
Article
Ischemic heart disease and acute cardiac care
REC Interv Cardiol. 2019;1:21-25
Access to side branches with a sharply angulated origin: usefulness of a specific wire for chronic occlusions
Acceso a ramas laterales con origen muy angulado: utilidad de una guía específica de oclusión crónica
Servicio de Cardiología, Hospital de Cabueñes, Gijón, Asturias, España
ABSTRACT
Introduction and objectives: Reperfusion therapy during an ST-segment elevation acute coronary syndrome (STEACS) can be performed using fibrinolytic agents or primary percutaneous coronary intervention (pPCI). The pPCI is the reperfusion strategy of choice, but many patients with STEACS initially come to non-PCI capable hospitals. Regional networks have been launched with both reperfusion therapies using thrombolysis in indicated cases followed by routine angiographic studies (pharmacoinvasive strategy). Our objective was to analyze the results of treatment in patients with STEACS in the Region of Murcia, Spain based on the patient’s place of origin.
Methods: Retrospective study of a cohort of patients admitted due to STEACS to 3 health areas: pPCI-capable Area 1 (Hospital Clínico Universitario Virgen de la Arrixaca), and non-pPCI capable Areas IV and V (Hospital Comarcal del Noroeste, Caravaca de la Cruz, and Virgen del Castillo, Yecla).
Results: Six hundred and seventy-nine patients from health areas I, IV, and V of the Region of Murcia were treated of STEACS from 2006 through 2010. Out of the 494 patients from Area I, 97.6% (482 patients) were treated with pPCI while 2.4% (12 cases) received thrombolysis. In Areas IV and V, 73% (135) of patients were treated with pPCI and 27% (50) with thrombolysis. After thrombolysis, 46 patients (34%) required rescue angioplasty and 79 (58.5%) underwent a scheduled coronary angiography (pharmacoinvasive strategy). No statistically significant differences were reported in the overall mortality rate at 30-day (8.3% in Area I vs 6% in Areas IV and V; P = .31) or 1 year follow-up (11.3% vs 8.2%; P = .23) in Area I compared to Areas IV and V, nor for cardiac mortality.
Conclusions: Although immediate pPCIs are less accessible in remote health areas, the healthcare network from the Region of Murcia can achieve similar mortality results compared to populations with pPCI availability.
Keywords: ST-segment elevation acute coronary syndrome. Reperfusion therapy. Fibrinolysis. Primary percutaneous coronary intervention.
RESUMEN
Introducción y objetivos: El tratamiento de reperfusión en un síndrome coronario agudo con elevación del segmento ST (SCACEST) se puede realizar con agentes fibrinolíticos o con angioplastia primaria (ICPp). La ICPp es la estrategia de elección, pero muchos de los pacientes con SCACEST acuden inicialmente a hospitales sin ICPp. Se han desarrollado programas de asistencia al SCACEST en los que se integran ambos tratamientos, utilizando la trombolisis en casos indicados, seguida de un estudio angiográfico (estrategia farmacoinvasiva). El objetivo del estudio es analizar los resultados del tratamiento del SCACEST según sea diagnosticado en áreas de salud con o sin disponibilidad de ICPp inmediata.
Métodos: Estudio retrospectivo de una cohorte de pacientes diagnosticados de SCACEST en 3 áreas de salud de Murcia: área I con ICPp (Hospital Clínico Universitario Virgen de la Arrixaca) y áreas IV y V sin ICPp (Hospital Comarcal del Noroeste, Caravaca de la Cruz y Virgen del Castillo, Yecla).
Resultados: Entre 2006 y 2010 se atendió por SCACEST a 679 pacientes de las áreas I, IV y V de Murcia. De los 494 pacientes del área I, recibieron tratamiento con ICPp el 97,6% (482) y trombolisis el 2,4% (12). En los pacientes de las áreas sanitarias IV y V se realizó trombolisis al 73% (135) e ICPp al resto 27% (50). De los pacientes sometidos a trombolisis, el 34% (46) precisaron angioplastia de rescate y al 58,5% (79) se les realizó coronariografía programada (estrategia farmacoinvasiva). No hubo diferencias en la mortalidad total a 30 días (8,3% en el área I y 6% en las áreas IV y V; p = 0,31) ni al año (11,3 frente a 8,2%; p = 0,23); tampoco en la mortalidad por causa cardiaca.
Conclusiones: A pesar de la menor accesibilidad a la ICPp en las áreas sanitarias más alejadas, la red asistencial regional de Murcia permite unos resultados comparables a los de las áreas sanitarias con disponibilidad de ICPp.
Palabras clave: Síndrome coronario agudo con elevación del segmento ST. Reperfusión. Fibrinolisis. Angioplastia primaria.
Abbreviations: pPCI: primary percutaneous coronary intervention. STEACS: ST-segment elevation acute coronary syndrome.
INTRODUCTION
The management of ST-segment elevation acute coronary syndrome (STEACS) is based on the quick opening of the culprit artery through the use of fibrinolytic drugs or a percutaneous coronary intervention (PCI) that limits the size of the infarction and improves prognosis.1 Fibrinolytic drugs have proven capable of increasing survival,2 but they are more effective when administered within the first 3 hours after symptom onset. The primary percutaneous coronary intervention (pPCI) improves survival and reduces recurrent infarctions and strokes, which is why it is seen as the optimal therapy as long as it can be performed in a timely manner.3,4
The pPCI main limitation is the impossibility to use it in the entire population due to its limited geographic availability and the delays involved in the transfer of patients from non-pPCI centers to reference hospitals. Clinical practice guidelines recommend performing pPCI < 120 min. after the diagnosis of STEACS.1 Regional networks have been created to speed up these times and increase access to pPCI for patients with STEACS in non-pPCI hospitals. Yet despite this effort, many patients with STEACS are transferred late to pPCI centers which increases mortality and morbidity rates.
In order to improve results and administer reperfusion therapy as early as possible the so-called pharmacoinvasive strategy was implemented. It consists of the administration of fibrinolytic drugs in the pre-hospital or non-pPCI setting followed by the immediate transfer of the patient to a pPCI center capable of performing a bailout angioplasty if drug therapy fails or an early systematic angiography if it is successful.5,6
The experience gained over the years performing pPCIs at the Hospital Clínico Universitario Virgen de la Arrixaca (HCUVA) has been used for the optimal management of patients with STEACS. The recommendations established by the clinical guidelines have been followed and adapted to the geographic characteristics of the region, structure, and healthcare resources available. A protocol for the management of reperfusion in the acute phase that distinguished 2 groups has been established: the first group with patients treated in pPCI centers; the second one, with patients from regional hospitals who live in remote areas far from reference hospitals where the treatment recommended is fibrinolysis in the absence of contraindications.
METHODS
Retrospective study of a cohort of 679 patients diagnosed with STEACS from 2006 through 2010 in 2 groups of healthcare regions: region I, with pPCI capabilities at the HCUVA (El Palmar, Murcia), and non-pPCI regions assigned to the HCUVA intensive care unit. This second group includes region IV with the Hospital Comarcal del Noroeste (Caravaca de la Cruz) and region V with the Hospital Virgen del Castillo (Yecla).
Patients diagnosed with STEACS based on traditional criteria1 and symptoms of less than 24-hour duration were included. Selection was done by reviewing the HCUVA catheterization laboratory database on all ICU admissions, hospital urgent care provided, and 061 ambulance emergency transfer reports during the study period. The most adequate reperfusion therapy was administered following recommendations and the regional protocol.
Follow-up was conducted by reviewing the patients’ medical records by phone or through physical consultations.
The variables analyzed were past medical history, time elapsed since symptom onset until reperfusion therapy, electrocardiogram, echocardiographic and angiographic characteristics of angioplasty, patient progression, and treatment after hospital discharge. Major hemorrhages were defined as lethal or symptomatic in a critical area or organ (intracranial, intraspinal, intraocular, retroperitoneal, intraarticular, pericardial or intramuscular) causing compartmental syndrome or bleeding with reduced hemoglobin levels > 20 g/L (1.24 mmol/L) or need for 2 concentrate transfusions.
The short and long-term cardiovascular events were recorded at the 30-day and 1-year follow-up, respectively including the rates of overall mortality and cardiac mortality, acute myo- cardial reinfarction (re-AMI), stroke, and need for a new revascularization.
The study primary endpoint was to compare mortality and major cardiovascular events in patients treated of STEACS from the Region of Murcia based on the healthcare region they received care at. The study secondary endpoints were the analysis and comparison of the clinical characteristics of these populations and the identification of angiographic or PCI differences.
Statistical analysis
The results of continuous variables were expressed as mean ± standard deviation, and those of categorical variables as frequency or percentage. Categorical variables were compared using the chi-square test with Yates correction when necessary. Quantitative variables were compared using the Student t test based on the variables normal distribution. Event-free survival rates (overall and cardiac mortality, stroke, re-AMI, and restenosis) were calculated using the Kaplan-Meier method and their results were represented through survival curves. The log rank test was used to compare the event-free survival rate. The level of statistical significance used for hypothesis testing was P < .05. The Mac OS version of the SPSS statistical software (version 20) was used.
The study was conducted in full compliance with the Declaration of Helsinki and the good clinical practice guidelines approved by HCUVA Research Ethics Committee.
RESULTS
From January 2006 through December 2010, 679 patients from regions I, IV, and V of the Region of Murcia Healthcare System were treated of STEACS of less than 24-hour duration and received reperfusion therapy (figure 1). Ninety-seven-point-six per cent of the 494 patients from region I (HCUVA) underwent pPCI (482) while 2.4% received thrombolysis (12). Seventy-three percent (135) and 27% (50) of patients from regions IV and V (127 and 58, respectively) underwent thrombolysis and pPCI, respectively. Thirty-four percent (46) of those who received thrombolysis required a bailout angioplasty and 58.5% (79) a scheduled coronary angiography (pharmacoinvasive strategy) during their hospital stay. Only 10 patients (7.4%) did not undergo a coronary angiography.
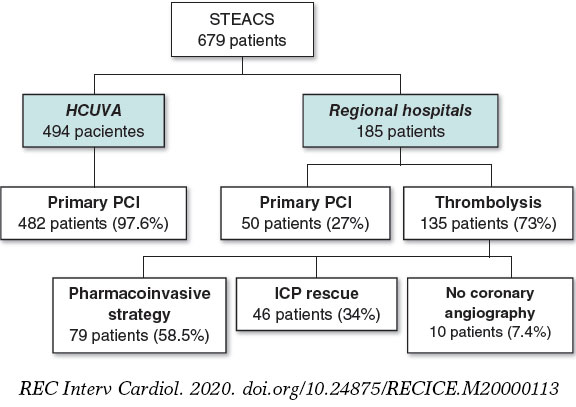
Figure 1. Summary of the study patients and the reperfusion strategies used based on the patients’ healthcare regions. HCUVA, Hospital Clínico Universitario Virgen de la Arrixaca; PCI, percutaneous coronary intervention or angioplasty; STEACS, ST-segment elevation acute coronary syndrome.
Baseline characteristics of the populations
Baseline characteristics are shown on table 1. The HCUVA population was older and had more diabetic patients compared to the population from regional hospitals. On the contrary, the rate of atrial fibrillation was higher in the latter. No significant differences were seen based on sex or the remaining risk factors.
Table 1. Baseline characteristics of the population
| HCUVA (n = 494) | Regional hospitals (n = 185) | P | |
|---|---|---|---|
| Age (years) | 65.3 ± 13.7 | 62.9 ± 13 | .044 |
| Sex (women) | 111 (22.5) | 41 (22.2) | .93 |
| High blood pressure | 290 (58.7) | 111 (60) | .76 |
| Diabetes | 180 (36.4) | 52 (28.1) | .042 |
| Dyslipidemia | 200 (40.5) | 64 (34.6) | .16 |
| Smoking | 304 (61.5) | 112 (60.5) | .81 |
| Previous ischemic heart disease | 53 (10.7) | 21 (11.4) | .810 |
| Previous revascularization | 53 (10.7) | 18 (9.7) | .88 |
| Peripheral arterial disease | 25 (5.1) | 4 (2.2) | .096 |
| Previous stroke | 43 (8.7) | 12 (6.5) | .35 |
| Atrial fibrillation | 21 (4.3) | 16 (8.6) | .025 |
| Heart failure | 12 (2.4) | 2 (1.1) | .271 |
| Kidney disease | 39 (7.9) | 19 (10.3) | .324 |
| COPD | 43 (8.7) | 18 (9.7) | .677 |
| Valve disease | 9 (1.8) | 1 (0.5) | .217 |
| Previous angina | 122 (24.7) | 39 (21.1) | .324 |
|
COPD, chronic obstructive pulmonary disease; HCUVA, Hospital Clínico Universitario Virgen de la Arrixaca. Data are expressed as no. (%) or mean ± standard deviation. |
|||
No differences were seen in the time to reperfusion between both groups with a mean of 180 min. (interquartile range: [120-240]) in HCUVA vs 150 min. in regional hospitals (interquartile range: [90-240]; P = .4). Ischemia times < 3 hours were achieved in 59.6% of the HCUVA patients compared to 68.9% of patients from regional hospitals (table 2). Forty-nine patients (9.9%) from the first group had cardiogenic shock vs 17 patients (9.2%) from the second one (not statistically significant differences).
Table 2. Progression time (from symptom onset to reperfusion) and angiographic and electrocardiographic characteristics
| HCUVA (n = 494) | Regional hospitals (n = 185) | P | |
|---|---|---|---|
| Progression time(median,min.) | 180 | 150 | .4 |
| < 3 h | 295 (59.7) | 128 (69.1) | |
| 3-6 h | 141 (28.5) | 33 (17.7) | |
| 6-9 h | 32 (6.4) | 10 (5.6) | |
| 9h -12 h | 15 (3.1) | 7 (4) | |
| > 12 h | 11 (2.2) | 7 (4) | |
| STEACS location | .298 | ||
| Anterior | 205 (41.6) | 89 (48.1) | |
| Inferior | 236 (47.7) | 75 (40.5) | |
| Lateral | 49 (9.9) | 18 (9.7) | |
| Indeterminate | 4 (0.8) | 3 (1.6) | |
| Culprit vessel | .022 | ||
| Left anterior descending coronary artery | 205 (41.5) | 83 (44.9) | .429 |
| Circumflex artery | 62 (12.6) | 25 (13.5) | .738 |
| Right coronary artery | 204 (41.3) | 64 (34.6) | .111 |
| Left main coronary artery/graft | 9 (1.8) | 0 | .065 |
| Unidentified | 14 (2.8) | 13 (7) | .013 |
| Previous stent thrombosis | 24 (4.8) | 3 (1.6) | .075 |
| Number of injured vessels | .001 | ||
| 0 | 5 (1) | 15 (8) | .001 |
| 1 | 274 (55.4) | 109 (58.9) | .416 |
| 2 | 133 (27) | 38 (20.6) | .093 |
| 3 | 82 (16.6) | 23 (12.6) | .227 |
| Initial TIMI flow | .001 | ||
| 0 | 351 (71.1) | 65 (34.9) | .001 |
| 1 | 21 (4.2) | 4 (2.4) | .281 |
| 2 | 13 (2.7) | 9 (4.7) | .206 |
| 3 | 109 (22) | 107 (58) | .001 |
| Final TIMI flow grade 3 | 464 (93.9) | 171 (92.3) | .845 |
| Second revascularization | 95 (19.2) | 30 (16.2) | .322 |
| Complete revascularization | 347 (70.2) | 138 (74.6) | |
|
HCUVA, Hospital Clínico Universitario Virgen de la Arrixaca; STEACS, ST-segment elevation acute coronary syndrome; TIMI, Thrombolysis in Myocardial Infarction. Data are expressed as no. (%) |
|||
Regarding the coronary angiography, the percentage of radial access was similar: 45% and 48%, respectively. No significant differences were found either in the location of the STEACS (table 2). However, significant differences were seen in the culprit artery since it was a common thing to not be able to identify the vessel in patients from regional hospitals because the coronary arteries were patent. Differences were seen too in the initial TIMI flow (Thrombolysis in Myocardial Infarction) between both groups (P = .001) at the expense of a worse initial flow in HCUVA patients. After reperfusion therapy, TIMI flow grade-3 was achieved in the culprit artery in 93.9% of HCUVA patients and 92.3% of patients from regional hospitals. Revascularization was complete in 70.2% of the patients from region I and 74.6% of the patients from regions IV and V.
Analytic and echocardiographic characteristics and clinical progression
No differences were seen in the highest levels of cardiac necrosis markers between the different regions (table 3). On average the left ventricular ejection fraction was 52.15% in HCUVA patients and 52.29% in patients from regional hospitals without any significant differences in the systolic or diastolic function (table 3).
Table 3. Analytic, echocardiographic and disease progression characteristics at the hospital floor
| HCUVA (n = 494) | Regional hospitals (n = 185) | P | |
|---|---|---|---|
| Peak creatine kinase levels (µg/dL) | 1864.4 ± 1917.3 | 1938.3 ± 1834.4 | .671 |
| Peak creatine kinase-MB levels | 175.39 ± 132.34 | 182.26 ± 159.86 | .668 |
| Peak troponin T levels | 5.79 ± 9.4 | 9.38 ± 27.5 | .118 |
| Ejection fraction (%) | 52.15 ± 10.93 | 52.29 ± 11.46 | .886 |
| Normal | 255 (50.6) | 95 (51.5) | |
| Mild dysfunction | 152 (30.7) | 52 (28.1) | |
| Moderate dysfunction | 63 (12.8) | 32 (17.3) | |
| Severe dysfunction | 29 (5.9) | 6 (3.5) | |
| Diastolic pattern | .056 | ||
| Restrictive pattern | 19 (3.9) | 10 (5.3) | |
| Pseudo-normal pattern | 125 (25.3) | 33 (18) | |
| Prolonged relaxation | 307 (62.2) | 113 (61.3) | |
| Normal | 37 (7.6) | 23 (12.4) | |
| Atrial fibrillation | 5 (1.1) | 6 (3.3) | |
| Hospital stay (days) | 9.04 ± 5.72 | 9.81 ± 7.94 | .259 |
| Major hemorrhage | 11 (2.2) | 7 (3.8) | .261 |
| STEACS related complications | 6 (1.2) | 3 (1.6) | .71 |
| Killip Class I | 357 (72.3) | 154 (83.3) | .012 |
|
HCUVA, Hospital Clínico Universitario Virgen de la Arrixaca; STEACS, ST-segment elevation acute coronary syndrome; Data are expressed as no. (%) or median ± standard deviation. |
|||
No differences were seen in the rates of major bleeding and complications (cardiac ruptures: 2 and 2; intraventricular communication: 1 in regional hospitals, 2 in the HCUVA; papillary muscle rupture: 1 and 1). Patients from region I had more heart failure during their hospital stay (28.7% in the HCUVA vs 16.7% in regional hospitals).
30-day and 1-year follow-up results
Mean follow-up was 962 days in HCUVA patients and 1062 days in patients from regional hospitals. No differences were seen in the overall mortality or cardiac mortality rates at the 30-day or 1-year follow-up. No differences were seen either in the rates of AMI, stroke, and revascularization at the follow-up (table 4). Kaplan-Meier survival curves (figure 2) did not show any significant differences regarding mortality, cardiac death, AMI, and stroke.
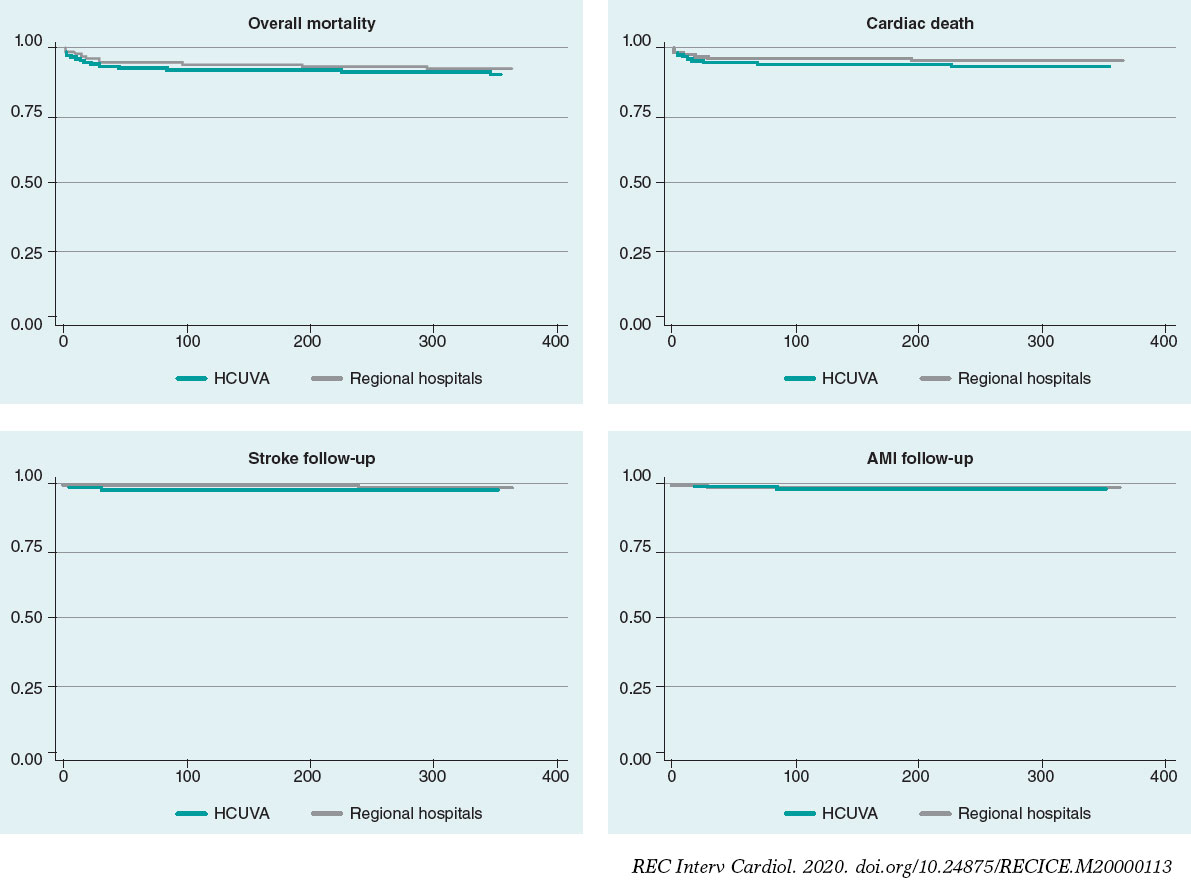
Figure 2. Survival curves. Mortality, cardiac death, stroke, and AMI at the follow-up. AMI, acute myocardial infarction; HCUVA, Hospital Clínico Universitario Virgen de la Arrixaca.
Table 4. Mortality and major cardiovascular events
| Results (%) | HCUVA (n = 494) | Regional hospitals (n = 185) | P |
|---|---|---|---|
| Mortality | |||
| 30 days | 41 (8.3) | 11 (6) | .312 |
| 1 year | 56 (11.3) | 15 (8,2) | .229 |
| Cardiac death | |||
| 30 days | 35 (7.1) | 8 (4.3) | .19 |
| 1 year | 43 (8.7) | 9 (4.9) | .095 |
| Reinfarction | |||
| 30 days | 7 (1.4) | 2 (1.1) | .735 |
| 1 year | 20 (4) | 5 (2.7) | .409 |
| Stroke | |||
| 30 days | 8 (1.6) | 3 (1.6) | .996 |
| 1 year | 15 (3) | 3 (1.6) | .309 |
| Revascularization | |||
| 30 days | 7 (1.4) | 4 (2.2) | .494 |
| 1 year | 35 (7.1) | 9 (4.9) | .294 |
|
HCUVA: Hospital Clínico Universitario Virgen de la Arrixaca. Data are expressed as no. (%). |
|||
DISCUSSION
This study assessed the results of the management of STEACS from a population perspective and analyzed the consequences of the different care provided in each patient’s healthcare region. This was an observational and retrospective study conducted in 3 population areas from the Region of Murcia that share the same interventional cardiology unit and the same intensive care unit. A 5-year period was analyzed with an mean annual rate of 140 patients with STEACS who were admitted to the ER with symptoms of < 24-hour duration. To make the analysis more consistent and thorough, the past medical histories of patients admitted to their respective hospitals and the out-of-hospital ER system and 061 emergency service reports were reviewed to detect prehospital deaths.
The regional plan for the management of STEACS7 is part of the recommendation of designing regional networks beyond the idea of isolated hospital healthcare towards more comprehensive community healthcare systems including scientific recommendations, geographical peculiarities, resources and infrastructures available, and the characteristics of healthcare organization. This plan suggests initiating reperfusion therapy as early as possible whether mechanical with pPCI o pharmacological with fibrinolysis.
The pPCI is considered the treatment of choice for patients admitted to the ER within 60 min. since symptom onset.1,8,9 This is how patients diagnosed with STEACS in the metropolitan area of Murcia and nearby municipalities are treated.7 For remote areas such as healthcare regions IV and V, fibrinolytic therapy is recommended in the absence of contraindications followed by transfer to the HCUVA ICU plus urgent coronary angiography in the absence of reperfusion signs (bailout PCI) or elective coronary angiography within the first 24 hours to 48 hours (pharmacoinvasive strategy).7 The hospitals from such areas are 75 km and 110 km away (figure 3) respectively from the pPCI reference hospital.
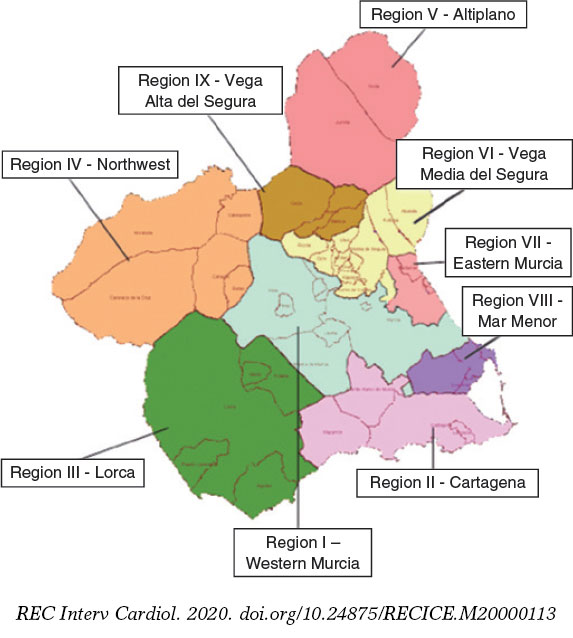
Figure 3. Healthcare regions within the Region of Murcia, Spain.
Populations from pPCI-capable regions (494 patients) and those from remote regions (185 patients) are rather similar: 78% males, many diabetic patients (> 28%), and over 60% smokers. The only differences between both groups are that patients from region I are older and have a higher prevalence of diabetes (36.4% vs 28.1%). The percentage of diabetics in this series is higher compared to that of international studies like the STREAM trial (12.1% to 13.1%) and other national studies like those conducted by Rodríguez-Leor et al.10 (24.8%), and Hernández-Pérez et al.11 (19.1%), and similar to the EUROASPIRE-IV registry (27%).12
The studies conducted until 2006 in patients with STEACS admitted to the ER in a timely manner showed that up to 25% to 30% did not receive reperfusion therapy.13,14 This has improved with the implementation of STEACS care networks. Proof of this are the results from several networks in Europe and the United States with percentages from 100% (the Mayo Clinic network)15 to 84% (the Alberta network, Canada).16 Our data are indicative of a high percentage of reperfusion therapy in the studied regions.
In region I the pPCI was performed in almost all of the cases (97.6%) while in the remaining 2 regions 27% of the 185 patients were referred to other centers for mechanical reperfusion. The existence of contraindications for thrombolysis, the long progression time or the possibility of agile hospital transfers to the interventional cardiology unit facilitated the performance of pPCI in 1 out of every 4 patients with STEACS from these regions; the rest (73%) received fibrinolysis. These data are indicative of a greater use of fibrinolytic therapy compared to the one reported by other studies. Thus, a Belgium registry17 reported that fibrinolytic therapy was prescribed to 28.7% of the population from regional hospitals over the first few years (2007-2008). However, this percentage dropped to 12.6% over the last few years (2009-2010). The higher percentage of thrombolytic therapy seen in our study is associated with a longer distance between regional hospitals and the reference pPCI hospital. Even so, over the last few years, a higher percentage of patients with STEACS referred to pPCI centers has been reported in our region. At the program early stages,18 in healthcare regions IV and V, the percentage of pPCIs performed was between 1% and 2% of all reperfusion therapies. In our study, this percentage grew to 27% after reducing patient transfer times between hospitals.
Coronary angiography was performed in 95% of the patients who received fibrinolytic therapy, a similar percentage compared to that reported by other registries (96% in the FAST-MI,19 and 97% in the Mayo Clinic Care Network registry15) and higher to the one reported by the Belgium registry (69%).17
Reperfusion mean times are also similar to those reported by the registries mentioned above. Time delay until reperfusion therapy was < 3 hours in 59.6% of the patients from region I and 68.9% of the patients from regions IV and V. These are similar rates to those from the Belgium trial17 in which the time elapsed since symptom onset until reperfusion therapy was < 4 hours in 67% of the patients from pPCI hospitals and 63% of the patients from regional hospitals and to those from the Mayo Clinic Care Network AMI protocol.15 This protocol establishes a pharmacoinvasive strategy where total ischemia times were 103 min. in patients who received thrombolysis and 278 min. in those referred to undergo pPCI (with a mean time until reperfusion in regional hospitals of 181 min.).
No differences were seen in the location of the infarction between both groups. Patients referred from regional hospitals had more coronary arteries without lesions and a higher preprocedural rate of TIMI flow grade-3 compared to a higher rate of occluded infarct related culprit arteries in those referred for pPCI. Upon arrival to the catheterization laboratory, the initial TIMI flow grade was 0-1 in 75.6% of the patients referred for pPCI and 37.3% in those who received thrombolysis. Different studies show that when the coronary angiography is performed there is a higher percentage of patients with TIMI flow grade-3 among patients who received thrombolysis.20
Clinical progression was similar with no differences regarding major bleeding complications (2.2% vs 3.8%), stroke (1.6% vs 1.6% at 30 days), re-AMI (1.4% vs 1.1% at 30 days), and need for revascularization (1.4% vs 2.2% at 30 days, 7.1% vs 4.9% at 1 year). However, the rate of heart failure during the hospital stay was higher in HCUVA patients (27.3% vs 16.7%). This result may be explained by a tendency towards a greater grade of advanced diastolic dysfunction in these patients (25.3% vs 18%). However, despite the longer ischemia time there were no significant differences in the AMI size due to systolic dysfunction or peak creatinine kinase-MB levels with peak values of 175 vs 182 µg/dL.
The mortality of patients looked after in regions assigned to non-pPCI regional hospitals is similar to that of patients looked after in the reference pPCI hospital. At 1-month, the overall mortality rate was 8.3% in region I with pPCI capabilities and 6% in the most remote areas assigned to regional hospitals; cardiovascular mortality rate was 7.1% and 4.3%, respectively. These rates are similar to those reported by other studies conducted in our setting like the 7.5% from the RESCATE II,21 7.26% from the RECALCAR trial,22 11% from the PRIAMHO-II trial,23 and 7.6% from the MASCARA trial.24 They are also similar to those from the Belgium infarction care network17 where the mortality rates of regional and pPCI hospitals were 7% and 6.7%, respectively or the Mayo Clinic AMI Care Network where the mortality rates of patients from regional hospitals and pPCI hospitals were 5.2% and 7.2%, respectively.15
Based on these findings a reflection is to be made on some of the things that worry healthcare providers, Administration, and patients such as accessibility and equity in the healthcare system. In the STEACS setting there is an ongoing debate on how to make pPCI available for the entire population. Data from this and other studies,19,25 show that even if pPCI is the preferred reperfusion strategy, it is not the only one. In patients looked after in remote areas far from hospitals with experienced heart teams a pharmacoinvasive strategy with fibrinolytic treatment in the absence of complications is a good alternative.
Limitations
The scarce population from regions IV and V brings down the annual number of patients with STEACS, which is why the timeframe studied had to be a large one in order to study a representative sample. This was a retrospective analysis with the limitations of this type of studies. Basically, this shows how difficult it was to obtain certain data like those regarding different timeframes. The findings from this study where patients were always transferred to the reference hospital intensive care unit may vary from those of other regions where delays could occur if fibrinolysis was not successful. Another possible limitation would be that only patients treated with reperfusion therapy were studied. As already discussed, patients who may have died during the transfer or at the ER were searched for to discard differences in the results obtained from patients assigned to a reperfusion strategy and those finally treated. However, patients with STEACS who did not receive reperfusion therapy were not studied (cases with long symptom duration, etc.). The study compared the results based on the patients’ healthcare region, which may be decisive when assessing the management of STEACS in different healthcare regions, and the different ways of administering various types of reperfusion therapy. This does not seem to be a problem at the moment since reperfusion therapy is administered to over 80% of the cases without significant regional differences.
CONCLUSIONS
Patients diagnosed with STEACS from the most remote healthcare regions of the Region of Murcia (regions IV and V) show similar clinical characteristics compared to patients from region I. However, they are younger patients with not so much diabetes. Yet despite the lower accessibility to immediate pPCI for populations from these healthcare regions, the regional network gives results that are similar to those of populations from pPCI-capable healthcare regions. Pharmacoinvasive strategy is a valid reperfusion therapy for populations from non-pPCI healthcare regions within the times recommended, with similar survival rates to those of pPCI regions, without a higher rate of complications, and with similar short and long-term results.
CONFLICTS OF INTEREST
The authors declared no conflicts of interest whatsoever.
WHAT IS KNOWN ABOUT THE TOPIC?
- Fibrinolysis and pPCI are reperfusion therapies for the management of STEACS. The latter is superior to the former if performed in a timely manner and under the right conditions.
- The pPCI main limitation is that it is impossible to offer it to the entire population due to time delays and availability issues.
- Regional networks have been created to reduce time to reperfusion and increase the availability of pPCI.
- Yet despite this effort, some patients with STEACS do not make it on time to the ER to be treated with pPCI. This delay is associated with higher mortality and morbidity rates.
WHAT DOES THIS STUDY ADD?
- Accessibility to pPCI for patients diagnosed with STEACS from remote areas is much lower.
- Being part of a healthcare regional network gives results that are similar to those of populations from pPCI-capable regions.
- This study shows that in an infarction care regional network system, reperfusion therapy can be performed by combining pharmacoinvasive strategy and pPCI.
- That is the way to achieve survival rates similar to those of patients who live close to pPCI-capable hospitals without a higher rate of complications.
REFERENCES
1. Steg PG, James SK, Atar D, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2012;33:2569-2619.
2. Fibrinolytic Therapy Trialists'(FTT) Collaborative Group. Indications for fibrinolytic therapy in suspected acute myocardial infarction:collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients. Lancet. 1994;343:311-322.
3. Andersen HR, Nielsen TT, Rasmussen K, et al. A comparison of coronary angioplasty with fibrinolytic therapy in acute myocardial infarction. N Engl J Med. 2003;349:733-742.
4. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction:a quantitative review of 23 randomised trials. Lancet. 2003;361:13-20.
5. Borgia F, Goodman SG, Halvorsen S, et al. Early routine percutaneous coronary intervention after fibrinolysis vs. standard therapy in ST-segment elevation myocardial infarction:a meta-analysis. Eur Heart J. 2010;31:2156-2169.
6. Armstrong PW, Gershlick AH, Goldstein P, et al. Fibrinolysis or primary PCI in ST-segment elevation myocardial infarction. N Engl J Med. 2013;368:1379-1387.
7. Servicio Murciano de Salud, Consejería de Sanidad y Consumo. Programa Integral de Atención a La Cardiopatía Isquémica 2010-2013. 2010. Disponible en:https://www.murciasalud.es/publicaciones.php?op=mostrar_publicacion&id=1771&idsec=88. Consultado 20 Dic 2020.
8. O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction:a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61:e78-140.
9. Windecker S, Kolh P, Alfonso F, et al. 2014 ESC/EACTS Guidelines on myocardial revascularization:The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2014;35:2541-2619.
10. Rodriguez-Leor O, Fernandez-Nofrerias E, Mauri F, et al. Analysis of reperfusion delay in patients with acute myocardial infarction treated with primary angioplasty based on first medical contact and time of presentation. Rev Esp Cardiol. 2011;64:476-483.
11. Hernandez-Perez FJ, Blasco-Lobo A, Goicolea L, et al. Use of the radial approach in primary angioplasty:results in 1029 consecutive patients and analyses in unfavorable subgroups. Rev Esp Cardiol. 2014;67:45-51.
12. Kotseva K, Wood D, De Bacquer D, et al. EUROASPIRE IV:a European Society of Cardiology survey on the lifestyle, risk factor and therapeutic management of coronary patients from 24 European countries. Eur J Prev Cardiol. 2016;23:636-648.
13. Eagle KA, Nallamothu BK, Mehta RH, et al. Trends in acute reperfusion therapy for ST-segment elevation myocardial infarction from 1999 to 2006we are getting better but we have got a long way to go. Eur Heart J. 2008;29:609-617.
14. Gibson CM, Pride YB, Frederick PD, et al. Trends in reperfusion strategies, door-to-needle and door-to-balloon times, and in-hospital mortality among patients with ST-segment elevation myocardial infarction enrolled in the National Registry of Myocardial Infarction from 1990 to 2006. Am Heart J. 2008;156:1035-1044.
15. Ting HH, Rihal CS, Gersh BJ, et al. Regional systems of care to optimize timeliness of reperfusion therapy for ST-elevation myocardial infarction:the Mayo Clinic STEMI Protocol. Circulation. 2007;116:729-736.
16. Shavadia J, Ibrahim Q, Sookram S, Brass N, Knapp D, Welsh RC. Bridging the gap for nonmetropolitan STEMI patients through implementation of a pharmacoinvasive reperfusion strategy. Can J Cardiol. 2013;29:951-959.
17. Claeys MJ, Sinnaeve PR, Convens C, et al. STEMI mortality in community hospitals versus PCI-capable hospitals:results from a nationwide STEMI network programme. Eur Heart J Acute Cardiovasc Care. 2012;1:40-47.
18. Valdés Chávarri M, Pinar Bermúdez E, Lacunza Ruiz J, et al. The primary percutaneous coronary intervention program in Murcia. Rev Esp Cardiol Supl. 2011;11(C):28-34.
19. Danchin N, Coste P, Ferrieres J, et al. Comparison of thrombolysis followed by broad use of percutaneous coronary intervention with primary percutaneous coronary intervention for ST-segment-elevation acute myocardial infarction:data from the french registry on acute ST-elevation myocardial inf. Circulation. 2008;118:268-276.
20. Giannopoulos G, Pappas L, Synetos A, et al. Association of virtual histology characteristics of the culprit plaque with post-fibrinolysis flow restoration in ST-elevation myocardial infarction. Int J Cardiol. 2014;174:678-682.
21. Garcia-Garcia C, Sanz G, Valle V, et al. Trends in in-hospital mortality and six-month outcomes in patients with a first acute myocardial infarction. Change over the last decade. Rev Esp Cardiol. 2010;63:1136-1144.
22. Bertomeu V, Cequier A, Bernal JL, et al. In-hospital mortality due to acute myocardial infarction. Relevance of type of hospital and care provided. RECALCAR study. Rev Esp Cardiol. 2013;66:935-942.
23. Aros F, Loma-Osorio A, Vila J, et al. Effect of combined beta-blocker and angiotensin-converting enzyme inhibitor treatment on 1-year survival after acute myocardial infarction:findings of the PRIAMHO-II registry. Rev Esp Cardiol. 2006;59:313-320.
24. Ferreira-Gonzalez I, Permanyer-Miralda G, Marrugat J, et al. MASCARA (Manejo del Sindrome Coronario Agudo. Registro Actualizado) study. General findings. Rev Esp Cardiol. 2008;61:803-816.
25. Larson DM, Duval S, Sharkey SW, et al. Safety and efficacy of a pharmaco-invasive reperfusion strategy in rural ST-elevation myocardial infarction patients with expected delays due to long-distance transfers. Eur Heart J. 2012;33:1232-1240.
Abstract
Introduction and objectives: Recent publications suggest that bioresorbable vascular scaffolds (BVS) are associated with an excess of thrombotic complications. We present the real-world, long-term results of a series of patients who received the Absorb BVS (Abbott Vascular, United States).
Methods: A total of 213 consecutive patients who received at least 1 BVS between May 2012 and December 2016 were analyzed. The main objective of the study was the rate of target vessel failure, a composite endpoint of infarction or target vessel revascularization and cardiac death.
Results: Seventy-five per cent of the patients were men (mean age, 61.4 years). The most common cause for admission was non-ST-elevation myocardial infarction (53.52%). The median follow-up was 44 months [28 months], the rate of the primary endpoint was 6.57% for the first 24 months and 7.98% at the end of the follow-up. Regarding the device, there were 6 cases (2.81%) of thrombosis (definitive, probable or possible) and 10 cases (4.69%) of restenosis. Patients with a past medical history of diabetes mellitus (HR, 1.72; 95%CI, 1.01-2.95; P = .05) and/or chronic oral anticoagulation (HR, 5.71; 95%CI, 1.12-28.94; P = .04) had a higher risk of target vessel failure.
Conclusions: In this series of patients, the rate of target vessel failure was similar to the one previously described by randomized clinical trials. Events were more common during the first 2 years of follow-up and in the presence of greater cardiovascular comorbidity.
Keywords: Absorb. Bioresorbable scaffolds. Coronary angioplasty.
RESUMEN
Introducción y objetivos: Las publicaciones sugieren que los armazones vasculares bioabsorbibles (AVB) conllevan un exceso de complicaciones trombóticas. Se describen los resultados en la vida real y a largo plazo de una serie de pacientes a los que se implantó un AVB Absorb (Abbott Vascular, EE.UU.).
Métodos: Se analizaron 213 pacientes consecutivos que recibieron al menos un AVB entre mayo de 2012 y diciembre de 2016. El objetivo principal del estudio fue la incidencia de fracaso del vaso diana, un evento compuesto que incluye infarto de miocardio, revascularización del vaso diana y muerte cardiaca.
Resultados: El 75% de los pacientes eran varones (edad media, 61,4 años). La causa más común de ingreso fue el infarto sin elevación del ST (53,52%). La mediana de seguimiento fue de 44 meses [28 meses]. La incidencia del evento primario fue del 6,57% durante los primeros 24 meses y del 7,98% al final del seguimiento. Respecto al dispositivo, hubo 6 casos (2,81%) de trombosis (definitiva, probable o posible) y 10 casos (4,69%) de reestenosis. Los pacientes con antecedentes de diabetes mellitus (HR = 1,72; IC95%, 1,01-2,95; p = 0,05) o con anticoagulación oral crónica (HR = 5,71; IC95%, 1,12-28,94; p = 0,04) tuvieron mayor riesgo de fracaso del vaso diana.
Conclusiones: En esta serie de pacientes, la incidencia de fracaso del vaso diana fue comparable a la descrita previamente en ensayos clínicos aleatorizados. Los eventos adversos fueron más frecuentes en los primeros 2 años de seguimiento y en presencia de mayor comorbilidad cardiovascular.
Palabras clave: Absorb. Armazón vascular bioabsorbible. Angioplastia coronaria.
Abbreviations BVS: bioresorbable vascular scaffold. AMI: acute myocardial infarction. DES: drug-eluting stent.
INTRODUCTION
Drug-eluting bioresorbable vascular scaffolds (BVS) were initially presented as a technological breakthrough to overcome the limitations and adverse events associated with permanent bare-metal stents, especially the development of neoatherosclerosis that is associated with a risk of thrombosis (0.2% per year) and secondary revascularization (2% to 3% per year).1-3
At the time, the implantation of a BVS was an innovative approach to treat coronary atherosclerosis by releasing the artery from a permanent metal jail and restoring the flow architecture. Also, it preserved parietal motility and its response to stimuli generated by coronary flow (shear stress). The Absorb (Abbott Vascular, United States)—a polymer everolimus-eluting scaffold with 157 µm-thick struts—was one of the first ones to be available in Spain and several clinical trials were conducted.4-8 The excellent initial results led to the widespread use of this device for several clinical indications.9-10 The Absorb BVS was approved by the U.S. Food and Drug Administration and obtained the CE marking certification in January 2011.11
However, the mid- and long-term data of the AIDA research group12,13 on the Absorb were disappointing. They showed a higher rate of late scaffold thrombosis compared to the XIENCE (Abbott Vascular, United States) (3.5% vs 0.9%; hazard ratio [HR], 3.87; 95% confidence interval [95%CI], 1.78-8.42; P < .001), an everolimus-eluting stent (EES).14,15 Therefore, the manufacturer stopped making the Absorb BVS and removed it from the market according to the European regulatory agency; however, some of these devices remain approved and are still available in Europe.16
Since the Absorb BVS was widely used in different clinical settings during market launch more than 7 years ago, the long-term follow-up results are available today. The objective of this study is to describe the incidence of long-term adverse events in a series of patients implanted with the Absorb BVS in different clinical settings of our multicenter registry.17
METHODS
Population, design, and definitions
The cases treated with percutaneous transluminal coronary angioplasty with at least 1 Absorb BVS in 3 hospitals between May 2012 and December 2016 were studied.17 Implantation was performed to the discretion of the operator in charge.
The study primary composite endpoint was the target vessel failure rate, a composite event of target vessel revascularization, target vessel related acute myocardial infarction (AMI), and cardiac death. The study secondary endpoint was the rate of the overall clinical endpoint including these adverse events: all-cause mortality, myocardial infarction, and all the new coronary revascularizations (including those of the non-target vessel).
The registry of the interventional cardiology unit of our hospital network was periodically reviewed every 6 to 12 months at the follow-up consultation at the interventional cardiology unit by a cardiologist. Also, it was completed through follow-up phone calls.
Statistical analysis
Data regarding quantitative variables are expressed as mean ± standard deviation and qualitative variables are expressed as percentages. Patients were grouped according to whether they had target vessel failure or not; inter-group averages were compared using the Student t test. Percentages were compared using the chi-square test. Kaplan-Meier analysis was conducted to estimate the likelihood of target vessel failure-free survival and BVS thrombosis and restenosis. Finally, the multivariate Cox regression analysis was conducted to study the survival function adjusted by different predefined variables: sex, age, cardiovascular risk factors, past medical history, clinical signs, size and length of the BVS implanted, overlapping of, at least, 2 BVSs, and use of intracoronary imaging modalities (optical coherence tomography [OCT] or intravascular ultrasound [IVUS]). Two-tailed P ≤ values .05 were considered statistically significant in all tests. Data were analyzed using the statistical software package Stata IC 14 (StataCorp, United States).
RESULTS
Study population
Two hundred and thirteen consecutive patients implanted with, at least, 1 Absorb BVS between May 2012 and December 2016 were included. Table 1 shows the baseline clinical characteristics of these patients. Most of the participants were males (75.12%) with a mean age of 61.40 ± 12.74 years, and a high prevalence of dyslipidemia (62.44%) and smoking (65.26%). Diabetes mellitus was present in 23.94% and 21.60% had been previously treated with a percutaneous coronary intervention. The most common clinical presentation during recruitment was non-ST-segment elevation acute coronary syndrome (53.52%).
Table 1. Baseline clinical characteristics of patients and differences based on the primary endpoint
| Characteristics | Patients who received BVS (n = 213) | Patients with BVS and target vessel failure (n = 17) | Patients with BVS without target vessel failure (n = 196) | P |
|---|---|---|---|---|
| Age (years) | 61.40 ± 12.74 | 66.71 ± 9.62 | 61.14 ± 12.98 | .07 |
| Sex (male) | 160 (75.12) | 12 (70.59) | 148 (75.51) | .65 |
| Risk factors | ||||
| Diabetes mellitus | 51 (23.94) | 7 (41.18) | 44 (22.45) | .06 |
| Hypertension | 118 (55.40) | 11 (64.71) | 107 (54.59) | .42 |
| Dyslipidemia | 133 (62.44) | 13 (76.47) | 120 (61.22) | .21 |
| Active smoking | 139 (65.26) | 10 (58.82) | 129 (65.82) | .56 |
| Past medical history | ||||
| Chronic kidney disease | 8 (3.76) | 1 (5.88) | 7 (3.57) | .63 |
| LVEF < 30% | 5 (4.5) | 1 (5.88) | 4 (2.04) | .55 |
| Previous stroke or TIA | 9 (4.2) | 3 (17.65) | 6 (3.06) | .01 |
| Chronic oral anticoagulation | 10 (4.69) | 3 (17.65) | 7 (3.57) | .01 |
| Peripheral vascular disease | 13 (6.10) | 1 (5.88) | 12 (6.12) | .96 |
| Previous myocardial infarction | 31 (14.55) | 1 (5.88) | 30 (15.31) | .29 |
| Previous PCI | 46 (21.60) | 4 (23.53) | 42 (21.43) | .84 |
| Previous coronary artery bypass surgery | 7 (3.29) | 2 (11.76) | 5 (2.55) | .04 |
| Clinical presentation | ||||
| STEACS | 31 (14.55) | 4 (23.53) | 27 (13.78) | .25 |
| Non-Q-wave AMI type of NSTEACS | 77 (36.15) | 6 (35.29) | 71 (36.22) | .66 |
| Unstable angina type of SCASEST | 37 (17.37) | 3 (17.65) | 34 (17.35) | .88 |
| Stable angina or documented ischemia | 68 (31.4) | 4 (23.53) | 64 (32.65) | .52 |
|
AMI, acute myocardial infarction; BVS, bioresorbable vascular scaffold; LVEF, left ventricular ejection fraction; NSTEACS, non-ST-segment elevation acute coronary syndrome; PCI, percutaneous coronary intervention; STEACS, ST-segment elevation acute coronary syndrome; TIA, transient ischemic attack. Data are expressed as no. (%) or mean ± standard deviation. |
||||
Index procedure of the bioresorbable vascular scaffold implantation
Table 2 shows the characteristics of the patients’ index procedure. Two hundred and thirty-three coronary lesions were treated with an average 1.3 ± 0.3 lesions per patient. Implantation was successful in 99.5% of the cases but failed in 1 patient due to the difficulty advancing the device across the lesions. The patient required the implantation of a DES, which is why he was excluded from the analysis. Predilatation occurred in 89.3% of the cases and postdilatation in 33.5% of the cases. Intracoronary imaging modalities (OCT or IVUS) were used to optimize the BVS implantation in 86 patients (40.38%).
Table 2. Characteristics of the index procedure and treatment
| Characteristics | Patients who received BVS (n = 213) |
|---|---|
| Lesions treated per patient | 1.3 ± 0.3 |
| Number of devices per patient | 1.2 ± 0.4 |
| Total length of the device per patient (mm) | 21.5 ± 13.5 |
| Minimum device diameter per patient (mm) | 2.75 ± 0.25 |
| Device implantation | |
| At least 1 BVS | 212 (99.5) |
| BVS only | 204 (95.8) |
| Overlapping with at least 2 AVBs | 20 (9.39) |
| Any DES | 8 (3.8) |
| After BVS implantation failure | 1 (0.5) |
| Procedural time (min.) | 44 ± 23 |
| Iodinated contrast used per procedure (mL) | 161 ± 72 |
| Predilatation of the first lesion treated | 189 (88.7) |
| Procedural success | 212 (99.5) |
| Lesions treated | |
| Total number | 233 |
| Predilatation | 208 (89.3) |
| Postdilatation | 78 (33.5) |
| 0.5 mm postdilatation balloon plus BVS | 21 (9.86) |
| Overall number of devices implanted | 261 |
| Overall number of devices per lesion | 1.12 ± 0.4 |
| Intracoronary imaging modality during implantation | |
| OCT or IVUS | 86 (40.38) |
|
BVS, bioresorbable vascular scaffold; DES, drug-eluting stent; IVUS, intravascular ultrasound; OCT, optical coherence tomography. Data are expressed as no. (%) or mean ± standard deviation. |
|
Clinical follow-up
The median follow-up was 44 months [28 months] with minimum times < 1 month. The primary composite endpoint of target vessel failure rate was 6.57% at the 24-month follow-up (table 3) and 7.98% at the end of the follow-up. Figure 1 shows the target vessel failure-free survival curve; at the 48-month follow-up it was 0.92 (95%CI, 0.87-0.95; P = .02). Regarding the secondary endpoint, the overall rate was 11.74% at the 24-month follow-up (table 3) and 17.84% at the end of the follow-up.
Table 3. Adverse events at the 2-year follow-up
| Adverse event | Patients who received BVS 2-year follow-up (n = 213) |
|---|---|
| Clinical events | |
| All-cause mortality | 5 (2.34) |
| Cardiac | 3 (1.41) |
| Non-cardiac | 2 (0.94) |
| All myocardial infarctions | 6 (2.82) |
| During index procedure | 2 (0.94) |
| Not during index procedure | 4 (1.88) |
| Target vessel | 3 (1.41) |
| Non-target vessel | 1 (0.47) |
| Death or myocardial infarction | 11 (5.16) |
| Any revascularization | 18 (8.46) |
| Target vessel | 11 (5.16) |
| Target lesion | 11 (5.16) |
| Device thrombosis | 3 (1.41) |
| Device restenosis | 8 (3.76) |
| Any other vessel | 7 (3.29) |
| Composite endpoint | |
| Target vessel failure | 14 (6.57) |
| Overall clinical endpoint | 25 (11.74) |
| Device thrombosis | |
| Definite | 3 (1.41) |
| Probable | 2 (0.94) |
| Possible | 1 (0.47) |
|
BVS, bioresorbable vascular scaffold. Data are expressed as no. (%). |
|
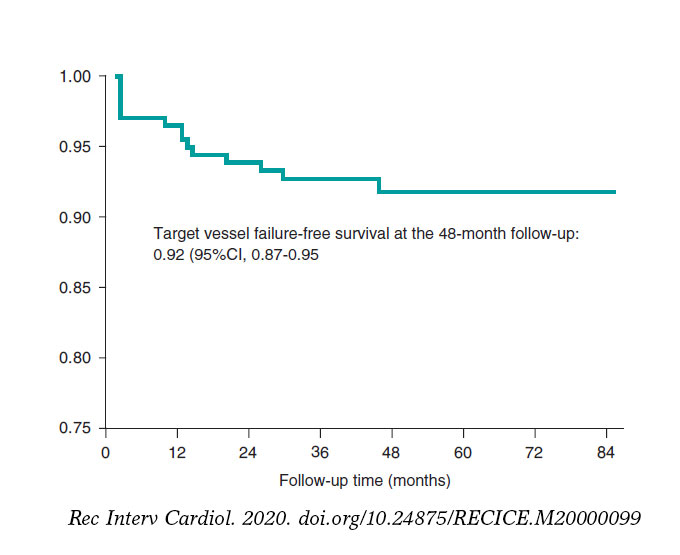
Figure 1. Kaplan-Meier survival curve for target vessel failure.
Figure 2 shows the rate of all adverse events depending on the time of clinical presentation. Regarding the primary endpoint, there were 3 (1.41%) cases of cardiac death, 4 (1.87%) cases of target vessel related AMI, and 14 (6.57%) cases of target vessel revascularization. Regarding the secondary endpoint, there were 7 (3.29%) cases of all-cause mortality, 7 (3,29%) cases of AMI, and 31 (14.56%) cases of any coronary revascularizations. Finally, regarding the device, there were 6 (2.81%) cases of thrombosis (definite, probable, and possible) all reported within the first 12 months. Dual antiplatelet therapy was kept, at least, for 12 months in 157 (73.7%) patients and 1 patient with late definite thrombosis received dual antithrombotic therapy (acenocoumarol and clopidogrel). Similarly, there were 10 (4.69%) cases of BVS restenosis within the first 48 months of follow-up (figure 3).

Figure 2. Chart of adverse events based on the time of presentation after the index procedure. AMI, acute myocardial infarction; BVS, bioresorbable vascular scaffold.
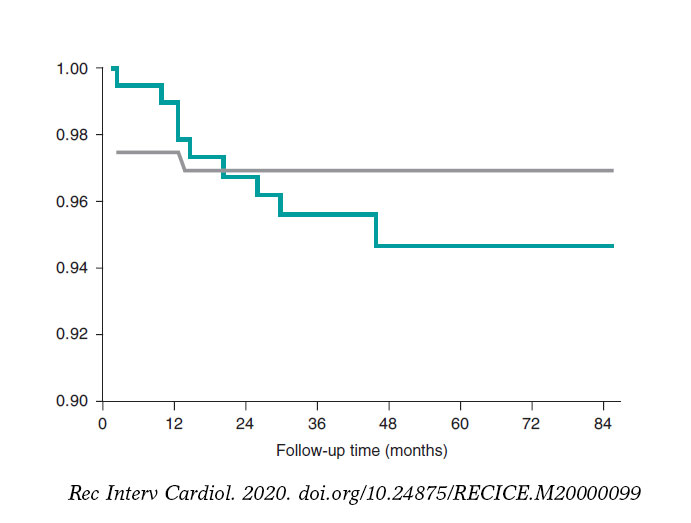
Figure 3. Kaplan-Meier survival curves for bioresorbable vascular scaffold restenosis and thrombosis.
Patients with target vessel failure had a higher prevalence of cerebrovascular disease (17.65% vs 3.06%; P = 0.01), chronic oral anticoagulation (17.65% vs 3.57%; P = .01), and previous coronary artery bypass graft surgery (11.76% vs 2.55%; P = .04). Similarly, there was a tendency towards a higher prevalence of diabetes mellitus in this group (41.18 vs 22.45%; P = .06) (table 1).
In the multivariate Cox regression analysis, a prior history of diabetes mellitus (HR, 1.72; 95%CI, 1.01-2.95; P = .05) and chronic oral anticoagulation (HR, 5.71; 95%CI, 1.12-28.94; P = .04) were identified as risk factors to develop target vessel failure at the follow-up. On the other hand, the use of intracoronary imaging modalities (OCT or IVUS) during BVS implantation showed a clear tendency towards significance as a protective factor (HR, 0.33; 95%CI, 0.10-1.07; P = .06) (table 4).
Table 4. Factors associated with target vessel failure: Cox regression analysis
| Univariate analysis | Multivariate analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95%CI | P | HR | 95%CI | P | |
| Past medical history | ||||||
| Diabetes mellitus | 1.72 | 1.04-2.86 | .04 | 1.72 | 1.01-2.95 | .05 |
| Previous stroke or TIA | 6.28 | 1.76-22.31 | .01 | 1.94 | 0.40-9.23 | .40 |
| Chronic oral anticoagulation | 5.34 | 1.51-18.97 | .01 | 5.71 | 1.12-28.95 | .04 |
| Use of intracoronary imaging modalities during implantation | ||||||
| OCT or IVUS | 0.32 | 0.11-1.03 | .06 | 0.33 | 0.10-1.06 | .06 |
|
95%CI, 95% confidence interval; HR, hazard ratio; IVUS, intravascular ultrasound; OCT, optical coherence tomography; TIA, transient ischemic attack. |
||||||
DISCUSSION
This study analyzed a consecutive series of patients who were implanted with, at least, 1 BVS in a high-volume setting and in real-life conditions. The primary composite endpoint of target vessel failure and the overall secondary composite clinical endpoint were similar to what had been reported by other previous randomized clinical trials on percutaneous coronary interventions.18-22
The AIDA clinical trial20 confirmed the lower rate of target vessel failure related AMI from our series. In our study, the patients’ baseline clinical characteristics and clinical presentation were similar to those of the population of the AIDA clinical trial. However, regarding the index procedure, the use of postdilatation was lower in our series. It has been reported that postdilatation does not bring any additional benefits to the implantation of a BVS in the ST-segment elevation acute coronary syndrome clinical setting. If elevation is excessive it could even have deleterious effects when destructuring or tearing the nonmetallic structure of the scaffold.23 The GHOST-EU registry24 proved that the PSP strategy (predilatation, scaffold sizing, and postdilatation) was a predictor of cardiovascular events.
The right selection of the lesion plays a crucial role in the clinical performance of BVS. Most of the patients of this series showed acute coronary syndrome. It is feasible that patients with AMI may benefit the most from BVS treatments.18 First, patients with acute coronary syndrome (with or without ST-segment elevation) often show a visible thrombus in the proximal segments and a less complex morphology with thin-cap fibroatheroma plaques and fewer calcified lesions. Secondly, aggressive antithrombotic therapy after an acute coronary syndrome may mitigate the rate of thrombotic complications.
Bioresorbable vascular scaffold thrombosis
A few studies have reported on a higher rate of BVS thrombosis associated with next-generation DESs,25,26 especially all in off-label uses.27 In our series, the definite or probable device thrombosis occurred in a similar percentage of the patients to that previously reported.12 Several mechanisms that may explain BVS thrombosis have been suggested including edge dissection, strut fracture, malapposition, and inadequate BVS sizing.28 In our series there were 2 cases of subacute definite thrombosis. In the coronary angiography, the OCT performed confirmed the presence of some structural mechanism (underexpansion or malapposition) that favored it. Early presentation at the follow-up is consistent with what has already been reported.29
Similarly, we identified that the use of intracoronary imaging modalities (OCT or IVUS) during BVS implantation showed a clear tendency towards significance as a protective factor of target vessel failure as Caixeta et al.30 had already confirmed in an international registry of 1933 patients. The recommendation here is to use intracoronary imaging modalities to optimize implantation and secure the correct apposition of the BVS, lack of underexpansion, and proper cover of the lesion.31
The main setback of the Absorb BVS is probably strut thickness and width (157 x 190.5 µm in 2.5 mm and 3.0 mm BVSs, and 157 µm x 216 µm in 3.5 mm BVSs), which can make the device more thrombogenic, especially when apposition is not the right one or expansion is incomplete. Today, ultra-thin drug-eluting stents (strut thickness < 70 µm) have lowered the risk of target lesion failure to just 1 year compared to modern second-generation DESs thanks to fewer AMIs and stent thrombosis.32 On this issue, the sirolimus-eluting MeRes100 BVS (Meril Life Sciences Pvt. Ltd., India) with thinner strut thickness (100 µm) confirmed the sustained efficacy and safety profile at the 2- and 3-year follow-up.33
Resistance to antiplatelet therapy can also be an important cause for BVS thrombosis.34 Both acetylsalicylic acid and clopidogrel are effective antiplatelet drugs for the secondary prevention of cardiovascular events. Still their clinical efficacy varies from one individual to the next.35 In our series, most of the patients remained on dual antiplatelet therapy for, at least, 12 months and there was 1 case of late thrombosis with dual antithrombotic therapy (acenocoumarol and clopidogrel). Due to his high bleeding risk, this last patient received dual antiplatelet therapy for the first 3 months; we do not know the international normalized ratio when the complication occurred, which is why the possibility of antiplatelet drug resistance cannot be discarded. However, the potential association between the BVS thrombosis and oral antiplatelet therapy had already been described.36 We know that the selection of duration of antiplatelet therapy following the implantation of the Absorb BVS was difficult,37 especially in anticoagulated patients because they are a population with comorbidities and high cardiovascular risk. Our data show that the implantation of the Absorb BVS in patients at high bleeding risk (including anticoagulated patients) shouldn’t probably be recommended according to the consensus document reached by the European Society of Cardiology and the European Association for Cardio-Thoracic Surgery. This document does not recommend the use of the Absorb BVS in patients intolerant to prolonged dual antiplatelet therapy or who require oral anticoagulation.16
Bioresorbable vascular scaffold restenosis
The most common cause for target lesion revascularization was stent restenosis within the first 48 months of follow-up. The mechanisms involved in bioresorbable vascular scaffold restenosis that may occur in the same patient are varied.38,39 The less intrinsic radial strength and its possible destructuring with an aggressive implantation may explain some of the early recurrences. In this study, aggressive implantation was less common since postdilatation with an up to 0.5 mm balloon combined with BVS implantation occurred in 9.86% of the cases. Also, postdilatation was not associated with restenosis at the follow-up. Also, it has been suggested that the slow resorption of the study device may have been associated with a significant spatial abnormality with loss of alignment of its structural elements, which favors restenosis.40,41 The complete disappearance of the BVS from the vascular wall won’t happen for another 3 years6 and most cases of scaffold restenosis occurred within the first 2 years of follow-up.
Our study results show that there is a correlation between the history of diabetes mellitus and chronic oral anticoagulation and the development of target vessel failure. It is well-known that this past medical history elevates cardiovascular morbimortality and that the CHADS2 and CHA2DS2-VASc scores can be used to estimate the risk of adverse clinical events in patients with acute coronary syndrome.42 In this sense, patients with a past medical history of diabetes mellitus, chronic oral anticoagulation, and coronary artery disease start with CHA2DS2-VASc scores of 4, that is, high risk of adverse clinical events.
Limitations
Selection bias was inevitable because, according to the operator’s criterion, the clinical assessment that may have influenced the decision to implant a BVS maybe did not come from the database, which is a common problem with observational studies like this one. However, the study shows a pragmatic approach to the use of this device in the real world.
CONCLUSIONS
In this series of patients implanted with the Absorb BVS, the composite endpoint of target vessel failure and the overall clinical composite endpoint were similar to what had already been reported by randomized clinical trials. Adverse events were more common within the first 2 years of follow-up in case of greater cardiovascular comorbidity and without intracoronary imaging modalities (OCT or IVUS) during implantation. Although the BVS studied is not available anymore there other bioresorbable devices are in the pipeline.16
FUNDING
R. Mori-Junco received the 2018 training grant from the European Society of Cardiology (APP000019660). L. Furuya-Kanamori received funding from the Australian National Health and Medical Research Council Early Career Fellowships (APP1158469).
CONFLICTS OF INTEREST
The authors declared no conflicts of interest whatsoever.
WHAT IS KNOWN ABOUT THE TOPIC?
- The implantation of a BVS is an innovative approach for the management of coronary atherosclerosis because it releases the coronary artery from a permanent metallic jail and restores the vessel architecture.
- However, the Absorb BVS has a higher rate of thrombotic complications compared to modern DESs, which is why it was removed.
WHAT DOES THIS STUDY ADD?
- In our interventional cardiology network, the implantation of the Absorb BVS showed rates of target vessel failure that were similar to those previously described by randomized clinical trials.
- Target vessel failure occurred basically within the first 24 months in patients with diabetes mellitus or chronic oral anticoagulation. The use of intracoronary imaging modalities during implantation showed a tendency towards becoming a protective factor.
- Our results will contribute to the proper selection of patients eligible for BVS implantation and to the implantation technique as well.
REFERENCES
1. Smits PC, Vlachojannis GJ, McFadden EP, et al. Final 5-Year Follow-Up of a Randomized Controlled Trial of Everolimus- and Paclitaxel-Eluting Stents for Coronary Revascularization in Daily Practice:The COMPARE Trial (A Trial of Everolimus-Eluting Stents and Paclitaxel Stents for Coronary Revas.cularization in Daily Practice). JACC Cardiovasc Interv. 2015;8:1157-1165.
2. Byrne RA, Stone GW, Ormiston J, Kastrati A. Coronary balloon angioplasty, stents, and scaffolds. Lancet. 2017;390:781-792.
3. Ellis SG, Riaz H. Bioresorbable stents:The future of interventional cardiology?Cleve Clin J Med. 2016;83:S18-S23.
4. Ellis SG, Kereiakes DJ, Metzger DC, et al. Everolimus-Eluting Bioresorbable Scaffolds for Coronary Artery Disease. N Engl J Med. 2015;373:1905-1915.
5. Ormiston JA, Serruys PW, Regar E, et al. A bioabsorbable everolimus-eluting coronary stent system for patients with single de-novo coronary artery lesions (ABSORB):a prospective open-label trial. Lancet. 2008;371:899-907.
6. Serruys PW, Garcia-Garcia HM, Onuma Y. From metallic cages to transient bioresorbable scaffolds:change in paradigm of coronary revascularization in the upcoming decade?Eur Heart J. 2012;33:16-25.
7. Serruys PW, Katagiri Y, Sotomi Y, et al. Arterial Remodeling After Biore.sorbable Scaffolds and Metallic Stents. J Am Coll Cardiol. 2017;70:60-74.
8. Serruys PW, Chevalier B, Sotomi Y, et al. Comparison of an everolim.us-eluting bioresorbable scaffold with an everolimus-eluting metallic stent for the treatment of coronary artery stenosis (ABSORB II):a 3 year, randomised, controlled, single-blind, multicentre clinical trial. Lancet. 2016;388:2479-2491.
9. Rampat R, Mayo T, Hildick-Smith D, Cockburn J. A randomized trial comparing two stent sizing strategies in coronary bifurcation treatment with bioresorbable vascular scaffolds –The Absorb Bifurcation Coronary (ABC) trial. Cardiovasc Revascularization Med. 2019;20:43-49.
10. Mitomo S, Naganuma T, Fujino Y, et al. Bioresorbable Vascular Scaffolds for the Treatment of Chronic Total Occlusions. Circ Cardiovasc Interv. 2017;10:e004265.
11. Abbott Laboratories. Abbott Receives CE Mark Approval for World's First Drug Eluting Bioresorbable Vascular Scaffold for Treatment of Coronary Artery Disease. Available online:https://www.prnewswire.com/news-releases/abbott-receives-ce-mark-approval-for-worlds-first-drug-eluting-bioresorbable-vascular-scaffold-for-treatment-of-coronary-artery-disease-113197364.html. Accessed 25 Aug 2019.
12. Wykrzykowska JJ, Kraak RP, Hofma SH, et al. Bioresorbable Scaffolds versus Metallic Stents in Routine PCI. N Engl J Med. 2017;376:2319-2328.
13. Kerkmeijer LSM, Tijssen RYG, Hofma SH, et al. Comparison of an evero.limus-eluting bioresorbable scaffold with an everolimus-eluting metallic stent in routine PCI:three-year clinical outcomes from the AIDA trial. EuroIntervention. 2019;15:603-606.
14. Stone GW, Gao R, Kimura T, et al. 1-year outcomes with the Absorb bioresorbable scaffold in patients with coronary artery disease:a patient-level, pooled meta-analysis. Lancet. 2016;387:1277-1289.
15. Katsikis A, Serruys PW. Bioresorbable scaffolds versus metallic stents in routine PCI:the plot thickens. J Thorac Dis. 2017;9:2296-2300.
16. Byrne RA, Stefanini GG, Capodanno D, et al. Report of an ESC-EAPCI Task Force on the evaluation and use of bioresorbable scaffolds for percutaneous coronary intervention:executive summary. Eur Heart J. 2018;39:1591-1601.
17. Nuñez Gil IJ, Bas M, Fernández-Ortiz A, et al. Long term experience with a novel interventional cardiology network model:Learned lessons. J Hosp Adm. 2016;5:87-94.
18. Byrne RA, Alfonso F, Schneider S, et al. Prospective, randomized trial of bioresorbable scaffolds vs. everolimus-eluting stents in patients undergoing coronary stenting for myocardial infarction:The Intracoronary Scaffold Assessment a Randomized evaluation of Absorb in Myocardial Infarction (ISAR-Absorb MI) trial. Eur Heart J. 2019;40:167-176.
19. Capodanno D, Gori T, Nef H, et al. Percutaneous coronary intervention with everolimus-eluting bioresorbable vascular scaffolds in routine clinical practice:Early and midterm outcomes from the European multicentre GHOST-EU registry. EuroIntervention. 2015;10:1144-1153.
20. Tijssen RYG, Kraak RP, Hofma SH, et al. Complete two-year follow-up with formal non-inferiority testing on primary outcomes of the AIDA trial comparing the Absorb bioresorbable scaffold with the XIENCE drug-eluting metallic stent in routine PCI. EuroIntervention. 2018;14:e426-e433.
21. Chevalier B, Onuma Y, Boven AJ Van. Randomised comparison of a bioresorbable everolimus- eluting scaffold with a metallic everolimus-eluting stent for ischaemic heart disease caused by de novo native coronary artery lesions:the 2-year clinical outcomes of the ABSORB II trial. EuroIntervention. 2016;12:1102-1107.
22. Alvarez M, Applegate RJ. Early and Late Bioresorbable Vascular Scaffold Thrombosis:Size Matters. JACC Cardiovasc Interv. 2017;10:2372-2374.
23. Yamaji K, Brugaletta S, SabatéM, et al. Effect of Post-Dilatation Following Primary PCI With Everolimus-Eluting Bioresorbable Scaffold Versus Everolimus-Eluting Metallic Stent Implantation. JACC Cardiovasc Interv. 2017;10:1867-1877.
24. Ortega-Paz L, Capodanno D, Gori T, et al. Predilation, sizing and post-dilation scoring in patients undergoing everolimus-eluting bioresorbable scaffold implantation for prediction of cardiac adverse events:Development and internal validation of the PSP score. EuroIntervention. 2017;12:2110-2117.
25. Lipinski MJ, Escarcega RO, Baker NC, et al. Scaffold Thrombosis After Percutaneous Coronary Intervention With ABSORB Bioresorbable Vascular Scaffold. JACC Cardiovasc Interv. 2016;9:12-24.
26. Alfonso F, Cuesta J. Very Late Bioresorbable Vascular Scaffold Thrombosis:Smoke or Fire?JACC Cardiovasc Interv. 2017;10:38-41.
27. Miyazaki T, Ruparelia N, Kawamoto H, Figini F, Latib A, Colombo A. Clinical outcomes following “off-label“versus “established“indications of bioresorbable scaffolds for the treatment of coronary artery disease in a real-world population. EuroIntervention. 2016;11:1475-1478.
28. Puricel S, Cuculi F, Weissner M, et al. Bioresorbable Coronary Scaffold Thrombosis. J Am Coll Cardiol. 2016;67:921-931.
29. Brugaletta S, Gori T, Low AF, et al. Absorb bioresorbable vascular scaffold versus everolimus-eluting metallic stent in ST-segment elevation myocardial infarction:1-year results of a propensity score matching comparison:the BVS-EXAMINATION Study (bioresorbable vascular scaffold - a clinical evaluation of everolimus eluting coronary stents in the treatment of patients with ST-segment elevation myocardial infarction). JACC Cardiovasc Interv. 2015;8:189-197.
30. Caixeta A, Campos CM, Felix C, et al. Predictors of long-term adverse events after Absorb bioresorbable vascular scaffold implantation:a 1,933.patient pooled analysis from international registries. EuroIntervention. 2019;15:623-630.
31. IJsselmuiden AJJ, Zwaan EM, Oemrawsingh RM, et al. Appropriate use criteria for optical coherence tomography guidance in percutaneous coronary interventions:Recommendations of the working group of interven.tional cardiology of the Netherlands Society of Cardiology. Neth Heart J. 2018;26:473-483.
32. Bangalore S, Toklu B, Patel N, Feit F, Stone GW. Newer-Generation Ultra-thin Strut Drug-Eluting Stents Versus Older Second-Generation Thicker Strut Drug-Eluting Stents for Coronary Artery Disease. Circulation. 2018;138:2216-2226.
33. Seth A, Onuma Y, Chandra P, et al. Three-year clinical and two-year multimodality imaging outcomes of a thin-strut sirolimus-eluting bioresorb.able vascular scaffold:MeRes-1 trial. EuroIntervention. 2019;15:607-614.
34. Fernández-Rodríguez D, Brugaletta S, Otsuki S, SabatéM. Acute Absorb bioresorbable vascular scaffold thrombosis in ST-segment elevation myocardial infarction:to stent or not to stent?EuroIntervention. 2014;10:600;discussion 600.
35. Tantry US, Navarese EP, Bliden KP, Gurbel PA. Acetylsalicylic acid and clopidogrel hyporesponsiveness following acute coronary syndromes. Kardiol Pol. 2018;76:1312-1319.
36. Cayla G, Koning R, Fajadet J, et al. Percutaneous coronary interventions with the Absorb Bioresorbable vascular scaffold in real life:1-year results from the FRANCE ABSORB registry. Arch Cardiovasc Dis. 2019;112:113-123.
37. Valgimigli M, Bueno H, Byrne RA, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS. Eur Heart J. 2018;39:213-260.
38. Núñez-Gil IJ, Echavarría M, Escaned J, Biagioni C, Feltes G, Fernández-Ortiz A. Bioresorbable stent restenosis:new devices, novel situations. J Invasive Cardiol. 2014;26:E164-6.
39. Longo G, Granata F, Capodanno D, et al. Anatomical features and manageµment of bioresorbable vascular scaffolds failure:A case series from the GHOST registry. Catheter Cardiovasc Interv. 2015;85:1150-1161.
40. Nakatani S, Onuma Y, Ishibashi Y, et al. Early (before 6 months), late (6-12 months) and very late (after 12 months) angiographic scaffold restenosis in the ABSORB Cohort B trial. EuroIntervention. 2015;10:1288-1298.
41. Räber L, Brugaletta S, Yamaji K, et al. Very Late Scaffold Thrombosis. J Am Coll Cardiol. 2015;66:1901-1914.
42. Chua S-K, Lo H-M, Chiu C-Z, Shyu K-G. Use of CHADS2 and CHA2DS2.VASc scores to predict subsequent myocardial infarction, stroke, and death in patients with acute coronary syndrome:data from Taiwan acute coro.nary syndrome full spectrum registry. PLoS One. 2014;9:e111167.
ABSTRACT
Introduction and objectives: Spontaneous coronary artery dissection (SCAD) is a rare but increasingly recognized cause for acute coronary syndrome. The optimal management and treatment of SCAD is still unknown.
Methods: Data analysis of a prospective protocol including centralized care management of a consecutive series of patients with SCAD diagnosed between January 2010 and December 2018. Major adverse cardiovascular events included all-cause mortality, new myocardial infarction, coronary revascularization, ventricular arrhythmia, heart failure or stroke.
Results: A total of 33 consecutive patients were included (41 lesions). Intravascular imaging modalities were used to confirm the diagnosis in 42% patients. None of the patient showed images of thrombus formation in the true lumen. Conservative treatment was the initial approach in most of the cases (82%). No deaths were reported during the index admission, but 15% experienced major adverse cardiovascular events. The coronary computed tomography angiography performed in 58% of patients during the admission identified SCADs in 79% of the patients. Most of the patients managed with conservative treatment received only 1 antiplatelet agent for a limited period of time (17 months [9-35]). During a median clinical follow-up of 33 months [13-49], 82% of patients did not have any adverse events. The angiographic surveillance obtained in 48% of patients at the 6-month follow-up confirmed the complete healing of the SCAD image in 86% of the patients. The screening for extracoronary vascular findings (97% of patients) resulted in a high prevalence of abnormalities (59%).
Conclusions: The unrestricted use of intravascular imaging modalities showed no thrombus in the true lumen of patients with SCAD. In patients managed with conservative treatment, a limited course of antiplatelet monotherapy is safe and provides good clinical outcomes. Performing a coronary computed tomography angiography in the acute phase of SCAD is useful at the follow-up. The screening for extracoronary vascular findings confirmed a high prevalence of abnormalities.
Keywords: Spontaneous coronary artery dissection. Coronary artery disease. Acute coronary syndrome. Optical coherence tomography. Fibromuscular dysplasia.
RESUMEN
Introducción y objetivos: La disección coronaria espontánea (DCE) constituye una causa infrecuente, pero cada vez más reconocida, de síndrome coronario agudo. La actitud diagnóstico-terapéutica idónea sigue sin esclarecerse.
Métodos: Análisis del seguimiento prospectivo y centralizado de una serie de pacientes consecutivos diagnosticados de DCE desde enero de 2010 hasta diciembre de 2018. Se definió evento cardiovascular adverso mayor como la aparición de muerte de cualquier causa, reinfarto no mortal, revascularización no planificada, arritmia ventricular, insuficiencia cardiaca o ictus.
Resultados: Se incluyó a 33 pacientes con DCE (41 lesiones). En el 42% se realizó un estudio con imagen intracoronaria para confirmar el diagnóstico, sin identificar trombo en la luz verdadera en ninguno de ellos. En la mayoría de los casos (82%) se eligió un tratamiento médico conservador. Ningún paciente falleció durante el ingreso, pero el 15% presentó algún evento mayor. En el momento agudo se realizó tomografía computarizada coronaria al 58% de los pacientes y se identificó la DCE en el 79% de los casos. La mayoría de los pacientes con tratamiento conservador recibieron antiagregación simple un tiempo limitado (17 meses [9-35]). Con una mediana de seguimiento de 33 meses [13-49], el 82% no sufrió ningún evento adverso. Al 48% se les realizó control angiográfico a los 6 meses, que mostró resolución en el 86% de los casos. El cribado de anomalías vasculares extracoronarias se realizó en el 97% de los pacientes y se hallaron alteraciones en el 59%, incluyendo 3 pacientes con aneurisma intracraneal.
Conclusiones: En esta serie, con una amplia utilización de imagen intracoronaria, no se ha identificado trombo en la luz verdadera en ningún caso de DCE. En los pacientes tratados de forma conservadora, la monoterapia antiagregante es segura y se asocia a buenos resultados clínicos. La tomografía computarizada coronaria durante el ingreso es útil en el seguimiento. El cribado sistemático de anomalías vasculares extracoronarias revela una alta prevalencia de alteraciones.
Palabras clave: Disección coronaria espontánea. Enfermedad coronaria. Síndrome coronario agudo. Tomografía de coherencia óptica. Displasia fibromuscular.
Abbreviations ACS: acute coronary syndrome. EVA: extracoronary vascular abnormalities. FMD: fibromuscular dysplasia. PCI: percutaneous coronary intervention. SCAD: spontaneous coronary artery dissection.
INTRODUCTION
Spontaneous coronary artery dissection (SCAD) is a rare cause of acute coronary syndrome (SCA). However, especially in women, it has been identified as the underlying pathophysiological mechanism in a growing percentage of cases. SCAD is defined as the separation of the coronary artery wall layers not associated with trauma, iatrogenesis, atherosclerosis or extension of an aortic dissection.1 Clinical signs are myocardial ischemia and are due to the coronary flow limitation that alters the arterial parietal structures.
The first description ever reported by Pretty2 back in 1931 was followed by the description of isolated cases and small series for years. However, we have recently seen a significant increase of information on SCADs lately. Nowadays, clinical profile, diagnostic and therapeutic approach, and prognosis can be found in the SCAD and they vary significantly compared to atherosclerosis—the most common cause of ACS.3,4 Even the European Society of Cardiology5 and the American Heart Association6 have recently published 2 consensus documents on this disease.
In light of the growing evidence and in an attempt to enrich it, back in 2010 our center started a specific program of diagnosis and follow-up of patients with SCAD. The results and conclusions are presented here.
METHODS
All cases of SCAD were collected prospectively since 2010. Diagnosis, treatment, and follow-up were centralized and unified according to the scientific evidence available at the time. Given the length of the study period (9 years) and the extensive medical literature available on this issue over the years, new aspects in the assessment of patients (such as fibromuscular dysplasia [FMD]) have been introduced gradually. This protocol and the data collection book were approved by our center ethics committee and registered in a validated repository (NCT03607981). The patients’ informed consents were obtained in all cases.
Clinical information and follow-up
The demographic characteristics, the patients’ personal past medical histories, data at admission, and disease progression were collected in the clinical history at admission and follow-up in a SCAD monographic review (T. Bastante). The coronary angiography and intravascular imaging studies were analyzed by 3 expert interventional cardiologists (T. Bastante, M. García-Guimaraes, and F. Alfonso) and the final diagnosis of SCAD was only established if they all agreed unanimously. The use of intracoronary imaging modalities (intravascular ultrasound [IVUS] or optical coherence tomography [OCT]) was left to the operator’s discretion. However, it was recommended in cases of suspicious diagnosis (especially type 2 and 3 SCADs according to Saw angiographic classification7) or need to perform PCI as long as the segment under study was accessible and in a not overly tortuous artery. When the OCT was used, the intracoronary image was classified as double lumen when the separation of the arterial layers originated true and false lumens, both with lack of refraction due to complete contrast washout. Intramural hematoma was defined as the separation of arterial layers occupied by moderately refracting material with an attenuation consistent with intraparietal bleeding without complete contrast washout. Both the IVUS and the OCT tried to identify the communication between the false and the true lumen and the presence of thrombotic material in the latter (figure 1 shows typical examples). The initial recommended treatment was a wait-and-see conservative approach and the PCI was only performed in cases of clinical instability or symptom persistence. During admission, and as long as it was possible, a coronary computed tomography (CT) scan was performed for a better characterization of coronary lesions. This information was used during follow-up as a comparative pattern in a new coronary CT scan to confirm the healing of the SCAD or in the reappearance of symptoms for reevaluation purposes. Patients with a diagnosis suggestive, but not definitive, of SCAD were scheduled to receive a control coronary angiography within the following months.
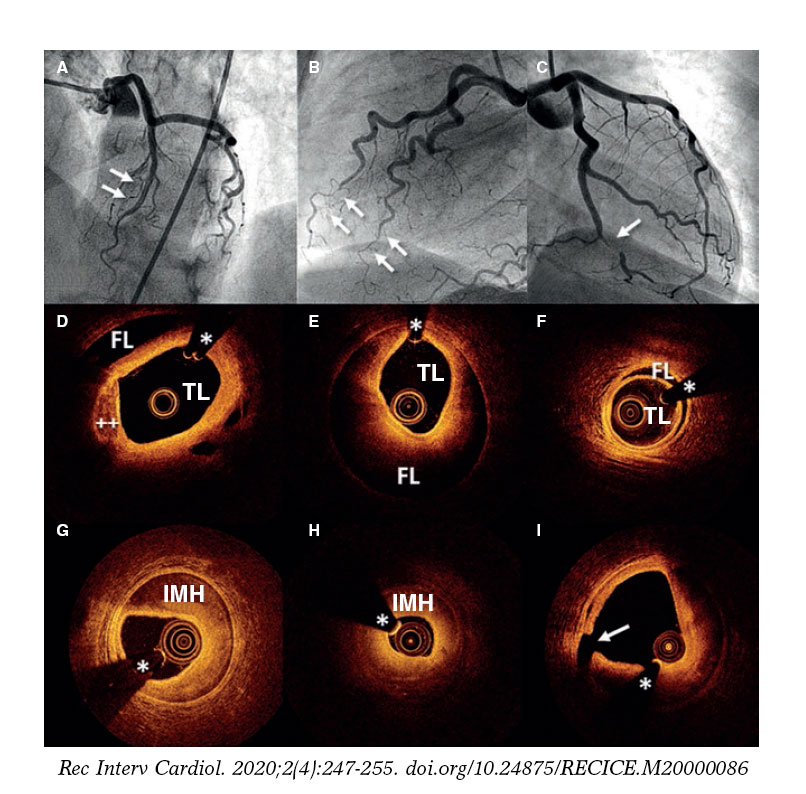
Figure 1. Images of angiography (A-C) and optical coherence tomography (OCT) (D-I). A: type 1 spontaneous coronary dissection (SCAD) in the medial portion of the left anterior descending coronary artery. The arrows point to the characteristic imaging of double lumen with linear intraluminal filling defect outlined by contrast (video 1 of the supplementary data). B: type 2 SCAD in distal left anterior descending coronary artery and diagonal branch. The arrows point to the sudden loss of vessel caliber with length > 20 mm (video 2 of the supplementary data). C: type 3 SCAD in obtuse marginal artery. The arrows point to focal stenosis with length < 20 mm similar to an atherosclerotic lesion (video 3 of the supplementary data). D-F: OCT images showing the double lumen morphology (TL, true lumen; FL, false lumen). Note the unusual image of subintimal calcium displaced with the flap (++). G-H: morphology of intramural hematoma (IMH). I: entry (arrow) with partially thrombosed false lumen. The asterisk (*) shows guidewire artifact.
Definitions
In order to classify the angiographic patterns of SCAD, the aforementioned specific classification developed by Saw et al.7 was used (figure 1 shows examples of this). Two different criteria of success were established for cases where a PCI was required. In the first place, conventional procedural success was defined as a final TIMI flow grade 2-3 (Thrombolysis in Myocardial Infarction) with residual stenosis < 30% after stent/scaffold implantation or < 50% after simple balloon angioplasty. Secondly, the PCI-SCAD was considered successful with flow improvements ≥ 1 grade in the TIMI score and a final TIMI flow grade of 2-3.8 Major cardiovascular adverse events (MACE) at the follow-up included all-cause mortality, reinfarction, unscheduled revascularization, ventricular arrhythmia, heart failure, and stroke.
Screening of extracoronary vascular abnormalities
Since 2013 and as long as it was possible, a selective angiography of both renal and iliac arteries during the diagnostic coronary angiography was performed. Also, 3 to 6 months after the event, the study was completed using the angio-CT scan to examine the floor of the middle cranial fossa up to the femoral arteries (modification of the protocol published by Liang et al.9) including intracranial vessels, supra-aortic trunks, the aorta, and mesenteric, renal, and iliac branches. FMD was defined as the presence of focal narrowing separated by dilatation areas with the traditional «pearl necklace» appearance (multifocal shape) or the presence of tubular focal lesions (unifocal shape). Aneurysms were defined as dilatations > 50% with respect to the caliber of the normal, adjacent arterial segment. Dissection was defined as a double lumen morphology in the arterial segment. The screening of extracoronary vascular abnormalities (EVA) was considered complete when the intracranial territories, supra-aortic trunks, the aorta, and the splanchnic, renal, and iliac territories all had been examined (using angiography, angio-CT scan or both).
Statistical analysis
Quantitative variables were expressed as mean ± standard deviation or median [interquartile range] according to their distribution. Categorical variables were expressed as numbers (percentage). The analysis was conducted using the STATA 12 statistical software package (StataCorp LLC, United States).
RESULTS
Between January 2010 and December 2018 our center performed 12 951 diagnostic coronary angiographies that identified 37 SCADs (41 lesions) in 33 patients (0.28%). Prevalence among the coronary angiographies performed due to ACS (4185) was 1%, although prevalence among women in this context rose to 3%. If the percentage of patients with a final diagnosis of SCAD in the group of women with ACS under 50 is analyzed, prevalence rose to 12.5%. There are more diagnoses over the years from 1 or 2 patients per year initially to 5-7 annual patients over the last period (figure 1 of the supplementary data).
The baseline characteristics of the patients included in the study are shown on table 1. Most (97%) were middle-aged women (56 ± 12 years). Only 7 women (21%) had no traditional cardiovascular risk factors. Five patients (15%) had a personal past medical history of ischemic heart disease, 2 of them with a confirmed diagnosis of SCAD. A study conducted a posteriori confirmed that the remaining 3 patients showed clinical signs consistent with an initially misdiagnosed SCAD (ACS with coronary arteries interpreted as normal, 1 of them in the peripartum).
Table 1. Baseline characteristics of the patients
| n = 33 | |
|---|---|
| Women | 32 (97) |
| Age (years) | 56 ± 12 |
| Race | |
| Caucasian | 28 (85) |
| Other | 5 (15) |
| Cardiovascular risk factors | |
| Smoking habit | |
| Current smoker | 9 (27) |
| Former smoker | 7 (21) |
| Hypertension | 12 (36) |
| Hypercholesterolemia | 14 (42) |
| Diabetes | 2 (6) |
| Family history of ischemic heart disease | 4 (12) |
| Family history of SCAD | 2 (6) |
| Relevant findings | |
| Previous diagnosis of ischemic heart disease | 5 (15) |
| Confirmed diagnosis of previous SCAD | 2 (6) |
| Chronic inflammatory disease | 3 (9) |
| Depressive disorder | 5 (15) |
| Anxiety disorder | 9 (27) |
| History of hypothyroidism | 11 (33) |
| Gynecological/obstetric past medical history | n = 32 |
| Menopause | 24 (75) |
| Menopause age (years) | 49 ± 4 |
| Hormone replacement therapy | 2 (7) |
| Oral hormonal contraceptive | 1 (3) |
| Intrauterine device | 1 (3) |
| Nulliparous | 3 (9) |
| Multiparous | 18 (44) |
| History of miscarriage | 3 (9) |
|
SCAD, spontaneous coronary artery dissection. Data are expressed as no. (%) or mean ± standard deviation. |
|
Table 2 shows the characteristics at hospital admission and during the angiographic assessment. All patients presented with myocardial infarction, most of them (73%) with non-ST-elevation acute myocardial infarction. There was a trigger factor in one third of the cases; the most common was emotional stress (21%) followed by intense physical exercise (9%). Presentation at the peripartum was rare (1 patient only). The artery most frequently compromised was the left anterior descending coronary artery (51%). Eighteen percent of the patients had multivessel disease. Intracoronary imaging modalities (IVUS or OCT) were used in 42% of the cases, mostly OCT (33%). Sixteen lesions in 14 patients were assessed. Those assessed through the OCT confirmed the presence of fenestration between the false and the true lumen in 7 lesions (58%). There were no images consistent with thrombi in the true lumen in any of the cases assessed using intracoronary imaging modalities.
Table 2. Characteristics of the patients at hospital admission and in the angiographic assessment
| n = 33 | |
|---|---|
| Clinical diagnosis at admission | |
| STEMI | 9 (27) |
| NSTEMI | 24 (73) |
| Event-triggering factors | 11 (33) |
| Intense physical exercise | 3 (9) |
| Emotional stress | 7 (21) |
| Peripartum | 1 (3) |
| Angiographic characteristics | n = 33 (41 lesions) |
| Access | |
| Radial | 29 (88) |
| Femoral | 4 (12) |
| Diseased vessel | |
| Left anterior descending coronary artery | 21 (51) |
| Circumflex artery | 10 (24) |
| Right coronary artery | 10 (24) |
| Diseased segment | |
| Proximal | 10 (24) |
| Medial | 11 (27) |
| Distal | 20 (49) |
| Secondary branches | 18 (44) |
| Multivessel disease | 6 (18) |
| Multi-segment disease | 13 (32) |
| Saw et al. angiographic classification7 | |
| Type 1 | 6 (15) |
| Type 2 | 32 (78) |
| Type 3 | 3 (7) |
| Percentage of stenosis (visual estimate) | 77 ± 24 |
| Length of the lesion (mm) | 41 ± 28 |
| Initial TIMI flow grade | |
| 0 | 5 (12) |
| 1 | 5 (12) |
| 2 | 1 (2) |
| 3 | 3 (73) |
| Intracoronary imaging modality | n = 14 (16 lesions) |
| IVUS | 4 lesiones |
| Fenestration | 0 |
| Thrombus | 0 |
| OCT | 12 lesions |
| Double lumen | 7 (58) |
| Intramural hematoma | 2 (16) |
| Both | 3 (25) |
| Fenestration | 7 (58) |
| Thrombus | 0 |
|
CT, computed tomography; IVUS, intravascular ultrasound; NSTEMI, non-ST-elevation acute myocardial infarction; OCT, optical coherence tomography; STEMI, ST-segment elevation myocardial infarction; TIMI, Thrombolysis in Myocardial Infarction. Data are expressed as no. (%) or mean ± standard deviation. |
|
Table 3 shows treatment and the in-hospital disease progression. Initial conservative treatment was the first option in most cases (82%). Only 6 patients were treated with PCI as the initial strategy, 4 of them due to progressive flow worsening with the injections of contrast. The PCI conventional success was reported in 50% of the cases, and the PCI-SCAD success in 67% of the cases. One iatrogenic dissection was reported in the left main coronary artery.
Table 3. Management and in-hospital disease progression of patients
| n = 33 | |
|---|---|
| Initial treatment | |
| Conservative | 27 (82) |
| PCI | 6 (18) |
| PTCA-balloon | 2 (6) |
| Bare-metal stent | 2 (6) |
| Drug-eluting stent | 1 (3) |
| Bioresorbable vascular scaffold device | 1 (3) |
| Results from the PCI group | n = 6 |
| Conventional success | 3 (50) |
| PCI-SCAD success | 4 (67) |
| In-hospital disease progression | n = 33 |
| Peak troponin T levels (ng/mL) | 378 [132-1705] |
| Peak creatine kinase levels (U/L) | 403 [169-1181] |
| Left ventricular dysfunction [LVEF < 50%] | 5 (17) |
| Segmental abnormalities on the TTE | 17 (52) |
| MACE | 5 (15) |
| Death | 0 |
| Reinfarction | 0 |
| New coronary angiography | 4 (12) |
| Unplanned revascularization | 3 (9) |
| PCI group (n = 6) | 2 (33) |
| Conservative management group (n = 27) | 1 (4) |
| Ventricular tachycardia/fibrillation | 2 (6) |
| Heart failure | 1 (3) |
| Hospital stay (days) | 4 [3-7] |
| Coronary CT scan at admission | n = 19 (58) |
| SCAD visible on the coronary CT scan | 15 (79) |
| Treatment at hospital discharge | n = 33 |
| ASA | 31 (94) |
| Clopidogrel | 9 (27) |
| Ticagrelor | 5 (15) |
| Prasugrel | 0 |
| Dual antiplatelet therapy | 14 (42) |
| Anticoagulation | 2 (6) |
| Beta-blockers | 28 (85) |
| ACEI/ARA II | 21 (64) |
| Statins | 25 (76) |
| Nitrates | 3 (9) |
| Calcium antagonists | 3 (9) |
|
ACEI, angiotensin-converting enzyme inhibitors; ARA-II, angiontensin II receptor antagonist; ASA, acetylsalicylic acid; CT, coronary tomography; LVEF, left ventricular ejection fraction; MACE, major cardiovascular adverse events; PCI, percutaneous coronary intervention; PTCA, percutaneous transluminal coronary angioplasty; SCAD, spontaneous coronary artery dissection; TTE, transthoracic echocardiography. Data are expressed as no. (%) or mean ± standard deviation or median [interquartile range]. |
|
During in-hospital disease progression no patient died or suffered any reinfarctions. However, a new coronary angiography was required in 4 patients with symptoms. Except for the patient with a left main coronary artery iatrogenic dissection initially treated with conservative treatment no case was due to failed initial conservative treatment. The remaining 3 patients had acute stent thrombosis, SCAD of a vessel other than the index, and progression of the SCAD adjacent to the segment treated with the stent. Overall, the rate of in-hospital MACE was 15% and events focused on patients who required PCI. Acetylsalicylic acid (ASA) was prescribed to 94% of the patients at hospital discharge and dual antiplatelet therapy to 14 patients only (42%) of whom 7 required PCI. Fifty-eight percent of the patients received coronary CT scans during admission and images consistent with SCAD were found in 79% of the cases.
Table 4 shows out-of-hospital disease progression. Median follow-up was 33 months [13-49], the overall rate of events was 18%. Two deaths were reported, 1 due to cardiovascular causes (sudden death 6 years after the SCAD) and the other due to non-cardiovascular causes (sepsis in the abdominal postoperative). Only 1 patient required a new revascularization due to restenosis of the stent implanted to treat the SCAD. Three out of the 4 patients (12%) with SCAD relapse had suffered events prior to the index event that were compatible with SCAD; that is, each one of them had presented with, at least, 3 events. Except for 1 recurrence at the 7-month follow-up, most events occurred more than 2 years after the index event (figure 2). Regarding pharmacological treatment, ASA was kept for a median 17 months [9-35] after the event and the second antiplatelet drug was withdrawn early in most of the patients. Of the patients who received conservative treatment, only 25% were still on dual antiplatelet therapy 6 months after the event (median 0 months [0-6]). In those patients who required PCI, dual antiplatelet therapy was keep for a median 5 months [1-7].
Table 4. Out-of-hospital disease progression and follow-up of the patients
| n = 33 | |
|---|---|
| Follow-up time (months) | 33 [13-49] |
| MACE | 6 (18) |
| Death | 2 (6) |
| New AMI | 3 (9) |
| Recurrence | 4 (12) |
| New revascularization | 1 (3) |
| Heart failure | 1 (3) |
| Stroke | 1 (3) |
| Time on ASA (months) | 17 [9-35] |
| Time on dual antiplatelet therapy (months) | |
| Conservative treatment group | 0 [0-6] |
| PCI group | 5 [1-7] |
| Control SCAD | n = 16 (48) |
| Coronary CT scan | 9 |
| Planned | 6 |
| Due to symptoms | 3 |
| Invasive coronary angiography | 11 |
| Planned | 3 |
| Due to symptoms | 8 |
| Screening of EVA | N = 32 (97) |
| Type of screening | |
| CT scan | 18 (56) |
| Angiography | 5 (16) |
| Angiography + CT scan | 9 (28) |
| Complete screening | 28 (88) |
| EVA data | 19 (59) |
| Type of EVA | |
| Fibromuscular dysplasia | 15 (47) |
| Aneurysm | 5 (15) |
| Other | 1 (3) |
| Location of EVA | |
| Renal arteries | 9 (28) |
| Iliac arteries | 7 (22) |
| Supra-aortic trunks | 5 (16) |
| Intracranial | 3 (9) |
| Other | 5 (16) |
|
AMI, acute myocardial infarction; ASA, acetylsalicylic acid; CT, computed tomography; EVA, extracoronary vascular abnormalities; MACE, major cardiovascular adverse events; PCI, percutaneous coronary intervention; SCAD, spontaneous coronary artery dissection. Data are expressed as no. (%) or mean ± standard deviation or median [interquartile range]. |
|
Angiography control was performed in 48% of the patients, in 9 of them using coronary CT scan and invasive coronary angiography in 11 patients. The coronary CT scan was performed in 3 patients in the context of a new episode of chest pain. After comparing it with the previous CT scan performed at the index event, the new SCAD was discarded (figure 3). However, most coronary angiographies were performed in the context of a new cardiac event; only 3 patients received a planned control coronary angiography. Out of the 16 patients on angiographic control, imaging improved with restitutio ad integrum in 75% of them. Six months after the SCAD, the documented rate of resolution rose to 86%.
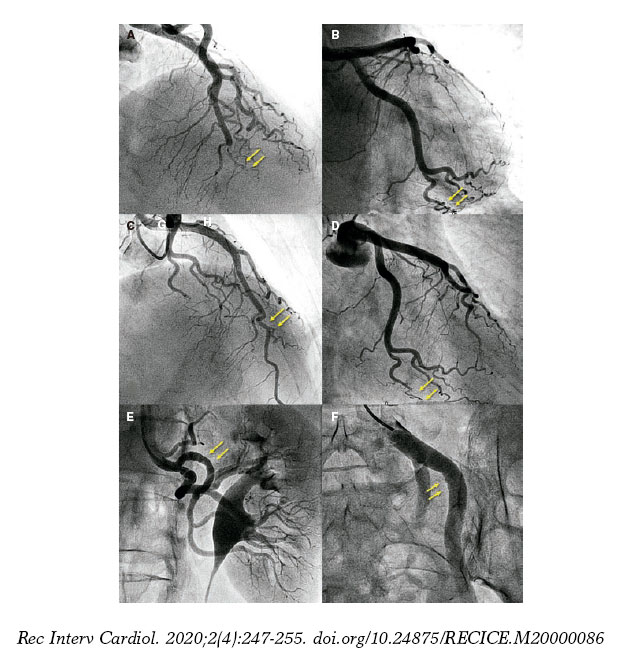
Figure 2. Fifty-five-year old woman with non-ST-elevation acute myocardial infarction (NSTEMI). She had experienced 2 previous acute myocardial infarctions with «normal coronary arteries» according to the coronary angiography. A: sudden caliber loss with tapering until the occlusion in the medial-distal portion of the left anterior descending coronary artery compatible with spontaneous coronary artery dissection (SCAD); conservative treatment. B: tortuous obtuse marginal artery without evident abnormalities. Two years later new hospitalization due to NSTEMI. C: caliber and flow recovery in the anterior descending coronary artery. D: obtuse marginal artery with sudden caliber loss and tapering (compare to B) compatible with SCAD; conservative treatment. E-F: selective angiographies of left renal and left iliac arteries with fibromuscular dysplasia.

Figure 3. Fifty-three-year old woman with non-ST-elevation acute myocardial infarction. After a tortuous segment, the sudden caliber loss of the left anterior descending coronary artery with vessel tapering can be seen (arrows) on the coronary angiography (A) and coronary computed tomography (CT) scan (B) compatible with a spontaneous coronary artery dissection (SCAD) at the medial-distal portion of the left anterior descending coronary artery. Four years later, the patient presents to the ER with prolonged chest pain without alterations on the ECG or high markers of myocardial damage. The coronary CT scan shows the coronary arteries without images indicative of SCAD. C: left anterior descending coronary artery. D: right coronary artery. E: circumflex artery.
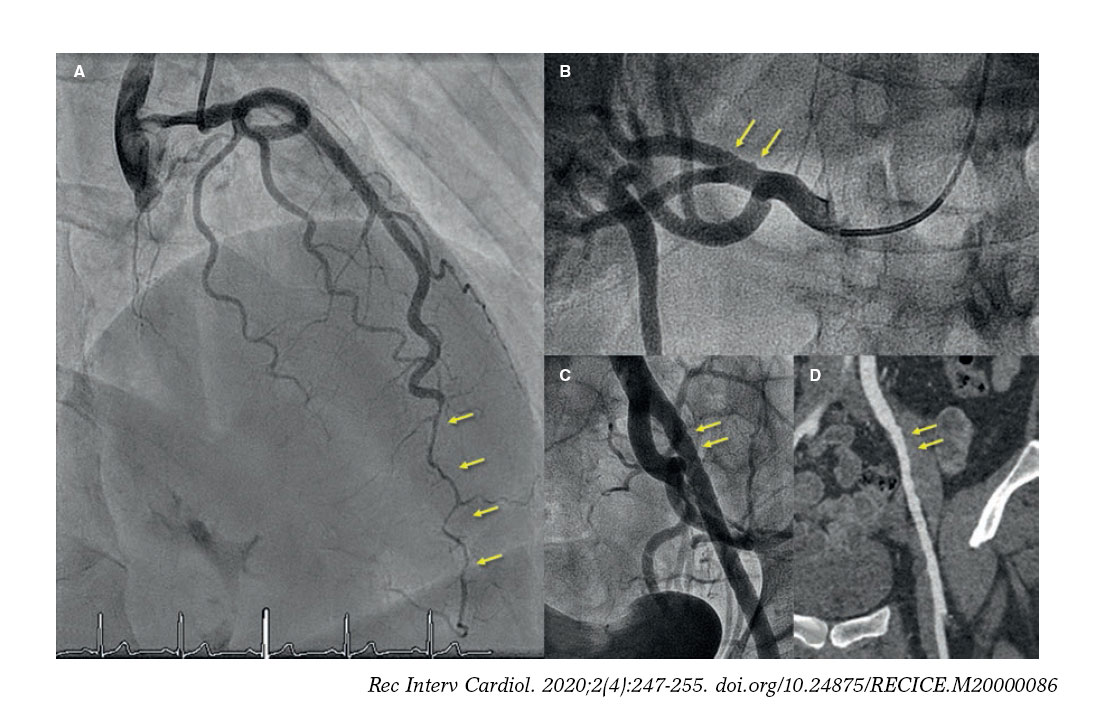
Figure 4. Forty-five-year old woman with non-ST-elevation acute myocardial infarction. The coronary angiography (A) shows a spontaneous coronary artery dissection at the medial-distal portion of the left anterior descending coronary artery (arrows). During catheterization the selective coronary angiography performed on the right renal (B) and left iliac arteries (C) shows wall irregularities compatibles with fibromuscular dysplasia (arrows). D: coronary computed tomography angiography at the follow-up with findings compatible with fibromuscular dysplasia on the left external iliac artery (arrows); note the greater sensitivity of coronary angiography (C) for the detection of subtle parietal abnormalities compared to coronary computed tomography angiography (D).
The screening of EVA was performed in 97% of the patients (full screening in 88%). Fifty-nine percent of the patients showed abnormalities that went up to 61% when the screening of EVA was complete. The abnormality most commonly found was FMD (47%) followed by arterial aneurysms (in 5 patients, 3 of which were intracranial aneurysms). The renal and iliac arteries were the most commonly compromised arteries of all: half of the patients studied showed abnormalities in either one of these arteries (examples in figure 2 and figure 4). After the study, the stroke team indicated the closure of the 3 intracranial aneurysms.
DISCUSSION
This study prospectively reports on the results of a current series of patients with SCAD with an updated and systematized diagnostic-therapeutic process and prolonged clinical follow-up. The clinical profile is consistent with what it is known about this disease:3,8,10 middle-aged woman with risk factors and low concomitance of chronic inflammatory disorders, autoimmune diseases or collagen diseases. Both the presentation and the angiographic characteristics were consistent with what has already been described: non-ST-elevation acute myocardial infarction that damaged the medial-distal segments and secondary branches predominantly with a higher incidence reported on the left anterior descending coronary artery. The most common Saw angiographic classification was type 2. Comparatively, in this series, the use of intracoronary imaging modalities was superior to other larger and recent series (42% vs 7.6% and 13% in the series of Saw et al.10 and Tweet et al.,8 respectively); this brings high reliability in the inequivocal diagnosis of SCAD. The most important conclusions of intracoronary imaging are: a) when OCT was the imaging modality used, the fenestration of both lumens could be identified in half of the lesions; b) the presence of mixed patterns (double lumen and intramural hematoma) within the same lesion is not an uncommon finding, which supports the evolutionary theory between both patterns; and c) lastly and probably the most important conclusion of all, intraluminal thrombi were not found in any of the lesions studied.
As it has already been described, an initial wait-and-see conservative approach with no interventions seems to bring good results to patients with SCAD.8,10,11 The rate of in-hospital MACE was low (15%). No deaths were reported, and bailout revascularizations were not necessary in any of the patients who received conservative treatment, except for 1 case due to iatrogenic dissection of left main coronary artery during the initial catheterization. Also, during the patients’ initial disease progression, they already showed preserved left ventricular ejection fraction. Similarly, out-of-hospital disease progression was good: 2 deaths were reported (1 due to non-cardiovascular causes) at the 2.7-year median follow-up, and 12% had a new episode of SCAD. These are similar data to those described in a Canadian series12 (10.4% at the 3.1-year median follow-up) and significantly lower to the rate of recurrence of 27% at the 2.3-years of median follow-up reported by Mayo Clinic.8
Unlike the atherosclerosis related ACS, in SCAD the ideal antithrombotic therapy has not been totally established. It seems logical to avoid aggressiveness, especially when 1 of the most plausible etiopathogenic theories is intraparietal bleeding of vasa vasorum as the initial event.13,14 Therefore, given the lack of intraluminal thrombus in a high percentage of patients studied with IVUS and OCT in this series a low-intensity antithrombotic therapy was used. ASA was kept for an average 1.5 years and the second antiplatelet drug was only indicated at hospital discharge in patients who required PCI and for the shortest period of time possible. The satisfactory disease progression reported with rates of out-of-hospital events consistent with those reported in other large series (from 10% to 20%)1 and the low rate of recurrence suggest that low-intensity antithrombotic therapy can be an excellent option for these patients.
There is very little information on the value of coronary CT scan during SCAD related hospitalizations. It was performed in 58% of patients from this series and SCAD was identified in three fourths of the cases. A more extensive analysis of these findings has been recently published by our group.15 The current study shows that this information was very useful in the follow-up of 3 patients to discard new episodes of SCAD and avoid the coronary angiography and associated risks for the patients (3.4% of iatrogenic dissections in patients with SCAD).16 However, in one fourth of the patients the SCAD could not be identified in the acute phase not even with the previous coronary angiography as guidance. Therefore, the value of coronary CT scan as an early diagnostic imaging modality is limited in this context.
Back in 2012 the association between SCAD and FMD17 was described for the first time, and later studies only not confirmed the high prevalence of this association but also of other EVA (aneurysms, dissections, and thrombosis).18-20 In the European consensus document recently published the screening of EVA is recommended in patients with SCAD.5 To our knowledge and up to this day this study shows the results of the most complete screening of FMD and other EVA. With a study in 97% of the patients—complete in 88%—the great presence of EVA (60%) confirms this interesting association. The need to conduct these studies may be put into question since most findings are associated with discrete and typical parietal abnormalities of FMD that do not lead necessarily to significant functional disorders. As a matter of fact, after the long follow-up of patients and despite the high prevalence of EVA, the extracardiac arterial events reported were only 1 stroke. However, there are 3 reasons to support the screening: a) in case of suspicious diagnosis, it may be the key to confirm the diagnosis of SCAD;21 b) knowing arterial parietal structural alterations can be useful for the diagnosis and treatment of future extracardiac events; and c) the finding of intracranial aneurysms is not negligible (9% in our series, but up to 14% in the Canadian series16) and it is relevant due to the risk of intracranial bleeding and secondary morbimortality. As a matter of fact, in 3 of our patients a percutaneous coronary intervention was indicated to seal the intracranial aneurysm.
Limitations
The main limitations of this study are the small size of the sample and the fact that it focused on a single center only. However, this study has a long follow-up with a unified treatment given the centralization of the patients.
CONCLUSIONS
In our center the centralization and protocolization of patients with SCAD systematized both treatment and the performance of additional tests. Intracoronary imaging allows us to confirm diagnosis in angiographically suspicious cases without showing any thrombi in the true lumen whatsoever. A low-intensity antithrombotic strategy with ASA only and for a limited period of time seems to give good results in the management of SCADs with conservative treatment. The high rate of spontaneous resolution of SCAD was confirmed in the 6-month images. Over half of the patients with SCADs show some EVA. Performing a coronary CT scan in the acute phase was useful, comparatively speaking, in new events and scheduled controls.
CONFLICTS OF INTEREST
F. Alfonso is an associate editor of REC: Interventional Cardiology; the editorial protocol of the journal was observed to guarantee an impartial manuscript handling.
WHAT IS KNOWN ABOUT THE TOPIC?
- SCAD is a rare disease more commonly regarded as the cause of ACS, especially in women.
- The pathophysiological substrate and prognosis are different from common atherosclerosis as well as the management recommended.
- To this day, the information on SCADs comes from many retrospective series since no randomized, controlled clinical trials have been conducted yet.
WHAT DOES THIS STUDY ADD?
- This was a prospective study with a fairly long follow-up that collected data on a specific diagnostic, therapeutic, centralized, and updated approach based on the new scientific evidence available on the management of SCAD.
- The study presented the results of an almost universal screening of ECA with a high percentage of patients with unequivocal diagnosis of SCAD (thanks to the common use of intravascular imaging modalities) and angiographic control during disease progression.
- Treatment with a very low-intensity antithrombotic strategy (antiplatelet therapy with ASA only and not indefinitely) is safe with excellent results during disease progression.
SUPPLEMENTARY DATA

Video 1. Bastante T. DOI: 10.24875/RECICE.M20000096
Video 2. Bastante T. DOI: 10.24875/RECICE.M20000096
Video 3. Bastante T. DOI: 10.24875/RECICE.M20000096
REFERENCES
1. Saw J, Mancini GBJ, Humphries KH. Contemporary Review on Spontaneous Coronary Artery Dissection. J Am Coll Cardiol. 2016;68:297-312.
2. Pretty H. Dissecting aneurysms of coronary artery in woman aged 42:rupture. BMJ. 1931;1:667.
3. Alfonso F, Bastante T. Spontaneous coronary artery dissection novel diagnostic insights from large series of patients. Circ Cardiovasc Interv. 2014;7:638-641.
4. Bastante T, Cuesta J, García-Guimaraes M, et al. Current management of spontaneous coronary artery dissection. Expert Rev Cardiovasc Ther. 2017;15:619-628.
5. Adlam D, Alfonso F, Maas A, et al. European Society of Cardiology, acute cardiovascular care association, SCAD study group:a position paper on spontaneous coronary artery dissection. Eur Heart J. 2018;39:3353-3368.
6. Hayes SN, Kim CESH, Saw J, et al. Spontaneous Coronary Artery Dissection:Current State of the Science:A Scientific Statement from the American Heart Association. Circulation. 2018;137:e523-e557.
7. Saw J. Coronary angiogram classification of spontaneous coronary artery dissection. Catheter Cardiovasc Interv. 2014;84:1115-1122.
8. Tweet MS, Eleid MF, Best PJM, et al. Spontaneous coronary artery dissection:Revascularization versus conservative therapy. Circ Cardiovasc Interv. 2014;7:777-786.
9. Liang JJ, Prasad M, Tweet MS, et al. A novel application of CT angiography to detect extracoronary vascular abnormalities in patients with spontaneous coronary artery dissection. J Cardiovasc Comput Tomogr. 2014;8:189-197.
10. Saw J, Starovoytov A, Humphries K, et al. Canadian spontaneous coronary artery dissection cohort study:in-hospital and 30-day outcomes. Eur Heart J. 2019;40:1188-1197.
11. Alfonso F, Paulo M, Lennie V, et al. Spontaneous coronary artery dissection:long-term follow-up of a large series of patients prospectively managed with a “conservative“ therapeutic strategy. JACC Cardiol Intv. 2012;5:1062-1070.
12. Saw J, Humphries K, Aymong E, et al. Spontaneous coronary artery dissection:Clinical outcomes and risk of recurrence. J Am Coll Cardiol. 2017;70:1148-1158.
13. Waterbury TM, Tweet MS, Hayes SN, et al. Early natural history of spontaneous coronary artery dissection. Circ Cardiovasc Interv. 2018;11:e006772.
14. Jackson R, Al-Hussaini A, Joseph S, et al. Spontaneous coronary artery dissection. Patophisiological insights from optical coherence tomography. JACC Cardiovasc Imaging. 2019;12:2475-2488.
15. Pozo-Osinalde E, García-Guimaraes M, Bastante T, et al. Characteristic findings of acute spontaneous coronary artery dissection by cardiac computed tomography. Coron Artery Dis. 2019. https://doi.org/10.1097/MCA.0000000000000819
16. Prakash R, Starovoytov A, Heydari M, et al. Catheter-Induced iatrogenic coronary artery dissection in patients with spontaneous coronary artery dissection. J Am Coll Cardiol Intv. 2016;9:1851-1852.
17. Saw J, Poulter R, Fung A, et al. Spontaneous coronary artery dissection in patients with fibromuscular dysplasia:a case series. Circ Cardiovasc Interv. 2012;5:134-137.
18. Saw J, Aymong E, Sedlak T, et al. Spontaneous coronary artery dissection:association with predisposing arteriopathies and precipitating stressors and cardiovascular outcomes. Circ Cardiovasc Interv. 2014;7:645-655.
19. Bastante T, Rivero F, Cuesta J, et al. Association of spontaneous coronary artery dissection with fibromuscular dysplasia. Rev Esp Cardiol. 2015;68:719-720.
20. Prasad M, Tweet MS, Hayes SN, et al. Prevalence of extracoronary vascular abnormalities and fibromuscular dysplasia in patients with spontaneous coronary artery dissection. Am J Cardiol. 2015;115:1672-1677.
21. Bastante T, García-Guimaraes M, Rivero F, et al. Isolated septal branch lesion as the only diagnostic clue for spontaneous coronary artery dissection. Coron Artery Dis. 2020;31:98-99.
ABSTRACT
Introduction and objectives: Chronic total coronary occlusion (CTO) is often a complex entity to deal with through a percutaneous coronary intervention, and the clinical benefits of successful recanalization still remain uncertain. Most registries feature data in limited time periods and do not reflect the impact that specific dedicated programs have on recanalization. Our study evaluates the results of a CTO program on a long-term period of time.
Methods: All patients’ CTOs treated with percutaneous coronary interventions at our center from 2002 through 2017 were prospectively included in the registry. The clinical, angiographic and procedural data were collected, and clinical follow-up was conducted. Three consecutive periods of time were considered for the analysis of temporal trends.
Results: Atotal of 424 CTOs (408 patients) were included. In 339 patients (80%) the procedure was successful. The rate of success increased over time, from 57% in 2002-2006 to 87% in 2012-2017 (P = .001). The most important independent predictor of procedural failure was lesion tortuosity. After a median follow-up of 39.7 months, the rates of major adverse cardiovascular events and cardiovascular mortality in success vs failed groups were 13.9% vs 24.7% (P = .015) and 3.6% vs 14.1% (P = .001), respectively. These were the independent predictors of cardiovascular mortality: chronic kidney disease, left anterior descending artery occlusion, and procedural failure.
Conclusions: Our series shows a high rate of success in CTO recanalization, which has increased over the last few years due to greater expertise and improved program-specific technical advances. Several angiographic and procedural variables have been identified as predictors of failure. Successful procedures, especially on the left anterior descendent coronary artery, were associated with lower rates of cardiovascular mortality.
Keywords: Chronic total coronary occlusion. Percutaneous coronary intervention. Ischemic heart disease.
RESUMEN
Introducción y objetivos: La oclusión total coronaria crónica (OTC) es generalmente compleja de abordar con intervencionismo percutáneo y el beneficio clínico de su recanalización sigue siendo incierto. La mayoría de los registros aportan datos limitados en el tiempo y no reflejan el impacto de un programa específico para su tratamiento. Nuestro estudio evalúa los resultados de un programa de OTC a largo plazo.
Métodos: Se incluyeron de forma prospectiva todos los pacientes tratados con un intento de revascularización percutánea de una OTC entre los años 2002 y 2017. Se obtuvieron datos clínicos, angiográficos, intraprocedimiento y del seguimiento. Se consideraron 3 periodos temporales consecutivos para el análisis.
Resultados: Se incluyeron 408 pacientes (424 OTC). La desobstrucción fue exitosa en 339 lesiones (80%). El éxito se incrementó con el tiempo, de un 57% en 2002-2006 a un 87% en 2012-2017 (p = 0,001). El predictor independiente más potente de procedimiento fallido fue la tortuosidad intralesional. Tras una mediana de seguimiento de 39,7 meses, las tasas de eventos adversos cardiacos mayores y de muerte cardiaca en los grupos de éxito y fracaso fueron del 13,9 frente al 24,7% (p = 0,015) y del 3,6 frente al 14,1% (p = 0,001), respectivamente. Los predictores independientes de mortalidad cardiaca fueron la insuficiencia renal crónica, la oclusión de la arteria descendente anterior y el fallo del procedimiento.
Conclusiones: Nuestra serie muestra unas tasas elevadas de éxito en la recanalización de una OTC, incrementada en los últimos años debido a la experiencia y al desarrollo técnico del programa. Se han identificado numerosas variables clínicas y angiográficas como predictoras de fallo del procedimiento. El éxito en el procedimiento, en especial en la arteria descendente anterior, se asoció con una menor mortalidad cardiaca.
Palabras clave: Oclusión total crónica. Intervención coronaria percutánea. Cardiopatía isquémica.
Abbreviations ACS: acute coronary syndrome. CABG: coronary artery bypass graft. CTO: chronic total coronary occlusion. LAD: left anterior descending coronary artery. MACE: major adverse cardiovascular events. PCI: percutaneous coronary intervention.
INTRODUCTION
Percutaneous coronary interventions (PCI) of chronic total coronary occlusions (CTO) represent up to 12% of all PCIs performed.1 The reason to perform the percutaneous recanalization of a CTO is to improve clinical symptoms which, ultimately, has potential survival benefits as suggested by some observational studies.2-4 However, the clinical benefits of successful recanalization remain undefined and to this day accepting that opening CTOs saves lives, despite the favorable consistent results from several contemporary registries, is still not supported by randomized clinical trials.5
Given the complexity of these procedures, a specific program with dedicated CTO-trained operators is encouraged. Also, most of the published registries and randomized clinical trials are performed in highly skilled centers and feature results in limited periods of time usually on specific devices, but not long-term results.2-5
We present the results of a specific PCI program for CTO lesions, starting with the introduction of drug-eluting stents from 2002 through 2017. The profile of patients and lesions, procedural data, results, and long-term clinical outcomes have been analyzed during the time frame of the program.
METHODS
This prospective registry conducted in a single center with an active PCI program for CTOs started back in 2002. It included 1 single operator who would progressively develop proper skills.
All consecutive patients treated of their CTOs, at least once, through percutaneous recanalization during the period 2002–2017 were included. Clinical data, angiographic characteristics, and procedural features were collected. The patients gave their informed consent and the study was approved by the local review board.
The indication for the recanalization of the CTO was the presence of angina, confirmation of ischemia through provocation tests or viable myocardium assessed through magnetic resonance imaging since 2004 when this diagnostic imaging modality became available at our center. No angiographic exclusion criteria were applied. Therefore, long occlusions, severely calcified lesions, and ostial locations were included if clinically indicated. Patients with an indication for coronary artery bypass graft (CABG) were excluded.
CTOs diagnosed in the setting of an ST-segment elevation acute coronary syndrome were scheduled for intervention that was performed at least 4 weeks after the index procedure. In cases of non-ST-segment elevation, CTOs were approached during the initial catheterization or in a subsequent staged procedure at the operator’s discretion. Also, in 28 out of the 101 cases of CTOs diagnosed in the context of an ACS, the ad-hoc desobstruction of the CTO was attempted.
Most CTOs were performed by the lead operator who focused their experience on trying to improve the rate of success for the benefit of the patient.
For the analysis of temporal trends regarding techniques and results, patients were classified into 3 consecutive periods of time: 2002-2006, 2007-2011, and 2012-2017. Also, the entire cohort was divided into 2 groups regarding success or failure in the recanalization of the CTO. Follow-up data were obtained from hospital records and the contact kept with the patients and the information provided were prospectively included in a database. No routine angiographic follow-up assessment was conducted.
Procedures were performed according to standard practices through the femoral or radial approach. Antithrombotic therapy consisted of unfractionated heparin (100 U/Kg) with additional administration when appropriate, to achieve activated clotting times of 250 seconds or 300 seconds using the antegrade and retrograde approaches, respectively. Aspirin 100 mg was administered orally prior to the PCI. Before stent implantation patients received perioperatively 300 mg to 600 mg of clopidogrel followed by a daily administration of 75 mg for the prescribed period of dual antiplatelet therapy.
CTOs were defined as coronary obstructions with TIMI flow grade 0 of at least 3 months duration.
Procedural success was defined as achieving residual post-PCI stenosis < 30% associated with TIMI flow 2–3.
Mortality was considered cardiovascular unless an evident non-cardiac cause was identified. Myocardial infarction was defined according to the Third Universal Definition established by the European Society of Cardiology and the American College of Cardio- logy Foundation. Target lesion revascularization was defined as a repeated PCI on the target lesion or CABG on the target vessel following ischemia-driven restenosis. Target vessel revascularization was defined as repeated PCI or CABG on any segments of the target vessel. Major adverse cardiovascular events (MACE) were defined as cardiovascular death, myocardial infarction or need for surgical or percutaneous target vessel revascularization. Stent thrombosis was defined according to the Academic Research Consortium criteria.
The angiographic characteristics expected to be predictive of procedural success were classified according to the recommendations proposed by the Euro-CTO club consensus document.6 The J-score was calculated for each lesion based on the length of the occlusion, morphology of the stump, calcification, tortuosity, and prior attempt to open the CTO.7
Continuous variables were expressed as mean ± standard deviation or median (interquartile range [IQR]), when appropriate. Categorical variables were expressed as percentages. The chi square test or Fisher’s exact test were used to compare the categorical variables. The Kolmogorov-Smirnov test was used to verify the normal distribution of continuous data. Continuous variables were compared according to their distributions using the Student t test or Mann-Whitney U test (success vs failed subgroups), and the ANOVA or Kruskal-Wallis test (comparison of 3 time periods). The estimates of cardiovascular death-and-MACE-free survival were shown by the Kaplan-Meier curves. Inter-groupt differences were assessed using the log-rank test. The logistic regression and Cox proportional hazard models were used to assess the independent contribution of variables to procedural success and mortality, respectively. Multivariate models included variables with P values < .2 in the univariate analysis. All statistical analyses were 2-tailed, and P values < .05 were considered statistically significant. The statistical analysis was performed using the statistical software package SPSS 15.0 (SPSS Inc., United States).
RESULTS
A total of 424 CTOs (408 patients) were included. In 339 patients (80%) procedural success was achieved. The number of procedures and the corresponding rate of success per period is shown on figure 1 .
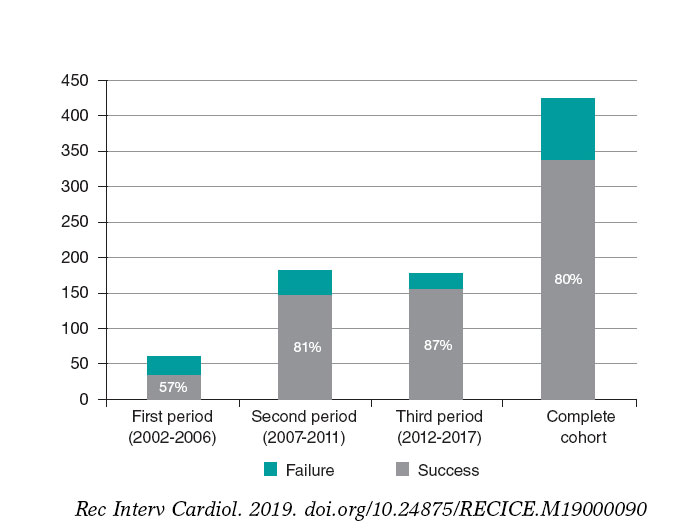
Figure 1. Number of procedures and corresponding rate of success per period.
The baseline characteristics regarding the success or failure of the CTO procedure are featured on table 1 and table 2. Previous CABG and the ACS setting were more common among failed cases. Patients with successful procedures were more prone to left anterior descending coronary artery (LAD) involvement, microchannels, and Rentrop grade 3 collateral blood flow. Procedural success was higher in the LAD compared to other target vessels (87% vs 77%; P = .02). Procedural success in the circumflex artery was the lowest of all (76%). The complexity of the CTO according to the J-score was higher in failed cases.
Table 1. Baseline characteristics
| All (n = 424) | Success (n = 339) | Failure (n = 85) | P | |
|---|---|---|---|---|
| Age | 63 ± 12 | 63 ± 12 | 64 ± 13 | .48 |
| Male sex | 350 (83%) | 277 (82%) | 73 (86%) | .37 |
| Hypertension | 279 (66%) | 217 (64%) | 62 (73%) | .15 |
| Diabetes Mellitus | 120 (28%) | 95 (28%) | 25 (29%) | .91 |
| Dyslipidemia | 275 (65%) | 222 (65%) | 53 (62%) | .45 |
| Past/current smoker | 292 (69%) | 236 (70%) | 56 (66%) | .48 |
| Previous infarction | 147 (35%) | 111 (33%) | 36 (42%) | .72 |
| Previous CABG | 31 (7%) | 18 (5%) | 13 (15%) | .002 |
| Multivessel disease | 297 (70%) | 234 (69%) | 63 (74%) | .38 |
| Left ventricular ejection fraction | 55 ± 13 | 55 ± 13 | 57 ± 13 | .17 |
| Serum creatinine (mg/dL) | 1.03 ± 0.53 | 1.02 ± 0.49 | 1.04 ± 0.64 | .76 |
| Acute coronary syndrome | 103 (24%) | 74 (22%) | 29 (34%) | .021 |
|
CABG, coronary artery bypass graft. |
||||
Table 2. Angiographic characteristics of occlusive lesions
| All (n = 424) | Success (n = 339) | Failure (n = 85) | P | |
|---|---|---|---|---|
| Left anterior descending coronary artery | 129 (30%) | 112 (33%) | 17 (20%) | .02 |
| Right coronary artery | 211 (50%) | 163 (48%) | 48 (56%) | .17 |
| Left circumflex artery | 81 (19%) | 62 (18%) | 19 (22%) | .39 |
| Diameter (mm) | 3.15 ± 0.45 | 3.15 ± 0.46 | 3.16 ± 0.58 | .97 |
| Length (mm) | 23 ± 16 | 21 ± 13 | 29 ± 21 | .001 |
| Moderate-to-severe calcification | 303 (74%) | 232 (72%) | 71 (84%) | .028 |
| Moderate-to-severe tortuosity | 150 (35%) | 95 (28%) | 55 (65%) | .001 |
| Severe distal disease | 122 (29%) | 91 (27%) | 31 (36%) | .14 |
| Tandem occlusions | 53 (13%) | 31 (9%) | 22 (26%) | .001 |
| Microchannels | 86 (20%) | 75 (22%) | 11 (13%) | .04 |
| Ostial/side branch location | 163 (38%) | 120 (35%) | 43 (51%) | .033 |
| Tapered stump | 208 (49%) | 171 (50%) | 37 (44%) | .12 |
| Rentrop grade 3 collateral flow | 206 (48%) | 171 (50%) | 35 (41%) | .09 |
| J score > 3 | 192 (45%) | 129 (38%) | 63 (74%) | .001 |
|
Data are expressed as no. (%) or mean ± standard deviation. |
||||
Procedural details are shown on table 3. The use of 8-Fr catheters and dual injections was significantly higher among successful cases with a strong trend towards retrograde approach and intravascular ultrasound guidance. Drug-eluting stents were deployed in most of cases and limus-eluting stents were the most widely used by far (79%). PCIs were performed on at least 1 additional vessel in about two-thirds of the patients from the 2 groups. Independent predictors of failure were previous CABG, moderate-to-severe lesion tortuosity, tandem occlusions, lack of dual injection, and CTOs diagnosed in the ACS setting (table 4).
Table 3. Procedural characteristics
| All (n = 424) | Success (n = 339) | Failure (n = 85) | P | |
|---|---|---|---|---|
| Femoral access | 265 (63%) | 215 (63%) | 50 (59%) | .39 |
| 8-Fr catheter | 207 (49%) | 175 (52%) | 32 (38%) | .03 |
| Dual injection | 367 (87%) | 302 (89%) | 65 (76%) | .02 |
| Intervention | ||||
| Drug-eluting stent | 294 (87%) | NA | ||
| Bare metal stent | 20 (6%) | NA | ||
| Drug-eluting and bare-metal stent | 15 (4%) | NA | ||
| Balloon | 10 (3%) | 1 (1.2%) | ||
| Retrograde approach | 94 (22%) | 69 (20%) | 25 (29%) | .07 |
| IVUS | 61 (14%) | 56 (17%) | 5 (6%) | .06 |
| Duration (min) | 105 ± 41 | 106 ± 42 | 102 ± 39 | .43 |
| Fluoroscopy dose (cGy/m²) | 26 037 ± 2066 | 26 403 ± 2222 | 24 867 ± 13 019 | .57 |
| Contrast volume (mL) | 367 ± 175 | 377 ± 177 | 327 ± 158 | .002 |
|
IVUS, intravascular ultrasound. |
||||
Table 4. Multivariate predictors
| Failed procedure | HR | HR | P |
|---|---|---|---|
| Previous CABG | 7.51 | 2.83-19.90 | .0001 |
| Moderate-to-severe tortuosity | 3.78 | 2.02-7.08 | .0001 |
| ACS setting | 2.42 | 1.26-4.61 | .008 |
| Tandem occlusion | 2.32 | 1.11-4.87 | .027 |
| Lack of dual injection | 2.43 | 1.14-5.55 | .027 |
| Cardiovascular mortality | HR | HR | P |
| Renal failure (< 60 mL/min) | 5.67 | 1.95-16.48 | .002 |
| LAD occlusion | 3.30 | 1.12-9.74 | .032 |
| Failed procedure | 7.14 | 2.44-20.0 | .0001 |
|
ACS, acute coronary syndrome; CABG, coronary artery bypass graft; LAD, left anterior descending coronary artery. |
|||
Twenty-six coronary dissections (6.2%) and 21 femoral hematomas (5%) were the most common procedural complications of all. In the course of the attempts, perforations occurred in 5 successful cases (1.5%) and in 9 failed cases (10.8%). However, emergent pericardiocentesis due to cardiac tamponade was required in 1 patient only. Contrast-induced nephropathy occurred in 8 successful cases (2.5%) and in 1 failed case (3.1%). One patient died during hospitalization due to cardiogenic shock that occurred 24 hours after a failed CTO attempt.
The differences seen among the 3 time periods led us to think that procedural technical advances, the operator’s increasing skills, and the improvements made in the assessment of the patients’ profile and selection of the lesions, contributed to the 87% rate of success reported at the final time frame. The temporal trends shown on table 5 describe the techniques developed in each corresponding period, not that all procedures were performed with that technique. Since June 2013 numerous cases have been successfully completed using the dissection/re-entry technique.The median follow-up was 39.7 months [22–102]. Follow-up information was available in 407 patients (99.8%). Clinical outcomes during follow-up are shown on table 6.
Table 5. Temporal trends in baseline angiographic characteristics, procedural data, and results
| 1st period (2002-2007) | 2nd period (2007-2011) | 3rd period (2011-2017) | Total | P | |
|---|---|---|---|---|---|
| Age | 62 ± 16 | 63 ± 11 | 64 ± 11 | 63 ± 12 | NS |
| Multivessel disease | 61.7% | 60.1% | 82% | 70% | .0001 |
| ACS setting | 36.1% | 21.8% | 23.6% | 24.3% | .025 |
| Previous CABG | 9.8% | 10.0% | 3.9% | 7.3% | .020 |
| LAD | 27.9% | 33.3% | 28.5% | 30.4% | NS |
| Length (mm) | 23 ± 14 | 22 ± 13 | 21 ± 18 | 23 ± 16 | NS |
| J score > 3 | 45.0% | 44.8% | 45.8% | 45.2% | NS |
| Rentrop grade 3 cc. | 44.8% | 62.8% | 39.4% | 48.6% | .0001 |
| Femoral access | 49.2% | 68.0% | 62.6% | 62.5% | .016 |
| 8-Fr catheter | 11.7% | 58.3% | 54.3% | 48.8% | .0001 |
| Dual injection | 65.0% | 90.1% | 92.1% | 86.5% | .0001 |
| Retrograde approach | 1.6% | 23.3% | 28.8% | 22.1% | .0001 |
| IVUS | 21.2% | 18.3% | 11.1% | 14.4% | .033 |
| Fluoroscopy time (cGy/m²) | 33245 | 30310 | 19830 | 26037 | .0001 |
| Contrast volume (mL) | 453 ± 208 | 434 ± 178 | 281 ± 127 | 367 ± 175 | .0001 |
| Success rate | 57% | 81% | 87% | 80% | .001 |
| More widely used wires | Polymer coated wires (Whisper ES or MS, Pilot 50, 150 or 200, Abbott Vascular, United States) and tapered, stiff wires (Confianza Pro 12, Asahi Intecc., Japan). Used in 58%. | Runthrough wire (Terumo, Japan) and nontapered, stiff wires (Miracle 3 or 6 and Ultimate Bross 3, Asahi Intecc., Japan). Used in 62%. | Runthrough and nontapered, stiff wires widely used (59%). Sion and Gaia wires (Asahi Intecc., Japan) were used in 21%. | ||
| Specific devices and techniques | Antegrade approach only. Parallel and seesaw wiring techniques. | Retrograde approach, Corsair specific catheter (Asahi Intecc., Japan) and Guideliner (Vascular Solutions, United States). Kissing and reverse CART techniques. | Double lumen Nhancer catheter (Interventional Medical Device Solutions, The Netherlands). Hybrid techniques with the CrossBoss and Styngray catheters (Boston Scientific, United States). | ||
|
ACS, acute coronary syndrome; CABG, coronary artery bypass graft; ES, extra support; IVUS, intravascular ultrasound; LAD, left anterior descending coronary artery; MS, medium support. |
|||||
Table 6. Clinical outcomes at follow-up
| All (n = 424) | Success (n = 339) | Failure (n = 85) | P | |
|---|---|---|---|---|
| Overall mortality | 64 (15.1%) | 40 (11.8%) | 24 (28.2%) | .001 |
| Cardiovascular mortality | 24 (5.7%) | 12 (3.6%) | 12 (14.1%) | .001 |
| Myocardial infarction | 10 (2.4%) | 8 (2.4%) | 2 (2.4%) | .99 |
| Target vessel revascularization | 45 (10.6%) | 34 (10.1%) | 11 (12.9%) | .44 |
| Target lesion revascularization | 40 (9.5%) | 31 (9.2%) | 9 (10.6%) | .69 |
| CTO stent thrombosis | ||||
| Definite | 5 (1.5%) | NA | ||
| Probable | 1 (0.3%) | NA | ||
| MACE | 68 (16.1%) | 47 (13.9%) | 21 (24.7%) | .0015 |
|
CTO, chronic total coronary occlusion; MACE, major adverse cardiovascular events (cardiovascular death, myocardial infarction or need for surgical or percutaneous target vessel revascularization). |
||||
In the success group, 33 restenosis (9.7%) were angiographically diagnosed, 42% of which ended up being occlusive. Target lesion revascularization was achieved in 31 of these restenotic lesions (9.2%). Four of the 5 cases of definite thrombosis corresponded to a successfully opened right coronary artery.
One case of severe radiodermatitis was identified and it was successfully treated with local surgery 6 years after the intervention.
A remarkable difference in MACE was observed in favor of the success group, mainly driven by a lower rate of cardiovascular mortality. The cumulative cardiac survival and MACE survival curves associated with the success or failure of the PCI are shown on figure 2 and figure 3.
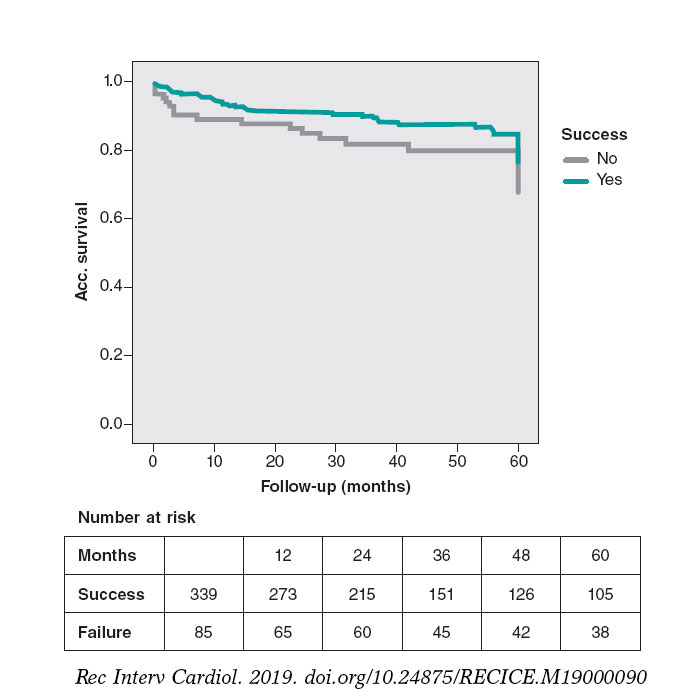
Figure 2. MACE-free at the 5-year follow-up. The rate of MACE (cardiovascular death, infarction, and surgical or percutaneous TVR) was lower in successful cases (P = .03).
MACE, major adverse cardiovascular events (cardiovascular death, myocardial infarction or need for surgical or percutaneous TVR); TVR, target vessel revascularization.
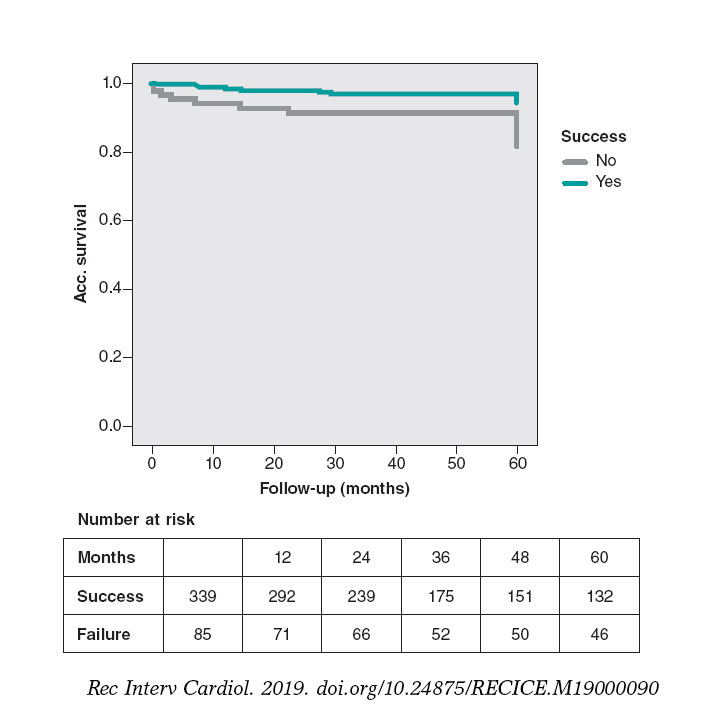
Figure 3. Cardiovascular mortality-free at the 5-year follow-up. Significant lower cardiovascular mortality in the success group (P = .005).
The multivariate analysis confirmed that a past medical history of chronic kidney disease with creatinine clearance < 60 mL/min, LAD occlusions, and procedural failure were independent predictors of cardiovascular mortality (table 4). Actually, increased mortality-related success rates were only seen in cases of failed LAD-CTO recanalization attempts compared to failed non-LAD CTO attempts (35% vs 9% P = .012).
DISCUSSION
These are the main results of this registry: a) the higher rates of success seen over the last 15 years confirm the improvements made in CTO recanalization devices and in the operator’s skills; b) the recanalization of CTOs shows high rates of success (80.0%) and low rates of complications; c) the rates of success were significantly lower in patients with previous CABG, moderate-to-severe lesion tortuosity, tandem occlusions, lack of dual injection, and patients with CTO treated in the ACS setting; d) successful procedures, especially in LAD occlusions, were associated with lower rates of cardiovascular mortality and MACE at the long-term follow-up.
The recanalization of the CTO is still uncertain and is not yet supported by randomized clinical trials. Several retrospective observational studies8-10 provide evidence that support this strategy. The results found in this analysis are consistent with previously published data, but disagree with others.11,12. In this sense, the more recent registries show better results regarding cardiovascular and overall mortality.13,14
Regarding randomized clinical trials, the EUROCTO trial revealed that the PCI of a CTO improves health status with improvements in angina frequency in patients with stable angina.15 However, the EXPLORE trial did not reveal any differences in the left ventricular function of patients with ST-segment elevation myocardial infarction. The DECISION-CTO showed similar inter-group rates of death, MI, stroke or TLR in patients with ACS or stable angina at the 3-year follow-up.16,17 The most recent clinical trial (REVASC) did not show an improved regional myocardial function. Although it was underpowered to measure clinical outcomes, it showed the advantage of performing the PCI of a CTO for clinically-driven repeat revascularization.18
Several characteristics of the current study should be emphasized to put the results into perspective. We believe this series of CTOs to be the big picture of interventional cardiology regarding CTOs since the start of the drug-eluting stent era until the arrival of contemporary new technologies. The study is based on a large cohort of consecutive patients from a single center. Most of them had multivessel disease and were treated in different time frames according to a specific dedicated CTO program.
Among the procedural characteristics that could explain the lower rates of success obtained with CTOs in the ACS setting we found the lowest use of retrograde approach and 8-Fr catheters in non-adequately staged procedures.
Regarding procedural features, the use of IVUS was limited to cases that required assessment of the distal vessel diameter and to optimize procedures with severe calcifications. It is very likely that more IVUS-guided procedures should have been performed.
Regarding variables related to procedural outcomes in the multivariable analysis, previous CABGs and more complicated CTOs were associated with failure as shown by other registries.13 However, intralesional tortuosity seems to us like the most consistent multivariable predictor with greater contribution to the model due to its narrow confidence interval. It might be possible that the inclusion of several angiographic variables in the regression model is responsible for the J-score not becoming an independent predictor. The high rate of retrograde procedures reveals the complexity of the CTOs in our series with J score > 3 in 45% of cases.
After dividing the series into 3 different periods of time, significant improvements in the rates of success were emphasized. As a result, we saw some interesting changes over time, such as the contribution of the retrograde approach to success. Considering that 73% of retrograde procedures were successful, it can be said that this technique led to a 19% increase in the rates of success in absolute terms. The rate of complications was quite similar to that from other studies.2-4,8-14
Our data provide additional evidence on the lower rate of cardiovascular mortality reported in patients with successful CTO recanalization in the long-term follow-up. As a matter of fact, the success of the PCI was a strong independent predictor of survival as several observational studies and 1 meta-analysis have consistently suggested.13,14,19
Possible explanations of the survival benefit from revascularizing a CTO may include a better left ventricular function and more tolerance for future acute coronary occlusive events.20 However, this cannot be confirmed as we didn’t measure the left ventricular ejection fraction systematically during follow-up. However, the trend showing a worst clinical profile in failed CTOs would validate this statement.
The role of LAD occlusions is decisive, as it seems an independent predictor of mortality. It should be mentioned that this effect of LAD occlusions on cardiovascular mortality was basically due to the higher mortality rate of failed cases compared to LAD recanalization attempts. The fact that LAD CTOs are much easier to open than CTOs located in other vessels makes LAD attempts not only feasible but also mandatory.
In conclusion, we think that this study —performed in a contemporary single cardiac catheterization laboratory for a long period of time practice in the drug eluting stent era— features new information on procedural results and long-term outcomes on CTO recanalizations.
This study was a prospective analysis and is subject to the limitations inherent to this type of research. The study does not allow us to draw any comparisons with other therapeutic strategies like medical therapy or CABG. Patients with failed procedures had different clinical and angiographic characteristics, which may have impacted prognosis.
Angiographic characteristics were not analyzed in a core lab but provided by a local investigator. There was no adjudication of clinical outcomes by a clinical events committee.
CONCLUSIONS
The implementation of a specific PCI program for CTOs has been associated with higher rates of success over time thanks to growing expertise and new technical advances. The rate of procedural success was lower when there was a history of previous CABG, moderate-to-severe lesion tortuosity, tandem occlusions, lack of dual injection, and in CTOs diagnosed in the ACS setting. Preserved renal function and successful recanalization —especially of the LAD— were associated with a lower rate of cardiovascular mortality in the long-term follow-up.
CONFLICTS OF INTEREST
J.M. de la Torre is the Editor-in-chief of REC: Interventional Cardiology; the editorial procedure established by REC: Publications was followed to guarantee the fair and unbiased handling of the manuscript.
WHAT IS KNOWN ABOUT THE TOPIC?
- CTOs are the most complex lesions to treat, and the prognostic benefit associated with their recanalization has not been properly established and if so, it could be selective.
- Most registries are limited in size and feature results in restricted time frames, often focused on specific devices, and not on long-term outcomes.
- The results of specific CTO programs in the long run have not been reported.
WHAT DOES THIS STUDY ADD?
- Our study describes the very long-term evolution of a PCI program for CTOs including the management and outcomes of PCI attempts on CTOs from 2002-2017.
- Our data, collected since the start of the drug-eluting stent era, confirm that implementing a program leads to higher rates of success over time. Independent predictors of PCI failure were identified in this large cohort.
- Lower rates of cardiovascular mortality were found in patients with successful recanalizations in the long-term follow-up.
- Also, the study provided new insights on the role played by LAD-CTO recanalizations on better outcomes.
REFERENCES
1. Anderson HV, Shaw RE, Brindis RG, et al. A contemporary overview of percutaneous coronary interventions. The American College of Cardiology-National Cardiovascular Data Registry (ACC-NCDR). J Am Coll Cardiol. 2002;39:1096-1103.
2. Suero JA, Marso SP, Jones PJ, et al. Procedural outcomes and long-term survival among patients undergoing percutaneous coronary intervention of chronic total occlusion in native coronary arteries:a 20-year experience. J Am Coll Cardiol. 2001;38:409-414.
3. Hoye A, van Domburg RT, Sonnenschein K, et al. Percutaneous coronary intervention for chronic total occlusions:the Thoraxcenter experience 1992-2002. Eur Heart J. 2005;26:2630-2636.
4. Noguchi T, Miyazaki S, Morii I, et al. Percutaneous transluminal coronary angioplasty of chronic total occlusions. Determinants of primary success and long-term clinical outcome.Cathet Cardiovasc Interv.2000;49:258-264.
5. Di Mario C, Sorini Dini C MD, Werner GS. Thousand Registries Are Not Worth a Randomized Trial. Also True for Chronic Total Occlusions?J Am Coll Cardiol Intv. 2017;10:1535-1537.
6. Di Mario C, Werner GS, Sianos G, et al. European perspective in the recanalisation of Chronic Total Occlusions:consensus document from the EuroCTO Club. Eurointervention. 2007;3:30-43.
7. Morino Y, Kimura T, Hayashi Y, et al. In-hospital outcomes of contemporary percutaneous coronary intervention in patients with chronic total occlusion insights from the J-CTO Registry (Multicenter CTO Registry in Japan). J Am Coll Cardiol Intv. 2010;3:143-151.
8. Olivari Z, Rubartelli P, Piscione F, et al.;TOAST-GISE Investigators. Immediate results and one-year clinical outcome after percutaneous coronary interventions in chronic total occlusions:data from a multicenter, prospective, observational study (TOAST-GISE). J Am Coll Cardiol. 2003;41:1672-1678.
9. Aziz S, Stables RH, Grayson AD, et al. Percutaneous coronary intervention for chronic total occlusions:improved survival for patients with successful revascularization compared to a failed procedure. Catheter Cardiovasc Interv. 2007;70:15-20.
10. Valenti R, Migliorini A, Signorini U, et al. Impact of complete revascularization with percutaneous coronary intervention on survival in patients with at least one chronic total occlusion. Eur Heart J. 2008;29:2336-2342.
11. Prasad A, Rihal CS, Lennon RJ, et al. Trends in outcomes after percutaneous coronary intervention for chronic total occlusions. A 25-year experience from the Mayo Clinic. J Am Coll Cardiol. 2007;49:1611-1618.
12. Labriolle A, Bonello B, Roy P, et al. Comparison of Safety, Efficacy, and Outcome of Successful Versus Unsuccessful Percutaneous Coronary Intervention in “True“Chronic Total Occlusions. Am J Cardiol.2008;102:1175-1181.
13. Borgia F,Viceconte N, Ali O, et al. Improved cardiac survival, freedom from MACE and angina-related quality of life after successful percutaneous recanalization of coronary artery chronic total occlusions. Int J Cardiol. 2012;161:31-38.
14. Tsai TT, Stanislawski MA, Shunk KA, et al. Contemporary Incidence, Management, and Long-Term Outcomes of Percutaneous Coronary Interventions for Chronic Coronary Artery Total Occlusions Insights From the VA CART Program. J Am Coll Cardiol Intv. 2017;10:866-875.
15. Werner GS. A Randomized Multicentre Trial to Evaluate the Utilization of Revascularization or Optimal Medical Therapy for the Treatment of Chronic Total Coronary Occlusions (EuroCTO) trial. Presented at;the PCR Congress Scientific Session 2017:Paris. Available online:https://www.pcronline.com/Cases-resources-images/Resources/Course-videos-slides/2017/Late-breaking-trials-and-trial-updates2?auth =true. Accessed 19 Dec 2019.
16. Park SJ. Drug-Eluting Stent Implantation Versus Optimal Medical Treatment in Patients With Chronic Total Occlusion (DECISION-CTO) trial. Presented at:the American College of Cardiology (ACC) 2017 Scientific Session. Washington, DC. Available online: http://www.acc.org/latest-in-cardiology/clinical-trials/2017/03/17/08/40/decision-cto. Accessed 19 Dec 2019.
17. Henriques JP, Hoebers LP, Råmunddal T, et al. :EXPLORE Trial Investigators. Percutaneous Intervention for Concurrent Chronic Total Occlusions in Patients With STEMI:The EXPLORE Trial. J Am Coll Cardiol.2016;68:1622-1632.
18. Mashayekhi K. REVASC:a randomized trial to assess recovery of left ventricular function after PCI of coronary artery chronic total occlusions. Presented at;TCT 2017. October 31, 2017:Denver, CO). Available online: https://www.tctmd.com/news/revasc-cto-pci-does-not-improve-lv-function-seems-provide-symptom-relief. Accessed 19 Dec 2019.
19. Khan MF, Wendel CS, Thai HM, et al. Effects of percutaneous revascularization of chronic total occlusions on clinical outcomes:a meta-analysis comparing successful versus failed percutaneous intervention for chronic total occlusion. Catheter Cardiovasc Interv. 2013;82:95-107.
20. Silva JC, Rochitte CE, Junior JS, et al. Late coronary artery recanalization effect on left ventricular remodelling and contractility by magnetic resonance imaging. Eur Heart J. 2005;26:36-43.
ABSTRACT
Introduction and objectives: Complex calcified lesions can affect stent expansion and lead to stent failure and adverse outcomes. Intracoronary lithotripsy (ICL) has emerged as a new tool that enables calcium modification. The Disrupt CAD II clinical trial has recently evaluated the safety and feasibility of ICL in patients with stable coronary disease and calcified coronary lesions. Although its use has increased rapidly, the experience already reported with this new device is limited. We report the results in real-life complex patients with heavy coronary calcification.
Methods: From October 2018 to March 2019, 25 patients (37 calcified lesions) were treated in 2 Spanish centers, which accounted for 2.7% of the patients treated with percutaneous coronary intervention.
Results: The device and clinical success rates were 84% and 95%, respectively. No procedure-related complications were seen. The crossing rate of the ICL balloon was 100% and balloon rupture during inflation occurred in 8%. The ICL was performed in a subset of highly complex lesions like left main coronary artery lesions and chronic total coronary occlusions. Compared to the Disrupt CAD II trial, our patients were younger but their clinical scenario was worse with a higher prevalence of diabetes (68%), renal failure (22%), and up to 76% suffered from acute coronary syndrome. The ICL failed to reach proper expansion in 3 out of 4 cases of stent underexpansion. The procedure was performed safely, and clinical and device success were high with no in-hospital mortality. One patient died of non-cardiac causes at the 30-day follow-up.
Conclusions: The ICL-assisted percutaneous coronary intervention was performed safely and effectively in a real-life cohort of patients with calcified and highly complex lesions.
Keywords: Lithotripsy. Calcium. Shockwave.
RESUMEN
Introducción y objetivos: Las lesiones coronarias calcificadas pueden impedir una correcta expansión del stent que en ocasiones conduce a eventos adversos. La litotricia intracoronaria es una nueva herramienta de modificación de la placa, cuyas seguridad y viabilidad en pacientes con enfermedad coronaria estable han sido evaluadas en el ensayo Disrupt CAD II. Aunque su uso ha aumentado rápidamente, hasta el momento solo se han comunicado casos aislados en escenarios concretos. Se presentan los resultados en pacientes clínicamente complejos de la vida real con calcificación coronaria grave.
Métodos: Entre octubre de 2018 y marzo de 2019 se trató a 25 pacientes (37 lesiones) en 2 centros españoles, lo que representa el 2,7% de los pacientes tratados con intervención coronaria percutánea.
Resultados: Las tasas de éxito clínico y del dispositivo fueron del 84 y el 95%, y no se observaron complicaciones relacionadas con el procedimiento. En todos los casos se consiguió cruzar la lesión con el balón de litotricia intracoronaria, si bien en el 8% de los casos se rompió el balón durante el inflado. Se trataron con éxito lesiones complejas, como oclusiones coronarias totales y estenosis del tronco común. En comparación con el estudio Disrupt CAD II, nuestros pacientes eran más jóvenes, pero tenían peor escenario clínico, con mayor prevalencia de diabetes (68%) e insuficiencia renal (22%), y hasta el 76% se presentó como síndrome coronario agudo. En 3 de 4 pacientes con infraexpansión de stent tratados con litotricia intracoronaria no se consiguió una expansión adecuada tras el procedimiento. No hubo complicaciones ni mortalidad hospitalaria. Un paciente falleció por causa no cardiaca a los 30 días de seguimiento.
Conclusiones: La litotricia intracoronaria se ha demostrado efectiva y segura en una cohorte de pacientes complejos de la vida real con lesiones calcificadas.
Palabras clave: Litotricia intracoronaria. Calcio. Ondas de choque.
Abreviaturas CTO: chronic total coronary occlusion. ICL: intracoronary lithotripsy. OCT: optical coherence tomography. PCI: percutaneous coronary intervention.
INTRODUCTION
Percutaneous coronary intervention (PCI) in calcified coronary lesions is often challenging and may be associated with suboptimal stent expansion and apposition both related to stent failure due to stent thrombosis and in-stent restenosis.1-3 The balloon angioplasty used in calcified lesions increases the risk of dissection of non-calcified segments usually without significant modification of calcified plaques and often without a proper luminal gain.4 The management of this subset of lesions is complex and often requires complex techniques such as rotational atherectomy or excimer laser coronary atherectomy.
Intracoronary lithotripsy (ICL) (Shockwave Medical, Freemont, CA, United States) has emerged as a new tool to modify calcium by applying a diffuse acoustic pulse through a balloon inflated at 4 to 6 atmospheres without damage to endovascular soft tissues. The multicenter, prospective, single-arm Disrupt CAD II clinical trial5 has recently evaluated the safety and feasibility of the ICL system prior to stent implantation in 120 patients with coronary artery disease and calcified coronary lesions. This study showed that the ICL appeared feasible with favorable initial success and complication rates in selected patients.5 Although its use has grown rapidly among interventional cardiologists and there are many case reports on the medical literature available to us, the experience already reported on this new device is quite limited. We present the initial results of lithotripsy-assisted PCIs in a real-life cohort of high-risk patients with complex, calcified lesions.
METHODS
Patient population and data collection
Two-center, prospective, observational registry including all consecutive PCI cases that required ICL prior to stent implantation to the operator’s discretion from October 2018 to March 2019. The baseline characteristics and procedural and in-hospital outcomes were prospectively recorded.
Intracoronary lithotripsy procedure
The ICL system is a portable and rechargeable generator connected to the ICL catheter. The catheter consists of a rapid exchange semi-compliant 12-mm balloon with 2 radiopaque emitters mounted inside available in 2.5, 3.0, 3.5, and 4 mm diameters. The catheter is compatible with a 6-Fr guiding catheter with a crossing profile range of 0.042 in and it is placed across the calcified lesion through a 0.014 in guidewire. Once in position, the balloon is inflated at 4 atmospheres to make intimate contact with the vessel wall and facilitate an efficient the transfer of energy. An electrical discharge from the emitters vaporizes the fluid inside the balloon generating sonic pressure waves that create a localized field effect. The ICL catheter is connected to a generator preprogrammed to deliver 10 pulses at a rate of 1 pulse per second. Each catheter can administer a maximum of 80 pulses. The sonic pulses through the soft vascular tissue cause selective microfractures at the intimal and medial calcium level of the vessel wall. After the pulse emission and the corresponding modification of calcium, the balloon is inflated up to 6 atmospheres to maximize luminal gain.
Definitions and outcomes
The use of the ICL catheter was based on the presence of a significant and severely calcified lesion (70% stenosis in an epicardial coronary vessel) on the angiography or intravascular imaging.
Coronary calcified lesions were defined by: a) the presence of radiopacities prior to contrast injection often involving both sides of the arterial wall; b) the presence of ≥ 270 degrees of calcium on at least one single cross-section on the intravascular ultrasound or optical coherence tomography (OCT); or c) subsets of calcified lesions with previous failed revascularization attempts.
According to the Disrupt CAD II trial criteria,5 lithotripsy delivery was considered successful when it facilitated stent delivery with < 50% residual stenosis and without any serious angiographic complications like severe dissection, perforation, slow flow or persistent no-reflow. In addition, clinical success was defined as residual stenosis < 50% after stenting without any evidence of in-hospital adverse events. We also assessed procedural complications such as PCI-related myocardial infarction (type 4a myocardial infarction, defined according to the fourth universal definition of myocardial infarction),6 and in-hospital and 30-day outcomes.
Statistical analysis
Categorical variables were expressed as number (percentage) and continuous variables as mean ± standard deviation or median according to their distribution. We analyzed all data using the STATA statistical package version 15.0 (StataCorp LP, College Station, Texas, United States).
RESULTS
Patients
Between October 2018 and March 2019, 25 patients with 37 calcified lesions were treated, which amounted to 2.7% of the patients treated with PCIs in both centers. The baseline characteristics of the patients are shown on table 1. Mean age was 71 ± 9 years and 68% of the patients were males. The traditional cardiovascular risk factors were common and the vast majority of patients had undergone a previous revascularization (PCI or coronary artery bypass graft). The indication for PCI was acute coronary syndrome in most cases (76%), all of them non–ST-elevation myocardial infarctions.
Table 1. Baseline characteristics (per patient)
| Clinical characteristics | N = 25 |
|---|---|
| Age, years | 71 ± 9 |
| Male sex | 17 (68) |
| Diabetes | 17 (68) |
| Renal failure | 7 (28) |
| Peripheral vascular disease | 8 (32) |
| Previous PCI | 14 (56) |
| Previous CABG | 3 (12) |
| LVEF | 49 ± 17 |
| ACS on admission | 19 (76) |
|
ACS, acute coronary syndrome; CABG, coronary artery bypass graft; LVEF, left ventricular ejection fraction; PCI, percutaneous coronary intervention. Data are expressed as no. (%) or mean ± standard deviation. |
|
Procedural characteristics
Procedural characteristics are shown on table 2. The mean SYNTAX score (Synergy between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery) was 19.3 ± 2, and the left anterior descending artery was the most-treated vessel. A non-negligible proportion of complex coronary artery lesions like chronic total coronary occlusions (CTO), bifurcation and ostial lesions, and stent underexpansion were also treated.
Table 2. Procedural characteristics
| Lesion characteristics | N = 37 |
|---|---|
| Protected LMCA | 1 (3) |
| Unprotected LMCA | 4 (11) |
| LAD | 17 (46) |
| LCx | 3 (8) |
| RCA | 12 (32) |
| Syntax Score | 19.3 ± 2 |
| Stent underexpansion treatment | 4 (11) |
| Ostial lesions | 13 (35) |
| Bifurcation lesion | 13 (35) |
| CTO | 3 (8) |
| Lesion severity by QCA | N = 37 |
| Pre-PCI diameter stenosis | 81.6 ± 2.5 |
| Post-PCI diameter stenosis | 15.9 ± 3.4 |
| Pre-PCI area stenosis | 84.6 ± 3.8 |
| Post-PCI area stenosis | 21.6 ± 3.5 |
| Total lesion length, mm | 20.7 ± 3 |
| Mean luminal diameter, mm | 0.77 ± 0.1 |
| Procedural characteristics | N = 25 |
| Radial access | 15 (60) |
| Mechanical support Impella device | 5 (20) |
| Fluoroscopy time, min | 31.5 ± 4.8 |
| Contrast, mL | 212 ± 28 |
| Number of vessels treated (per patient) | 1.3 ± 0.5 |
| Number of lesions treated (per patient) | 1.7 ± 0.8 |
| PCI characteristics | N = 37 |
| Pre-ICL balloon pre-dilatation | 23 (62) |
| Pre-ICL rotational atherectomy | 10 (27) |
| Pre-ICL cutting balloon | 2 (5) |
| ICL number of pulses | 46 ± 19 |
| ICL balloon rupture | 3 (8%) |
| Number of stents implanted | 1.2 ± 0.6 |
| Stent diameter, mm | 3.3 ± 1 |
| Stent length, mm | 23.1 ± 10 |
| Angiographical success | 35 (95) |
|
CTO, chronic total coronary occlusion; ICL, intracoronary lithotripsy; LAD, left anterior descending coronary artery; LCx, left circumflex artery; LMCA, left main coronary artery; PCI, percutaneous coronary intervention; QCA, quantitative coronary angiography; RCA, right coronary artery. Data are expressed as no. (%) or mean ± standard deviation. The ICL was used after a failed attempt of balloon pre-dilatation in 62% of the lesions, of which 10% showed balloon rupture. Ten lesions (27%) had previously been treated with rotational atherectomy. Only one lithotripsy catheter per lesion was required, and the mean number of pulses was 46 ± 19. The crossing rate of the lithotripsy balloon was 100% in pre-dilated and non-pre-dilated lesions, and the ICL balloon rupture occurred in 3 cases (8%) with no associated complications. An OCT prior to the ICL therapy was performed in a small percentage of cases (10%) to the operator’s discretion. All stents implanted were drug-eluting stents and successful angiographic result according to the definition was achieved in 95% of cases. |
|
Intracoronary lithotripsy in complex lesions
A subset of complex lesions was also treated with lithotripsy balloon (table 2). Success rate was 100% for left main coronary artery revascularizations, 100% for CTOs, and 86% for bifurcations.
Left main coronary artery lesions
Five patients with left main coronary artery lesions were treated with the ICL balloon. Four were unprotected lesions and were treated under hemodynamic support using the Impella device (all of them showed a severely depressed ejection fraction and/or a right coronary artery chronic total occlusion). Device and clinical success were achieved in all cases.
Bifurcation lesions
Seven lesions treated involved bifurcations, 4 were treated using a provisional stenting technique, and 3 cases were treated using the 2-stent technique (V stenting).
Chronic total coronary occlusions
The CTOs of 3 patients were treated using the ICL with complete success in all of them. The first patient had a severely calcified aorto-ostial lesion in the right coronary artery, a Japanese chronic total coronary occlusion score (Japanese Multicenter CTO Registry) of 2 (presence of calcification ≥ 20 mm in length). After unsuccessful pre-dilation using 2 balloons (1 of them ruptured) the ICL was performed and good balloon expansion was achieved without need for post-dilatation prior to the stenting. The second successfully treated CTO case involved the mid portion of the left anterior descending coronary artery (bifurcation according to the Medina classification 1,1,1), Japanese CTO score of 2 (calcification ≥ 20 mm in length) that had been treated with rotational atherectomy prior to the ICL. The third case was the CTO of a distal right coronary artery involving bifurcation (according to the Medina classification 1,0,0) and a Japanese CTO score of 3 (blunt-tip entry, calcification ≥ 20 mm in length). The artery was dilated using 5 balloons, some of which ruptured before performing the ICL. Lesion expansion was completed with a cutting balloon after the ICL, which allwed proper stent implantation.
Stent underexpansion
Four cases of stent underexpansion were treated, but results after the ICL were only successful in one case. There was 1 case that needed additional very high-pressure balloon dilatation (up to 40 atmospheres) for proper expansion, and 2 cases that remained unexpanded even after very high-pressure balloon dilatation (up to 40 atmospheres), and in-stent rotational atherectomy with 1.75 and 2.00 mm burrs.
In-hospital and 30-day outcomes
The procedure was performed safely in all cases. Both the clinical and device success were high with no in-hospital mortality. One patient died of non-cardiac causes at the 30-day follow-up (sepsis due to spontaneous bacterial peritonitis in the presence of hepatic cirrhosis). Procedural, in-hospital, and 30-day outcomes are shown on table 3.
Table 3. In-hospital and 30-day outcomes
| Clinical outcomes | N = 25 |
|---|---|
| Procedural complications | |
| Dissection | 0 (0) |
| Perforation | 0 (0) |
| No-reflow | 0 (0) |
| Type 4a acute myocardial infarction | 3 (12) |
| In-hospital mortality | 0 (0) |
| 30-d myocardial infarction | 0 (0) |
| 30-d target-vessel revascularization | 0 (0) |
| 30-d stent thrombosis | 0 (0) |
| 30-d mortality | 0 (0) |
| Cardiac death | 0 (0) |
| Non-cardiac death | 1 (4) |
|
Data are expressed as no. (%) or mean ± standard deviation. |
|
DISCUSSION
We present our initial experience with ICL in a cohort of real-life clinically complex patients with heavy coronary artery calcification and showed that the ICL is feasible with favorable initial outcomes and low complication rates.
Debulking techniques like rotational atherectomy, orbital atherectomy or excimer laser coronary atherectomy are commonly used to treat calcified coronary lesions. Back in 2018, in Spain up to 1517 patients were treated with rotational atherectomy and 88 with excimer laser coronary atherectomy.7 Recently, the ICL has emerged as an attractive option for the management of patients with severely calcified coronary lesions. Nevertheless, the experience reported on this new technique is still limited. The recently published single-arm Disrupt CAD II clinical trial confirmed the safety and performance of ICL to treat calcified coronary lesions.5 However, the clinical characteristics of the patients enrolled in this trial show a relatively low-risk population. Complex calcified coronary lesions are a common thing and they amount to 25% to 30% of all PCIs performed.3 Among our population, 2.7% of patients were considered eligible to receive ICL therapy, indicative of a highly demanding indication criterion. Compared to the Disrupt CAD II clinical trial5 our patients were younger but had a worse clinical scenario with a higher prevalence of diabetes (68% vs 32%) and renal failure (22% vs 9%), and up to 76% had suffered an acute coronary syndrome (none in the Disrupt CAD II trial). Another recent report described the initial experience with ICL in a cohort of 26 patients with calcified coronary lesions with findings for the clinical characteristics and results similar to the Disrupt CAD II.8
Regarding the procedure, it should be noted that the crossing rate for the ICL balloon was 100% despite a high percentage of plaque preparation was required (62% balloon pre-dilatation, 27% rotational atherectomy). Recently, the combination of rotational atherectomy and ICL has been described as RotaTripsy, suggestive that these 2 calcium debulking techniques may be complementary, since rotational atherectomy facilitates the ICL balloon crossing, and the latter facilitates proper expansion in the presence of circumferential deep calcium plaques.9 The device success rate was 84% (100% in the Disrupt CAD II linical trial) and the clinical success rate was 95% (94% in the Disrupt CAD II trial). And most important of all, no major procedural complications were seen, which is consistent with the Disrupt CAD II trial results. The rupture of the ICL balloon during inflation occurred in 3 cases (12%) without associated complications, yet the rupture of the balloon has been described in a case report resulting in a type C coronary dissection; the interventional cardiologist needs to be aware of this lithotripsy-related potential complication.10 Intravascular imaging were performed in few cases probably because the operator thought it would be difficult to cross an especially severe and calcified lesion with the OCT or IVUS catheter. Consistent with the results of the Disrupt CAD I and II clinical trials and OCT substudy,5,11 it was confirmed that the modification of calcium and the presence of fractures lead to an acute area gain and favorable stent expansion in the lesions assessed through OCT in our series. Figure 1 shows the coronary angiography and OCT of one complex patient treated with ICL; the red arrows seen on figure 1D,E indicate calcium fractures after the ICL.
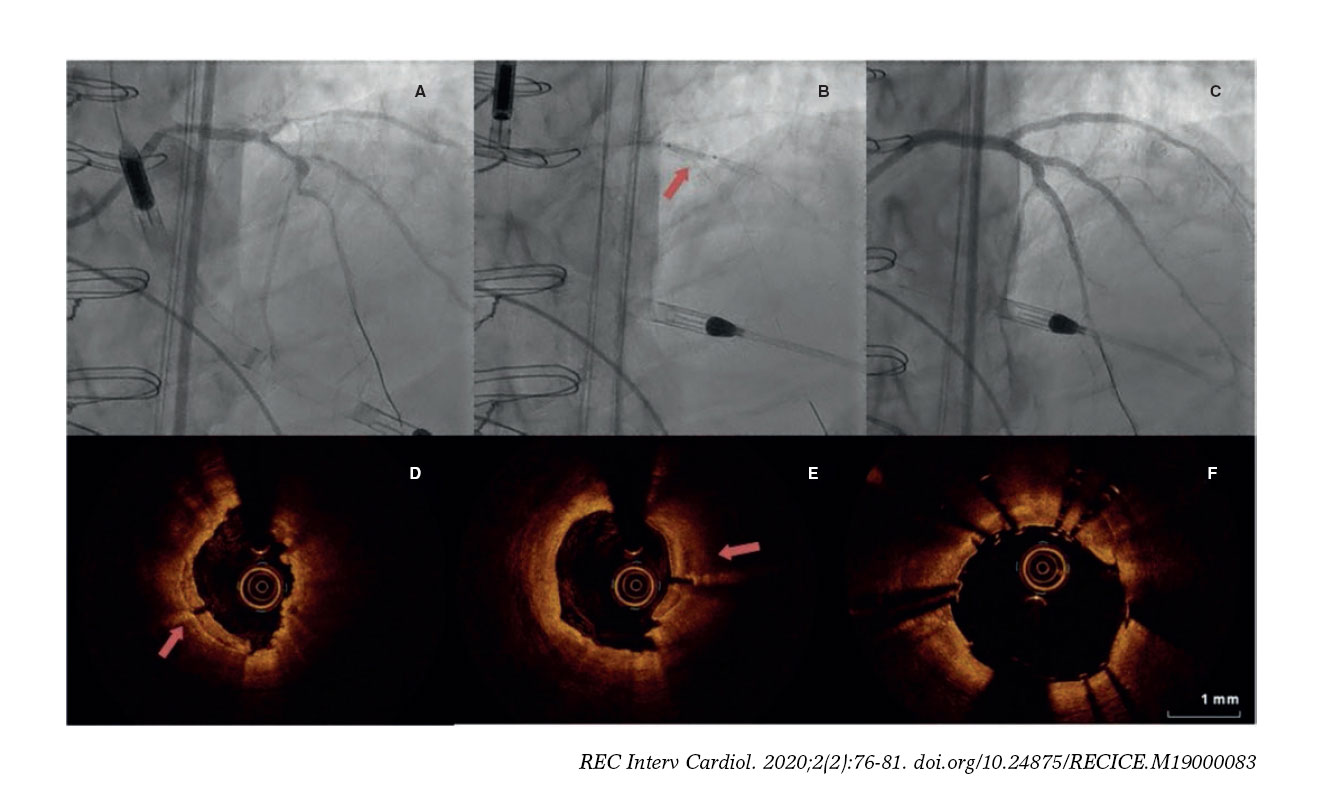
Figure 1. Intracoronary lithotripsy, angiography, and optical coherence tomography. Patient with severe coronary artery heart disease with severely depressed left ventricular ejection fraction previously treated with coronary artery bypass graft (venous graft-left anterior descending coronary artery, currently occluded). Treatment of left main coronary artery, left anterior descending artery, and diagonal branches. A: pre-intracoronary lithotripsy angiography. B: Impella-assisted PCI of left anterior descending coronary artery. Arrow indicates inflated lithotripsy balloon. C: successful final angiographic result after stenting. D, E and F: optical coherence tomography cross-sectional images of a post-lithotripsy calcified lesion. Red arrows indicate calcium microfractures after intracoronary lithotripsy.
We used the ICL in a subset of highly complex lesions like left main coronary artery stenosis, CTO, stent underexpansion, and bifurcation lesions.
Five complex patients with calcified left main coronary artery and severe stenosis were treated with ICL; mechanical support with the Impella device was needed in 4 patients due to a depressed left ventricular ejection fraction. Recently, a case report with 2 patients that were successfully treated with ICL in a left main coronary artery stenosis has also been published.12 The ICL seems like a safe treatment option to treat calcified left main coronary artery stenoses even in technically complex cases that require hemodynamic support, a clinical scenario where the use of rotational atherectomy or excimer laser coronary atherectomy is rare.
Three patients with CTO lesions were successfully treated with ICL. Treatment of CTO with ICL has been previously described in 2 case reports. The first one was a patient with a CTO in the proximal right coronary artery. In this case, the ICL allowed the reverse controlled antegrade/retrograde tracking at the location of heavy calcification at the site of the chronic occlusion.13 The second case was a patient with a proximal right coronary artery CTO due to heavily calcified in-stent restenosis. The ICL achieved good lesion expansion prior to stent implantation.14 If performed properly, the ICL can be an alternative to other debulking techniques in heavily calcified CTO lesions to guarantee proper lesion expansion.
Several case reports of stent underexpansion due to heavily calcified lesions successfully treated with ICL have been reported recently.15,16 Surprisingly, in our series the ICL failed to achieve proper stent expansion in 3 out of the 4 cases attempted. The management of stent underexpansion using ICL should be performed with extra caution because sound waves can damage the metallic structure of the stent.
The management of calcified bifurcation lesions is often complex due to the high risk of side branch occlusion when applying debulking techniques such as rotational atherectomy or excimer laser coronary atherectomy because the treatment cannot be performed using a guidewire for side branch protection purposes.17,18 The ICL allows us to treat the main branch bifurcation with a guidewire in the side branch to guarantee quick access in case of flow impairment just like conventional procedures do.
Compared to atherectomy or specialty balloons, the ICL is said to offer several potential advantages5 and requires no specific training as the device is delivered similar to the standard catheter-based PCI. ICL therapy is balloon based, and, therefore, the risk of atheromatous embolization may be lower compared to free debulking devices; according to the Disrupt CAD I (19) or Disrupt CAD II trial5 results, none of the patients from our series experienced no-reflow events and the rate of periprocedural myocardial infarction was relatively low. Whereas standard and specialty balloons are inflated at high atmospheric pressure to modify calcium, the ICL is typically performed at low atmospheric pressure balloon inflation, thus minimizing mechanical vascular trauma. Lastly, side-branch protection using a guidewire may be easily performed using ICL, without running the risk of wire entrapment or severing associated with rotational or orbital atherectomy. However, there is no evidence regarding stent restenosis of lesions treated with ICL therapy. New studies like the Disrupt CAD III trial that has just begun and will be recruiting up to 400 patients with a 2-year follow-up are needed to determine long-term outcomes.
Limitations
This 2-center experience using the ICL balloon has the limitations inherent to an observational study with a small sample size, which limits drawing conclusions especially in subgroups of high-risk lesions treated with ICL. However, in our opinion, it may contribute by adding more evidence supporting the use of ICL. This study did not have a comparison group either among existing plaque-modifying techniques.
CONCLUSIONS
In our own experience, the ICL-enhanced PCI was performed safely and effectively in a real-life cohort of complex patients with severely calcified and highly complex lesions.
CONFLICTS OF INTEREST
The authors of the manuscript declared no conflicts of interest.
WHAT IS KNOWN ABOUT THE TOPIC?
-
Calcified lesions continue to be a challenge for interventional cardiologists since poor plaque preparation prevents proper stent expansion, which leads to a higher rate of periprocedural complications and long-term adverse events.
-
The ICL balloon is a new plaque modification tool whose safety and efficacy in patients with stable coronary heart disease has recently been evaluated in a cohort of 120 patients in the Disrupt CAD II clinical trial.
-
The use of the ICL balloon has grown rapidly in the cardiac catheterization laboratories. However, to this day extensive series in real-life patients have not been reported yet.
WHAT DOES THIS STUDY ADD?
-
We present the results of the ICL balloon in real-life patients referred to undergo coronary angioplasty.
-
Although the size of the sample in our series was not big enough to draw any conclusions, the patients included were clinically complex and a high percentage of acute coronary syndromes and technically complex interventions (left main coronary artery lesions, bifurcation lesions, CTOs and stent underexpansion) was reported.
-
The procedure was performed safely and successfully in a large percentage of cases (95%). In-hospital mortality was zero and only one patient died at the 30-day follow-up (due to non-cardiac reasons).
REFERENCES
1. Bourantas CV, Zhang YJ, Garg S, et al. Prognostic implications of coronary calcification in patients with obstructive coronary artery disease treated by percutaneous coronary intervention:a patient-level pooled analysis of 7 contemporary stent trials. Heart. 2014;100:1158-1164.
2. Fitzgerald PJ, Ports TA, Yock PG. Contribution of localized calcium deposits to dissection after angioplasty. An observational study using intravascular ultrasound. Circulation. 1992;86:64-70.
3. Khattab AA, Otto A, Hochadel M, Toelg R, Geist V, Richardt G. Drug-eluting stents versus bare metal stents following rotational atherectomy for heavily calcified coronary lesions:late angiographic and clinical follow-up results. J Interv Cardiol. 2007;20:100-106.
4. Mehanna E, Bezerra HG, Prabhu D, et al. Volumetric characterization of human coronary calcification by frequency-domain optical coherence tomography. Circ J. 2013;77:2334-2340.
5. Ali ZA, Nef H, Escaned J, et al. Safety and effectiveness of coronary intravascular lithotripsy for treatment of severely calcified estenoses. The Disrupt CAD II Study. Circ Cardiovasc Interv. 2019;12:e008434.
6. Thygesen K, Alpert JS, Jaffe AF, et al. ESC Scientific Document Group;Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40:237-269.
7. Cid-Alvarez AB, Rodriguez-Leor O, Moreno R, Pérez de Prado A. Registro Español de Hemodinámica y Cardiología Intervencionista. XXVIII Informe Oficial de la Sección de Hemodinámica y Cardiología Intervencionista de la Sociedad Española de Cardiología (1990-2018). Rev Esp Cardiol. 2019. https://doi.org/10.1016/j.recesp.2019.07.023.
8. Wong B, El-Jack S, Newcombe R, Glenie T, Armstrong G, Khan A. Shockwave Intravascular Lithotripsy for Calcified Coronary Lesions:First Real-World Experience. J Invasive Cardiol. 2019;31:46-48.
9. Jurado-Román A, Gonzálvez A, Galeote G, Jiménez-Valero S, Moreno R. RotaTripsy:Combination of Rotational Atherectomy and Intravascular Lithotripsy for the Treatment of Severely Calcified Lesions. JACC Cardiovasc Interv. 2019;12:e127-e129.
10. López-Lluva MT, Jurado-Román A, Sánchez-Pérez I, Abellán-Huerta J, Lozano Ruíz-Poveda F. Shockwave:Useful But Potentially Dangerous. JACC Cardiovasc Interv. 2019;12:500-501.
11. Ali ZA, Brinton TJ, Hill JM, et al. Optical coherence tomography characterization of coronary lithoplasty for treatment of calcified lesions:first description. JACC Cardiovasc Imaging. 2017;10:897-906
12. Salazar CH, Travieso A, Gonzalo N, Escaned J. Intracoronary lithotripsy in percutaneous treatment of calcified left main coronary stenoses. JACC:Case Rep. 2019;1:46-49.
13. Yeoh J, Hill J, Spratt JC. Intravascular lithotripsy assisted chronic total occlusion revascularization with reverse controlled antegrade retrograde tracking. Catheter Cardiovasc Interv. 2019;93:1295-1297.
14. Azzalini L, Bellini B, Montorfano, Carlino M. Intravascular lithotripsy in chronic total occlusion percutaneous coronary intervention. EuroIntervention. 2019. https://doi.org/10.4244/EIJ-D-19-00175.
15. Ali ZA, McEntegart M, Hill JM, Spratt JC. Intravascular lithotripsy for treatment of stent under expansion secondary to severe coronary calcification. Eur Heart J. 2018. https://doi.org/10.1093/eurheartj/ehy747.
16. Watkins S, Good R, Hill J, Brinton TJ, Oldroyd KG. Intravascular lithotripsy to treat a severely under-expanded coronary stent. EuroIntervention. 2019;15:124-125.
17. Rawlins J, Din JN, Talwar S, O'Kane P. Coronary intervention with the Excimer Laser:review of the technology and outcome data. Interv Cardiol. 2016;11:27-32.
18. Nageh T, Kulkarni NM, Thomas MR. High-speed rotational atherectomy in the treatment of bifurcation-type coronary lesions. Cardiology. 2001;95:198-205.
19. Brinton TJ, Ali ZA, Hill JM, et al. Feasibility of shockwave coronary intravascular lithotripsy for the treatment of calcified coronary stenosis. Circulation. 2019;139:834-836.
Corresponding author: Departamento de Cardiología Intervencionista, Institut del Cor (ICOR), Hospital Germans Trias i Pujol, Ctra. de Canyet s/n, 08916 Badalona, Barcelona, Spain.
E-mail address: (O. Rodríguez-Leor).
- Prognostic impact of early coronary angiography in patients with non-ST-elevation acute myocardial infarction
- Functional assessment of intermediate lesions of collateral donor artery in chronic total coronary occlusions
- Procedural and clinical benefits of selective thrombus aspiration in primary PCI. Insights from the TAPER Registry
- Gender-related differences among patients with STEMI: a propensity score analysis







Interviews

An interview with Bruno Scheller
aServicio de Cardiología, Hospital Universitario de La Princesa, Instituto de Investigación Sanitaria de La Princesa (IIS-IP), Universidad Autónoma de Madrid, Spain
bCentro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain




