
ABSTRACT
Introduction and objectives: Plaque modification techniques are important for the percutaneous treatment of severely calcified coronary lesions. The aim of this study was to retrospectively analyze patients who underwent orbital atherectomy for calcified coronary lesions at a hospital without on-site cardiac surgery.
Methods: Patients treated with orbital atherectomy between April 2021 and April 2025 were included. Procedural success was analyzed, defined as treatment of the target vessel with < 20% residual percent diameter stenosis and final TIMI grade-3 flow, as well as the composite endpoint of target vessel failure (TVF) at 12 months.
Results: A total of 116 patients were included, with a mean age of 73.24 years; 82.2% were male and 77 cases (66.4%) were admitted for acute coronary syndrome. The procedural success rate with adequate angiographic results was 98.3%. Regarding immediate complications, 1 patient died during the procedure (0.9%), 2 patients presented coronary dissection (1.7%), 3 presented coronary perforation (2.6%), and 2 experienced slow-flow or no reflow phenomena (1.7%). Mean clinical follow-up was 1.63 ± 1.2 years. The cumulative incidence rate of acute myocardial infarction was 19.3% (95%CI, 11.7-26.9); target vessel revascularization (TVR), 16.3% (95%CI, 3.7-28.9); stent thrombosis, 1.8% (95%CI, 0-4.3); and symptom-guided target lesion revascularization (TLR), 8.7% (95%CI, 0.1-16.3). All-cause mortality rate was 16.7% (95%CI,7.2–26.2), and cardiovascular mortality was 5.4% (95%CI, 1.3-9.5). Target vessel failure showed a cumulative incidence rate at the 12-month follow-up of 10% (95%CI, 3.8-16.2).
Conclusions: We present a large real-world registry of patients with calcified coronary lesions treated with orbital atherectomy (OA), showing a high procedural success rate and a low complication rate during long-term follow-up.
Keywords: Coronary artery calcification. Orbital atherectomy. Coronary plaque modification.
RESUMEN
Introducción y objetivos: Las técnicas de modificación de la placa son importantes para el tratamiento percutáneo de las lesiones coronarias con calcificación grave. El objetivo de este estudio fue analizar de forma retrospectiva los pacientes sometidos a aterectomía orbitacional en lesiones coronarias calcificadas en un hospital sin cirugía cardiaca.
Métodos: Se incluyeron pacientes tratados con aterectomía orbitacional desde abril de 2021 hasta abril de 2025. Se analizaron el éxito del procedimiento, definido como tratamiento del vaso diana con estenosis residual menor del 20% y flujo TIMI 3 final, y la variable combinada denominada fallo del vaso diana a 12 meses.
Resultados: Del total de 116 pacientes, con una edad media de 73,24 años y el 82,2% varones, 77 (66,4%) ingresaron por síndrome coronario agudo. La tasa de éxito con adecuado resultado angiográfico fue del 98,3%. Respecto a las complicaciones inmediatas: 1 paciente falleció durante el procedimiento (0,9%), 2 presentaron disección coronaria (1,7%), 3 tuvieron perforación coronaria (2,6%) y 2 mostraron reflujo lento o nulo (1,7%). El seguimiento clínico fue de 1,63 ± 1,2 años, con una incidencia acumulada de infarto agudo de miocardio del 19,3% (IC95%, 11,7-26,9), revascularización del vaso diana en el 16,3% (IC95%, 3,7-28,9), trombosis del stent en el 1,8% (IC95%, 0-4,3) y revascularización de la lesión diana guiada por síntomas en el 8,7% (IC95% 0,1-16,3). La mortalidad por todas las causas fue del 16,7% (IC95%, 7,2-26,2) y por causa cardiovascular del 5,4% (IC95%, 1,3-9,5). El fallo del vaso diana a 12 meses tuvo una tasa de incidencia acumulada a los 12 meses de seguimiento del 10% (IC95%, 3,8-16,2).
Conclusiones: Presentamos un amplio registro de la vida real de pacientes con lesiones coronarias calcificadas tratados con aterectomía orbitacional, con una alta tasa de éxito del procedimiento y una baja tasa de complicaciones en el seguimiento a largo plazo.
Palabras clave: Calcificación arterial coronaria. Aterectomía orbitacional. Modificación de placa coronaria.
Abbreviations
CAC: coronary artery calcification. OA: orbital atherectomy. TLR: target lesion revascularization. TVR: target vessel revascularization. TVF: target vessel failure.
INTRODUCTION
Coronary artery calcification (CAC) is a consequence of the progression of atherosclerotic disease, as well as an independent predictor of major adverse cardiovascular events (MACE).1,2 The etiology of CAC is multifactorial, and, among other clinical conditions, is associated with conventional cardiovascular risk factors, ethnicity, and chronic kidney disease.3-6
Patients with CAC have worse short- and long-term follow-up outcomes after percutaneous coronary intervention (PCI), including lower rates of complete revascularization and higher risks of stent underexpansion, coronary dissection, coronary perforation, and stent deformation or loss.7-10 Furthermore, CAC has been associated with a higher risk of in-stent restenosis and a greater long-term need for target lesion revascularization (TLR). In addition, approximately 50% of stents implanted in calcified lesions show asymmetric expansion, which increases the risk of stent thrombosis or in-stent restenosis.11-14 Adequate lesion preparation before stent implantation is therefore essential to reduce procedural difficulty and prevent complications. Dedicated techniques for calcified lesion modification, including calcium ablation or fracture, can improve vascular compliance. Among these techniques, orbital atherectomy (OA) has shown favorable results in the treatment of CAC and is the focus of the present study.15
METHODS
We conducted a retrospective observational study including all patients with significant calcified coronary lesions treated with OA. The aim of the study was to assess the safety and efficacy profile of OA for the treatment of patients with CAC in a hospital without on-site cardiac surgery in Spain.
The primary endpoint was procedural success, defined as treatment of the target vessel with residual percent diameter stenosis < 20% and final TIMI grade-3 flow. A composite endpoint, defined as target vessel failure (TVF) at 12 months, included cardiac death, target vessel myocardial infarction, and target vessel revascularization (TVR).
Procedure-related secondary safety endpoints included acute or subacute stent thrombosis, slow-flow or no-reflow phenomena, type C-F coronary dissections, and coronary perforations.
Clinical follow-up of the patients was performed by telephone consultation at 6 months and an in-person visit at 12 months.
The OA clinical database was approved by the Ethics Committee of the Servicio Gallego de Salud, with waiver of informed consent because of the characteristics of the study. Sex and gender variables were considered in full compliance with the SAGER guidelines.
Orbital atherectomy technique
OA is an ablative coronary technique performed using a 1.25-mm diamond-coated crown (Diamondback 360, Abbott, United States), a dedicated guidewire (ViperWire Advance, Abbott, United States), and a lubricant infused during ablation (ViperSlide, Abbott, United States). Driven by centrifugal force, the crown orbits at 2 rotational speeds (80 000 rpm or 120 000 rpm), sanding the calcium within the arterial wall and causing deep calcium fractures.16,17
Statistical analysis
Qualitative variables are expressed as number and percentage, and the quantitative ones as mean and SD. Survival curves were generated using the Kaplan-Meier method, and statistical differences in events between patients undergoing scheduled procedures and those admitted for acute coronary syndrome (ACS) were assessed using the log-rank test. A multivariate Cox regression analysis was performed to identify factors independently associated with TVF at 1 year. Variables associated with TVF in the univariable analysis at P < .1 were entered into the regression. Afterwards, the least associated variables were removed one by one using backward stepwise regression until a parsimonious model was obtained in which all variables were associated with TVF. Statistically significant difference was set at P < .05. Analyses were performed using SPSS statistical software version 17 (IBM, United States).
RESULTS
From April 2021 through April 2025, a total of 116 patients with CAC were treated with OA. Regarding the patients’ clinical charac- teristics, their mean age was 73.24 years, most were men (82.8%), and exhibited multiple classic cardiovascular risk factors. The mean left ventricular ejection fraction (LVEF) was 50.3 ± 11.9%, and up to 37.1% of patients had LVEF < 50%. Chronic kidney disease, defined as glomerular filtration rate < 60 mL/min, was present in 38.8% of patients; in 10 patients (8.6%) glomerular filtration rate was < 20 mL/min. Approximately one third of patients (30.2%) had chronic ischemic heart disease; of these, 25 (21.6%) had previously undergone revascularization by PCI and 16 (13.8%) by coronary artery bypass grafting (table 1).
Table 1. Baseline characteristics of patients treated with orbital atherectomy
| Characteristics | n = 116 |
|---|---|
| Age, years | 73.24 ± 8.23 |
| Men | 96 (82.8) |
| Height, m | 1.64 ± 0.09 |
| Weight, kg | 77.37 ± 15.59 |
| Body mass index | 28.67 ± 4.82 |
| Hypertension | 97 (83.6) |
| Dyslipidemia | 90 (77.6) |
| Diabetes mellitus | 58 (50) |
| Smoking status | |
| Nonsmokers | 62 (53.4) |
| Smokers | 13 (11.2) |
| Former smokers | 41 (35.3) |
| LVEF, % | 50.29 ± 11.93 |
| Creatinine, mg/dL | 1.41 ± 1.51 |
| GFR, mL/min/1.73 m2 | |
| < 15 | 5 (4.3) |
| 15-59 | 40 (34.5) |
| 60-89 | 53 (45.7) |
| > 90 | 18 (15.5) |
| History of coronary revascularization | 35 (30.2) |
| Previous PCI | 25 (21.6) |
| Previous CABG | 16 (13.8) |
|
CABG, coronary artery bypass grafting; GFR, glomerular filtration rate; LVEF, left ventricular ejection fraction; PCI, percutaneous coronary intervention. Data are expressed as No. (%) or mean ± SD. |
|
Regarding clinical presentation, 77 patients (66.4%) were admitted with ACS, 61 (52.1%) with non-ST-segment elevation acute coronary syndrome (NSTEACS) and 16 (13.8%) with ST-segment elevation acute coronary syndrome (STEACS). Among the latter, the artery treated with OA was the infarct-related artery in 5 cases (4.3%) (table 2). Regarding the extent of coronary artery disease, 32 patients (27.6%) had 3-vessel disease and 27 (23.3%) had left main coronary artery disease (figure 1).
Table 2. Distribution of cases based on clinical presentation
| Presentación clínica | n = 116 |
|---|---|
| Acute coronary syndrome | 77 (66.4) |
| Unstable angina | 7 (6.0) |
| NSTEACS | 54 (46.6) |
| STEACS (second-stage nonculprit lesion) | 11 (9.5) |
| STEACS (culprit lesion) | 5 (4.3) |
| Chronic ischemic heart disease | 39 (33.6) |
|
NSTEACS, non-ST-segment elevation acute coronary syndrome; STEACS, ST-segment elevation acute coronary syndrome. Data are expressed as No. (%). |
|
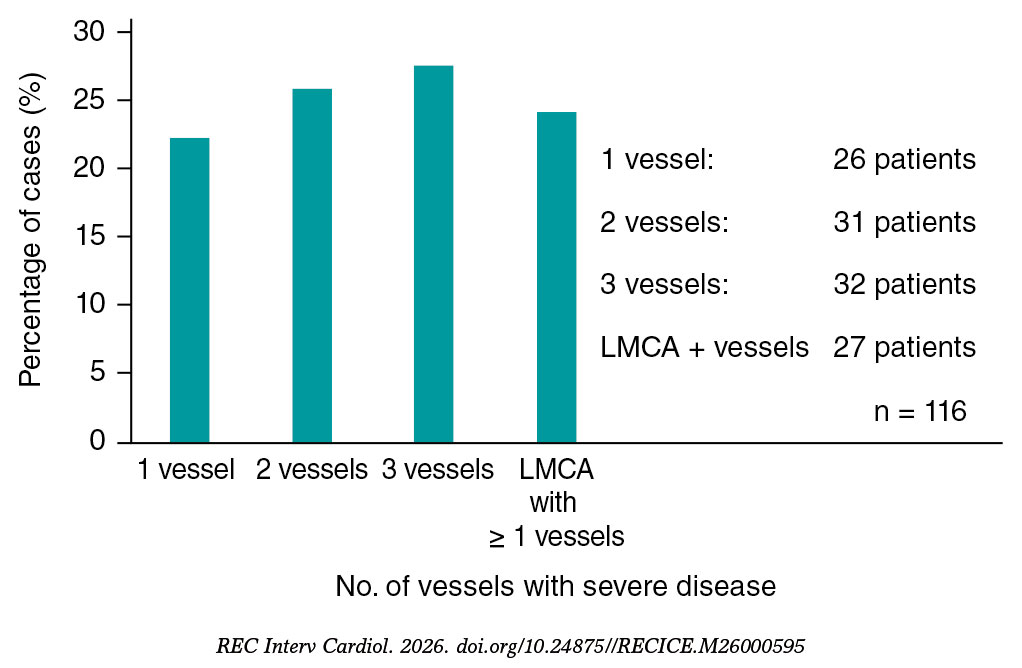
Figure 1. Distribution of cases treated with orbital atherectomy based on the number of coronary arteries with severe disease (n = 116). LMCA, left main coronary artery.
Regarding procedural characteristics, radial access was the most widely used vascular approach (77.2%). The vessel most frequently treated with OA was the left anterior descending coronary artery, in 57 cases (49.1%), followed by the right coronary artery in 34 cases (29.3%) and the left main coronary artery in 18 cases (15.5%). Intravascular imaging was used before the PCI in 42 cases (37.2%), mainly intravascular ultrasound, and after the PCI in 18 cases (15.4%). As an adjunctive plaque-modification technique to OA, a cutting balloon was used in 61 cases (52.6%), excimer laser atherectomy in 2 cases (1.7%), and intravascular lithotripsy in 1 case (0.9%). Rotational atherectomy was not used in any patient. In most patients, 1 or 2 stents were implanted (35.3% and 28.4%, respectively), with a mean stent length of 23.3 ± 6.4 mm and a mean stent diameter of 3.3 ± 0.6 mm. The mean procedure duration was 85 ± 29.5 minutes; mean fluoroscopy time, 28.7 ± 17 minutes; and mean contrast volume, 179.3 ± 65.2 mL. Procedural success rate, with an adequate angiographic result and final TIMI grade-3 flow was achieved in 98.3% of cases. Immediate complications included 1 intraprocedural death (0.9%), and in 1 case the device failed to cross the lesion (0.9%). Regarding the secondary safety endpoint, 1 patient had acute or subacute stent thrombosis (0.9%), 2 had type C-F coronary dissections (1.7%), 3 had coronary perforations (2.6%), and 2 had slow-flow or no-reflow phenomena (1.7%). Of note, all complications occurred in the subgroup of patients with ACS (table 3).
Table 3. Characteristics and materials of percutaneous coronary intervention with orbital atherectomy
| Orbital atherectomy procedure | n = 116 |
|---|---|
| Radial | 88 (77.2) |
| Femoral | 19 (16.7) |
| Other | 7 (6.1) |
| Target vessel | |
| Left anterior descending coronary artery | 57 (49.1) |
| Right coronary artery | 34 (29.3) |
| Left circumflex artery | 7 (6.0) |
| Left main coronary artery | 18 (15.5) |
| Initial TIMI grade flow | |
| 0 | 1 (0.9) |
| I | 4 (3.4) |
| II | 6 (5.2) |
| III | 105 (90.5) |
| Lesion length, mm | 36.89 ± 21.31 |
| Lesion reference diameter, mm | 3.68 ± 1.59 |
| Chronic total coronary occlusion | 1 (0.9) |
| Bifurcation | 25 (21.6) |
| Tortuosity | |
| No | 108 (93.1) |
| Mild | 4 (3.4) |
| Moderate | 3 (2.6) |
| Severe | 1 (0.9) |
| Intravascular imaging before OA | |
| IVUS | 27 (23.9) |
| OCT | 15 (13.3) |
| Intravascular imaging after OA | |
| IVUS | 9 (7.8) |
| OCT | 9 (7.8) |
| Use of other devices associated with OA | |
| Semicompliant balloon | 45 (38.8) |
| Noncompliant balloon | 63 (54.3) |
| Scoring balloon | 61 (52.6) |
| Very-high-pressure balloon | 4 (3.4) |
| Laser | 2 (1.7) |
| Intravascular lithotripsy | 1 (0.9) |
| No. of stents implanted | |
| 1 | 41 (35.3) |
| 2 | 33 (28.4) |
| 3 | 24 (20.7) |
| 4 | 9 (7.8) |
| 5 | 7 (6.0) |
| 6 | 2 (1.7) |
| Stent length, mm | 23.31 ± 6.39 |
| Stent diameter, mm | 3.34 ± 0.61 |
| Treatment with drug-coated balloon | 3 (2.6) |
| Final TIMI grade flow | |
| 0 | 1 (0.9) |
| I | 0 (0) |
| II | 2 (1.7) |
| III | 113 (98.3) |
| Procedural time, min | 85.03 ± 29.49 |
| Fluoroscopy time, min | 28.77 ± 17.03 |
| Contrast volume used, mL | 179.32 ± 65.25 |
| Procedural success | 114 (98.3) |
| Immediate complications | |
| Acute stent thrombosis | 1 (0.9) |
| Coronary dissection | 2 (1.7) |
| Coronary perforation | 3 (2.6) |
| No-flow phenomenon | 2 (1.7) |
| Intraprocedural death | 1 (0.9) |
|
IVUS, intravascular ultrasound; OA, orbital atherectomy; OCT, optical coherence tomography; TIMI, Thrombolysis in Myocardial Infarction. Data are expressed as No. (%) or mean ± SD. |
|
Mean follow-up was 1.63 ± 1.2 years, with a median of 1.48 years, Q1 of 0.53 years, and Q3 of 2.58 years. Out-of-hospital follow-up was lost in 2 cases (1.7%).
During follow-up, 11 patients had acute myocardial infarction, with a 4-year cumulative incidence rate of 19.3% (95%CI, 11.7-26.9) (figure 2A); 8 required TVR, with a 4-year cumulative incidence rate of 16.3% (95%CI, 3.7-28.9) (figure 2B); 2 had stent thrombosis, with a 4-year cumulative incidence rate of 1.8% (95%CI, 0-4.3) (figure 2C); and 4 required symptom-guided TLR, with a 4-year cumulative incidence rate of 8.7% (95%CI, 0.1-16.3) (figure 2D). There were no admissions for STEACS.
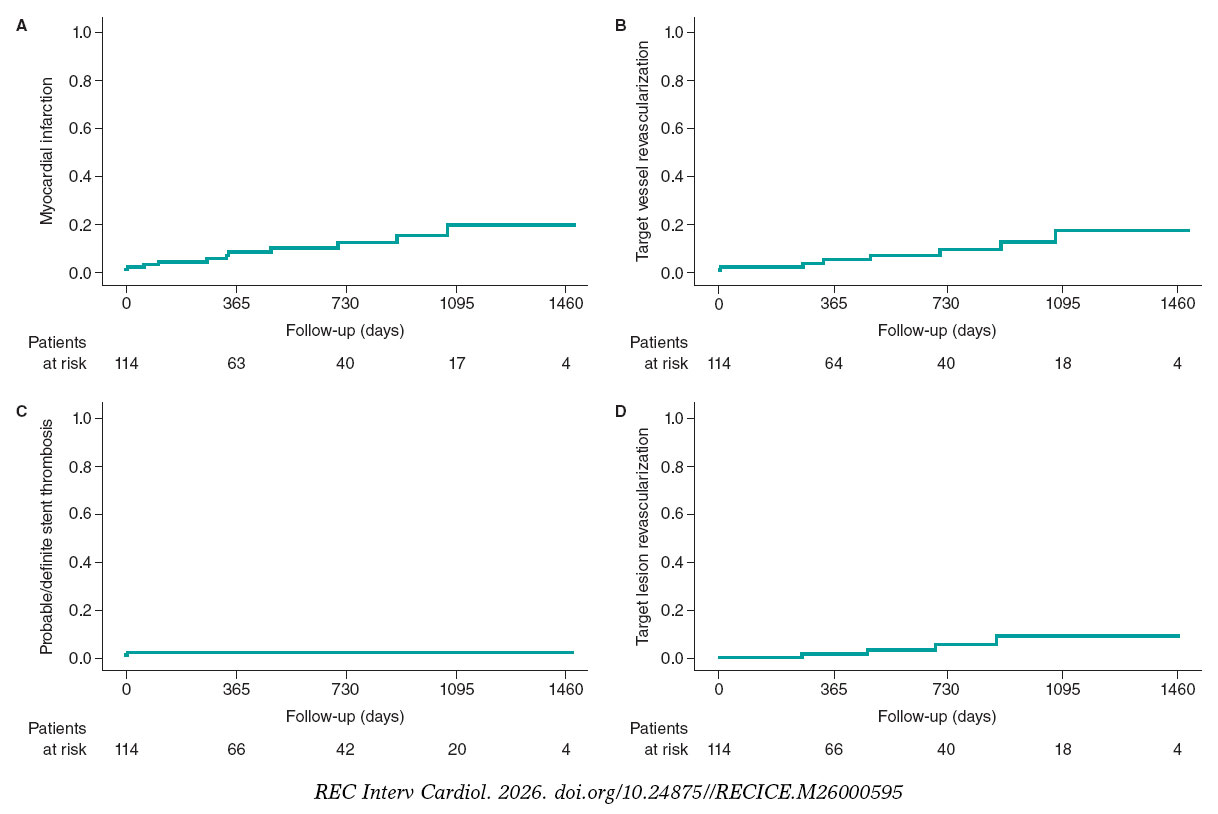
Figure 2. Cumulative incidence curves for events during follow-up: myocardial infarction (A), target vessel revascularization (B), stent thrombosis (C), and symptom-guided target lesion revascularization (D).
During follow-up, 13 patients died, with a 4-year cumulative incidence rate of 16.7% (95%CI, 7.2-26.2) (figure 3A). Cardiovascular mortality occurred in 7 cases, with a 4-year cumulative incidence rate of 5.4% (95%CI, 1.3-9.5) (figure 3B). When noncardiovascular mortality was analyzed, 3 patients died of severe infection or septic shock, 2 of cancer, and 1 of an accidental cause.
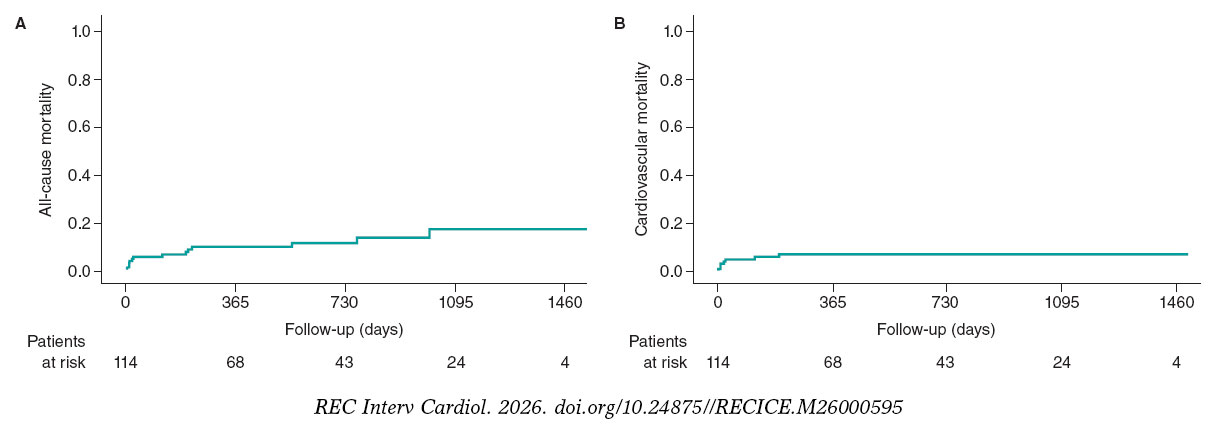
Figure 3. Kaplan-Meier mortality curves during follow-up: all-cause (A) and cardiovascular mortality (B).
The composite endpoint occurred in 10 patients, with a 12-month cumulative incidence rate of 10% (95%CI, 3.8-16.2).
Multivariable analysis showed that age < 70 years (HR, 0.35; 95%CI, 0.14-0.92), LVEF as a continuous variable (HR, 0.92; 95%CI, 0.88-0.96), and presentation as ACS (HR, 3.95; 95%CI, 1.12-13.97) were independent predictors of TVF during follow-up.
DISCUSSION
CAC is associated with an increase in adverse clinical events related to percutaneous revascularization procedures.18 OA has emerged as a safe and effective technology for the percutaneous treatment of CAC across its entire clinical spectrum. Although robust scientific evidence exists for uncrossable lesions remains limited, favorable clinical experiences with its use have been reported.19
In the registry by Lee et al.,18 stent implantation was successful in 99.1% of patients, with low rates of angiographic complications. The 30-day MACE rate, defined as a composite of cardiac death, myocardial infarction, target vessel revascularization, and stroke, was 1.7%, and the 30-day all-cause mortality rate was low, at 1.3%. Although our registry included a smaller sample, the proportions of patients with acute myocardial infarction, a past medical history of chronic ischemic heart disease, and chronic kidney disease were higher, reflecting a greater burden of high-risk clinical features. Despite this, our procedural success and immediate complication rates were comparable.
The ORBIT I study evaluated OA for the treatment of de novo calcified coronary lesions and showed sustained favorable outcomes at 5 years. Procedural success was achieved in 94% of cases. The cumulative MACE rate, defined as a composite of cardiac death, myocardial infarction, and target vessel revascularization, was 4% during hospitalization, 6% at 30 days, 8% at 6 months, 18.2% at 3 years, and 21.2% at 5 years. The rate of cardiovascular mortality was 6.1% at 2 years, 9.1% at 3 years, and 12.1% at 5 years.20-22 Of note, compared with the ORBIT I study, our registry included more than twice as many patients and a population at higher cardiovascular risk. Even so, procedural success was higher in our series (98%), and cardiovascular mortality at a mean follow-up of 1.6 years was lower than that reported in the ORBIT I beyond 2 years (5.4% vs 6.1%).
The ORBIT II study evaluated OA for de novo calcified lesions, with successful stent implantation in 97.7% and residual percent diameter stenosis < 50% in 98.6% of patients. Regarding complications, immediate and 30-day cardiovascular mortality rate was 0.2%, with low rates of severe coronary dissection, coronary perforation, slow-flow phenomenon, and acute coronary occlusion.23 These rates were similar to or lower than those reported in previous studies of rotational atherectomy, such as the ROTAXUS.24,25 The MACE rate in the ORBIT II, defined as a composite of cardiac death, myocardial infarction, and target vessel revascularization, was 16.4% at the 1-year follow-up, 19.4% at 2 years, and 23.5% at 3 years. The cardiovascular mortality at 1, 2, and 3 years was 3%, 4.3%, and 6.7%, respectively.26-28 In our registry, with a mean follow-up of 1.6 years, the rate of cardiovascular mortality was slightly higher than that reported in the ORBIT II study at 2 years (5.4% vs 4.3%). A factor that could have possibly influenced our results is that > 60% of patients in our series presented with ACS, whereas this population was excluded from the ORBIT II. In addition, the ORBIT II study excluded patients with chronic kidney disease, except those receiving dialysis, patients with serum creatinine levels > 2.5 mg/dL, and those with LVEF ≤ 25%, whereas our study included a higher-risk cardiovascular population. The ROLLER COASTR-EPIC2229 study compared rotational atherectomy, intravascular lithotripsy, and excimer laser atherectomy for the treatment of patients with CAC. The study showed that intravascular lithotripsy is noninferior to rotational atherectomy in terms of stent expansion, whereas excimer laser atherectomy did not meet the criterion for noninferiority compared with rotational atherectomy. In this context, we believe that a clinical trial including OA would be necessary and of substantial practical value to compare the optimal strategy for the treatment of CAC.
The ECLIPSE study compared OA with balloon angioplasty in severely calcified lesions and concluded that the ideal scenario for OA use would be lesions with severe superficial or nodular calcification that are nondilatable or cannot be crossed with a balloon.30 In the ECLIPSE study, 12-month TVF in the OA group was 11.5%, compared with 10% in our series, and procedural success was 86%, compared with 98% in our series. Compared with our registry, the ECLIPSE population had lower cardiovascular risk characteristics: 44% of patients had diabetes compared with 50% in our study, 24% had chronic kidney disease compared with 38.8% in our study, and the mean age was 70 years compared with 73 years in our study. In addition, the ECLIPSE study only included 13.7% of patients with ACS, including 1.3% with STEACS, compared with 66.4% with ACS (13.8% with STEACS) in our study. Thus, despite including a higher-risk population, our registry showed a higher stent implantation success rate and a slightly lower 12-month TVF rate.
Limitations
This study has several limitations. First, it is a retrospective observational registry from a single hospital; therefore, the findings may not be generalizable of other centers. Second, the OA technique is associated with a learning curve, and the results cannot be extrapolated to hospitals without experience in this technique. Third, the use of intravascular imaging was relatively low, at approximately 40% of cases, which may have led to underestimation of the severity of coronary lesion calcification. However, the use of intravascular imaging in this registry was slightly higher than that reported in previous real-world registries.
CONCLUSIONS
This large real-world registry of patients with CAC treated with OA showed a high procedural success rate and a low complication rate during long-term follow-up.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
The orbital atherectomy care database was approved by the Ethics Committee of the SERGAS of Hospital Universitario Lucus Augusti, and the requirement for informed consent was waived because of the characteristics of the study. Sex and gender variables were considered in full compliance with the SAGER guidelines.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
Artificial intelligence was not used in the preparation of the article.
AUTHORS’ CONTRIBUTIONS
J. Bayón drafted the manuscript and prepared the images. R.A. Mori-Junco reviewed the manuscript. A. Negrete-Marcolongo and A. López-Pena participated in the literature search. C. González- Juanatey performed the final review of the manuscript. All authors approved the final version.
CONFLICTS OF INTEREST
J. Bayón is a proctor for Abbott Diamondback 360 orbital atherectomy. The remaining authors declared no conflicts of interest whatsoever.
WHAT IS KNOWN ABOUT THE TOPIC?
- Orbital atherectomy is a plaque-modification technique for calcified coronary lesions, with safety and efficacy data in patients with stable coronary artery disease.
WHAT DOES THIS STUDY ADD?
- Our registry provides real-world data on a large series of patients with calcified coronary artery disease treated with orbital atherectomy, two thirds of whom presented with acute coronary syndrome. The stent implantation rate was approximately 98%, comparable to that reported in previous studies, with relatively low rates of complications and mortality during follow-up beyond 12 months.
REFERENCES
1. Mohan J, Shams P, Bhatti K, Zelster R. Coronary Artery Calcification. [Internet]. Treasure Island (FL):StatPearls Publishing;2026. Available at:https://www.ncbi.nlm.nih.gov/books/NBK519037/.
2. Onnis C, Virmani R, Kawai K, et al. Coronary Artery Calcification:Current Concepts and Clinical Implications. Circulation. 2024;149:251-266.
3. Mori H, Torii S, Kutyna M, et al. Coronary Artery Calcification and its Progression:What Does it Really Mean?JACC Cardiovasc Imaging. 2018;11:127-142.
4. Vervloet M, Cozzolino M. Vascular calcification in chronic kidney disease:different bricks in the wall?Kidney Int. 2017;91:808-817.
5. Carson AP, Steffes MW, Carr JJ, et al. Hemoglobin a1c and the progression of coronary artery calcification among adults without diabetes. Diabetes Care. 2015;38:66-71.
6. Bild DE, Detrano R, Peterson D, et al. Ethnic differences in coronary calcification:the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2005;111:1313-1320.
7. Genereux P, Madhavan MV, Mintz GS, et al. Ischemic outcomes after coronary intervention of calcified vessels in acute coronary syndromes. Pooled analysis from the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) and ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) trials. J Am Coll Cardiol. 2014;63:1845-1854.
8. Kawashima H, Serruys PW, Hara H, et al. 10-Year All-Cause Mortality Following Percutaneous or Surgical Revascularization in Patients With Heavy Calcification. JACC Cardiovasc Interv. 2022;15:193-204.
9. Kobayashi Y, Okura H, Kume T, et al. Impact of target lesion coronary calcification on stent expansion. Circ J. 2014;78:2209-2214.
10. Genereux P, Madhavan MV, Mintz GS, et al. Relation between coronary calcium and major bleeding after percutaneous coronary intervention in acute coronary syndromes (from the Acute Catheterization and Urgent Intervention Triage Strategy and Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction Trials). Am J Cardiol. 2014;113:930-935.
11. Bourantas CV, Zhang YJ, Garg S, et al. Prognostic implications of coronary calcification in patients with obstructive coronary artery disease treated by percutaneous coronary intervention:a patient-level pooled analysis of 7 contemporary stent trials. Heart. 2014;100:1158-1164.
12. Konigstein M, Madhavan MV, Ben-Yehuda O, et al. Incidence and predictors of target lesion failure in patients undergoing contemporary DES implantation-Individual patient data pooled analysis from 6 randomized controlled trials. Am Heart J. 2019;213:105-111.
13. Guedeney P, Claessen BE, Mehran R, et al. Coronary Calcification and Long-Term Outcomes According to Drug-Eluting Stent Generation. JACC Cardiovasc Interv. 2020;13:1417-1428.
14. Kawashima H, Serruys PW, Hara H, et al. 10-Year All-Cause Mortality Following Percutaneous or Surgical Revascularization in Patients With Heavy Calcification. JACC Cardiovasc Interv. 2022;15:193-204.
15. Jurado-Román A, Gómez-Menchero A, Gonzalo N, et al. Plaque modification techniques to treat calcified coronary lesions. Position paper from the ACI-SEC. REC Interv Cardiol. 2023;5:46-61.
16. Shlofmitz E, Martinsen BJ, Lee M, et al. Orbital atherectomy for the treatment of severely calcified coronary lesions:evidence, technique, and best practices. Expert Rev Med Devices. 2017;14:867-879.
17. Kirtane AJ, Ribichini F. Atherectomy for calcified plaques:orbital for most?Pros and cons. EuroIntervention. 2024;20:e627-e629.
18. Lee MS, Shlofmitz E, Kaplan B, et al. Real-World Multicenter Registry of Patients with Severe Coronary Artery Calcification Undergoing Orbital Atherectomy. J Interv Cardiol. 2016;29:357-362.
19. Bayón J, Mori-Junco RA, JuskováM, et al. Feasibility and safety of orbital atherectomy in uncrossable lesions. REC Interv Cardiol. 2025;7:269-271.
20. Parikh K, Chandra P, Choksi N, et al. Safety and feasibility of orbital atherectomy for the treatment of calcified coronary lesions:the ORBIT I trial. Catheter Cardiovasc Interv. 2013;81:1134-1139.
21. Bhatt P, Parikh P, Patel A, et al. Orbital atherectomy system in treating calcified coronary lesions:3-Year follow-up in first human use study (ORBIT I trial). Cardiovasc Revasc Med. 2014;15:204-208.
22. Bhatt P, Parikh P, Patel A, et al. Long-term safety and performance of the orbital atherectomy system for treating calcified coronary artery lesions:5-Year follow-up in the ORBIT I trial. Cardiovasc Revasc Med. 2015;16: 213-216.
23. Chambers JW, Feldman RL, Himmelstein SI, et al. Pivotal trial to evaluate the safety and efficacy of the orbital atherectomy system in treating de novo, severely calcified coronary lesions (ORBIT II). JACC Cardiovasc Interv. 2014;7:510-518.
24. Abdel-Wahab M, Richardt G, Joachim Büttner H, et al. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions:the randomized ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) trial. JACC Cardiovasc Interv. 2013;6:10-19.
25. de Waha S, Allali A, Büttner HJ, et al. Rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions:two-year clinical outcome of the randomized ROTAXUS trial. Catheter Cardiovasc Interv. 2016;87:691-700.
26. Généreux P, Lee AC, Kim CY, et al. Orbital Atherectomy for Treating De Novo Severely Calcified Coronary Narrowing (1-Year Results from the Pivotal ORBIT II Trial). Am J Cardiol. 2015;115:1685-1690.
27. Généreux P, Bettinger N, Redfors B, et al. Two-year outcomes after treatment of severely calcified coronary lesions with the orbital atherectomy system and the impact of stent types:Insight from the ORBIT II trial. Catheter Cardiovasc Interv. 2016;88:369-377.
28. Lee M, Généreux P, Shlofmitz R, et al. Orbital atherectomy for treating de novo, severely calcified coronary lesions:3-year results of the pivotal ORBIT II trial. Cardiovasc Revasc Med. 2017;18:261-264.
29. Jurado-Román A, Gómez-Menchero A, Rivero-Santana B, et al. Rotational Atherectomy, Lithotripsy, or Laser for Calcified Coronary Stenosis:The ROLLER COASTR-EPIC22 Trial. JACC Cardiovasc Interv. 2025;18: 606-618.
30. Kirtane AJ, Généreux P, Lewis B, et al. Orbital atherectomy versus balloon angioplasty before drug-eluting stent implantation in severely calcified lesions eligible for both treatment strategies (ECLIPSE):a multicentre, open-label, randomised trial. Lancet. 2025;405:1240-1251.












