
Article
Ischemic heart disease and acute cardiac care
REC Interv Cardiol. 2019;1:21-25
Access to side branches with a sharply angulated origin: usefulness of a specific wire for chronic occlusions
Acceso a ramas laterales con origen muy angulado: utilidad de una guía específica de oclusión crónica
Servicio de Cardiología, Hospital de Cabueñes, Gijón, Asturias, España
ABSTRACT
Introduction and objectives: During the lockdown due to the pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a decrease in the number of admissions due to acute coronary syndrome (ACS) was observed. The objective of our study was to evaluate the impact lockdown had on the incidence, morbidity and mortality, and management of ACS.
Methods: A retrospective and multicenter study was conducted including patients admitted due to ACS from February 14 through June 24, 2020. Patients with acute myocardial infarction and coronary arteries without significant lesions were excluded. The following groups were established based on the period of admission: a) 1 month before lockdown; b) during lockdown; and c) 1 month after lockdown. The differences in mortality seen among the 3 groups were evaluated, as well as the temporal differences reported between symptom onset and the first medical contact (FMC).
Results: a total of 634 patients were included (group a, 205; group b, 303, and group c, 126). A 41% decrease in the number of admissions due to ACS was observed during the first month of lockdown compared to the previous month, as well as diagnostic delay during this same period (group a, 66 minutes (45-180), group b, 120 minutes (60-240), and group c, 120 minutes (60-240), P = .007). However, a higher mortality rate during confinement was not reported (RR, 1.26; 95%CI, 0.53-2.97; P = .60).
Conclusions: During lockdown, a remarkable decrease in the number of admissions due to ACS was observed, and although there was an increase in the time elapsed from symptom onset to the FCM in this period in patients with STEMI, the mortality rate was similar in the 3 groups studied.
Keywords: COVID-19. SARS-CoV-2. Acute coronary syndrome. Pandemic. Revascularization. Lockdown.
RESUMEN
Introducción y objetivos: Durante el confinamiento por la pandemia provocada por el coronavirus del síndrome respiratorio agudo grave de tipo 2 (SARS-CoV-2) se observó un descenso en los ingresos por síndrome coronario agudo (SCA). El objetivo de este estudio fue evaluar el impacto del confinamiento en la incidencia, la morbimortalidad y el tratamiento del SCA.
Métodos: Estudio retrospectivo y multicéntrico, en el que se incluyeron los pacientes ingresados por SCA entre el 14 de febrero y el 24 de junio de 2020. Se excluyeron los pacientes con infarto agudo de miocardio y coronarias sin lesiones significativas. Se establecieron 3 grupos en función del periodo de ingreso: a) 1 mes antes del confinamiento; b) durante el confinamiento; y c) 1 mes después del confinamiento. Se evaluaron las diferencias en la mortalidad entre los 3 grupos, así como las diferencias temporales entre el inicio de los síntomas y el primer contacto médico.
Resultados: Se incluyeron 634 pacientes (grupo A: 205; grupo B: 303; grupo C: 126). Se observó un descenso del 41% en los ingresos por SCA durante el primer mes del confinamiento respecto al mes previo, así como un retraso en el diagnóstico durante este mismo periodo: grupo A, 66 minutos (45-180); grupo B, 120 minutos (60-240); grupo C, 120 minutos (60-240) (p = 0,007). Sin embargo, no hubo mayor mortalidad durante el confinamiento (riesgo relativo, 1.26; intervalo de confianza del 95%, 0.53-2.97; p = 0,60).
Conclusiones: Durante el confinamiento se produjo un marcado descenso en los ingresos por SCA y, a pesar de que se dilató el tiempo desde el inicio de los síntomas hasta el primer contacto médico en este periodo en los pacientes con SCA con elevación del segmento ST, la mortalidad fue similar en los 3 grupos estudiados.
Palabras clave: COVID-19. SARS-CoV-2. Síndrome coronario agudo. Pandemia. Revascularización. Confinamiento.
Abbreviations
ACS: acute coronary syndrome. SARS-CoV-2: severe acute respiratory syndrome coronavirus 2. STEMI: ST-segment elevation myocardial infarction.
INTRODUCTION
By the end of December 2019, The People’s Republic of China reported the World Health Organization on the first cases detected of an unknown pneumonia caused by a new type of coronavirus in the City of Wuhan, China.1,2 Since then, the disease caused by this virus has spread rapidly bringing the healthcare systems of several countries to the point of collapse ultimately triggering dramatic preventive measures by the health authorities.
The pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has had a tremendous social, economic, and health impact across the world. Again and again, the healthcare setting has sustained several organizational and care changes that have triggered significant variations in the management therapeutic approach of the remaining diseases.3-5 Some studies have reported a lower number of admissions due to cardiovascular diseases, which has had a significant impact on morbidity and mortality alike.6-8
Pressure to the healthcare system due to COVID-19, the lockdown, and the lower demand for assistance are some of the reasons that may account for these changes. The objective of this study is to assess the rate of acute coronary syndrome (ACS) across the different stages of the pandemic in Spain, as well as the impact it has had on morbidity, mortality, and therapeutic management.
METHODS
Retrospective, observational, and multicenter study including data from patients admitted to 4 tertiary care centers of our country from 3 autonomous communities due to ACS from February 14, 2020 through June 24, 2020. Patients with ST-segment elevation acute coronary syndrome (STEACS), and non-ST-segment elevation acute coronary syndrome and were included. Patients with acute myocardial infarction and without significant lesions in coronary arteries were excluded. Patients were categorized into 3 groups based on the length of hospital stay: group A, from February 14 through March 14, 2020 (1 month before the lockdown); group B, from March 15 through May 24, 2020 (during the lockdown), and group C, from May 25 through June 24, 2020 (1 month after the stay-at-home lockdown). The patients’ baseline characteristics, acute complications, and cardiovascular events reported at the follow-up like all-cause mortality, cardiac death, stroke, reinfarction, stent thrombosis, and need for rehospitalization were recorded. In patients with STEACS the times elapsed between symptom onset and the first medical contact (FMC), and between electrocardiographic diagnosis until reperfusion were recorded. Clinical follow-up was completed back in July 25, 2020. Data curation was approved by the local ethics committee of each participant center.
The study primary endpoint was to assess the differences reported in all-cause mortality after 30 days since the onset of the acute coronary event among the 3 study groups. The study secondary endpoint was to analyze the differences reported in a composite of cardiac death, stroke, admission due to new ACS, stent thrombosis, and need for new revascularization. Complications reported after infarction at the follow-up, a high left ventricular ejection fraction, and revascularization times (from symptom onset until the first medical contact, and from diagnosis until reperfusion) were also studied in a secondary analysis and compared among the 3 groups.
Statistical analysis
Categorical variables were expressed as number and percentage using brackets and compared using the chi-square test or Fisher’s exact test, when appropriate. Continuous variables were expressed as mean and standard deviation or median and interquartile range in cases without a normal distribution. The Shapiro-Wilk test was used to assess the normal distribution of continuous variables that were compared using the analysis of variance (ANOVA) for independent samples or Kruskall-Wallis H test based on their normal distribution looking for differences among the 3 groups. Survival was studied using the Kaplan-Meier curves, and differences were assessed using the log-rank test. Cox proportional hazards regression analysis was used to assess the impact of group B (lockdown period) in the overall mortality of the patients. All estimates were performed using the statistical software package STATA version 15.1. P values < .05 were considered statistically significant.
RESULTS
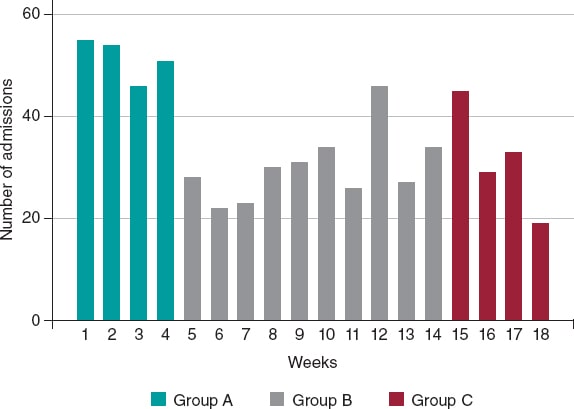
A total of 634 patients were included from February 14, 2020 through June 24, 2020. Of these, 205 were patients from group A, 303 from group B, and 126 from group C with a median follow-up of 98 days (63-137 days). The number of admissions due to ACS was 120, 138, and 151 within the first, second, and third months since the state of alarm declared. This lowered the rate of admissions due to ACS by 41%, 33%, and 26%, respectively compared to the rates reported 1 month before the lockdown for the same 30-day period (figure 1).
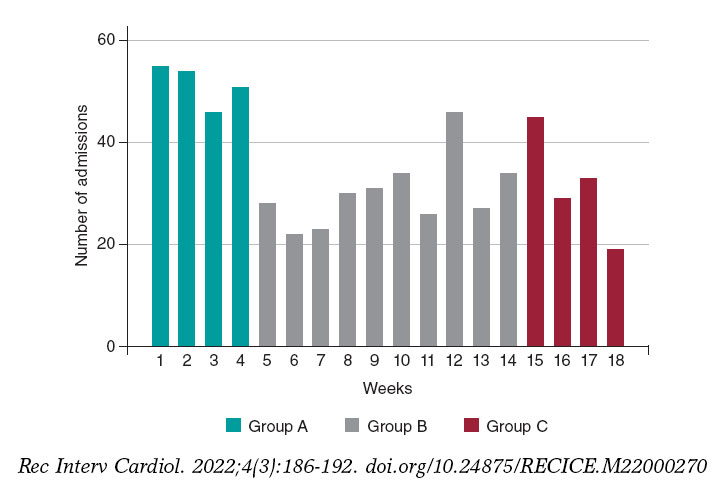
Figure 1. Absolute number of patients admitted due to acute coronary syndrome, expressed in weeks and categorized into group A, B, and C.
A total of 356 (56.2%) from the overall number of patients were admitted due to STEACS, and 278 (43.8%) due to non-ST-segment elevation acute coronary syndrome. The cohort baseline characteristics are shown on table 1. Patients admitted during the lockdown (group B) were younger (P = .012) and had lower levels of hypertension and dyslipidemia. On the other hand, these patients’ past medical history showed less ischemic heart disease, and coronary revascularization (P < .001).
Table 1. Baseline characteristics, diagnosis at admission, and treatment
| Variable | Total (N = 634) | Group A (N = 205) | Group B (N = 303) | Group C (N = 126) | P |
|---|---|---|---|---|---|
| Age | 66.3 ±12.6 | 67.4 ±11.6 | 64.8 ±12.7 | 68.2 ±13.6 | .012 |
| Sex, male | 494 (77.9) | 158 (77.1) | 241 (79.5) | 95 (75.4) | .603 |
| AHT | 400 (63.1) | 143 (69.8) | 176 (58.1) | 81 (64.3) | .027 |
| DM | 191 (30.1) | 71 (35.1) | 89 (29.4) | 30 (23.8) | .086 |
| DL | 368 (58.0) | 137 (66.8) | 164 (54.1) | 67 (53.2) | .008 |
| Smoking | 364 (57.4) | 124 (60.5) | 182 (60.1) | 58 (46.0) | .015 |
| PVD | 36 (5.7) | 15 (7.3) | 16 (5.3) | 5 (4.0) | .405 |
| Stroke | 37 (5.8) | 11 (5.4) | 16 (5.3) | 110 (7.9) | .531 |
| CKD (GF < 60) | 30 (4.7) | 18 (8.8) | 7 (2.3) | 5 (4.0) | .003 |
| COPD | 45 (7.1) | 14 (6.8) | 22 (7.3) | 9 (7.1) | .981 |
| AF | 40 (6.3) | 16 (7.8) | 16 (5.3) | 8 (6.4) | .517 |
| IHD | 150 (23.7) | 79 (38.5) | 46 (15.2) | 25 (19.8) | < .001 |
| AMI | 103 (16.3) | 52 (25.4) | 31 (10.2) | 20 (15.9) | < .001 |
| PCI | 117 (18.5) | 60 (29.3) | 36 (11.9) | 21 (16.7) | < .001 |
| CABG | 23 (3.6) | 12 (5.9) | 7 (2.3) | 4 (3.2) | .112 |
| Diagnoses | |||||
| UA | 83 (13.1) | 36 (17.6) | 27 (8.9) | 20 (15.9) | .003 |
| NSTEMI | 195 (30.8) | 67 (32.7) | 83 (27.4) | 45 (35.7) | .003 |
| STEACS | 356 (56.2) | 102 (49.8) | 193 (63.7) | 61 (48.4) | .003 |
| GRACE | 120.1 ±35.6 | 118.4 ±35.4 | 119.1 ±34.6 | 124.8 ±38.3 | .264 |
| CRUSADE | 31.4 ±13.8 | 34.1 ±15.2 | 30.4 ±13.3 | 29.7 ±11.8 | .001 |
| Cardiac catheterization | 616 (97.5) | 198 (96.6) | 295 (97.7) | 123 (98.4) | .565 |
| Emergency | 375 (59.5) | 112 (54.9) | 190 (63.1) | 73 (58.4) | .447 |
| Deferred | 242 (38.4) | 87 (42.7) | 105 (34.9) | 50 (40.0) | .447 |
| Fibrinolysis | 29 (5.1) | 10 (5.7) | 13 (4.5) | 6 (6.1) | .652 |
| PCI | 534 (94.3) | 165 (93.2) | 276 (95.2) | 93 (94.0) | .652 |
| CABG | 29 (4.6) | 11 (5.4) | 8 (2.7) | 10 (8.1) | .045 |
| LMCA or 3-vessel disease | 136 (21.5) | 52 (25.4) | 55 (18.6) | 29 (23.0) | .135 |
| CABG (LMCA or 3-vessels) | 22 (16.3) | 9 (17.7) | 3 (5.5) | 10 (34.5) | .003 |
| Conservative treatment | 3 (0.5) | 2 (1.1) | 1 (0.3) | 0 (0) | .652 |
| Complete revascularization | 456 (75.6) | 138 (74.6) | 223 (76.1) | 95 (76.0) | .926 |
| LVEF at discharge | 49.2 ±11.1 | 49.7 ±11.6 | 48.6 ±11.2 | 49.9 ±10.0 | .421 |
|
AF, atrial fibrillation; AHT, arterial hypertension; AMI, acute myocardial infarction; CABG, coronary artery bypass graft; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DL, dyslipidemia; DM, diabetes mellitus; GF, glomerular filtration; HT, arterial hypertension; IHD, ischemic heart disease; LMCA, left main coronary artery; LVEF, left ventricular ejection fraction; NSTEMI, non-ST-segment elevation myocardial infarction; PCI, percutaneous coronary intervention; PVD, peripheral vascular disease; STEACS, ST-segment elevation acute coronary syndrome; UA, unstable angina. Data are expressed as no. (%) or mean ± standard deviation. |
|||||
A diagnostic coronary angiography was performed on 97.1% of the cohort without any differences being reported regarding percutaneous coronary intervention throughout the different periods studied (P = .652); however, a significant reduction in the number of surgical coronary revascularizations performed during the lockdown was reported (group A, 5.4%; group B, 2.7%; group C, 8.1%; P = .045) including the subgroup of patients with left main coronary artery disease or 3-vessel disease (P = .003) (table 1).
A total of 36 deaths were reported, 22 of which were due to cardiovascular causes. No statistically significant differences were reported in the all-cause mortality rate after 30 days among the 3 groups (P = .327). According to a Cox regression analysis, being in the lockdown group (group B) was not associated with a higher all-cause mortality rate (P = .60). No survival differences were reported either among the 3 groups (figure 2).
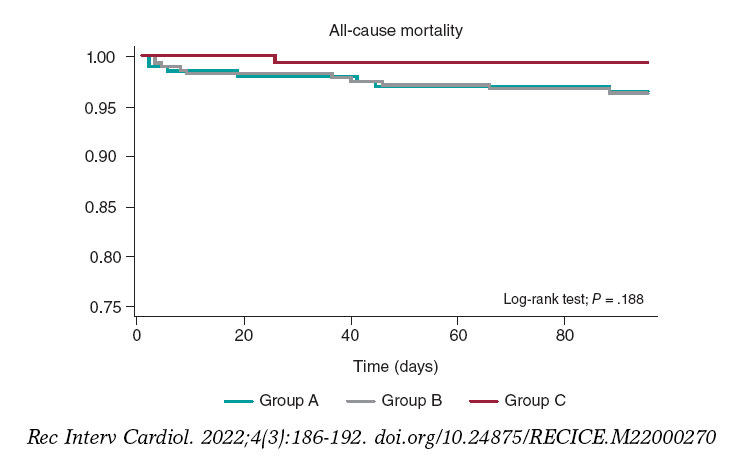
Figure 2. Kaplan-Meier survival curves for all-cause mortality in groups A (February 14-March 14), B (March 15-May 24), and C (May 25-June 24).
No significant differences were reported at the follow-up in a composite of cardiac death, stroke, readmission due to new ACS, stent thrombosis, and new revascularization (P = .120). The remaining clinical events at the follow-up are shown on table 2 and the in-hospital events on table 3.
Table 2. Clinical events at the follow-up
| Variable | Total (N = 634) | Group A (N = 205) | Group B (N = 303) | Group C (N = 126) | P |
|---|---|---|---|---|---|
| All-cause mortality | 36 (5.7) | 15 (7.3) | 13 (4.3) | 8 (6.4) | .327 |
| Cardiac death | 22 (64.7) | 7 (50) | 9 (75) | 6 (75) | .427 |
| Stroke | 20 (3.2) | 9 (4.4) | 8 (2.6) | 3 (2.4) | .551 |
| Re-AMI | 4 (0.7) | 1 (0.5) | 2 (0.7) | 1 (0.8) | 1.000 |
| Stent thrombosis | 12 (2.0) | 8 (4.1) | 1 (0.3) | 3 (2.4) | .006 |
| New revascularization | 6 (1.0) | 4 (2.0) | 2 (0.7) | 0 (0) | .259 |
| CV death + stroke + Re-AMI + stent thrombosis + new revascularization | 57 (9.0) | 24 (11.7) | 20 (6.6) | 13 (10.3) | .120 |
|
CV, cardiovascular; Re-AMI, new acute myocardial infarction. Data are expressed as no. (%). |
|||||
| Variable | Total (N = 634) | Group A (N = 205) | Group B (N = 303) | Group C (N = 126) | P |
|---|---|---|---|---|---|
| Inotropic agents | 53 (8.5) | 17 (8.4) | 27 (9.0) | 9 (7.2) | .836 |
| PM at admission | 12 (1.9) | 4 (2.0) | 8 (2.7) | 0 (0) | .188 |
| IABP | 11 (1.7) | 7 (3.4) | 4 (1.3) | 0 (0) | .048 |
| OTI | 41 (6.5) | 15 (7.3) | 21 (7.0) | 5 (4.0) | .444 |
| NIMV | 18 (2.9) | 6 (2.9) | 7 (2.3) | 5 (4.0) | .604 |
| RRT | 10 (1.6) | 6 (3) | 3 (1.0) | 1 (0.8) | .192 |
| AVB | 20 (3.2) | 7 (3.4) | 12 (4.0) | 1 (0.8) | .227 |
| SMVT | 18 (2.9) | 6 (2.9) | 9 (3.0) | 3 (2.4) | 1.000 |
| VF | 29 (4.6) | 12 (5.9) | 12 (4.0) | 5 (4.0) | .582 |
| AF at admission | 42 (6.7) | 11 (5.4) | 23 (7.6) | 8 (6.4) | .597 |
| BARC bleeding type > 3 | 16 (2.5) | 2 (1.0) | 9 (3.0) | 5 (4.0) | .161 |
| Infection | 57 (9.0) | 12 (6.0) | 28 (10.1) | 17 (11.0) | .184 |
| ARDS | 12 (1.9) | 1 (0.5) | 7 (2.5) | 4 (2.6) | .208 |
| Mechanical complications | 10 (1.6) | 3 (1.5) | 6 (2.0) | 1 (0.8) | .774 |
| Killip III or IV | 62 (9.8) | 20 (9.8) | 31 (10.3) | 11 (8.8) | .898 |
|
AF, atrial fibrillation; ARDS, acute respiratory distress syndrome; AVB, atrioventricular block; BARC, Bleeding Academic Research Consortium; IABP, intra-aortic balloon pump; NIMV, non-invasive mechanical ventilation; OTI, orotracheal intubation; PM, pacemaker; RRT, renal replacement therapy; SMVT, sustained monomorphic ventricular tachycardia; VF, ventricular fibrillation. Data are expressed as no. (%). |
|||||
Regarding delay times, significant differences were reported among the different groups with longer times elapsed between symptom onset and the first medical contact during (group B) and after lockdown (group C) compared to the previous period (group A): group A, 66 min (45-180), group B, 120 min (60-240), group C, 120 min (60-240); P = .007). The time elapsed between symptom onset until the first medical contact was similar in groups B and C (P = .7102). Finally, the time elapsed between diagnosis and reperfusion was shorter in patients from group C (P = .025) compared to the remaining cohort (table 4).
Table 4. Times between symptom onset and the first medical contact, and between electrocardiographic diagnosis and reperfusion (guidewire passage), in minutes, in the cohort of patients with ST-segment elevation acute coronary syndrome
| Variable | Total | Grupo A | Grupo B | Grupo C | p |
|---|---|---|---|---|---|
| Symptom onset-first medical contact (N = 332) | 120 [60-240] | 66 [45-180] (N = 97) | 120 [60-240] (N = 180) | 120 [60-240] (N = 55) | .007 |
| Diagnosis-reperfusion (N = 322) | 120 [60-180] | 120 [60-186] (N = 93) | 120 [60-225] (N = 176) | 60 [60-120] (N = 53) | .025 |
|
Data are expressed as median [interquartile range]. |
|||||
DISCUSSION
The main findings from this study were a lower number of admissions due to ACS within the first few months of lockdown, and longer periods of time elapsed between symptom onset and the first medical contact in patients with STEACS that did not translate into higher morbidity and mortality rates.
Lower rate of acute coronary syndrome
Former studies have reported less activity at the cath lab due to fewer admissions due to ACS during the pandemic, especially in the STEACS setting.7,9-11 Our findings confirm this trend with a significant 41% drop within the first 30 days compared to the previous month. This reduction was kept in the remaining time during and after lockdown; however, as the isolation measures were being lifted and the rate of cases of COVID-19 dropped, a gradual increase in the number of admissions due to ACS was confirmed. One of the contributing factors may have been the intense pressure put to the healthcare system within the first few months of lockdown with the corresponding underdiagnosis of ACS and fewer admissions reported.12 Another hypothesis that may justified the lower rate of ACS during this time is the higher number of out-of-hospital sudden deaths reported. Although reported by other authors in the past, this was not cause for analysis in our study.13-16
Times elapsed among symptom onset, the first medical contact, and revascularization in patients with ST-segment elevation myocardial infarction, and association with adverse events
During the lockdown (group B) patients with STEACS were admitted more often (P = .003). The time elapsed between symptom onset and the first medical contact was significantly longer during this time compared to other times, which is consistent with the peak number of cases reported (similar findings to those reported by former studies);17 however, this delay did not increase the rates of mechanical complications or mortality. This can be explained because patients admitted during the lockdown (group B) were younger and had fewer comorbidities.18,19 Data suggests that elderly patients with more serious past medical histories and associated comorbidities may have delayed or even postponed indefinitely their access to the healthcare system over fears of getting infected.20,21
Rodríguez-Leor et al.22 reported time delays between symptom onset and the first medical contact, and similar times between diagnosis and reperfusion. This delay was associated with a higher mortality rate during the pandemic (7.5% vs 5.1%), which contradicts our findings. The lack of a direct association between time delays until diagnosis and the appearance of adverse events is not easy to explain. However, a plausible hypothesis can be the higher number of out-of-hospital sudden deaths reported due to mechanical complications or malignant arrhythmias followed by the corresponding selection bias since this study included hospitalized patients only.
Therapeutic strategies: percutaneous coronary intervention and surgical revascularization
No differences were found regarding the percutaneous invasive management of patients with ACS before, during or after lockdown. This data is consistent with most studies published on the management of ACS during the pandemic.12,22
However, we should mention the significant decrease of myocardial revascularization procedures despite the non-negligible number of patients with left main coronary artery disease or 3-vessel disease. A total of 17.7% of these patients were treated with myocardial revascularization 1 month before the lockdown, only 5.5% during the lockdown, and 34.5% the following month. Although some registries confirm the lower number of coronary artery bypass grafts performed,23 this tendency has not been confirmed in other studies.18,23
The fact that fewer myocardial revascularization procedures were performed during the lockdown can be explained by the overall tendency to delay any surgical acts as much as possible during these months, something already hypothesized in other studies.24
Limitations
This study has some limitations associated with the analysis of multicenter and observational data. Also, the study short follow-up period may have prevented the finding of potential consequences or differential events among the study groups. The lack of information on cases of ACS treated during the pandemic that never really made it to tertiary care centers also casts a shadow over the conclusions that can be drawn.
CONCLUSIONS
Significantly fewer admissions due to ACS were reported during the lockdown. Also, although time between symptom onset and the first medical contact was longer during this period in patients with STEACS, the mortality rate was similar among the 3 study groups.
FUNDING
None reported.
AUTHORS’ CONTRIBUTIONS
J. Echarte-Morales: clinical data mining, manuscript drafting, project design, and management of the study. C. Minguito-Carazo: data analysis, manuscript drafting and revision process. PL Cepas-Guillén, V. Vallejo García, ID. Poveda Pinedo, A. Salazar Rodríguez, E. Arbas Redondo, J. Guzmán Bofarull, and D. Tebar Márquez: data mining and manuscript revision process. E. Sánchez Muñoz: data mining. E. Martínez Gómez: data mining, manuscript drafting and revision process. T. Benito-González: statistical counselling, and manuscript revision process. M. López Benito, A. Viana Tejedor, I. Cruz-González, PL Sánchez Fernández, M. Sabaté, and F. Fernández-Vázquez: project organization. Authors submitting this manuscript accept full responsibility for its content as defined by the International Committee of Medical Journal Editors (ICMJE).
CONFLICTS OF INTEREST
None whatsoever.
WHAT IS KNOWN ABOUT THE TOPIC?
- Admissions due to STEACS decreased during the lockdown.
- More mechanical complications were reported during the pandemic due to delayed treatments.
WHAT DOES THIS STUDY ADD?
- Unlike former studies that mainly focused on patients with STEACS, this study includes patients admitted before, during, and 1 month after lockdown with a diagnosis of ACS (including STEACS and non-ST-segment elevation acute coronary syndrome).
- Fewer myocardial revascularization procedures were performed during the lockdown despite the growing number of patients with left main coronary artery disease or 3-vessel disease.
- Although time between symptom onset and the first medical contact was longer in the group of patients with STEACS, the mortality rate was similar before, during, and after lockdown, as it happened with mechanical complications.
REFERENCES
1. WHO. World Health Organization. Pneumonia of Unknown Cause –China. 2020. Available online:https://www.who.int/emergencies/disease-outbreak-news/item/2020-DON229. Accessed 20 Sep 2021.
2. Zhu N, Zhang D, Wang W, et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med. 2020;382:727-733.
3. Morelli N, Rota E, Terracciano C, et al. The Baffling Case of Ischemic Stroke Disappearance from the Casualty Department in the COVID-19 Era. Eur Neurol. 2020;83:213-215.
4. Babu N, Kohli P, Mishra C, et al. To evaluate the effect of COVID-19 pandemic and national lockdown on patient care at a tertiary-care ophthalmology institute. Indian J Ophthalmol. 2020;68:1540-1544.
5. De Vincentiis L, Carr RA, Mariani MP, Ferrara G. Cancer diagnostic rates during the 2020 âlockdown', due to COVID-19 pandemic, compared with the 2018-2019:An audit study from cellular pathology. J Clin Pathol. 2021;74:187-189.
6. De Rosa S, Spaccarotella C, Basso C, et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur Heart J. 2020;41:2083-2088.
7. Rodríguez-Leor O, Cid-Álvarez B, Ojeda S, et al. Impacto de la pandemia de COVID-19 sobre la actividad asistencial en cardiología intervencionista en España. REC Interv Cardiol. 2020;2:82-89.
8. Romaguera R, Cruz-González I, Jurado-Román A, et al. Consideraciones sobre el abordaje invasivo de la cardiopatía isquémica y estructural durante el brote de coronavirus COVID-19. REC Interv Cardiol. 2020;2:112-117.
9. Garcia S, Albaghdadi MS, Meraj PM, et al. Reduction in ST-Segment Elevation Cardiac Catheterization Laboratory Activations in the United States During COVID-19 Pandemic. J Am Coll Cardiol. 2020;75:2871-2872.
10. Metzler B, Siostrzonek P, Binder RK, Bauer A, Reinstadler SJ. Decline of acute coronary syndrome admissions in Austria since the outbreak of COVID-19:The pandemic response causes cardiac collateral damage. Eur Heart J. 2020;41:1852-1853.
11. Pessoa-Amorim G, Camm CF, Gajendragadkar P, et al. Admission of patients with STEMI since the outbreak of the COVID-19 pandemic:A survey by the european society of cardiology. Eur Heart J Qual Care Clin Outcomes. 2020;6:210-216.
12. Salinas P, Travieso-González A, Vergara-Uzcategui CE, Macaya F, Núñez-Gil IJ, Fernández-Ortiz A. Relación temporal entre ingresos por síndrome coronario agudo con tratamiento invasivo y confinamiento durante la pandemia de COVID-19. REC Interv Cardiol. 2020;2:307-309
13. Laura E. Wong;MD;PhD;Jessica E. Hawkins;MSEd;Simone Langness;Karen L. Murrell;Patricia Iris;MD &Amanda Sammann;MPH. Where Are All the Patients?Addressing Covid-19 Fear to Encourage Sick Patients to Seek Emergency Care. NEJM Catal. 2020. Available online:https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0193. Accessed 20 Sep 2021.
14. Lai PH, Lancet EA, Weiden MD, et al. Characteristics Associated with Out-of-Hospital Cardiac Arrests and Resuscitations during the Novel Coronavirus Disease 2019 Pandemic in New York City. JAMA Cardiol. 2020;5:1154-1163.
15. Marijon E, Karam N, Jost D, et al. Out-of-hospital cardiac arrest during the COVID-19 pandemic in Paris, France:a population-based, observational study. Lancet Public Health. 2020;5:e437-e443.
16. Baldi E, Sechi GM, Mare C, et al. Out-of-Hospital Cardiac Arrest during the Covid-19 Outbreak in Italy. N Engl J Med. 2020;383:496-498.
17. Tam CCF, Cheung KS, Lam S, et al. Impact of Coronavirus Disease 2019 (COVID-19) Outbreak on ST-Segment-Elevation Myocardial Infarction Care in Hong Kong, China. Circ Cardiovasc Qual Outcomes. 2020;13:e006631.
18. Gluckman TJ, Wilson MA, Chiu ST, et al. Case Rates, Treatment Approaches, and Outcomes in Acute Myocardial Infarction during the Coronavirus Disease 2019 Pandemic. JAMA Cardiol. 2020;5:1419-1424.
19. Wu J, Mamas M, Rashid M, et al. Patient response, treatments, and mortality for acute myocardial infarction during the COVID-19 pandemic. Eur Heart J Qual Care Clin Outcomes. 2021;7:238-246.
20. Franchini S, Spessot M, Landoni G, et al. Stranger months:How SARS-CoV-2, fear of contagion, and lockdown measures impacted attendance and clinical activity during February and March 2020 at an urban Emergency Department in Milan. Disaster Med Public Health Prep. 2020;15(5):e33-e42.
21. Baldi E, Savastano S. Fear of contagion:One of the most devious enemies to fight during COVID-19 pandemic. Disaster Med Public Health Prep. 2021;15:e8-e9.
22. Rodríguez-Leor O, Cid-Álvarez B, Pérez de Prado A, et al. Impact of COVID-19 on ST-segment elevation myocardial infarction care. The Spanish experience. Rev Esp Cardiol. 2020;73:994-1002.
23. Mafham MM, Spata E, Goldacre R, et al. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England. Lancet. 2020;39:381-389.
24. Álvarez Gallego M, Gortázar de las Casas S, Pascual Migueláñez I, et al. SARS-CoV-2 pandemic on the activity and professionals of a General Surgery and Digestive Surgery Service in a tertiary hospital. Cir Esp. 2020;98:320-327.
ABSTRACT
Introduction and objectives: Coronary artery disease and mental health disorders are often coexistent. Selective serotonin reuptake inhibitors (SSRIs) are often used in this context but have been associated with an increased risk of bleeding due to platelet dysfunction. Previous studies have assessed this risk in patients treated with clopidogrel-based dual antiplatelet therapy (DAPT) with contradictory results. However, there is no data regarding the use of SSRIs and potent P2Y12 inhibitors or triple antithrombotic therapy after percutaneous coronary intervention (PCI). The purpose of this study was to assess the impact of SSRIs on bleeding outcomes after PCI in patients treated with clopidogrel, prasugrel or ticagrelor-based DAPT or triple antithrombotic therapy.
Methods: Retrospective study including all patients undergoing PCI at a high-volume center during 2018. Patients on SSRIs were propensity-score-matched on a 1:1 ratio with patients naive to SSRIs adjusting for the baseline differences. The primary endpoint was major bleeding (BARC type 3 or 5 bleeding) at the 1-year follow-up. Secondary endpoints were a composite of major/non-major clinically relevant bleeding (BARC type 2, 3 or 5 bleeding), and a composite of major adverse cardiovascular events.
Results: Out of a total of 1063 patients treated with PCI during the study period, 1002 met the selection criteria, and 139 (13.9%) were on SSRIs. The latter had a higher bleeding risk before matching [PRECISE-DAPT, 16 [10-24] vs 13 [9-21]; P = .040]. No differences were reported in major bleeding (2.9% vs 2.9%, P = .991), major/non-major clinically relevant bleeding (2.9% vs 7.2%, P = .120) or in major adverse cardiovascular events (7.9% vs 7.9%, P = .979) in patients treated with SSRIs.
Conclusions: The use of SSRIs was frequent in patients treated with PCI, and although it was a marker of a higher bleeding risk at baseline, this was not associated with an additional bleeding liability.
Keywords: Bleeding. Coronary artery disease. Percutaneous coronary intervention. Selective serotonin reuptake inhibitors. Antithrombotic therapy.
RESUMEN
Introducción y objetivos: La cardiopatía isquémica y la enfermedad mental coexisten a menudo. Los inhibidores selectivos de la recaptación de serotonina (ISRS) se utilizan con frecuencia en este contexto, pero se han asociado con un incremento en el riesgo hemorrágico. Los estudios previos han evaluado este fenómeno en pacientes tratados con clopidogrel, con resultados contradictorios. No hay datos sobre el uso de ISRS e inhibidores del P2Y12 potentes o triple terapia antitrombótica. El objetivo de este estudio fue examinar el impacto de los ISRS en los eventos hemorrágicos en pacientes tratados con doble (incluyendo clopidogrel, prasugrel o ticagrelor) o triple terapia antitrombótica tras una intervención coronaria percutánea (ICP).
Métodos: Estudio retrospectivo en el que se incluyeron todos los pacientes tratados con ICP en un centro de alto volumen durante 2018. Los pacientes en tratamiento con ISRS fueron emparejados mediante puntaje de propensión con pacientes sin ISRS. El objetivo primario fue el sangrado mayor al año de seguimiento (BARC 3 o 5). Los objetivos secundarios fueron un combinado de sangrado mayor o menor clínicamente relevante (BARC 2, 3 o 5) y un combinado de eventos cardiovasculares adversos mayores.
Resultados: De los 1.063 pacientes tratados con ICP durante el periodo del estudio, 1.002 cumplieron los criterios de selección y 139 (13,9%) recibían ISRS. Los pacientes con ISRS tenían un mayor riesgo de sangrado antes del emparejamiento (PRECISE-DAPT: 16 [10-24] frente a 13 [9-21]; p = 0,040). No hubo diferencias en el objetivo primario (2,9% frente a 2,9%; p = 0,991) ni en los objetivos secundarios de sangrado mayor o menor clínicamente relevante (2,9 frente a 7,2%; p = 0,120) y eventos cardiovasculares adversos mayores (7,9 frente a 7,9%; p = 0,979).
Conclusiones: El uso de ISRS fue frecuente en los pacientes tratados con ICP, y aunque fue un marcador de riesgo hemorrágico basal, no se asoció con un mayor riesgo de sangrado en el seguimiento.
Palabras clave: Sangrado. Enfermedad coronaria. Intervencionismo coronario percutáneo. Inhibidores selectivos de la recaptación de serotonina. Terapia antitrombótica.
Abbreviations
DAPT: dual antiplatelet therapy. PCI: percutaneous coronary intervention. SSRIs: selective serotonin reuptake inhibitors.
INTRODUCTION
Coronary artery disease and mental health disorders frequently coexist and have a bidirectional relationship.1,2 Patients with mental health disorders have an increased risk of coronary artery disease and, inversely, it is not rare for patients to experience symptoms of depression or anxiety after a cardiac event.3 Moreover, depression in patients with CHD is associated with a poor adherence to treatment, unhealthy lifestyle habits, and a poor prognosis.4-8
Selective serotonin reuptake inhibitors (SSRIs) are often prescribed as first-line agents to treat depression and anxiety,9,10 but have a potential for increased bleeding risk due to the concomitant inhibitory effect on the platelet serotonin reuptake transporter (5-HTT).11 Platelet 5-HTT inhibition has been associated with a reduced platelet activation and aggregation, and with a prolonged bleeding time.12,13 On the other hand, some studies have linked SSRI-related bleeding risk to older age, comorbidities or polypharmacy.14,15
Bleeding risk due to antithrombotic therapy is a major concern following percutaneous coronary intervention (PCI) as hemorrhagic events are prognostically unfavorable as recurrent ischemic events.16,17 While bleeding risk depends on multiple clinical and laboratory features,18,19 the identification of potential modifiable factors is key to optimize the balance between ischemic and bleeding risk.20 Prior studies have evaluated the bleeding risk of patients with a concomitant treatment of SSRIs and dual antiplatelet therapy (DAPT) plus aspirin and clopidogrel with contradictory results.21-23 However, the impact of SSRIs plus therapy with more potent P2Y12 inhibitors (eg, ticagrelor or prasugrel) or triple antithrombotic therapy with DAPT plus an oral anticoagulant (OAC) has never been explored. In this study we tried to compare the 1-year risk of bleeding after PCI and concomitant guideline-recommended antithrombotic therapy (including clopidogrel, ticagrelor or prasugrel-based DAPT and triple antithrombotic therapy) in patients with or without prescribed SSRIs.
METHODS
Study design and setting
Retrospective study including all consecutive patients discharged after PCI performed at a single center during 2018. Those treated with SSRIs were propensity score-matched (PSM) to a control group to compare bleeding outcomes at the 1-year follow-up. Antithrombotic treatment was decided by the clinical cardiologist in accordance with the current clinical practice guidelines.24 This study was conducted according to the Declaration of Helsinki and was approved by the local clinical research ethics committee. Written informed consent was obtained from all patients before the PCI.
Population
All patients discharged after the PCI performed during the study period were eligible. Those treated at discharge with single antiplatelet therapy, DAPT were excluded—not including acetylsalicylic acid—as well as those anticoagulated with low-molecular-weight heparin for other reasons. Patients with missing information at the follow-up were also excluded. Clinical and procedural data, treatment at discharge, and outcomes during the first year were reviewed through electronic health records. Patients were treated with SSRIs if their list of prescriptions at discharge included one of the following: citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine or sertraline.
Endpoints
The primary safety endpoint was major bleeding at the 1-year follow-up. Secondary endpoints were a composite of major or non-major clinically relevant bleeding, and a composite of major adverse cardiovascular events (MACE). Major bleeding was defined as a bleeding event type 3 or 5 according to the Bleeding Academic Research Consortium (BARC). Major/non-major clinically relevant bleeding was defined as BARC type 2, 3 or 5 bleeding event.25 MACE was defined as a composite outcome of cardiovascular death, non-fatal myocardial infarction or unplanned revascularization. Events were independently adjudicated by 2 cardiologists who were unaware of the SSRIs group.
Statistical analysis
Categorical variables were expressed as counts (percentages), and the continuous ones as mean ± standard deviation or median [interquartile range] according to their distribution assessed using the Shapiro-Wilk test. P values were obtained using the chi-square test or the Mann-Whitney U test, as appropriate. PSM was conducted to account for the confounding biases.26 Logistic regression was used to determine the probability of being treated with SSRIs and included the following confounding variables potentially associated with SSRIs treatment and the primary endpoint:27 age, sex, prior relevant bleeding, hypertension, cancer, past medical history of hematologic disease or anemia, liver disease, creatinine clearance, treatment with potent P2Y12 inhibitors or concomitant OAC. The nearest neighbor matching method with no replacement, and a caliper width of 0.1 were used in the PSM on a 1:1 ratio. Propensity score histograms and standardized mean differences before and after the PSM were used to evaluate the balance of the groups regarding the covariates.28 Time-to-event analyses were conducted using the Kaplan-Meier and Cox proportional hazards methods. To determine major bleeding predictors in the unmatched cohort, a multivariate Cox regression model was conducted that used a purposeful selection model and prioritized parsimony. Clinical meaningful variables and those showing P values < 0.2 in the univariate analysis were included. Statistical analyses were performed using SPSS software (version 24; IBM Corp., United States) and R software (version 4.0.3; R Foundation for Statistical Computing, Austria). Matching was performed using the MatchIt R package (Ho, Imai, King, & Stuart, 2011) while covariate balance was assessed using the Cobalt R package (Greifer, 2021).
RESULTS
Baseline clinical characteristics
A total of 1063 patients were treated with PCI during the study period, 1002 of whom met the selection criteria and were included in the analysis. A total of 139 patients (13.9%) were treated with SSRIs at discharge (figure 1). Median age was 66 years (58-75), and 745 patients (74.4%) were male with a median PRECISE-DAPT score of 13 [9-22]. Regarding antithrombotic therapy, 684 patients (68.3%) were treated with potent P2Y12 inhibitors and 102 (10.2%) were concomitantly treated with OAC. The baseline clinical characteristics of the overall population and the unmatched groups are shown on table 1. Patients from the SSRIs group were more likely to be women. They also had a more extensive past medical history of hypertension, diabetes mellitus, cancer, significant bleeding, and hematologic disease or anemia. Both the HAS-BLED and the PRECISE-DAPT bleeding risk scores were higher in the SSRIs group.
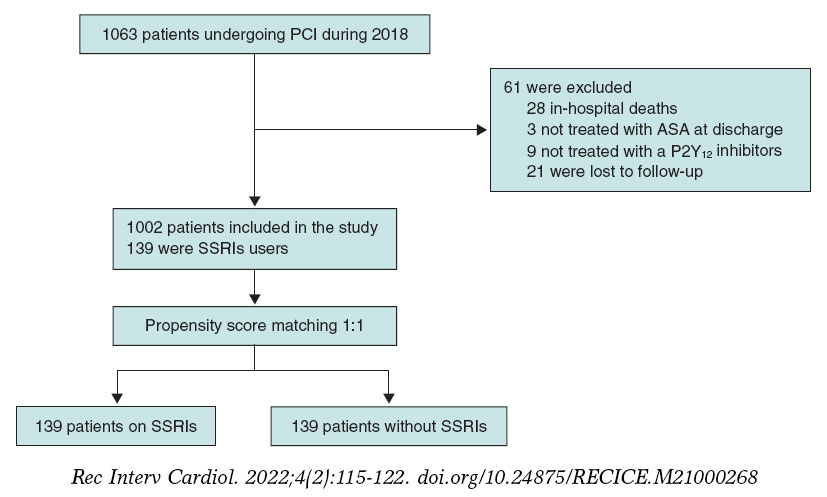
Figure 1. Patient flowchart. PCI, percutaneous coronary intervention; SSRIs, selective serotonin reuptake inhibitors.
Table 1. Baseline clinical characteristics of the overall population, and SSRIs/non-SSRIs users before matching
| Variable | Overall (N = 1002) | SSRI (N = 139) | Non-SSRI (N = 863) | P |
|---|---|---|---|---|
| Age, years | 66 [58-75] | 67 [60-76] | 66 [57-75] | .530 |
| Sex, male | 745 (74.4) | 76 (54.7) | 669 (77.5) | .001* |
| BMI | 28.7 [25.9-31.8] | 30.0 [25.8-32.0] | 28.6 [25.9-31.7] | .067 |
| Hypertension | 688 (68.7) | 112 (80.6) | 576 (66.7) | .001* |
| Diabetes mellitus | 370 (36.9) | 64 (46.0) | 306 (35.5) | .017* |
| Hyperlipidemia | 525 (52.4) | 83 (59.7) | 442 (51.2) | .059 |
| Smoking (current or former) | 260 (25.9) | 34 (24.5) | 226 (26.2) | .709 |
| Previous revascularization | 248 (24.8) | 41 (29.5) | 207 (24.0) | .174 |
| COPD | 67 (6.7) | 10 (7.2) | 57 (6.6) | .740 |
| Chronic kidney disease | 115 (11.5) | 17 (12.2) | 98 (11.4) | .774 |
| Cancer | 98 (9.8) | 20 (14.4) | 78 (9.0) | .044* |
| Liver disease | 37 (3.7) | 8 (5.8) | 29 (3.4) | .166 |
| Hematologic disease or anemia | 99 (9.9) | 25 (18) | 74 (8.6) | .001* |
| Previous relevant bleeding | 31 (3.1) | 9 (6.5) | 22 (2.5) | .010* |
| Atrial fibrillation | 87 (8.7) | 11 (7.9) | 76 (8.8) | .871 |
| Oral anticoagulant | 102 (10.2) | 9 (6.5) | 93 (10.8) | .119 |
| Potent P2Y12 inhibitors | 684 (68.3) | 90 (64.7) | 594 (68.8) | .323 |
| Ticagrelor, no. (%) | 660 (65.9) | 86 (61.8) | 574 (66.5) | .543 |
| Prasugrel | 24 (2.4) | 4 (2.9) | 20 (2.3) | .543 |
| DAPT duration (months) | 8 [6-12] | 6 [6-12] | 8 [6-12] | .440 |
| PRECISE-DAPT | 13 [9-22] | 16 [10-24] | 13 [9-21] | .040* |
| PRECISE-DAPT ≥ 25 | 195 [19.5] | 34 [24.5] | 161 [18.7] | .109 |
| HAS-BLED | 2 (2-3) | 3 (2-3) | 2 (2-3) | .034* |
| Creatinine clearance, mL/min/1.73 m2 | 100 [82.3-124.1] | 94.8 [72.9-125.2] | 100 [82.7-124.1] | .154 |
| Clinical presentation | ||||
| CCS | 441 (44.0) | 66 (47.5) | 375 (43.5) | .375 |
| ACS | 561 (56.0) | 73 (52.5) | 488 (56.5) | |
|
ACS, acute coronary syndrome; BMI, body mass index (kg/m2); CCS, chronic coronary syndrome; COPD, chronic obstructive pulmonary disease; DAPT, dual antiplatelet therapy; SSRI, selective serotonin reuptake inhibitors. Data are expressed as no. (%), mean ± standard deviation or median [interquartile range]. * Indicates a statistically significant difference with P values < .05. |
||||
Unmatched analysis
In the overall population there were a total of 19 major bleeding events at the 1-year follow-up: 4 (2.9%) in the SSRIs group, and 15 (1.7%) in the unmatched non-SSRIs group (P = .350). Of these, 4 (21.1%) were fatal, 10 (52.6%) GI bleedings, 4 (21.1%) intracranial bleedings while the remaining ones occurred in other locations.
The multivariable Cox model identified the following independent predictors for the primary endpoint of major bleeding: PRECISE-DAPT score ≥ 25, and concomitant anticoagulation. Table 2 shows the univariable and multivariable Cox predictors for the primary endpoint.
Table 2. Univariable and multivariable Cox predictors for major bleeding
| Variable | Univariable analysis | Multivariable analysis | ||
|---|---|---|---|---|
| HR (95%CI) | P | HR (95%CI) | P | |
| Age, years | 1.06 (1.02-1.11) | .008 | ||
| Sex, male | 0.47 (0.19-1.18) | .107 | ||
| BMI | 0.98 (0.89-1.09) | .756 | ||
| Hypertension | 0.99 (0.38-2.61) | .989 | ||
| Diabetes mellitus | 1.91 (0.78-4.79) | .160 | ||
| Hyperlipidemia | 0.82 (0.33-2.01) | .664 | ||
| Chronic kidney disease | 3.67 (1.39-9.66) | .008 | ||
| Cancer | 2.47 (0.82-7.46) | .107 | ||
| Liver disease | 1.48 (0.19-11.05) | .705 | ||
| Hematologic disease or anemia | 2.47 (0.82-7.46) | .107 | ||
| Previous relevant bleeding | 3.91 (0.90-16.91) | .068 | ||
| Atrial fibrillation | 5.45 (2.05-14.53) | .001 | ||
| Oral anticoagulant | 8.22 (3.34-20.23) | .001 | 6.99 (2.78-17.64) | .001 |
| Potent P2Y12 inhibitors | 0.16 (0.06-0.45) | .001 | ||
| PRECISE-DAPT ≥ 25 | 4.77 (1.94-11.75) | .001 | 3.59 (1.44-8.98) | .006 |
| HAS-BLED | 1.69 (1.17-2.43) | .005 | ||
| Creatinine clearance | 0.98 (0.97-0.99) | .024 | ||
| SSRI | 1.68 (0.56-5.07) | .356 | 1.95 (0.64-5.93) | .241 |
|
95%CI, 95% confidence interval; BMI, body mass index (kg/m2); HR, hazard ratio; SSRI, selective serotonin reuptake inhibitors. |
||||
The major/non-major clinically relevant bleeding endpoint occurred in 4 patients (2.9%) from the SSRIs group, and in 43 patients (4.9%) from the unmatched no-SSRIs group (P = .290). The rate of MACE was similar in both groups: 11 events (7.9%) in the SSRIs group and 50 events (5.8%) in the non-SSRIs group.
The Kaplan-Meier curves and the associated risk tables for each endpoint of the unmatched cohorts are shown on figure 2.
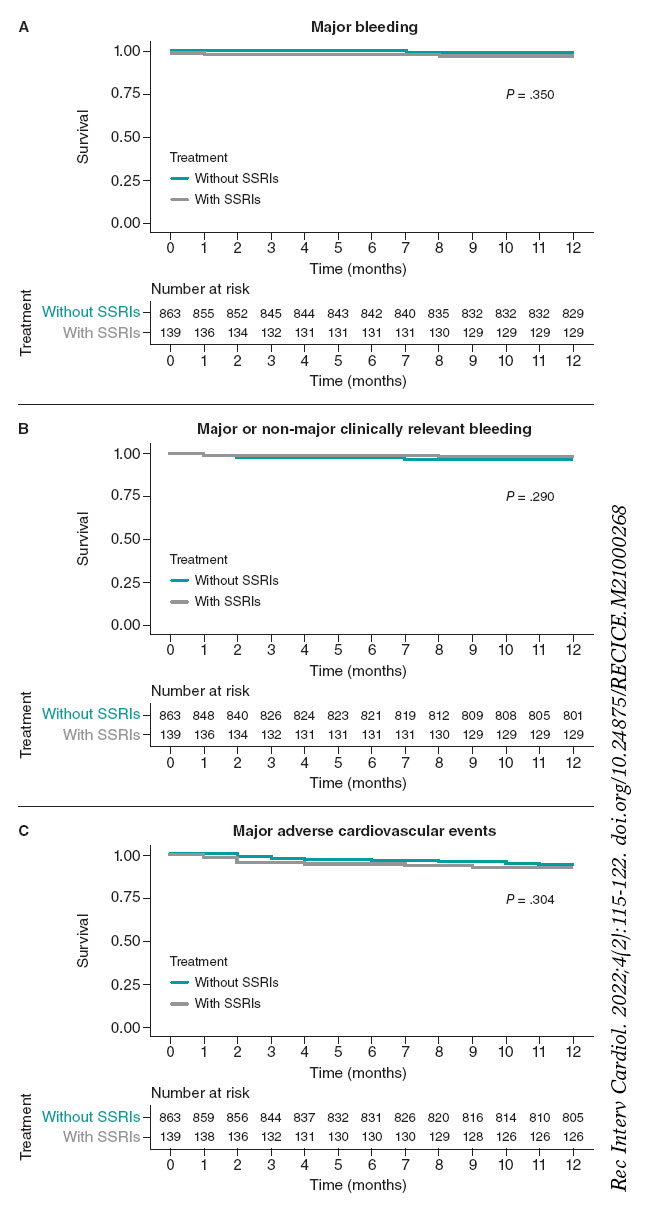
Figure 2. Kaplan-Meier curves for the primary bleeding outcome (A), the secondary composite bleeding (B), and the ischemic outcomes (C). Unmatched cohort. SSRIs, selective serotonin reuptake inhibitors.
Propensity score matching analysis
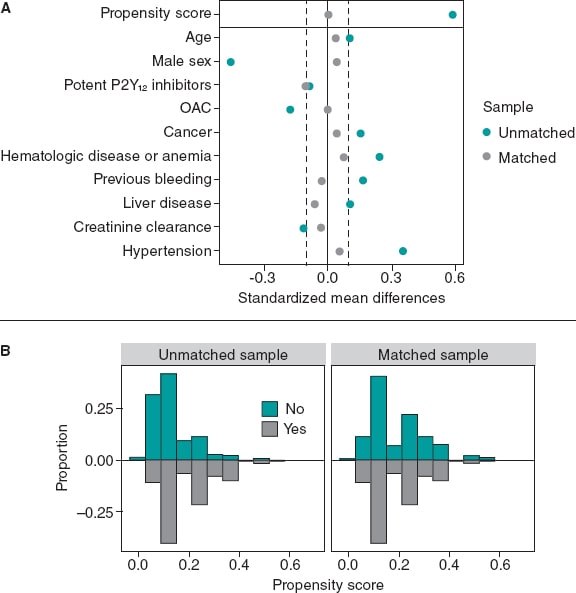
The variables used in the PSM, the standardized mean differences, and the Propensity score distributions of the unmatched and matched samples are shown on figure 3. PSM resulted in an excellent balance of covariates with standardized mean differences ≤ 10% in all variables included in the Propensity score. There was also a very good balance across the other baseline characteristics and bleeding risk scores except for diabetes mellitus and hyperlipemia that were more prevalent in the SSRIs group (table 3).
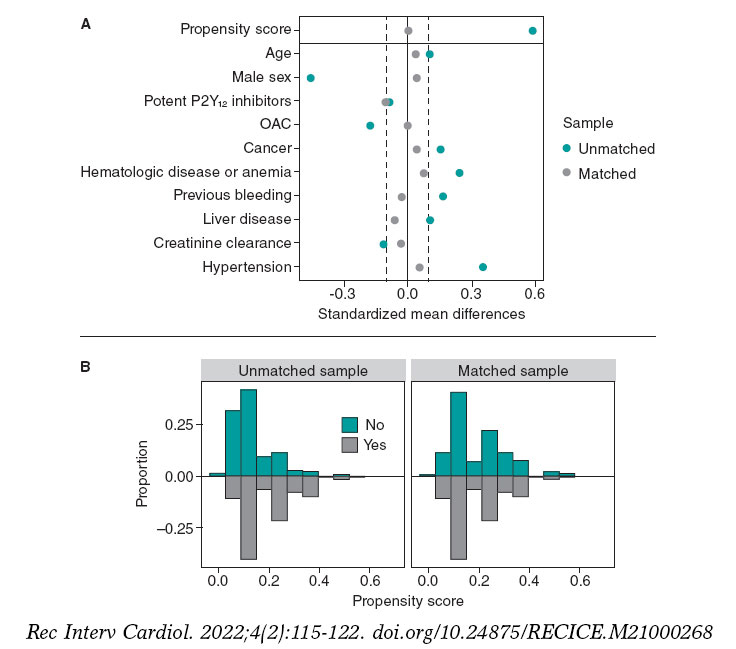
Figure 3. Variables used in the propensity score matching analysis and their standardized differences (A), and the propensity score distributions (B) of the unmatched and matched samples. OAC, oral anticoagulant.
Table 3. Baseline clinical characteristics of SSRIs/non-SSRIs users after matching
| Variable | SSRI (N = 139) | Non-SSRI (N = 139) | P |
|---|---|---|---|
| Chronic obstructive pulmonary disease | |||
| Age, years | 68 [60-76] | 67 [58-75] | .757 |
| Sex, male | 76 (54.7) | 73 (52.5) | .810 |
| BMI | 30.0 [25.8-32.0] | 28.4 [25.3-32.4] | .143 |
| Hypertension | 112 (80.6) | 109 (78.4) | .656 |
| Diabetes mellitus | 64 (46.0) | 48 (34.5) | .050 |
| Hyperlipidemia | 83 (59.7) | 67 (48.2) | .045 |
| Smoking (current or former) | 34 (24.5) | 28 (20.1) | .330 |
| Previous revascularization | 41 (29.5) | 30 (21.6) | .153 |
| COPD | 10 (7.2) | 9 (6.5) | .816 |
| Chronic kidney disease | 17 (12.2) | 19 (13.7) | .721 |
| Cancer | 20 (14.4) | 18 (12.9) | .727 |
| Liver disease | 8 (5.8) | 10 (7.2) | .626 |
| Hematologic disease or anemia | 25 (18) | 21 (15.1) | .519 |
| Previous relevant bleeding | 9 (6.5) | 10 (7.2) | .812 |
| Atrial fibrillation | 11 (7.9) | 11 (7.9) | 1.000 |
| Oral anticoagulant | 9 (6.5) | 9 (6.5) | 1.000 |
| Potent P2Y12 inhibitors | 90 (64.7) | 97 (69.8) | .371 |
| Ticagrelor | 86 (61.8) | 91 (65.5) | .749 |
| Prasugrel | 4 (2.9) | 6 (4.3) | .749 |
| DAPT duration, months | 6 [6-12] | 6 [6-12] | .810 |
| PRECISE-DAPT | 16 [10-24] | 15 [10-24] | .863 |
| PRECISE-DAPT ≥ 25 | 34 (24.5) | 32 (23.0) | .778 |
| HAS-BLED | 3 [2-3] | 3 [2-3] | .560 |
| Creatinine clearance, | |||
| mL/min/1.73 m2 | 94.8 [72.9-125.2] | 100 [82.7-114.0] | .747 |
| Clinical presentation | |||
| CCS | 66 (47.5) 73 (52.5) |
63 (45.3) 76 (54.7) |
.718 |
| ACS | |||
|
ACS, acute coronary syndrome; BMI, body mass index (kg/m2); CCS, chronic coronary syndrome; COPD, chronic obstructive pulmonary disease; DAPT, dual antiplatelet therapy; SSRI, selective serotonin reuptake inhibitors. Data are expressed as no. (%), mean ± standard deviation or median [interquartile range]. |
|||
The rate of major bleeding at the 1-year follow-up was 2.9% for both patients on SSRIs and the matched SSRIs non-users (HR, 1.01; 95%CI, 0.25-4.03; P = .991). There were no non-major clinically relevant bleedings in the SSRIs group and 6 (4.3%) among SSRIs non-users (HR, 0.39; 95%CI, 0.16-1.27; P = .120). No differences in MACE were reported between the SSRI and the non-SSRIs groups (HR, 1.01; 95%CI, 0.44-2.33; P = .979) (figure 4).
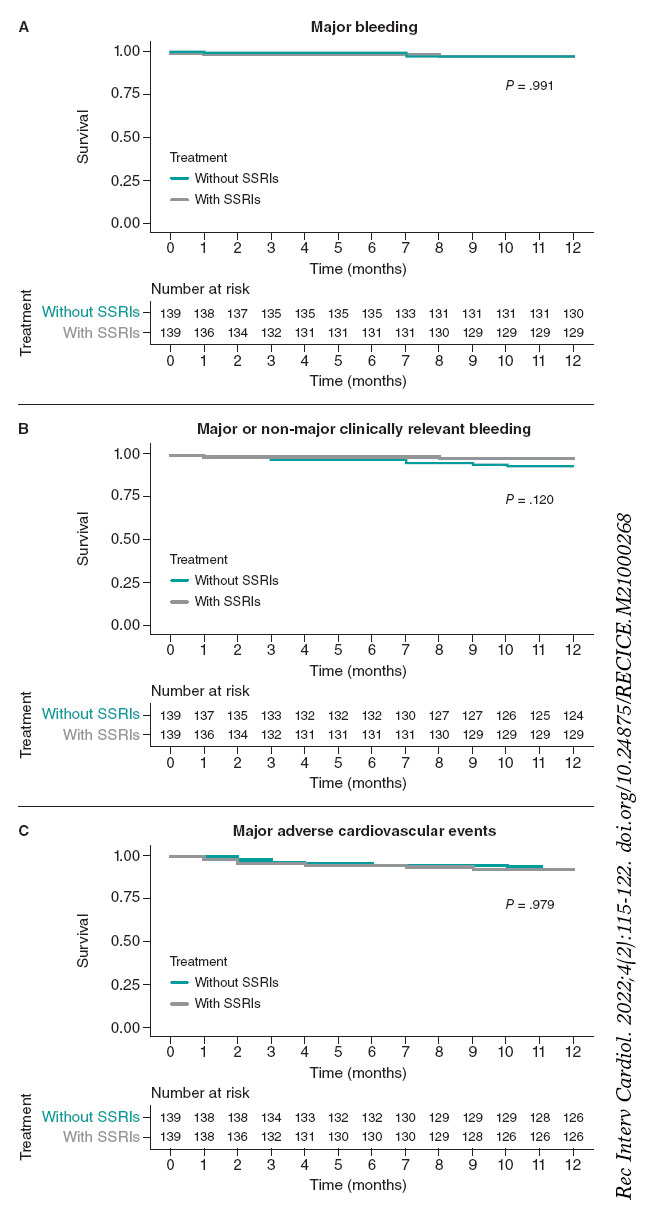
Figure 4. Kaplan-Meier curves for the primary bleeding outcome (A), the secondary composite bleeding (B), and the ischemic outcomes (C). Matched cohorts. SSRIs, selective serotonin reuptake inhibitors.
DISCUSSION
The main findings of this study can be summarized as follows: a) the use of SSRIs was frequent among patients undergoing PCI; b) patients prescribed with SSRIs had a higher baseline bleeding risk; c) despite the imbalance reported in the baseline characteristics, after adjustment SSRIs users were not associated with a significant excess of major or clinically relevant bleeding at the 1-year follow-up.
There is a strict correlation between coronary artery disease and mental health disorders. In our study up to 13.9% of patients treated with PCI were prescribed SSRIs. This group has more comorbidities and bleeding risk factors with the potential to complicate the clinical decision-making process regarding antithrombotic therapy selection. Importantly, whether SSRIs trigger a higher bleeding risk through a biological effect on platelet 5-HTT receptors or are a marker of a higher bleeding risk through concomitant comorbidities has been the matter of discussion in prior studies.
Labos et al.21 reported an increased risk of bleeding in patients taking both SSRIs and acetylsalicylic acid or clopidogrel-based DAPT after myocardial infarction. On the contrary, Lasella et al.22 assessed the impact of SSRI therapy on patients on DAPT after PCI finding no excessive bleedings in patients on SSRIs. Interestingly, they reported a lower risk of MACE in patients on SSRIs compared to those on mirtazapine, but a higher risk compared to patients on either one of the 2 antidepressants. This may be explained by a protective effect of SSRIs on MACE29 that could be exceeded by the unfavorable effect of mental health disorders on cardiovascular events.30 Another interpretation could be associated with the pharmacokinetics of clopidogrel since it is a prodrug that requires enzymatic conversion into its active metabolite by cytochrome P450 (CYP).31 Bykov et al.23 reported an increased risk of ischemic events in patients on clopidogrel and a CYP2C19-inhibiting SSRI compared to those on noninhibiting SSRIs. No differences were found regarding major bleeding. The study did not include a group of patients without SSRI treatment.
We should mention that none of the aforementioned studies included patients treated with potent P2Y12 inhibitors, which is currently the standard of care of patients with ACS. To our knowledge, this is the first study to assess the impact of SSRIs on a cohort of patients treated with potent P2Y12 inhibitors prasugrel or ticagrelor. In our population, two thirds of the patients were treated with potent P2Y12 inhibitors, which is more consistent with the antiplatelet strategies recommended by the current clinical practice guidelines.32,33 In this clinical setting, despite the imbalances reported in the baseline bleeding risk in an unadjusted analysis, we found no differences regarding major or clinically relevant bleeding events among patients on SSRIs and the matched group without a SSRI prescription. Hence, while the prescription of SSRIs can be a marker of a higher risk population with more comorbidities and risk factors, this may not translate into an independent predictor of bleeding events after accounting for the potential confounders. This is consistent with prior evidence in the medical literature. In the study conducted by Labos et al.21 patients on SSRI had a more significant past medical history of hypertension, renal failure, anemia or other hematologic disease, and non-GI bleeding. Lasella et al.22 reported that SSRIs users were more likely to have diabetes, hypertension, dyslipidemia, COPD, and chronic kidney disease.
Our findings are clinically relevant for different reasons. Although SSRIs have been associated with a potential for an increased bleeding risk, a direct translation into an excess of adverse events has not been confirmed yet. Our data provide reassurance on the relative safety profile of potent antithrombotic therapies in association with SSRIs, which did not substantially increase the risk of bleeding during the first year after PCI when the treatment decision-making process is based on a thorough evaluation of the features of bleeding and ischemic risk.
Our study also included a proportion of patients treated with concomitant antiplatelet and OAC therapy (~10%), which is consistent with the current standard practice.34 The impact of SSRIs on bleeding outcomes in patients with AF treated with OAC has also been examined in the past. Various authors have reported a higher risk of major bleeding in patients concurrently treated with SSRIs and warfarin.35,36 On the contrary, Quinn et al.37 did not find a significantly increased risk of bleeding among patients from the ROCKET AF trial assigned to warfarin or rivaroxaban who were also on SSRIs. However, there was a modest but non-statistically significant higher risk of major bleeding in the warfarin group. Since SSRIs are CYP2C9 inhibitors, an increase of warfarin plasma concentrations could explain these findings.38 This reaffirms the importance of non-vitamin k antagonists to reduce the risk of bleeding also in this population given the need for multiple antithrombotic agents after the PCI and the higher baseline bleeding risk reported.39
Limitations
The current study has several limitations. First, its retrospective observational design, and the relatively small size of the sample limits our ability to provide definitive conclusions due to the residual possibility of type-2 errors. Secondly, despite the PSM resulted in a good balance between the selected potential confounders and the other baseline characteristics, the presence of residual confounding factors cannot be completely ruled out. For example, some variables associated with bleeding like the presence of diabetes mellitus or peripheral arterial disease were not included in the propensity score model. Yet similar findings were observed in the adjusted and unadjusted analyses. Thirdly, the classification of SSRI users was based on treatment at discharge without accounting for treatment adherence or discontinuation.
CONCLUSIONS
In this real-world study, a combination of SSRIs and potent antithrombotic therapies was frequently prescribed after PCI. Although the prescription of SSRIs was associated with a higher baseline bleeding risk in the unadjusted analysis this was not the case with an excess of major or clinically relevant bleeding reported at the follow-up.
FUNDING
None reported.
AUTHORS’ CONTRIBUTIONS
R. González-Manzanares, and S. Ojeda conceived and designed the study. R. González-Manzanares, M. Ruiz-Moreno, C. Fernández-Avilés, L. Carmona-Artime, G. Flores-Vergara, and F. Costa collected analyzed data and interpreted the results. R. González-Manzanares, M. Ruiz-Moreno, S. Ojeda, and F. Hidalgo drafted the manuscript and completed the critical revisions. S. Ojeda, F. Hidalgo, G. Flores-Vergara, F. Costa, J. Suárez de Lezo, and M. Pan reviewed and revised the manuscript, and approved its final version before submission. All authors gave their final approval to the version that would eventually be published.
CONFLICTS OF INTEREST
S. Ojeda is an associate editor of REC: Interventional Cardiology. The journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. S. Ojeda, and M. Pan declared having received honoraria for lectures given for Abbott, Boston, World Medical, and Terumo. J Suárez de Lezo declared having received honoraria for lectures given for Abbott. The remaining authors declared no conflicts of interest whatsoever.
WHAT IS KNOWN ABOUT THE TOPIC?
- Coronary artery disease and mental health disorders frequently coexist. The combination of SSRIs and potent antithrombotic therapies is common.
- Bleeding events after PCI worsen prognosis same as recurrent ischemic events.
- SSRIs have been potentially associated with an increased risk of bleeding. Data regarding the concomitant use of SSRIs and potent antithrombotic therapies is scarce and inconclusive.
WHAT DOES THIS STUDY ADD?
- This is the first study to assess the impact of SSRIs on the bleeding outcomes in the current PCI practice using potent P2Y12 inhibitors or triple antithrombotic therapy.
- SSRIs users have a higher bleeding risk profile.
- The use of SSRIs was not associated with a higher risk of major bleeding after adjusting for the potential confounders.
REFERENCES
1. De Hert M, Detraux J, Vancampfort D. The intriguing relationship between coronary heart disease and mental disorders. Dialogues Clin Neurosci. 2018;20:31-40.
2. Jha MK, Qamar A, Vaduganathan M, Charney DS, Murrough JW. Screening and Management of Depression in Patients With Cardiovascular Disease:JACC State-of-the-Art Review. J Am Coll Cardiol. 2019;73:1827-1845.
3. Lane D, Carroll D, Ring C, Beevers DG, Lip GY. The prevalence and persistence of depression and anxiety following myocardial infarction. Br J Health Psychol. 2002;7:11-21.
4. Gehi A, Haas D, Pipkin S, Whooley MA. Depression and medication adherence in outpatients with coronary heart disease:findings from the Heart and Soul Study. Arch Intern Med. 2005;165:2508-2513.
5. Sin NL, Kumar AD, Gehi AK, Whooley MA. Direction of Association Between Depressive Symptoms and Lifestyle Behaviors in Patients with Coronary Heart Disease:the Heart and Soul Study. Ann Behav Med. 2016;50:523-532.
6. Meijer A, Conradi HJ, Bos EH, et al. Prognostic association of depression following myocardial infarction with mortality and cardiovascular events:a meta-analysis of 25 years of research. Gen Hosp Psychiatry. 2011;33:203-216.
7. Carney RM, Blumenthal JA, Freedland KE, et al. Depression and late mortality after myocardial infarction in the Enhancing Recovery in Coronary Heart Disease (ENRICHD) study. Psychosom Med. 2004;66:466-474.
8. Valgimigli M, Garcia-Garcia HM, Vrijens B, et al. Standardized classification and framework for reporting, interpreting, and analysing medication non-adherence in cardiovascular clinical trials:a consensus report from the Non-adherence Academic Research Consortium (NARC) [published correction appears in Eur Heart J. 2019;40:2774]. Eur Heart J. 2019;40:2070-2085.
9. Ghaffari Darab M, Hedayati A, Khorasani E, Bayati M, Keshavarz K. Selective serotonin reuptake inhibitors in major depression disorder treatment:an umbrella review on systematic reviews. Int J Psychiatry Clin Pract. 2020;24:357-370.
10. Bandelow B. Current and Novel Psychopharmacological Drugs for Anxiety Disorders. Adv Exp Med Biol. 2020;1191:347-365.
11. Berger M, Gray JA, Roth BL. The expanded biology of serotonin. Annu Rev Med. 2009;60:355-366.
12. Abdelmalik N, RuhéHG, Barwari K, et al. Effect of the selective serotonin reuptake inhibitor paroxetine on platelet function is modified by a SLC6A4 serotonin transporter polymorphism. J Thromb Haemost. 2008;6:2168-2174.
13. De Abajo FJ. Effects of selective serotonin reuptake inhibitors on platelet function:mechanisms, clinical outcomes and implications for use in elderly patients. Drugs Aging. 2011;28:345-367.
14. Hougardy DM, Egberts TC, van der Graaf F, Brenninkmeijer VJ, Derijks LJ. Serotonin transporter polymorphism and bleeding time during SSRI therapy. Br J Clin Pharmacol. 2008;65:761-766.
15. Yuan Y, Tsoi K, Hunt RH. Selective serotonin reuptake inhibitors and risk of upper GI bleeding:confusion or confounding?Am J Med. 2006;119:719-727.
16. Valgimigli M, Costa F, Lokhnygina et al. Trade-off of myocardial infarction vs. bleeding types on mortality after acute coronary syndrome:lessons from the Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome (TRACER) randomized trial. Eur. Heart J. 2017;38:804-810.
17. Mehran R, Pocock SJ, Stone GW, et al. Associations of major bleeding and myocardial infarction with the incidence and timing of mortality in patients presenting with non-ST-elevation acute coronary syndromes:a risk model from the ACUITY trial. Eur Heart J. 2009;30:1457-1466.
18. Mehran R, Pocock SJ, Nikolsky E, et al. A risk score to predict bleeding in patients with acute coronary syndromes. J Am Coll Cardiol. 2010;55:2556-2566.
19. Costa F, van Klaveren D, James S, et al. Derivation and validation of the predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy (PRECISE-DAPT) score:a pooled analysis of individual-patient datasets from clinical trials. Lancet. 2017;389:1025-1034.
20. Kang DO, An H, Park GU, et al. Cardiovascular and Bleeding Risks Associated With Nonsteroidal Anti-Inflammatory Drugs After Myocardial Infarction. J Am Coll Cardiol. 2020;76:518-529.
21. Labos C, Dasgupta K, Nedjar H, Turecki G, Rahme E. Risk of bleeding associated with combined use of selective serotonin reuptake inhibitors and antiplatelet therapy following acute myocardial infarction. CMAJ. 2011;183:1835-1843.
22. Iasella CJ, Kreider MS, Huang L, Coons JC, Stevenson JM. Effect of Selective Serotonin Reuptake Inhibitors on Cardiovascular Outcomes After Percutaneous Coronary Intervention:A Retrospective Cohort Study. Clin Drug Investig. 2019;39:543-551.
23. Bykov K, Schneeweiss S, Donneyong MM, Dong YH, Choudhry NK, Gagne JJ. Impact of an Interaction Between Clopidogrel and Selective Serotonin Reuptake Inhibitors. Am J Cardiol. 2017;119:651-657.
24. Valgimigli M, Bueno H, Byrne RA, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS:The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2018;39:213-260.
25. Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding definitions for cardiovascular clinical trials:a consensus report from the Bleeding Academic Research Consortium. Circulation. 2011;123:2736-2747.
26. Austin PC. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivariate Behav Res. 2011;46:399-424.
27. Brookhart MA, Schneeweiss S, Rothman KJ, Glynn RJ, Avorn J, Stürmer T. Variable selection for propensity score models. Am J Epidemiol. 2006;163:1149-1156.
28. Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28:3083-3107.
29. Fernandes N, Prada L, Rosa MM, et al. The impact of SSRIs on mortality and cardiovascular events in patients with coronary artery disease and depression:systematic review and meta-analysis. Clin Res Cardiol. 2021;110:183-193.
30. Zhang WY, Nan N, Song XT, Tian JF, Yang XY. Impact of depression on clinical outcomes following percutaneous coronary intervention:a systematic review and meta-analysis. BMJ Open. 2019;9:e026445.
31. Price MJ, Tantry US, Gurbel PA. The influence of CYP2C19 polymorphisms on the pharmacokinetics, pharmacodynamics, and clinical effectiveness of P2Y(12) inhibitors. Rev Cardiovasc Med. 2011;12:1-12.
32. Patel A, Goodman SG, Tan M, et al. Contemporary use of guideline-based higher potency P2Y12 receptor inhibitor therapy in patients with moderate-to-high risk non-ST-segment elevation myocardial infarction:Results from the Canadian ACS reflective II cross-sectional study. Clin Cardiol. 2021;44:839-847.
33. De Luca L, Zeymer U, Claeys MJ, et al. Comparison of P2Y12 receptor inhibitors in patients with ST-elevation myocardial infarction in clinical practice:a propensity score analysis of five contemporary European registries. Eur Heart J Cardiovasc Pharmacother. 2021;7:94-103.
34. Costa F, Garcia-Ruiz V, Licordari R, Fimiani L. The High Bleeding Risk Patient with Coronary Artery Disease. Cardiol Clin. 2020;38:481-490.
35. Quinn GR, Singer DE, Chang Y, et al. Effect of selective serotonin reuptake inhibitors on bleeding risk in patients with atrial fibrillation taking warfarin. Am J Cardiol. 2014;114:583-586.
36. Schelleman H, Brensinger CM, Bilker WB, Hennessy S. Antidepressant-warfarin interaction and associated gastrointestinal bleeding risk in a case-control study [published correction appears in PLoS One. 2015;10:e0121926]. PLoS One. 2011;6:e21447.
37. Quinn GR, Hellkamp AS, Hankey GJ, et al. Selective Serotonin Reuptake Inhibitors and Bleeding Risk in Anticoagulated Patients With Atrial Fibrillation:An Analysis From the ROCKET AF Trial. J Am Heart Assoc. 2018;7(15):e00∳.
38. Sansone RA, Sansone LA. Warfarin and Antidepressants:Happiness without Hemorrhaging. Psychiatry (Edgmont). 2009;6:24-29.
39. Costa F, Valgimigli M, Steg PG, et al. Antithrombotic therapy according to baseline bleeding risk in patients with atrial fibrillation undergoing percutaneous coronary intervention:applying the PRECISE-DAPT score in RE-DUAL PCI [published online ahead of print, 2020 Dec 1]. Eur Heart J Cardiovasc Pharmacother. 2020;pvaa135.
ABSTRACT
Introduction and objectives: Coronary lesions with stent overlapping are associated with higher neointimal proliferation that leads to more restenosis. Furthermore, the tapering of coronary arteries is a major challenge when treating long coronary lesions. This study attempted to assess the safety and clinical level of performance of long nontapered sirolimus-eluting coronary stent systems (> 36 mm) to treat long and diffused de novo coronary lesions in real-world scenarios.
Methods: This was a prospective, non-randomized, multicentre study that included 696 consecutive patients treated with the long nontapered BioMime sirolimus-eluting coronary stent system in long and diffused de novo coronary lesions. The safety endpoint was major adverse cardiovascular events defined as a composite of cardiac death, myocardial infarction, clinically driven target lesion revascularization, stent thrombosis, and major bleeding at the 12-month follow-up.
Results: Of a total of 696 patients, 38.79% were diabetic. The mean age of all the patients was 64.6 ± 14 years, and 80% were males. The indication for revascularization was acute coronary syndrome in 63.1%. A total of 899 lesions were identified out of which 742 were successfully treated with long BioMime stents (37 mm, 40 mm, 44 mm, and 48 mm). The cumulative incidence of major adverse cardiovascular events was 8.1% at the 12-month follow-up including cardiac death (2.09%), myocardial infarction (1.34%), and total stent thrombosis (0.5%).
Conclusions: This study confirms the safety and good performance of long nontapered BioMime coronary stents to treat de novo coronary stenosis. Therefore, it can be considered a safe and effective treatment for long and diffused de novo coronary lesions in the routine clinical practice.
Keywords: Coronary angioplasty. Drug-eluting stent. Nontapered stents.
RESUMEN
Introducción y objetivos: Las lesiones coronarias largas y difusas, cuando se tratan percutáneamente, requieren a menudo superposición de los stents, que se asocia a una mayor tasa de reestenosis. Por otro lado, el adelgazamiento progresivo de las arterias dificulta el tratamiento de las lesiones largas. En este estudio se analizan la seguridad y la eficacia clínica de los stents liberadores de sirolimus largos no cónicos (> 36 mm) para el tratamiento de lesiones largas de novo en un escenario real.
Métodos: Estudio prospectivo, no aleatorizado, multicéntrico, con 696 pacientes consecutivos con implantación de stent BioMime largo no cónico para el tratamiento de lesiones coronarias de novo largas y difusas. El criterio de valoración de seguridad fueron los eventos adversos cardiovasculares mayores en el seguimiento, definidos como la combinación de muerte cardiaca, infarto de miocardio, necesidad de nueva revascularización en la misma lesión guiada por la clínica, trombosis del stent o hemorragia mayor a los 12 meses.
Resultados: De los 696 pacientes incluidos, el 38,79% eran diabéticos. La edad media fue de 64,6 ± 14 años y el 80% eran varones. La indicación de revascularización fue un síndrome coronario agudo en el 63,1%. Se identificaron 899 lesiones, de las que 742 se trataron con éxito con stents BioMime (37-40-44-48 mm). La incidencia acumulada de eventos adversos cardiovasculares mayores fue del 8,1% a los 12 meses, con un 2,09% de muertes de causa cardiaca, un 1,34% de infartos de miocardio y un 0,5% de trombosis del stent.
Conclusiones: El presente estudio confirma la seguridad y el buen perfil clínico a 12 meses del stent BioMime largo no cónico para el tratamiento de lesiones coronarias de novo largas y difusas, por lo que debe considerarse un tratamiento seguro y eficaz para este tipo de lesiones en la práctica clínica habitual.
Palabras clave: Angioplastia coronaria. Stents farmacoactivos. Stents largos no cónicos.
Abbreviations
CAD: coronary artery disease. DES: drug-eluting stent. MACE: major adverse cardiovascular events. PCI: percutaneous coronary intervention. SES: sirolimus-eluting stent. ST: stent thrombosis.
INTRODUCTION
The most widely used strategy to treat coronary artery disease (CAD) is percutaneous coronary intervention (PCI) with stent implantation, particularly with the current generation of drug-eluting coronary stents (DES), since their distinctive features improve the clinical outcomes of PCI.1 However, the treatment of long and diffused coronary lesions remains challenging, especially in long lesions in tapered coronary arteries where variations in vessel diameter may require the implantation of > 1 stent per lesion.2,3
The use of either multiple stents or a single long stent are the most common treatment strategies for long and diffused lesions in tapered arteries. Both approaches may be associated with clinical failure due to the potential risk of mechanical mismatch of the stent size.1,4,5 Multiple short overlapping stents with variable diameters are often implanted to adequately match the size of long tapered lesions. Because of potential discrepancies regarding diameters when using long nontapered stents, a proximal optimization technique may be used to reconstruct the vessel natural geometry. However, this solution does not come without problems such as stent fracture due to vessel rigidity, restenosis due to a higher vascular injury, delayed healing, very late stent thrombosis (ST), vessel aneurysm, side branch jailing, higher treatment cost, overuse of antirestenotic drugs, and increased exposure to radiation and contrast media, and death or myocardial infarction.6,7
A single long BioMime (Meril Life Sciences Pvt. Ltd., India), an ultrathin biodegradable polymer coated sirolimus-eluting coronary stent (SES) system, is often enough to treat long and diffused lesions. Thus, the local arterial walls can be saved from overexposure to drug/metal avoiding any potential associated adverse events at the follow-up like delayed healing, perioperative myocardial infarction (MI), risk of target lesion revascularization, and very late ST. The aim of this study was to evaluate the safety and level of performance of the long nontapered BioMime SES system (37 mm, 40 mm, 44 mm, 48 mm) in consecutive real-world patients with long and diffused de novo coronary lesions.
METHODS
Study design and population
This was a prospective, non-randomized, multicentre study that included a total of 696 consecutive patients (aged ≥ 18 years) from 14 clinical centers across Spain. All the study investigators are listed in the appendix of this article.
All consecutive patients included had been treated of long and diffuse de novo coronary lesions through the implantation of, at least, 1 long nontapered BioMime system (37 mm, 40 mm, 44 mm, 48 mm). The study was conducted in observance of the privacy policy of each research center including its rules and regulations for the appropriate use of data in patient-oriented research. This study was also conducted in observance of the Declaration of Helsinki, and approved by the ethics committee. Written informed consents were obtained from all the participants before the procedure.
Study device and procedure
The BioMime is a biodegradable polymer coated SES system with different lengths available to treat long and diffused coronary lesions. It uses an ultra-thin strut (65 µm), and a cobalt-chromium platform that has a unique hybrid design of open and closed cells with uniformly thin coating (2 µm) of bioabsorbable polymers, PLLA (poly-L-lactic acid), and PLGA (poly-lactic-co-glycolic acid). The stent elutes sirolimus (1.25 µg/mm2) between 30 and 40 days after implantation. The currently available long lengths of BioMime are 37 mm, 40 mm, 44 mm, and 48 mm. The device is CE marked.
The PCI was performed according to the standard treatment guidelines and followed by each participant center. Predilatation and postdilatation were left to the operator’s discretion though postdilatation was recommended per protocol.
Preoperatively, a 300 mg loading dose of aspirin plus a second anti-platelet agent (clopidogrel, ticagrelor, or prasugrel according to the clinical settings and operator’s preference) were administered in all the consecutive patients included.
Postoperatively, all patients were administered a 12-month course of dual antiplatelet therapy plus aspirin (75 mg to 100 mg once a day) indefinitely beyond the first year. A 1.6- and 12-month clinical follow-up was conducted after the index procedure, as required, and based on symptoms.
Endpoints and definitions
The safety endpoints were the occurrence of major adverse cardiovascular events (MACE) at the 1-, 6-, and 12-month follow-up after the index procedure. MACE was defined as a composite of cardiac death, target vessel myocardial infarction, clinically driven target lesion revascularization, ST, and major bleeding.
MI was defined as the development of new pathological Q waves on the electrocardiogram or elevated creatinine kinase (CK) levels ≥ 2 times the upper limit of normal with elevated CK-MB levels in the absence of new pathological Q waves or new ischemic symptoms (eg, chest pain or shortness of breath).8 Cardiac death was defined as any deaths resulting from AMI, sudden cardiac death, heart failure mortality or stroke. Clinically driven target lesion revascularization was defined as a new PCI performed on the target lesion or coronary artery bypass graft of the lesion in the previously treated segment or within the 5 mm proximal or distal to the stent site or edge of DES inflation. ST was classified based on the definitions established by the Academic Research Consortium.9 Moderate-to-severe bleeding events were defined according to the GUSTO (Global Use of Strategies to Open Occluded Arteries) criteria. Procedural success was defined as a successful PCI without in-hospital major clinical complications including death, MI, and clinically driven target lesion revascularization. Device success was defined as the deployment of the study stent at the intended target lesion attaining final residual stenosis < 30% of the target lesion estimated both angiographically and through visual estimation.
Statistical analysis
Since there is no intervention, to study this cohort of patients we thought that the best method was to perform a descriptive analysis for an objective, comprehensive, and informative study of data. A a descriptive statistical analysis of the relevant variables was performed after collecting data. All statistical analyses were performed using the SPSS statistical software platform. Measures of central tendency such as means summarize the level of performance of a group of scores while measures of variability describe the spread of scores among the participants. Both are important to understand the behavior of this cohort. One provides information on the level of performance, and the other tells us how consistent that performance is. Categorical data were expressed as frequency and percentages. No further models were conducted as the idea of this paper was to describe a group of patients, not to compare groups or search for significant inter-group differences.
RESULTS
Baseline demographic and clinical characteristics
The data of 696 consecutive patients (742 BioMime stents implanted, 157 different stents) were collected in the study that mostly included males (80.1%). The baseline demographic and clinical characteristics of patients are shown on table 1. The patients’ mean age was 64.6 ± 14 years. Conventional risk factors for CAD in the study population were diabetes mellitus (39%), hypertension (67.2%), dyslipidemia (64.8%), and active smoking (26.44%). The clinical status at admission is shown on table 1. Most patients (63.39%) had acute coronary syndrome.
Table 1. Baseline demographic and clinical characteristics
| Patients | N = 696 |
|---|---|
| Patients, demographics | |
| Age, years | 64.6 ± 14 |
| Male | 556 (80.1) |
| Baseline past medical history | |
| Diabetes mellitus | 271 (38.79) |
| Hypertension | 466 (66.80) |
| Dyslipidemia | 452 (64.80) |
| Active smoker | 180 (26.44) |
| Previous CABG | 57 (8.54) |
| Previous PCI | 223 (32.07) |
| Vascular peripheral disease | 69 (10.64) |
| Previous MI | 181 (25.63) |
| Cardiac status at the index procedure | |
| Stable angina | 254 (36.49) |
| Unstable angina | 29 (4.16) |
| STEMI | 227 (32.61) |
| NSTEMI | 186 (26.72) |
| Left ventricular ejection fraction < 30% | 181 (26) |
|
CABG, coronary artery bypass graft; NSTEMI, non-ST-elevation acute myocardial infarction; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction. Data are expressed as no. (%) or mean ± standard deviation. |
|
Lesion and procedural characteristics
Out of a total of 899 lesions identified in 696 consecutive patients, 742 long and diffused de novo type C coronary lesions (1.07 lesions per patient) were successfully treated with long BioMime stents. No other stents were needed to treat the lesion initially handled with a long BioMime device. A total of 157 other lesions were treated with 157 different stents. Therefore, no overlapping was needed in any of the lesions treated with a long BioMime device. A total of 40% of the patients had 1-vessel disease, 37% 2-vessel disease and 23% of the patients had 3-vessel disease. The left anterior descending coronary artery followed by the right coronary artery were the main arteries treated. In 3.8% of the cases BioMime implantation involved the left main coronary artery. The mean length of the implanted BioMime SES system was 43.8 mm along with an average diameter of 3.1 mm. The immediate procedural and device success rates were 99.7% and 100%, respectively. The procedural variables are shown on table 2 and table 3.
Table 2. Lesion and procedural characteristics
| Patients | N = 696 |
|---|---|
| Total no. of lesions treated with the BioMime Morph SES system | 742 |
| Total no. of lesions treated with other stents | 157 |
| BioMime target lesion location | |
| Left anterior descending coronary artery | |
| Proximal LAD | 146 (21.40) |
| Mid LAD | 216 (30.80) |
| Distal LAD | 28 (4.50) |
| Diagonal | 11 (1.60) |
| Right coronary artery | |
| Proximal RCA | 174 (25.10) |
| Mid RCA | 257 (36.80) |
| Distal RCA | 97 (14.10) |
| Left circumflex artery | |
| Proximal LCX | 56 (8.20) |
| Mid LCX | 90 (12.90) |
| Distal LCX | 28 (4.10) |
| Left main coronary artery | 26 (3.80) |
| Diseased vessel | 1.84 ± 0.78 |
|
LAD, left anterior descending coronary artery; LCX, left circumflex artery; RCA, right coronary artery; SES, sirolimus-eluting stent. Data are expressed as no. (%). |
|
Table 3. BioMime sirolimus-eluting stent system characteristics
| Stent lenght (mm) | |
| 37 | 100 |
| 40 | 189 |
| 44 | 128 |
| 48 | 325 |
| Average stent length (mm) | 43.80 |
| Stent diameter (mm) | |
| 2.25 | 42 |
| 2.5 | 153 |
| 2.75 | 84 |
| 3 | 263 |
| 3.5 | 185 |
| 4 | 13 |
| 4.5 | 2 |
| Maximum pressure | |
| Predilatation | 298 (86) |
| Postdilatation | 376 (54) |
| Maximum pressure | 14.6 ± 3.2 |
| Average stent diamenter used (mm) | 3.1 |
|
Data are expressed as no. (%). |
|
Clinical outcomes at follow-up
Clinical follow-up was completed in 96.12% of the patients included at the 12-month follow-up. A total of 3.88% out of 696 patients were lost to follow-up after 12 months.
The cumulative incidence of MACE at the 1-, 6-, and 12-month follow-up was 2.2%, 6.6%, and 8.1%, respectively. The individual MACE at the follow-up are shown on table 4. The rates of cardiac death were 0.59% and 2.09% after 1 month and 1 year, respectively.
Table 4. MACE at the follow-up
| % of patients | MACE | |
|---|---|---|
| Follow-up | ||
| 1 month | 682 (97.99) | 13 (2.2) |
| 6 to 9 months | 675 (97.27) | 44 (6.57) |
| 12 months | 668 (96.12) | 53 (8.1) |
| MACE | ||
| Bleeding at 1-M | 20 (0.29) | |
| Death at 1-M | 41 (0.59) | |
| MI at 1-M | 41 (0.59) | |
| Bleeding at 12-M | 5 (0.75) | |
| Death at 12-M | 13 (2.09) | |
| MI at 12-M | 9 (1.34) | |
| Total ST at 12-M | 3 (0.50) | |
|
MACE, major adverse cardiovascular events; M, month; MI, myocardial infarction; ST, stent thrombosis. Data are expressed as no. (%). |
||
DISCUSSION
In the current study, the long nontapered BioMime SES system proved its safety and level of performance in consecutive real-world patients with long and diffused de novo coronary lesions. Despite the all-comers inclusion criteria defining a high-risk population, and the anatomical need for a long stent, procedural (99.7%) and device (100%) success were achieved and the clinical follow-up was quite favorable.
Studies have shown that the dimensions of coronary arteries taper naturally along with their length. They observed that 23% of the arteries had ≥ 1 mm taper and 19% arteries a 0.5 mm to 0.99 mm taper.10 Stent sizing is critical for a successful PCI regarding the treatment of long tapered lesions. Stent oversizing (stents that are larger in diameter compared to the healthy artery) may induce pathological stress on the arterial wall, aneurysm formation, late ST, and even late perforations. Stent undersizing, on the other hand, (stents that are smaller in diameter compared to the healthy artery) may lead to ST due to stent malapposition.11 Consistent with this, tapered stents were developed to potentially minimize clinical failure and maximize clinical benefits in these patients. This fact may be due to the specific design of the BioMime stents.
Ultrathin struts facilitate navegability, flexibility, and conformability of the vessel geometry while maintaining an excellent radial force. In addition, the open cell design throughout the entire body of the stent favors a less stiff device that follows more closely the tapered contour of the artery resulting in less arterial wall stress. Compliant stents should be considered for tapered artery applications, perhaps even to avoid the need for tapered stents, at least up to 48 mm length, as shown in our data.12-16
The use of long coronary stents (≥ 30 mm), but not as long as the lesions treated in this registry, to treat long and diffuse native vessel disease, saphenous vein graft disease, and long coronary dissections is associated with a reasonable procedural success rate and acceptable early and intermediate-term clinical outcomes.17 The treatment of very long CAD showed similar target lesion faliure at the 2-year follow-up for single DESs compared to overlapped DESs.18 Our results suggest that both strategies are reasonable therapeutic options for patients with diffuse CAD. However, DES overlap occurs in > 10% of the patients treated with PCI in the routine clinical practice, and has been associated with impaired angiographic and long-term clinical outcomes including death or myocardial infarction.19 In addition, the development of risk areas for malapposition with a single stent is significantly lower compared to overlapping stents. In cases where stent overlap cannot be avoided, deployment strategies should be optimized or new stent designs considered to reduce the risk of restenosis.20 A single stent strategy is often more cost-effectiveness, and involves the administration of fewer contrast and fewer balloons. New designs of very long stents allow us not only to treat increasingly complex lesions, but also to simplify the procedure, and reduce the number of stents used with very favorable results, at least, similar to those obtained with overlapping stents.21 Former studies have confirmed the safety and level of performance of the BioMime Morph, a very long tapered stent (60 mm) that can be considered the treatment of choice for very long and diffused tapered de novo coronary lesions in the routine clinical practice.22 However, in long lesions treated with single stents of up to 48 mm in length, our results suggest that nontapered stents give very good clinical results.
Limitations
One limitation may be the follow-up period that may not be enough to determine the long-term safety and level of performance of long BioMime SES system in patients with long and diffused de novo coronary lesions.
CONCLUSIONS
This study confirmed the favorable procedural and device success, and the optimal safety outcomes reported at the follow up, of the long nontapered BioMime SES system, up to 48 mm length, in real-world patients with long and diffused de novo coronary lesions.
FUNDING
The current study was partially funded by Palex Medical, and Meril (data collection, web design, and ethical committee).
AUTHORS’ CONTRIBUTIONS
E. Domingo contributed to the study design, database completion, clinical follow-up, data analysis, and manuscript writing. J. Guindo contributed to the study design. R. Calviño Santos, J. Antoni Gomez, X. Carrillo, J. Sánchez, L. Andraka, A. Torres, J. Casanova-Sandoval, R. Ocaranza Sanchez, J. León Jiménez, J.F. Muñoz, R. Trillo Nouche, and M. Fuertes contributed to the database completion, and clinical follow-up. I. Otaegui contributed to the database completion, data analysis, and clinical follow-up. B. García del Balnco contributed to the study design, data analysis, and manuscript writing.
CONFLICTS OF INTEREST
None reported.
APPENDIX 1: STUDY INVESTIGATORS
-
Gerard Marti Aguasca. Hospital Universitario Vall d’Hebron, Servicio de Cardiología.
-
Vicenç Serra García. Hospital Universitario Vall d’Hebron, Servi- cio de Cardiología.
-
Bernat Serra Creus. Hospital Universitario Vall d’Hebron, Ser- vicio de Cardiología.
-
Neus Bellera Gotarda. Hospital Universitario Vall d’Hebron, Servi- cio de Cardiología.
-
Jorge Salgado Fernández. Complejo Hospitalario Universitario A Coruña, Servicio de Cardiología.
-
Montserrat Gracida Blancas. Hospital Universitari de Bellvitge, Servicio de Cardiología.
-
Lara Fuentes Castillo. Hospital Universitari de Bellvitge, Servicio de Cardiología.
-
Eduard Fernández-Nofrerias, Hospital Germans Trias i Pujol, Servicio de Cardiología.
-
Oriol Rodríguez-Leor. Hospital Germans Trias i Pujol, Servicio de Cardiología.
-
Omar Abdul Jawad Altisent. Hospital Germans Trias i Pujol, Servicio de Cardiología.
-
Gabriel Galache. Hospital Universitario Miguel Servet, Servicio de Cardiología.
-
Rosario Hortas. Hospital Universitario Miguel Servet, Servicio de Cardiología.
-
Eduard Bosch. Parc Taulí Hospital Universitari, Servicio de Cardiología.
-
Daniel Valcarcel. Parc Taulí Hospital Universitari, Servicio de Cardiología.
-
Maite Alfageme. HUA – Txagorritxu, Servicio de Cardiología.
-
Merche Sanz. HUA – Txagorritxu, Servicio de Cardiología.
-
Melisa Santás Álvarez. Hospital Lucus Augusti, Servicio de Cardiología.
-
Diego López Otero. Hospital Clínico Universitario de Santiago – CHUS, Servicio de Cardiología.
-
Juan Carlos Sanmartin Pena. Hospital Clínico Universitario de Santiago -CHUS, Servicio de Cardiología.
-
Ana Belén Cid Álvarez. Hospital Clínico Universitario de Santiago -CHUS, Servicio de Cardiología.
REFERENCES
1. Tan CK, Tin ZL, Arshad MKM, et al. Treatment with 48-mm everolimus eluting stents:Procedural safety and 12-month patient outcome. Herz. 2019;44:419-424.
2. Roach MR, MacLean NF. The importance of taper proximal and distal to Y-bifurcations in arteries. Front Med Biol Eng. 1993;5:127-133.
3. Zubaid M, Buller C, Mancini GB. Normal angiographic tapering of the coronary arteries. Can J Cardiol. 2002;18:973-980.
4. Sgueglia GA, Belloni F, Summaria F, et al. One-year follow-up of patients treated with new-generation polymer-based 38 mm everolimus-eluting stent:the P38 study. Catheter Cardiovasc Interv. 2015;85:218-224.
5. Timmins LH, Meyer CA, Moreno MR, Moore JE, Jr. Mechanical modeling of stents deployed in tapered arteries. Ann Biomed Eng. 2008;36:2042-2050.
6. Ellis SG, Holmes DR. Strategic approaches in coronary intervention. 2006:Lippincott Williams &Wilkins. P. 299-304.
7. Raber L, Juni P, Loffel L, et al. Impact of stent overlap on angiographic and long-term clinical outcome in patients undergoing drug-eluting stent implantation. J Am Coll Cardiol. 2010;55:1178-1188.
8. Mendis S, Thygesen K, Kuulasmaa K, et al. World Health Organization definition of myocardial infarction:2008- 09 revision. Int J Epidemiol. 2011;40:139-146.
9. Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials:a case for standardized definitions. Circulation. 2007;115:2344-2351.
10. Banka VS, Baker HA, 3rd, Vemuri DN, Voci G, Maniet AR. Effectiveness of decremental diameter balloon catheters (tapered balloon). Am J Cardiol. 1992;69:188-193.
11. Kitahara H, Okada K, Kimura T, et al. Impact of stent size selection on acute and long-term outcomes after drug-eluting stent implantation in de novo coronary lesions. Circ Cardiovasc Interv. 2017;10:e004795.
12. Sinha SK, Mahrotra A, Abhishekh NK, et al. Acute stent loss and its retrieval of a long, tapering morph stent in a tortuous, calcified lesion. Cardiol Res. 2018;9:63-67.
13. Zivelonghi C, van Kuijk JP, Nijenhuis V, et al. First report of the use of long-tapered sirolimus-eluting coronary stent for the treatment of chronic total occlusions with the hybrid algorithm. Catheter Cardiovasc Interv. 201;5:1-9.
14. Matchin YG, Atanesyan RV, Kononets EN, Danilov NM, Bubnov DS, Ageev FT. The first experience of using very long stents covered with sirolimus (4060 mm) in the treatment of patients with extensive and diffuse lesions of the coronary arteries. Kardiologiia. 2017;57:19-26.
15. Timmins LH, Meyer CA, Moreno MR, Moore Jr. JE. Mechanical modeling of stents deployed in tapered arteries. Ann Biomed Eng. 2008;36:2042-2050.
16. Xiang Shen, Yong-Quan Deng, Song Ji, Zhong-Min Xie. Flexibility behavior of coronary stents:the role of linker investigated with numerical simulation. J Mech Med Biol. 2017. https://doi.org/10.1142/S0219519417501123.
17. Mushahwar SS, Pyatt JR, Lowe R, Morrison WL, Perry RA, Ramsdale DA. Clinical outcomes of long coronary stents:a single-center experience. Int J Cardiovasc Intervent. 2001;4:29-33.
18. Sim HW, Thong EH, Loh PH, et al. Treating very long coronary artery lesions in the contemporary drug-eluting-stent era:single long 48 mm stent versus two overlapping stents showed comparable clinical results. Cardiovasc Revasc Med. 2020;21:1115-1118.
19. Peter Jüni RL, Löffel L, Wandel S, et al. Impact of Stent Overlap on Angiographic and Long-Term Clinical Outcome in Patients Undergoing Drug-Eluting Stent Implantation. J Am Coll Cardiol. 2010;55:1178–1188.
20. Lagache M, Coppel R, Finet G, et al. Impact of Malapposed and Overlapping Stents on Hemodynamics:A 2D Parametric Computational Fluid Dynamics Study. Mathematics. 2021;9:795.
21. Jurado-Román A, Abellán-Huerta J, Antonio Requena J, et al. Comparison of Clinical Outcomes Between Very Long Stents and Overlapping Stents for the Treatment of Diffuse Coronary Disease in Real Clinical Practice. Cardiovasc Revasc Med. 2019;20:681-686.
22. Patted SV, Jain RK, Jiwani PA, et al. Clinical Outcomes of Novel Long-Tapered Sirolimus Eluting Coronary Stent System in Real-World Patients With Long Diffused De Novo Coronary Lesions. Cardiol Res. 2018;9:350-357.
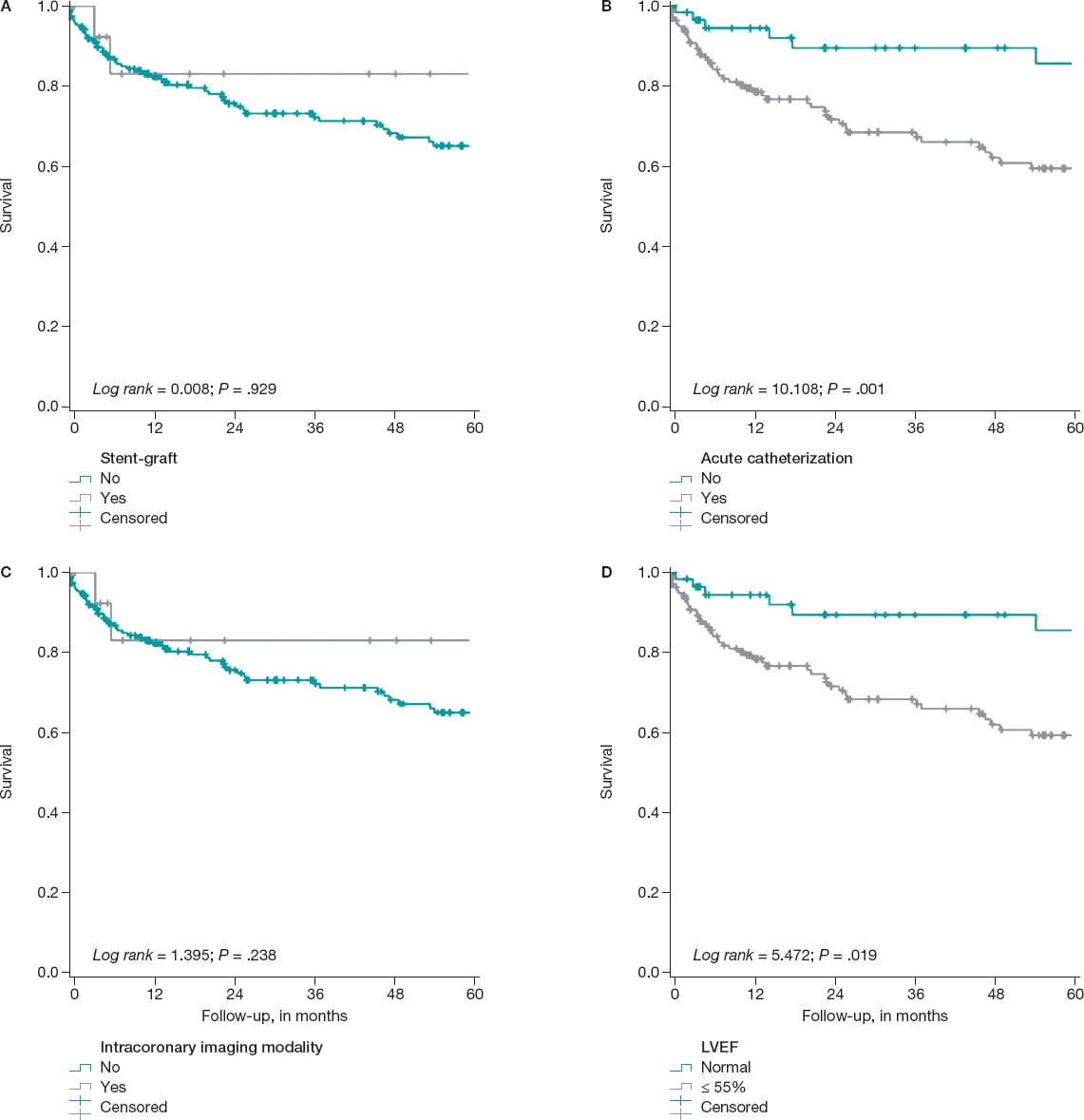
ABSTRACT
Introduction and objectives: Coronary artery aneurysms are a complex situation. Our main objective is to describe the frequency of use of covered stents (grafts) for their management, as well as to characterize their long-term results compared to drug-eluting stents.
Methods: Ambispective observational study with data from the International Coronary Artery Aneurysm Registry (CAAR) (NCT-02563626). Only patients who received a stent-graft or a drug-eluting stent where the aneurysm occurred were selected.
Results: A total of 17 patients received, at least, 1 stent-graft while 196 received 1 drug-eluting in the aneurysmal vessel. Male predominance, a higher rate of dyslipidemia, a past medical history of coronary artery disease, previously revascularized coronary artery disease, and giant aneurysms were reported in the stent-graft cohort. The independent predictive variables of the composite endpoint of all-cause mortality, heart failure, unstable angina, reinfarction, stroke, systemic embolism, bleeding or any aneurysmal complications at the median follow-up of 38 months were suggestive of the existence of connective tissue diseases (HR, 5.94; 95%CI, 1.82-19.37), left ventricular dysfunction ≤ 55% (HR, 1.84; 95%CI, 1.09-3.1), and an acute indication for heart catheterization (HR, 2.98; 95%CI, 1.39-6.3). The use of stent-grafts was not associated with the occurrence of more composite endpoints (23.5% vs 29.6%; P = .598).
Conclusions: The use of stent-grafts to treat coronary aneurysms is feasible and safe in the long-term. Randomized clinical trials are needed to decide what the best treatment is for these complex lesions.
Keywords: Coronary aneurysm. Registry. Stent. Stent graft. Angioplasty.
RESUMEN
Introducción y objetivos: Los aneurismas coronarios son una situación compleja. Planteamos como objetivo principal describir la frecuencia de utilización de stents recubiertos (grafts) para su tratamiento y caracterizar sus resultados a largo plazo en comparación con stents farmacoactivos.
Métodos: Estudio observacional ambispectivo, con información procedente del Registro Internacional de Aneurismas Coronarios (CAAR) (NCT-02563626). Se seleccionaron los pacientes que recibieron un stent-graft o un stent farmacoactivo en la zona del aneurisma.
Resultados: Un total de 17 pacientes recibieron al menos un stent-graft y 196 un stent farmacoactivo en la zona aneurismática. Se observa un predominio del sexo masculino y una mayor frecuencia de dislipemia, antecedentes de coronariopatía, enfermedad coronaria revascularizada previamente y aneurismas gigantes en la cohorte de stent-graft. Como variables independientes predictoras del desarrollo del evento combinado (muerte por cualquier causa, insuficiencia cardiaca, angina inestable, reinfarto, ictus, embolia sistémica, sangrado o cualquier complicación en el aneurisma), tras una mediana de seguimiento de 38 meses, destacaron la existencia de conectivopatías (hazard ratio [HR] = 5,94; intervalo de confianza del 95% [IC95%], 1,82-19,37), la disfunción del ventrículo izquierdo ≤ 55% (HR = 1,84; IC95%, 1,09-3,1) y la indicación aguda del cateterismo índice (HR = 2,98; IC95%, 1,39-6,3). El uso de stent-grafts comparado con el de stents farmacoactivos no se asoció al desarrollo de más eventos combinados (23,5 frente a 29,6%; p = 0,598).
Conclusiones: El uso de stents recubiertos en aneurismas coronarios es factible y seguro a largo plazo. Se necesitan estudios clínicos aleatorizados para decidir el mejor tratamiento de este tipo de lesiones complejas.
Palabras clave: Aneurismas coronarios. Registro. Resultados. Stent. Stent-graft. Angioplastia.
Abbreviations
LVEF: Left ventricular ejection fraction.
INTRODUCTION
The first descriptions of a coronary aneurysm were reported by Morgagni back in 1761, and the first series of 21 patients were reported in 1929.1-4 Since then, a variable incidence rate—between 0.3% and 12%—has been reported in several series following the implementation of imaging modalities and coronary angiography.5 The overall incidence rate reported in a cohort of over 436 000 contemporary coronary angiographies from an international registry is 0.35%.5 Same as it happens with the clinical presentation and profile, treatment varies significantly.5,6 Still, revascularization is often required here.6 Over the last few years, some of the alternatives available propose the use of stent-grafts for the exclusion of coronary aneurysms.5-14
These devices—initially developed for other indications15 such as coronary perforations—have proven useful and safe in the short-term, and in cases and series previously published.7-10,12
The main goal of this paper is to describe the frequency of use of this type of stents for the management of coronary aneurysms and characterize its long-term results using patients with drug-eluting stents as the control group since they have had good results in this context.5
METHODS
This paper uses data curated from the International Coronary Artery Aneurysm Registry (CAAR) (NCT-02563626).16 Using a methodology already published, this ambispective registry included data from adult patients (≥ 18 years) who underwent a coronary angiography for whatever reason in 32 hospitals from 9 different countries.5 Coronary aneurysm was defined as a focal dilatation (< 1/3 of the vessel) 1.5 times larger compared to the vessel diameter in a healthy adjacent segment; the giant aneurysm was defined as a dilatation 4 times larger compared to the reference diameter.16 Investigators were advised to collect a consecutive case series in specific closed periods of time. Both the clinical and the procedural variables were collected, as well as the events occurred during the index hospital stay considered as that moment when it was first reported that the patient had, at least, 1 coronary aneurysm. Then, after validating which patients were eligible, the clinical follow-up was performed with information from the health records collected via medical consultations or phone calls. As stated in former reports, the protocol was initially approved by the coordinating center ethics committee and then by the centers that required it. Data were collected anonymously, and patients gave their informed consent to all the study procedures. Clinical decisions were always made by the treating physician of every patient without any influence from the study protocol whatsoever. The analysis of this study only included patients who received a stent-grafts or drug-eluting stents in an aneurysmal area.
The study primary endpoint was to describe the real-life use of stent-grafts to treat coronary aneurysms. Secondary endpoints were to determine the occurrence of events at the long-term follow-up. Similarly, another secondary endpoint was to conduct a comparison with patients who received drug-eluting stents in the aneurysmal area. If both types of stents were implanted, the patient from the stent-graft group was considered. Similarly, the analyses were conducted individually in each patient.
Statistical analysis
The statistical package SPSS v24.0 (IBM-SPSS, United States) was used to conduct the statistical analysis. Data are expressed as mean ± standard deviation or as median and interquartile range, when appropriate. Categorical variables were expressed as percentages. Inter-group comparisons were made using the chi-square test with qualitative variables. On the other hand, the Student t test, Mann-Whitney U test or Wilcoxon test were used, when appropriate, with continuous variables. The long-term event-free survival curves for the different analyses and groups were obtained using the Kaplan-Meier method. In them, the inter-group comparisons were performed using the log-rank test.
Based on the principle of parsimony, multivariable models were used in which, to avoid ann excess of variables in the analysis, only those with P values ≤ .10 were included in the univariate study that will be further explained later. Both the hazard ratio (HR) and the confidence intervals were estimated at 95% (95%CI) based on a Cox logistic regression model with backward elimination (Wald). Two-tailed P values < .05 were considered statistically significant.
RESULTS
Out of a total of 1565 patients eventually considered in the global registry, 250 were referred for coronary artery surgery and 829 to receive some type of percutaneous revascularization.5 A total of 17 of these patients received, at least, 1 stent-graft to treat their coronary aneurysm. Also, 196 patients received a drug-eluting stent in the aneurysmal area. Therefore, the 17 and 196 patients mentioned before were included in the subsequent analyses of this study. Figure 1 shows the flow of patients.

Figure 1. Flow of the registry patients. The devices encircled in an oval were analyzed in this study. In the stent-graft group it was studied whether patients received a device of this type regardless of other devices.
Approximately, 8% of the patients specifically treated in the aneurysmal area received a stent-graft. Table 1 shows the clinical and angiographic characteristics, and the long-term events of both patients who received stent-grafts and those who received drug-eluting stents. Males were predominant and often showed signs of dyslipidemia, previous coronary arteriopathy, coronary artery disease with previous revascularization, and giant aneurysms in the cohort implanted with stent-grafts. The frequency and type of complications reported at the long-term follow-up with an overall median follow-up of 38 months are shown on table 1. No statistically significant differences were seen at the follow-up regarding the clinical events. A composite event rate of major adverse cardiovascular events (MACE) of 29.6% was reported in patients treated with drug-eluting stents compared to 23.5% in those treated with stent-grafts. Individually, the most common event reported in the group implanted with stent-grafts was unstable angina (11.8%). In the group treated with drug-eluting stents, the most common event was unstable angina (10.2%) and death (10.2%). Every individual event is shown on table 1.
Table 1. Overall characteristics of patients treated with stent-grafts compared to those treated with drug-eluting stents as first-line therapy for the management of coronary aneurysms
| Patients | Stent-graft (N = 17) | Drug-eluting stent (N = 196) | P |
|---|---|---|---|
| Clinical characteristics | |||
| Age, years | 61.47 ± 13.8 | 63.84 ± 12.8 | .467 |
| Sex, male | 16 (94.1) | 146 (74.5) | .069 |
| Arterial hypertension | 11 (64.7) | 142 (72.4) | .496 |
| Dyslipidemia | 15 (88.2) | 119 (60.7) | .024 |
| Diabetes | 3 (17.6) | 58 (29.6) | .296 |
| Smoking habit | .218 | ||
| Active smoker | 10 (58.8) | 82 (41.8) | |
| Former smoker | 3 (17.6) | 25 (12.8) | |
| Family history of coronary arteriopathy | 7 (41.2) | 14 (7.1) | < .001 |
| Kidney disease (CrCl < 30) | 1 (5.9) | 14 (7.1) | .846 |
| Peripheral vasculopathy | 1 (5.9) | 18 (9.2) | .647 |
| Aortopathy – aneurysms | 1 (5.9) | 6 (3.1) | .531 |
| Atrial fibrillation | 1 (5.9) | 7 (3.6) | .631 |
| Connective tissue disease | 0 | 3 (1.5) | .607 |
| LVEF | 56.8 ± 6.1 | 55.6 ± 11.4 | .657 |
| Previous revascularization | 8 (47.0) | 41 (20.9) | .014 |
| Angiographic characteristics | |||
| Right dominance | 14 (82.4) | 166 (84.7) | .641 |
| Serious coronary stenoses | 15 (88.2) | .132 | |
| 1 vessel disease | 4 (23.5) | 62 (31.6) | |
| 2-vessel disease | 6 (35.3) | 68 (34.7) | |
| 3-vessel disease | 5 (29.4) | 62 (31.6) | |
| Location of the aneurysma | |||
| Left main coronary artery | 0 | 3 (1.5) | .607 |
| LAD | 7 (41.2) | 125 (63.8) | .066 |
| LCX | 4 (23.5) | 49 (25) | .893 |
| RCA | 6 (35.3) | 53 (27.0) | .466 |
| Type of aneurysmb | .450 | ||
| Fusiform | 5 (29.4) | 85 (43.8) | |
| Saccular | 12 (70.6) | 107 (55.2) | |
| Giant aneurysm | 3 (17,6) | 5 (2,6) | .02 |
| Number of aneurysms per patient | .940 | ||
| 1 | 15 (88.2) | 155 (79.1.2) | |
| 2 | 2 (6.3) | 30 (15.3) | |
| 3 | 0 | 6 (3.1) | |
| 4 or more | 0 | 5 (2.5) | |
| Indication for catheterization, acute | 11 (64.7) | 144 (73.5) | .436 |
| Indication for catheterization | .179 | ||
| STEACS | 6 (35.3) | 49 (25.0) | |
| NSTEACS | 4 (23.5) | 91 (46.4) | |
| Heart failure | 1 (5.9) | 2 (1) | |
| Stable angina | 6 (35.3) | 32 (16.3) | |
| Other | 0 | 22 (11.2) | |
| Type of stent | – | ||
| Aneugraft | 4 (23.5) | ||
| Jostent-graftmaster | 11 (64.7) | ||
| Papyrus | 1 (5.9) | ||
| Undetermined stent-graft | 1 (5.9) | ||
| ABSORB | 2 (1.0) | ||
| ACTIVE | 28 (14.3) | ||
| BIOFREEDOM | 1 (0.5) | ||
| BIOMATRIX | 4 (2.0) | ||
| COMBO | 2 (1.0) | ||
| COROFLEX | 1 (0.5) | ||
| CRE8 | 8 (4.1) | ||
| CYPHER | 3 (1.5) | ||
| GENOUS | 1 (0.5) | ||
| JANUS | 2 (1.0) | ||
| NO ESPECIF | 8 (4.1) | ||
| ONYX | 1 (0.5) | ||
| ORSIRO | 3 (1.5) | ||
| PROMUS | 20 (10.2) | ||
| RESOLUTE | 23 (11.7) | ||
| STENTYS | 6 (3.1) | ||
| SYNERGY | 12 (6.1) | ||
| XIENCE | 47 (24.0) | ||
| TAXUS | 22 (11.2) | ||
| YUKON | 2 (1.0) | ||
| Size of the stent-graft, medians | |||
| Diameter | 3.5 (3.5-4.0) | 3.5 (3.0-3.75) | .336 |
| Length | 18.0 (16.0-26.0) | 20.0 (15.0-28.0) | .014 |
| Intracoronary imaging modalities | |||
| IVUS | 5 (29.4) | 19 (9.7) | .014 |
| OCT | 1 (5.9) | 7 (3.6) | .631 |
| Any or both | 6 (35.3) | 26 (13.3) | .015 |
| Follow-up | |||
| Median follow-up, months | 29.9 (2.33-51.54) | 46.95 (11.92-76.75) | .093 |
| Dual antiplatelet therapy at discharge | 17 (100) | 193 (99.5) | .767 |
| Duration of dual antiplatelet therapy, median | 12.0 (11.0-12.0) | 12 (12.0-12.0) | .372 |
| Oral anticoagulation/new indication | 2/0 | 9/0 | |
| Adverse events | |||
| Heart failure | 0 | 3 (1.5) | .607 |
| Unstable angina | 2 (11.8) | 20 (10.2) | .839 |
| Reinfarction | 1 (5.9) | 16 (8.2) | .739 |
| Clinically relevant bleeding | 1 (5.9) | 8 (4.1) | .723 |
| Embolism | 0 | 1 (0.5) | .768 |
| Stroke | 0 | 2 (1) | .676 |
| Dead | 0 | 20 (10.2) | .166 |
| All of the above or complicated aneurysm (MACE) | 4 (23.5) | 58 (29.6) | .598 |
| Coronary angiography at the follow-up | 8 (47.0) | 61 (31.1) | .187 |
| Control | 3 (17.6) | 16 (8.2) | |
| Stable angina | 3 (17.6) | 6 (3.1) | |
| NSTEACS | 2 (11.8) | 25 (12.8) | |
| STEACS | 0 | 6 (3.1) | |
| Other | 0 | 8 (4.0) | |
| Aneurysmal complications on the angiographyc | |||
| Growth | 0 | 7 (11.5) | .312 |
| New aneurysms | 0 | 3 (4.9) | .521 |
| Thrombosis | 0 | 6 (9.8) | .353 |
| In-stent restenosis | 1 (12.5) | 0 | .005 |
|
Cr, creatinine; IVUS, intravascular ultrasound; LAD, left anterior descending coronary artery; LCX, left circumflex artery; LVEF, left ventricular ejection fraction; MACE, major adverse cardiovascular events; NSTEACS, non-ST-segment elevation acute coronary syndrome; OCT, optical coherence tomography; RCA, right coronary artery; STEACS, ST-segment elevation acute coronary syndrome. Data are expressed as no. (%) or mean ± standard deviation. a There are more aneurysms than patients because the same patient can have several aneurysms. b Aneurysm was categorized as mixed (fusiform and saccular) in 2 patients. c Statistics is performed on a lower N, only in those with a coronary angiography at the follow-up. |
|||
Coronary angiographies at the follow-up became available for 69 patients (32.4%). Eight of them were performed in the group with stent-grafts and only 1 confirmed failed stent implantation due to in-stent restenosis. In the group treated with drug-eluting stents, the aneurysm grew bigger or new aneurysms appeared in over 15% of the patients with follow-up coronary angiographies available. The rate of thrombosis in this selected group reached 9.8%. Table 2 provides an overall comparison between patients with the composite endpoint of MACE and those without it.
Table 2. Clinical and angiographic characteristics of patients depending on whether they showed, at least, 1 major adverse cardiovascular event at the follow-upa
| Patients | Without events (N = 151) | Some MACE (N = 62) | P |
|---|---|---|---|
| Clinical characteristics | |||
| Age, years | 62.99 ± 12.37 | 65.29 ± 13.93 | .234 |
| Sex, make | 115 (76.2) | 47 (75.8) | .956 |
| Arterial hypertension | 107 (70.9) | 456 (74.2) | .623 |
| Dyslipidemia | 93 (61.6) | 41 (66.1) | .533 |
| Diabetes | 39 (25.8) | 22 (35.5) | .157 |
| Smoking habit | .808 | ||
| Active smoker | 64 (42.4) | 28 (30.4) | |
| Former smoker | 19 (12.6) | 9 (14.5) | |
| Family history of coronary arteriopathy | 17 (11.3) | 4 (6.5) | .285 |
| Kidney disease (CrCl < 30) | 8 (5.3) | 7 (11.3) | .120 |
| Peripheral vasculopathy | 9 (6.0) | 10 (16.1) | .018 |
| Aortopathy – aneurysms | 3 (2.0) | 4 (6.5) | .097 |
| Atrial fibrillation | 5 (3.3) | 3 (4.8) | .594 |
| Connective tissue disease | 0 | 3 (4.8) | .006 |
| LVEF | 56.62 ± 9.74 | 53.67 ± 13.44 | .080 |
| Previous revascularization | 36 (23.8) | 13 (21.0) | .651 |
| Angiographic characteristics | |||
| Right dominance | 127 (84.1) | 53 (85.5) | .237 |
| Serious coronary stenoses | 147 (97.4) | 60 (96.8) | .817 |
| 1 vessel disease | 47 (31.1) | 19 (30.6) | |
| 2-vessel disease | 52 (34.4) | 22 (35.5) | |
| 3-vessel disease | 48 (31.8) | 19 (30.6) | |
| Location of the aneurysmb | .429 | ||
| Left main coronary artery | 3 (2.0) | 0 | |
| LAD | 88 (58.3) | 44 (71) | |
| LCX | 41 (27.2) | 12 (19.4) | |
| RCA | 41 (27.2) | 18 (29.0) | |
| Type of aneurysmc | .676 | ||
| Fusiform | 62 (41.1) | 28 (45.2) | |
| Saccular | 86 (57.0) | 33 (53.2) | |
| Giant aneurysm | 4 (2.6) | 4 (6.5) | .185 |
| Number of aneurysms per patient | |||
| 1 | 122 (80.8) | 48 (77.4) | |
| 2 | 20 (13.2) | 12 (19.4) | |
| 3 | 6 (4.0) | 0 | |
| 4 or more | 3 (2.0) | 2 (3.2) | |
| Indication for catheterization, acute | 101 (66.9) | 54 (87.1) | .002 |
| Indication for catheterization | .053 | ||
| STEACS | 38 (25.1) | 17 (27.4) | |
| NSTEACS | 61 (40.4) | 34 (54.8) | |
| Heart failure | 2 (1.3) | 1 (1.6) | |
| Stable angina | 33 (21.8) | 5 (8.1) | |
| Other | 17 (11.2) | 5 (8.1) | |
| Type of stent | .598 | ||
| Stent-graft | 13 (8.6) | 4 (6.5) | |
| Drug-eluting stent | 138 (91.4) | 58 (93.5) | |
| Size of the stent-graft, medians | |||
| Diameter | 3.38 (3.0-4.0) | 3.28 (3.0-3.5) | .521 |
| Length | 22.00 (15.0-28.0) | 21.74 (15.0-25.0) | .843 |
| Intracoronary imaging modalities | |||
| IVUS | 17 (11.3) | 7 (11.3) | .995 |
| OCT | 8 (5.3) | 0 | .065 |
| Median follow-up, months | 34.0 (12.0-76.0) | 46.93 (18.75-79.75) | .646 |
|
CD: coronaria derecha; CX: circunfleja; Cr: creatinina; DA: descendente anterior; FEVI: fracción de eyección del ventrículo izquierdo; IVUS: ecocardiografía intravascular; MACE: eventos adversos cardiovasculares mayores; OCT: tomografía de coherencia óptica; SCACEST: síndrome coronario agudo con elevación del segmento ST; SCASEST: síndrome coronario agudo sin elevación del segmento ST. Los datos se expresan como n (%) o media ± desviación estándar. a Se consideró como MACE el combinado de muerte de cualquier causa, ingreso por insuficiencia cardiaca, angina inestable, reinfarto, ictus, embolia sistémica, sangrado que precisó atención médica o cualquier complicación del aneurisma (crecimiento, nuevo aneurisma, reestenosis o trombosis). b Hay más aneurismas que pacientes, porque cada enfermo puede presentar varios. c En varios pacientes (3 y 1, respectivamente) el aneurisma fue considerado mixto. |
|||
The multivariate analysis on the occurrence of MACE included in the model the use of stent-grafts. On the other hand, the univariate analysis included variables with P values ≤ .10. All of them are shown on table 2 including the presence or not, of peripheral vasculopathy (on therapy), previous diagnosis of aneurysm (in a territory different from the coronary one), diagnosed connective tissue disease, left ventricular ejection fraction, use of intracoronary imaging modalities (optical coherence tomography or intravascular ultrasound), and acute indication to perform index catheterization.
It was confirmed that the following variables remain in the model as independent predictors of the development of the composite endpoint: the existence of connective tissue disease (HR, 5.94; 95%CI, 1.82-19.37), left ventricular dysfunction—below 55%—(HR, 1.84; 95%CI, 1.09-3.1), and the acute indication for index catheterization (HR, 2.98; 95%CI, 1.39-6.3) (figure 2). The use of intracoronary imaging modalities—more common in the cohort implanted with stent-grafts—reached differences that were not statistically significant in the multivariate analysis. It was not a discriminator either regardless of the use of stent-grafts or drug-eluting stents (table 1, table 2, and figure 2).

Figure 2. Kaplan Meier survival curves free of the composite MACE event. A: on the use, or not of the stent-graft for the management of the aneurysm. B: based on whether the indication for index catheterization was acute (acute coronary syndrome, heart failure, etc.). C: regarding the use, during the angioplasty, of any of these intracoronary imaging modalities (intravascular ultrasound, optical coherence tomography or both), D: stratification based on the left ventricular ejection fraction (LVEF) when the angioplasty was performed.
DISCUSSION
This analysis is one of the largest series of coronary aneurysms published including data from real-life patients. It compares 2 of the most widely used therapeutic strategies in this context,5 and its main findings are:
a) The most widely used revascularization method in patients with coronary aneurysms was percutaneous.
b) The exclusion technique, that is, the use of stent-grafts, was used in a relatively lower number of cases (8%).
c) The clinical profile of patients treated with drug-eluting stents was similar compared to patients treated with stent-grafts. However, the presence of giant aneurysms is more common in the latter group. Also, it is probably one of the factors that operators pay most attention to when choosing one stent over the other.
d) An acute indication for the index catheterization and the presence of ventricular dysfunction, at that particular moment, are independent factors of poor prognosis in the study cohort.
e) In the long-term, a similar safety and efficacy profile can be seen in both arms of treatment making stent-grafts a reasonable alternative in selected cases with coronary aneurysms.
The specific treatment of patients with coronary aneurysms has not been well-defined yet to the point that it is not even quoted by the international clinical guidelines on revascularization.5 Over the last few years, several series and registries have been published trying to shed light on this issue.5,6,8,11 Generally speaking, coronary aneurysm is a rare coronary comorbidity. Nonetheless, the average interventional cardiologist sees 1 or several cases each year in his cath lab.7,16 As a matter of fact, in our own experience its estimated that its incidence rate is around 0.35% according to over 430 000 coronary angiographies performed,5 and around 1% according to a recent Chinese series of a little over 11 000 coronary angiographies.17 For this reason, it is important to have clinical data available to guide the management of this entity.7
Also, the coronary aneurysm is a clear marker of anatomic complexity and in adult patients it is suggestive of extensive coronary artery disease, and possibly, poor prognosis compared to milder forms of coronary arteriopathy.7 In previous analyses, the use of drug-eluting stents in patients with coronary aneurysms has been proposed as a therapeutic option clearly superior to conventional stents.5 That is why—as it happens with the rest of patients with ischemic heart disease—this type of platforms is widely recommended for patients with coronary aneurysms. Similarly, the use of an intense and thorough antithrombotic therapy is probably associated with fewer evolutionary complications, which is really reasonable considering the already mentioned high ischemic risk of these patients.11,18
The use of stent-grafts has been proposed as an alternative that can restore the anatomy of the blood vessel. Although the early design of these stents originally served other purposes, the data supporting the feasibility of their use with a high rate of success are extensive.8 In our series, the stent most widely used was the classically designed Jostent Graftmaster coronary stent graft system (Abbott Vascular, United States) (nearly 65%). It is composed of a PTFE layer between 2 stainless-steel stents that may have influenced the results. As a matter of fact, in our setting, Jurado-Román et al.15 conducted a multicenter registry on a certain state-of-the-art stent-graft. They proved that, in several real-life indications, the rate of events is reasonable (MACE, 7.1% at an average 22 months). However, the rate of stent thrombosis was slightly higher (3%) compared to the rate reported by drug-eluting stents in common uses.
The use of intracoronary imaging modalities to perform angioplasties in patients with coronary aneurysms possibly has prognostic implications as it happens in other complex clinical situations (diagnostic doubts, left main coronary artery, bifurcations). In this series, although they were more widely used in the group with stent-grafts implanted, no statistically significant differences were seen on the development of MACE (figure 2). This possibly has to do with the size of the study sample. Also, a tendency was seen towards fewer events in the group of patients with procedures optimized through intracoronary imaging guidance whether intravascular ultrasound or optical coherence tomography.
Limitations
This study has limitation associated with the particular design of the study. Also, a relatively small number of participants was included, which may have complicated the detection of differences in the analyses due to the lack of statistical power. The decision to implant stent-grafts or drug-eluting stents was entirely left to each patient’s medical team, which may have been associated with a certain degree of heterogeneity in the protocols that could have also been more dynamic in time. At the very complete follow-up from the clinical standpoint, control angiographies became available for a limited number of patients only (32%) who met the criterion set by the treating physicians. This may have underestimated the rate of complications, especially the subclinical ones, or be associated with selection biases in both groups.
However, this study is an approach to real-life clinical practice for a relatively rare heart disease on which there is little information available. It also includes a long-term clinical follow-up.
CONCLUSIONS
Stents-grafts can be used to treat coronary aneurysms and are safe in the long-term. Randomized clinical trials are needed to decide what the best treatment is for this type of complex coronary lesions.
FUNDING
None.
AUTHORS’ CONTRIBUTIONS
I. J. Núñez-Gil, CAAR coordinator: study design, data analysis, and draft writing. E. Cerrato, M. Bollati, L. Nombela-Franco, and A. Fernández-Ortiz: study design. E. Cerrato, M. Bollati, B. Terol, E. Alfonso-Rodríguez, S. J. Camacho-Freire, P. A. Villablanca, I. J. Amat-Santos, J.M. de la Torre-Hernández, I. Pascual, C. Liebetrau, B. Camacho, M. Pavani, R. A. Latini, F.Varbella, V. A. Jiménez Díaz, D. Piraino, MM, F. Alfonso, J. Antonio Linares, J. M. Jiménez-Mazuecos, J. Palazuelos- Molinero, and I. Lozano: data mining and recruitment. E. Cerrato, M. Bollati, B. Terol, L. Nombela-Franco, E. Alfonso-Rodríguez, S. J. Camacho-Freire, P. A. Villablanca, I. J. Amat-Santos J.M. de la Torre-Hernández, I. Pascual, C. Liebetrau, B. Camacho, M. Pavani, R. A. Latini, F.Varbella, V. A. Jiménez Díaz, Davide Piraino, M. Mancone, F. Alfonso, J. A. Linares, J. M. Jiménez-Mazuecos, J. Palazuelos- Molinero, IÍ. Lozano, and A. Fernández-Ortiz: reading and critical review of the manuscript.
CONFLICTS OF INTEREST
J. M. de la Torre Hernández is the editor-in-chief of REC: Interventional Cardiology, and F. Alfonso is an associate editor of this journal. The journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. No other conflicts of interest have been declared whatsoever.
WHAT IS KNOWN ABOUT THE TOPIC?
- Coronary aneurysms are a complex entity whose incidence rate is between 0.3 and 12% in the different series already published.
- Treatment, like the presentation and the clinical profile, is varied. However, revascularization is often required.
- In this sense, over the last few years, some of the alternatives available propose the use of stent-grafts for the exclusion of coronary aneurysms.
WHAT DOES THIS STUDY ADD?
- The main goal of this paper was to describe the frequency of use of this type of stents to treat coronary aneurysms and then characterize its long-term results.
- From a total of 829 patients with coronary aneurysms treated with some type of percutaneous revascularization, data on the use of stent-grafts and drug-eluting stents was collected in 17 and 196 patients, respectively.
- It seems obvious that patients treated with stent-grafts for the management of coronary aneurysms have a high ischemic load, often complex anatomies, and even more often giant aneurysms.
- The use of stent-grafts for the management of coronary aneurysms is feasible and safe in the long-term. However, randomized clinical trials are still needed to decide what the best therapy is for this type of complex coronary lesions.
SUPPLEMENTARY DATA

REFERENCES
1. Bourgon A. Biblioth Med. 1812;37:183. Citado por Scott DH. Aneurysm of the coronary arteries. Am Heart J. 1948;36:403-421.
2. Packard M, Wechsler H. Aneurysms of coronary arteries. Arch Intern Med. 1929;43:1-14.
3. Swaye PS, Fisher LD, Litwin P, et al. Aneurysmal coronary artery disease. Circulation. 1983;67:134-138.
4. Cohen P, O'Gara PT. Coronary artery aneurysms:a review of the natural history, pathophysiology, and management. Cardiol Rev. 2008;16:301-304.
5. Núñez-Gil IJ, Cerrato E, Bollati M, et al. Coronary artery aneurysms, insights from the international coronary artery aneurysm registry (CAAR). Int J Cardiol. 2020;299:49-55.
6. Núñez-Gil IJ, Terol B, Feltes G, et al. Coronary aneurysms in the acute patient:Incidence, characterization and long-term management results. Cardiovasc Revasc Med. 2018;19(5 Pt B):589-596.
7. Kawsara A, Núñez Gil IJ, Alqahtani F, Moreland J, Rihal CS, Alkhouli M. Management of Coronary Artery Aneurysms. JACC Cardiovasc Interv. 2018;11:1211-1223.
8. Will M, Kwok CS, Nagaraja V, et al. Outcomes of patients who undergo elective covered stent treatment for coronary artery aneurysms. Cardiovasc Revasc Med. 2021:S1553-8389(21)00264-5.
9. Núñez-Gil IJ, Alberca PM, Gonzalo N, Nombela-Franco L, Salinas P, Fernández-Ortiz A. Giant coronary aneurysm culprit of an acute coronary syndrome. Rev Port Cardiol (Engl Ed). 2018;37:203.e1-203.e5.
10. Cha JJ, Kook H, Hong SJ, et al. Successful Long-term Patency of a Complicated Coronary Aneurysm at a Prior Coronary Branch Stent Treated with a Stent-graft and Dedicated Bifurcation Stent. Korean Circ J. 2021;51:551-553.
11. Khubber S, Chana R, Meenakshisundaram C, et al. Coronary artery aneurysms:outcomes following medical, percutaneous interventional and surgical management. Open Heart. 2021;8:e001440.
12. Arbas-Redondo E, Jurado-Román A, Jiménez-Valero S, Galeote-García G, Gonzálvez-García A, Moreno-Gómez R. Acquired coronary aneurysm after stent implantation at a bifurcation excluded with a Papyrus covered stent subsequently fenestrated. Cardiovasc Interv Ther. 2022;37:215-216.
13. Della Rosa F, Molina-Martin de Nicolas J, Bonfils L, Fajadet J. Symptomatic giant coronary artery aneurysm treated with covered stents. Coron Artery Dis. 2020;31:658-659.
14. Tehrani S, Faircloth M, Chua TP, Rathore S. Percutaneous coronary intervention in coronary artery aneurysms;technical aspects. Report of case series and literature review. Cardiovasc Revasc Med. 2021;28S:243-248.
15. Jurado-Román A, Rodríguez O, Amat I, et al. Clinical outcomes after implantation of polyurethane-covered cobalt-chromium stents. Insights from the Papyrus-Spain registry. Cardiovasc Revasc Med. 2021;29:22-28.
16. Núñez-Gil IJ, Nombela-Franco L, Bagur R, et al. Rationale and design of a multicenter, international and collaborative Coronary Artery Aneurysm Registry (CAAR). Clin Cardiol. 2017;40:580-585.
17. Jiang X, Zhou P, Wen C, et al. Coronary Anomalies in 11,267 Southwest Chinese Patients Determined by Angiography. Biomed Res Int. 2021;2021:6693784.
18. D'Ascenzo F, Saglietto A, Ramakrishna H, et al. Usefulness of oral anticoagulation in patients with coronary aneurysms:Insights from the CAAR registry. Catheter Cardiovasc Interv. 2021;98(5):864-871.
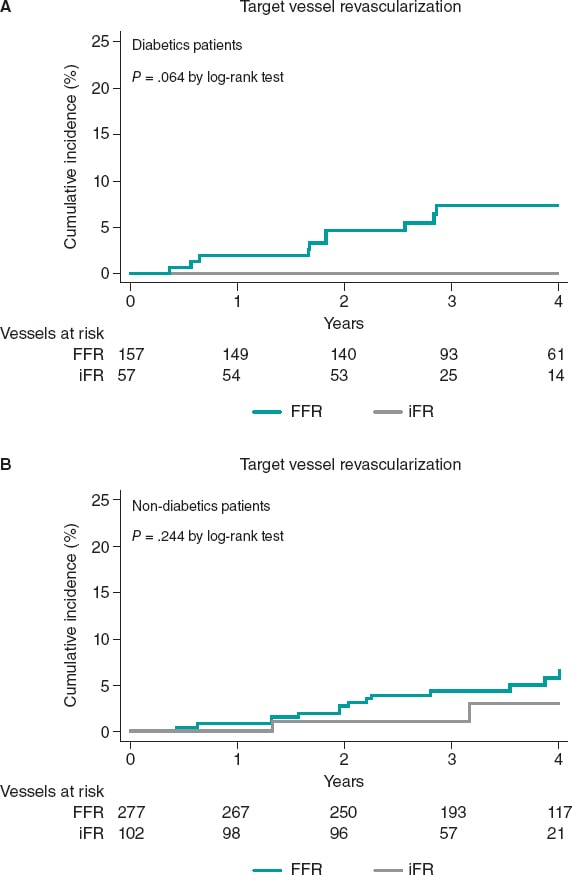
ABSTRACT
Introduction and objectives: The safety of physiology-based revascularization in patients with diabetes mellitus has been scarcely investigated. Our objective was to determine the safety of deferring revascularization based on the fractional flow reserve (FFR) or the instantaneous wave-free ratio (iFR) in diabetic patients.
Methods: Single-center, retrospective analysis of patients with intermediate coronary stenoses in whom revascularization was deferred based on FFR > 0.80 or iFR > 0.89 values. The long-term rate of major adverse cardiovascular events, a composite of all-cause mortality, myocardial infarction, and target vessel revascularization (TVR), was assessed in diabetic and non-diabetic patients at the follow-up. The rate of TVR based on the type of physiological index used to defer the lesion was also evaluated.
Results: We evaluated 164 diabetic (214 vessels) and 280 non-diabetic patients (379 vessels). No significant differences in the rate of major adverse cardiovascular events was seen between diabetic and non-diabetic patients (20.1% vs 13.2%; P = .245) at a median follow-up of 43 months. All-cause mortality and cardiac death were not statistically different between both groups in the adjusted analysis (P > .05). A trend towards a higher rate of myocardial infarction was seen in diabetic patients (6.7% vs 2.9%; P = .063). However, the rate of target vessel myocardial infarction was similar in both groups (P = .874). Overall, TVR was similar in diabetics and non-diabetics (4.7% vs 4.2%; P = .814); however, when analyzed based on the physiological index, numerically, diabetics had a higher rate of TVR when the FFR was used in the decision-making process compared to when the iFR was used (6.4% vs 0.0%; P = .064).
Conclusions: Deferring the revascularization of intermediate stenoses in patients with DM based on the FFR or the iFR is safe regarding the risk of TVR or target vessel myocardial infarction, with a rate of events at the long-term follow-up similar to that seen in non-diabetic patients.
Keywords: Fractional flow reserve. Instantaneous wave-free ratio. iFR. Diabetes mellitus.
RESUMEN
Introducción y objetivos: La seguridad de la revascularización fisiológica en pacientes diabéticos ha sido poco investigada. El objetivo fue determinar la seguridad de diferir la revascularización basándose en la reserva fraccional de flujo (FFR) o en el índice instantáneo libre de ondas (iFR) en pacientes con diabetes mellitus.
Métodos: Análisis retrospectivo, unicéntrico, de pacientes con estenosis coronarias intermedias en quienes se había diferido la revascularización en función de unos valores de FFR > 0,80 o de iFR > 0,89. Se analizó la incidencia a largo plazo de eventos cardiovasculares adversos mayores, una combinación de muerte por cualquier causa, infarto miocárdico y revascularización del vaso diana (RVD) en pacientes con y sin diabetes. También se evaluó la incidencia de RVD según el tipo de índice fisiológico utilizado para diferir la revascularización.
Resultados: Se evaluaron 164 pacientes diabéticos (214 vasos) y 280 pacientes no diabéticos (379 vasos), con una mediana de seguimiento de 43 meses. No se observaron diferencias significativas en los eventos cardiovasculares adversos mayores entre pacientes con y sin diabetes mellitus (20,1 frente a 13,2%; p = 0,245). La mortalidad por cualquier causa y de causa cardiaca no fue estadísticamente diferente entre ambos grupos en el análisis ajustado (p > 0,05). Se observó una tendencia a una mayor incidencia de infarto de miocardio en los pacientes con diabetes mellitus (6,7 frente a 2,9%; p = 0,063), pero el infarto relacionado con el vaso diana fue similar en ambos grupos (p = 0,906). En general, la RVD fue similar en diabéticos y no diabéticos (4,7 frente a 4,2%; p = 0,787); sin embargo, cuando se analizó según el índice fisiológico, los diabéticos tuvieron una mayor tasa numérica de RVD cuando se utilizó la FFR en la toma de decisiones en comparación con el iFR (6,4 frente a 0,0%; p = 0,064).
Conclusiones: Diferir la revascularización de estenosis intermedias en pacientes con diabetes mellitus según la FFR o el iFR es seguro en términos de RVD e infarto relacionado con el vaso diana, con una tasa de eventos en el seguimiento a largo plazo similar a la observada en pacientes sin diabetes mellitus.
Palabras clave: Reserva fraccional de flujo. Indice instantaneo libre de ondas. iFR. Diabetes mellitus.
Abbreviations
DM: diabetes mellitus. FFR: fractional flow reserve. iFR: instantaneous wave-free ratio. MACE: major adverse cardiovascular events. TVR: target vessel revascularization.
INTRODUCTION
Physiological evaluation has a class IA recommendation to guide coronary revascularization in the current clinical practice guidelines.1 Fractional flow reserve (FFR) and instantaneous wave-free ratio (iFR) have proven to be safe tools to guide revascularization therapy in several clinical scenarios.2-4
The results of the DEFER trial at the 15-year follow-up showed the long-term safety of FFR to defer therapy in functionally non-significant stenosis.5 Afterwards, the DEFINE-FLAIR and the iFR-SWEDEHEART trials proved the non-inferiority of the iFR compared to the FFR to guide revascularization of moderate stenosis at the 1-year follow-up.3,6 The utility of physiological guidance to guide revascularization in multivessel disease has been confirmed in the FAME and the SYNTAX II clinical trials.7,8
However, the prognostic value of pressure guidewire assessment in certain high-risk groups has not been firmly established yet. A pooled analysis of the DEFINE-FLAIR and the iFR-SWEDEHEART trials found a higher rate of events in patients with acute coronary syndrome in whom revascularization of non-culprit vessels was deferred based on the FFR or the iFR compared to stable patients.3,6 Patients with diabetes mellitus (DM) are a high-risk group with a well-known higher burden of cardiovascular disease and worse prognosis including more extensive atherosclerosis, more prevalence of multivessel disease, and a faster disease progression compared to non-diabetic patients.9-11 The special characteristics of the extent and spread of atherosclerosis in patients with DM raises concerns on the safety surrounding deferring revascularization in this population. Our objective was to evaluate the safety of revascularization deferral based on pressure guidewire interrogation in diabetic patients at the long-term follow-up.
METHODS
Study population
This is a single center, retrospective, and open-label trial. The study population was recruited from a total of 1321 consecutive patients with coronary artery disease in whom the iFR or the FFR indices were used to determine the need for coronary revascularization from January 2012 through December 2016. In 444 patients (34%) the revascularization of ≥ 1 lesions was deferred based on FFR values > 0.80 or iFR values > 0.89. Patients with stable angina and acute coronary syndrome (with non-culprit stenosis interrogated with pressure guidewires) were included in the study. For the analysis, the overall population was divided into 2 groups: DM and non-DM. The DM group was defined based on their past personal history included in their medical records. The study flow chart depicting patient selection is shown on figure 1.
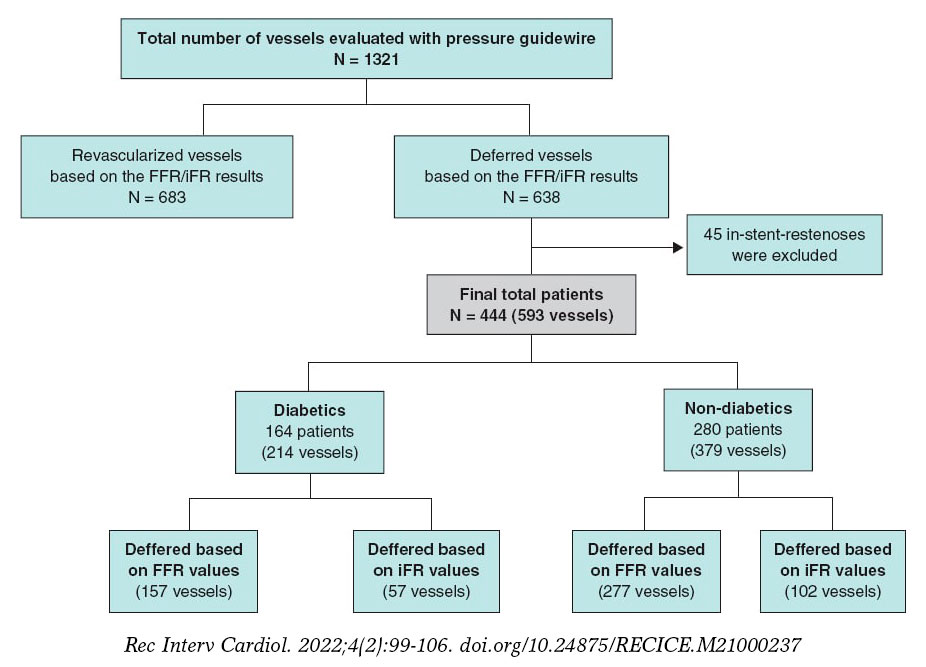
Figure 1. Study flow chart. iFR, instantaneous wave-free ratio; FFR, fractional flow reserve.
This retrospective, cohort study was conducted according to the principles established by the Declaration of Helsinki. Both the informed consent and the research committee assessment were spared due to the retrospective nature of the study; each patient included in the database was encrypted and de-identified to protect everyone’s privacy.
The physiological procedure
Pressure guidewire assessment was performed using a commercial guidewire (Verrata, Philips Healthcare, United States; PressureWire [Certus. Aeris, X] St. Jude Medical, United States) and the standard technique previously reported.3,12 As a standard practice, an intracoronary bolus of nitrates (200 mcg) was administered before the FFR or iFR measurements. The cases submitted for FFR assessment received IV adenosine at a rate of 140 µg/kg/min. The cut-off values to defer revascularization were FFR > 0.80 or iFR > 0.89. The presence of significant drift was discarded by placing the sensor of the pressure guidewire on the tip of the guiding catheter at the end of the physiological measurements acquisition.
In patients with stable angina, the physiological evaluation was performed as part of the same procedure, and all intermediate stenoses were assessed. In patients with acute coronary syndrome, interrogation with the pressure guidewire was performed at a staged procedure in non-culprit vessels only.
Endpoints
The primary endpoint was the 4-year risk of major adverse cardiovascular events (MACE) defined as a composite endpoint of all-cause mortality, myocardial infarction or unplanned target vessel revascularization (TVR). The secondary endpoints were a) the individual components of MACE, b) the rate of target vessel myocardial infarction, and c) the rate of unplanned TVR based on the physiological index used (FFR or iFR)
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD). Discrete variables are summarized as frequency (percentages). Under baseline conditions, group comparisons were made using the Student t test or the Mann Whittney U test for continuous variables and Pearson’s chi-square test for discrete data.
Time-to-event analysis was performed using the Kaplan-Meier method, and group comparison was performed using the Mantel-Cox (log-rank) test. For the primary and secondary endpoint comparison between diabetics and non-diabetics, a Cox Proportional hazards model was used to estimate hazard ratios (HR). The adjusted analysis was performed based on age, sex, hypertension, dyslipidemia, smoking habit, chronic kidney disease, previous stroke, previous percutaneous coronary intervention, and coronary artery bypass graft surgery.
All probability values were 2-sided with 95% confidence intervals (95%CI). P values < .05 were considered statistically significant. The SPSS version 23.0 (IBM Corp, Armonk, NY, United States) and STATA version 15 (Stata Corp, College Station, TX, United States) statistical packages were used for statistical analyses.
RESULTS
Baseline clinical and angiographic characteristics
The baseline clinical characteristics are shown on table 1. In the overall study population, mean age was 68.4 years, and 39.6% were patients with DM (164 patients). As expected, patients with DM had more cardiovascular risk factors and comorbidities compared to patients without DM. There were no significant differences in the clinical presentation between both study groups (P > .05). Most patients received optimal medical treatment at the hospital discharge without significant differences between DM and non-DM patients (P > .05).
Table 1. Baseline characteristics
| Total (N = 444) | Diabetics (N = 164) | Non-diabetics (N = 280) | P | |
|---|---|---|---|---|
| Clinical characteristics, N (%) | ||||
| Sex | .026 | |||
| Male | 340 (76.5) | 116 (70.7) | 224 (80.0) | |
| Female | 104 (23.4) | 48 (29.3) | 56 (20.0) | |
| Age (year) | 68.41 | 70.02 | 67.46 | .003 |
| Arterial hypertension | 321 (72.3) | 138 (84.1) | 183 (65.4) | <.001 |
| Hyperlipidemia | 287 (64.6) | 124 (75.6) | 163 (58.2) | <.001 |
| Current smoker | 253 (57.0) | 85 (51.8) | 168 (60.0) | .093 |
| Chronic kidney disease | 41 (9.2) | 29 (17.7) | 12 (4.3) | .000 |
| COPD | 30 (6.8) | 9 (5.5) | 21 (7.5) | .415 |
| Previous cerebrovascular disease | 21 (4.7) | 12 (7.3) | 9 (3.2) | .049 |
| Peripheral vascular disease | 38 (8.6) | 18 (11.0) | 20 (7.1) | .164 |
| Previous AMI | 47 (10.6) | 17 (10.4) | 30 (10.7) | .908 |
| Previous PCI | 220 (49.5) | 70 (42.7) | 150 (53.6) | .027 |
| Previous CABG | 13 (2.9) | 9 (5.5) | 4 (1.4) | .019 |
| Clinical presentation, N (%) | ||||
| Myocardial infarction | 148 (33.3) | 46 (28.0) | 102 (36.4) | .302 |
| Unstable angina | 89 (20.0) | 33 (20.1) | 56 (20.0) | |
| Stable angina | 112 (25.2) | 44 (26.8) | 68 (24.3) | |
| Silent ischemia | 46 (10.4) | 22 (13.4) | 24 (8.6) | |
| Other | 49 (11.0) | 19 (11.6) | 30 (10.7) | |
| Therapy at discharge, N (%) | ||||
| Aspirina | 408 (93.8) | 150 (94.3) | 258 (93.5) | .720 |
| Clopidogrela | 165 (37.9) | 53 (33.3) | 112 (40.6) | .134 |
| Prasugrela | 22 (5.1) | 9 (5.7) | 13 (4.7) | .663 |
| Ticagrelora | 78 (17.9) | 30 (18.9) | 48 (17.4) | .699 |
| DAPT | 332 (56.3) | 111 (52.6) | 221 (58.3) | .181 |
| Statinsb | 396 (93.2) | 148 (93.1) | 248 (93.2) | .952 |
| Beta-blockersb | 334 (78.6) | 121 (76.1) | 213 (80.1) | .334 |
| ACEIb | 324 (76.2) | 126 (79.2) | 198 (74.4) | .260 |
| Acenocoumarola | 41 (9.4) | 18 (11.3) | 23 (8.3) | .304 |
| Insulin | 53 (8.9) | 53 (24.8) | ||
|
ACEI, angiotensin converting enzyme inhibitors; AMI, acute myocardial infarction; CABG, coronary artery bypass grafting;; COPD, chronic obstructive pulmonary disease; PCI, percutaneous coronary intervention. a n = 435. b n = 425. |
||||
Characteristics of vessels with deferred revascularization
On average, deferred revascularization was performed in vessels with stenoses of intermediate severity (percent diameter stenosis, 59.73% ± 9.2%). The most frequently interrogated artery was the left anterior descending coronary artery (43.2%). In most patients, only 1 vessel was deferred (72.7%). Nevertheless, in about 4% of patients, revascularization was deferred in 3 vessels within the same procedure.
In our study population, revascularization deferral was based more frequently in the FFR (434 vessels, 73.2%) compared to the iFR (159 vessels, 26.8%). The same ratio applied to patients with DM: revascularization was deferred in 157 vessels (73.4%) based on FFR values compared to 57 vessels (26.6%) based on iFR values. The mean FFR and iFR values of the overall population were 0.87 ± 0.46 and 0.94 ± 0.41, respectively without any significant differences between diabetic and non-diabetic patients (table 2).
Table 2. Characteristics of the deferred arteries
| Total (N = 593) | Diabetics (N = 214) | Non-diabetics (N = 379) | P | |
|---|---|---|---|---|
| Deferred vessel | ||||
| LMCA | 25 (4.2) | 8 (3.7) | 17 (4.5) | .664 |
| LAD | 256 (43.2) | 90 (42.1) | 166 (43.8) | .681 |
| LCX | 173 (29.2) | 59 (27.6) | 114 (30.1) | .519 |
| RCA | 138 (23.3) | 57 (26.6) | 81 (21.4) | .145 |
| Number of deferred vessels per patient* | ||||
| 1 vessel | 323 (72.7) | 122 (74.4) | 201 (71.8) | .475 |
| 2 vessels | 98 (22.1) | 35 (21.3) | 63 (22.5) | |
| 3 vessels | 19 (4.3) | 7 (4.3) | 12 (4.3) | |
| 4 vessels | 4 (0.9) | 4 (1.4) | 0 (0.0) | |
| Coronary physiological parameters | ||||
| Mean FFR | 0.87 ± 0.46 | 0.86 ± 0.41 | 0.87 ± 0.48 | .387 |
| Mean iFR | 0.94 ± 0.41 | 0.94 ± 0.43 | 0.95 ± 0.40 | .091 |
| Deferred based on FFR values | 434 (73.2) | 157 (73.4) | 277 (73.1) | .942 |
| Deferred based on iFR values | 159 (26.8) | 57 (26.6) | 102 (26.9) | .942 |
|
FFR, fractional flow reserve; iFR, instantaneous wave-free ratio; LAD, left anterior descending coronary artery; LCX, left circumflex artery; LMCA, left main coronary artery; RCA, right coronary artery. * n = 444. |
||||
Clinical outcomes at the long-term follow-up based on the presence of diabetes
The median follow-up was 43 months [interquartile range, 31.1-55.8] without any differences being reported between DM and non-DM patients. The clinical outcomes are shown on table 3. Diabetic patients had higher rates of MACE (33 [20.1%] vs 37 [13.2%] in non-DM patients) although this difference did not reach statistical significance in the adjusted analysis (HR, 0.98, 95%CI; 0.46-2.11, P = .964). The all-cause mortality rate was higher in diabetics (18 [10.8%] vs 15 [5.3%] in non-diabetics), but the rates of cardiovascular death were not statistically different in either group (3.1% vs 2.1%). A trend towards a higher rate of myocardial infarction was seen in patients with DM (6.7% vs 2.9%; P = .063), yet target vessel myocardial infarction was similar in both groups (HR, 0,87; 95%CI, 0.15-4.89, P = .906). Similar rates of unplanned revascularization and TVR were seen between diabetics and non-diabetics (figure 2 and table 3).
Table 3. Clinical events at the 4-year follow-up based on the presence of diabetes
| Diabetics (N = 164) |
Non-diabetics (N = 280) |
Unadjusted analysis | Fully adjusted analysis* | |||
|---|---|---|---|---|---|---|
| HR (95%CI) | P | HR (95%CI) | P | |||
| MACE | 33 (20.1) | 37 (13.2) | 1.58 (0.99-2.53) | .058 | 0.98 (0.46-2.11) | .964 |
| All-cause mortality | 18 (10.8) | 15 (5.3) | 2.10 (1.06-4.17) | .034 | 2.01 (0.92-4.40) | .079 |
| Cardiovascular death | 5 (3.1) | 6 (2.1) | 1.45 (0.44-4.74) | .543 | 0.72 (0.19- 2.76) | .641 |
| Myocardial infarction | 11 (6.7) | 8 (2.9) | 2.54 (1.02-6.32) | .045 | 2.56 (0.95- 6.91) | .063 |
| Unplanned revascularization | 17 (10.4) | 20 (7.1) | 1.53 (0.80-2.93) | .195 | 1.55 (0.77- 3.10 | .219 |
| Diabetic vessels (N = 214) |
Non-diabetic vessels (N = 379) |
Unadjusted analysis | Fully adjusted analysis* | |||
| HR (95%CI) | P | HR (95%CI) | P | |||
| Target vessel myocardial infarction | 2 (0.9) | 4 (1.1) | 0.96 (0.18-5.23) | .971 | 0.87 (0.15-4.89) | .874 |
| Target vessel revascularization | 10 (4.7) | 16 (4.2) | 1.15 (0.52-2.54) | .767 | 1.14 (0.38-3.42) | .814 |
|
95%CI, 95% confidence interval; HR, hazard ratio; MACE, mayor adverse cardiovascular events (all-cause mortality, myocardial infarction, target vessel revascularization). * HR and P values are obtained after adjusting the model with different baseline variables (age, hypertension, dyslipidemia, smoking habit, chronic kidney disease, previous percutaneous coronary intervention, and previous coronary artery bypass grafting). |
||||||
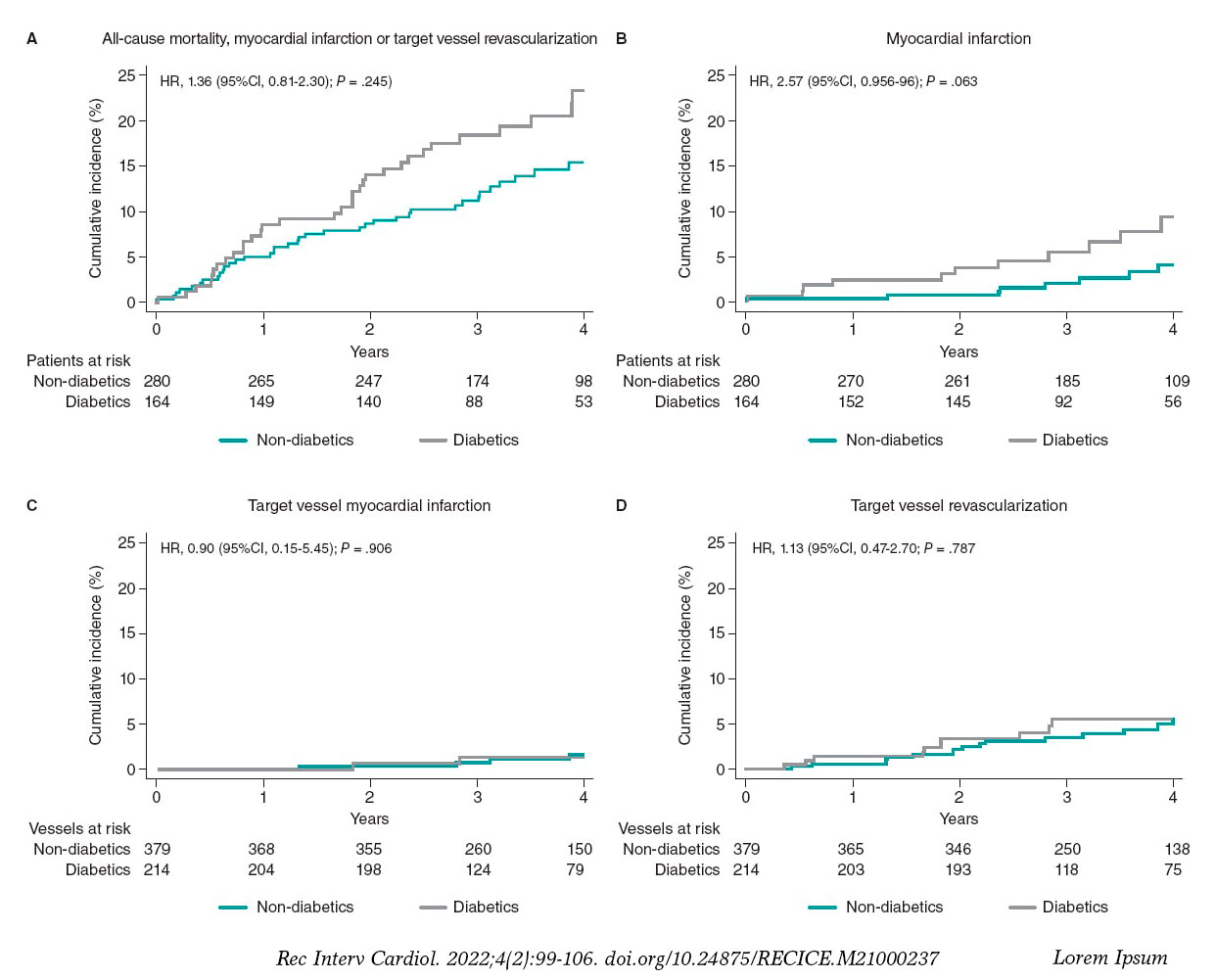
Figure 2. Clinical outcomes in diabetic and non-diabetic patients at the 4-year follow-up. 95%CI, 95% confidence interval; HR, hazard ratio.
Clinical outcomes at the long-term follow-up based on the physiological index used to defer revascularization
In patients with DM the physiological index used (FFR or iFR) that led to revascularization deferral was not associated with a significant difference in the rate of MACE (P = .688) or with significant differences in all-cause mortality, cardiovascular death, myocardial infarction or unplanned revascularization. Similar rates of target vessel myocardial infarction were seen in patients deferred with both techniques (DM or non-DM) (table 4).
Table 4. Clinical outcomes at the 4-year follow-up based on the technique to defer revascularization
| Patients deferred based on FFR values (N = 347) |
Patients deferred based on iFR values (N = 97) |
P (log-rank) |
|
|---|---|---|---|
| MACE | 59 (17.0) | 11 (11.3) | .288 |
| Diabetics | 27 (21.1) | 6 (16.7) | .688 |
| Non-diabetics | 32 (14.6) | 5 (8.2) | .277 |
| All-cause mortality | 25 (7.2) | 8 (8.3) | .574 |
| Diabetics | 13 (10.2) | 5 (13.9) | .417 |
| Non-diabetics | 12 (5.5) | 3 (4.9) | .972 |
| Cardiovascular mortality | 8 (2.3) | 3 (3.1) | .593 |
| Diabetics | 4 (3.1) | 1 (2.8) | .964 |
| Non-diabetics | 4 (1.8) | 2 (3.3) | .436 |
| Myocardial infarction | 16 (4.6) | 3 (3.1) | .762 |
| Diabetics | 10 (7.8) | 1 (2.8) | .396 |
| Non-diabetics | 6 (2.7) | 2 (3.3) | .596 |
| Unplanned revascularization | 33 (9.5) | 4 (4.1) | .133 |
| Diabetics | 16 (12.5) | 1 (2.8) | .112 |
| Non-diabetics | 17 (7.8) | 3 (4.9) | .542 |
| Patients deferred based on FFR values (N = 434) |
Patients deferred based on iFR values (N = 159) |
P (log-rank) |
|
| Target vessel myocardial infarction | 4 (0.9) | 2 (1.3) | .527 |
| Diabetics | 2 (1.3) | 0 (0.0) | .433 |
| Non-diabetics | 2 (0.7) | 2 (2.0) | .172 |
| Target vessel revascularization | 24 (5.5) | 2 (1.3) | .037 |
| Diabetics | 10 (6.4) | 0 (0.0) | .064 |
| Non-diabetics | 14 (5.1) | 2 (2.0) | .244 |
|
iFR, instantaneous wave-free ratio; FFR, fractional flow reserve; MACE, mayor adverse cardiovascular events (all cause-mortality, myocardial infarction, target vessel revascularization). |
|||
The rate of TVR was significantly higher in patients deferred based on FFR values compared to patients deferred based on iFR values (24 [5.5%] vs 2 [1.3%], P = .037). This result was mainly driven by a significant trend towards a higher rate of TVR in patients with DM deferred based on FFR values compared to diabetic patients deferred based on iFR values (10 [6.4%] vs 0 [0%]), a result that did not achieve statistical significance (P = .065). This trend towards a lower rate of TVR in iFR-deferred vessels was not seen in non-DM patients (14 [5.1%] vs 2 [2.0%], P = .244) (figure 3).
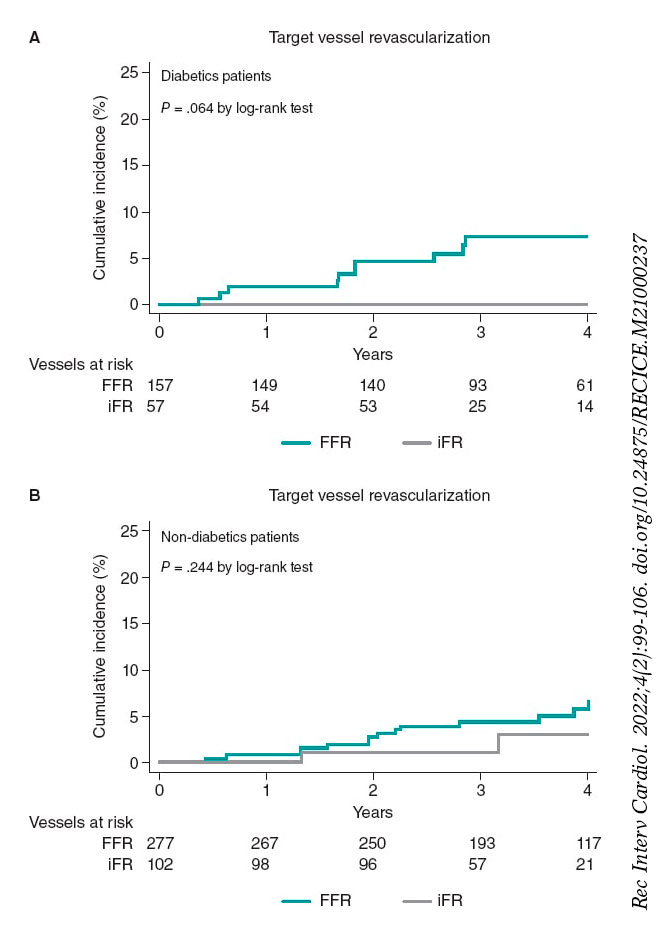
Figure 3. Target vessel revascularization based on the technique used to defer revascularization at the 4-years follow-up. iFR, instantaneous wavefree ratio; FFR, fractional flow reserve.
DISCUSSION
The main findings of this study are: a) patients with DM had high rates of MACE. However, deferring the revascularization of intermediate stenoses in patients with DM based on the physiological assessment results with pressure guidewires is safe regarding the risk of TVR or target vessel myocardial infarction with a similar rate of events at the long-term follow-up compared to that seen in non-diabetic patients; b) both the FFR and the iFR can be used safely to defer intermediate stenosis in diabetic patients. c) there was a trend towards a higher rate of TVR in diabetic patients deffered based on FFR values.
Clinical outcomes based on the presence of diabetes mellitus
The use of coronary physiology to guide revascularization improves patient outcomes compared to angiographic assessment.3,6,7,13 Currently both the FFR and the iFR have a class IA recommendation in the clinical practice guidelines regarding revascularization for the functional assessment of coronary stenoses.1
Diabetic patients are a high-risk population with a more aggressive and accelerated atherosclerosis compared to non-diabetic patients. In the PARADIGM (Progression of atherosclerotic plaque determined by computed tomographic angiography imaging) study, the presence of DM was an independent risk factor for plaque progression.14 In a pooled analysis of 5 intravascular ultrasound trials, Nicholls SJ et al. found that patients with DM had a greater percent atheroma volume and a more rapid progression.15
Around 25% of the patients enrolled in pivotal studies that proved the effectiveness of the FFR and the iFR had DM.3,4,6,16,17 The safety of physiology-guided revascularization deferral in the DM setting has not been specifically assessed in randomized clinical trials. On the other hand, the results of the few non-randomized studies that have evaluated physiology-guided management in diabetics show conflicting results.18,19
Domínguez-Franco et al. analyzed the prognostic safety of the FFR in diabetics. Although, their results are consistent with ours in the sense that no differences were found in the TVR at the long-term follow-up after revascularization deferral in DM vs non-DM patients, the applicability and strength of that study is limited by its small sample size (136 patients, 144 lesions). Also, the use of a FFR cut-off value for the decision-making process was 0.75 while in contemporary practice cut-off values of 0.80 are often used.18
Recently, Kennedy et al. analyzed 250 patients (128 DM, and 122 non-DM patients) and found that DM was associated with a higher rate of failed deferred stenoses (18.1% vs 7.5%, P ≤ .01, Cox regression-adjusted (HR, 3.65; 95%CI, 1.40-9.53, P < .01), and target lesion revascularization of the deferred lesion (17.2% vs 7.5%; HR, 3.52; 95%CI, 1.34-9.30; P = .01). Nevertheless, and consistent with our results, no significant differences in the rate of target vessel myocardial infarction were seen (6.1% vs 2.0%; HR, 3.34; 95%CI, 0.64-17.30; P = 0.15).19 The TLR reported in the former study is much higher than the one seen in our population and the one reported by former studies (eg, in the FAME study the 2-year rate of TLR was 3.2% in FFR-negative lesions).2 These differences can be associated with the characteristics of concomitant medical therapy, which was not specified and may affect the evolution of patients with DM critically. In our study population most patients received optimal medical therapy with over 93% receiving statins while the former study did not specify the medical treatment used. Another important factor can be the percentage of insulin-treated patients with DM (42% in the former study vs 24% in our population). In a different study the same authors found that insulin therapy was a predictive factor of deferred lesion failure in patients with FFR values > 0.80.20 Differences in the risk profile of the populations may, therefore, explain the different results obtained. Our study, with a larger sample size, proves that compared to non-diabetics deferring the revascularization of intermediate stenoses in diabetic patients is safe, and with no differences in TVR at the follow-up. Another study with similar results was the one conducted by Van Belle et al. who saw that the FFR is an important tool to redefine the severity of stenosis in patients with DM with good results at 1 year in deferred patients (HR, 0.77; 95%CI, 0.47-1.25; P = .29; reclassified vs non-reclassified patients with DM).21
Clinical outcomes based on the physiological index used to defer revascularization
Our results suggest that both the FFR and the iFR can be used safely to defer intermediate stenoses in patients with DM. Our findings regarding the low rates of MACE at the follow-up are consistent with the sub-analysis of patients with DM from the DEFINE-FLAIR trial compared to the 1-year follow-up.22 Interestingly enough, we found a trend towards a higher rate of TVR in diabetics deffered with the FFR compared to the iFR. This can be associated with the presence of microvascular dysfunction in diabetic patients, and with the better correlation of iFR with indices that assess microcirculation like coronary flow reserve (CFR). One study evaluated the performance of the iFR and the FFR against invasive CFR in 216 stenoses to find a significantly stronger correlation and a higher diagnostic performance for the iFR (iFR area under the ROC curve, 0.82 vs FFR area under the ROC curve, 0.72; P < .001, for a coronary flow velocity reserve of 2).23 Cook et al. evaluated 567 vessels with sensor-tipped pressure and Doppler ultrasound guidewires and found that with discordant FFR–/iFR+ , the hyperemic flow velocity and the CFR were similar to the FFR+/iFR+ group (P > .05). However, with discordant FFR+/iFR–, the hyperemic flow velocity and the CFR were similar to both the FFR–/iFR– and the coronary unobstructed groups (P > .05).24 These findings may potentially explain the lower performance of FFR in the presence of microvascular dysfunction, and the tendency we found towards a higher TVR in diabetic patients deferred with FFR. Interestingly enough, this tendency was not found in non-DM patients, which supports the hypothesis of microvascular compromise as one of the potential causes for the differences observed between the 2 indices.
Limitations
This study has several limitations. First, this is a single-center observational, retrospective, non-randomized study. The results should be analyzed with caution and can only be interpreted as hypothesis-generating given the small sample size that limits the study statistical power. There were more patients evaluated with the FFR compared to the iFR, which may have influenced the results. Neither clinicians nor patients were blinded to the physiological results, which may have influenced future decisions on revascularization. Most patients had a single deferred vessel, meaning that extrapolation of this data to patients with multivessel disease is complex. Finally, microvascular dysfunction was not evaluated in this population, and the actual impact on the results cannot be determined.
CONCLUSIONS
Deferring the revascularization of intermediate stenoses in patients with DM based on the FFR or the iFR is safe regarding the risk of TVR or target vessel myocardial infarction, with a similar rate of these events at the long-term follow-up compared to the rate seen in non-diabetic patients.
FUNDING
None whatsoever.
AUTHORS’ CONTRIBUTIONS
A.F. Castro-Mejía, and A. Travieso-González contributed to the study idea, design, acquisition, analysis, and interpretation of data, and writing of the article, M.J. Pérez-Vizcayno contributed to both the analysis and interpretation of data, H. Mejía-Rentería, I.J. Núñez-Gil, P. Salinas, L. Nombela-Franco, P. Jiménez-Quevedo, A. Fernández-Ortiz, and C. Macaya contributed to the writing of the article, and made a critical review of its intellectual content. J. Escaned, and N. Gonzalo contributed to the writing of the article, made a critical review of its intellectual content, and gave their final approval to the version that would eventually be published.
CONFLICTS OF INTEREST
I.J Núñez-Gil is a consultant for Aztraseneca. P. Salinas received speaker fees from Boston Scientific, Terumo, Alvinedica, and Biomenco. L. Nombela-Franco has served as a proctor for Abbott, and received speaker fees from Edwards Lifesciences Inc. A. Fernández-Ortiz is a speaker at the educational events of Medtronic, Biotronik, Biosensor, and Bayer. J. Escaned is a speaker and consultant for Abbott, Boston Scientific, and Philips, and received personal fees from Philips Volcano, Boston Scientific, and Abbott/St. Jude Medical outside the submitted work. N. Gonzalo is a speaker at educational events for Abbott, and Boston Scientific. The remaining authors declared no conflicts of interest.
WHAT IS KNOWN ABOUT THE TOPIC?
- The FFR and the iFR have proven to be safe tools to guide revascularization treatment in several clinical scenarios at the long-term follow-up. However, the safety of physiology-based revascularization in diabetics, who have a high-risk of cardiovascular events, has been scarcely investigated.
WHAT DOES THIS STUDY ADD?
- Deferring the revascularization of intermediate stenosis in diabetic patients based on the results of physiological evaluation with pressure guidewires is safe, and has a low rate of secondary events being the deferred vessel similar to those seen in non-diabetic patients at the longterm follow-up.
REFERENCES
1. Neumann F-J, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2018;40:87-165.
2. Pijls NH, Fearon WF, Tonino PA, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention in patients with multivessel coronary artery disease:2-year follow-up of the FAME (Fractional Flow Reserve Versus Angiography for Multivessel Evaluation) study. J Am Coll Cardiol. 2010;56:177-184.
3. Davies JE, Sen S, Dehbi HM, et al. Use of the Instantaneous Wave-free Ratio or Fractional Flow Reserve in PCI. New Engl J Med. 2017;376:1824-1834.
4. Escaned J, Ryan N, Mejia-Renteria H, et al. Safety of the Deferral of Coronary Revascularization on the Basis of Instantaneous Wave-Free Ratio and Fractional Flow Reserve Measurements in Stable Coronary Artery Disease and Acute Coronary Syndromes. JACC Cardiovasc Interv. 2018;11:1437-1449.
5. Zimmermann FM, Ferrara A, Johnson NP, et al. Deferral vs performance of percutaneous coronary intervention of functionally non-significant coronary stenosis:15-year follow-up of the DEFER trial. Eur Heart J. 2015;36:3182-3188.
6. Gotberg M, Christiansen EH, Gudmundsdottir IJ, et al. Instantaneous Wave-free Ratio versus Fractional Flow Reserve to Guide PCI. New Engl J Med. 2017;376:1813-1823.
7. Escaned J, Collet C, Ryan N, et al. Clinical outcomes of state-of-the-art percutaneous coronary revascularization in patients with de novo three vessel disease:1-year results of the SYNTAX II study. Eur Heart J. 2017;38:3124-3134.
8. van Nunen LX, Zimmermann FM, Tonino PA, et al. Fractional flow reserve versus angiography for guidance of PCI in patients with multivessel coronary artery disease (FAME):5-year follow-up of a randomised controlled trial. Lancet. 2015;386:853-1860.
9. Norhammar A, Malmberg K, Diderholm E, et al. Diabetes mellitus:the major risk factor in unstable coronary artery disease even after consideration of the extent of coronary artery disease and benefits of revascularization. J Am Coll Cardiol. 2004;43:585-591.
10. Castro Mejia A, Ortega Armas M, Lopez Ferreo L. Factores de riesgo en pacientes con cardiopatía isquémica angiográficamente severa:diferencias según sexo. Rev Cuba Cardiol Cir Cardiovasc. 2015;21:7p.
11. Esper RB, Farkouh ME, Ribeiro EE, et al. SYNTAX Score in Patients With Diabetes Undergoing Coronary Revascularization in the FREEDOM Trial. J Am Coll Cardiol. 2018;72:2826-2837.
12. Jeremias A, Kirtane AJ, Stone GW. A Test in Context. Fractional Flow Reserve:Accuracy, Prognostic Implications, and Limitations. J Am Coll Cardiol. 2017;69:2748-2758.
13. Tonino PA, De Bruyne B, Pijls NH, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. New Engl J Med. 2009;360:213-224.
14. Kim U, Leipsic JA, Sellers SL, et al. Natural History of Diabetic Coronary Atherosclerosis by Quantitative Measurement of Serial Coronary Computed Tomographic Angiography. Results of the PARADIGM Study (Progression of Atherosclerotic Plaque Determined by Computed Tomographic Angiography Imaging). J Am Coll Cardiol Img. 2018:11:1461-1471.
15. Nicholls SJ, Tuzcu EM, Kalidindi S, et al. Effect of Diabetes on Progression of Coronary Atherosclerosis and Arterial Remodeling:A Pooled Analysis of 5 Intravascular Ultrasound Trials. J Am Coll Cardiol.2008;52:255-262.
16. Xaplanteris P, Fournier S, Pijls NHJ, et al. Five-Year Outcomes with PCI Guided by Fractional Flow Reserve. New Engl J Med. 2018;379:250-259.
17. De Bruyne B, Fearon WF, Pijls NH, et al. Fractional flow reserve-guided PCI for stable coronary artery disease. New Engl J Med. 2014;371:1208-1217.
18. Domínguez-Franco AJ, Jiménez-Navarro MF, Muñoz-García AJ, et al. Pronóstico a largo plazo de diferir la intervención coronaria en diabéticos sobre la base de la reserva fraccional de flujo. Rev Esp Cardiol. 2008;61:352-359.
19. Kennedy MW, Kaplan E, Hermanides RS, et al. Clinical outcomes of deferred revascularisation using fractional flow reserve in patients with and without diabetes mellitus. Cardiovasc Diabetol. 2016;15:100.
20. Kennedy MW, Fabris E, Hermanides RS, et al. Factors associated with deferred lesion failure following fractional flow reserve assessment in patients with diabetes mellitus. Catheter Cardiovasc Interv.2017;90:1077-1083.
21. Van Belle E, Cosenza A, Baptista SB, et al. Usefulness of Routine Fractional Flow Reserve for Clinical Management of Coronary Artery Disease in Patients With Diabetes. JAMA Cardiol. 2020;5:272-281.
22. Lee JM, Choi KH, Koo BK, et al. Comparison of Major Adverse Cardiac Events Between Instantaneous Wave-Free Ratio and Fractional Flow Reserve-Guided Strategy in Patients With or Without Type 2 Diabetes:A Secondary Analysis of a Randomized Clinical Trial. JAMA Cardiol. 2019;4:857-864.
23. Petraco R, van de Hoef TP, Nijjer S, et al. Baseline instantaneous wave-free ratio as a pressure-only estimation of underlying coronary flow reserve:results of the JUSTIFY-CFR Study (Joined Coronary Pressure and Flow Analysis to Determine Diagnostic Characteristics of Basal and Hyperemic Indices of Functional Lesion Severity-Coronary Flow Reserve). Circ Cardiovasc Interv. 2014;7:492-502.
24. Cook CM, Jeremias A, Petraco R, et al. Fractional Flow Reserve/Instantaneous Wave-Free Ratio Discordance in Angiographically Intermediate Coronary Stenoses:An Analysis Using Doppler-Derived Coronary Flow Measurements. JACC Cardiovasc Interv. 2017;10:2514-2524.
- Deflation speed of the stent delivery system and primary angioplasty results: a randomized study
- Rationale and design of the Concordance study between FFR and iFR for the assessment of lesions in the left main coronary artery. The ILITRO-EPIC-07 Trial
- Comparison of quantitative calcium parameters between optical coherence tomography and invasive coronary angiography
- 5-year results of cutting or scoring balloon before drug-eluting balloon to treat in-stent restenosis







Interviews

An interview with Bruno Scheller
aServicio de Cardiología, Hospital Universitario de La Princesa, Instituto de Investigación Sanitaria de La Princesa (IIS-IP), Universidad Autónoma de Madrid, Spain
bCentro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain




