
Available online: 09/04/2019
Editorial
REC Interv Cardiol. 2020;2:310-312
The future of interventional cardiology
El futuro de la cardiología intervencionista
Emory University School of Medicine, Atlanta, Georgia, United States
Thirty years ago, in 1996, the concept of evidence-based medicine took hold; David Sackett, one of its leading advocates, defined it as the conscientious, explicit, and judicious use of the current best evidence for clinical decision-making. Since then, the properly designed randomized clinical trial has been the method par excellence for demonstrating the efficacy of medical interventions and generating robust evidence to inform the recommendations of scientific societies. However, over the past few decades, the scientific community has learned a great deal about the limitations of this methodology.
The results of the OPTIMAL trial have recently been published; the trial was designed to determine whether intravascular ultrasound (IVUS)-guided percutaneous revascularization of the unprotected left main coronary artery (LMCA) leads to better clinical outcomes than revascularization guided by conventional angiography alone.1 In this trial, a total of 806 patients with a mean age of 71 years and a mean SYNTAX score of 30 were randomized to one of the two interventions; 78% of them were women. After a median follow-up of 2.9 years, the primary endpoint occurred in 135 patients (33.7%) in the IVUS-guided group and in 125 patients (30.9%) in the angiography-guided group. The incidence of death, myocardial infarction, or revascularization was similar in both groups. The incidence of stroke was higher in the IVUS group, although these events occurred at a median of 19 months, which may suggest a chance finding. The authors concluded that, among patients with LMCA disease, IVUS-guided percutaneous revascularization showed no additional benefit compared with angiography- guided revascularization. This is not the first time that trial results have conflicted with initial expectations.
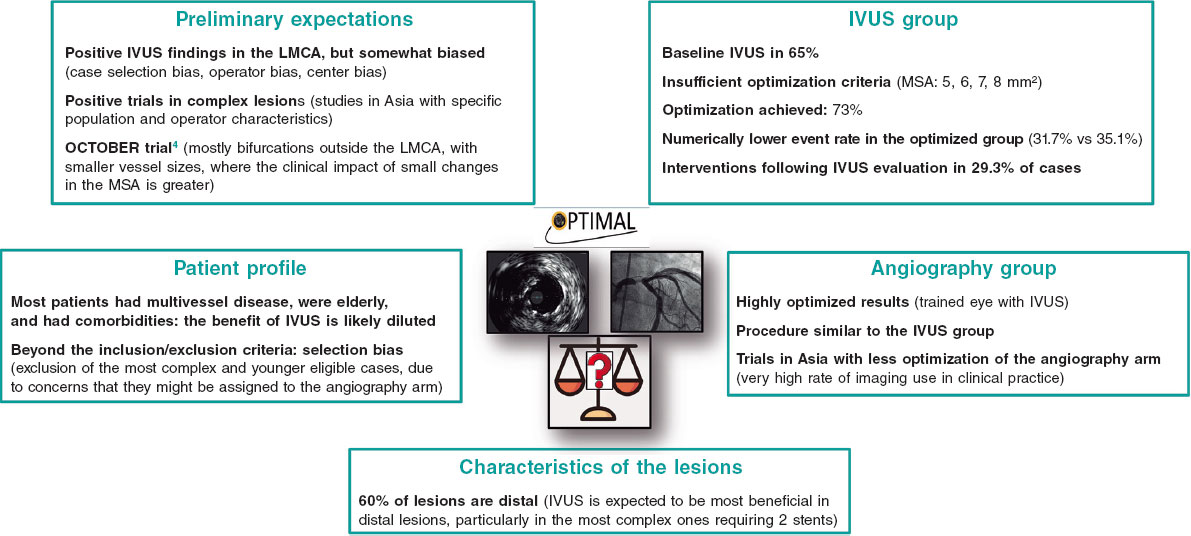
For many years, I have been an advocate and promoter of the use of IVUS to guide drug-eluting stent angioplasty procedures in the LMCA, based on a conviction derived from my own experience, but primarily on the results of numerous observational studies, including some that we conducted in our country.2,3 Therefore, being one of the principal investigators and the second author of the OPTIMAL trial manuscript places me in a unique position. On the one hand, I must accept the results of a trial that was executed flawlessly in every respect; on the other hand, I remain convinced that the use of IVUS can continue to add value in many cases of LMCA disease, especially when used appropriately. In the following paragraphs, I will attempt to explain and justify this position (figure 1).
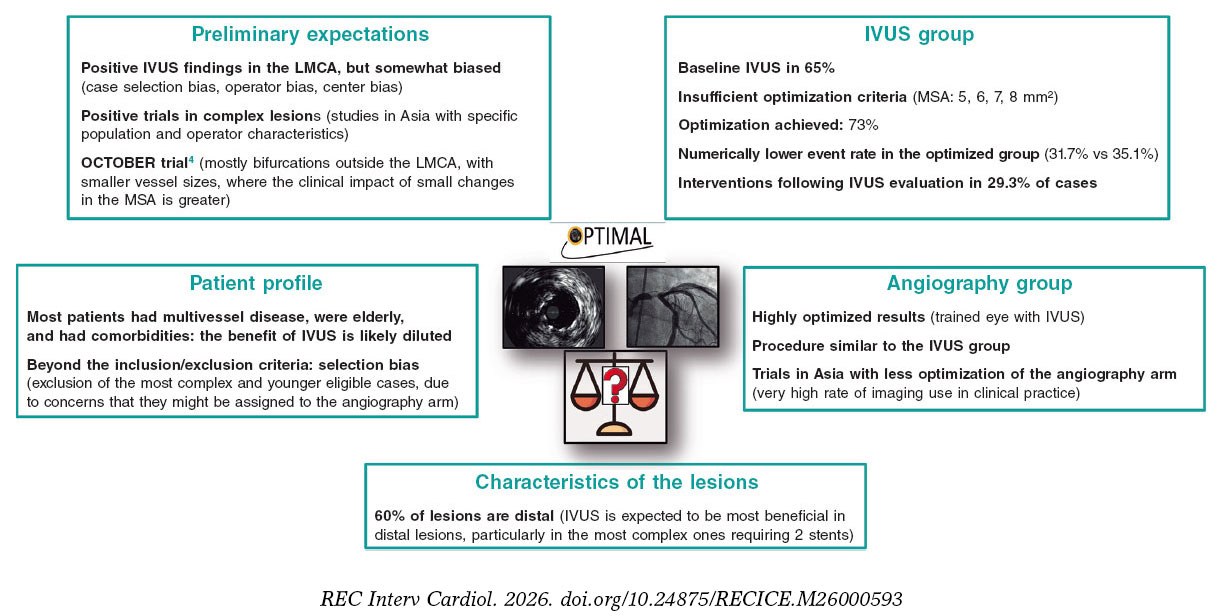
Figure 1. Various factors explaining the relative discrepancy between the expected results and those ultimately obtained in the OPTIMAL study. IVUS: intravascular ultrasound; LMCA: left main common artery; MSA: minimum stent area. The bibliographical references mentioned in this figure correspond to Testa et al.1 (OPTIMAL trial) and Holm et al.4 (OCTOBER trial).
EXPECTATIONS PRIOR TO THE OPTIMAL TRIAL
In recent years, several observational studies and corresponding meta-analyses have been published, all of which demonstrated that the use of IVUS in percutaneous revascularization of the LMCA was associated with a reduction in events, including cardiac death, myocardial infarction, and revascularization.5 However, it is evident that the benefits observed in registries are often exaggerated, and this is due to certain biases. First, selection bias. Comparing cases in which IVUS was used versus those in which it was not within a registry implies selection bias, since that decision was based on certain variables, which ultimately affected certain characteristics of the patients and the lesions. Even with statistical matching techniques, it is very difficult to completely eliminate the confounding effect of partially hidden biases.2 In this regard, the use of IVUS may have been more likely in patients in better clinical condition, who were more stable, and younger. This could explain the differences in overall mortality observed as early as the short- to medium-term between the IVUS and angiography groups in some registries.6
Another potential source of bias relates to the operator and the center. It is plausible that operators who used IVUS more frequently were also more meticulous in other technical and patient management aspects and were based at centers with higher patient volumes and greater experience. A large British registry found that the benefit of IVUS was greater when operators had higher case volumes, suggesting this bias.6
The positive results of some randomized trials, although not focused on the LMCA and conducted in Asian countries, also instilled considerable optimism.7-10
The OCTOBER trial, which compared optical coherence tomography-guided versus angiography-guided treatment of bifurcations, showed a lower incidence of the primary endpoint at 2 years (10.1% vs 14.1%).4 It should be noted that these were mostly bifurcations that did not involve the LMCA and involved smaller vessels, where a greater effect of small changes in the minimum stent area (MSA) on clinical outcomes is expected.
PATIENT PROFILE
In the OPTIMAL trial, the mean age of patients was 71 years, 5 years older than that of patients in the OCTOBER trial.1,4 Fifty-eight percent had three-vessel disease, with a mean SYNTAX score of 30. This explains the high incidence of events, exceeding 30% at 2.9 years.1
As is often the case in many trials, and especially when there are pre-existing biases, patient enrollment may have taken into account factors beyond the inclusion/exclusion criteria, leading to selection bias. Consequently, it is possible that some patients for whom IVUS was deemed necessary (such as those with more complex distal lesions or younger patients) were excluded.
CHARACTERISTICS OF LMCA LESIONS
In the OPTIMAL trial, 60% of the treated LMCA lesions involved the bifurcation. In a large Spanish multicenter registry, with two matched groups of 505 patients each, we found that the benefit associated with the use of IVUS in LMCA angioplasty with drug-eluting stents was greater in distal lesions and, particularly, in those requiring two stents.2 Therefore, the inclusion of a relatively high proportion of non-distal lesions may have reduced the overall impact of IVUS in the OPTIMAL study.
In the recently published IVUS-CHIP trial, which evaluated the use of IVUS in 2020 patients with complex lesions and demostrated no differences compared with angiography, a trend toward a benefit from IVUS was observed in distal LMCA lesions.11
THE IVUS GROUP
IVUS is not a therapeutic tool, it is an imaging technique, and the benefit it may provide depends on how the operator uses it. The resulting clinical advantage derived from its use will be solely due to the corrective measures prompted by the imaging findings, the optimization criteria pursued, and the extent to which those criteria are met. In the OPTIMAL trial, the use of IVUS prior to the procedure was 65%, whereas a higher rate of use would have been expected to better understand the characteristics of the plaques and plan plaque management.
Among the optimization criteria, those related to expansion are particularly relevant, specifically the MSA cutoff values that were considered mandatory to achieve in this trial.12 These values were 8 mm² for the LMCA, 7 mm² for the confluence polygon, 6 mm² for the left anterior descending artery, and 5 mm² for the left circumflex artery, which were acceptable at the time the trial was designed but have since been surpassed by more recent studies. Currently, the optimal MSA cutoff values are estimated at 10 mm² for the TCI, 7 mm² for the left anterior descending artery, and 6 mm² for the left circumflex artery.13-17 In fact, just as this editorial was being written, the European Association of Percutaneous Cardiovascular Interventions and the European Bifurcation Club published a consensus document on the use of imaging in LMCA angioplasty that incorporates these new target values.18
In the OPTIMAL study, the final MSA in the LMCA was 12.99 ± 4.09 mm², 7.79 ± 2.43 mm² in the left anterior descending artery, and 6.75 ± 1.92 mm² in the left circumflex artery, indicating that in 15% of cases the MSA in the LMCA was less than 9 mm², less than 5.3 mm² in the anterior descending artery, and less than 4.8 mm² in the circumflex artery.1
However, in addition to establishing criteria, it is advisable to attempt, within the bounds of what is feasible and safe, to achieve these objectives. In the OPTIMAL study, corrective actions were observed in 29.3% of cases, and optimization was confirmed in 73%, with a numerically lower event rate in the optimized group (31.7% vs. 35.1%).1 It should be noted that failure to achieve the targets cannot be attributed solely to lack of adherence but is often due to safety considerations. In this regard, it is noteworthy that there were no differences in periprocedural complications between the groups.
The consideration of appropriate criteria and their implementation under a standardized protocol provides a benefit compared to the non-protocolized use of IVUS.3
THE GROUP ASSIGNED TO ANGIOGRAPHY
Another striking aspect is the high degree of similarity between the groups regarding the technical aspects of the procedure, with a similar rate of post-dilatation and similar device sizes. This may suggest that the operator working solely with angiography acted based on the knowledge and experience of someone who has performed many IVUS-guided procedures, which could be considered an angiography- guided intervention but inspired by prior experience with IVUS.
In this regard, while we previously noted that Asian trials7-10 generally yielded more positive results than Western ones,1,11,19 it is worth noting that the angiography group in the former shows clear differences from the intravascular imaging group, with much lower use of post-dilatation and selection of stents with significantly smaller diameters. It is likely that the very high use of IVUS in Asian countries may influence this different approach when angiography is the only option available. Furthermore, it cannot be ruled out that these operators adhered more strictly to the protocol for optimization based on intravascular imaging.
FINAL COMMENTS AND RECOMMENDATIONS
Further subgroup analyses of the OPTIMAL trial are needed to address issues such as the effect of IVUS in cases of isolated LMCA disease, to explore outcomes based on different MSA values, and, above all, to identify anatomical or clinical subgroups that benefit most from IVUS-guided procedures.
The conclusions drawn from these reflections are as follows:
- –The routine use of IVUS to guide percutaneous revascularization in all cases of LMCA lesions is not clinically justified when operators have sufficient experience in performing the procedure.
- – It is necessary to identify which LMCA lesion profiles benefit most from the use of intravascular imaging techniques (most likely distal lesions).
- – Appropriate optimization criteria should be established.
- – Efforts should be made to achieve these objectives within safety margins.
- – The implementation of automated intravascular image assessment systems (based on artificial intelligence) can be of great help in this regard.
- – It is essential to continue promoting training and the use of intravascular imaging techniques among less experienced professionals.
Finally, in my opinion, it would be advisable to conduct a new randomized trial that includes patients with distal LMCA lesions without a high SYNTAX score and uses the most up-to-date optimization criteria.
Karl Popper
FUNDING
No funding was received for the preparation of this manuscript.
CONFLICTS OF INTEREST
J.M. de la Torre-Hernández is the editor-in-chief of
REFERENCES
1. Testa L, De la Torre Hernandez JM, De Maria GL, et al.;OPTIMAL Investigators. IVUS-Guided versus Angiography-Guided PCI in Unprotected Left Main Coronary Disease. N Engl J Med. 2026. https://doi.org/ 10.1056/NEJMoa2600440.
2. De la Torre Hernandez JM, Baz Alonso JA, Gómez Hospital JA, et al.;IVUS-TRONCO-ICP Spanish study. Clinical impact of intravascular ultrasound guidance in drug-eluting stent implantation for unprotected left main coronary disease:pooled analysis at the patient-level of 4 registries. JACC Cardiovasc Interv. 2014;7:244-254.
3. de la Torre Hernandez JM, Garcia Camarero T, Baz Alonso JA, et al. Outcomes of predefined optimisation criteria for intravascular ultrasound guidance of left main stenting. EuroIntervention. 2020;16:210-217.
4. Holm NR, Andreasen LD, Neghabat O, et al.;OCTOBER Trial Group. OCT or Angiography Guidance for PCI in Complex Bifurcation Lesions. N Engl J Med. 2023;389:1477-1487.
5. Karim K, Akbar MR, Pramudyo M, Martha JW. Intravascular Ultrasound versus Angiography Guided Drug Eluting Stent Implantation in Patients with Left Main Coronary Artery Disease —A Systematic Review and Meta-Analysis. Rev Cardiovasc Med. 2024;25:32.
6. Kinnaird T, Johnson T, Anderson R, et al. Intravascular Imaging and 12-Month Mortality After Unprotected Left Main Stem PCI:An Analysis From the British Cardiovascular Intervention Society Database. JACC Cardiovasc Interv. 2020;13:346-357.
7. Kim BK, Shin DH, Hong MK, et al. Clinical Impact of Intravascular Ultrasound-Guided Chronic Total Occlusion Intervention With Zotarolimus-Eluting Versus Biolimus-Eluting Stent Implantation:Randomized Study. Circ Cardiovasc Interv. 2015;8:e002592.
8. Hong SJ, Kim BK, Shin DH, et al. Effect of Intravascular Ultrasound-Guided vs Angiography-Guided Everolimus-Eluting Stent Implantation:The IVUS-XPL Randomized Clinical Trial. JAMA. 2015;314:2155-2163.
9. Gao XF, Ge Z, Kong XQ, et al.;ULTIMATE Investigators. 3-Year Outcomes of the ULTIMATE Trial Comparing Intravascular Ultrasound Versus Angiography-Guided Drug-Eluting Stent Implantation. JACC Cardiovasc Interv. 2021;14:247-257.
10. Lee JM, Kim O, Song YB, et al. RENOVATE COMPLEX-PCI Investigators. Intravascular Imaging- vs Angiography-Guided Complex PCI:5-Year Outcomes From a Randomized Trial. J Am Coll Cardiol. 2026;87:2099-2113.
11. Diletti R, Daemen J, Faurie B, et al.;for the IVUS-CHIP Investigators. Intravascular Ultrasound-Guided or Angiography-Guided Complex High-Risk PCI. N Engl J Med. 2026. https://doi.org/10.1056/NEJMoa2601521.
12. De Maria GL, Testa L, de la Torre Hernandez JM, et al. A multi-center, international, randomized, 2-year, parallel-group study to assess the superiority of IVUS-guided PCI versus qualitative angio-guided PCI in unprotected left main coronary artery (ULMCA) disease:Study protocol for OPTIMAL trial. PLoS One. 2022;17:e0260770.
13. Kang SJ, Ahn JM, Song H, et al. Comprehensive intravascular ultrasound assessment of stent area and its impact on restenosis and adverse cardiac events in 403 patients with unprotected left main disease. Circ Cardiovasc Interv. 2011;4:562-569.
14. Maehara A, Mintz G, Serruys P, et al. Impact of final minimal stent area by IVUS on 3-year outcome after PCI of left main coronary artery disease:the EXCEL trial. J Am Coll Cardiol. 2017;69:S963.
15. Kim JH, Kang DY, Ahn JM, et al. Optimal Minimal Stent Area and Impact of Stent Underexpansion in Left Main Up-Front 2-Stent Strategy. Circ Cardiovasc Interv. 2024;17:e013006.
16. Kim JH, Kang DY, Ahn JM, et al. Optimal minimal stent area after crossover stenting in patients with unprotected left main coronary artery disease. EuroIntervention. 2025;21:1069-1080.
17. De la Torre Hernandez JM. Evolving cutoff values for optimising left main stenting with intravascular imaging. EuroIntervention. 2025;21:e1043-e1044.
18. Johnson TW, Gonzalo N, De la Torre Hernandez JM, et al. Intracoronary imaging for left main percutaneous coronary intervention:a clinical consensus statement of the European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the ESC and the European Bifurcation Club (EBC). Eur Heart J. 2026. https://doi.org/10.1093/eurheartj/ehag353.
19. Ali ZA, Landmesser U, Maehara A, et al.;ILUMIEN IV Investigators. Optical Coherence Tomography-Guided versus Angiography-Guided PCI. N Engl J Med. 2023;389:1466-1476.
Drug-coated balloon (DCB) is a therapeutic tool that has been available for the treatment of coronary artery disease for more than 20 years. Initially developed for in-stent restenosis,1,2 its use has expanded given its potential in native coronary lesions. In Spain, annual registry data show a marked increase in DCB utilization, from approximately 4% of percutaneous coronary interventions in 2012 to 15% in the most recent report,3 accompanied by a parallel decline in drug-eluting stent (DES) use. This growing adoption over the past few years has been driven largely by the “leave nothing behind” concept rather than by robust clinical evidence. Accordingly, American clinical practice guidelines do not recommend DCB over DES,4 and European clinical practice guidelines restrict their indication to in-stent restenosis.5 Nevertheless, DCB use has extended to increasingly complex clinical scenarios, including small vessels, diffuse disease, chronic total coronary occlusions, calcified lesions, acute coronary syndrome, patients at high bleeding risk, and bifurcation lesions.
In bifurcation lesions, 2 principal approaches have been described. The pure DCB technique involves treatment of both the main vessel and the side branch (SB) with DCB, and is limited to the SB in Medina 0,0,1 lesions. In contrast, the hybrid technique combines DES implantation in the main vessel with DCB dilation in the SB. Two variants of the hybrid approach exist: SB predilation with DCB before DES implantation in the main vessel, and SB postdilation with DCB after DES deployment in the main vessel through the stent struts. The former allows direct access to the SB with the DCB without compromising drug delivery but may be affected by carina shift following DES implantation, potentially requiring repeat dilation of the new segment treated with DCB. The latter carries the risk of DCB drug loss when crossing the stent struts, and the need to correct the deformation induced in the DES when dilating the SB.
The hybrid strategy has been evaluated in multiple observational studies for years. Its rationale lies in the ability of DCB to reduce late lumen loss through an antiproliferative effect in SB lesions, thereby decreasing restenosis, and the need for repeat revascularization, with a potential reduction in clinical events during follow-up. A reduction in late lumen loss at the SB ostium has indeed been demonstrated in most studies.6-9 However, the translation of this favorable effect into fewer clinical events is more difficult, with most studies reporting neutral results. The randomized DCB-BIF study, which had sufficient statistical power, compared the hybrid strategy with the provisional stenting technique.10 Although a significant reduction in events during follow-up was demonstrated, this was driven by myocardial infarction (periprocedural and spontaneous) and not by the need for repeat target lesion revascularization. After excluding periprocedural myocardial infarctions, no significant differences in major adverse events were observed at 1 year (5.1% vs 2.6%;
Regarding the use of the pure DCB strategy, there is still no evidence available, and we will have to wait for the results of the EBC-DCB study [NCT06822322], which is still in the patient inclusion phase.
In a recent article published in
This study is timely, given the ongoing controversy in this field. However, several limitations warrant consideration beyond those already discussed. The use of the proximal optimization technique was notably low, particularly in the control group (only 12%). With the exception of Medina 0,0,1 bifurcations, this maneuver is recommended and generally considered mandatory in current consensus documents from the European Bifurcation Club.15 The presence of significant differences between the 2 groups penalizes the control group. Another noteworthy finding is the absence of myocardial infarction and target lesion revascularization in the DCB group over a 3-year period. Given the prolonged enrollment period (approximately 6 years), incomplete data capture at the time of analysis cannot be excluded, and some events may have been underreported.
Overall, this study provides relevant insights into a highly topical and debated issue, and the authors should be acknowledged for their effort in comprehensive data collection and long follow-up. Although the impact of DCB on clinical event reduction remains controversial, these findings support the potential clinical utility of this therapeutic strategy in the management of bifurcation lesions.
FUNDING
None declared.
CONFLICTS OF INTEREST
M. Pan declares having received minor payments for lectures from Abbott and Boston Scientific.
REFERENCES
1. Scheller B, Hehrlein C, Bocksch W, et al. Treatment of coronary in-stent restenosis with a paclitaxel-coated balloon catheter. N Engl J Med. 2006;355:2113-2124.
2. Alfonso F, Scheller B. State of the art: balloon catheter technologies —drug-coated balloon. EuroIntervention. 2017;13:680-695.
3. Bastante T, Arzamendi D, Martín-Moreiras J, Cid-Álvarez AB;ACI-SEC. Spanish cardiac catheterization and coronary intervention registry. 34th official report of the Interventional Cardiology Association of the Spanish Society of Cardiology (1990-2024). Rev Esp Cardiol. 2025;78:992-1003.
4. Neumann FJ, Sousa-Uva M, Ahlsson A, et al.;ESC Scientific Document Group. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40:87-165.
5. Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79:e21-e129.
6. Herrador JA, Fernandez JC, Guzman M, Aragon V. Drug-eluting vs. conventional balloon for side branch dilation in coronary bifurcations treated by provisional T stenting. J Interv Cardiol. 2013;26:454-462.
7. López Mínguez JR, Nogales Asensio JM, Doncel Vecino LJ, et al. A prospective randomised study of the paclitaxel-coated balloon catheter in bifurcated coronary lesions (BABILON trial): 24-month clinical and angiographic results. EuroIntervention. 2014;10:50-57.
8. Jing QM, Zhao X, Han YL, et al. A drug-eluting Balloon for the trEatment of coronarY bifurcatiON lesions in the side branch: a prospective multicenter ranDomized (BEYOND) clinical trial in China. Chin Med J (Engl). 2020;133:899-908.
9. Dohi T, Ishihara T, Kida H, et al. Comparison of drug-coated versus conventional balloons for the side branch of the bifurcation lesion —multicenter randomized controlled study —(OCVC-BIF): Design and rationale. Cardiovasc Revasc Med. 2025;81:57-61.
10. Gao X, Tian N, Kan J, et al. Drug-Coated Balloon Angioplasty of the Side Branch During Provisional Stenting: The Multicenter Randomized DCB-BIF Trial. J Am Coll Cardiol. 2025;85:1-15.
11. Rocchetti M, Tua L, Cereda A, et al. Drug-Coated Balloons Versus Non-Coated Balloons for Side Branch Treatment in Bifurcation Lesions: A Systematic Review and Meta-Analysis. Catheter Cardiovasc Interv. 2025;106:530-539.
12. Dillen DMM, van Beek KAJ, Vermeer AJE, et al. Hybrid drug-coated balloon strategy for coronary bifurcation lesions: a systematic review and meta-analysis. BMJ Open. 2026;16:e114024.
13. Quevedo-Candela F, Cieza T, Ruhl A, Nolte C, Bertrand OF. Drug-Coated Balloons Versus Drug-Eluting Stents for Side Branch Lesions in Coronary Bifurcations: An Updated Comparative Meta-Analysis. Am J Cardiol. 2026. https://doi.org/10.1016/j.amjcard.2026.03.041.
14. Valencia J, Torres-Mezcua F, Herrero-Brocal M, et al. Drug-coated balloon for the side branch compared with conventional strategy in left anterior descending-diagonal bifurcation lesions. REC Interv Cardiol. 2026. https://doi.org/10.24875/RECICE.M26000574.
15. Burzotta F, Lassen JF, Lefèvre T, et al. Percutaneous coronary intervention for bifurcation coronary lesions: the 15th consensus document from the European Bifurcation Club. EuroIntervention. 2021;16:1307-1317.

Paclitaxel-coated balloons (PCB) have long dominated the drug-coated balloon (DCB) landscape, supported by favourable pharmacokinetics and extensive randomised evidence.1 Sirolimus, by contrast, is inherently less lipophilic and biologically dependent on sustained arterial wall exposure, rendering simple balloon-coating strategies suboptimal. Consequently, early-generation sirolimus- coated balloons (SCB) were met with skepticism regarding effective drug transfer and durable tissue retention. Signals of attenuated late lumen gain with SCB in early randomised comparisons, including the TRANSFORM I, highlighted these limitations.2 However, subsequent randomised trials in both de novo lesions and in-stent restenosis have failed to demonstrate a meaningful difference in late lumen loss versus PCB.3 Crucially, in contemporary meta-analyses, even when modest angiographic differences are observed, these have not translated into significant differences in clinically relevant outcomes, including target lesion failure, repeat revascularisation, or myocardial infarction.4,5
The SELUTION SLR platform (Cordis, United States) is a deliberate evolution in this field, incorporating a proprietary phospholipid carrier and micro-reservoir architecture designed to enable controlled and prolonged sirolimus release with minimal drug loss.6 The key question is whether this technological maturation translates into meaningful therapeutic equivalence.
In a recent paper published in REC: Interventional Cardiology, Faria et al. present a prospective single-center registry of 257 patients with 316 de novo lesions and provide a contemporary head-to-head comparison between the SELUTION SLR and the established Pantera Lux (Biotronik, Germany) PCB.7 The authors are to be congratulated for assembling a real-world cohort that included both acute and chronic coronary syndromes, a high prevalence of bifurcation disease, and frequent hybrid strategies. At 12 months, clinical outcomes were reassuringly low and statistically similar between devices, with a MACE rate of 5.8% and a target lesion failure rate of 3.8% overall. Target lesion revascularisation occurred in fewer than 1% of lesions.
Several aspects of the study merit recognition. The registry was prospective with complete 1-year follow-up. The investigators appropriately avoided multivariable or propensity modelling in the setting of low event counts, thereby avoiding the risk of statistical overreach. Lesion preparation was systematic, imaging use was encouraged, and bailout criteria was clearly defined, reflecting thoughtful procedural strategy.
Nevertheless, these findings do require careful interpretation. The treated population was predominantly small-vessel disease, with a mean DCB diameter of 2.25 mm and only 18.7% of vessels ≥ 3.0 mm. As such, these findings primarily reinforce the established role of DCB in small-calibre arteries rather than expanding indications into larger vessels. Although subgroup analysis in larger vessels did not reveal excess adverse events, bailout stenting was notably higher in ≥ 3 mm arteries (18.6%), suggesting that operator thresholds for permanent scaffolding may differ by vessel calibre. The observed reduction in mild, non–flow-limiting dissections with the SELUTION SLR (6.7% vs 14.7%) warrants careful interpretation. Types A-B dissections are expected following DCB angioplasty and are typically benign when TIMI 3 flow is preserved.8,9 Whether this difference reflects intrinsic coating behaviour, mechanical interaction, lesion preparation variability, or simply procedural nuance cannot be determined in the absence of randomisation or imaging adjudication. Similarly, the absence of no-reflow events in the SCB arm compared with 2.7% in the PCB group is hypothesis-generating but numerically small. The small number of events precludes definitive mechanistic interpretation.
Taken together, what conclusion can be reasonably drawn from these data? This study demonstrates that the SELUTION SLR platform is safe and clinically comparable to an established PCB in a predominantly small-vessel, real-world population. It does not demonstrate superiority in clinical endpoints. The procedural signals—fewer mild dissections and less no-reflow—are intriguing but remain angiographic observations rather than outcome-altering findings.
In this context, the evolution of sustained-release technology appears incremental rather than revolutionary. Importantly, these findings sit alongside a growing body of randomised evidence. In SELUTION DeNovo RCT, a sirolimus-eluting balloon strategy demonstrated non-inferiority to contemporary drug-eluting stents in selected de novo lesions, supporting the feasibility of a “leave-nothing-behind” approach.10 Whether such platforms will ultimately displace paclitaxel balloons or simply broaden therapeutic choice, remains to be determined by longer-term and adequately powered comparative trials.
For now, the balance has not decisively shifted—but the field is more competitive.
FUNDING
No external funding was received for this paper.
CONFLICTS OF INTEREST
R. Natarajan and K. Chandrasekharan have no conflict of interests and have received no funding related to this study. S.C. Eccleshall received speaker fees and acts as a consultant for B. Braun, Medtronic, Cordis and MedAlliance, and received grants for investigator- initiated research from B. Braun.
REFERENCES
1. Scheller B, Vukadinovic D, Jeger R, et al. Survival After Coronary Revascularization With Paclitaxel-Coated Balloons. J Am Coll Cardiol. 2020;75:1017–1028.
2. Ninomiya K, Serruys PW, Colombo A, et al. A Prospective Randomized Trial Comparing Sirolimus-Coated Balloon With Paclitaxel-Coated Balloon in De Novo Small Vessels. JACC Cardiovasc Interv. 2023;16:2884–2896.
3. Scheller B, Mangner N, Jeger RV, et al. A randomised trial of sirolimus- versus paclitaxel-coated balloons for de novo coronary lesions. EuroIntervention. 2024;20:e1322–e13299.
4. Liu H, Li Y, Fu G, et al. Sirolimus- vs Paclitaxel-Coated Balloon for the Treatment of Coronary In-Stent Restenosis. JACC:Cardiovascular Interventions. JACC Cardiovasc Interv. 2025;18:963–971.
5. Rath S, Khan A, Khan H, et al. Assessing paclitaxel-coated vs sirolimus-coated balloon angioplasty for coronary artery diseases:A systematic review and meta-analysis. World J Cardiol. 2025;17:112018.
6. Spaulding C, Krackhardt F, Bogaerts K, et al. Comparing a strategy of sirolimus-eluting balloon treatment to drug-eluting stent implantation in de novo coronary lesions in all-comers:Design and rationale of the SELUTION DeNovo Trial. Am Heart J. 2023;258:77–84.
7. Faria D, Neves D, Hamann L, et al. SELUTION SLR sirolimus-eluting balloon compared with the Pantera Lux paclitaxel drug-coated balloon in the management of de novo coronary lesions. REC Interv Cardiol. 2026. https://doi.org/10.24875/RECICE.M25000551.
8. Natarajan R, Corballis N, Merinopoulos I, Vassiliou VS, Eccleshall SC. Coronary Artery Dissection Series –Back to the Future II:The ARM Strategy (Avoid, Recognize and Manage Dissections) in Drug-coated Balloon Angioplasty. 2025. Available at: https://touchcardio.com/cardiovascular-disease/journal-articles/coronary-artery-dissection-series-back-to-the-future-ii-the-arm-strategy-avoid-recognize-and-manage-dissections-in-drug-coated-balloon-angioplasty/. Accessed 22 Feb 2026.
9. Natarajan R, Corballis N, Merinopoulos I, Vassiliou VS, Eccleshall SC. Coronary Dissection –Back to the Future –Finding Good in the Bad!2024. Available at: https://touchcardio.com/interventional-cardiology/journal-articles/coronary-dissection-back-to-the-future-finding-good-in-the-bad/. Accessed 22 Feb 2026.
10. Safirstein J. SELUTION DeNovo:PCI With a Sirolimus-Eluting Balloon and Provisional Stenting Shows Comparable Outcomes to Routine DES Implantation for Treatment of De Novo Coronary Lesions—Coverage of TCT 2025 |SCAI, 2025. Available at: https://www.scai.org/selution-denovo-pci-sirolimus-eluting-balloon-and-provisional-stenting-shows-comparable-outcomes. Accessed 22 Feb 2026.
Secondary ventricular mitral regurgitation (MR) is a common valvular disorder resulting from ventricular dilation or dysfunction rather than primary leaflet abnormalities.1 Progressive left ventricular (LV) dilation and spherical reshaping displace the papillary muscles laterally and apically, increasing leaflet tethering forces and restricting systolic closure. Moreover, annular dilation and flattening reduce leaflet coaptation, while impaired LV contractility diminishes closing forces across the valve. This imbalance between tethering and closing forces leads to incomplete leaflet apposition and regurgitant flow into the left atrium during systole. Thus, the regurgitation reflects geometric distortion of the mitral apparatus secondary to LV remodeling rather than intrinsic leaflet pathology.
Moderate-to-severe regurgitation is present in approximately one-quarter to one-third of patients with chronic systolic dysfunction, depending on the population studied and the echocardiographic definitions applied.2 Its prevalence increases with progressive LV dilation, prior myocardial infarction, longer duration of heart failure, and inadequate reverse remodeling despite guideline- directed medical therapy (GDMT). Beyond its prevalence, secondary MR carries substantial prognostic implications. Numerous observational analyses have demonstrated that moderate-to-severe secondary MR is independently associated with increased all-cause and cardiovascular mortality, even after adjustment for LV ejection fraction and clinical markers of disease severity.3 The hemodynamic burden imposed by regurgitant volume increases left atrial and pulmonary venous pressures, promoting congestion, recurrent heart failure hospitalizations, and progressive right ventricular dysfunction. Patients with significant secondary ventricular MR also exhibit reduced functional capacity and poorer quality of life.
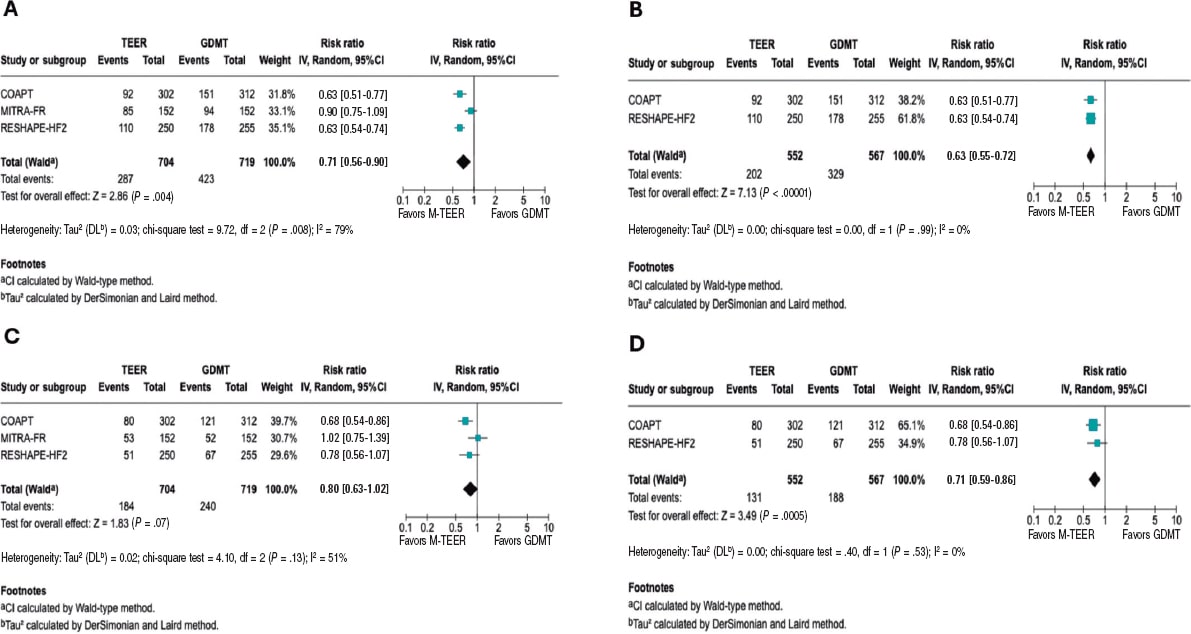
Historically, mitral valve surgery has been considered the main interventional approach for patients with significant secondary MR. Over the past few decades, several studies, including randomized clinical trials and meta-analyses, have evaluated the role of mitral valve surgery in this setting. These investigations showed that although surgery can reduce MR severity and, in some cases, promote reverse ventricular remodeling, evidence supporting a survival benefit vs optimal medical therapy alone remained limited.4 On the other hand, transcatheter interventions offer a less invasive alternative to open-heart surgery. Among these, percutaneous procedures, particularly transcatheter edge-to-edge repair (TEER), have been increasingly adopted. As supporting evidence grew accumulated, mitral TEER has been widely implemented in contemporary interventional practice worldwide. In recent years, 3 randomized clinical trials have compared GDMT plus mitral TEER with GDMT alone in patients with secondary significant MR. In a recent study published in REC: Interventional Cardiology, Paulino-González et al.5 conducted a systematic review and meta-analysis of the main clinical endpoints evaluated in randomized clinical trials comparing mitral TEER and optimal medical therapy thus far. They conducted a systematic search of electronic databases and identified 3 randomized clinical trials including more than 1400 patients overall. The primary endpoints were all-cause mortality and heart failure hospitalization. An exploratory analysis excluding patients from the MITRA-FR study6 was also performed to reduce heterogeneity between study populations. Overall, there was a trend towards lower all-cause mortality which did not meet statistical significance (risk ratio [RR], 0.80; 95% confidence interval [95%CI], 0.63–1.02; P = .07). Heart failure-related hospitalization rates were signifi- cantly lower among patients who underwent mitral TEER (RR, 0.71; 95%CI, 0.56-0.90; P = .004). In the exploratory analysis excluding MITRA-FR patients, both all-cause mortality (RR, 0.71; 95%CI, 0.59–0.86; P = .0005) and heart failure hospitalization (RR, 0.63; 95%CI, 0.55-0.72; P < .00001) were significantly reduced with the percutaneous approach, with minimal heterogeneity between studies. The reduction in the composite endpoint of heart failure-related hospitalization or death with mitral TEER was consistent among patients presenting grade 3+ and grade 4+ MR at baseline. There were no significant differences between mitral TEER and optimal medical treatment in terms of safety endpoints, including stroke and myocardial infarction.
Several aspects of this meta-analysis merit further consideration:
- – Differences in baseline clinical features across the included studies. When the COAPT trial7 was published in 2018, it provided compelling evidence that TEER reduced both heart failure-related hospitalizations and mortality in carefully selected patients with symptomatic heart failure and moderate-to-severe or severe secondary MR. Importantly, COAPT required rigorous optimization of GDMT before enrollment and objective confirmation of persistent, significant MR. In contrast, the MITRA-FR trial, reported in the same year, failed to demonstrate a reduction in death or heart failure-related hospitalization.6 At first glance, the results seemed contradictory to those of COAPT. However, closer examination reveals fundamental differences in trial design and patient phenotype. MITRA-FR applied broader MR severity thresholds and enrolled patients with substantially larger LV volumes. In these patients, MR severity was more proportionate to the degree of ventricular remodeling, suggesting that regurgitation was primarily a consequence, rather than a cause, of advanced myocardial disease.8 The RESHAPE-HF2 trial9 aimed to evaluate this comparison in a contemporary therapeutic landscape. Conducted in the era of more comprehensive GDMT, including greater uptake of sacubitril/valsartan, mineralocorticoid receptor antagonists, and SGLT2 inhibitors, its findings, showing reduction in heart failure events and symptomatic improvement, with a less pronounced mortality effect than COAPT), suggest that TEER may confer benefit across a broader spectrum of MR severity than that represented in COAPT, albeit with a smaller effect size.
- – Grades of residual MR after percutaneous intervention. As the authors stated in the discussion,5 MR reduction was less effective in the MITRA-FR trial. In conclusion, MR reduction to ≤ 2+ in MITRA FR (75.6% MR ≤ 2+ at discharge) was markedly lower than that obtained in COAPT (94.8% MR ≤ 2+ at 12 months) and the RESHAPE HF2 (90.4% MR ≤ 2+ at 12 months). In MITRA-FR the degree of MR reduction was modest relative to what has been observed in other studies, with many patients remaining with moderate residual regurgitation. Because baseline regurgitation in MITRA-FR tended to be less severe, based on effective regurgitant orifice area and regurgitant volume thresholds, and proportionate to LV dilation, the capacity of TEER to achieve a large absolute reduction in regurgitant volume was inherently limited. Analyses of residual MR in RESHAPE-HF2 suggest that the degree and durability of regurgitation correction remained an important determinant of clinical response: patients with sustained mild or lesser degrees of MR demonstrated the most favorable clinical outcomes, whereas those with persistent moderate regurgitation derived attenuated benefit.10 Additional factors may also have influenced trial outcomes, including increasing operator experience and advances in device technology over time. For example, the G4 generation of the MitraClip system (Abbott, United States) utilized in the RESHAPE-HF2 trial enables independent leaflet grasping and provides a wider range of device sizes, ultimately enabling tailored device selection potentially improving treatment of complex mitral valve anatomies.
Overall, Paulino-González et al.5 should be commended for their work and contribution to the field. Consistent with the findings of the abovementioned trials, this meta-analysis supports the fact that secondary ventricular MR is not merely an epiphenomenon of LV dysfunction but a modifiable contributor to adverse outcomes. Moreover, mitral TEER in combination to GDMT clearly constitute the best therapeutic strategy for improving clinical prognosis.
FUNDING
None declared.
CONFLICTS OF INTEREST
None declared.
REFERENCES
1. Huang AL, Dal-Bianco JP, Levine RA, Hung JW. Secondary Mitral Regurgitation:Cardiac Remodeling, Diagnosis, and Management. Struct Heart. 2022;7:100129.
2. Zhao C, Jin C, Shen Y, Lin X, Yu Y, Xiang M. The Prevalence and Characteristics of Mitral Regurgitation in Heart Failure:A Chart Review Study. Rev Cardiovasc Med. 2022;23:235.
3. Sannino A, Smith RL, Schiattarella GG, Trimarco B, Esposito G, Grayburn PA. Survival and Cardiovascular Outcomes of Patients With Secondary Mitral Regurgitation:A Systematic Review and Meta-analysis. JAMA Cardiol. 2017;2:1130.
4. Eapen SR, Zaky MH, Kostibas MP, Robich MP. Secondary mitral regurgitation surgical management:a narrative review. Cardiovasc Diagn Ther. 2024;14:958-973.
5. Paulino-González D, Pardiño-Vega MA, García-Loera AL, Zúñiga-Montaño KP, Navarro-Martínez DA. Transcatheter mitral edge-to-edge repair vs optimal medical therapy in secondary mitral regurgitation:a meta-analysis. REC Interv Cardiol. 2025. https://doi.org/10.24875/RECICE.M25000558.
6. Obadia JF, Messika-Zeitoun D, Leurent G, et al. Percutaneous repair or medical treatment for secondary mitral regurgitation. N Engl J Med. 2018;379:2297-2306.
7. Stone GW, Lindenfeld JA, Abraham WT, et al. Transcatheter mitral-valve repair in patients with heart failure. N Engl J Med. 2018;379:2307-2318.
8. Grayburn PA, Sannino A, Packer M. Proportionate and Disproportionate Functional Mitral Regurgitation:A New Conceptual Framework That Reconciles the Results of the MITRA-FR and COAPT Trials. JACC Cardiovasc Imaging. 2019;12:353-362.
9. Anker SD, Friede T, von Bardeleben RS, et al. Transcatheter Valve Repair in Heart Failure with Moderate to Severe Mitral Regurgitation. N Engl J Med. 2024;391:1799-1809.
10. Ponikowski P, Friede T, von Bardeleben RS, et al. Hospitalization of Symptomatic Patients With Heart Failure and Moderate to Severe Functional Mitral Regurgitation Treated With MitraClip:Insights From RESHAPE-HF2. J Am Coll Cardiol. 2024;84:2347-2363.
Balloon failure during percutaneous coronary intervention (PCI), which occurs particularly in severely stenotic and extensively calcified lesions, remains one of the most complex and frustrating scenarios for the interventional cardiologist. In addition, initial balloon failure is associated with prolonged procedures, greater resource consumption, and an increased risk of complications.1 All this occurs despite the development and availability of different plaque-modification techniques, including excimer laser coronary atherectomy (ELCA).2,3
Across different studies over the years, the concept of balloon failure has encompassed various scenarios, including both uncrossable and undilatable lesions. This terminological imprecision may affect the interpretation of the available results from these studies, which in turn may have an impact on decision-making in clinical practice.
In the context of PCI for complex uncrossable or undilatable lesions, a better understanding of the underlying anatomical mechanisms is essential. This may be facilitated by a more systematic use of intracoronary imaging modalities. Nevertheless, dedicated studies in this setting are clearly needed. Their results may help improve lesion characterization and optimize the therapeutic approach through more appropriate selection of plaque-modification techniques.2,3
In a recent article published in REC: Interventional Cardiology, Jurado-Román et al.4 present the design of the LUDICO study (Coronary laser in undilatable and uncrossable lesions; NCT07206082), a prospective, multicenter, single-arm observational trial to evaluate the safety and efficacy profile of ELCA in 230 patients with an indication for PCI and lesions in which balloon failure has occurred. The main strength of the study lies in its methodological approach, as it explicitly distinguishes between uncrossable and undilatable lesions. This distinction may contribute to a better understanding of the role and positioning of this technique, given that in both scenarios—after failure to cross or dilate the lesion with a balloon—ELCA would represent the first plaque-modification strategy to be used. Another relevant aspect of the study is the recommendation to use intracoronary imaging, specifically optical coherence tomography. This approach allows assessment not only of procedural success but also of the structural changes induced in the lesion. Currently, these changes have been poorly characterized in the context of ELCA, particularly in cases of in-stent restenosis.5
The most evident limitation of the study, appropriately acknowledged by the authors, is the absence of a control group, which makes direct comparison with other plaque-modification techniques impossible. A comparison between these techniques has recently been performed in PCI for complex lesions in the randomized ROLLER COASTR-EPIC22 study (Rotational atherectomy, lithotripsy or laser for the treatment of calcified stenosis).6 Such a comparison could also have been of interest in the specific context of the study under discussion. Another aspect worth noting is that the definition of an undilatable lesion is based on an objective criterion (balloon expansion < 80% after 1:1 noncompliant balloon inflation at 18 atm). In contrast, a stricter or more precise definition of an uncrossable lesion is lacking. In this study, an uncrossable lesion was defined after failure to advance a low-profile balloon despite adequate guide support at the operator’s discretion. This approach may introduce a degree of variability that should be considered when interpreting the results.
From a broader perspective, the use of ELCA in clinical practice remains limited. This may be partly explained, in addition to the relatively scarce scientific evidence, by a certain paradox: although the technique is technically straightforward from the operator’s standpoint, its application entails a degree of conceptual complexity. Specifically, the procedural parameters must be adjusted according to the clinical scenario in which the device is used. This may help explain its relatively limited adoption in catheterization laboratories across Spain.6 Indeed, the safety and efficacy of ELCA largely depend on several procedural decisions that remain incompletely standardized. These include the optimal timing of ELCA use during the procedure, the selection of catheter diameter, the potential combination with other plaque-modification techniques, and the appropriate selection and modulation of device parameters. These parameters include energy intensity and frequency, application duration, total number of pulses, and even the adjunctive use of contrast medium (amplification).7 Table 1 proposes a practical framework for adjusting ELCA parameters according to the clinical context in which it is used. In conclusion, although ELCA is not technically demanding from an operator-handling perspective, its optimal use requires a certain degree of experience. Maximizing its benefits depends on a thorough understanding of the predominant mechanism underlying each lesion, a process that can be facilitated by the performance and appropriate interpretation of intracoronary imaging.
Table 1. Proposed excimer laser configuration in different scenarios
| Clinical scenario | Frequency (Hz) | Energy (mJ/mm2) | Adjunctive use of contrast | Practical comments |
|---|---|---|---|---|
| Underexpanded stent | 60-80 (high) | 60–80 (high) | No, according to device labeling. Observational studies support the usefulness of contrast amplification in lesions resistant to ELCA with saline solution | Start with high parameters if saline solution is used. If contrast is used, it is prudent to initially reduce ELCA parameters (frequency 25–40 Hz, energy 30–45 mJ/mm2), and they may be progressively increased with caution |
| Severely calcified lesion | 60-80 (high) | 60–80 (high) | No, according to device labeling. Limited evidence supports the potential usefulness of contrast in lesions resistant to ELCA with saline solution | Start with high parameters if saline solution is used. The use of contrast is not well established; if used, it is reasonable to consider an initial reduction in frequency and energy, which may then be progressively increased with caution |
| Thrombotic lesion | 25-40 (low/medium) | 30–60 (low/medium) | No | In “pure” thrombotic lesions, low energy and frequency are generally sufficient. In cases of thrombus with a large plaque burden, energy and frequency parameters may be gradually increased |
|
ELCA, excimer laser coronary angioplasty. |
||||
When examining the available evidence on ELCA, which remains generally limited, the technique has demonstrated clearer usefulness in certain specific scenarios.8 One of these is the treatment of uncrossable lesions,9 in which ELCA can advance over the same angioplasty guidewire. This represents a clear advantage and suggests that ELCA could be considered one of the preferred plaque-modification techniques in this setting. Moreover, ELCA may facilitate subsequent device advancement in extremely hostile anatomies and assist in the management of undilatable lesions, particularly those related to stent underexpansion. In these cases, its ability to modify both the underlying plaque and resistant neointimal tissue may allow more effective subsequent expansion.10 In another challenging scenario—the treatment of lesions with a high thrombotic burden—ELCA has also shown potential usefulness.11 Supporting this application, a contemporary series of patients undergoing primary PCI demonstrated that ELCA can “vaporize” thrombotic material, reducing it to microscopic particles and improving coronary flow, thereby facilitating safer and more effective stent implantation.12
FUNDING
None declared.
CONFLICTS OF INTEREST
A. Pernigotti declares having received consulting fees from Iberhospitex and B. Braun. M. Mohandes declares having received consulting fees from Philips. J.L. Ferreiro declares having received speaker or consulting fees from Eli Lilly Co, Daiichi Sankyo, Inc., AstraZeneca, Pfizer, Abbott, Boston Scientific, Boehringer Ingelheim, Bristol-Myers Squibb, Rovi, Terumo, Sahajanand Medical Tech- nologies, Iberhospitex, and Ferrer, and a research grant from AstraZeneca.
REFERENCES
1. Pesarini G, Hellig F, Seth A, Shlofmitz RA, Ribichini FL. Percutaneous coronary intervention for calcified and resistant lesions. EuroIntervention. 2025;21:339-355.
2. Riley RF, Patel MP, Abbott JD, et al. SCAI expert consensus statement on the management of calcified coronary lesions. J Soc Cardiovasc Angiogr Interv. 2024;3:101259.
3. Jurado-Román A, Gómez-Menchero A, Gonzalo N, et al. Plaque modification techniques to treat calcified coronary lesions. Position paper from the ACI-SEC. REC Interv Cardiol. 2023;5:46-61.
4. Jurado-Román A, Zubiaur J, Basile M, et al. Design of the LUDICO study:effectiveness and safety of coronary laser in undilatable or uncrossable lesions. REC Interv Cardiol. 2025. https://doi.org/10.24875/RECICE.M25000560.
5. Lee T, Shlofmitz RA, Song L, et al. The effectiveness of excimer laser angioplasty to treat coronary instent restenosis with peri-stent calcium as assessed by optical coherence tomography. EuroIntervention. 2019; 15:279-288.
6. Jurado-Román A, Gómez-Menchero A, Rivero-Santana B, et al. Rotational atherectomy, lithotripsy, or laser for calcified coronary stenosis:the ROLLER COASTR-EPIC22 trial. JACC Cardiovasc Interv. 2025;18:606-618.
7. Mohandes M, Pernigotti A, Moreno C, et al. Coronary laser with simultaneous contrast injection for the treatment of stent underexpansion. Cardiol J. 2024;31:235-242.
8. Golino L, Caiazzo G, CalabròP, et al. Excimer laser technology in percutaneous coronary interventions:Cardiovascular Laser Society's position paper. Int J Cardiol. 2022;350:19-26.
9. Ojeda S, Azzalini L, Suárez de Lezo J, et al. Excimer laser coronary atherectomy for uncrossable coronary lesions:a multicenter registry. Catheter Cardiovasc Interv. 2021;98:1241-1249.
10. Vizzari G, Caminiti R, Ielasi A, et al. Contrast-enhanced excimer laser stepwise approach during PCI for resistant coronary lesions. Catheter Cardiovasc Interv. 2024;104:220-226.
11. Topaz O, Ebersole D, Das T, et al. Excimer laser angioplasty in acute myocardial infarction (the CARMEL multicenter trial). Am J Cardiol. 2004;93:694-701.
12. Mohandes M, Pernigotti A, Torres M, et al. Safety and efficacy profile of excimer laser coronary angioplasty for thrombus removal in STEMI. REC Interv Cardiol. 2026;8:26-31.