas T, van der Horst IC, et al. Cardiac death and reinfarction after 1 year in the Thrombus Aspiration during Percutaneous coronary intervention in Acute myocardial infarction Study (TAPAS): a 1-year follow-up study. Lancet. 2008;371:1915-1920.
7. Lagerqvist B, Fröbert O, Olivecrona GK, et al. Outcomes 1 Year after Thrombus Aspiration for Myocardial Infarction. N Engl J Med. 2014;371:1111-1120.
8. Levine GN, Bates ER, Blankenship JC, et al. ACC/AHA/SCAI Focused Update on Primary Percutaneous Coronary Intervention for Patients with ST-Elevation Myocardial Infarction: An Update of the 2011 ACCF/AHA/SCAI and the 2013 ACCF/AHA Guidelines. J Am Coll Cardiol. 2016;67:1235-1250.
9. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119-177.
10. Sianos G, Papafaklis MI, Serruys PW. Angiographic thrombus burden classification in patients with ST-segment elevation myocardial infarction treated with percutaneous coronary intervention. J Invasive Cardiol. 2010;22:6B-14B.
11. Freixa X, Jurado-Román A, Cid B, et al. Spanish cardiac catheterization and coronary intervention registry. 31st official report of the Interventional Cardiology Association of the Spanish Society of Cardiology (1990-2021). Rev Esp Cardiol. 2022;75:1040-1049.
12. Kimura K, Kimura T, Ishihisa M, et al. JCS 2018 Guideline on diagnosis and treatment of acute coronary syndrome. Circulation. 2019;83:1085-1196.
13. Qu Y-Y, Zhang X-G, Ju C-W, et al. Age-Related Utilization of Thrombus Aspiration in Patients with ST-Segment Elevation Myocardial Infarction: Findings From the Improving Care for Cardiovascular Disease in China Project. Front Cardiovasc Med. 2022;9:791007.
14. Svilaas T, Vlaar PJ, van der Horst IC, et al. Thrombus aspiration during primary percutaneous coronary intervention. N Engl J Med. 2008;358:557-567.
15. Jolly SS, James S, Džavík V, et al. Thrombus Aspiration in ST-Segment–Elevation Myocardial Infarction, An Individual Patient Meta-Analysis: Thrombectomy Trialists Collaboration. Circulation. 2017;135:143-152.
16. Jolly SS, Cairns JA, Yusuf S, et al. Randomized trial of primary PCI with or without routine manual thrombectomy. N Engl J Med. 2015;372:1389-1398.
17. Angeras O, Haraldsson I, Redfors B, et al. Impact of Thrombus Aspiration on Mortality, Stent Thrombosis, and Stroke in Patients with ST-Segment–Elevation Myocardial Infarction: A Report From the Swedish Coronary Angiography and Angioplasty Registry. J Am Heart Assoc. 2018;7:e007680.
18. Carol A, Bernet M, Curós A, et al. Thrombus age, clinical presentation, and reperfusion grade in myocardial infarction. Cardiovasc Pathol. 2014;23:126-130.
19. Sim DS, Jeong MH, Ahn Y, et al. Manual thrombus aspiration during primary percutaneous coronary intervention: Impact of total ischemic time. J Cardiol. 2017;69:428-435.
20. Vlaar PJ, Svilaas T, van der Horst IC, et al. Cardiac death and reinfarction after 1 year in the Thrombus Aspiration during Percutaneous coronary intervention in Acute myocardial infarction Study (TAPAS): a 1-year follow-up study. Lancet. 2008;371:1915-1920.
21. Fröbert, O, Lagerqvist B, Olivecrona GK, et al. Thrombus aspiration during ST-segment elevation myocardial infarction. N Engl J Med. 2013;369:1587-1597.
22. Inohara T, Kohsaka S, Yamaji K, et al. Use of Thrombus Aspiration for Patients with Acute Coronary Syndrome: Insights from the Nationwide J-PCI Registry. J Am Heart Assoc. 2022;11:e025728.
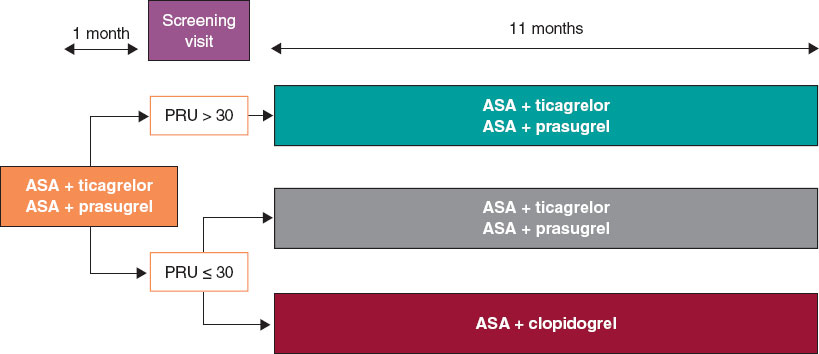
ABSTRACT
Introduction and objectives: De-escalation from prasugrel and ticagrelor to clopidogrel in patients undergoing percutaneous coronary intervention after acute coronary syndrome (ACS) is a strategy aimed at reducing bleeding. This study evaluates whether VerifyNow (Werfen, Spain)–guided de-escalation, based on platelet aggregation measurement, provides a therapeutic benefit in ACS management.
Methods: This ongoing multicenter, prospective, randomized 1:1 trial will enroll 634 patients with ACS who underwent revascularization with a sirolimus-eluting stent and were discharged on dual antiplatelet therapy with ticagrelor or prasugrel. Only those patients with a very low platelet reactivity level (platelet reactivity units ≤ 30) based on VerifyNow 1 month after discharge will be included. The primary endpoint is a composite of cardiovascular death, nonfatal acute myocardial infarction, nonfatal stroke, and bleeding at 1-year follow-up.
Results: The EPIC17-VERONICA study (NCT04654052) will reveal the efficacy profile of the de-escalation strategy, based on the VerifyNow platelet aggregation test, and determine the role of this device in the selection of patients who are eligible to benefit from this strategy.
Conclusions: This study will determine whether platelet function testing provide clinical benefit in the management of patients with ACS.
Keywords: Acute coronary syndrome. Antiplatelet therapy. Platelet function test. Bleeding.
RESUMEN
Introducción y objetivos: La desescalada desde prasugrel y ticagrelor a clopidogrel en pacientes tras intervencionismo coronario percutáneo por síndrome coronario agudo (SCA) constituye una de las estrategias para intentar disminuir las hemorragias. El objetivo de este estudio es averiguar si dicha desescalada guiada por la prueba de agregación plaquetaria VerifyNow (Werfen, España) tiene un efecto beneficioso en el tratamiento del SCA.
Métodos: Estudio multicéntrico, prospectivo y aleatorizado 1:1, en curso. Se incluirán 634 pacientes con SCA y revascularización con stent de sirolimus que sean dados de alta con doble terapia antiagregante con ticagrelor o prasugrel. Solo se incluirán aquellos con un nivel de reactividad plaquetaria muy bajo (unidades de reactividad plaquetaria ≤ 30) basado en VerifyNow al mes del alta. El objetivo primario es un combinado de muerte por causa cardiovascular, infarto agudo de miocardio no fatal, accidente cerebrovascular no fatal y sangrado en un seguimiento a 1 año.
Resultados: El estudio EPIC17-VERONICA (NCT04654052) permitirá averiguar la eficacia de la estrategia de desescalada basada en la prueba de agregación plaquetaria VerifyNow, además de conocer el papel de este dispositivo en la selección de los pacientes candidatos a beneficiarse de esta estrategia.
Conclusiones: Este estudio determinará si las pruebas de función plaquetaria aportan beneficio en el tratamiento tras el SCA.
Palabras clave: Síndrome coronario agudo. Terapia antiagregante. Prueba de función plaquetaria. Sangrado.
Abbreviations
ACS: acute coronary syndrome. PCI: percutaneous coronary intervention. PRU: platelet reactivity units.
INTRODUCTION
Following percutaneous coronary intervention (PCI) in patients with acute coronary syndrome (ACS), a 12-month regimen of dual antiplatelet therapy with a P2Y12 receptor inhibitor and acetylsalicylic acid is recommended, regardless of the type of stent implanted, except when contraindicated.1 Although prasugrel and ticagrelor are preferred over clopidogrel in this setting, there is ongoing debate regarding the potency and duration of dual antiplatelet therapy. This controversy stems from the fact that most patients concurrently face 2 opposing and potentially fatal risks—ischemic and hemorrhagic—which must be carefully balanced on an individual basis.
The introduction of stents with reduced thrombogenicity, together with evidence that thrombotic risk is highest during the first few months after PCI while hemorrhagic risk remains relatively constant throughout time, has led to research efforts focused on minimizing bleeding complications. These strategies include shortening dual antiplatelet therapy, using P2Y12 inhibitors as monotherapy, and implementing de-escalation strategies.2,3
De-escalation consists of switching from prasugrel or ticagrelor to clopidogrel and can be guided (using genetic or platelet function testing) or unguided. Because this strategy may increase ischemic events, it is not recommended within the first month after PCI.1
In the TOPIC trial,4 the unguided de-escalation strategy initiated 1 month after ACS significantly reduced hemorrhagic events (Bleeding Academic Research Consortium [BARC] grade ≥ 2 bleeding events) at 1 year without increasing the ischemic ones. In the TROPICAL-ACS trial,5 the platelet function testing–guided de-escalation from prasugrel to clopidogrel 2 weeks after revascularization was noninferior to standard therapy, showing a trend toward fewer hemorrhages at 12 months and a similar rate of thrombotic events.1,2,6 In the TALOS-AMI trial,7 12-month event rates were lower, primarily because of fewer hemorrhagic events among patients who underwent unguided de-escalation 1 month after ACS. Table 1 summarizes these studies.
Table 1. De-escalation clinical trials in patients with acute coronary syndrome
| TOPIC (2017)4 | TROPICAL-ACS (2018)5 | TALOS-AMI (2021)12 | |
|---|---|---|---|
| Population | n = 645 | n = 2610 | n = 2697 |
| Design | Open-label, single-center, randomized, superiority trial | Open-label, multicenter, randomized, noninferiority trial | Open-label, multicenter, randomized, noninferiority trial |
| Strategy | Standard therapy vs unguided de-escalation | Standard therapy vs platelet function testing–guided therapy (Multiplate device) | Standard therapy vs unguided de-escalation |
| Control group | Continued dual antiplatelet therapy with acetylsalicylic acid and ticagrelor or prasugrel | Continued dual antiplatelet therapy with acetylsalicylic acid and prasugrel | Continued dual antiplatelet therapy with acetylsalicylic acid and ticagrelor |
| Experimental group | De-escalation to acetylsalicylic acid and clopidogrel | 1-week regimen of prasugrel, followed by 1-week regimen of clopidogrel and either prasugrel or clopidogrel from day 14 onward, according to platelet function testing results | De-escalation to acetylsalicylic acid and clopidogrel |
| Time from revascularization to de-escalation | 1 month | 2 weeks | 1 month |
| Follow-up | 1 year | 1 year | 1 year |
| Primary endpoint | Cardiac death, emergency revascularization, stroke, or BARC ≥ 2 bleeding events | Cardiac death, myocardial infarction, stroke, or BARC ≥ 2 bleeding events | Cardiac death, myocardial infarction, stroke, or BARC ≥ 2 bleeding events |
| Results | 13.4% in experimental group vs 26.3% in control group (HR, 0.48; 95%CI, 0.34–0.68; P < .01) | 7.3% in experimental group vs 9.0% in control group (HR, 0.81; 95%CI, 0.62–1.06; P = .0004) | 4.6% in experimental group vs 8.2% in control group (HR, 0.55; 95%CI, 0.42–0.76; P < .0001) |
|
95%CI, 95% confidence interval; BARC, Bleeding Academic Research Consortium; HR, hazard ratio. |
|||
After the positive results of the TOPIC trial, the VerifyNow to optimise platelet inhibition in coronary acute syndrome (EPIC17-VERONICA) trial (ClinicalTrials.gov: NCT04654052) aims to further refine this strategy by only applying de-escalation to patients with excessive antiplatelet effects from prasugrel or ticagrelor after the first month who are at theoretical risk of hemorrhage based on the VerifyNow platelet aggregation test (Werfen, Spain). Thus, patients demonstrating an adequate pharmacologic response will continue prasugrel or ticagrelor therapy for 1 year, whereas those with very low platelet reactivity after a 1-month regimen of dual antiplatelet therapy with these agents constitute the target population of this study.
METHODS
Design
We are conducting a multicenter, prospective, randomized clinical trial at 16 Spanish centers. Based on the results of the platelet aggregation test for P2Y12 inhibition (platelet reactivity units [PRU]) using the VerifyNow system, patients with very low platelet reactivity (PRU ≤ 30) are randomized in a 1:1 ratio to either continue treatment with ticagrelor or prasugrel, or to de-escalate to clopidogrel. Patients with PRU > 30 are not randomized. The study flowchart is shown in figure 1.
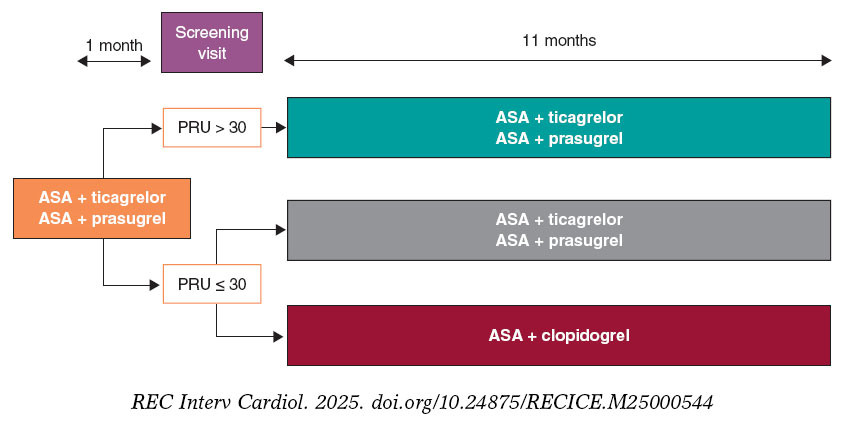
Figure 1. Study flowchart. AAS, acetylsalicylic acid; PRU, platelet reactivity units.
The study is being conducted in full compliance with the principles outlined in the Declaration of Helsinki and has been approved by the central ethics committee (Comité del Bierzo, León, Spain) and endorsed by the ethics committees of all participant centers. The appendix lists the participant centers and principal investigators.
The study sponsor (Fundación para la Educación en Procedimientos de Intervencionismo en Cardiología [EPIC]) is fully responsible, together with the principal investigators, for data management and confidentiality.
Population
Inclusion and exclusion criteria
Table 2 summarizes the inclusion and exclusion criteria. Briefly, all patients with ACS undergoing PCI with a sirolimus-eluting stent and a bioresorbable polymer during hospitalization and discharged on dual antiplatelet therapy with acetylsalicylic acid and ticagrelor or prasugrel are eligible for inclusion.
Table 2. Inclusion and exclusion criteria
| Inclusion criteria |
|---|
| Patients > 18 years |
| Patients with acute coronary syndrome undergoing percutaneous revascularization with a sirolimus-eluting stent with a bioresorbable polymer and discharged on dual antiplatelet therapy with acetylsalicylic acid and ticagrelor or prasugrel |
| Signed informed consent |
| Exclusion criteria |
| History of intracranial hemorrhage |
| Contraindication to acetylsalicylic acid, clopidogrel, prasugrel, or ticagrelor |
| Major ischemic or bleeding events during the first month of antiplatelet therapy |
| Thrombocytopenia < 50 000/µL |
| Permanent oral anticoagulation |
| Pregnancy or breastfeeding |
| Inability to complete the 1-year follow-up |
| Life expectancy < 24 months |
Written informed consent must be obtained before the platelet aggregation tes is performed.
Study protocol and randomization
Eligible patients are scheduled for P2Y12 receptor inhibition testing with the VerifyNow system between 30 and 40 days after hospital discharge. Measurements are obtained at least 6 hours after the administration of the last P2Y12 inhibitor dose. Patients with PRU ≤ 30 (very low platelet reactivity) are randomized in a 1:1 ratio using an electronic system to either continue their current treatment or de-escalate to clopidogrel, 75 mg once daily. De-escalation is preceded by a loading dose of 600 mg administered 24 hours after the last dose of ticagrelor or 75 mg 24 hours after the last dose of prasugrel, in accordance with the 2017 European Society of Cardiology clinical practice guidelines.8
The remaining patients with PRU > 30 are not randomized, and their dual antiplatelet therapy remains unchanged from discharge.
Clinical follow-up
Patients in the 2 randomized groups undergo telephone follow-up to monitor clinical events at 2, 5, 8, and 11 months after enrollment, corresponding to 3, 6, 9, and 12 months after hospital discharge.
For patients with PRU > 30 on the 1-month VerifyNow platelet aggregation test who are not randomized, only baseline characteristics are recorded, and no further follow-up is conducted.
Protocol of the VerifyNow platelet aggregation test
The VerifyNow system determines platelet activity by measuring in vitro aggregation in a blood sample exposed to specific agonists. This optical detection instrument (figure 2), which operates on a turbidimetric principle, uses single-use cartridges. In this study, PRUTest-specific kits are employed. (Werfen, Spain) to assess platelet aggregation while on P2Y12 receptor inhibitor therapy (ticagrelor, prasugrel, and clopidogrel). Each PRUTest kit contains lyophilized microbeads coated with fibrinogen, platelet activators, and a buffered solution. The test is based on the ability of activated platelets to bind fibrinogen-coated microbeads. Light transmission increases as activated platelets bind to and aggregate with the fibrinogen-coated microspheres. The kit measures this change in the optical signal and reports the results in PRU units (figure 3).

Figure 2. VerifyNow system. Reproduced with permission from Werfen.
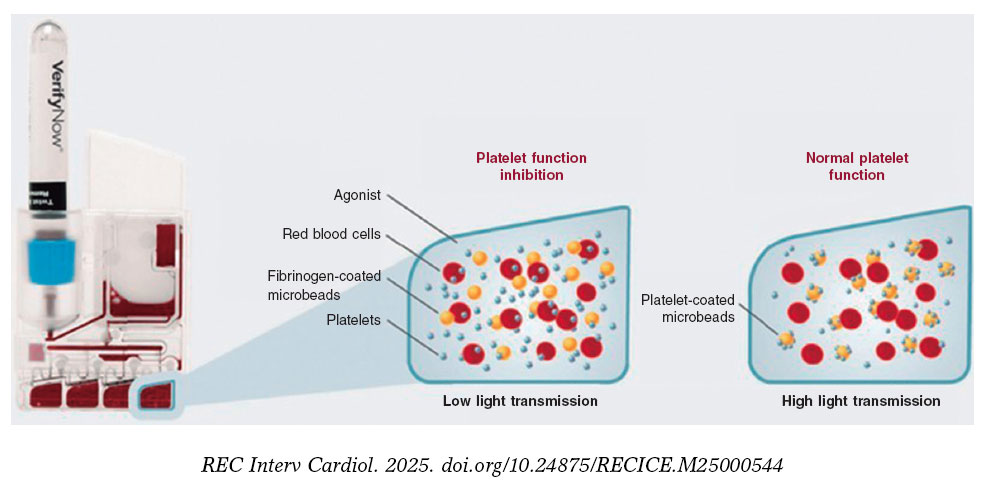
Figure 3. Performance of the VerifyNow system based on light transmission aggregometry. Light transmission increases as activated platelets bind and aggregate to the fibrinogen-coated microbeads in the kit. Therefore, high light transmission (corresponding to elevated platelet reactivity unit [PRU] values) indicates normal platelet function, whereas low light transmission (decreased PRU values) reflects platelet inhibition induced by the tested drugs.
An antiplatelet effect of the drug is considered present with PRU ≤ 180 (figure 4). Only patients with PRU ≤ 30 are randomized, as these are considered to have very low platelet reactivity while on antiplatelet therapy.
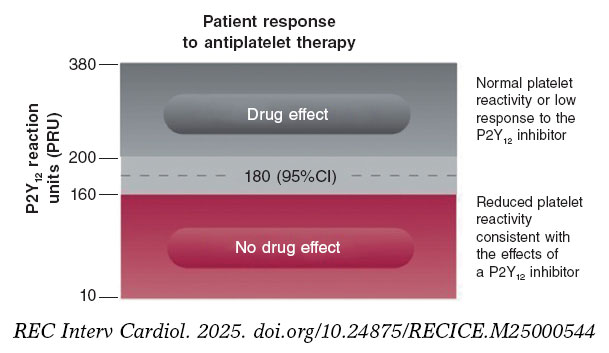
Figure 4. Reference levels for platelet reactivity units (PRU). 95%CI, 95% confidence interval.
Endpoints
The primary endpoint of the study is to compare the efficacy of de-escalation from ticagrelor or prasugrel to clopidogrel in patients undergoing PCI in the ACS setting, using the VerifyNow platelet aggregation test vs standard dual antiplatelet therapy at the 1-year follow-up. The rate of net adverse cardiovascular events is the primary endpoint of the study, defined as a composite of cardiac death, nonfatal myocardial infarction, nonfatal stroke, and hemorrhage (defined as Bleeding Academic Research Consortium [BARC] grade ≥ 2 bleeding events). The BARC scale is shown in table S1.
Furthermore, the study aims to compare several secondary endpoints (table 3), such as the occurrence of ischemic events during follow-up: cardiac death and all-cause mortality, acute myocardial infarction, stroke, stent thrombosis, and need for emergency revascularization. Moreover, the hemorrhage rate (defined as BARC grade ≥ 2 bleeding events) will be compared. The definitions of all study endpoints are shown in table S2.
Table 3. Endpoints of the study
| Primary endpoint |
|---|
| To compare the percentage of net adverse cardiovascular events between the 2 subgroups of patients with low platelet reactivity (PRU ≤ 30) who were randomized to de-escalation to clopidogrel vs standard therapy |
| Secondary endpoints |
| To compare the rate of cardiac death between the 2 randomized patient subgroups |
| To compare the rate of all-cause mortality between the 2 randomized patient subgroups |
| To compare the rate of acute myocardial infarction between the 2 randomized patient subgroups |
| To compare the rate of stroke between the 2 randomized patient subgroups |
| To compare the rate of stent thrombosis between the 2 randomized patient subgroups |
| To compare the rate of emergency revascularization between the 2 randomized patient subgroups |
| To compare the rate of bleeding events (defined as BARC ≥ 2) between the 2 randomized patient subgroups |
|
BARC, Bleeding Academic Research Consortium; PRU, platelet reactivity units. |
Statistics
Sample size calculation
Sample size was calculated for the randomized clinical trial cohort. The total number of patients (including those not randomized with PRU > 30) will depend on the total required to reach the estimated sample size for the randomized clinical trial.
We estimate a smaller difference in event rates across the groups than that observed in the TOPIC trial,4 specifically, 14% in the de-escalation group vs 22% in the standard therapy group. Assuming a significance level of 0.05, a power of 80%, a 2-tailed P-value and a 10% loss to follow-up, a total of 634 randomized patients (317 per group) will be required.
Statistical analysis plan
Quantitative variables will be expressed as mean and standard deviation if normally distributed, or as median and interquartile range otherwise. Categorical variables will be expressed as absolute values and percentages. Study data will be analyzed using one-way analysis of variance (ANOVA) for continuous variables, and Fisher’s exact or chi-square tests for categorical variables, as appropriate. Nonparametric tests will be used for variables that are not normally distributed or cannot be normalized. For the main outcome measure, Kaplan-Meier survival curves with log-rank statistics will be presented for prespecified criteria, and multivariable Cox regression will be performed to adjust for known risk factors and potential confounders. Hazard ratios and 95% confidence intervals will be reported for all statistically significant variables.
Intention-to-treat (according to randomization assignment) and per-protocol analyses (in case of crossover) will be conducted. The former will serve as the study primary analysis.
DISCUSSION
The EPIC17-VERONICA trial aims to demonstrate the efficacy of a VerifyNow platelet aggregation test-guided de-escalation strategy in reducing hemorrhagic events without increasing ischemic events in patients with ACS who have undergone percutaneous revascularization and exhibit very low platelet reactivity after the first month of treatment with prasugrel or ticagrelor.
The initial lack of expected results from platelet function testing to identify patients at risk for thrombotic events while on clopidogrel in the GRAVITAS,9 TRIGGER-PCI,10 and ARCTIC11 trials relegated its use to a class IIb recommendation in the European Society of Cardiology antiplatelet guidelines for determining the optimal timing of cardiac surgery after ACS.8 However, the 1-year results of the large-scale multicenter ADAPT-DES trial12 with 8500 PCI patients demonstrated that platelet reactivity assessed with the VerifyNow platelet aggregation test is an independent predictor of bleeding events.
In the TOPIC4 and TALOS-AMI7 trials, the unguided de-escalation strategy significantly reduced bleeding events without increasing ischemic events. In the TROPICAL-ACS5 trial, this platelet aggregation test–guided de-escalation strategy showed a trend toward fewer hemorrhages, with a similar rate of thrombotic complications.
The EPIC17-VERONICA study further seeks to improve the application of this de-escalation strategy by using the VerifyNow platelet aggregation test to identify patients with very low platelet reactivity (PRU ≤ 30) as those most likely to benefit from de-escalation.
CONCLUSIONS
The EPIC17-VERONICA trial has been designed to investigate the efficacy of de-escalating from the most potent antiplatelet agents (ticagrelor and prasugrel) to clopidogrel after the first month of therapy in patients with ACS and very low platelet reactivity, aiming to reduce bleeding events without increasing ischemic complications. Furthermore, it will provide evidence on the clinical utility of the VerifyNow platelet aggregation test for patient selection.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
The study is being conducted in full compliance with the principles outlined in the Declaration of Helsinki on clinical research and has been approved by the central ethics committee (Comité del Bierzo, León, Spain) and endorsed by the ethics committees of all participant centers. Written informed consent is required prior to performing ant platelet aggregation measurements. Sex and gender bias considerations have been addressed.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence was used in the preparation of this manuscript.
AUTHORS’ CONTRIBUTIONS
C. Garilleti Cámara and I. Lozano Martínez-Luengas drafted the manuscript; the remaining authors critically revised the document and approved the final version.
CONFLICTS OF INTEREST
J.M. de la Torre-Hernández is Editor-in-Chief of REC: Interventional Cardiology; A. Pérez de Prado is Associate Editor of REC: Interventional Cardiology. In both cases, the journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. The remaining authors declared no conflicts of interest whatsoever.
WHAT IS KNOWN ABOUT THE TOPIC?
- De-escalation from the most potent antiplatelet agents to clopidogrel is one of the strategies used to reduce hemorrhage after percutaneous revascularization in acute coronary syndrome. This de-escalation can be performed guided or unguided by genetic or platelet function testing.
WHAT DOES THIS STUDY ADD?
- The EPIC17-VERONICA trial is the first to use the VerifyNow platelet aggregation test to select patients eligible for de-escalation.
SUPPLEMENTARY DATA
REFERENCES
1. Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44:3720-3826.
2. Angiolillo DA, Galli M, Collet JP, Kastrati A, O’Donoghue MO. Antiplatelet therapy after percutaneous coronary intervention. EuroIntervention. 2022; 17:e1371-e1396.
3. Angiolillo DJ. The Evolution of Antiplatelet Therapy in the Treatment of Acute Coronary Syndromes. Drugs. 2012;72:2087-2116.
4. Cuisset T, Deharo P, Quilici J, et al. Benefit of switching dual antiplatelet therapy after acute coronary syndrome: the TOPIC (timing of platelet inhibition after acute coronary syndrome) randomized study. Eur Heart J. 2017;38:3070-3078.
5. Sibbing D, Aradi D, Jacobshagen C, et al. Guided de-escalation of antiplatelet treatment in patients with acute coronary syndrome undergoing percutaneous coronary intervention (TROPICAL-ACS): a randomised, open-label, multicentre trial. Lancet. 2017;390:1747-1757.
6. Gorog DA, Ferreiro JL, Ahrens I, et al. De-escalation or abbreviation of dual antiplatelet therapy in acute coronary syndromes and percutaneous coronary intervention: a Consensus Statement from an international expert panel on coronary thrombosis. Nat Rev Cardiol. 2023;20:830-844.
7. Kim CJ, Park MW, Kim MC, et al. Unguided de-escalation from ticagrelor to clopidogrel in stabilised patients with acute myocardial infarction undergoing percutaneous coronary intervention (TALOS-AMI): an investigator-initiated, open-label, multicentre, non-inferiority, randomised trial. Lancet. 2021;398:1305-1316.
8. Valgimigli A del G de TM, Bueno H, Byrne RA, et al. Actualización ESC 2017 sobre el tratamiento antiagregante plaquetario doble en la enfermedad coronaria, desarrollada en colaboración con la EACTS. Rev Esp Cardiol. 2018;71:42.e1-42.e58.
9. Price MJ, Berger PB, Teirstein PS, et al. Standard- vs high-dose clopidogrel based on platelet function testing after percutaneous coronary intervention: the GRAVITAS randomized trial. JAMA. 2011;305:1097-105. Erratum in: JAMA. 2011;305;2174. Stillablower, Michael E [corrected to Stillabower, Michael E]. PMID: 21406646.
10. Trenk D, Stone GW, Gawaz M, et al. A Randomized Trial of Prasugrel Versus Clopidogrel in Patients With High Platelet Reactivity on Clopidogrel After Elective Percutaneous Coronary Intervention With Implantation of Drug-Eluting Stents. J Am Coll Cardiol. 2012;59:2159-2164.
11. Collet JP, Cuisset T, Rangé G, et al. Bedside Monitoring to Adjust Antiplatelet Therapy for Coronary Stenting. N Engl J Med. 2012;367:2100-2109.
12. Sibbing D, Schulz S, Braun S, et al. Antiplatelet effects of clopidogrel and bleeding in patients undergoing coronary stent placement. J Thromb Haemost. 2010;8:250-256.
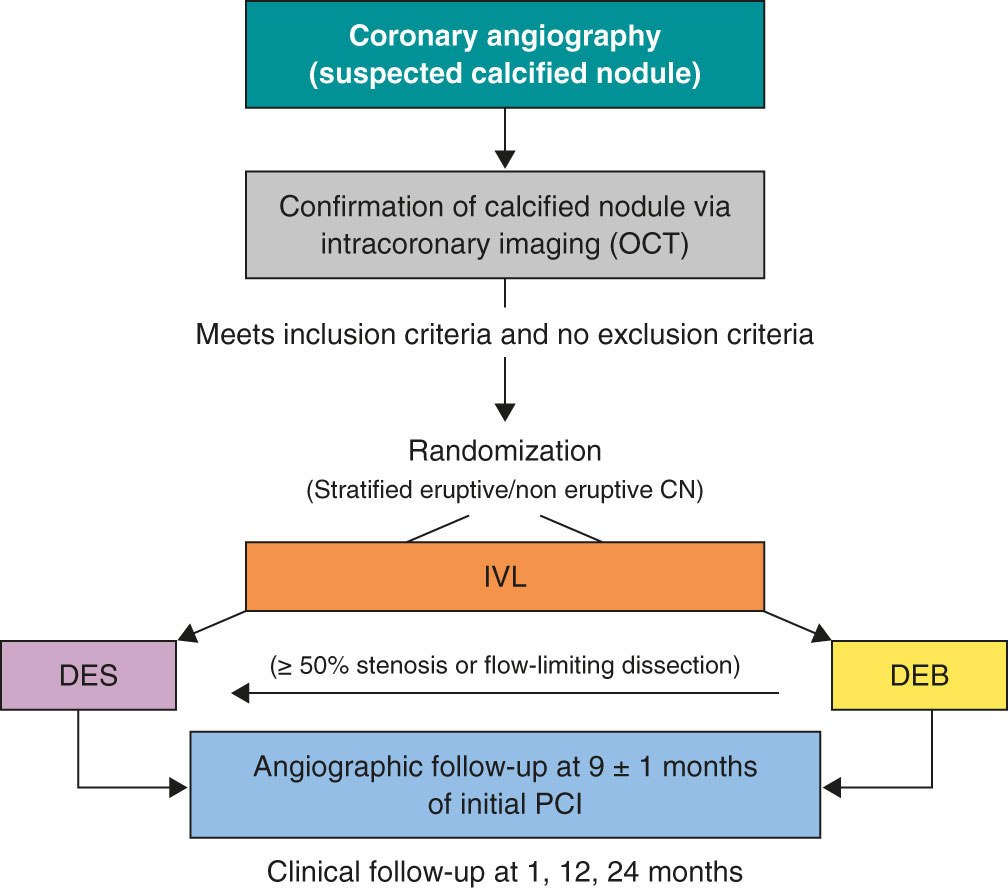
ABSTRACT
Introduction and objectives: Calcified coronary nodules (CN) are among the most challenging lesions for percutaneous coronary intervention, as drug-eluting stents (DES) frequently result in suboptimal expansion, malapposition, and recurrent adverse events. Although intravascular lithotripsy (IVL) provides effective plaque modification, the optimal definitive strategy remains unclear. Drug-eluting balloons (DEB) have demonstrated potential in the treatment of complex lesions in which stent implantation may be less desirable. This trial aims to compare the safety and efficacy profile of DEB vs DES after IVL in patients with CN.
Methods: We conducted a retrospective, investigator-initiated, multicenter, non-inferiority, randomized clinical trial.
Results: A total of 128 patients with de novo CN confirmed by intracoronary imaging in vessels measuring 2.5 mm to 4.0 mm in diameter will be enrolled across 10 high-volume percutaneous coronary intervention centers. After lesion preparation with IVL, patients will be randomized on a 1:1 ratio to receive a DEB or a DES. The co-primary endpoints are late lumen loss and net luminal gain at 9 ± 1 months of angiographic follow-up, both assessed by an independent core laboratory. Secondary endpoints include procedural, angiographic, and clinical outcomes, adjudicated by a blinded clinical events committee. Clinical follow-up will be conducted at 1 month, 1 year, and 2 years.
Conclusions: The DEBSCAN-IVL trial will provide the first randomized evidence comparing DEB and DES after IVL for CN.
Registered at ClinicalTrials.gov: NCT06657833.
Keywords: Calcified nodule. Intravascular lithotripsy. Drug-eluting balloons. Drug-eluting stents. Complex percutaneous coronary intervention.
RESUMEN
Introducción y objetivos: Los nódulos coronarios calcificados (NC) se encuentran entre las lesiones más desafiantes para la intervención coronaria percutánea, ya que los stents farmacoactivos (SFA) con frecuencia presentan expansión subóptima, mala aposición y eventos adversos recurrentes. La litotricia intravascular (LIV) permite una modificación eficaz de la placa, pero la estrategia definitiva óptima sigue sin estar clara. Los balones farmacoactivos (BFA) han mostrado resultados prometedores en lesiones complejas en las que la implantación de stents podría ser menos favorable. Este ensayo tiene como objetivo comparar la seguridad y la eficacia del BFA frente al SFA después de la LIV en pacientes con NC.
Métodos: Ensayo clínico prospectivo, por iniciativa del investigador, multicéntrico, de no inferioridad y aleatorizado.
Resultados: Un total de 128 pacientes con NC de novo confirmados mediante imagen intracoronaria en vasos de 2,5-4,0 mm de diámetro serán incluidos en 10 centros de intervencionismo coronario percutáneo de alto volumen. Tras la preparación de la lesión con LIV, los pacientes serán aleatorizados 1:1 para ser tratados con BFA o SFA. Los criterios de valoración coprimarios son la pérdida luminal tardía y la ganancia luminal neta en el seguimiento angiográfico a 9 ± 1 meses, evaluadas por un laboratorio central independiente. Los criterios secundarios incluyen resultados procedimentales, angiográficos y clínicos, adjudicados por un comité de eventos clínicos enmascarado. El seguimiento clínico se realizará a 1 mes, 1 año y 2 años.
Conclusiones: El ensayo DEBSCAN-IVL proporcionará la primera evidencia de comparación de BFA y SFA aleatorizados después de IVL en NC.
Registrado en ClinicalTrials.gov: NCT06657833.
Palabras clave: Nódulo calcificado. Litotricia intravascular. Balón farmacoactivo. Stent farmacoactivo. Intervención coronaria percutánea compleja.
Abreviaturas
CN: calcified coronary nodule. DEB: drug-eluting balloon. DES: drug-eluting stent. IVL: intravascular lithotripsy. OCT: optical coherence tomography. PCI: percutaneous coronary intervention.
INTRODUCTION
Calcified coronary nodules (CN) represent the most complex type of calcified lesion for percutaneous coronary intervention (PCI), as they are associated with worse angiographic and clinical outcomes after drug-eluting stent (DES) implantation.1-8
Intravascular lithotripsy (IVL) has shown favorable results in this context.9 However, stent implantation after IVL may not always be the best treatment option due to suboptimal stent expansion and severe malapposition in a non-negligible percentage of patients which, along with possible nodule protrusion through the stent struts, may be associated with an increased need for new target lesion revascularization (TLR), and a higher rate of major adverse cardiovascular events (MACE).10-12
Drug-eluting balloons (DEB) have demonstrated to be a safe and effective alternative to DES in various settings, especially in those in which stenting is associated with worse outcomes, such as small vessel disease and in-stent restenosis.13 Therefore, their use has increased exponentially in recent years and has expanded to other lesion types.14
In the specific setting of calcified lesions, there are some data on the safety and efficacy profile of DEB after an adequate plaque modification.15-19 Moreover, in this setting, DEB have shown similar clinical outcomes with favorable late lumen loss rate compared with DES.20-23
Despite the increasing use of DEB in calcified lesions, evidence on the safety and efficacy profile of CN treatment is lacking. In this setting, where the risj of suboptimal stent expansion and apposition—and the consequent likelihood of MACE— is higher,24 a leave-nothing-behind strategy using DEB following optimal plaque modification technique may be a more appealing approach.Therefore, our aim is to compare the safety and efficacy profile of the use of DEB or DES after IVL in CN within the context of a randomized controlled trial.
METHODS
Patients and study design
The DEBSCAN-IVL trial is an investigator-initiated, multicenter, open-label, prospective, randomized, controlled clinical trial including 10 high-volume centers.
Patients will be randomized to receive a DEB or a DES after optimal treatment with IVL if they meet all the inclusion criteria and have no exclusion criteria. Inclusion criteria are age ≥ 18 years with a clinical indication for PCI (presenting with chronic or acute coronary syndromes) in a CN-induced de novo severe coronary lesion (confirmed via intracoronary imaging) in vessels with a reference diameter between 2.5 mm and 4.0 mm. Patients who meet at least 1 of the following conditions will be excluded: inability to provide oral and written informed consent or unwillingness to return for systematic angiographic follow-up; pregnant or breastfeeding patients; cardiogenic shock or cardiac arrest at the time of the index procedure; inability to maintain dual antiplatelet therapy for at least 1 month; life expectancy < 1 year; index lesion located at the left main coronary artery or in an aorto-ostial location; target lesion previously treated with stents or DEB or with high thrombus burden at the time of PCI (Thrombolysis In Myocardial Infarction [TIMI] thrombus grade ≥ 3).
Patients who meet all the inclusion criteria and none of the exclusion criteria will be treated with IVL and randomized to receive final therapy with DEB or DES. Randomization will occur via a web-based system. The complete inclusion and exclusion criteria are shown in table 1, and the study flowchart in figure 1.
Table 1. Inclusion and exclusion criteria
| Inclusion criteria | Exclusion criteria |
|---|---|
Patients must meet all inclusion criteria:
|
Patients must not meet any criteria:
|
|
DEB, drug-eluting balloon; IVUS, intravascular ultrasound; OCT, optical coherence tomography; PCI, percutaneous coronary intervention; TIMI, Thrombolysis in Myocardial Infarction. |
|
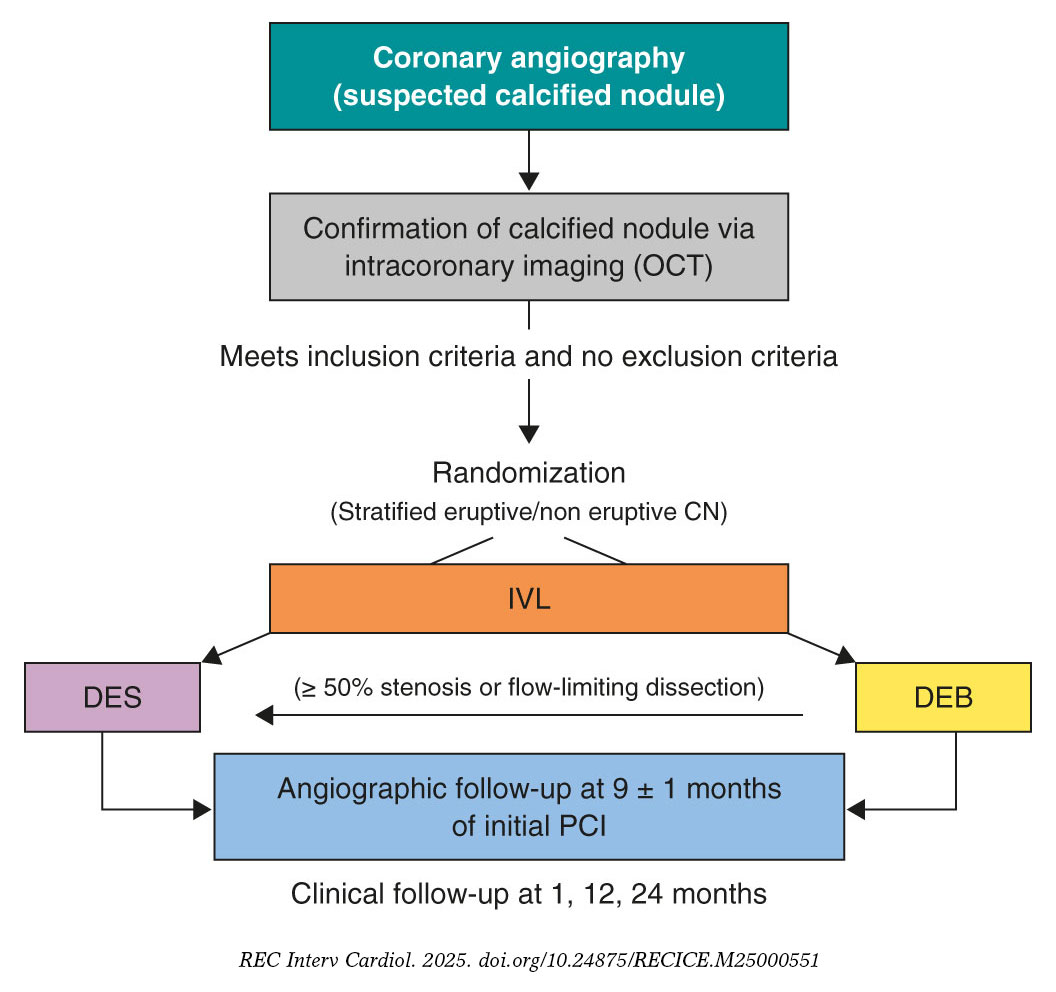
Figure 1. Central illustration. Study design flowchart. CN, calcified coronary nodule; DEB, drug-eluting balloons; DES, drug-eluting stents; IVL, intravascular lithotripsy; OCT, optical coherence tomography; PCI, percutaneous coronary intervention.
Primary and secondary endpoints
The endpoint of this study is to evaluate and compare the safety and efficacy profile of DEB or DES as final treatment strategies for CN previously modified by IVL.
Co-primary endpoints will be the late lumen loss (LLL) and net luminal gain at 9 ± 1 months of angiographic follow-up, as assessed by an independent core laboratory, with a non-inferiority hypothesis between the 2 groups. LLL is defined as the difference between postoperative and follow-up minimal lumen diameter, whereas net gain is defined as the difference between follow-up and preoperative minimal lumen diameter, according to the latest Drug Coated Balloon Academic Research Consortium Consensus Document.25
Secondary endpoints of the study will include procedural, angiographic and clinical outcomes. Procedural endpoints will include the rate of crossover between treatment groups, angiographic success (defined as final TIMI grade-3 flow and a residual final percent diameter stenosis < 30% in the DEB group or < 20% in the DES group), device success (defined as angiographic success without crossover between treatment group), procedural success (defined as angiographic success without the occurrence of severe procedural complications, including cardiac death, target vessel perioperative myocardial infarction [MI], need for new clinically driven TLR, stent thrombosis [ST], stroke, flow-limiting dissection or vessel perforation). Angiographic endpoints will include the minimal lumen diameter measured immediately after the intervention and at the time of angiographic follow-up, the residual percent diameter stenosis at both timeframes, and the rate of binary restenosis, defined as a luminal diameter reduction o≥ 50% during follow-up.25 Secondary endpoints will include procedural adverse events (such as dissection, perforation, acute vessel occlusion, slow flow or no-reflow, and intraoperative thrombosis), major hemorrhagic events (classified as Bleeding Academic Research Consortium [BARC] type ≥ 3),26 and hemodynamic instability (requiring unplanned administration of vasopressors, inotropes, or ventricular support devices), cardiac death, target lesion-related MI (TL-MI), need for TLR, and ST, and MACE (defined as a composite of cardiac death, TL-MI, and TLR). TLR and ST are defined according to the Academic Research Consortium criteria.27 MACE and its components will be assessed during the index hospitalization and at 6-month, 1-year, and 2-year follow-up visits. Detailed endpoints definitions are shown in appendix S1.
Primary outcome assessment will be conducted by a central independent core laboratory. All medical data will be anonymized and stored, and confidentiality will be protected at any time in full compliance with the current legislation. The clinical events committee (CEC) and the independent core laboratory will be blinded to the treatment group. Secondary outcomes will be assessed via centralized angiographic analysis and structured clinical follow-up, either in person or via telephone, at scheduled time points.
Devices
- – IVL: Shockwave Balloon (Shockwave Medical, United States).
- – Optical coherence tomography (OCT) or intracoronary ultrasound (IVUS) system, based on availability at each participating center.
- – DEB: paclitaxel-eluting balloon (Pantera Lux, Biotronik, Switzerland).
- – DES: new-generation zotarolimus eluting stent (Onyx Frontier, Medtronic, United States).
Procedure
When a CN is suspected on coronary angiography, intracoronary imaging—preferably OCT, with IVUS as an alternative—will be performed to confirm the diagnosis. After confirmation of a CN in the target lesion, patients will be randomized on a 1:1 ratio to receive a DEB or a DES. Randomization will be stratified to ensure a balanced distribution of eruptive and non-eruptive nodules across both treatment groups. A CN (figure 2) will be defined as a calcified segment with an accumulation of protruding nodular calcification (small calcium deposits) with disruption of the fibrous cap (eruptive CN) or an intact thick fibrous cap (non-eruptive CN).28-30
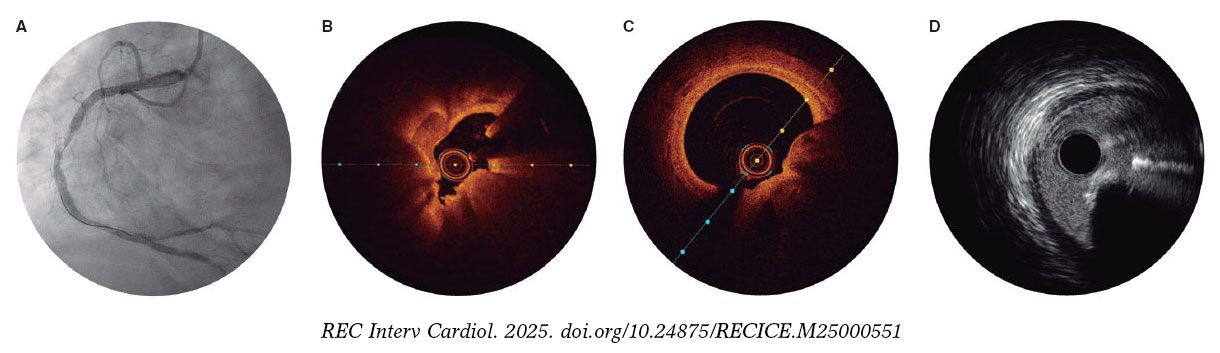
Figure 2. Calcified nodule appearance on angiography (A), optical coherence tomography (eruptive [B] and non-eruptive [C]) and intravascular ultrasound (D).
All patients will be treated with IVL, using a balloon sized 1:1 to the vessel reference diameter. A minimum of 80 pulses per lesion is recommended. If the IVL balloon cannot cross the lesion, predilation with smaller balloons is permitted. Additionally, the use of adjuvant techniques such as rotational atherectomy or excimer laser coronary atherectomy will be allowed only when deemed necessary to facilitate IVL balloon crossing. Postdilation with a non-compliant balloon after IVL is recommended before proceeding with the final assigned treatment modality.
Once optimal lesion preparation has been achieved, defined as > 80% balloon expansion in 2 orthogonal projections with a balloon sized 1:1 to the vessel, patients will receive a DEB or a DES, according to their initial randomization. If a patient randomized to the DEB group experiences a flow-limiting dissection or exhibits a percent diameter stenosis > 50%, conversion to DES implantation will be permitted at the operator’s discretion. Similarly, any crossover from DES to DEB will be documented, along with the reasons for these procedural decisions.
It is recommended that the DEB reach the target lesion within 2 minutes, as drug loss may occur during transit.13 Thus, operators need to anticipate difficulties in reaching the target lesion (proximal coronary disease or tortuosity) and ensure optimal support prior to using the DEB. If difficulties in reaching the target lesion are anticipated, the use of guide extension catheters is recommended. The recommended DEB inflation time is 60 seconds.
The PCI will be performed according to current European Society of Cardiology (ESC) guidelines, including perio- and postoperative antithrombotic management.31,32 Patients should ideally receive dual antiplatelet therapy at least 2 to 4 hours prior to the PCI to ensure optimal platelet inhibition. In cases where this is not feasible, administration of IV antiplatelet agents, such as acetylsalicylic acid with or without cangrelor, immediately before the procedure is recommended.
Intracoronary imaging with either OCT or IVUS (the same imaging modality that was initially used) is recommended at the end of the procedure.
Angiographic analysis
Quantitative coronary imaging and intracoronary analysis of baseline and follow-up angiographies will be conducted by an independent central laboratory (Barcicore, Spain). At least 2 well-selected orthogonal views—free of foreshortening and side-branch overlap—focused on the target lesion are required after intracoronary nitroglycerine administration. These views should be obtained before treatment, after the intervention, and during follow-up angiography to ensure consistent angulation and enable accurate, reproducible measurements.
Follow-up
Post-PCI antithrombotic therapy will abide by the latest ESC clinical practice guidelines, considering the individual ischemic and bleeding risk profile of each patient.31,32 Regardless of the assigned treatment group (DEB or DES), a 6-month regimen of dual antiplatelet therapy (aspirin and clopidogrel) is recommended in patients with stable coronary artery disease, and a 12-month regimen of dual antiplatelet therapy (preferably using prasugrel or ticagrelor as a P2Y12 inhibitor) in patients with acute coronary syndrome. For patients requiring chronic oral anticoagulation, the choice and duration of antithrombotic therapy will follow current guideline recommendations, with triple therapy (oral anticoagulant + aspirin + clopidogrel) limited to 1 month, whenever feasible. Electrocardiogram and troponin assessment will be performed 24 hours after the PCI. All patients will be discharged with a scheduled angiographic follow-up at 9 ± 1 months. OCT is recommended during this follow-up, especially if angiography suggests progression of coronary artery disease in the target lesion. In cases where angiography or intracoronary imaging indicates disease progression, but the percent diameter stenosis is < 90%, revascularization should be guided by ischemia and confirmed with a pressure guidewire. Clinical follow-up visits are scheduled at 12 and 24 months. Schedule of visits and data assessment throughout the study are shown in table S1.
Statistical analysis
The primary endpoint analysis will be performed by lesion and by intention-to-treat with a 1-sided Student t test with an alfa of 0.05 between the DES and the DEB group. A per-protocol analysis, including crossover cases, will also be conducted for sensitivity purposes. If the hypothesis of non-inferiority is confirmed, a superiority 2-sided analysis will be performed. Clinical endpoints will be analyzed on a per-patient basis.
Quantitative variables will be expressed as mean ± standard deviation if normally distributed, and as median with minimum and maximum values if they do not follow a normal distribution. Normality will be assessed using the Kolmogorov-Smirnov test. Qualitative variables will be described by their absolute values and frequencies, and will be expressed as absolute counts and percentages. A P < .05 will be considered statistically significant, and 95% confidence intervals (95%CI) will be reported for all main analyses. For comparisons of continuous variables between the 2 groups, the Student t test will be used if normality is confirmed, or the Mann-Whitney U test if non-parametric. For comparisons across > 2 groups, the ANOVA test or the Kruskal-Wallis test will be applied, as appropriate. Associations across categorical variables will be analyzed using the chi-square test or Fisher’s exact test when expected frequencies are small. Correlations between continuous variables will be explored using Pearson’s or Spearman’s correlation coefficient, depending on their distribution.
A multivariate analysis will be conducted using Cox proportional hazards regression with forward stepwise selection, including variables that are significantly associated with outcomes (or show a trend) in the univariate analysis. Kaplan-Meier curves will be generated for event-free survival, and differences will be assessed using the log-rank test.
Prespecified subgroup analysis
Subgroup analysis will be performed according to the following prespecified categories: type of calcified nodule (eruptive vs non-eruptive), age (< 75 vs ≥ 75 years), sex (male vs female), presence of diabetes mellitus (yes vs no), location of the calcified nodule within a true bifurcation lesion involving a side branch ≥ 2.5 mm (yes vs no), and clinical presentation (acute coronary syndrome vs chronic coronary syndrome). In addition, a prespecified OCT subgroup analysis will be performed in patients with available OCT imaging at both the end of the procedure and follow, including assessments of minimal lumen area (or minimal stent area in stented segments) and minimal lumen diameter.
Sample size calculation
The hypothesis is that DEB-PCI for CN is not inferior to state-of-the-art DES-PCI in terms of LLL and net luminal gain at the lesion. The sample size calculation was based on an expected LLL of 0.20 mm in the DES group, with a non-inferiority margin (delta) of 0.30 mm, a significance level (alpha) of 5%, and a statistical power of 80%. The estimate of LLL in the control group was derived from previous studies evaluating the same DES platform.33-35 Assuming a 20% attrition rate for angiographic follow-up, 64 patients per group (128 patients in total) will be required to provide adequate statistical power. The study is not powered for clinical endpoints, which will be considered exploratory and hypothesis-generating.
Organization and ethical concerns
The study protocol has been approved by the local ethics committees of all participant centers. Written informed consent will be obtained from all patients prior to enrollment. The DEBSCAN-IVL trial is an investigator-initiated study conducted in full compliance with Good Clinical Practice guidelines applicable to interventional and epidemiological research. The rights, safety, and well-being of all participants will be protected full compliance with the principles set forth in the Declaration of Helsinki, applicable EU legislation, and local legal requirements. Participant data will be handled confidentially and anonymously. The trial is registered at ClinicalTrials.gov (NCT06657833). The sponsor of the study is Fundación EPIC. The study is supported by unrestricted research grants from Fundación EPIC, Shockwave Medical, Biotronik, and Medtronic.
The steering committee serves as the primary decision-making body of the trial and bears full responsibility for its scientific and clinical conduct. A clinical events committee (CEC), composed of independent interventional cardiologists not participating in the study and blinded to treatment allocation, will adjudicate all clinical events and endpoints. The CEC will operate according to pre-specified definitions outlined in the study protocol and will remain blinded to the overall trial outcomes.
DISCUSSION
CN represent the most complex type of calcified lesion for PCI, as they are associated with the worst angiographic and clinical outcomes after DES implantation.1-8 Three main factors may contribute to these unfavorable results: the nature of the nodule per se, the plaque modification technique used, and the final revascularization strategy (DES or DEB). Although our understanding of the origin and behavior of calcified nodules has grown, it remains unclear which lesions are likely to respond favorably to PCI, and which are not. Eruptive CN, for instance, may be more amenable to initial modification, yet paradoxically, they have also been associated with higher rates of adverse clinical events during follow-up.29,36
Regarding plaque modification techniques, current evidence is limited. Rotational atherectomy (RA), while commonly used, is constrained by wire bias and frequently requires large burr sizes.2 Although orbital atherectomy might overcome some of these limitations, randomized data comparing it with other advanced plaque modification techniques are lacking.37 Balloon-based techniques, in contrast, may fail to cross severely stenotic nodular lesions but have the advantage of avoiding the wire bias inherent to atherectomy.
However, conventional or scoring/cutting balloons often prove insufficient to fully modify the depth of nodular calcium, and very high-pressure special balloons carry the risk of overstretching the usually normal opposite vessel wall causing perforation. In this context, IVL has emerged as a promising alternative, offering the most robust evidence to date for nodular plaque modification.29,38
Traditionally, stent implantation has been the standard definitive treatment for CN.23 However, stenting in nodular lesions frequently leads to suboptimal expansion and incomplete apposition, particularly at the shoulders of the nodule. Moreover, In these patients, TLR is often driven not by classic in-stent restenosis, but by late protrusion of the calcified nodule through the stent struts.10,11,39 These limitations have generated interest in a “leave nothing behind” strategy after effective plaque modification.
DEB have demonstrated to be safe and effective in various settings, particularly small vessel disease and in-stent restenosis, where DES implantation may be less favorable.13 Therefore, their use has grown significantly in recent years.14 In the context of calcified lesions, there are concerns that adequate drug-uptake may be compromised, but preliminary evidence suggests DEB may offer good outcomes after adequate plaque preparation.15-17 For instance, Ito et al.18 evaluated a total of 81 patients with de novo lesions treated with DEB, including 46 with calcified lesions. While LLL and restenosis appeared slightly higher in the calcified group, these differences were not statistically significant and did not translate into worse clinical outcomes at 2 years. Notably, 82% of these lesions were pre-treated with RA. Similarly, Nagai et al. reported a TLR rate of 16.3% in 190 severely calcified lesions treated with RA followed by DEB.19 Rissanen et al. found MACE rates of 14% and 20% at 12 and 24 months, respectively, in 82 complex de novo calcified lesions treated with DEB after RA and balloon predilation, with very low rates of clinically driven TLR.20 Furthermore, favorable findings have been reported by Shiraishi et al., including a subset of calcified nodules.16
Comparative studies have further explored DEB vs DES in calcified lesions. Ueno et al.21 conducted a single-center cohort study comparing the clinical outcomes of 166 severe calcified lesions treated with either DEB or DES after RA at a median follow-up of 3 years. The TLR rates were similar across the groups (15.6% vs 16.3%; P = .99), while LLL was significantly lower in the DEB group (0.09 mm vs 0.52 mm; P =.009). Iwasaki et al.22 compared 194 patients with de novo calcified lesions in non-small vessels the RA + DEB vs RA + DES strategies. There were no significant differences at 1 year in terms of MACE, cardiac death, myocardial infarction, TLR or hemorrhage.
Despite this data on the performance of DEB in calcified lesions, evidence on the safety and efficacy profile in the CN setting is lacking. However, given the high likelihood of suboptimal stent expansion and malapposition in this setting, which may lead to increased MACE risk,24 a metal-free strategy using DEB following optimal plaque modification seems to be an attractive and feasible approach.
Intracoronary imaging-guided PCI has been consistently associated with improved procedural outcomes and a reduction in major adverse cardiovascular events, including mortality, particularly in complex lesions.40 Intracoronary imaging plays a pivotal role in this context. Compared with conventional angiography, it provides a far more accurate assessment of coronary disease severity and plaque morphology.1 This is particularly relevant in calcified and complex lesions, where procedural planning and outcomes are significantly impacted by the detailed anatomical insights obtained. OCT, in particular, offers superior spatial resolution compared to IVUS, allowing for precise quantification of the calcium burden.28,41
In the case of CN, OCT enables accurate assessment of the plaque substrate and procedural results, including stent expansion and apposition, or in DEB-treated lesions, the extent of plaque modification.
The DEBSCAN-IVL trial will be comparing the safety and efficacy profile of DEB vs DES after lesion preparation with IVL in patients with CN, assessing both angiographic and clinical outcomes. Moreover, the trial will provide valuable information on the underlying plaque morphology and the response to different PCI strategies following the systematic use of intracoronary imaging. The central hypothesis of the study is that a DEB strategy, after IVL-based plaque modification in calcified nodules, is not inferior to DES implantation in terms of LLL and net gain, while potentially reducing the risk of long-term adverse events through improved biocompatibility and vessel healing. In addition, the analysis will be stratified according to nodule morphology, specifically differentiating eruptive vs non-eruptive CN, 2 entities that are thought to have distinct biological behavior and potentially different response to plaque modification and PCI.6,7,29,36 This stratified analysis may provide novel insights into the prognostic and therapeutic implications of nodule subtype and guide future individualized interventional strategies.
CONCLUSIONS
The DEBSCAN-IVL trial is an investigator-initiated, multicenter, open-label, prospective, randomized, controlled clinical trial designed to compare the safety and efficacy profile of the use of DEB or DES after IVL in CN. The co-primary endpoints are LLL and net gain at 9 ± 1 months of angiographic follow-up. The findings are expected to inform clinical decision-making and support a more individualized approach on the management of this specific type of calcified coronary disease.
DATA AVAILABILITY
This manuscript refers to the protocol of a study, therefore there is not available data related to this manuscript.
FUNDING
The DEBSCAN-IVL study was supported by non-restricted grants from Shockwave, Biotronik and Medtronic.
ETHICAL CONSIDERATIONS
The study was conducted in full compliance with the principles set forth in the Declaration of Helsinki. Institutional Ethics Committee approval was obtained, and all participants gave their written informed consent prior to enrollment. The confidentiality and anonymity of participants were strictly preserved throughout the study. Sex and gender considerations were addressed following the recommendations of the SAGER guidelines to ensure accurate and equitable reporting.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
Artificial intelligence assisted technologies were used exclusively to support language editing and improvement of style. No artificial intelligence tools were employed to generate, analyze, or interpret the data. The authors take full responsibility for the integrity, accuracy, and originality of the manuscript content.
AUTHORS’ CONTRIBUTIONS
A. Jurado-Román, M. Basile and R. Moreno drafted the manuscript. The remaining authors performed a critical review, and all authors approved the final version for publication.
CONFLICTS OF INTEREST
A. Jurado-Román is a proctor for Abbott, Boston Scientific, World Medica, and Philips; has received consulting fees from Boston Scientific and Philips; and has received speaker fees from Abbott, Boston Scientific, Shockwave Medical, Philips, and World Medica. J.M. Montero-Cabezas received a research grant from Shockwave Medical and speaker fees from Abiomed, Boston Scientific, and Penumbra Inc. A. Pérez de Prado reports receiving institutional research grants from Abbott and Shockwave Medical and speaker honoraria and consulting fees from iVascular, Boston Scientific, Terumo, B. Braun, and Abbott Vascular. I.J. Amat-Santos is proctor for Boston Scientific. A. Pérez de Prado, F. Alfonso and R. Moreno are associate editors of REC: Interventional Cardiology; the journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
WHAT IS KNOWN ABOUT THE TOPIC?
- CN are among the most complex calcified lesions for PCI, as DES often result in suboptimal expansion, malapposition, and long-term adverse events. IVL is an effective and safe technique for modifying nodular calcium. DEB have proven effective in complex lesions such as small vessel disease and in-stent restenosis, suggesting potential utility where stent implantation might be suboptimal. However, robust evidence on the safety and efficacy of DEB specifically for CN after IVL is currently lacking.
WHAT DOES THIS STUDY ADD?
- The DEBSCAN-IVL trial will be the first randomized study to compare DEB and DES after IVL in patients with CN. It will evaluate angiographic endpoints such as late lumen loss and net luminal gain, as well as procedural and clinical outcomes. The study is expected to provide crucial insights into whether a “leave-nothing-behind“ approach with DEB can achieve comparable efficacy to DES while potentially improving vessel healing and reducing longterm complications in this challenging patient population.
SUPPLEMENTARY DATA
REFERENCES
1. Jurado-Román A, Gómez-Menchero A, Gonzalo N, et al. Plaque modification techniques to treat calcified coronary lesions. Position paper from the ACI-SEC. REC Interv Cardiol. 2023;5:46-61.
2. Morofuji T, Kuramitsu S, Shinozaki T, et al. Clinical impact of calcified nodule in patients with heavily calcified lesions requiring rotational atherectomy. Catheter Cardiovasc Interv. 2021;97:10-19.
3. Lee T, Mintz GS, Matsumura M, et al. Prevalence, Predictors, and Clinical Presentation of a Calcified Nodule as Assessed by Optical Coherence Tomography. JACC Cardiovasc Imaging. 2017;10:883-891.
4. Lei F, Yin Y, Liu X, et al. Clinical Outcomes of Different Calcified Culprit Plaques in Patients with Acute Coronary Syndrome. J Clin Med. 2022;11:4018.
5. Mintz GS. Intravascular Imaging of Coronary Calcification and Its Clinical Implications. JACC Cardiovasc Imaging. 2015;8:461-471.
6. Torii S, Sato Y, Otsuka F, et al. Eruptive Calcified Nodules as a Potential Mechanism of Acute Coronary Thrombosis and Sudden Death. J Am Coll Cardiol. 2021;77:1599-1611.
7. Sato T, Matsumura M, Yamamoto K, et al. Impact of Eruptive vs Noneruptive Calcified Nodule Morphology on Acute and Long-Term Outcomes After Stenting. JACC Cardiovasc Interv. 2023;16:1024-1035.
8. Nagata T, Minami Y, Katsura A, et al. Optical coherence tomography factors for adverse events in patients with severe coronary calcification. Int J Cardiol. 2023;376:28-34.
9. Ali ZA, Nef H, Escaned J, et al. Safety and Effectiveness of Coronary Intravascular Lithotripsy for Treatment of Severely Calcified Coronary Stenoses:The Disrupt CAD II Study. Circ Cardiovasc Interv. 2019;12:e008434.
10. Kaihara T, Higuma T, Kotoku N, et al. Calcified Nodule Protruding Into the Lumen Through Stent Struts:An In Vivo OCT Analysis. Cardiovasc Revasc Med. 2020;21:116-118.
11. Kawai K, Akahori H, Imanaka T, et al. Coronary restenosis of in-stent protruding bump with rapid progression:Optical frequency domain imaging and angioscopic observation. J Cardiol Cases. 2019;19:12-14.
12. Isodono K, Fujii K, Fujimoto T, et al. The frequency and clinical characteristics of in-stent restenosis due to calcified nodule development after coronary stent implantation. Int J Cardiovasc Imaging. 2021;37:15-23.
13. Jeger RV, Eccleshall S, Wan Ahmad WA, et al. Drug-Coated Balloons for Coronary Artery Disease. JACC Cardiovasc Interv. 2020;13:1391-1402.
14. Jurado-Román A, Freixa X, Cid B, et al. Spanish cardiac catheterization and coronary intervention registry. 32nd official report of the Interventional Cardiology Association of the Spanish Society of Cardiology (1990-2022). Rev Esp Cardiol. 2023;76:1021-1031.
15. Basavarajaiah S, Loku Waduge BH, Watkin R, Athukorala S. Is a high calcific burden an indication, or a contraindication for Drug Coated Balloon?Rev Cardiovasc Med. 2021;22:1087-1093.
16. Shiraishi J, Kataoka E, Ozawa T, et al. Angiographic and Clinical Outcomes After Stent-less Coronary Intervention Using Rotational Atherectomy and Drug-Coated Balloon in Patients with De Novo Lesions. Cardiovasc Revasc Med. 2020;21:647-653.
17. Ho HH, Lee JH, Khoo DZL, Hpone KKS, Li KFC. Shockwave intravascular lithotripsy and drug-coated balloon angioplasty in calcified coronary arteries:preliminary experience in two cases. J Geriatr Cardiol. 2021;18:689-691.
18. Ito R, Ueno K, Yoshida T, et al. Outcomes after drug?coated balloon treatment for patients with calcified coronary lesions. J Intervent Cardiol. 2018;31:436-441.
19. Nagai T, Mizobuchi M, Funatsu A, Kobayashi T, Nakamura S. Acute and mid-term outcomes of drug-coated balloon following rotational atherectomy. Cardiovasc Interv Ther. 2020;35:242-249.
20. Rissanen TT, Uskela S, Siljander A, et al. Percutaneous Coronary Intervention of Complex Calcified Lesions With Drug?Coated Balloon After Rotational Atherectomy. J Intervent Cardiol. 2017;30:139-146.
21. Ueno K, Morita N, Kojima Y, et al. Safety and Long-Term Efficacy of Drug-Coated Balloon Angioplasty following Rotational Atherectomy for Severely Calcified Coronary Lesions Compared with New Generation Drug-Eluting Stents. J Intervent Cardiol. 2019;2019:1-10.
22. Iwasaki Y, Koike J, Ko T, et al. Comparison of drug-eluting stents vs drug-coated balloon after rotational atherectomy for severely calcified lesions of nonsmall vessels. Heart Vessels. 2021;36:189-199.
23. Rivero-Santana B, Jurado-Roman A, Galeote G, et al. Drug-eluting balloons in Calcified Coronary Lesions:A Meta-Analysis of Clinical and Angiographic Outcomes. J Clin Med. 2024;13:2779.
24. Muramatsu T, Kozuma K, Tanabe K, et al. Clinical expert consensus document on drug-coated balloon for coronary artery disease from the Japanese Association of Cardiovascular Intervention and Therapeutics. Cardiovasc Interv Ther. 2023;38:166-176.
25. Fezzi S, Scheller B, Cortese B, et al. Definitions and standardized endpoints for the use of drug-coated balloon in coronary artery disease:consensus document of the Drug Coated Balloon Academic Research Consortium. EuroIntervention. 2025;21:e1116-e1136.
26. Mehran R, Rao SV, Bhatt DL, et al. Standardized Bleeding Definitions for Cardiovascular Clinical Trials:A Consensus Report From the Bleeding Academic Research Consortium. Circulation. 2011;123:2736-2747.
27. Garcia-Garcia HM, McFadden EP, Farb A, et al. Standardized End Point Definitions for Coronary Intervention Trials:The Academic Research Consortium-2 Consensus Document. Circulation. 2018;137:2635-2650.
28. Johnson TW, Räber L, Di Mario C, et al. Clinical use of intracoronary imaging. Part 2:acute coronary syndromes, ambiguous coronary angiography findings, and guiding interventional decision-making:an expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. Eur Heart J. 2019;40:2566-2584.
29. Fernández-Cordón C, Brilakis ES, García-Gómez M, et al. Calcified nodules in the coronary arteries:systematic review on incidence and percutaneous coronary intervention outcomes. Rev Esp Cardiol. 2025;78:977-991.
30. Guagliumi G, Pellegrini D, Maehara A, Mintz GS. All calcified nodules are made equal and require the same approach:pros and cons. EuroIntervention. 2023;19:e110-e112.
31. Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC Guidelines for the management of acute coronary syndromes:Developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC). Eur Heart J. 2023;44:3720-3826.
32. Vrints C, Andreotti F, Koskinas KC, et al. 2024 ESC Guidelines for the management of chronic coronary syndromes:Developed by the task force for the management of chronic coronary syndromes of the European Society of Cardiology (ESC) Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2024;45:3415-3537.
33. Latib A, Colombo A, Castriota F, et al. A Randomized Multicenter Study Comparing a Paclitaxel Drug-eluting balloon With a Paclitaxel-Eluting Stent in Small Coronary Vessels. J Am Coll Cardiol. 2012;60:2473-2480.
34. Cannon LA, Simon DI, Kereiakes D, et al. The XIENCE nanoTM everolimus eluting coronary stent system for the treatment of small coronary arteries:The SPIRIT small vessel trial. Catheter Cardiovasc Interv. 2012;80:546-553.
35. Cortese B, Di Palma G, Guimaraes MG, et al. Drug-Coated Balloon Versus Drug-Eluting Stent for Small Coronary Vessel Disease. JACC Cardiovasc Interv. 2020;13:2840-2849.
36. Prati F, Gatto L, Fabbiocchi F, et al. Clinical outcomes of calcified nodules detected by optical coherence tomography:a sub-analysis of the CLIMA study. EuroIntervention. 2020;16:380-386.
37. Shin D, Dakroub A, Singh M, et al. Debulking Effect of Orbital Atherectomy for Calcified Nodule Assessed by Optical Coherence Tomography. Circ Cardiovasc Interv. 2024;17.
38. Ali ZA, Kereiakes D, Hill J, et al. Safety and Effectiveness of Coronary Intravascular Lithotripsy for Treatment of Calcified Nodules. JACC Cardiovasc Interv. 2023;16(9):1122-1124.
39. Madhavan MV, Alsaloum M, Maehara A, et al. Recurrent Calcified Nodule Protrusion Through Stent Struts After Percutaneous Coronary Intervention of the RCA. JACC Cardiovasc Interv. 2023;16:2463-2465.
40. Stone GW, Christiansen EH, Ali ZA, et al. Intravascular imaging-guided coronary drug-eluting stent implantation:an updated network meta-analysis. Lancet. 2024;403:824-837.
41. Amabile N, RangéG, Landolff Q, et al. OCT vs Angiography for Guidance of Percutaneous Coronary Intervention of Calcified Lesions:The CALIPSO Randomized Clinical Trial. JAMA Cardiol. 2025;10:666.
- Safety and efficacy profile of excimer laser coronary angioplasty for thrombus removal in STEMI
- Drug-coated balloons vs drug-eluting stents for the treatment of large native coronary artery disease. Meta-analysis of randomized controlled trials
- Heparin pretreatment for STEMI primary angioplasty: a meta-analysis
- Angiography-derived index versus fractional flow reserve for intermediate coronary lesions: a meta-analysis review





Interviews

An interview with Bruno Scheller
aServicio de Cardiología, Hospital Universitario de La Princesa, Instituto de Investigación Sanitaria de La Princesa (IIS-IP), Universidad Autónoma de Madrid, Spain
bCentro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain




