
Thirty years ago, in 1996, the concept of evidence-based medicine took hold; David Sackett, one of its leading advocates, defined it as the conscientious, explicit, and judicious use of the current best evidence for clinical decision-making. Since then, the properly designed randomized clinical trial has been the method par excellence for demonstrating the efficacy of medical interventions and generating robust evidence to inform the recommendations of scientific societies. However, over the past few decades, the scientific community has learned a great deal about the limitations of this methodology.
The results of the OPTIMAL trial have recently been published; the trial was designed to determine whether intravascular ultrasound (IVUS)-guided percutaneous revascularization of the unprotected left main coronary artery (LMCA) leads to better clinical outcomes than revascularization guided by conventional angiography alone.1 In this trial, a total of 806 patients with a mean age of 71 years and a mean SYNTAX score of 30 were randomized to one of the two interventions; 78% of them were women. After a median follow-up of 2.9 years, the primary endpoint occurred in 135 patients (33.7%) in the IVUS-guided group and in 125 patients (30.9%) in the angiography-guided group. The incidence of death, myocardial infarction, or revascularization was similar in both groups. The incidence of stroke was higher in the IVUS group, although these events occurred at a median of 19 months, which may suggest a chance finding. The authors concluded that, among patients with LMCA disease, IVUS-guided percutaneous revascularization showed no additional benefit compared with angiography- guided revascularization. This is not the first time that trial results have conflicted with initial expectations.
For many years, I have been an advocate and promoter of the use of IVUS to guide drug-eluting stent angioplasty procedures in the LMCA, based on a conviction derived from my own experience, but primarily on the results of numerous observational studies, including some that we conducted in our country.2,3 Therefore, being one of the principal investigators and the second author of the OPTIMAL trial manuscript places me in a unique position. On the one hand, I must accept the results of a trial that was executed flawlessly in every respect; on the other hand, I remain convinced that the use of IVUS can continue to add value in many cases of LMCA disease, especially when used appropriately. In the following paragraphs, I will attempt to explain and justify this position (figure 1).
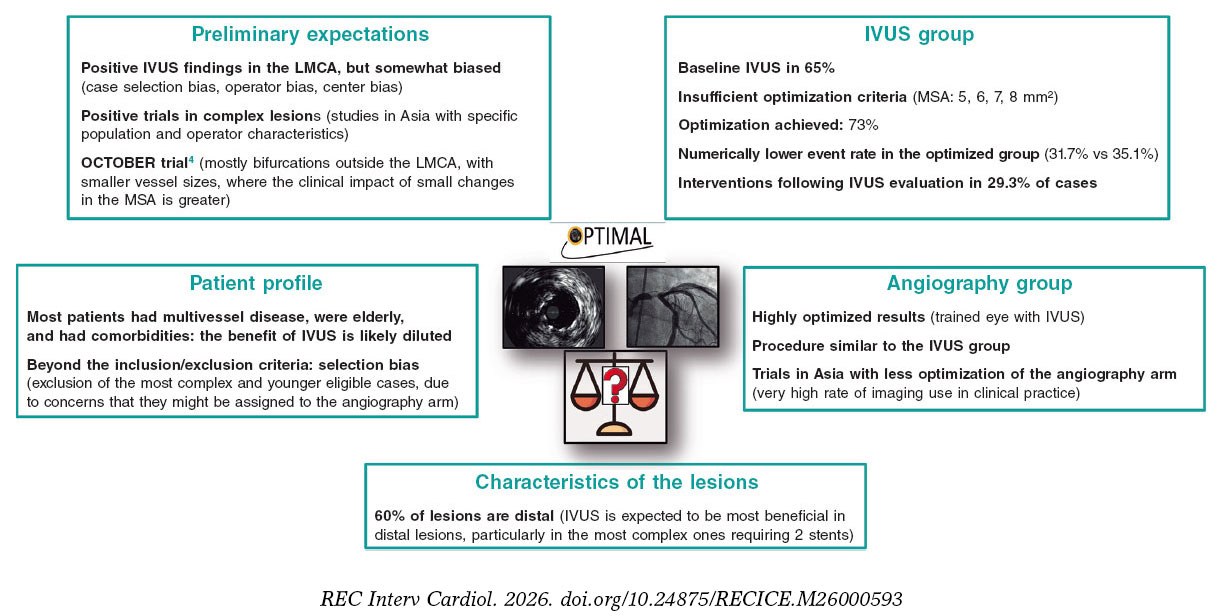
Figure 1. Various factors explaining the relative discrepancy between the expected results and those ultimately obtained in the OPTIMAL study. IVUS: intravascular ultrasound; LMCA: left main common artery; MSA: minimum stent area. The bibliographical references mentioned in this figure correspond to Testa et al.1 (OPTIMAL trial) and Holm et al.4 (OCTOBER trial).
EXPECTATIONS PRIOR TO THE OPTIMAL TRIAL
In recent years, several observational studies and corresponding meta-analyses have been published, all of which demonstrated that the use of IVUS in percutaneous revascularization of the LMCA was associated with a reduction in events, including cardiac death, myocardial infarction, and revascularization.5 However, it is evident that the benefits observed in registries are often exaggerated, and this is due to certain biases. First, selection bias. Comparing cases in which IVUS was used versus those in which it was not within a registry implies selection bias, since that decision was based on certain variables, which ultimately affected certain characteristics of the patients and the lesions. Even with statistical matching techniques, it is very difficult to completely eliminate the confounding effect of partially hidden biases.2 In this regard, the use of IVUS may have been more likely in patients in better clinical condition, who were more stable, and younger. This could explain the differences in overall mortality observed as early as the short- to medium-term between the IVUS and angiography groups in some registries.6
Another potential source of bias relates to the operator and the center. It is plausible that operators who used IVUS more frequently were also more meticulous in other technical and patient management aspects and were based at centers with higher patient volumes and greater experience. A large British registry found that the benefit of IVUS was greater when operators had higher case volumes, suggesting this bias.6
The positive results of some randomized trials, although not focused on the LMCA and conducted in Asian countries, also instilled considerable optimism.7-10
The OCTOBER trial, which compared optical coherence tomography-guided versus angiography-guided treatment of bifurcations, showed a lower incidence of the primary endpoint at 2 years (10.1% vs 14.1%).4 It should be noted that these were mostly bifurcations that did not involve the LMCA and involved smaller vessels, where a greater effect of small changes in the minimum stent area (MSA) on clinical outcomes is expected.
PATIENT PROFILE
In the OPTIMAL trial, the mean age of patients was 71 years, 5 years older than that of patients in the OCTOBER trial.1,4 Fifty-eight percent had three-vessel disease, with a mean SYNTAX score of 30. This explains the high incidence of events, exceeding 30% at 2.9 years.1
As is often the case in many trials, and especially when there are pre-existing biases, patient enrollment may have taken into account factors beyond the inclusion/exclusion criteria, leading to selection bias. Consequently, it is possible that some patients for whom IVUS was deemed necessary (such as those with more complex distal lesions or younger patients) were excluded.
CHARACTERISTICS OF LMCA LESIONS
In the OPTIMAL trial, 60% of the treated LMCA lesions involved the bifurcation. In a large Spanish multicenter registry, with two matched groups of 505 patients each, we found that the benefit associated with the use of IVUS in LMCA angioplasty with drug-eluting stents was greater in distal lesions and, particularly, in those requiring two stents.2 Therefore, the inclusion of a relatively high proportion of non-distal lesions may have reduced the overall impact of IVUS in the OPTIMAL study.
In the recently published IVUS-CHIP trial, which evaluated the use of IVUS in 2020 patients with complex lesions and demostrated no differences compared with angiography, a trend toward a benefit from IVUS was observed in distal LMCA lesions.11
THE IVUS GROUP
IVUS is not a therapeutic tool, it is an imaging technique, and the benefit it may provide depends on how the operator uses it. The resulting clinical advantage derived from its use will be solely due to the corrective measures prompted by the imaging findings, the optimization criteria pursued, and the extent to which those criteria are met. In the OPTIMAL trial, the use of IVUS prior to the procedure was 65%, whereas a higher rate of use would have been expected to better understand the characteristics of the plaques and plan plaque management.
Among the optimization criteria, those related to expansion are particularly relevant, specifically the MSA cutoff values that were considered mandatory to achieve in this trial.12 These values were 8 mm² for the LMCA, 7 mm² for the confluence polygon, 6 mm² for the left anterior descending artery, and 5 mm² for the left circumflex artery, which were acceptable at the time the trial was designed but have since been surpassed by more recent studies. Currently, the optimal MSA cutoff values are estimated at 10 mm² for the TCI, 7 mm² for the left anterior descending artery, and 6 mm² for the left circumflex artery.13-17 In fact, just as this editorial was being written, the European Association of Percutaneous Cardiovascular Interventions and the European Bifurcation Club published a consensus document on the use of imaging in LMCA angioplasty that incorporates these new target values.18
In the OPTIMAL study, the final MSA in the LMCA was 12.99 ± 4.09 mm², 7.79 ± 2.43 mm² in the left anterior descending artery, and 6.75 ± 1.92 mm² in the left circumflex artery, indicating that in 15% of cases the MSA in the LMCA was less than 9 mm², less than 5.3 mm² in the anterior descending artery, and less than 4.8 mm² in the circumflex artery.1
However, in addition to establishing criteria, it is advisable to attempt, within the bounds of what is feasible and safe, to achieve these objectives. In the OPTIMAL study, corrective actions were observed in 29.3% of cases, and optimization was confirmed in 73%, with a numerically lower event rate in the optimized group (31.7% vs. 35.1%).1 It should be noted that failure to achieve the targets cannot be attributed solely to lack of adherence but is often due to safety considerations. In this regard, it is noteworthy that there were no differences in periprocedural complications between the groups.
The consideration of appropriate criteria and their implementation under a standardized protocol provides a benefit compared to the non-protocolized use of IVUS.3
THE GROUP ASSIGNED TO ANGIOGRAPHY
Another striking aspect is the high degree of similarity between the groups regarding the technical aspects of the procedure, with a similar rate of post-dilatation and similar device sizes. This may suggest that the operator working solely with angiography acted based on the knowledge and experience of someone who has performed many IVUS-guided procedures, which could be considered an angiography- guided intervention but inspired by prior experience with IVUS.
In this regard, while we previously noted that Asian trials7-10 generally yielded more positive results than Western ones,1,11,19 it is worth noting that the angiography group in the former shows clear differences from the intravascular imaging group, with much lower use of post-dilatation and selection of stents with significantly smaller diameters. It is likely that the very high use of IVUS in Asian countries may influence this different approach when angiography is the only option available. Furthermore, it cannot be ruled out that these operators adhered more strictly to the protocol for optimization based on intravascular imaging.
FINAL COMMENTS AND RECOMMENDATIONS
Further subgroup analyses of the OPTIMAL trial are needed to address issues such as the effect of IVUS in cases of isolated LMCA disease, to explore outcomes based on different MSA values, and, above all, to identify anatomical or clinical subgroups that benefit most from IVUS-guided procedures.
The conclusions drawn from these reflections are as follows:
- –The routine use of IVUS to guide percutaneous revascularization in all cases of LMCA lesions is not clinically justified when operators have sufficient experience in performing the procedure.
- – It is necessary to identify which LMCA lesion profiles benefit most from the use of intravascular imaging techniques (most likely distal lesions).
- – Appropriate optimization criteria should be established.
- – Efforts should be made to achieve these objectives within safety margins.
- – The implementation of automated intravascular image assessment systems (based on artificial intelligence) can be of great help in this regard.
- – It is essential to continue promoting training and the use of intravascular imaging techniques among less experienced professionals.
Finally, in my opinion, it would be advisable to conduct a new randomized trial that includes patients with distal LMCA lesions without a high SYNTAX score and uses the most up-to-date optimization criteria.
Karl Popper
FUNDING
No funding was received for the preparation of this manuscript.
CONFLICTS OF INTEREST
J.M. de la Torre-Hernández is the editor-in-chief of
REFERENCES
1. Testa L, De la Torre Hernandez JM, De Maria GL, et al.;OPTIMAL Investigators. IVUS-Guided versus Angiography-Guided PCI in Unprotected Left Main Coronary Disease. N Engl J Med. 2026. https://doi.org/ 10.1056/NEJMoa2600440.
2. De la Torre Hernandez JM, Baz Alonso JA, Gómez Hospital JA, et al.;IVUS-TRONCO-ICP Spanish study. Clinical impact of intravascular ultrasound guidance in drug-eluting stent implantation for unprotected left main coronary disease:pooled analysis at the patient-level of 4 registries. JACC Cardiovasc Interv. 2014;7:244-254.
3. de la Torre Hernandez JM, Garcia Camarero T, Baz Alonso JA, et al. Outcomes of predefined optimisation criteria for intravascular ultrasound guidance of left main stenting. EuroIntervention. 2020;16:210-217.
4. Holm NR, Andreasen LD, Neghabat O, et al.;OCTOBER Trial Group. OCT or Angiography Guidance for PCI in Complex Bifurcation Lesions. N Engl J Med. 2023;389:1477-1487.
5. Karim K, Akbar MR, Pramudyo M, Martha JW. Intravascular Ultrasound versus Angiography Guided Drug Eluting Stent Implantation in Patients with Left Main Coronary Artery Disease —A Systematic Review and Meta-Analysis. Rev Cardiovasc Med. 2024;25:32.
6. Kinnaird T, Johnson T, Anderson R, et al. Intravascular Imaging and 12-Month Mortality After Unprotected Left Main Stem PCI:An Analysis From the British Cardiovascular Intervention Society Database. JACC Cardiovasc Interv. 2020;13:346-357.
7. Kim BK, Shin DH, Hong MK, et al. Clinical Impact of Intravascular Ultrasound-Guided Chronic Total Occlusion Intervention With Zotarolimus-Eluting Versus Biolimus-Eluting Stent Implantation:Randomized Study. Circ Cardiovasc Interv. 2015;8:e002592.
8. Hong SJ, Kim BK, Shin DH, et al. Effect of Intravascular Ultrasound-Guided vs Angiography-Guided Everolimus-Eluting Stent Implantation:The IVUS-XPL Randomized Clinical Trial. JAMA. 2015;314:2155-2163.
9. Gao XF, Ge Z, Kong XQ, et al.;ULTIMATE Investigators. 3-Year Outcomes of the ULTIMATE Trial Comparing Intravascular Ultrasound Versus Angiography-Guided Drug-Eluting Stent Implantation. JACC Cardiovasc Interv. 2021;14:247-257.
10. Lee JM, Kim O, Song YB, et al. RENOVATE COMPLEX-PCI Investigators. Intravascular Imaging- vs Angiography-Guided Complex PCI:5-Year Outcomes From a Randomized Trial. J Am Coll Cardiol. 2026;87:2099-2113.
11. Diletti R, Daemen J, Faurie B, et al.;for the IVUS-CHIP Investigators. Intravascular Ultrasound-Guided or Angiography-Guided Complex High-Risk PCI. N Engl J Med. 2026. https://doi.org/10.1056/NEJMoa2601521.
12. De Maria GL, Testa L, de la Torre Hernandez JM, et al. A multi-center, international, randomized, 2-year, parallel-group study to assess the superiority of IVUS-guided PCI versus qualitative angio-guided PCI in unprotected left main coronary artery (ULMCA) disease:Study protocol for OPTIMAL trial. PLoS One. 2022;17:e0260770.
13. Kang SJ, Ahn JM, Song H, et al. Comprehensive intravascular ultrasound assessment of stent area and its impact on restenosis and adverse cardiac events in 403 patients with unprotected left main disease. Circ Cardiovasc Interv. 2011;4:562-569.
14. Maehara A, Mintz G, Serruys P, et al. Impact of final minimal stent area by IVUS on 3-year outcome after PCI of left main coronary artery disease:the EXCEL trial. J Am Coll Cardiol. 2017;69:S963.
15. Kim JH, Kang DY, Ahn JM, et al. Optimal Minimal Stent Area and Impact of Stent Underexpansion in Left Main Up-Front 2-Stent Strategy. Circ Cardiovasc Interv. 2024;17:e013006.
16. Kim JH, Kang DY, Ahn JM, et al. Optimal minimal stent area after crossover stenting in patients with unprotected left main coronary artery disease. EuroIntervention. 2025;21:1069-1080.
17. De la Torre Hernandez JM. Evolving cutoff values for optimising left main stenting with intravascular imaging. EuroIntervention. 2025;21:e1043-e1044.
18. Johnson TW, Gonzalo N, De la Torre Hernandez JM, et al. Intracoronary imaging for left main percutaneous coronary intervention:a clinical consensus statement of the European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the ESC and the European Bifurcation Club (EBC). Eur Heart J. 2026. https://doi.org/10.1093/eurheartj/ehag353.
19. Ali ZA, Landmesser U, Maehara A, et al.;ILUMIEN IV Investigators. Optical Coherence Tomography-Guided versus Angiography-Guided PCI. N Engl J Med. 2023;389:1466-1476.












