
Available online: 09/04/2019
Editorial
REC Interv Cardiol. 2020;2:310-312
The future of interventional cardiology
El futuro de la cardiología intervencionista
Emory University School of Medicine, Atlanta, Georgia, United States

WHAT DO WE KNOW ABOUT FRACTIONAL FLOW RESERVE AFTER STENTING?
The introduction of the concept of fractional flow reserve (FFR) in the mid 90s moved coronary physiology from experimental science to routine use at the cath lab.1-3 Added to the better understanding of basic physiological mechanisms such as self-regulation and compensatory vasodilation and the coronary flow reserve introduced 20 years earlier by Gould et al.,4 FFR has undeniably changed our interpretation of coronary angiograms and had a major influence on the clinical decision-making process, and patient outcomes.3,5,6 This has resulted in the unique adoption of FFR as the only physiological index with a class I A indication for use in the clinical practice guidelines produced by the most important cardiologic societies worldwide.7,8
FFR has taught us that coronary angiography and the anatomic images we can acquire at the cath lab only provide moderately reliable measures of the functional significance of coronary artery disease and myocardial ischemia. Also, there is undeniable proof that the decision-making process based on functional measurements leads to better outcomes compared to angiography alone.3,5,6
In contrast, the interpretation of FFR after coronary intervention is still ambiguous. Basically, we should be aware that the status of a coronary artery immediately after a percutaneous coronary intervention (PCI) changes and is prone to much more variability compared to a situation of chronic stable coronary artery disease. An excellent result of a PCI performed today can change rapidly within hours due to thrombus formation, progressive dissection or other unforeseen complications. Therefore, the FFR measured immediately after a PCI should be interpreted with caution. Also, whereas the ischemic FFR threshold (0.80) in the stable angina has been clearly established, FFR values within the first days, weeks or months after a PCI can change quickly due to the healing process in the coronary artery itself, intimal hyperplasia, thrombus formation, etc. This means that by definition, the FFR after a PCI is more dynamic and that an adequate FFR value immediately after a PCI should be considerably higher than 0.80 to compensate for any intravascular changes that may occur in the short-term.
Therefore, it is not surprising to see FFR values of at least 0.90 in medical literature as indicative of an acceptable PCI result.9,10 Having said that, at the same time we should realize that most post-stent FFR values in earlier studies were obtained in patients with focal stenosis and without much diffuse disease. It is plausible to think that if diffuse disease is present inside a coronary artery, FFR values ≥ 0.90 will probably not be achieved by just stenting a focal stenosis.
Most likely, in such cases, hyperemic pressure pullback recording (whether motorized or not) or a sophisticated variety called hyperemic pressure pullback gradient will better qualify the functional result after stenting. They will also reveal if the remaining gradients inside the coronary artery are due to insufficient stent deployment or more diffuse disease.11
Despite these limitations, the existence of a clear correlation between the FFR values measured immediately after PCI and long-term outcomes is undeniable. This was first described in the FFR-post-STENT Registry of 750 patients that revealed the existence of an inverse correlation between the FFR values measured immediately after the PCI and the rate of restenosis at the 6-month follow-up (figure 1). Such an inverse correlation between high FFR values post-stenting and the mid-term risk of restenosis has been confirmed ever since.12 Still, it is not completely clear if suboptimal FFR values after stenting are due to a focal problem in the stented segment or to diffuse disease elsewhere in the artery. Hyperemic pressure pullback recording and pressure pullback gradient recording have proven that a considerable pressure gradient across the stent is often associated with inappropriate deployments as seen on intravascular ultrasounds or optical coherence tomographies.
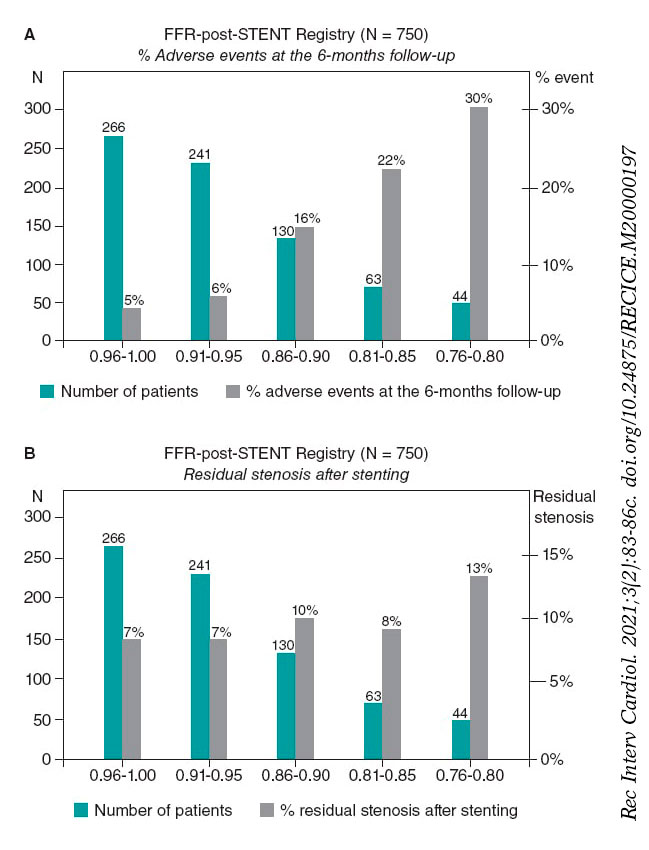
Figure 1. Superiority of functional testing compared to angiography alone to predict the outcomes after stenting. A: correlation between post-stenting fractional flow reserve (FFR) and the rate of adverse events at the 6-month follow-up in 750 patients from the FFR-Post-Stent registry. B: correlation between post-stenting angiography and the rate of adverse events at the 6-month follow-up. Reproduced with permission from Pijls et al.9
PATIENT AND VESSEL RELATED PREDICTORS OF POST-PROCEDURAL FFR
At this point, the study conducted by van Zandvoort et al. and recently published on REC: Interventional Cardiology comes into perspective.10 In this study, a large registry of 1000 consecutive patients from 1 large volume cardiac center, the FFR was consistently measured after an angiographically successful PCI without the intention of performing any additional procedures in cases of unexpectedly low FFR values. The authors should be praised for their adherence to this protocol. Afterwards, independent patient and vessel related characteristics were determined as associated with the post-procedural FFR values. Considering that in this study no information was available on the outcomes and that the relationships were not causal per se but associative, a few important lessons can be learned.
In the first place, a very strong predictor of lower FFR values was stent implantation in the left anterior descending coronary artery (LAD). In truly normal LADs, the FFR is not different from other arteries and is very close to 1.00.13 However, even in cases of mild disease, the FFR values measured in the LAD are often more damaged compared to other arteries. This is explained by the fact that the LAD perfusion territory is large. One of the major advantages of FFR with respect to other methodologies that only address a coronary artery injury is that the FFR does not only measure the stenosis itself, but also the extent of the perfusion territory. If a similar stenosis (with similar angiographic, intravascular ultrasound or optical coherence tomography characteristics) is located in a coronary artery with a larger perfusion territory, the FFR will be lower. In this regard, the FFR is actually the link between stenosis severity, coronary blood flow, extent of the myocardial perfusion territory, and myocardial ischemia.14 As such, it is plausible that after a successful PCI, the FFR of the LAD will be somehow lower compared to other coronary arteries.
A second interesting observation is that in women, the FFR measured after apparently successful stenting was often higher compared to the males. Van Zandvoort et al. suggest that this might be due to the fact that in women, microvascular disease plays a more predominant role compared to men. Also, that the generation of a hyperemic gradient within the epicardial coronary artery may be blunted by the presence of microvascular disease.10 To confirm that position, more detailed studies of coronary microvasculature are needed. For many years, the assessment of microvascular disease in a true quantitative way has been too hard to pin down. However, recently developed methodology has changed that as follows.15
SIMULTANEOUS ASSESSMENT OF EPICARDIAL AND MICROVASCULAR DISEASE
Recently, the technique for measuring absolute coronary blood flow and microvascular resistance has been introduced as an adjunctive to FFR measurement. This technique is based on the continuous infusion of a saline solution at a low rate and thermodilution. The technique is simple, elegant, accurate, and operator independent.15
In short, immediately after measuring the FFR, a specifically designed infusion catheter (Rayflow, Hexacath, Paris) is advanced while mounted on the pressure guidewire and placed inside the stent (to study the microvascular resistance of the territory distal to the stent). Then, the infusion of a saline solution at a low rate is started and the absolute coronary blood flow in mL/min is measured in the area of interest using this equation:
Q = Qi × T/Ti × 1.08
where Q is blood flow in the myocardial territory distal to the stent, Qi is the infusion rate of the saline solution (mL/min), Ti is the temperature of the infused saline solution (°C), and T is the temperature in the distal coronary artery after mixing blood and the saline solution. T and Ti are expressed as the difference with respect to body temperature.
With infusion rates = 8 to 10 mL/min, resting blood flow values are obtained and with infusion rates = 20 mL/min, maximum hyperemic values are obtained since the saline solution itself at that rate induces maximum hyperemia in a matter of seconds (figure 2; unpublished data).
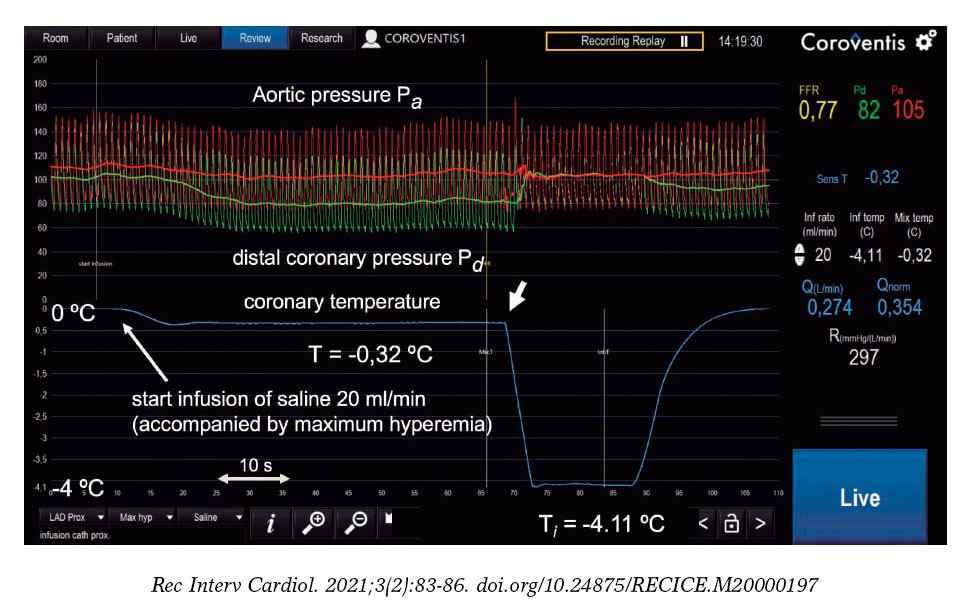
Figure 2. Example of absolute coronary blood flow and microvascular resistance measurement in left anterior descending coronary artery following routine fractional flow reserve measurement. On the figure upper side, aortic pressure (Pa), and distal coronary pressure (Pd) are shown in red and green, respectively. The blue line represents coronary temperature as a difference with respect to body temperature (T = 0). After starting the infusion of 20 mL/min of a saline solution (Qi) at room temperature through a dedicated infusion catheter, maximum hyperemia occurs within seconds. Then, after a complete mix of blood and saline solution, a steady-state distal coronary temperature T of 0.32 oC below body temperature is achieved. After withdrawing the pressure/temperature sensor from the tip of the infusion catheter, the infusion temperature (Ti) measured is 4.11 oC below body temperature. Absolute flow (Q) in the coronary artery is calculated using the equation shown in this article (274 mL/min). Microvascular resistance is simply calculated now by Pd/Q and equals 297 Wood units, which is a normal value for the anterior wall. Since the fractional flow reserve value is also known, the normal reference value of coronary flow can be calculated. All parameters are shown online supported by dedicated software (Coroventis, Sweden).
Immediately after the simultaneous measurement of distal coronary pressure and blood flow values, quantitative microvascular resistance Rµ (Wood units) is estimated. In this same way, epicardial disease (indicated by FFR) and microvascular disease (indicated by Rµ) can be assessed and independently distinguished. The position taken by van Zandvoort et al. suggesting that higher FFR values after PCI are related to a higher microvascular resistance in women could be elegantly validated this way.
WHAT IS THE BEST TECHNIQUE TO MEASURE THE FFR VALUES AFTER A PCI?
In the study conducted by van Zandvoort et al. the FFR values measured after the PCI are only briefly described.10 The authors do not report if hyperemic pressure pullback recordings were performed or other techniques used to assess the entire artery. Also, we should mention that to measure intracoronary pressure, not a single true pressure guidewire was used, but the Navvus system instead (ACIST Medical Systems, Eden Prairie, MN, United States). This system is known to overestimate pressure gradients and underestimate FFR mildly in cases of minimal disease or moderately in cases of more severe disease.16 Also, this system is not validated against regular pressure guidewires in post-PCI vessels.
Nevertheless, the measurements were taken meticulously using IV adenosine at a rate of 140 µg/kg/min, giving the opportunity of an easy and reliable estimation of the FFR under stable conditions. We should mention that only 2 out of 1000 patients showed adenosine intolerance, meaning that the infusion of adenosine had to be interrupted due to harmless adenosine-induced, angina-like chest pain. This underlines the safety profile of IV adenosine infusions as seen in tens of thousands of patients in a myriad of other studies.
In future studies on the meaning and interpretation of post-PCI FFR, it would be adviseable to perform hyperemic pressure pullback recordings as outlined in the first part of this article or use the even more sophisticated technique for whole vessel evaluation after PCI recently introduced by Collet et al. and called hyperemic pressure pullback gradient.11 Obviously, all pressure analyses performed inside the stented coronary artery should preferably be performed at maximum hyperemia since gradients at rest inside the artery are 2 to 3 times smaller. Consequently, the signal-to-noise ratio of a resting pullback recording is 2 to 3 times less sensitive.
In conclusion, although outcome data were not presented which, by the way, was not the objective of the study, the interesting trial conducted by van Zandvoort et al.10 teches us about several interesting patient and vessel related predictors of post-procedural FFR measurement. Also, it anticipates the need for future physiological studies to unravel the different factors involved using new research methods on coronary circulation like hyperemic pressure pullback gradients and truly quantitative microvascular resistance (Rµ) measurements.
FUNDING
No funding whatsoever with regards to this article.
CONFLICTS OF INTEREST
N.H.J. Pijls has received institutional research grants from Abbott and Hexacath. Also, he is a consultant for Abbott, Opsens, and General Electric, and a minor stockholder of Philips, GE, ASML, and Heartflow. L.X. van Nunen declared no conflicts of interest whatsoever.
REFERENCES
1. Pijls NH, van Son JA, Kirkeeide RL, De Bruyne B, Gould KL. Experimental basis of determining maximum coronary, myocardial, and collateral blood flow by pressure measurements for assessing functional stenosis severity before and after percutaneous transluminal coronary angioplasty. Circulation. 1993;87:1354-1367.
2. Pijls NH, De Bruyne B, Peels K, et al. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N Engl J Med. 1996;334:1703-1708.
3. Tonino PA, De Bruyne B, Pijls NH, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360:213-224.
4. Gould KL, Lipscomb K, Hamilton GW. Physiologic basis for assessing critical coronary stenosis. Instantaneous flow response and regional distribution during coronary hyperemia as measures of coronary flow reserve. Am J Cardiol. 1974;33:87-94.
5. De Bruyne B, Fearon WF, Pijls NH, et al. Fractional flow reserve-guided PCI for stable coronary artery disease. N Engl J Med. 2014;371:1208-1217.
6. Zimmermann FM, Omerovic E, Fournier S, et al. Fractional flow reserve-guided percutaneous coronary intervention vs. medical therapy for patients with stable coronary lesions:meta-analysis of individual patient data. Eur Heart J. 2019;40:180-186.
7. Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41:407-477.
8. Patel MR, Calhoon JH, Dehmer GJ, et al. ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS 2017 Appropriate Use Criteria for Coronary Revascularization in Patients With Stable Ischemic Heart Disease:A Report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for T. J Am Coll Cardiol. 2017;69:2212-2241.
9. Pijls NH, Klauss V, Siebert U, et al. Coronary Pressure Measurement After Stenting Predicts Adverse Events at Follow-Up. Circulation. 2002;105:2950-2954.
10. van Zandvoort LJC, Masdjedi K, Neleman T, et al. Predictors of postprocedural fractional flow reserve:insights from the FFR-SEARCH study. REC Interv Cardiol. 2020. 2021;3:91-97.
11. Collet C, Sonck J, Vandeloo B, et al. Measurement of Hyperemic Pullback Pressure Gradients to Characterize Patterns of Coronary Atherosclerosis. J Am Coll Cardiol. 2019;74:1772-1784.
12. Rimac G, Fearon WF, De Bruyne B, et al. Clinical value of post-percutaneous coronary intervention fractional flow reserve value:A systematic review and meta-analysis. Am Heart J. 2017;183:1-9.
13. Pijls NH, Van Gelder B, Van der Voort P, et al. Fractional flow reserve. A useful index to evaluate the influence of an epicardial coronary stenosis on myocardial blood flow. Circulation. 1995;92:3183-3193.
14. De Bruyne B, Hersbach F, Pijls NH, et al. Abnormal epicardial coronary resistance in patients with diffuse atherosclerosis but 'Normal'coronary angiography. Circulation. 2001;104:2401-2406.
15. Xaplanteris P, Fournier S, Keulards DC, et al. Catheter-Based Measurements of Absolute Coronary Blood Flow and Microvascular Resistance:Feasibility, Safety, and Reproducibility in Humans. Circ Cardiovasc Interv. 2018;11:e006194.
16. Wijntjens GW, van de Hoef TP, Kraak RP, et al. The IMPACT Study (Influence of Sensor-Equipped Microcatheters on Coronary Hemodynamics and the Accuracy of Physiological Indices of Functional Stenosis Severity). Circ Cardiovasc Interv. 2016;9:e004645.

It comes as no surprise that the progression of medical training would eventually take a leap into the digital world where we would be able to access information without leaving our working place or the comfort of our homes. Our specialty, interventional cardiology, predominantly visual, has always benefited from the most advanced technology regarding communication. Actually, we have been doing this for years, even in our country: by the mid-1980s, the Madrid Interventional Course (MIC) organized by Dr. J.L. Delcán and Dr. E. García, was already broadcasting live cases via satellite to analyze and discuss new insights with larger audiences compared to those that can fit in a room. These days, live cases are an essential part of the meetings held in our setting (whether international like the ones organized by EuroPCR and TCT or national like the ones held by the Società Italiana di Cardiologia Interventistica [GISE] and the Interventional Cardiology Association of the Spanish Society of Cardiology [ACI-SEC])3. These cases are discussed remotely by panels of experts with a growing interaction with in-person and remote attendees thanks to specific computer tools and social media. But it is not only the broadcast of live cases which benefit from these advances. We have had access to information on late breaking clinical trials through the Internet many times even before in-person meeting where these trials are often presented. Also, we have had access to the recordings of many simultaneous sessions we couldn’t attend in-person but can review later when we have the time.
The situation of the pandemic caused by the new SARS-CoV-2 coronavirus has accelerated this cross over to virtual meetings due to the impossibility of travelling to places and holding large in-person meetings.1 The main in-person cardiology meetings scheduled for 2020 have been suspended or turned into virtual meetings. The two largest international meetings already mentioned, EuroPCR and TCT, have become virtual meetings. Also, mass meetings like the ones held by the American College of Cardiology, the American Heart Association or the European Society of Cardiology (ESC) have followed in the footsteps of this digital transition. Our sister societies, the Italian GISE and the Portuguese Associação Portuguesa de Intervenção Cardiovascular (APIC) have done the same thing. But, when these restrictions are lifted, will in-person activities like large face-to-face congresses and meetings be gone for good? Let us look at the pros and the cons of virtual and in-person meetings2 (Figure 1).
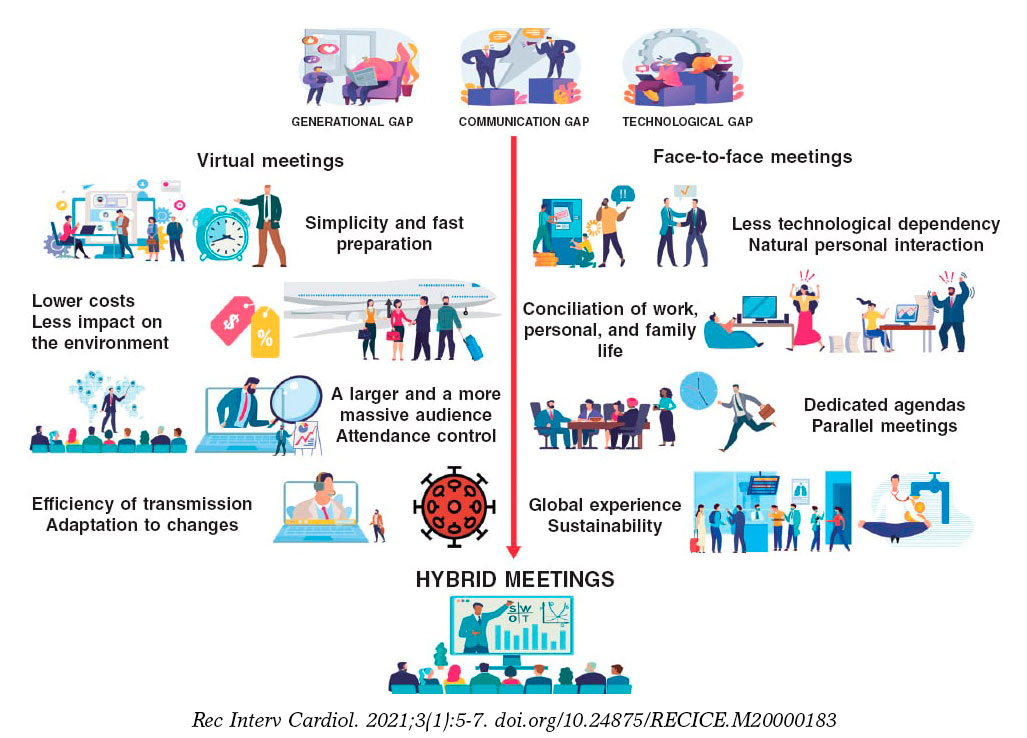
Figure 1. Pros of virtual meetings compared to face-to-face meetings.
These are the basic strengths of virtual meetings:
-
The speed at which these meetings are prepared is much faster compared to in-person meetings since there are many different tasks that the cardiology society does not need to do.
-
Lower costs: it is obvious that reducing travel and accomodation expenses, renting fewer available spaces, etc. reduces the overall budget. A direct consequence of this is a lower impact on the environment thanks to lower mobility.
-
Greater efficiency in the transmission of the message without time losses when going to the meeting or in-between sessions, possibility of increasing the capacity of the virtual rooms on demand and reviewing pre-recorded sessions on demand (even so, personal interaction will be gone).
-
Better attendance control: computer tools facilitate the comprehensive registry of attendance to every session, time, origin, and interaction developed, etc., but not the quality. Although we cannot fully know to what extent these attendees’ profit from these face-to-face meetings (exams may be an option?) leaving a device connected to these activities is no guarantee either.
-
Universal access brings meetings to larger audiences erasing geographical borders: in the fully virtual EuroPCR of 2020 there were over 15 000 registrations (compared to 11 200 registrations in the 2019 in-person edition).3 This phenomenon was even more evident in the ESC congress of 2020. This meeting still holds the registration record with 125 000 registrations from 213 different countries4 compared to the previous year (33 500 registrations).5 (Figure 2). Can these figures be compared? Probably not because registration to these virtual editions was free of charge.
-
Adaptation to changing situations: this virtual format allows us to accommodate meetings to travel limitations or potentially infectious situations like the one posed by the current pandemic.
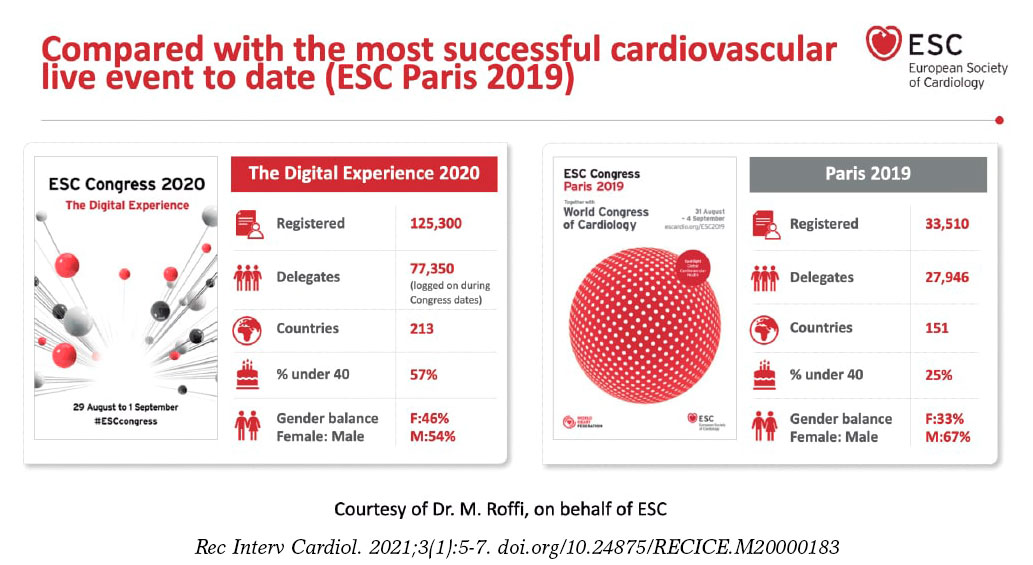
Figure 2. Registration comparison of the annual meetings held by the European Society of Cardiology back in 2019 and 2020.
The downsides of virtual meetings are:
-
Dependency on technical factors: technical support systems are excellent, but still depend on variables like the Internet bandwidth, the quality of connectivity or the incompatibilities of presentations and videos. After 25 years of use of the DICOM standard for the communication and management of medical imaging we still have issues when we try to play video sequences in virtual meetings.
-
To a great extent, the format of these sessions keeps the same structure as face-to-face meetings. The adaptation to the new virtual environment has been more cosmetic than a true reality with the implementation of several technological advances to mimic the in-person experience (avatars, virtual common rooms, chats to replace direct communication). However, fully developed specific methods of communication have not been implemented yet.
-
More difficult personal interaction: asynchronous communication and other virtual borders like lack of types of nonverbal communication (beyond emoticons) complicate connectivity among speakers, moderators, and audience. Speakers feel some kind of «digital loneliness» because they don’t receive any feedback from the audience. In turn, the audience experience “digital fatigue” and they can’t remain focused on anything for more than 30 minutes. New systems to encourage audience participation are desperately needed, particularly in the virtual format.
-
Agendas, time zones, and time devoted to work: in these virtual meetings it is not unusual to find conflicting time schedules since participants come from all across the world. It is not unusual either that these time schedules invade our spare time or affect our working day. The proliferation of these activities is associated with digital overload that has sometimes been referred to as «death-by-webinars»
-
Program sustainability: although our political representatives can’t wait to stop the private sector from funding our medical training programs, the truth is that this is crucial if we want to develop this kind of activity. If some of the activities that used to take place at face-to-face meetings are gone, will support still be the same? Isn’t it more profitable to conduct sponsored meetings and not independent activities?
Those of us who have been trained in the “traditional” meeting environment have a hard time thinking that they can be totally replaced by the virtual format. Here are some of the reasons why:
-
Attending a scientific meeting is a comprehensive experience that includes training as well as other activities: research coordination meetings, building up professional relations, consultancy and counseling, etc. It is almost impossible to conduct these activities outside the context of a scientific meeting.
-
In this sense, attending a face-to-face meeting is time-bound. It is not always easy to disassociate attendance to these meetings from working or face-to-face obligations (especially when the meeting is held in our own town), but it is actually easier compared to virtual meetings. In our setting there are work permits that can be issued to attend training sessions: could this be applicable to virtual meetings particularly with the current extended time schedules of such events?6
-
Most of the advantages seen in the broadcast of contents have long been part of face-to-face meetings. Consequently, most sessions are recorded for immediate broadcast and further reproduction. The same thing happens with in-person and remote audience interaction where the use of social media has proven very useful.
Will the digital gap between the analogical and the digital world, between immigrants and digital natives, between boomers and millennials grow? I don’t think so. Their coexistence will prevail and bring us the best of both worlds: hybrid meetings. If these two worlds were actually ever there…
FUNDING
No funding was received for this work.
CONFLICTS OF INTEREST
A. Pérez de Prado declared having received professional fees for his consultancy work or meetings held for iVascular, Boston Scientific, Terumo, BBraun, and Abbott totally unrelated to this article; he is the current president of the education and learning organization Fundación Epic.
REFERENCES
1. Alkhouli M, Coylewright M, Holmes DR. Will the COVID-19 Epidemic Reshape Cardiology? Eur Heart J Qual Care Clin Outcomes. 2020;6:217-220.
2. Sandars J, Correia R, Dankbaar M, et al. Twelve tips for rapidly migrating to online learning during the COVID-19 pandemic. MedEdPublish. 2020. https://doi.org/10.15694/mep.2020.000082.1.
3. PCR e-Course 2020. Thanks to the 15,000+online learners. 2020. Available online: https://www.pcronline.com/Courses/PCR-e-Course. Accessed 20 Sep 2020.
4. European Society of Cardiology. ESC Congress 2020 ? The Digital Experience. A record-breaking event:125,000 healthcare professionals from 213 countries. Available online: https://www.escardio.org/Congresses-%26-Events/ESC-Congress. Accessed 20 Sep 2020.
5. European Society of Cardiology. Figures from ESC Congress ? Statistics from the world's largest cardiovascular congress. Participation 2015-2019. Available online:https://www.escardio.org/Congresses-&-Events/ESC-Congress/About-the-congress/Figures-from-ESC-Congress. Accessed 20 Sep 2020.
6. Margolis A, Balmer JT, Zimmerman A, López-Arredondo A. The Extended Congress:Reimagining scientific meetings after the COVID-19 pandemic. MedEdPublish. 2020. https://doi.org/10.15694/mep.2020.000128.1.
Mitral regurgitation (MR) is one of the most prevalent valvular heart diseases in the world.1 Although surgical mitral valve replacement has shown to improve clinical outcomes in patients with severe primary MR, surgery is still being denied in a significant number of patients due to their multiple clinical comorbidities.2 The current clinical practice guidelines for the management of severe secondary MR recommend the surgical valve intervention only in cases where concomitant coronary revascularization is indicated.3
Transcatheter mitral valve repair using the edge-to-edge technique (MitraClip, Abbott Menlo Park, CA, United States) has shown to improve quality of life and reduce all-cause mortality in patients with heart failure and secondary MR refractory to the optimal medical treatment.4 However, the level of MR reduction achieved by MitraClip is inferior compared to the surgical techniques, and its overall use is limited by several anatomical factors.5 Transcatheter mitral valve implantation is emerging as a potential therapeutic alternative that could overcome some of the current limitations of edge-to-edge repair.6 Due to their technical design features, most transcatheter mitral valve implantation systems use the surgical transapical approach. Limited experience has been gathered on the use of dedicated transseptal systems. Finally, complex anatomical features such as the possibility of left ventricular outflow tract obstruction and presence of mitral annular calcification have limited the fast clinical adoption of this technology.
The field of catheter-based mitral valve intervention is rapidly expanding, and translational experimental models are seriously needed for the proper validation of these technologies. Unlike aortic valve disease, MR is due to several pathological conditions that result in different anatomical substrates that are not easy to reproduce in experimental models. Catheter-based technologies are designed taking into consideration specific anatomical targets such as annular dilatation or chord elongation, which are also challenging to reproduce in experimental animal models. Significant differences exist between humans and animal models. In the first place, one of the most important challenges we face is annular size. Devices developed for human use are typically larger compared to the annulus seen in common experimental models, which at times, requires developing customized valve sizes. Secondly, the aortomitral curtain is particularly small, which often leads to device interaction with the aortic valve. Thirdly, the mitral tissue is thin and friable providing little support to technologies that require the use of anchors or pads to remain in position. Finally, the left atrium is flat and shallow and provides little room for the validation of technologies via transseptal access.
The use of diseased animal models is not typically required to validate structural heart technologies and most of the validation work can be done on the bench or on healthy animal models. Healing and thrombogenicity of valve materials is particularly important and can be validated in healthy animals. The stability of the frame and durability of the leaflets can also be tested and is of particular significance in the transcatheter mitral valve implantation space. The mechanism of the deployment and delivery system can also be tested but, overall, the retention of the valve depends on the mechanism of anchoring used, which could be challenging due to the lack of structural support. In these cases, the surgical placement of the valves is needed for the long-term stability of the implant.
The use of diseased animal models is often spared to assess the efficacy of the device or test particular device features (ie, anchoring). Several animal species, primarily dogs suffer from primary MR due to leaflet prolapse and have been used to test several catheter-based technologies.7 However, these models are expensive and difficult to provide. Several groups have already developed secondary MR models by inducing ischemia of the posteromedial papillary muscle.8,9 These models have resulted in a high periprocedural mortality rate and moderate levels of clinically relevant MR. The study conducted by Rodríguez-Santamarta et al. recently published on REC: Interventional Cardiology presents a variation of this model by adding volume overload and creating an aorto-pulmonary fistula following the myocardial infarction of the circumflex artery.10 The number of animals was small, but researchers were able to prove the feasibility of model development. In this study, the level of MR was moderate (at most) and other features associated with MR such as annular dilatation were present. These morphological features, although obvious on the image assessment, were subtle in nature and probably in their early stages compared to patients who suffer from severe MR.
The field of structural heart procedures is changing very rapidly, and experimental models are essential for the proper validation of these technologies. Healthy animal models are perhaps enough to test the mechanism of the device delivery system, healing, and durability. Diseased animal models can help validate device efficacy, mechanisms of anchoring, and the long-term stability of the device. However, due to the high anatomical variability seen in humans compared to animals, long-term results may be confusing and require careful analysis by multidisciplinary teams before starting the first tests in humans. A multi-modality approach is highly desirable in the validation process of structural heart technologies. Although animal data are key, proper validation including human tissue and imaging correlation studies may help minimize the misinterpretation of experimental signals and define the developmental pathway of structural heart technologies.
FUNDING
No funding was received for this work.
CONFLICTS OF INTEREST
J. Granada is co-founder of Cephea Valve Technologies.
REFERENCES
1. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases:a population-based study. Lancet. 2006;368:1005-1011.
2. Mirabel M, Iung B, Baron G, et al. What are the characteristics of patients with severe, symptomatic, mitral regurgitation who are denied surgery?Eur Heart J. 2007;28:1358-1365.
3. Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, Fleisher LA, et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease:A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2017;135:1159-1195.
4. Stone GW, Lindenfeld JA, Abraham WT, et al. Transcatheter mitral-valve repair in patients with heart failure. N Engl J Med. 2018;379:2307-2318.
5. Boekstegers P, Hausleiter J, Baldus S, et al. Percutaneous interventional mitral regurgitation treatment using the Mitra-Clip system. Clin Res Cardiol. 2014;103:85-96.
6. Del Val D, Ferreira-Neto AN, Wintzer-Wehekind J, et al. Early Experience With Transcatheter Mitral Valve Replacement:A Systematic Review. J Am Heart Assoc. 2019;8:e013332.
7. Morgan KRS, Monteith G, Raheb S, Colpitts M, Fonfara S. Echocardiographic parameters for the assessment of congestive heart failure in dogs with myxomatous mitral valve disease and moderate to severe mitral regurgitation. Vet J. 2020;263:105518.
8. Pasrija C, Quinn RW, Alkhatib H, et al. Development of a Reproducible Swine Model of Chronic Ischemic Mitral Regurgitation:Lessons Learned. Ann Thorac Surg. 2020;111:117-125.
9. Hamza O, Kiss A, Kramer AM, Tillmann KE, Podesser BK. A novel percutaneous closed chest swine model of ischaemic mitral regurgitation guided by contrast echocardiography. EuroIntervention. 2020;16:e518-e522.
10. Rodríguez-Santamarta M, Estévez-Loureiro R, Pérez Martínez C, et al. Experimental model of mitral regurgitation in a porcine model. REC Interv Cardiol. 2021;1:12-18.
According to data from the National Statistics Institute, life expectancy has increased from 73.5 years in 1975 to 83.6 years in Spain in the year 2019. Also, the mean age of the population has gone up 10 years during this same period.1 In this sense, the results from the study conducted by Dégano et al.2 in 2013 come as no surprise. They already anticipated a strong increase in the rate of acute coronary syndrome (ACS) within the next 35 years when the Spanish population > 75 years will represent almost a quarter of the national census. This study anticipated that between 2013 and 2049, the cases of ACS in elderly patients would increase over 70%, but keep a discrete growth in patients under 75 years. These data are but a glimpse of a not so distant future when our patients will be older and their life expectancy longer. Also, the association between aging and comorbidity means that we will have to treat more complex patients.
Elderly patients with comorbidities are misrepresented in clinical trials studying the efficacy of both early invasive strategy for the management of non-ST-segment elevation acute coronary syndrome (NSTEACS) and the most suitable antithrombotic treatment.3 Therefore, despite the fact that clinical practice guidelines recommend early invasive strategy in most patients,4 its generalization to these patients is controversial. It is often decided to individualize the decision-making process by weighing risks and benefits and taking into consideration the treating physician’s perception on the possible complications. Hence, conducting clinical trials focused on this subpopulation as creating large registries representative of the actual clinical practice is of paramount importance.
In an article recently published by Pernias et al.5 on REC: Interventional Cardiology, the authors present a wide registry of elderly patients with NSTEACS conducted thanks to the collaborative work of different cardiology units from several Spanish autonomous communities. With over 7000 patients included, this study evaluated the impact of comorbidities on the indication to perform coronary angiographies. The 6 comorbidities studied (cerebrovascular disease, anemia, kidney disease, peripheral arteriopathy, chronic pulmonary disease, and diabetes mellitus) turned out to be independent predictors of a non-invasive approach. Also, it was confirmed that patients with more comorbidities had lower the chances of undergoing an invasive strategy despite having higher GRACE scores.
The comorbidities reported in this study are associated with a worse prognosis in this clinical setting.6 However, this does not necessarily involve low short-term life expectancy per se. Therefore, given the futility of an eventual revascularization a conservative strategy would not be justified. This clearly shows the need for a proper comprehensive geriatric assessment of these patients, since the accumulation of concomitant comorbidities is often followed by frailty, cognitive impairment, and functional dependency. These variables are key finding out why there is a paradoxically reverse correlation in these patients between the risk of ischemic events and the frequency of performing coronary angiographies. In this sense, we should mention the LONGEVO-SCA, a registry conducted in our setting that studied in detail the impact of frailty and geriatric syndromes on the therapeutic approach and vital prognosis of elderly patients with NSTEACS. Important conclusions can be drawn from this registry, like the negative impact of frailty both on the prognosis of elderly patients with NSTEACS and on the benefits of an invasive strategy.7,8
The usefulness of the invasive strategy in elderly patients is not well established. The randomized clinical trial After Eighty included 457 patients > 80 years with non-ST-elevation acute myocardial infarction (NSTEMI). It confirmed a lower incidence rate of the composite endpoint of death or cardiovascular events at the 1.5-year follow-up with the invasive strategy.9 However, this clinical trial did not consider frailty and included less than 25% of the possible candidates, indicative of bias in favor of elderly patients in better general health conditions and with fewer comorbidities.9 The MOSCA clinical trial10 included 106 elderly patients with NSTEMI and comorbidities. Although there were fewer chances of death or ischemic events in this study at the 3-month follow-up in patients randomized to the invasive strategy, no benefits were seen with this strategy at the end of the follow-up (2.5 years).
Currently underway, the MOSCAFRAIL clinical trial11 will assess the efficacy and safety of the invasive strategy and its prognostic effect within the first year after NSTEMI in elderly patients with confirmed frailty. This trial, that included over 10 tertiary and secondary Spanish hospitals, is a systematic geriatric and comorbidity study conducted with widely validated scales. Its results should provide valuable information and greatly impact clinical practice in the coming future.
Another controversial issue with studies of elderly patients with ACS is what clinical outcomes should be assessed. Most randomized and observational studies focus on “traditional” clinical outcomes like mortality or ischemic events. However, on many occasions there are no data on the impact on symptoms, perceived quality of life, and need for readmission, which may indicate better the clinical benefits of this population. In this sense, we should mention the After Eighty clinical trial found no differences regarding quality of life between patients treated with the invasive strategy and those treated conservatively.12
In conclusion, elderly patients with high comorbidities who are hospitalized due to NSTEACS are a common problem today and will remain so in the future. Given the scarce scientific evidence on the therapeutic approach of these patients, studies like the one conducted by Pernias et al.5 improve our understanding of this complicated clinical scenario and remind us of the importance of collaborative research to conduct large registries that show the reality of this emerging problem in our setting.
FUNDING
No funding was received for this work.
CONFLICTS OF INTEREST
None reported.
REFERENCES
1. Instituto Nacional de Estadística. Edad Media de la Población por provincia, según sexo. Available online: https://www.ine.es/jaxiT3/Datos.htm?t=3199#!tabs-tabla. Accessed 11 Jul 2020.
2. Dégano IR, Elosua R, Marrugat J. Epidemiología del síndrome coronario agudo en España:estimación del número de casos y la tendencia de 2005 a 2049. Rev Esp Cardiol. 2013;66:472-481.
3. Tahhan AS, Vaduganathan M, Greene SJ, et al. Enrollment of Older Patients, Women, and Racial/Ethnic Minority Groups in Contemporary Acute Coronary Syndrome Clinical Trials:A Systematic Review. JAMA Cardiol. 2020;5:714-722.
4. Roffi M, Patrono C, Collet J-P, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2016;37:267-315.
5. Pernias V, García Acuña JM, Raposeiras-Roubín S. Influencia de las comorbilidades en la decisión del tratamiento invasivo en ancianos con SCASEST. REC Interv Cardiol. 2021;3:19-24.
6. Canivell S, Muller O, Gencer B, et al. Prognosis of cardiovascular and non-cardiovascular multimorbidity after acute coronary syndrome. PLoS One. 2018;13:e0195174.
7. Alegre O, Formiga F, López-Palop R, et al. An Easy Assessment of Frailty at Baseline Independently Predicts Prognosis in Very Elderly Patients With Acute Coronary Syndromes. J Am Med Dir Assoc. 2018;19:296-303.
8. LlaóI, Ariza-SoléA, Sanchís J, et al. Invasive strategy and frailty in very elderly patients with acute coronary syndromes. EuroIntervention. 2018;14:e336-e342.
9. Tegn N, Abdelnoor M, Aaberge L, et al. Invasive versus conservative strategy in patients aged 80 years or older with non-ST-elevation myocardial infarction or unstable angina pectoris (After Eighty study):An openlabel randomised controlled trial. Lancet. 2016;387:1057-1065.
10. Sanchis J, Núñez E, Barrabés JA, et al. Randomized comparison between the invasive and conservative strategies in comorbid elderly patients with non-ST elevation myocardial infarction. Eur J Intern Med. 2016;35:89-94.
11. Sanchis J, Ariza-SoléA, Abu-Assi E, et al. Invasive Versus Conservative Strategy in Frail Patients With NSTEMI:The MOSCA-FRAIL Clinical Trial Study Design. Rev Esp Cardiol. 2019;72:154-159.
12. Tegn N, Abdelnoor M, Aaberge L, et al. Health-related quality of life in older patients with acute coronary syndrome randomised to an invasive or conservative strategy. The After Eighty randomised controlled trial. Age Ageing. 2018;47:42-47.
During the second half of 2019, cangrelor started selling in our country, a “new” antiplatelet drug with especial pharmacological properties that make it especially appealing for the management of certain clinical situations in the percutaneous coronary intervention (PCI) setting. The adjective “new” is in quotation marks because the clinical trial conducted proved its superiority compared to clopidogrel with ICP. The CHAMPION PHOENIX trial1 was published in 2013 and it was approved by regulatory authorities back in 2015. This delay has probably caused the scientific evidence to lose relevance and, in consequence this drug might not be widely accepted within the cardiology community. Also, the indication specified in the technical label is only based on the conditions of the clinical trial that prompted its approval—which is mandatory—not on real-world practices. This may be confusing when selecting those patients who may benefit from this drug.2
In short, cangrelor is an intravenous reversible, high-affinity antagonist of the platelet P2Y12 receptor of adenosine diphosphate to which it binds directly (without need for conversion into an active metabolite). In pharmacodynamic terms, the properties of cangrelor are: a) rapid onset of action (3 to 6 minutes); b) powerful dose-dependent effect (inhibition > 90% of the P2Y12 receptor signaling pathway) in relation to the dose used in the PCI; and c) rapid offset of action (shot half-life of 3 to 5 minutes) with recovery of the baseline platelet function in 60 to 90 minutes after infusion.3
Given its pharmacological properties, cangrelor may help solve some of the problems posed by other antiplatelet agents. For example, oral P2Y12 receptor inhibitors (iP2Y12), especially clopidogrel and to a lesser extent prasugrel and ticagrelor, have a delayed optimal platelet inhibition, which is even more significant in the ST-segment elevation myocardial infarction (STEMI) setting, where the bioavailability of oral drugs may be compromised (worse intestinal absorption, vomiting, use of opioids or situations like intubation, therapeutic hypothermia or cardiogenic shock).3,4 Also, despite their efficacy in reducing thrombotic events, the use of parenteral glycoprotein IIb/IIIa inhibitors, may be associated with a higher risk of bleeding.
The clinical development of cangrelor as a coadjuvant therapy in the PCI setting is based on the CHAMPION program, in which the first 2 studies conducted (CHAMPION PCI5 and CHAMPION PLATFORM6) were prematurely interrupted due to their futility, in part attributed to a restrictive definition of myocardial infarction.3,7 On the contrary, the CHAMPION PHOENIX clinical trial did prove the superiority of cangrelor vs clopidogrel reducing the main variable of efficacy (a composite of death, myocardial infarction, ischemia guided revascularization or stent thrombosis) after 48 hours in patients who underwent PCI to treat stable angina or any type of acute coronary syndrome (ACS) and who were not eligible for oral iP2Y12 pretreatment.1 We should mention that in a combined analysis of the 3 trials, cangrelor was associated with a slightly higher risk of bleeding mainly at the cost of minor bleeding;8 this good safety profile is probably due to the fact that the drug is administered over a very limited span of time and its effect rapidly goes away after infusion.
The CHAMPION PHOENIX trial has received 2 important criticisms that may condition its implementation in our routine clinical practice. The first is that cangrelor was never compared to prasugrel or ticagrelor (more powerful and effective than clopidogrel and drugs of choice in patients with ACS). The second is that iP2Y12 pretreatment before the PCI was considered an exclusion criterion. We should remember that, although there are serious doubts about its pretreatment benefit in the ACS setting, especially in the non-ST-segment elevation acute coronary syndrome setting,9 this strategy is widely used in our country. As a matter of fact, the European technical label of this drug specifically says that cangrelor is indicated in association with acetylsalicylic acid in patients “who undergo PCI and have not received an oral P2Y12 inhibitor before the PCI, and in whom oral treatment with P2Y12 inhibitors is not possible or desired”.2 Still, the pharmacological properties of cangrelor make it especially interesting in situations where not only the aforementioned pretreatment has not occurred, but also in circumstances where it is considered insufficient. Proof of this is the experience published from the Swedish national registry (SCAAR) during the first 2 years of drug use that found an almost exclusive use of cangrelor in patients with STEMI who underwent primary percutaneous coronary intervention; in this real-world study, cangrelor was combined with ticagrelor mainly, although the latter had already been administered in over 50% of the times in the prehospital setting, which is why in such cases the use of cangrelor would be considered an off-label indication.10
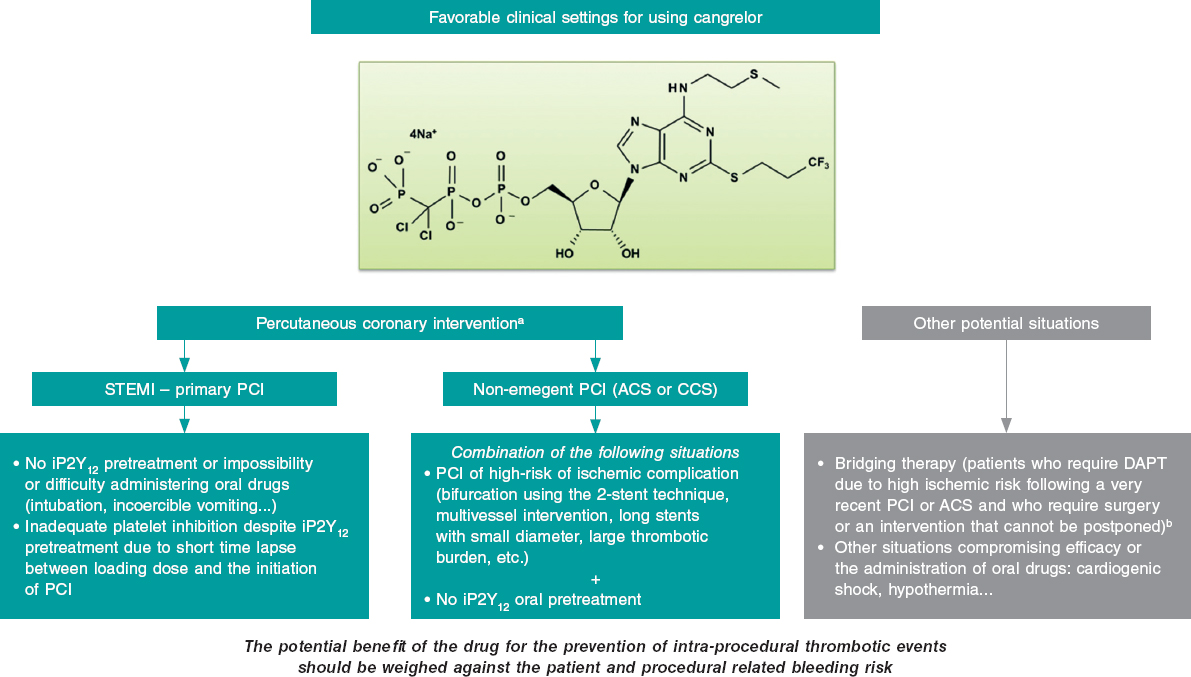
The clinical settings where, in our opinion, cangrelor can be useful both in the PCI setting (most of the cases) and in other situations are shown on figure 1. The most relevant setting would be the primary percutaneous coronary intervention in the management of STEMI, where its use is appropriate in the absence of proper pretreatment with iP2Y12 due to the impossibility or difficulty administering oral drugs (intubation or incoercible vomiting); it may also be considered if the loading dose of iP2Y12 is ineffective during the procedure (short span of time elapsed from its administration until the PCI is performed). Another acceptable situation (much less common than the latter) would be non-emergent high-risk PCIs (such as bifurcations using the dual stent technique, multivessel interventions, in the presence of great thrombotic load, etc.) in patients without iP2Y12 pretreatment. In any case, the drug potential benefit should always be weighed to prevent intraprocedural thrombotic events associated with the procedure and the patient’s bleeding risk. Also, we should remember that the use of cangrelor is ill-advised if glycoprotein IIb/IIIa inhibitors are going to be administered.
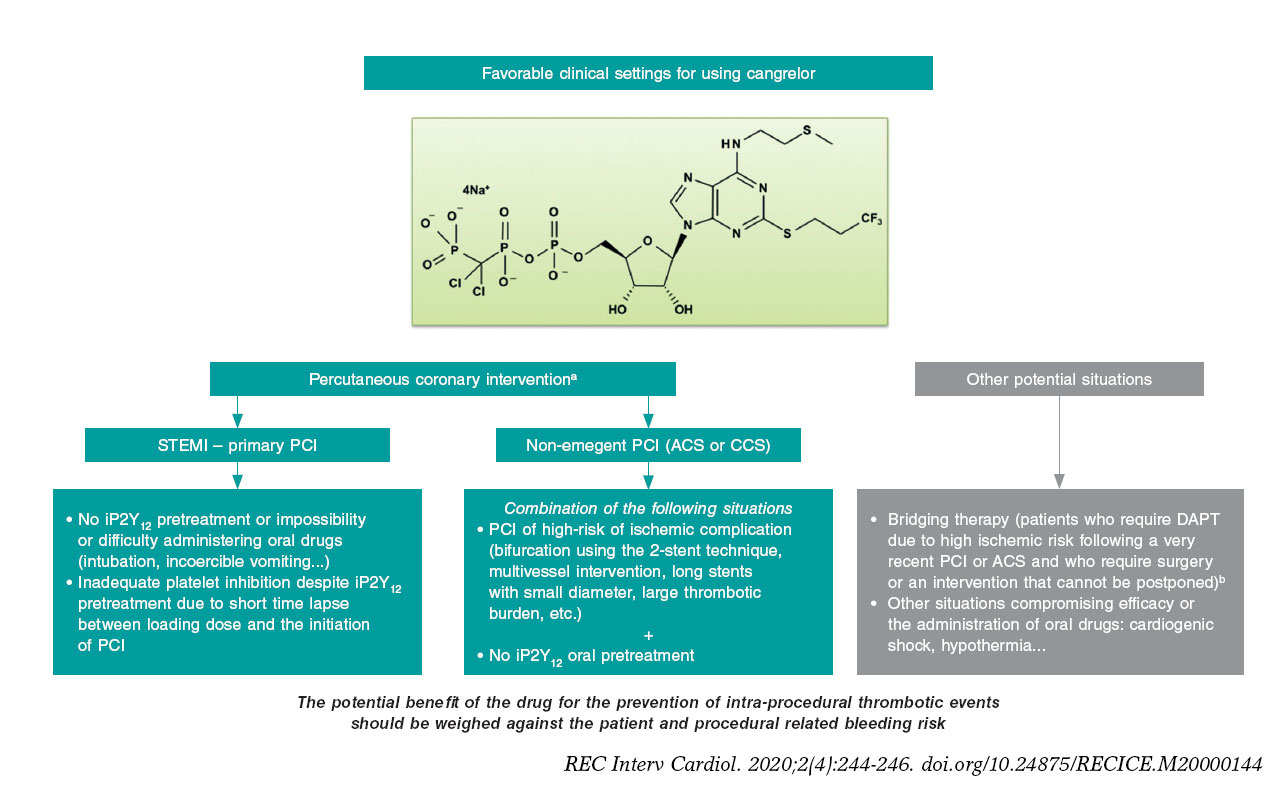
Figure 1. Potential favorable clinical settings for the use of cangrelor. ACS, acute coronary syndrome; CCS, chronic coronary syndrome; DAPT, dual antiplatelet therapy; iP2Y12, platelet P2Y12 receptor inhibitors; PCI, percutaneous coronary intervention; STEMI, ST-segment-elevation acute myocardial infarction.
a) The dose in the percutaneous coronary intervention setting should be 30 µg/kg in bolus followed by an infusion at rate of 4 µg/kg/min.
b) The dose studied in the bridging therapy is an infusion of 0.75 µg/kg/min.
Other relevant aspects are the duration of infusion that can be reasonably maintained for at least 2 hours after the PCI. According to the drug technical label, it should be started before the procedure and the infusion lasting at least 2 hours or for as long as the pro- cedure lasts, which ever is longer. Still, this may not be enough in situations where the oral drugs early action is delayed. Also, special care is needed when transitioning to oral drugs; in general, the recommendation here is that ticagrelor can be administered at all times (before, during or after infusion) while thienopyridines can be prescribed after infusion (to avoid an interaction that would imply a time lapse without the proper antiplatelet therapy).3
Taking all this into consideration, cangrelor should be primarily used in the cath lab in situations of periprocedural high thrombotic risk when oral iP2Y12 pretreatment has not occurred, is ill-advised or insufficient. The availability of the drug will probably not change our antiplatelet strategy radically in the short term in the PCI setting. However, in some situations (especially primary percutaneous coronary interventions) its particular pharmacological profile will be very useful. Therefore, its use will probably grow in the interventional cardiology community as we become more familiar with it. In conclusion, cangrelor is an interesting addition to our therapeutic armamentarium in the PCI setting because it can individualize and, therefore, optimize our antithrombotic strategy.
CONFLICTS OF INTEREST
J.L. Ferreiro has declared he has received funds for his lectures for Eli Lilly Co., Daiichi Sankyo, Inc., AstraZeneca, Roche Diagnostics, Pfizer, Abbott, Boehringer Ingelheim, Bristol-Myers Squibb, and Ferrer; also, he has received funds for his counselling for AstraZeneca, Eli Lilly Co., Ferrer, Boston Scientific, Pfizer, Boehringer Ingelheim, Daiichi Sankyo, Inc., Bristol-Myers Squibb; he has also receive research grants from AstraZeneca. J.A. Gómez-Hospital has declared he has received funds for his counselling for Abbott, Medtronic, Boston Scientific, Terumo, and IHT.
REFERENCES
1. Bhatt DL, Stone GW, Mahaffey KW, et al. Effect of platelet inhibition with cangrelor during PCI on ischemic events. N Engl J Med. 2013;368: 1303-1313.
2. Kengrexal. Technical label or summary of product characteristics. Available online: https://cima.aemps.es/cima/pdfs/es/ft/115994001/FT_115994001.pdf. Accessed 18 May 2020.
3. Marcano AL, Ferreiro JL. Role of New Antiplatelet Drugs on Cardiovascular Disease: Update on Cangrelor. Curr Atheroscler Rep. 2016;18:66.
4. Ferreiro JL, Sánchez-Salado JC, Gracida M, et al. Impact of mild hypothermia on platelet responsiveness to aspirin and clopidogrel: an in vitro pharmacodynamic investigation. J Cardiovasc Transl Res. 2014;7:39-46.
5. Harrington RA, Stone GW, McNulty S, et al. Platelet inhibition with cangrelor in patients undergoing PCI. N Engl J Med. 2009;361: 2318-2329.
6. Bhatt DL, Lincoff AM, Gibson CM, et al. Intravenous platelet blockade with cangrelor during PCI. N Engl J Med. 2009;361:2330-2341.
7. White HD, Chew DP, Dauerman HL, et al. Reduced immediate ischemic events with cangrelor in PCI: a pooled analysis of the CHAMPION trials using the universal definition of myocardial infarction. Am Heart J. 2012;163:182-190.e4.
8. Steg PG, Bhatt DL, Hamm CW, et al. Effect of cangrelor on periprocedural outcomes in percutaneous coronary interventions: a pooled analysis of patient-level data. Lancet. 2013;382:1981-1992.
9. Ferreiro JL. Pre-Treatment With Oral P2Y12 Inhibitors in Non-ST-Segment Elevation Acute Coronary Syndromes: Does One Size Fit All? JACC Cardiovasc Interv. 2020;13:918-920.
10. Grimfjärd P, Lagerqvist B, Erlinge D, Varenhorst C, James S. Clinical use of cangrelor: nationwide experience from the Swedish Coronary Angiog raphy and Angioplasty Registry (SCAAR). Eur Heart J Cardiovasc Pharmacother. 2019;5:151-157.
- Routine endomyocardial biopsy in heart transplantation: in search of lost evidence
- Spontaneous coronary artery dissection: new insights on diagnosis and management
- Transcatheter mitral valve replacement: there is no one-size-fits-all solution
- Scientific debates among professionals in social media: a fantastic, but not risk-free scenario
Subcategories







Interviews

An interview with Bruno Scheller
aServicio de Cardiología, Hospital Universitario de La Princesa, Instituto de Investigación Sanitaria de La Princesa (IIS-IP), Universidad Autónoma de Madrid, Spain
bCentro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain




