
Available online: 09/04/2019
Editorial
REC Interv Cardiol. 2020;2:310-312
The future of interventional cardiology
El futuro de la cardiología intervencionista
Emory University School of Medicine, Atlanta, Georgia, United States
Over the last few years, the risk profile of patients referred to receive a coronary angiography has deteriorated and angiographic findings as well. Therefore, the progressive aging of the population and the development of better techniques to address the complexity of the different angiographic scenarios have conditioned the current situation of percutaneous coronary interventions. The balance between demand and supply in this field is in an ongoing expansion. The management of these delicate situations—which is often competence of cardiac surgery—requires profound knowledge of dedicated techniques and a precise clinical judgment.1-3 This population is often discarded for coronary artery bypass graft surgery. There are times that even percutaneous treatment is denied because of a high clinical risk or unfavorable angiographic profile.
According to different series,4 to this day complex calcified coronary lesions are a common finding in up to 25% to 30% of all percutaneous coronary interventions. De Maria et al.5 published a review on the management of calcified lesions. They portrayed an accurate, contemporary big picture on the treatment of these lesions. The review basically focused on the technologies in intravascular imaging and tools available to solve today’s technical complexities. The authors emphasize that today the objective of percutaneous coronary intervention when treating these lesions is to modify the plaque. If it fails to do so, the procedure is more likely to fail also in the clinical and technical aspects. Clinically because there would be more major complications, and techni- cally because the result would compromise stent expansion and apposition, with the resulting increase in the rates of in-stent restenosis and thrombosis, etc.6,7
Intracoronary lithotripsy (ICL) is the latest technology available for the management of severely calcified lesions. Its mechanism of action has been well described in the document. Basically, ultrasound energy interacts with the atherosclerotic plaque causing vibrations that crack and tear the calcified components of superficial and deep layers. Compared to ablation techniques, since it is based on balloons, it is easy to use and there is a short learning curve. This, together with an early apparent evidence of efficacy, suggests that it will soon become the standard of care for the management of many severely calcified lesions. Similarly, this effect on deep calcium is an important benefit of ICL compared to other plaque-modifying techniques. Compared to rotational and orbital atherectomies, both of which reduce the plaque burden, ICL does not ablate or reduce it but cracks it supposedly improving stent apposition and expansion. The long-term follow-up will confirm whether this is enough to see long-term benefits.
In a recent article published in REC: Interventional Cardiology, Vilalta del Olmo et al.8 commented on their first experience with an ICL device in a high-risk population. Their data provide useful information to assess the role, safety, and feasibility profile of ICL in high-risk patients not included in other studies. The authors report on procedural success and the short-term clinical outcomes of a non-randomized registry. The data published show the utility of ICL improving the clinical and angiographic results of complex patients with advanced, diffuse, multivessel, and calcified atherosclerotic disease. Their patients often presented with critical conditions such as acute coronary syndrome or left ventricular dysfunction.
Since they recruited their first patient, many things have changed and new information has come to light. By performing OCTs in 31 patients, Ali et al.9 confirmed that ICL cracks the calcified arch in 43% of the patients with multiple fractures caused in over 25% of the cases. According to these authors, the efficacy of this technique is proportional to the burden of calcium with a higher rate of calcium fractures (77%) in cases with a higher degree of coronary calcifications. Serious safety issues or technical complications (coronary perforations, important dissections or slow flow/no reflow) have not been reported in the studies. Unlike former reports,10 Vilalta del Olmo et al.8 share encouraging data on a high-risk population with results that are as good as those from other authors.
Although the use of ICL has grown rapidly, the experience published on this device is limited, especially that coming from randomized clinical trials, and some considerations should be made on this regard. The first one is that the navigation capabilities of the device are an important limitation of this technique. Although Vilalta del Olmo et al.8 reported that the ICL balloon crossing rate was 100%, our data show that 89% of the lesions required preconditioning with balloon angioplasty (62%) or rotational atherectomy (27%). Therefore, with the current design of the ICL device, in most cases a coadjuvant technique is required prior to the ICL so it can be used effectively which increases the cost of both procedures. Secondly, since the population of the Disrupt CAD II clinical trial10 included stable patients with concentric lesions, the role of this technique in unstable patients and eccentric calcified lesions should be studied in a randomized controlled trial. Although it is a registry with a small sample size, the data from Vilalta del Olmo et al.8 are encouraging on this regard. In the third place, life often outruns science. Although it is a friendly, easy to use technique, randomized clinical trials should be performed to select the patients and establish the indications. For instance, because of the simultaneous presence of compression and decompression forces (pull and push) and the fact that flow is compromised with ICL, its role should be studied in detail in different clinical and angiographic contexts like ST-segment elevation myocardial infarction, chronic total coronary occlusion via subintimal pathway, patients with pacemakers, etc. Other contexts suggested are patients with in-stent restenosis or to facilitate transfemoral access in patients with transcatheter aortic valve implantation. The fourth consideration to make is closely associated with the previous one and is inherent to any new technique: the lack of data on its use and long-term benefit. With the ICL rapid expansion we run the risk of using it in non-studied settings making it a useless and unsafe technique that may increase the rate of complications or lead to worse results. For example, a few isolated clinical cases have been reported on the role of ICL on in-stent restenosis due to stent underexpansion. The study conducted by Vilalta del Olmo et al.8 did not report on any of this. Maybe the underlying mechanism of restenosis may explain the oberved differences (underexpansion, malapposition, neoatherosclerosis, etc.). Nevertheless, we still need time to study these issues in randomized and controlled clinical trials. ICL balloon tears have also been reported with the resulting added risk.11 In the fifth place, a very important aspect is that ICL may complement other plaque- modifying techniques; its use is feasible and safe with different angioplasty balloons (non-compliant balloons, cutting balloons, and other), rotational atherectomy, etc.12
In conclusion, the ICL is a new, attractive, easy-to-learn and use technique for the management of calcified lesions. Randomized clinical trials and further data are needed to establish its indications and benefits. In the coming future this technique will probably simplify the complex procedures associated with percutaneous coronary interventions and improve the outcomes of patients.
CONFLICTS OF INTEREST
None reported.
REFERENCES
1. Hahn JY, Chun WJ, Kim JH, et al. Predictors and outcome of side branch occlusion after main vessel stenting in coronary bifurcation lesions (COBIS II registry). J Am Coll Cardiol. 2013;62:1654-1659.
2. Burzotta F, Trani C, Todaro D, et al. Prospective Randomized Comparison of Sirolimus- or Everolimus-Eluting Stent to Treat Bifurcated Lesions by Provisional Approach. JACC Cardiovasc Interv. 2011;4:327-335.
3. Dahdouh Z, Roule V, DuguéAE, Sabatier R, LognonéT, Grollier G. Rotational Atherectomy for Left Main Coronary Artery Disease in Octogenarians:Transradial Approach in a Tertiary Center and Literature Review. J Interv Cardiol. 2013;26:173-182.
4. Khattab AA, Otto A, Hochadel M, Toelg R, Geist V, Richardt G. Drug-eluting stents versus bare metal stents following rotational atherectomy for heavily calcified coronary lesions:late angiographic and clinical follow-up results. J Interv Cardiol. 2007;20:100-106.
5. De Maria GL, Scarsini R, Banning AP. Management of Calcific Coronary Artery Lesions. Is it time to change our interventional therapeutic approach?JACC Cardiovasc Interv. 2019;12:1465-1478.
6. Lassen JF, Burzotta F, Banning AP, et al. Percutaneous coronary intervention for the left main stem and other bifurcation lesions:12th consensus document from the European Bifurcation Club. EuroIntervention. 2018;13: 1540-1553.
7. Barbato E, CarriéD, Dardas P, et al. European expert consensus on rotational atherectomy. EuroIntervention. 2015;11:30-36.
8. Vilalta del Olmo V, Rodríguez-Leor O, Redondo A, et al. Intracoronary lithotripsy in a high-risk real-world population. First experience in severely calcified, complex coronary lesions. REC Interv Cardiol. 2019. https://doi.org/10.24875/RECICE.M19000083.
9. Ali ZA, Brinton TJ, Hill JM, et al. Optical coherence tomography characterization of coronary lithoplasty for treatment of calcified lesions:first description. JACC Cardiovasc Imgaging. 2017;10:897-906.
10. Ali ZA, Nef H, Escaned J, et al. Safety and effectiveness of coronary intravascular lithotripsy for treatment of severely calcified stenoses. The Disrupt CAD II Study. Circ Cardiovasc Interv. 2019;12:e008434.
11. López-Lluva MT, Jurado-Román A, Sánchez-Pérez I, Abellán-Huerta J, Lozano Ruíz-Poveda F. Shockwave:Useful But Potentially Dangerous. JACC Cardiovasc Interv. 2019;12:500-501.
12. Jurado-Román A, Gonzálvez A, Galeote G, Jiménez-Valero S, Moreno R. RotaTripsy:Combination of Rotational Atherectomy and Intravascular Lithotripsy for the Treatment of Severely Calcified Lesions. JACC Cardiovasc Interv. 2019;12:e127-e129.
Corresponding author: Unidad de Cardiología Invasiva, Servicio de Cardiología, Hospital La Luz, Maestro Ángel Llorca 8, 28003 Madrid, Spain.
E-mail address: ; (J. Palazuelos).
INTRODUCTION
Therapies for the management of heart failure have been responsible for the great benefit experienced by the population in terms of hope and quality of life. However, they are nothing more than palliative measures that have not resolved the tissue destruction due to this problem whose malignity causes 20 million cardiac deaths worldwide every year.1 Reparative and regenerative medicine was born over 2 decades ago as a biological response to the pressing need for innovation in this field. Its objective is to orchestrate diagnostic tools and therapeutic strategies to restore the molecular, cellular, and tissue health of the cardiac organs damaged.2
Although we can categorically say that the adult heart has a limited capacity for regeneration that depends on the formation of new cardiac muscle, endothelial and smooth muscle cells from a reservoir of existing heart stem cells,3 we can also say that this capacity is marginal and insufficient to repair cardiac organs after sustaining ischemic, toxic, valvular or inherited damage,4 even after physiological aging.5 On the contrary, the myocardium major repair response consists of cellular hypertrophy, in some cases, and replacement of damaged functional tissue by more or less dense fibrous tissue (scar) in most cases. Process that causes the adverse ventricular remodeling that defines the advanced stages of heart failure (systolic ventricular disfunction and cardiac cavity dilatation) of both ischemic and non-ischemic origin (figure 1).
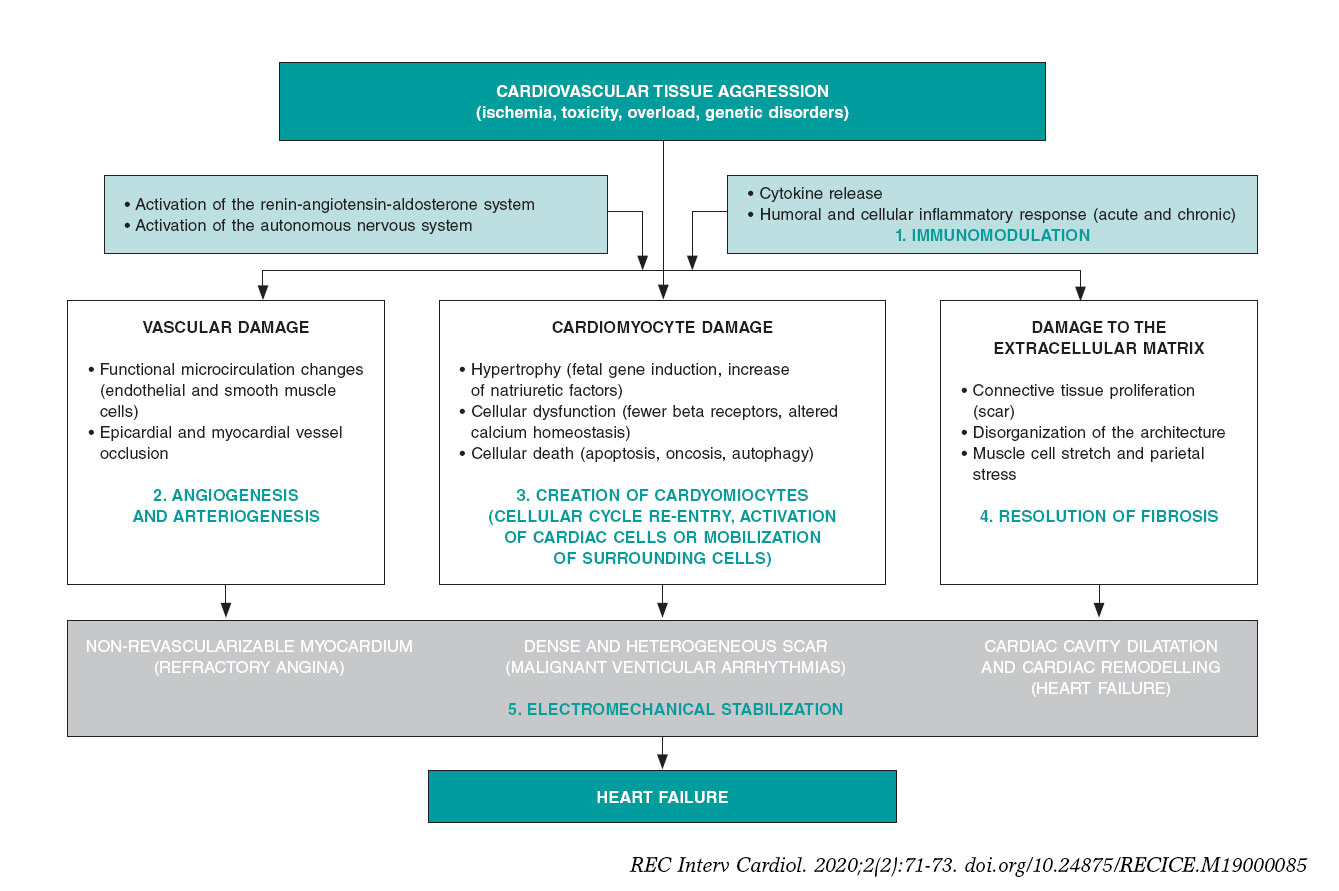
Figure 1. Common biopathological mechanisms indicative of myocardial damage in its vascular, muscular, extracellular components due to different types of tissue damage including the role of neurohormonal compensatory mechanisms and inflammatory response. The bottom shows the 3 main componentes of heart failure (angina, ventricular arrhythmias and ventricular remodelling). In green, the 5 beneficial action mechanisms confirmed by basic, preclinical research through which reparative and regenerative therapies work.
FUNDAMENTALS OF PATHOBIOLOGY AND PRECLINICAL EXPERIENCES
Ever since the 1990s, different types of cells have been studied in the lab in small and large animal models; in chronological order: skeletal myoblasts, hematopoietic end endothelial cells (in most cases harvested from the bone marrow), mesenchymal cells (harvested from bone marrow or adipose tissue), cardiac cells and, recently, embryonic or adult somatic induced pluripotent stem cells.6 All these types of cells have been studied mostly in ischemic heart disease models. In some cases, they have been explored in their allogenic origin of healthy donors of the same species (unlike autologous stem cells that are harvested from the same recipient). As years have gone by, new products have appeared with regenerative or reparative capabilities. Added to gene therapy that has coexisted with cell therapy almost since the beginning, “non-cellular” products have been developed (growth factors, cytokines, proteins or types of ribonucleic acid—microARN). Many of them contained in microvesicles or exosomes that release stem cells or adult cells when they suffer an aggression. These products together with tissue engineering platforms (nanoparticles, gels, and matrices), have recently become part of regenerative medicine; and clinical research is still in its infancy.
Lab experiments and animal model experimentation have been useful because they have proved that: a) the process of myocardial and vascular repair is incredibly complex, both on the molecular, cellular, and tissue levels, which to this day, it is mostly unknown; b) the contribution made by cardiac stem cells to this process is marginal as it is the re-entry process of mature cardiomyocytes to the cellular cycle; c) the beneficial effects of the different products in the myocardium are due to the effect of the proteins and cytokines released by the cells administered (paracrine effect). They are not due to cellular fusion, proliferation or differentiation of these cells into cardiomyocytes, endothelial cells or smooth muscle cells (this has only been confirmed with pluripotent and embryonic cells that are still not used in clinical research); and d) these positive effects include protection from apoptosis, reduced fibrous tissue resulting from myocardial damage, modulation of the inflammation that precedes or is associated with such damage, creation of new blood vessels or formation of small amounts of cardiomyocytes (figure 1).
However, as in other areas of cardiovascular research,7 there has also been a significant “translational gap” in regenerative medicine, and the closer animal research has been to human clinical features the lower the impact of the therapies applied. For example, a meta-analysis of 80 studies showed that in small animal models, the average reduction of the infarction size with different products was 11%.8 However, in large animals, this reduction was only 5%, and it is well-known that in humans it is between 2% and 4%.9 This discrepancy in the results obtained in animals and humans is partly explained by the complexity of cellular processes that regulate cardiac repair, the enormous size difference among species, and the amount of cells (or products) needed to revert it. Other areas with room for improvement and other concepts that require further study regarding preclinical research are doses, administration times, and combination of products. Lastly, the rigor of clinical research is not always thoroughly applied to animal research. This means that it is required to standardize animal models and protocols to obtain and prepare repair products and develop multicenter, randomized and previously registered studies.2
CLINICAL EVIDENCE
The pressing need for innovation in the management of heart failure promoted research in human regenerative therapies early on. Phase I and pilot studies would soon be followed by clinical trials with small numbers of patients. Some products reached phase III in clinical research, particularly in patients with acute myocardial infarction, refractory angina or ischemic and non-ischemic heart failure. Of all the evidence available to this day these conclusions can be drawn: a) except for exceptional well-identified cases (ventricular arrhythmias with initial cellular types), all products administered in humans have proven safe and no cases of rejection (not even with allogenic products), oncogenesis, worsening of the patients’ cardiovascular status or major complications during the administration have been reported; b) the real clinical efficacy of these therapies has not been undeniably confirmed through hard endpoints. While some studies have shown neutral results, others have confirmed a reduction of the infarction size, increased myocardial perfusion or ejection fraction, and better soft endpoints; c) the most promising scenarios are heart failure with systolic ventricular dysfunction and refractory angina; and d) a large and very sophisticated array of administration strategies, including surgical, has been developed (mostly percutaneous) to allow the injection of biological materials in certain cardiac regions using conventional or special catheters and navigational systems to accurately guide the administration.
Like the preclinical setting, the clinical evidence available allows us to identify some of the variables that should be confirmed and better defined before conducting large-scale clinical trials; among them, the selection of the type of product, the total dose, and the optimal administration time for every particular condition. Also, comparative studies of products, repeated administration, and improvement of myocardial retention in the products infused or injected. All these aspects should be rigorously analyzed through basic and preclinical research before conducting new studies in humans. At this point, the rigorous design of clinical trials with well-defined endpoints, adequate sample sizes, and strict regulatory control should be mentioned here.
INTERNATIONAL ALLIANCES AND SPECIFIC WORKING GROUPS
As part of the development of regenerative medicine, and to go deeper in its study and organize and structure a still marginal research, 2 main organizations have been created:
-
– The international consortium TACTICS (Transnational Alliance for Regenerative Therapies in Cardiovascular Syndromes).10 This consortium includes over top 100 international research working groups in this field. It is an worldwide, collaborative consortium network for the writing of position papers and recommendations, the rigorous promotion in all settings (scientific, institutional, and social), and for the design and development of coordinated and efficient clinical and preclinical research projects.
-
– The Working Group on Cardiovascular Regenerative and Reparative Medicine,11 is part of the European Society of Cardiology (ESC). It is a dynamic body founded on the pillars of training, education, research, congress participation, and field support as defined by the ESC rules and regulations.
The common initial objective of both associations is to analyze the evidence available on cardiovascular regenerative and reparative medicine, establish future research lines, and ultimately, facilitate the development of therapies to improve the patients’ cardiovascular health.
CONCLUSIONS
Although the clinical efficacy of regenerative and reparative medicine has not been confirmed yet to be able to include it in the routine clinical practice, it has overwhelmingly contributed to broaden our knowledge on the molecular biological, cellular, and tissue processes that govern functional loss, homeostasis, and cardiovascular system repair. By analyzing and planning future studies using multicenter, multidisciplinary, coordinated, evidence-based, rigorous methodology we will be closer to obtaining therapies capable of partially or totally reversing irreversible myocardial tissue damage and improving cardiovascular health.
CONFLICTS OF INTEREST
The authors declared no conflicts of interest whatsoever.
REFERENCES
1. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017:a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1736-1788.
2. Fernández-Avilés F, Sanz-Ruiz R, Climent AM, et al. Global position paper on cardiovascular regenerative medicine. Eur Heart J. 2017;38:2532-2546.
3. Messina E, De Angelis L, Frati G, et al. Isolation and expansion of adult cardiac stem cells from human and murine heart. Circ Res. 2004;95:911-921.
4. Bergmann O, Zdunek S, Felker A, et al. Dynamics of Cell Generation and Turnover in the Human Heart. Cell. 2015;161:1566-1575.
5. Climent AM, Sanz-Ruiz R, Fernández-Avilés F. Cardiac rejuvenation:a new hope in the presbycardia nightmare. Eur Heart J. 2017;38:2968-2970.
6. Buja LM. Cardiac repair and the putative role of stem cells. J Mol Cell Cardiol. 2019;128:96-104.
7. Roolvink V, Ibáñez B, Ottervanger JP, et al. Early Intravenous Beta-Blockers in Patients With ST-Segment Elevation Myocardial Infarction Before Primary Percutaneous Coronary Intervention. J Am Coll Cardiol. 2016;67:2705-2715.
8. Zwetsloot PP, Végh AM, Jansen of Lorkeers SJ, et al. Cardiac Stem Cell Treatment in Myocardial Infarction:A Systematic Review and Meta-Analysis of Preclinical Studies. Circ Res. 2016;118:1223-1232.
9. Fisher SA, Doree C, Mathur A, et al. Meta-analysis of cell therapy trials for patients with heart failure. Circ Res. 2015;116:1361-1377.
10. TACTICS Alliance. Available online: https://www.tacticsalliance.org. Accessed 7 Oct 2019.
11. ESC Working Group on Cardiovascular Regenerative and Reparative Medicine. Available online:https://www.escardio.org/Working-groups/Working-Group-on-Cardiovascular-Regenerative-and-Reparative-Medicine. Accessed 7 Oct 2019.
Corresponding author: Servicio de Cardiología, Hospital General Universitario Gregorio Marañón, Dr. Esquerdo 46, 28007 Madrid, Spain.
E-mail address: (F. Fernández-Avilés).
Talking about innovation can be confusing. The term “innovation” is used to refer to many different things and proof of this is the large number of different definitions currently available. In any case, innovation is almost a magical word often hiding huge expectations of possible solutions to the great challenges posed by society and that have a dramatic impact on healthcare. We present some of the current trends and reflections affecting the Spanish healthcare system providers.
INNOVATION: GENERATING THE PRODUCT
At this point in time, talking about lists in relation to research and development (R+D) and its situation in Spain is an obvious and overused argument these days. Figures are well-known, have already been confirmed, are widely accepted, and have showed room for improvement over the last few decades: our country ranks high in research but runs low on R+D funding (high efficiency), especially in the private sector (mainly related to the business structure of small and medium-sized enterprises) but innovation still lags behind. Coming to terms with the specific weight of the different possible causes for this gap between research and innovation (culture, funding, education, regulation, etc.) is even harder.1
The impact of a disadvantaged situation in innovation is relevant: we do not invent, so we never own what we need (understood as a product manufactured and marketed by Spanish companies), which means we have to import it. Regarding health—where the impact of technology and drugs is huge—the effect the trade balance may have is considerable. Undubitably, this is a field where the activity of the Spanish healthcare system as a country that generates products, patents or companies may have a significant economic impact.2,3
INNOVATION: INTRODUCING THE PRODUCT
Advances in medicine are the key to improve disease management and prevention. The speed at which new products like drugs, devices, machines, diagnostic procedures, etc. are available is now greater than ever. These advances are considered innovation and they become part of the therapeutic arsenal available after an often very expensive process of development where proprietary companies make big investments. The cost of these new products is sometimes considerable and their benefits in terms of incremental net health benefit do not usually match costs and are often limited. Two examples of striking innovations that have recently impacted the media because of their potential cost are the CAR T-cell therapy and proton radiotherapy. Another recent example of great therapeutic innovation is the curative treatment of hepatitis C. The total artificial heart is unquestionably relevant innovation in cardiology. The developing speed of technologies like 3D printing, artificial intelligence, big data, digital health or tele-healthcare forces us to understand what they are good for before implementing them in health organizations and also to assess their impact in the system. In these innovations, price, complexity, conditions of use, and effects greatly condition their use.
INNOVATION: USING THE PRODUCT
Management experts have been anticipating the arrival of a sustainable prevention healthcare model for decades because of the constant growth of healthcare spending due to a number of reasons: higher costs in healthcare innovation, increased chronicity and longevity, and greater expectations from the population.
Patients live longer but they also remain sick longer, and every month of life gained equals higher costs. Although this statement has several exceptions, it forces us to identify those patients who can live disease-free for longer, or, at least, not dependant on the healthcare system. Also, it shows what innovations bring real value both in general and particular terms. Precision medicine and innovation in management play a big role. Both concepts can be considered a spectral continuum in the decision-making process. On the other hand, knowing that these innovations are cost-effective is no longer enough; now it is required to know what their real impact is on population health outcomes like quality of life and disease progression. This is how the Spanish healthcare system is moving forward with the great challenge posed by value-based medicine.4
INNOVATION: ORGANIZATION AND HEALTH PROFESSIONALS
There are 3 different scenarios regarding innovation: production, introduction, and use. These 3 settings require 3 different fields of expert knowledge —innovation manager, health professional, and healthcare manager— with significant overlapping that still coincides in information systems and new data management. In this context, the great expectations generated by big data and artificial intelligence should not be a surprise. These are true innovations to help us make decisions, prioritize efforts, speed up healthcare processes, reduce the load of tasks with no added value for health professionals, and eventually focus on personal attention.5
Beyond the traditional concept of product understood as technology—devices or drugs—healthcare providers have always been involved by generating solutions in their setting adapted to their working framework and using the existing resources based on process innovation. Healthcare providers can change the way things are done, most of the time intuitively, and then adapt them to their setting thanks to years of experience. They often give their opinion on current needs and possible solutions to different settings. They also happen to be right most of the time.
This may be an organizational innovation we must face: to hear what health professionals have to say to share the decision-making process with them. Also, to support them in complex priority decision-making processes caused by limited resources in a society with growing well-being demands. It is the healthcare institutions that need to move towards more intelligent and collaborative ecosystems to promote a culture of innovation. Innovative ideas have always been there; time has come to listen to the people who had these ideas, evaluate them rigorously, focus on the impact they have on health outcomes, and promote innovation.6-8
FUTURE PERSPECTIVES
The road towards innovation is a long one and changing the productive model and the culture of an entire country is a huge challenge. However, over the last few decades, it has been proven that we can change the Spanish model of producing science together. Why not do the same thing with innovation?
Let’s give ourselves the time and opportunity to innovate in health, instead of letting others do the job. Let’s be us who, with our own knowledge, improve our healthcare system, one of the world’s most efficient healthcare systems now facing huge challenges ahead.9
FUNDING
The authors have received funding from the Medical Technology Innovation Platform (ITEMAS) (PTR2018.001071, PT17/0005/0036) sponsored by the Instituto de Salud Carlos III. Project co-funded by the European Regional Development Fund (ERDF).
CONFLICTS OF INTEREST
None declared.
REFERENCES
1. Fundación Cotec. Informe Cotec 2019. Innovación en España. Madrid:Fundación Cotec para la Innovación;2019.
2. Mulet J. Política de innovación para España. Necesidad y condicionantes. Fedea Policy Papers. 2016. Available online:http://documentos.fedea.net/pubs/fpp/2016/07/FPP2016-12.pdf. Accessed 25 Oct 2019.
3. Aloini D, Martini A. Exploring the exploratory search for innovation:a structural equation modelling test for practices and performance. Int J Technol Manage. 2013;61:23-46.
4. Barge-Gil A, Modrego A. The impact of research and technology organizations on firm competitiveness:Measurement and determinants. J Technol Transfer. 2011;36;61-83.
5. Bason C, ed. Leading public sector innovation. Co-creating for a better society. 2nd ed. Bristol:Poliy Press;2018.
6. Pan SW, Stein G, Bayus B, et al. Systematic review of innovation design contests for health:spurring innovation and mass engagement. BMJ Innov. 2017;3:227-237.
7. Bergeron K, Abdi S, DeCorby K, Mensah G, Rempel B, Manson H. Theories, models and frameworks used in capacity building interventions relevant to public health:a systematic review. BMC Public Health. 2017;17:914.
8. Allen JD, Towne SD Jr, Maxwell AE, et al. Measures of organizational characteristics associated with adoption and/or implementation of innovations:A systematic review. BMC Health Serv Res. 2017;17:591.
9. GBD 2016 Healthcare Access and Quality Collaborators. Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations:a systematic analysis from the Global Burden of Disease Study 2016. Lancet. 2018;391:2236.
Corresponding author: Edificio IDIVAL, Avda. Cardenal Herrera Oria s/n, 39011 Santander, Cantabria, Spain.
E-mail address: (G. Peralta Fernández).
The sex-based differences in approach and mortality in the management of patients with acute coronary syndrome (ACS) have been known for a while now. Back in 1991 the New England Journal of Medicine published an editorial1 on this matter. In this article Healy coined the term “the Yentl Syndrome” to refer to the invisibility of women in the studies of cardiovascular disease. She argued that women should behave according to the masculine clinical standards to receive the same care; otherwise they were misdiagnosed and mistreated resulting in healthcare of a lower quality and effectiveness.
Over the last few decades, cardiovascular mortality has decreased thanks to the advances made in the prevention, diagnosis, and treatment of ischemic heart disease. This improvement has benefited women as well. According to the RESCATE II registry,2 between 1992 and 2003, in-hospital mortality after a first acute myocardial infarction decreased 25% in women. In spite of this, unlike what happens with males, circulatory system diseases are still the leading cause of mortality among women.3 In the study presented by Anguita et al.4 in the last European Congress of Cardiology, female sex was still an independent predictor factor of mortality in ST-segment elevation acute myocardial infarction (STEMI) in Spain. In this study, the authors retrospectively analyzed the Minimum Basic Data Set of the Spanish Ministry of Health from 2005 through 2015. They identified 325 017 patients with STEMI of whom 38.8% were women, and concluded that in-hospital adjusted mortality is still high in this group. It should be mentioned that odds ratio dropped from 1.28 in 2006 to 1.14 in 2014, which may indicative of better care to women with STEMI.
The article by Tomassini et al.5 recently published on REC: Interventional Cardiology is an in-depth analysis of primary angioplasty and midand long-term mortality in patients with STEMI based on sex differences. It is a retrospective analysis of all patients with STEMI presenting with < 12 h of chest pain who underwent a primary angioplasty at their center from March 2006 to December 2016; in total, 1981 patients (24.4%, women). According to other registries,6 compared to males, women are older (mean age 71.3 ± 11.6 vs 62.9 ± 11.8 years), have a higher prevalence of traditional cardiovascular risk factors, longer total ischemic times, and worse Killip functional class at admission. Oddly enough after matched propensity score analysis, with the same percentage of multivessel coronary artery disease (5.3% vs 4.7%) and stent implantation (82.9% vs 83.9%), the success of the procedure and ST-segment resolution were significantly lower in women (90.2% vs 94.4% and 47.5% vs 54.1%, respectively). The authors suggest that this is probably due to the different pathophysiology of acute myocardial infarction in women, but they do not say anything about the time elapsed from the first medical contact until guidewire crossing or subsequent medical therapy, variables that have a direct impact on the prognosis of patients.
As interventional cardiologists we have a hard time thinking that there may be different system delays because when the infarction code goes off, the most important thing is to find the ST-segment elevation on the EKG, the timeline of disease progression, and the patient’s clinical signs and hemodynamic status (not always in this order). In any case, we should not forget that treatment starts before and after our intervention.
A study conducted in Portugal7 revealed that delays from the first medical contact to radial access were 15 minutes longer among women. This is not an isolated datum. Huded et al.8 analyzed variability during management and the results of the STEMI care network from Cleveland Clinic (Ohio, United States). They observed worse quality of care in women, longer door-to-balloon times, and medical therapies inconsistent with the guidelines in a higher percentage of cases. The implementation of an adapted protocol improved these parameters, especially among women (the percentage of women who received medical therapy as recommended by the guidelines rose to 98%, and system delays were reduced in 20 minutes). Overall, in-hospital mortality decreased 43%. This makes us think that maybe the variability seen in the management of STEMI is something generalized, that the reduction of discrepancies is possible, and that it can reflect the quality and maturity of care networks.
It is noteworthy to discuss the atypical nature of symptoms in women as the cause for these delays. The VIRGO clinical trial9 interviewed 2009 women and 976 males between 18 and 56 years of age admitted due to an STEMI. In both groups, the main symptom was chest pain defined as pain, pressure, tension or discomfort (87% vs 89.5%). Also, women had more accompanying symptoms (58.5% showed more than 3 additional symptoms compared to 46.2% of males). These data are reproduced in another prospective study conducted at an ER that interviewed 1941 patients with suspected ACS. The study confirmed that 92% of women and 91% of males reported chest pain as the main symptom.10 When women were asked why did not they look for help earlier,11 most of them thought it was not an STEMI and they did not want to be called hypochondriacs if it was not serious after all. And they may be right. According to the VIRGO trial, 53% of women who previously sought medical attention were told that it was not an acute coronary event. Maybe as Healy used to say1 women do not belong in the medical and social category of ACS.
For all this, although the management of STEMI in women has improved over the last few decades, articles like Tomassini et al.’s5 are a friendly reminder that there is still work to be done. Not only clinical trials, but also daily gestures like rising the awareness of society and healthcare providers that STEMI affects everyone, women included.
CONFLICTS OF INTEREST
None declared.
REFERENCES
1. Healy B. The Yentl Syndrome. N Engl J Med. 1991;325:274-275.
2. García-García C, Molina L, Subirana I, et al. Sex-based Differences in Clinical Features, Management, and 28-day and 7-year Prognosis of First Acute Myocardial Infarction. RESCATE II Study. Rev Esp Cardiol. 2014;67:28-35.
3. Instituto Nacional de Estadística. Defunciones según la causa de muerte. 2017. Available online: https://www.ine.es/jaxi/Tabla.htm?path=/t15/p417/a2017/l0/&file=01001.px&L=0. Accessed 1 Jun 2019.
4. Anguita M, Sambola Ayala A, Elola J, et al. Female sex is an independent predictor of mortality in patients with STEMI in Spain:a study in 325,017 episodes over 11 years (2005-2015). En:Paris 2019. ESC Congress 2019;2019 31 Aug - 4 Sept;Paris, France. Available online: https://esc365.escardio.org/Congress/ESC-CONGRESS-2019/Poster-Session-2-Risk-Factors-and-Prevention-Cardiovascular-Disease-in-Spec/197767-female-sex-is-an-independent-predictor-of-mortality-in-patients-with-stemi-in-spain-a-study-in-325-017-episodes-over-11-years-2005-2015. Accessed 15 Sept 2019.
5. Tomassini F, Cerrato E, Rolfo C, et al. Gender-related differences among patients with STEMI:a propensity score analysis. REC Interv Cardiol. 2019. https://doi.org/10.24875/RECICE.M19000061.
6. Mehta L, Beckie T, Devon H, et al. Acute Myocardial Infarction in Women, A scientific statement from the American Heart Association. Circulation. 2016;133:916-947.
7. Araújo C, Laszczynska O, Viana M, et al. Quality of Care and 30-day Mortality of Women and Men With Acute Myocardial Infarction. Rev Esp Cardiol. 2019;72:543-552.
8. Huded CP, Johnson M, Kravitz K, et al. 4-Step Protocol for Disparities in STEMI Care and Outcomes in Women. J Am Coll Cardiol. 2018;71:2122-2132.
9. Lichtman J, Leifheit E, Safdar B, et al. Sex Differences in the Presentation and Perception of Symptoms Among Young Patients With Myocardial Infarction. Evidence from the VIRGO Study (Variation in Recovery:Role of Gender on Outcomes of Young AMI Patients). Circulation. 2018;137:781-790.
10. Ferry A, Anand A, Strachan F, et al. Presenting Symptoms in Men and Women Diagnosed with Myocardial Infarction Using Sex-Specific Criteria. J Am Heart Assoc. 2019;8:e01297.
11. Lichtman JH, Leifheit-Limson EC, Watanabe E, et al. Symptom recognition and healthcare experiences of young women with acute myocardial infarction. Circ Cardiovasc Qual Outcomes. 2015;8:S31-S38.
Spain was inducted in the European initiative Stent for Life in a ceremony hosted by the General Assembly of the European Association of Percutaneous Cardiovascular Interventions (EAPCI) back in 2009. As president of the Hemodynamics and Interventional Cardiology Section of the Spanish Society of Cardiology (SEC), Dr. Fina Mauri signed the declaration of commitment with this initiative aimed to improve the access of patients to reperfusion by the increasing use of primary percutaneous coronary interventions (pPCI) as the optimal treatment in the management of ST-segment elevation myocardial infarction (STEMI).
The Stent for Life initiative was born the previous year (September 2008) as an alliance among the Spanish Society of Cardiology, EAPCI, and Eucomed.1 In Europe the situation of reperfusion in the management of infarction was under discussion. They came to the conclusion that there was a great heterogeneity among the different countries with an overall scarce penetration of pPCI as the treatment of choice.2 These differences were not related to gross domestic product (GDP): countries with relative low GDPs (Czech Republic, Hungary, Slovakia, Slovenia, Poland, Lithuania) performed many more pPCIs per million inhabitants compared to other countries with higher GDPs like Spain.2 For this reason, Spain was among the 6 countries asked to participate in this initiative together with Turkey, France, Greece, Bulgaria, and Serbia. All performed less than 200 pPCIs per million inhabitants (in 2008 only 165 PCIs per million inhabitants were performed in Spain). The objectives established at that time are shown on table 1; they were numerical objectives of implementation and penetration of this technique in the management of STEMI with the implicit creation of acute myocardial infarction networks.
Table 1. Objectives of the Stent for Life initiative from 2008
| Define regions/countries with unmet medical needs for the implementation of the optimal management of acute coronary syndrome |
|---|
| Implement an action program to increase the access of patients to pPCIs: a) Increase the percentage of pPCIs performed in > 70% of STEMI patients b) Achieve pPCI rates > 600 per million inhabitants/year c) Offer a 24/7 service in all necessary angioplasty centers for the full coverage of the region/country |
|
pPCI, primary percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction. |
Back in 2008, there were only 4 well-structured infarction networks across in Spain: Murcia, Galicia, Balearic Islands, and the Chartered Community of Navarre performed between 200 and almost 400 pPCIs per million inhabitants. However, eventually only 12.8% of the entire Spanish population benefited from these 4 networks. In the remaining autonomous communities, the pPCIs were performed erratically with numbers lower or closer to 100 pPCIs per million inhabitants. Regions like the Community of Valencia, the Principality of Asturias, and Andalusia performed 61, 78, and 106 pPCIs per million inhabitants).3 Like Europe, these regional differences were not related to the GDP of the different Spanish autonomous communities. Therefore, the creation of a myocardial infarction network with full hospital infrastructure, trained professionals, and a system of medical emergencies in a developed country like ours became a purely organizational matter. In October 2010 and with the explicit support from the SEC and its affiliate sections Hemodynamics and Interventional Cardiology, Ischemic Heart Disease, and Coronary Units the different scientific societies of the autonomous communities signed the declaration of membership to the Stent for Life initiative (figure 1). From that moment on, the focus was on 3 different levels for the progressive and gradual implementation of infarction networks. In the first place, there was a political and media approach to the different health administrations involved. The publication of the comparative results from the different autonomous communities in the media (figure 2) contributed effectively to their involvement in this issue. Parallel to this and thanks to scientific publications and cardiology meetings, professionals became aware on the clinical need to implement these infarction networks.4-7 Finally, patients were approached through commercial campaigns and media announcements with positive short-term results.8 Everything was mostly funded with the unconditional support from the industry. After 10 years of many people working for the Stent for Life initiative it can be said that it has contributed to the implementation of infarction networks nationwide. In 2018, 21 261 pPCIs were performed (13 395 back in 2008) with an average rate of 416 pPCIs per million inhabitants. This rate is considered adequate given the prevalence of ischemic heart disease in our country without great differences among the different autonomous communities.9 At this point, what challenges will the next decade bring? The survey of a paper recently published by Rodriguez-Leor et al.10 in REC: Interventional Cardiology may have some of the answer to this question. The current objectives should focus on both the patient and the healthcare provider. At this point it is not about opening new centers or programs anymore, but about designing the procedures required for each center to keep quality outcomes. The satisfaction of well-trained professionals built on adequate retributions, regulating the rest periods, and the correct sizing of staff based on the healthcare needs are all key issues to take into consideration at the infarction centers. Similarly, generational replacement should occur while keeping the quality of the entire process. The Administration should consider payment to centers based on results and make sure that these payments reach the treating physician. On the other hand, very complex cases like STEMI patients complicated with cardiogenic shock should be referred to specialized centers capable of performing advanced ventricular assist techniques, heart surgery, and transplants. In this type of patients, mortality rate is still very high (around 50%). Therefore, each infarction network should be able to identify its shock centers for the adequate management of these patients.

Figure 1. A: induction ceremony of the scientific societies of the different autonomous communities into the Stent for Life initiative (Madrid, October 4, 2010); B: certificate of membership to the Stent for Life initiative of an affiliate society (Society of Cardiology of Castile and León).

Figure 2. Examples of news published by the media on comparative results among different autonomous communities on the management of ST-segment elevation myocardial infarction.
In conclusion, the objectives of the Stent for Life initiative in our country should look at the new clinical and professional challenges ahead with the patient as the protagonist of all clinical actions.
ACKNOWLEDGEMENTS
We wish to thank Dr. Matías Feldman, Dr. Ander Regueiro, Dr. José Ramón Rumoroso, and Dr. Miren Tellería for their dedication to the Stent for Life initiative in Spain over the last 10 years. We also wish to thank the members of the different boards of directors of the Hemodynamics and Interventional Cardiology Section of the SEC for their contribution to this paper.
CONFLICTS OF INTEREST
M. Sabaté was the national coordinator of the Stent for Life initiative in Spain between 2009 and 2013. No other conflicts of interest have been reported.
REFERENCES
1. Widimsky P, Wijns W, Kaifoszova Z. Stent for Life:how this initiative began? EuroIntervention. 2012;8 Suppl P:P8-10.
2. Widimsky P, Wijns W, Fajadet J, et al. Reperfusion therapy for ST elevation acute myocardial infarction in Europe:description of the current situation in 30 acountries. Eur Heart J. 2010;31:943-957.
3. Baz JA, Pinar E, Albarrán A, Mauri J;Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology. Spanish Cardiac Catheterization and Coronary Intervention Registry. 17th official report of the Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology (1990-2007). Rev Esp Cardiol. 2008;61:1298-1314.
4. Kristensen SD, Fajadet J, Di Mario C, et al. Implementation of primary angioplasty in Europe:Stent for Life initiative progress report. EuroIntervention. 2012;8:35-42.
5. Kristensen SD, Laut KG, Fajadet J, et al. Reperfusion therapy for ST elevation acute myocardial infarction 2010/2011:current status in 37 ESC countries. Eur Heart J. 2014;35:1957-1970.
6. Regueiro A, Bosch J, Martín-Yuste V, et al. Cost-effectiveness of a European ST-segment elevation myocardial infarction network:results from the Catalan Codi Infart network. BMJ Open. 2015;5:e009148.
7. Gómez-Hospital JA, Dallaglio PD, Sánchez-Salado JC, et al. Impact on delay times and characteristics of patients undergoing primary percutaneous coronary intervention in the southern metropolitan area of Barcelona after implementation of the infarction code program. Rev Esp Cardiol. 2012;65:911-918.
8. Regueiro A, Rosas A, Kaifoszova Z, et al. Impact of the “ACT NOW. SAVE A LIFE“public awareness campaign on the performance of a European STEMI network. Int J Cardiol. 2015;197:110-112.
9. Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology. Spanish Cardiac Catheterization and Coronary Intervention Registry. Available online: https://www.hemodinamica.com/cientifico/registro-de-actividad/. Accessed 3 Jul 2019.
10. Rodriguez-Leor O, Cid-Alvarez A, Moreno R, et al. Survey on the needs of primary angioplasty programs in Spain. REC Interv Cardiol. 2020;2:8-14.
- The challenge of integrating Ibero-America through research and scientific publications
- Cardiac allograft vasculopathy. A disease on the search for therapy
- From Prometheus to Element Care
- Novel oral anticoagulants, diagnostic catheterization, and coronary intervention: another step forward towards the optimal strategy
Subcategories







Interviews

An interview with Bruno Scheller
aServicio de Cardiología, Hospital Universitario de La Princesa, Instituto de Investigación Sanitaria de La Princesa (IIS-IP), Universidad Autónoma de Madrid, Spain
bCentro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain




