
To the Editor,
In-stent restenosis (ISR) remains a persistent challenge in contemporary interventional cardiology and is associated with worse clinical outcomes despite advances in percutaneous coronary intervention (PCI) techniques and newer drug-eluting stent (DES) platforms.1
Drug-coated balloons (DCB) provide a “leave-nothing-behind” strategy for the treatment of ISR, with the potential to preserve vascular vasomotor function and reduce the risk of late adverse events in complex lesions, including ISR; however data regarding DCB performance remain inconsistent.2,3 The clinical efficacy profile of DCB angioplasty is critically dependent on optimal lesion preparation.4 Specialty balloons, including cutting and scoring balloons, may facilitate more effective acute neointimal modification, enhance drug uptake and retention, and reduce residual stenosis and acute recoil.5 Nevertheless, real-world comparative data evaluating specialty balloon-based vs conventional balloon-based lesion preparation strategies (semi-compliant and non-compliant balloons) prior to DCB angioplasty in ISR remain limited.
The present study aimed to assess the impact of lesion preparation strategies on clinical outcomes in ISR treated with DCB angioplasty.
This lesion-level pooled analysis combined data from 4 prospective observational registries: EASTBOURNE,6 PEARL,7 RISE,8 and DRAGON.9 Lesions were categorized according to the predilation strategy: specialty balloons (cutting and scoring) vs conventional balloons (semi-compliant and non-compliant). The primary endpoint was major adverse cardiovascular events (MACE), defined as a composite of cardiac death, non-fatal myocardial infarction (MI), and target lesion revascularization (TLR). Unadjusted and adjusted hazard ratios (HR) with corresponding 95%CIs were estimated using Cox proportional hazards regression models. Multivariable adjustment was performed for baseline variables that differed significantly between groups (hypertension, previous MI, reference vessel diameter, and preoperative degree of stenosis). The study, conducted in full compliance with the principles outlined in the Declaration of Helsinki, was approved by the ethical committee of each participant centers. Written informed consent was obtained from all patients.
A total of 2128 ISR lesions were included in the pooled cohort, of which 125 (5.9%) were treated with specialty balloons and 2003 (94.1%) with a conventional preparation strategy. Baseline clinical characteristics of both cohorts are summarized in table 1. Patients treated with specialty balloons had lower rates of hypertension (79.2% vs 86.2%; P = .042) and previous myocardial infarction (45.6% vs 59.5%; P = .003), whereas no significant differences were observed for other variables. From an angiographic standpoint, lesions treated with specialty balloons were characterized by larger reference vessel diameters (3.1 ± 0.6 mm vs 3.0 ± 0.5 mm; P = .006) and greater baseline stenosis severity (85.2 ± 12.2% vs 81.1 ± 14.0%; P < .001). In the overall cohort, 85.3% of lesions were DES-ISR, a condition typically associated with more focal restenosis patterns and worse clinical outcomes compared with bare-metal stent (BMS)-ISR. The distribution of DES-ISR was similar between groups, with no significant difference between specialty balloon–based lesion preparation and conventional predilation (83.3% vs 85.5%; P = .873).
Table 1. Baseline clinical characteristics according to predilation strategy
| Variable | ISR population (N = 2128) | Specialty balloons group N = 125) | Conventional balloons group (N = 2003) | P |
|---|---|---|---|---|
| Male sex | 1606 (75.5) | 98 (78.4) | 1508 (75.3) | .498 |
| Hypertension | 1825 (85.8) | 99 (79.2) | 1726 (86.2) | .042 |
| DM | 943 (44.3) | 54 (43.2) | 889 (44.4) | .868 |
| Dyslipidemia | 1685 (79.2) | 94 (75.2) | 1591 (79.4) | .309 |
| Smoking history | 551 (25.9) | 42 (33.6) | 509 (25.4) | .055 |
| CKD | 392 (18.4) | 19 (15.2) | 373 (18.6) | .400 |
| Previous MI | 1248 (58.6) | 57 (45.6) | 1191 (59.5) | .003 |
| ACS | 1029 (48.4) | 64 (51.2) | 965 (48.2) | .573 |
| Age, years | 68.4 ± 10.0 | 69.3 ± 9.6 | 68.3 ± 10.0 | .286 |
| LVEF | 50.3 ± 10.6 | 49.5 ± 10.8 | 50.3 ± 10.6 | .540 |
| Lesion length, mm | 17.8 ± 7.2 | 18.2 ± 9.9 | 17.8 ± 7.0 | .611 |
| Reference vessel diameter, mm | 3.0 ± 0.5 | 3.1 ± 0.6 | 3.0 ± 0.5 | .006 |
| Degree of stenosis before PCI, % | 81.4 ± 13.9 | 85.2 ± 12.2 | 81.1 ± 14.0 | <.001 |
| Complex lesion | 1559 (73.3) | 98 (78.4) | 1461 (72.9) | .217 |
| Bifurcation lesion | 233 (10.9) | 11 (8.8) | 222 (11.1) | .519 |
| Moderate-severe calcification | 114 (5.4) | 8 (6.4) | 106 (5.3) | .742 |
| CTO | 79 (3.7) | 7 (5.6) | 72 (3.6) | .365 |
| ICI | 150 (8.4) | 5 (6.8) | 145 (8.4) | .770 |
| Predilation balloon diameter, mm | 3.0 ± 1.4 | 3.2 ± 1.3 | 3.0 ± 1.1 | .047 |
| DCB diameter, mm | 3.0 ± 0.7 | 3.2 ± 0.5 | 3.0 ± 0.7 | .006 |
| DCB length, mm | 21.3 ± 7.3 | 22.2 ± 8.4 | 21.3 ± 7.2 | .238 |
| SCB use | 1049 (49.3) | 62 (49.6) | 987 (49.3) | 1.000 |
| PCB use | 1079 (50.7) | 63 (50.4) | 1016 (50.7) | 1.000 |
| Bailout stenting | 86 (4.0) | 6 (4.8) | 80 (4.0) | .834 |
| TV angiographic dissection | 39 (1.8) | 5 (4.0) | 34 (1.7) | .129 |
| TV occlusion | 1 (0.0) | 0 (0.0) | 1 (0.0) | 1.000 |
| Degree of stenosis after PCI, % | 5.9 ± 9.7 | 3.3 ± 7.5 | 6.4 ± 10.0 | .015 |
|
ACS, acute coronary syndrome; CKD, chronic kidney disease; CTO, chronic total coronary occlusion; DCB, drug-coated balloon; DM, diabetes mellitus; ICI, intracoronary imaging; LVEF, left ventricular ejection fraction; MI, myocardial infarction; PCB, paclitaxel-coated balloon; PCI, percutaneous coronary intervention; SCB, sirolimus-coated balloon; SD, standard deviation; TV, target vessel. Data are expressed as No. (%) or mean ± standard deviation. |
||||
Procedurally, the specialty balloon group underwent preparation with larger predilation balloon diameters (3.2 ± 1.3 mm vs 3.0 ± 1.1 mm; P = .047) and was subsequently treated with larger DCB diameters (3.2 ± 0.5 mm vs 3.0 ± 0.7 mm; P = .006). Importantly, DCB angioplasty in this group resulted in significantly lower residual stenosis (3.3 ± 7.5% vs 6.4 ± 10.0%; P = .015).
At a mean follow-up of 734 ± 457 days, MACE occurred in 17.4% of lesions overall and was significantly lower in the specialty balloon group compared with the conventional strategy (8.0% vs 18.0%; P = .006). A consistent, although not statistically significant, reduction was observed across individual secondary endpoints, including all-cause mortality (1.6% vs 5.6%; P = .083), nonfatal MI (2.4% vs 7.0%; P = .069), and TLR (8.0% vs 13.7%; P = .094). Time-to-event analyses confirmed these findings, showing that the use of specialty balloons was associated with a significantly lower risk of MACE compared with conventional balloon angioplasty, both in unadjusted (HR, 0.44; 95%CI, 0.23–0.82; P = .010) and adjusted models (HR, 0.45; 95%CI, 0.24–0.84; P = .013). When stratified according to device type, cutting balloons (n = 101; 80.8%) and scoring balloons (n = 24; 19.2%) were associated with a similar risk of MACE (HR, 0.84; 95%CI, 0.15-5.32; P = .921). A graphical summary of these results is presented in figure 1.
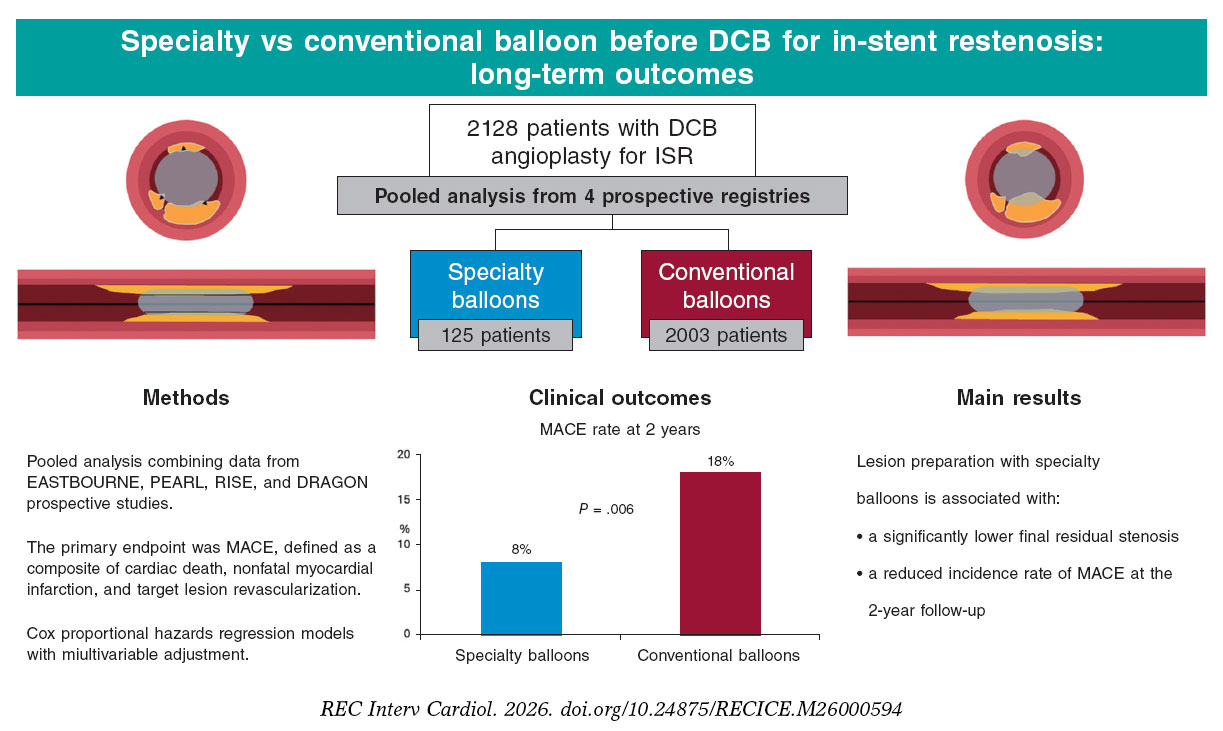
Figure 1. Specialty vs conventional balloon before drug coated balloon (DCB) treatment for in-stent restenosis: long term outcomes. DCB, drug-coated balloons; ISR, in-stent restenosis; MACE, major adverse cardiovascular events. The bibliographic references cited in this figure correspond to Cortese et al. (2023),6 Vlieger et al. (2022),7 Cortese et al. (2018),8 and Wańha et al. (2021).9
In this pooled analysis, specialty balloon–based lesion preparation prior to DCB angioplasty for ISR was associated with a significant reduction in MACE compared with conventional balloon angioplasty, even after adjustment using a Cox proportional hazard regression model. Evidence supporting the use of specialty balloons in this setting remains limited.10 In the ISAR-DESIRE 4 trial, Kufner et al. randomized 252 patients with clinically significant DES-ISR undergoing lesion preparation before DCB angioplasty to either a scoring or a standard balloon. Neointimal modification with the scoring balloon significantly improved angiographic outcomes, including lower in-segment diameter stenosis and reduced rates of binary restenosis 6 to 8 months. However, these angiographic benefits did not translate into significant differences in clinical endpoints at 1 year.11 Similarly, Linares-Vicente et al. reported a numerically lower rate of long-term TLR with cutting or scoring balloon–based lesion preparation prior to DEB angioplasty; however, this difference did not reach statistical significance.12
Our findings extend the existing evidence by providing a larger, real-world, multicenter analysis from prospective registries with long-term clinical follow-up. Notably, our data suggest that a more aggressive lesion preparation strategy may translate not only into improved acute procedural outcomes, reflected by lower residual stenosis, but also into a reduction in MACE at the 2-year follow-up. Collectively, these results underscore the pivotal role of lesion preparation in optimizing the efficacy profile of DCB-based treatment for ISR. The effectiveness of DCB angioplasty critically depends on achieving adequate luminal gain while ensuring efficient drug delivery in the absence of a permanent scaffold.4
The use of specialty balloons may play a crucial role in optimizing lesion preparation. By inducing controlled neointimal modification through scoring or microincisions, these devices enhance vessel expansion and mitigate acute elastic recoil. In this context, the lower residual stenosis observed in the specialty balloon group supports this mechanistic rationale. Beyond mechanical effects, controlled vessel injury may also enhance the biological efficacy of DCB therapy. Preclinical data suggest that targeted disruption of the neointima facilitates drug penetration and promotes a more homogeneous distribution within the vessel wall. In experimental models, the combination of cutting balloon and DCB therapy has been associated with deeper and more uniform medial smooth muscle cell depletion compared with standard predilation, supporting a mechanistic link between controlled plaque modification and enhanced drug uptake. This mechanistic framework may ultimately translate into improved clinical outcomes. In a recent study by Lee et al.13 evaluating OCT-guided DCB angioplasty for de novo coronary lesions, post-PCI dissections confined to the intima (eg, not involving the media) were associated with a significantly higher risk of target lesion failure compared with lesions exhibiting medial involvement (HR, 10.63; 95%CI, 3.77-29.9; P < .001), likely reflecting suboptimal antiproliferative drug uptake. Recently, the NATURE trial randomized a total of 201 patients in a 1:1 ratio to cutting vs standard balloons for lesion preparation before DCB therapy in de novo coronary lesions. Of note, DCB success was numerically higher with cutting balloons (79.2% vs 70.0%), with lower rates of bailout stenting.14
Nevertheless, several limitations of this study should be acknowledged. First, the observational design inherently exposes the analysis to residual confounding, despite statistical adjustment. Second, the relatively small number of lesions treated with specialty balloons in this dataset limits statistical power and precludes the performance of matched analyses. Third, operator selection bias cannot be excluded, although baseline angiographic complexity appeared comparable between groups. Moreover, studies differ substantially regarding included populations, devices used, type of follow-up performed, and follow-up duration. Finally, heterogeneity among DCB platforms reflects real-world practice but may have introduced additional variability.
In conclusion, in patients with ISR undergoing DCB angioplasty, lesion preparation with specialty balloons is associated with significantly lower residual stenosis and a reduced incidence rate of 2-year MACE compared with conventional strategies. These findings underscore the importance of optimal lesion preparation and support a potential role for specialty balloons in improving clinical outcomes. Dedicated randomized controlled trials are warranted to confirm these observations.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
The study, conducted in full compliance with the principles outlined in the Declaration of Helsinki, was approved by the ethical committee of each participant centers. Written informed consent was obtained from all patients.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence (AI) tools were used in the preparation, writing, analysis, or editing of this manuscript.
AUTHORS’ CONTRIBUTIONS
B. Khialani: conceptualization, draft review and editing, resources. F.L. Gurgoglione: original draft, draft review and editing, data interpretation, resources. J. Hasan: data interpretation, resources. W. Wan´ha: draft review and editing; resources. R.M. Oemrawsingh: resources. B. Cortese: conceptualization, supervision, draft review and editing, approval of the final draft.
CONFLICTS OF INTEREST
None declared.













