
Available online: 09/04/2019
Editorial
REC Interv Cardiol. 2020;2:310-312
The future of interventional cardiology
El futuro de la cardiología intervencionista
Emory University School of Medicine, Atlanta, Georgia, United States
Blood pressure indices like fractional flow reserve (FFR) and the instantaneous wave-free ratio (iFR) measure the distal-to-aortic pressure ratio of a lesion in a similar way using a pressure guidewire. FFR requires the induction of maximal hyperemia while the iFR is an index based on the assessment of pressure curves at rest. There is solid confirmation of the validity and efficacy of such indices from multiple studies while their use is widely backed by the clinical practice guidelines.1
However, the efficacy of blood pressure indices is based on 2 fundamental objectives. The first one is to prove that they are useful to indicate the revascularization of a lesion when the resulting value is below the cut-off point (≤ 0.80 for the FFR, and ≤ 0.89 for the iFR). The second one is to demonstrate that lesions with values above the cut-off point (> 0.80 or > 0.89, respectively) have a low risk of requiring revascularization, and lack of ischemic events at follow-up. Conceptually, the first indication is clear: a lesion with pathological values is an obstructive lesion that causes ischemia now. Therefore, if clinically indicated (and technically feasible) the best thing to do is to revascularize such a lesion. The second indication has a higher degree of uncertainty because a lesion that does not cause ischemia (now) does not necessarily mean that it will not cause it at some point in the future. This is so because the capacity of blood pressure indices (with normal results) to detect vulnerable plaques is limited, and they show a greater tendency towards progression or destabilization. Therefore, the negative predictive value of pressure indices is supposed to be worse when used in patients with a higher risk of progression into atherosclerotic cardiovascular disease.
Proof of this is that recent studies conducted in patients with acute myocardial infarction (AMI) and multivessel disease have demonstrated that the FFR of non-culprit lesions does not provide any clinical benefits regarding the revascularization of such lesions estimated visually and, therefore, under angiographic guidance.2,3 The prevalence of vulnerable plaques causing visual stenosis between 50% and 69% in non-culprit vessels of patients with AMI is estimated at around 30%. Actually this rate is probably higher when lesions with a greater degree of angiographic obstruction are studied.4 The COMBINE OCT-FFR trial also reported a similar rate of vulnerable plaques (25%) on the optical coherence tomography performed in diabetic patients with angiographic stenoses between 40% and 80% and normal FFR values.5 In this study, angiographic lesions with normal FFR values associated with vulnerable plaques had more adverse events (cardiac death, target vessel myocardial infarction, and clinically driven target lesion revascularization) compared to those not associated with vulnerable plaques (13% vs 3%; P < .001).
The article by Castro-Mejía et al.6 recently published in REC: Interventional Cardiology provides the mid-term follow-up (3.5 years) of a large single-center registry of patients with intermediate angiographic lesions assessed using blood pressure indices and with normal results. This study compared the adverse events between diabetic and nondiabetic patients with the necessary statistical adjustments to compensate for the inherent differences of the baseline characteristics of both groups. The authors conclude that blood pressure indices (FFR and iFR) had a similar efficacy in diabetic and nondiabetic patients for not predicting future target vessel myocardial infarctions or the need for target lesion revascularization. However, we should mention that diabetic patients had higher rates of all-cause mortality, AMI, and need for revascularization compared to nondiabetic patients.6 We should specifically mention that there was a 2.6-fold higher risk of infarction in any vessels at the follow-up in diabetic compared to nondiabetic patients (P < .063 after adjustments). However, only 13% of the AMIs registered were adjudicated to the study vessel in diabetic vs 38% in nondiabetic patients.6 This difference can be due to chance alone or to the fact that the lesions that cause AMIs at the follow-up are scarcely susceptible to be studied with a pressure guidewire at the index procedure in diabetic patients. It is well known that these patients have more diffuse atherosclerotic cardiovascular disease, which complicates the correct angiographic assessment of the lesions (and, also, prevents the use of a pressure guidewire in such vessel for assessment purposes). It is highly likely that a strategy based on intravascular imaging modalities alone or in combination like in the COMBINE OCT-FFR trial can be of greater utility to detect this type of lesions.
Three recent studies have reported contradictory outcomes regarding the negative predictive value of blood pressure indices in diabetic patients. Kennedy et al.7 found more AMIs and a greater need for target lesion revascularization with normal FFR values in diabetic patients at the 3-year follow-up. On the contrary, Van Belle et al.8 found no differences between diabetic and nondiabetic patients who were deferred (for having normal FFR values) in 2 large registries conducted in Portugal, and France at the 1-year follow-up. No significant differences were seen either in the DEFINE-FLAIR substudy that analyzed adverse events between diabetic and nondiabetic patients in deferred patients at 1-year follow-up.9 It should be interesting to assess the long-term follow-up of these last 2 studies to see if the negative predictive value of blood pressure indices stays the same in diabetic and nondiabetic patients.
Finally, Castro-Mejía et al.6 propose that resting physiological indices with nonpathological findings may have a better negative predictive value compared to the FFR values of diabetic patients. This would be explained by the fact that one of the causes of discrepancy between the FFR and the iFR is microvascular dysfunction (that is more common in diabetic patients). Patients with microvascular dysfunction can have smaller drops of the pressure index during maximal hyperemia since not enough hyperemia is induced. However, resting physiological indices are not hyperemia-dependent, meaning that they should be more sensitive to detect significant epicardial lesions. However, this hypothesis was not confirmed by the DEFINE-FLAIR substudy on deferred diabetic patients.9
In conclusion, diabetic patients still remain as one of the challenges of interventional cardiology because they have more adverse events compared to nondiabetic patients (despite the proper optimal medical therapy). A more aggressive strategy to assess intermediate coronary lesions using pressure guidewires is advisable to guide complete revascularization in diabetic patients. Future studies should also assess whether a mixed strategy with intravascular imaging modalities of nonfunctionally significant arteries can be useful to prevent future events in this group of patients.
FUNDING
None whatsoever.
CONFLICTS OF INTEREST
J. Gómez-Lara has received speaking fees for presentations on behalf of Abbott Vascular, Boston Scientific, and Terumo. R. Romaguera declared no conflicts of interests whatsoever.
REFERENCES
1. Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41:407-477.
2. Puymirat E, Cayla G, Simon T, et al. Multivessel PCI Guided by FFR or Angiography for Myocardial Infarction. N Engl J Med. 2021;385:297-308.
3. Denormandie P, Simon T, Cayla G, et al. Compared Outcomes of ST-Elevation Myocardial Infarction Patients with Multivessel Disease Treated with Primary Percutaneous Coronary Intervention and Preserved Fractional Flow Reserve of Non-Culprit Lesions Treated Conservatively and of Those with Low Fractional Flow Reserve Managed Invasively:Insights from the FLOWER MI trial. Circ Cardiovasc Interv. 2021. https://doi.org/10.1161/CIRCINTERVENTIONS.121.011314.
4. Pinilla-Echeverri N, Mehta SR, Wang J, et al. Nonculprit Lesion Plaque Morphology in Patients With ST-Segment-Elevation Myocardial Infarction:Results From the COMPLETE Trial Optical Coherence Tomography Substudys. Circ Cardiovasc Interv. 2020;13:e00≀.
5. Kedhi E, Berta B, Roleder T, et al. Thin-cap fibroatheroma predicts clinical events in diabetic patients with normal fractional flow reserve:the COMBINE OCT-FFR trial. Eur Heart J. 2021;42(45):4671-4679.
6. Castro-Mejía AF, Travieso-González A, Núñez-Gil IJ, et al. Diabetes mellitus and long-term safety of FFR and iFR-based coronary revascularization deferral. REC Interv Cardiol. 2022;4(2):99-106.
7. Kennedy MW, Kaplan E, Hermanides RS, et al. Clinical outcomes of deferred revascularisation using fractional flow reserve in patients with and without diabetes mellitus. Cardiovasc Diabetol. 2016;15:100.
8. Van Belle E, Cosenza A, Baptista SB, et al. Usefulness of Routine Fractional Flow Reserve for Clinical Management of Coronary Artery Disease in Patients With Diabetes. JAMA Cardiol. 2020;5:272-281.
9. DEFINE-FLAIR Trial Investigators, Lee JM, Choi KH, et al. Comparison of Major Adverse Cardiac Events Between Instantaneous Wave-Free Ratio and Fractional Flow Reserve-Guided Strategy in Patients With or Without Type 2 Diabetes:A Secondary Analysis of a Randomized Clinical Trial. JAMA Cardiol. 2019;4:857-864.
The use of drug-eluting stents (DES) for the treatment of coronary artery stenosis substantially reduced the need for repeat revascularization compared to bare-metal stents.1 However, as many patients undergoing stenting have long life expectancy, and the incidence rate of stent failure increases with time since implantation, the number of patients presenting with DES restenosis is not insignificant and the treatment of these patients remains a challenge.2
Current clinical practice guidelines recommend treatment of restenosis associated with angina or ischemia by repeat revascularization with either repeat stenting with DES or angioplasty with drug coated balloon (DCB).3 Certain situations favour repeat stenting with DES, most notably loss of mechanical integrity of the restenosed stent. In general, however, although repeat stenting with DES may be more effective than angioplasty with DCB in the short-to-medium-term,4 avoidance of additional stent layers is an important consideration in the longer-term. Indeed, many centres prefer DCB angioplasty as a first-line approach for the treatment of restenosis in the absence of a compelling indication for repeat stenting.
The efficacy of DCB treatment relies on rapid transfer and subsequent tissue retention of the anti-proliferative agent, which is necessary for a persistent suppression of cell proliferation.5 Preclinical data suggest that micro-injuries to the vessel wall may enhance the ability of DCBs to inhibit neointimal growth.6 These micro-injuries can be achieved with a number of different types of modified balloon catheters, such as cutting or scoring balloons. Cutting balloon angioplasty is an attractive option thanks to its ability to effectively incise neointimal tissue and its ease of use.7 Scoring balloons are based on the same principle and may offer superior flexibility and deliverability at the expense of a somehow lower plaque disruption.
In a recent paper published in REC: Interventional Cardiology, Linares Vicente et al. reported on the 5-year results of cutting or scoring balloon angioplasty combined with DCB to treat in-stent restenosis.8 A total of 51 lesions (42 patients) were treated with cutting balloons plus DCBs, and 56 lesions (49 patients) with a standard DCB angioplasty. Both the SeQuent Please (B. Braun Melsungen AG, Germany), and the Pantera Lux (Biotronik, Switzerland) balloons were used. The primary endpoint was clinically driven target lesion revascularization at 5 years. It appears that, compared to the standard DCB strategy, the use of cutting or scoring balloons considerably reduced the 5-year rate of target lesion revascularization, although this difference was not statistically significant (9.8% vs 23.6%; odds ratio = 0.36; 95% confidence interval, 0.19-1.09; P = .05) (figure 1).
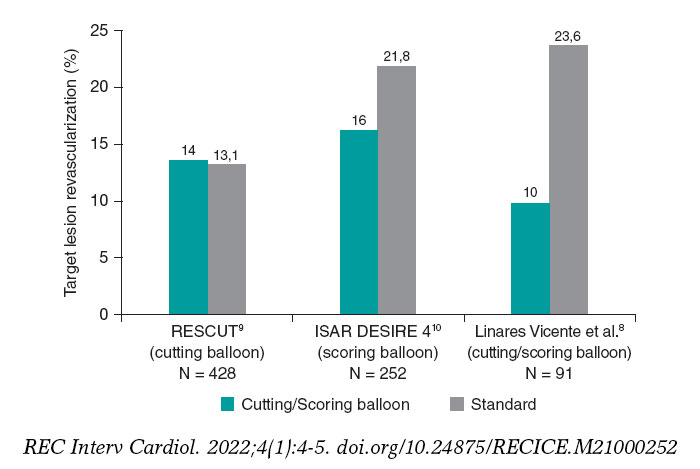
Figure 1. Target lesion revascularization (%): studies comparing cutting balloon/scoring balloon vs standard therapy in patients treated with percutaneous intervention for in-stent restenosis.
The study was retrospective and conducted at a single center with a small sample size of 91 patients. However, it is representative of real-world evidence, which may reflect clinical experiences across a broader and more diverse population of patients than those enrolled in randomized controlled trials. Regarding the baseline characteristics, almost 85% of patients were men with a mean age of 68.3 years. Patients had a high prevalence of diabetes mellitus and smoking (36% and 59%, respectively).
Interestingly, despite the current recommendations of the European Society of Cardiology,3 the use of intravascular ultrasound or optical coherence tomography was relatively low (5.9% in the cutting balloon group, and 8.9% in the standard group). Although this is consistent with rates observed in surveys of use in the clinical practice,11 it represents a missed opportunity for the mechanistic understanding of the disease etiology, and guidance for treatment optimization.12
The primary endpoint was the need for clinically driven target lesion revascularization at 5 years, which was 64% lower with cutting or scoring balloon angioplasty. Given the small sample size of this study and the relatively large treatment effect, it is a pity that insights from the angiographic follow-up were not available. Concordant data from systematic surveillance angiography would have given more confidence to the robustness of the observed treatment effect.
The results of this study should be interpreted in the context of earlier randomized controlled trials with cutting or scoring balloon angioplasty. In fact, evidence from such trials is scant including the RESCUT (Restenosis cutting balloon evaluation trial) trial9 published in 2003, and the more recent ISAR DESIRE 4 (Intracoronary stenting and angiographic results: optimizing treatment of drug-eluting stent in-stent restenosis 4) trial.10
In RESCUT, Albiero et al. randomized 428 patients with bare-metal stent in-stent restenosis across 23 European centers to receive either cutting balloon angioplasty or conventional balloon angioplasty.9 Overall, the trial showed neutral results: at late follow-up, the angiographic restenosis rate, minimal lumen diameter, and the rate of clinical events were similar in both arms (figure 1). Cutting balloon angioplasty, however, was associated with some important procedural advantages, such as use of fewer balloons, less requirement for additional stenting, and a significantly lower incidence of balloon slippage (6.5% vs 25%).
ISAR DESIRE 4 was a randomized, open-label, assessor-blinded trial that enrolled 252 patients with clinically significant DES restenosis undergoing DCB angioplasty at 4 different centres in Germany.10 This trial investigated scoring balloon rather than cutting balloon angioplasty. The primary endpoint–diameter stenosis at the 6-8-month follow-up angiography–was lower for the scoring balloon compared to the regular balloon angioplasty: 35% vs 40.4%; P = .047; in addition, target lesion revascularization was numerically lower (figure 1). Although, the size of treatment effect was modest, small incremental gains in efficacy in this challenging patient subset may translate into important clinical benefits.
Against this background, the observations made by Linares Vicente et al.8 are an important addition to the evidence supporting the clinical use of cutting or scoring balloons to treat stent failure. While repeat stenting with DES or angioplasty with DCB are the mainstay of in-stent restenosis procedures, the procedural efficiency and clinical efficacy of both approaches will likely improve with the adjunctive use of cutting or scoring balloons. The benefits of these devices are most likely mediated by a combination of factors: reduced balloon slippage (or watermelon-seeding), the mechanical advantage of increased disruption of restenotic tissue, and the potential for enhanced efficacy of the device-delivered drug. The management of patients with stent failure remains challenging and deserves the best treatment the operator can offer including the liberal use of cutting or scoring balloon lesion preparation. In this clinical setting, small margins can make a big difference.
FUNDING
L. McGovern is funded by the European Commission under the Horizons 2020 framework (grant agreement number 965246 CORE-MD).
CONFLICTS OF INTEREST
R.A. Byrne declared research or educational funding in the institution he currently works at from Abbott Vascular, Biosensors, Biotronik, and Boston Scientific. L. McGovern declared no conflicts of interest whatsoever.
REFERENCES
1. Cassese S, Byrne RA, Tada T, et al. Incidence and predictors of restenosis after coronary stenting in 10 004 patients with surveillance angiography. Heart. 2014;100:153-159.
2. Cutlip DE, Chhabra AG, Baim DS, et al. Beyond Restenosis. Circulation. 2004;110:1226-1230.
3. Neumann F-J, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2018;40:87-165.
4. Giacoppo D, Alfonso F, Xu B, et al. Paclitaxel-coated balloon angioplasty vs. drug-eluting stenting for the treatment of coronary in-stent restenosis:a comprehensive, collaborative, individual patient data meta-analysis of 10 randomized clinical trials (DAEDALUS study). Eur Heart J. 2020;41:3715-3728.
5. Byrne RA, Joner M, Alfonso F, Kastrati A. Drug-coated balloon therapy in coronary and peripheral artery disease. Nat Rev Cardiol. 2014;11:13-23.
6. Radke PW, Joner M, Joost A, et al. Vascular effects of paclitaxel following drug-eluting balloon angioplasty in a porcine coronary model:the importance of excipients. EuroIntervention. 2011;7:730-737.
7. Barath P, Fishbein MC, Vari S, Forrester JS. Cutting balloon:A novel approach to percutaneous angioplasty. Am J Cardiol. 1991;68:1249-1252.
8. Linares Vicente JA, Ruiz Arroyo JR, Lukic A, et al. 5-year results of cutting or scoring balloon before drug-eluting balloon to treat in-stent restenosis. REC Interv Cardiol. 2022;4:6-11.
9. Albiero R, Silber S, Di Mario C, et al. Cutting balloon versus conventional balloon angioplasty for the treatment of in-stent restenosis:Results of the restenosis cutting balloon evaluation trial (RESCUT). J Am Coll Cardiol. 2004;43:943-949.
10. Kufner S, Joner M, Schneider S, et al. Neointimal Modification With Scoring Balloon and Efficacy of Drug-Coated Balloon Therapy in Patients With Restenosis in Drug-Eluting Coronary Stents:A Randomized Controlled Trial. JACC Cardiovasc Interv. 2017;10:1332-1340.
11. Koskinas KC, Nakamura M, Raber L, et al. Current use of intracoronary imaging in interventional practice - Results of a European Association of Percutaneous Cardiovascular Interventions (EAPCI) and Japanese Association of Cardiovascular Interventions and Therapeutics (CVIT) Clinical Practice Survey. EuroIntervention. 2018;14:e475-e484.
12. Alfonso F, Sandoval J, Cárdenas A, Medina M, Cuevas C, Gonzalo N. Optical coherence tomography:from research to clinical application. Minerva Med. 2012;103:441-464.
In 1995, my colleagues and I at the Washington Hospital Center (Washington, DC, United States) published an intravascular ultrasound (IVUS) vs angiographic assessment of calcium in 1155 lesions targeted for percutaneous coronary intervention (figure 1)1. Angiography detected calcium in 440 lesions (38%), but IVUS detected lesion calcium in 841 lesions (73%). Among these 1155 lesions, 27% had no IVUS calcium, 26% had 1-quadrant IVUS calcium, 21% had 2 quadrants, 15% had 3 quadrants, and 11% had 4-quadrant IVUS calcium. When present, target lesion calcium was only superficial in 48%, only deep in 28%, and both superficial and deep in 24%. Therefore, some superficial calcium was present in 72% of the 841 calcium-containing lesions (1-quadrant superficial calcium in 35%, 2 quadrants in 31%, 3 quadrants in 18%, and 4-quadrant superficial calcium in 18%). The diagnostic ability of angiography to detect calcium was primarily dependent on the arc and length of calcium, but also on whether calcium was or not superficial (figure 1). However, there was also a curious 10% rate of angiographic false positives attributed to the difficulty differentiating perivascular or reference segment calcium from intralesional calcium. However, it was never clear whether there was a systematic problem with angiographic calcium detection or whether it was because, in the early 1990s, angiography was primitive compared to today and would improve over time.
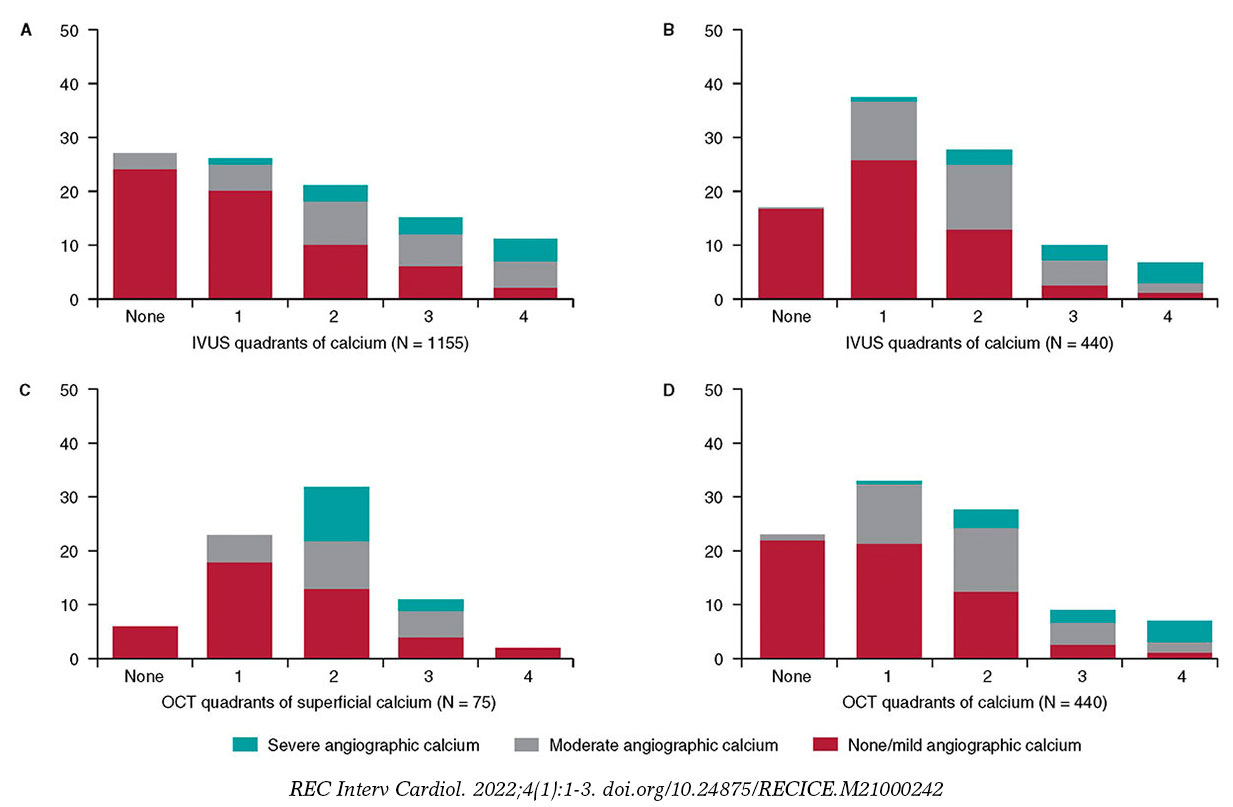
Figure 1. A total of 3 studies (clockwise starting in the upper left-hand corner) comparing intravascular imaging to the angiography detection of coronary lesion calcium. A: the study conducted by Mintz et al.1 from 1995. B and C: the study by Wang et al.2 from 2017. D: the study by McGuire et al.3 from 2021. IVUS, intravascular ultrasound; OCT, optical coherence tomography.
This experiment was repeated more than 20 years later by Wang et al. in a smaller cohort of 440 lesions using state-of-the-art angiographic equipment and both IVUS and optical coherence tomography (OCT) imaging (figure 1).2 Any amount of calcium was detected by coronary angiography in 40.2% (177 of 440) of the lesions, by IVUS in 82.7% (364 of 440) of the lesions, and by OCT in 76.8% (338 of 440) of the lesions. Notably and compared to the 1995 study, almost all calcium was superficial, fewer lesions had no calcium, and more lesions had 1- or 2-quadrant calcium (figure 1). In 13.2% of the lesions with IVUS-detected calcium, calcium was not visible by OCT mostly because of attenuation due to superficial lipid plaque accumulation. In a recent paper published in REC: Interventional Cardiology, McGuire et al.3 compared angiographic vs OCT calcium detection in 75 lesions. OCT detected calcium in 69 lesions vs 30 lesions by angiography with no angiographic false positives (figure 1).3 Compared to IVUS, OCT can measure the thickness, area, and volume that affect the angiographic detection of calcium in addition to its arc and length.2,3
Other than a reduced rate of false positives in the 2 contemporary studies, which could be attributed to the improved resolution of modern x-ray equipment, the lower x-ray doses being used today vs 1995, and the clinical recognition of the existence perivascular calcium, the results were remarkably similar to those of 1995. Thus, there appears to be a fundamental limitation to x-ray that cannot be improved by technological advances.
Why is calcium detection so important? The primary cause of in-stent restenosis is stent underexpansion, the primary cause of stent underexpansion is calcium, and the natural history of in-stent restenosis is not benign with an annual mortality rate of 5% to 7% (associated with treatment and at the follow-up).4-7 There are calcium scores for both OCT and IVUS that reliably predict calcium-related stent underexpansion (figure 2);8,9 and there are technologies and approaches that can be used to modify calcium to promote a better stent expansion.4,10
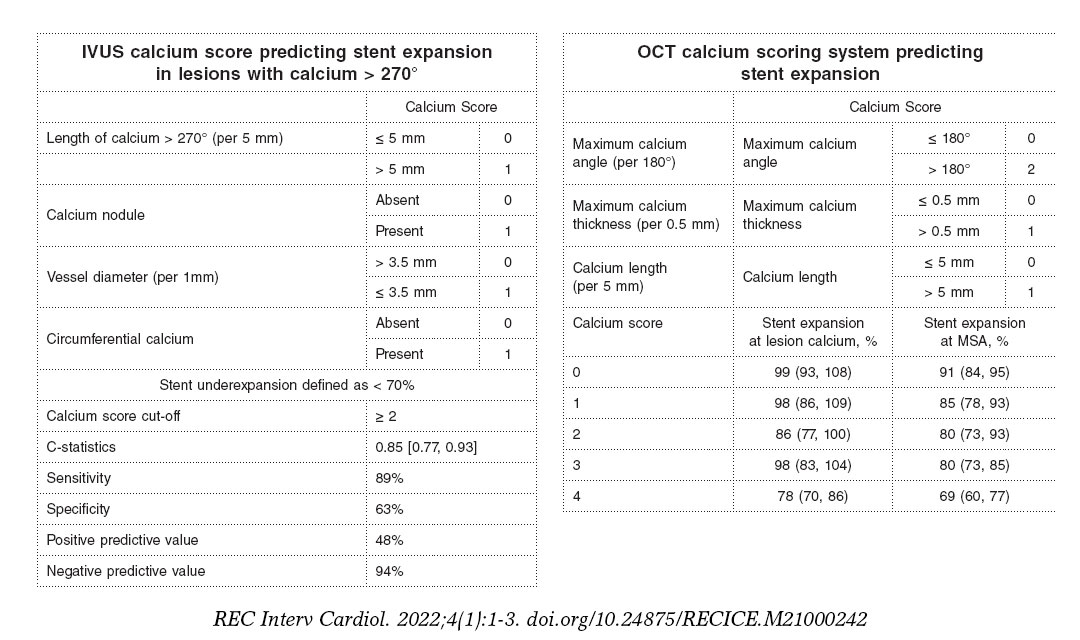
Figure 2. Intravascular ultrasound and optical coherence tomography calcium scores to predict stent underexpansion.8,9 IVUS, intravascular ultrasound; MSA, minimum stent area; OCT, optical coherence tomography.
There are predictors of target lesion calcium at patient level (older age, non-insulin treated diabetes, stable angina rather than an acute coronary syndrome, chronic kidney disease—especially if a patient is on dialysis—, and calcium elsewhere in the coronary tree), and predictors at lesion level too (smaller vessels, more severe stenoses).11-15 However, for the most part, lesions behave independently with regards to calcium accumulation. Only intravascular imaging can reliably detect and quantify target lesion calcium and predict stent underexpansion in the severe target lesion calcium setting.
FUNDING
None.
CONFLICTS OF INTEREST
G.S. Mintz declares having received honoraria from BostonScientific, Philips, Medtronic, and Abiomed outside the present work.
REFERENCES
1. Mintz GS, Popma JJ, Pichard AD, et al. Patterns of calcification in coronary artery disease. A statistical analysis of intravascular ultrasound and coronary angiography in 1155 lesions. Circulation. 1995;91:1959-1965.
2. Wang Z, Matsumura M, Mintz GS, et al. In vivo calcium detection by comparing optical coherence tomography, intravascular ultrasound, and angiography. JACC Cardiovasc Imaging. 2017;10:869-879.
3. McGuire C, Shlofmitz E, Melaku GD, et al. Comparison of quantitative calcium parameters in optical coherence tomography and invasive coronary angiography. REC Interv Cardiol. 2022;4:6-11.
4. Mintz GS, Ali ZA, Maehara A. Use of intracoronary imaging to guide optimal percutaneous coronary intervention procedures and outcomes. Heart. 2021;107:755-764.
5. Wiebe J, Kuna C, Ibrahim T, et al. Long-term prognostic impact of restenosis of the unprotected left main coronary artery requiring repeat revascularization. JACC Cardiovasc Interv. 2020;13:2266-2274.
6. Tamez H, Secemsky EA, Valsdottir LR, et al. Long-term outcomes of percutaneous coronary intervention for in-stent restenosis among Medicare beneficiaries. EuroIntervention. 2021;17:e380-e387.
7. Shlofmitz E, Torguson R, Zhang C, et al. Impact of intravascular ultrasound on Outcomes following PErcutaneous coronary interventioN for In-stent Restenosis (iOPEN-ISR study). Int J Cardiol. 2021 https://doi.org/10.1016/j.ijcard.2021.08.003.
8. Fujino A, Mintz GS, Matsumura M, et al. A new optical coherence tomography-based calcium scoring system to predict stent underexpansion. EuroIntervention. 2018;13:e2182-e2189.
9. Zhang M, Matsumura M, Usui E, et al. Intravascular ultrasound-derived calcium score to predict stent expansion in severely calcified lesions. Circ Cardiovasc Interv. 2021;14:e010296.
10. De Maria GL, Scarsini R, Banning AP. Management of calcific coronary artery lesions:Is it time to change our interventional therapeutic approach?JACC Cardiovasc Interv. 2019;12:1465-1478.
11. Mintz GS, Pichard AD, Popma JJ, et al. Determinants and correlates of target lesion calcium in coronary artery disease:a clinical, angiographic and intravascular ultrasound study. J Am Coll Cardiol. 1997;29:268-274.
12. Mintz GS, Pichard AD, Kent KM, Satler LF, Popma JJ, Leon MB. Interrelation of coronary angiographic reference lumen size and intravascular ultrasound target lesion calcium. Am J Cardiol. 1998;81:387-391.
13. Tuzcu EM, Berklap B, DeFranco AC, et al. The dilemma of diagnosing coronary calcification:angiography versus intravascular ultrasound. J Am Coll Cardiol. 1996;27:832-838.
14. Gruberg L, Rai P, Mintz GS, et al. Impact of renal function on coronary plaque morphology and morphometry in patients with chronic renal insufficiency as determined by intravascular ultrasound volumetric analysis. Am J Cardiol. 2005;96:892-896.
15. Chin CY, Matsumura M, Maehara A, et al. Coronary plaque characteristics in hemodialysis-dependent patients as assessed by optical coherence tomography. Am J Cardiol. 2017;119:1313-1319.
The arrival of drug-eluting stents (DES) nearly 2 decades ago ignited a revolution in the field of interventional cardiology. The addition of antiproliferative drugs to the stent platform reduced the rate of in-stent restenosis significantly and increased the number of patients that, to this date, have benefited from percutaneous revascularization.1,2 However, its Achilles tendon was initially the higher rate of late stent thrombosis involved. The permanent polymer used in the first generation of DES induced inflammatory and hypersensitivity reactions that delayed endothelization. A health alert followed3 that made the medical community recommend extended courses of dual antiplatelet therapy and put into question the convenience of DES. Beyond the increased rate of stent thrombosis, the first-generation of this type of stents had additional limitations: they were stainless-steel platforms with up to 140 µm thick struts, worse stent navigability, and fewer crossing capabilities. Also, the stent maximum expansion was limited (3.5 mm in the Cypher stent, Cordis Corp.), which occasionally prevented treating left main coronary artery lesions. With the passing of time, this stent technology has been refined to a point that there has been a major overhaul in its 3 main components: platform, polymer, and antiproliferative drug.
The changes made to the stent platform have been the development of more biocompatible alloys that have reduced strut thickness significantly and, consequently, improved stent navigability. Additionally, radial strength has been preserved to prevent recoil (table 1). Most of the stents commonly used today consist of cobalt-chromium or platinum-chromium alloys. The open-cell design has won the battle over the closed-cell design because it reduces the number of inter-strut links, the degree of jailed side-branch while improving stent navigability and conformability. Also, the new generation of DES have wider overexpansion limits (4.5 mm to 6 mm), which allows us to treat left main coronary artery lesions by adapting the stent area to the corresponding lunimal references without damage to the platform.
Table 1. Characteristics of drug-eluting stents
| Stent | Plataform | Polymer/ coating | Drug | Strut thickness (µm) | Maximum expansion (mm) | Studies with 1 month DAPT duration |
|---|---|---|---|---|---|---|
| XIENCE | Cobalt-chromium | Permanent/ circumferential | Everolimus | 81 | 2-3.25 → 3.75 3.5-4 → 5.5 |
Xience 28 USA (NCT03815175) |
| SYNERGY | Platinum-chromium | Bioresorbible/ abluminal | Everolimus | 74 | 2.25 → 3.5 3-3.5 → 4.25 4-5 → 5.75 |
SENIOR (NCT02099617) |
| Onyx | Nickel-platinum-chronium | Permanent/ circumferential | Zotarolimus | 81 | 2.5-3 → 3.75 3.5-4 → 4.75 4.5-5 → 5.75 |
Onyx ONE (NCT03344653) |
| Orsiro | Cobalt-chromium | Bioresorbible/ circumferential | Sirolimus | 60 | 2.5-3 → 3.5 3.5-4 → 4.5 |
Bioflow-DAPT (NCT04137510) |
| Ultimaster Tansei | Cobalt-chromium | Bioresorbible/ abluminal | Sirolimus | 80 | 2.25-3 → 4.5 3.5-4 → 5.5 |
Master DAPT (NCT03023020) |
| BioFreedom | Stainless-steel | Polymer-free/ abluminal | Umirolimus | 112 | 2.5-3 → 4.76 3.5-4 → 5.96 |
LEADERS FREE (NCT01623180) |
| Angiolite | Cobalt-chromium | Permanent/circumferential | Sirolimus | 75-85 | 2-2.5 → 4 2.75-3.5 → 5.25 4-4.5 → 6 |
– |
|
DAPT, dual antiplatelet therapy. |
||||||
Polymers are the reservoir from which the drug is released in a controlled way towards the arterial wall. XIENCE (Abbott), and Resolute Onyx (Medtronic) stents include permanent polymers, but with improved biocompatibility. The XIENCE polymer is highly fluorinated, which minimizes adhesion and platelet activation increasing the safety profile. The Onyx stent uses Biolinx that consists of a mixture of polymers with hydrophilic capabilities that make it biocompatible and hydrophobic for a prolonged and uniform drug release. However, despite the good results reported with the new permanent polymers, some companies have decided to develop bioresorbable polymers (SYNERGY [Boston Scientific], Orsiro [Biotronik], Ultimaster Tansei [Terumo] stents, etc.). The use of a bioresorbable polymer-based coating facilitates degradation after the drug complete release just leaving 1 bare-metal stent behind 3-4 months after implantation, which prevents the remaining polymer from participating in the immune response associated with stent thrombosis. The biodegradable polymer-based SYNERGY stent has shown a rate of stent thrombosis of 0% at the 6-month follow-up, and a rate of target lesion revascularization similar to the one observed with the permanent polymer-based Promus Element stent (Boston Scientific).4 On the other hand, the biodegradable polymer-based Orsiro stent had a significantly lower rate of target lesion failure compared to the XIENCE stent with permanent polymer.5 However, the XIENCE stent group had more and longer stents implanted, both factors associated with adverse events at follow-up.
Polymer-free stents stand as an alternative to biodegradable polymer-based stents. The most representative of the former is the BioFreedom (Biosensors). It consists of a stainless-steel platform with micropores that store biolimus for a 1-month release of the drug. The lack of a polymer may potentially allow to shorten the duration of the period on dual antiplatelet therapy down to 1 month, like with bare metal stents. In the LEADERS FREE trial,6 the BioFreedom was compared to a bare metal stent in patients with high-risk of bleeding and a 1-month course of dual antiplatelet therapy. The outcomes proved that it was superior regarding the primary evaluation criteria for the safety and efficacy profile. Afterwards, almost every company has conducted or started safety and efficacy trials with 1-month courses of dual antiplatelet therapy (table 1).
Therefore, several advances have been made with new generation DES. The clinical impact associated with strut thickness reduction or the selection of bioresorbable polymer-based stents vs permanent or polymer-free stents is still under discussion. However, these improvements have had significant repercussions in the stent navigability, overexpansion capabilities, and selection of duration for dual antiplatelet therapy. However, these stent properties highly demanded by interventional cardiologists should always be based on a robust set of trials that confirm the efficacy and safety profile of each stent. Currently, the Angiolite stent (iVascular) is in this stage. It has recently joined the family of DES. This stent is an ultra-thin strut (75 µm to 85 µm) cobalt-chromium platform made from a biostable fluorinated polymer plus sirolimus as the antiproliferative drug. In the ANCHOR trial it showed an excellent degree of endothelization on the optical coherence tomography,7 with an 83% strut endothelial coverage at 3 months. Afterwards, the ANGIOLITE trial compared it to the standard DES and found a 0.04 mm late luminal loss vs the 0,08 mm of the XIENCE stent, as well as a low rate of events at the 2-year follow-up in both groups8 (target lesion failure, 7.1% with the Angiolite vs 7.6% with the XIENCE). In an article published on REC Interventional Cardiology, Pérez de Prado et al.9 presented a multicenter real-world registry of patients treated with the Angiolite stent. This registry could be considered the «moment of truth» for this stent. We should remember that the Absorb stent (Abbott) had excellent immediate results and at the 5-year follow-up10 in the early trials. However, it showed a high rate of stent thrombosis when used in real-world patients. The ANCHOR registry included 646 patients with a 2-year clinical follow-up. A total of 30% of these patients were diabetics. ST-segment elevation myocardial infarction was the clinical presentation in almost 25% of these patients, and nearly 50% of them had multivessel disease. The rate of target vessel failure and the rate of stent thrombosis at the 2-year follow-up were 3.4%, and 0.9%, respectively. In this sense, the stent offers similar results to those obtained with state-of-the-art DES as the table of the supplementary data of the aforementioned article shows.9 However, these promising results will need to be confirmed at the 5-year follow-up. The behavior of the stent in the most complex lesions like bifurcations or chronic total occlusions associated with worse clinical outcomes—underrepresented in the registry—also needs to be assessed.
FUNDING
The authors received no funding whatsoever while preparing this manuscript.
CONFLICTS OF INTEREST
J. Suárez de Lezo has received fees from Terumo for his role as a consultor for Abbott and AstraZeneca, as well as for his presentations in training courses and seminars. P. Martín received fees from Cathmedical for his role as a consultor, as well as from Abbott and Boston Scientific for his presentations in training courses and seminars.
REFERENCES
1. Moses JW, Leon MB, Popma JJ, et al.;SIRIUS Investigators. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med. 2003;349:1315-1323.
2. Stone GW, Ellis SG, Cox DA, et al.;TAXUS-IV Investigators. A polymer-based, paclitaxel-eluting stent in patients with coronary artery disease. N Engl J Med. 2004;350:221-231.
3. Camenzind E, Steg PG, Wijns W. Stent thrombosis late after implantation of first-generation drug-eluting stents:a cause for concern. Circulation. 2007;115:1440-1455.
4. Meredith IT, Verheye S, Dubois CL, et al. Primary endpoint results of the EVOLVE trial:a randomized evaluation of a novel bioabsorbable polymer-coated, everolimus-eluting coronary stent. J Am Coll Cardiol. 2012:59:1362-1370.
5. Kandzari DE, Mauri L, Koolen JJ, et al. Ultrathin, bioresorbable polymer sirolimus-eluting stents versus thin, durable polymer everolimus-eluting stents in patients undergoing coronary revascularisation (BIOFLOW V):a randomised trial. Lancet. 2017;390:1843-1852.
6. Urban P, Meredith IT, Abizaid A, et al. Polymer-free drug-coated coronary stents in patients at high bleeding risk. N Engl J Med. 2015;373:2038-2047.
7. Puri R, Otaegui I, Sabate M, et al. Three- and 6-month optical coherence tomographic surveillance following percutaneous coronary intervention with the Angiolite(R) drug-eluting stent:The ANCHOR study. Catheter Cardiovasc Interv. 2018;91:435-443.
8. Moreu J, Moreno-Gomez R, Perez de Prado A, et al. First-in-man randomised comparison of the Angiolite durable fluoroacrylate polymer-based sirolimus-eluting stentversus a durable fluoropolymer-based everolimus-eluting stentin patients with coronary artery disease:the ANGIOLITE trial. EuroIntervention. 2019;15:e1081-e1089.
9. Pérez de Prado A, Ocaranza-Sánchez R, Lozano Ruiz-Poveda F, et al. Real-world registry of the durable Angiolite fluoroacrylate polymer-based sirolimus-eluting stent:the EPIC02–RANGO study. REC Interv Cardiol. 2021. https://doi.org/10.24875/RECICE.M21000223.
10. Onuma Y, Dudek D, Thuesen L, et al. Five-Year Clinical and Functional Multislice Computed Tomography Angiographic Results After Coronary Implantation of the Fully Resorbable Polymeric Everolimus-Eluting Scaffold in Patients With De Novo Coronary Artery Disease:The ABSORB Cohort A Trial. JACC Cardiovasc Interv. 2013;6:999-1009.
Transcatheter aortic valve implantation (TAVI) has become a widely used therapeutic strategy to treat symptomatic severe aortic stenosis. Certain randomized clinical trials available have already described the prognostic benefit of this technique in elderly patients with high or very high surgical risk. Also, when implanted via transfemoral access, it has proven non-inferior or even superior compared to surgical aortic valve replacement in low- and intermediate-risk patients. Therefore, the current recommendations support its use in elderly patients with severe aortic stenosis regardless of their surgical risk.1
However, since it is an age-related heart valve disease without an effective medical therapy yet, the prevalence of severe aortic stenosis has been growing parallel to life expectancy. As a matter of fact, this disease has huge repercussions in the patients’ survival rate and quality of life.2 Consequently, nonagenarian patients with severe aortic stenosis are a group in continuous expansion, and, to this date, the best way to treat them is still under discussion. Since most of these patients have traditionally been misrepresented in the clinical trials and there are registries with good results but a possible selection bias, the decision to treat these patients with TAVI is still challenging and is made on an individual basis after meticulous assessment of the patients by the heart team.
Data from the STS/ACC TVT registry on the results of 3773 patients ≥ 90 age provide us with relevant information on this clinical setting.3 Data show a higher mortality rate compared to younger patients at 30 days (8.8% vs 5.9%; P < .001) and 1 year (24.8% vs 22.0%; P < .001) mainly due to higher rates of in-hospital major bleeding (8.1% vs 6.8%; P < .001) and strokes (2.7% vs 2.1%; P = .021). Table 1 shows the data from the main international registries on nonagenarian patients treated with TAVI.
Table 1. Data of nonagenarian patients treated with TAVI from the main international registries
| Study, year | N (≥ 90 years) | Procedural success | Major bleeding | 30-day mortality rate | 1-year mortality rate |
|---|---|---|---|---|---|
| SwissTAVI,4 2021 | 507 | N/A | 13% | 6.7% | 19.7% |
| Mentias et al.,5 2019 | 13 544 | N/A | 10% | 3.6% | 26.6% |
| Vlastra et al.,6 2019 | 882 | N/A | 8% | 9.9% | N/A |
| Doshi et al.,7 2018 | 1163 | N/A | 35% | 6.0% | N/A |
| Elgendy et al.,8 2018 | 5840 | N/A | 28% | 6.6% | N/A |
| McNeely et al.,9 2017 | 3531 | N/A | 34% | 8.4% | 25.4% |
| STS/ACC TVT,3 2016 | 3773 | N/A | 8% | 8.8% | 24.8% |
|
N/A, not available; TAVI, transcatheter aortic valve implantation. |
|||||
In a study recently published on REC: Interventional Cardiology, Cepas-Guillén et al. describe the national experience with TAVI in nonagenarian patients with severe aortic stenosis between 2009 and 2018.10 The findings were compared to those from patients between 75 and 90 years who received the same treatment during the same period of time. A total of 8073 patients—387 nonagenarians and 7686 patients between 75 and 90 years—were included. The authors saw a higher in-hospital mortality rate in nonagenarian patients without significant differences at the 1-year follow-up (although with a tendency towards a higher mortality rate in patients ≥ 90 years). In the multivariate analysis, age was not significantly associated with a higher all-cause mortality rate, but the presence of comorbidities such as atrial fibrillation or worsening renal function. Also, a higher surgical risk was reported.10 The role of comorbidities in nonagenarian patients was analyzed by a former substudy that included 117 consecutive patients around 90 years old (median age, 91.1 years; 117 women) from the PEGASO (Prognosis of symptomatic severe aortic stenosis in octogenarians) and IDEAS (Influence of the severe aortic stenosis diagnosis) registries conducted in our country.11 A high comorbidity burden, characterized by scores ≥ 3 in the Charlson comorbidity index, present in a high number of patients, was associated with a high mortality rate at the 1-year follow-up.
Nonetheless, data from the SwissTAVI registry confirmed a tendency towards higher rates of mortality, stroke, and pacemaker implantation in the elderly group (< 70, 70-79, 80-89, and > 90 years) among the 7097 patients treated with TAVI between 2011 and 2018 (median age, 82 ± 6.4 years; 49.6% women) in Switzerland.4 It is interesting that older age was associated with a lower standard mortality rate compared to the general population of the same group without any differences reported among nonagenarian patients. Same as in the study conducted by Cepas-Guillén et al.,10 the mean comorbidity rate of nonagenarian patients included in this registry was lower compared to that of patients < 90 years, suggestive that it is a highly selected population, which is unequivocally associated with a better prognosis in the short- and long-term. Despite of this, in this series, vascular complications and major bleeding increased significantly among nonagenarian patients. In the metanalysis conducted by Sun et al.,12 the rate of major bleeding reported was similar above and below the 90-year mark with a relative risk of 1.17 (95% confidence interval, 1.04-1.32). On the contrary, the rate of vascular complications went up > 90 years, especially when non-femoral access techniques were used. In the Spanish national series, transfemoral access was more frequently used in patients < 90 years. Although no random comparison of the access routes was conducted, most data support the idea that risks are higher when the non-femoral access is used.13 Also, these data recommend the use of this access in elderly patients whenever possible. Also, a tendency towards better results has been confirmed as heart teams have been gaining experienced in the management of this group of patients, both in the selection and implantation technique used as well as in further approaches with lower rates of complications and 30-day mortality > 50% at the 4-year follow-up.5 Noteworthy, it would be interesting to have more data on the treatment received by the patients, especially regarding antiplatelet therapy, given these patients’ higher risk of bleeding with the use of 2 different antiplatelet drugs, instead of 1,14 and a longer follow-up too.
Added to all this, we should recognise not only the presence of comorbidities, but also frailty, and other geriatric symptoms—prevalent all of them—that have a significant prognostic impact in elderly patients treated with TAVI.15 Different scales have been described, some of them very easy to implement and based on easy parameters like the presence of lower-limb frailty, cognitive impairment, anemia, and hypoalbuminemia, which allow us to predict mortality at the 1-year follow-up.16 The implementation of measures is essential to reverse frailty—if present—and prevent the appearance of delirium and other complications during admission since this improves the prognosis of patients significantly.
Finally, we wish to congratulate the Interventional Cardiology Association of the Spanish Society of Cardiology Association for their remarkable work in this area—in continuous expansion and growth—since the experience and learning gained on this regard will contribute to improve the treatments that we will administer to our patients.
FUNDING
No funding whatsoever.
CONFLICTS OF INTEREST
None declared.
REFERENCES
1. Baumgartner H, Falk V, Bax JJ, et al.;ESC Scientific Document Group. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38:2739-2791.
2. Osnabrugge RLJ, Mylotte D, Head SJ, et al. Aortic stenosis in the elderly:disease prevalence and number of candidates for transcatheter aortic valve replacement:a meta-analysis and modeling study. J Am Coll Cardiol. 2013;62:1002-1012.
3. Arsalan M, Szerlip M, Vemulapalli S, et al. Should transcatheter aortic valve replacement be performed in nonagenarians?:insights from the STS/ACC TVT registry. J Am Coll Cardiol. 2016;67:1387-1395.
4. Attinger-Toller A, Ferrari E, Tueller D, et al. Age-Related Outcomes After Transcatheter Aortic Valve Replacement:Insights From the SwissTAVI Registry. JACC Cardiovasc Interv. 2021;14:952-960.
5. Mentias A, Saad M, Desai MY, et al. Temporal Trends and Clinical Outcomes of Transcatheter Aortic Valve Replacement in Nonagenarians. J Am Heart Assoc. 2019;8:e013685.
6. Vlastra W, Chandrasekhar J, Vendrik J, et al. Transfemoral TAVR in Nonagenarians:From the CENTER Collaboration. JACC Cardiovasc Interv. 2019;12:911-920.
7. Doshi R, Patel V, Shah P. Comparison of in-hospital outcomes between octogenarians and nonagenarians undergoing transcatheter aortic valve replacement:a propensity matched analysis. J Geriatr Cardiol. 2018;15:123-130.
8. Elgendy IY, Mahmoud AN, Elbadawi A, et al. In-hospital outcomes of transcatheter versus surgical aortic valve replacement for nonagenarians. Catheter Cardiovasc Interv. 2019;93:989-995.
9. McNeely C, Zajarias A, Robbs R, Markwell S, Vassileva CM. Transcatheter Aortic Valve Replacement Outcomes in Nonagenarians Stratified by Transfemoral and Transapical Approach. Ann Thorac Surg. 2017;103:1808-1814.
10. Cepas-Guillén PL, Regueiro A, Sanmiguel Cervera D, et al. Outcomes of nonagenarians after transcatheter aortic valve implantation. REC Interv Cardiol. 2021. https://doi.org/10.24875/RECICE.M21000220.
11. Bernal E, Ariza-SoléA, Formiga F, et al.;Influencia del Diagnóstico de Estenosis Aórtica Severa (IDEAS) Registry Investigators. Conservative management in very elderly patients with severe aortic stenosis:Time to change?J Cardiol. 2017;69:883-887.
12. Sun Y, Liu X, Chen Z, et al. Meta?analysis of predictors of early severe bleeding in patients who underwent transcatheter aortic valve implantation. Am J Cardiol. 2017;120:655?661.
13. Drudi LM, Ades M, Asgar A, et al. Interaction between frailty and access site in older adults undergoing transcatheter aortic valve replacement. JACC Cardiovasc Interv. 2018;11:2185?2192.
14. Sanz-Sánchez J, Pivato CA, Leone PP, et al. Tratamiento antiagregante plaquetario único o doble tras implante percutáneo de válvula aórtica. Metanálisis de ensayos clínicos aleatorizados. REC Interv Cardiol. 2021. https://doi.org/10.24875/RECIC.M21000206.
15. Díez-Villanueva P, Arizá-SoléA, Vidán MT, et al. Recommendations of the Geriatric Cardiology Section of the Spanish Society of Cardiology for the Assessment of Frailty in Elderly Patients With Heart Disease. Rev Esp Cardiol. 2019;72:63-71.
16. Afilalo J, Lauck S, Kim DH, et al. Frailty in Older Adults Undergoing Aortic Valve Replacement:The FRAILTY-AVR Study. J Am Coll Cardiol. 2017;70:689-700.
Subcategories







Interviews

An interview with Bruno Scheller
aServicio de Cardiología, Hospital Universitario de La Princesa, Instituto de Investigación Sanitaria de La Princesa (IIS-IP), Universidad Autónoma de Madrid, Spain
bCentro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain




