
To the Editor,
The complex and highly variable 3D anatomy of the left atrial appendage (LAA) makes it challenging for planning and device sizing for left atrial appendage closure (LAAC).1 Echocardiography and multi-slice computed tomography (CT) are widely used imaging modalities for this purpose. 3Mensio Structural Heart (Pie Medical Imaging BV, The Netherlands) is the most widely used software for CT evaluation of LAA providing automatic segmentation of the heart. TribusConnect (TribusMed Beheer BV, The Netherlands) is a novel cloud-based Digital Imaging and Communications in Medicine (DICOM) viewer that can also be used to securely access, review, interpret, manipulate, measure and visualize images with automatic cardiac segmentation for LAA evaluation. Furthermore, TribusConnect allows for manual correction or adjustment of the automatically generated measurements or segmentation which could be crucial for centers with varying image quality, or challenging anatomies. This study aimed to investigate the feasibility, accuracy and reproducibility of evaluating the LAA in TribusConnect compared with the 3Mensio for preprocedural planning of LAAC.
Seventeen patients who underwent LAAC at Hospital Clínico Universitario de Valladolid (Valladolid, Spain) were included in our study. A total of 52.9% (9 patients) of these patients underwent LAAC by Amplatzer Amulet (Abbott, United States) while 17.6% (3 patients) and 29.4% (5 patients) received the Watchman (Boston Scientific, United States) and Omega (Vascular Innovations, Thailand) left atrial appendage occlude devices, respectively. The device size used varied from 18 mm to 35 mm. Only 1 of the 17 patients had mild peridevice leak (< 3 mm) due to device malapposition while 0 patients had device embolization or need for changing the device size or device type during the procedure. All patients underwent preoperative contrast-enhanced, electrocardiogram-gated high-pitch spiral acquisition mode CT. Images were obtained at 30%-60% of the R-R interval with a delayed scan after contrast injection in full compliance with LAA-specific expert recommendations on CT acquisition.2 All datasets were saved as DICOM files and processed with dedicated software (3mensio Structural Heart) and novel TribusConnect. In the presence of inadequate delineation of the endocardial border due to incomplete contrast opacification of the LAA, the images were considered insufficient and excluded from the study. All datasets were evaluated, and measurements were performed by 2 independent cardiologists. Conventional measurements of LAA sizes (ostium, landing zone, depth, and working depth) were compared. The landing zone (LZ) was defined at a location 10 mm from the ostium into the LAA after adjusting the angle. The working depth was measured as a perpendicular line drawn from ostium to the LAA roof.
The intraclass correlation coefficients (ICC) between TribusConnect and 3Mensio for minimum, maximum, and mean diameters were, respectively, 0.912 (95%CI, 0.780-0.967), 0.826 (95%CI, 0.592-0.933), and 0.944 (95%CI, 0.852-0.979) at the ostium, and 0.667 (95%CI, 0.058-0.887), 0.806 (95%CI, 0.548-0.925), and 0.835 (95%CI, 0.371-0.948) at the LZ. This showed a good intraclass correlation. The Bland Altman plot for the measurements of ostium and LZ using the 2 software applications is shown in figure 1. ICC were 0.666 (95%CI, 0.286-0.865) for LAA depth and 0.753 (95%CI, 0.451-0.902) for working depth.
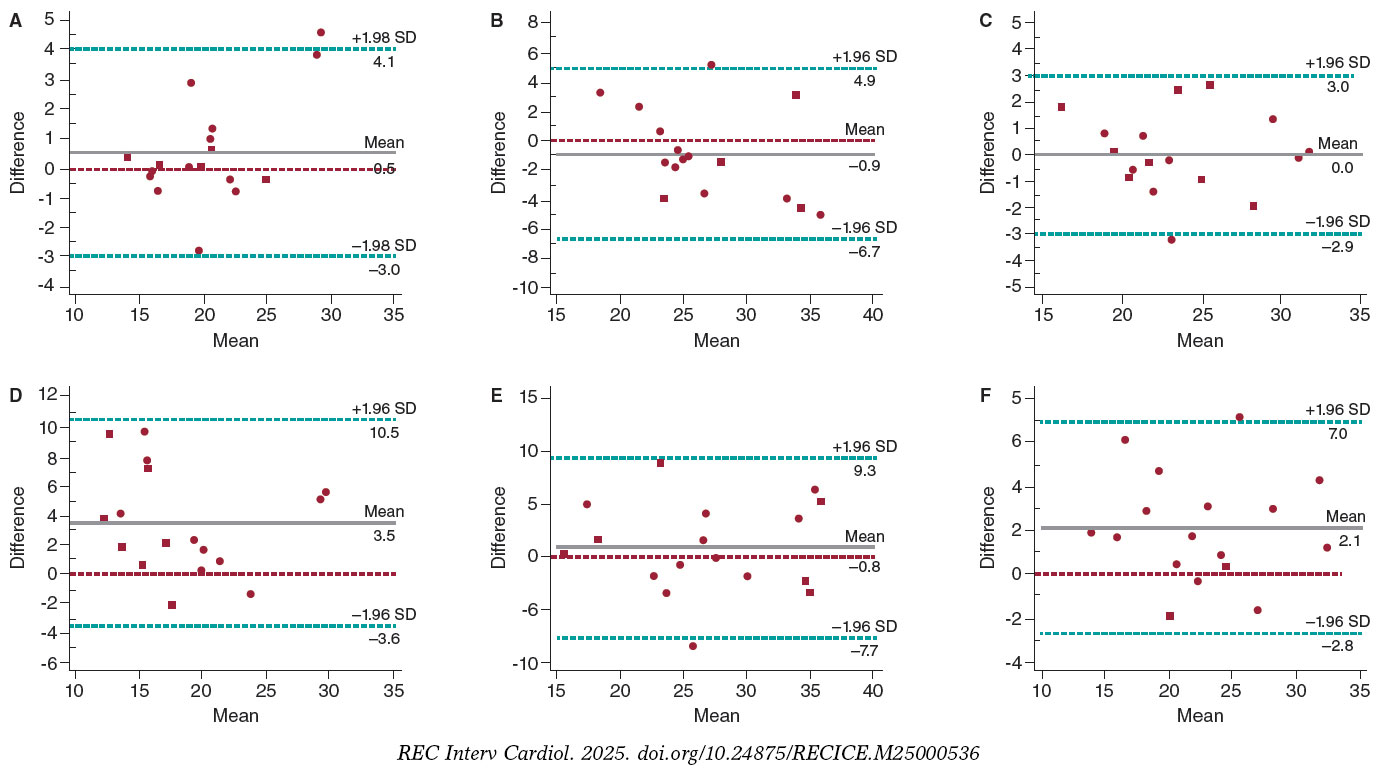
Figure 1. Bland Altman Plot showing the difference in measurement of minimum, maximum and mean diameter at ostium (A,B,C) and landing zone (D,E,F) between TribusConnect and 3Mensio. SD, standard deviation.
The ICC for the interobserver analysis for TribusConnect at the ostium (minimum, maximum, mean diameters) was 0.941 (0.846-0.978), 0.978 (0.941-0.992) and 0.973 (0.928-0.990) vs 0.901 (0.753-0.963), 0.815 (0.526-0.931) and 0.861 (0.662-0.947) for 3Mensio. Similarly, at the LZ, the ICC for TribusConnect (minimum, maximum, mean diameters) was 0.887 (0.719-0.957), 0.873 (0.689-0.952) and 0.941 (0.849-0.978) vs 0.736 (0.404-0.896), 0.718 (0.390-0.887) and 0.831 (0.602-0.935) for 3Mensio reflecting a better reproducibility of results across different operators with TribusConnect.
ICC for depth and working depth measurements was high for both systems. For TribusConnect, ICCs were 0.813 (95%CI, 0.445-0.935) for depth and 0.828 (95%CI, 0.467-0.941) for working depth. For 3Mensio, ICCs were 0.761 (95%CI, 0.348-0.914) for depth and 0.845 (95%CI, 0.629-0.941) for working depth.
TribusConnect was deemed by the operators to have better accessibility (video 1 of the supplementary data). Since it is a cloud-based software with no need for any licensing or software installation into a device, CT images can be retrieved from any device and location across the globe. Secondly, TribusConnect has a workflow agnostic approach, bringing the user directly into the LAA without the need for restrictive steps in a workflow. Thirdly, TribusConnect ensures better data safety as no patient data is downloaded and the CT is anonymised by the software. Fourthly, all results are automatically saved, and the analysed results can be shared wherein multiple users can view, edit or improve the analysis. This was a retrospective study with a small number of patients with potential influence of unknown confounders. Further progressive studies might be needed to assess the impact of usability of this novel software on LAA device sizing and eventually clinical outcomes.
The study demonstrates a strong ICC between TribusConnect and 3Mensio in the CT assessment of the LAA for LAAC. TribusConnect exhibited lower interobserver variability and provided the added benefit of remote access to patient data.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
This study did not involve patient participants or animals, which is why ethical clearance was deemed unnecessary. Although this study included male and female patients alike, sex disaggregated analyses were not performed due to lack of expected sex related differences.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence tools were used in the writing of this study.
AUTHORS’ CONTRIBUTIONS
A. Jain and I.J. Amat-Santos conducted the study and wrote the draft. The remaining authors helped to collect the data. All authors approved the final version.
CONFLICTS OF INTEREST
L. Verstraaeten and J. Vogelaar are shareholders and employees of TribusMed. The remaining authors declared no conflicts of interest whatsoever.
SUPPLEMENTARY DATA
Vídeo 1. Jain A. DOI: 10.24875/RECICE.M25000536
REFERENCES
1. Heidari H, Kanschik D, Erkens R, et al. Left atrial appendage sizing for percutaneous closure in virtual reality-a feasibility study. Front Cardiovasc Med. 2023;10:1188571.
2. Korsholm K, Berti S, Iriart X, et al. Expert Recommendations on Cardiac Computed Tomography for Planning Transcatheter Left Atrial Appendage Occlusion. JACC Cardiovasc Interv. 2020;13:277-292.












