
ABSTRACT
Introduction and objectives: Resuscitated cardiac arrest before primary angioplasty (RCABPA) in ST-segment elevation myocardial infarction (STEMI) is associated with a worse prognosis. Mortality according to the place of occurrence has not been previously analyzed. Assessment of potential differences depending on where RCABPA occurs may lead to improvements in care and, consequently, reductions in STEMI-related mortality.
Methods: Observational study of a cohort of patients included in a regional infarction code program between 1 January 2021, and 31 December 2024. Thirty-day mortality and its determinants were compared according to the location of RCABPA occurrence: out-of-hospital, primary care, medicalized ambulance, or hospital.
Results: A total of 2344 patients with STEMI were included, 170 (7.3%) with RCABPA, 40 (1.7%) in the hospital setting, 13 (0.6%) in primary care, 33 (1.4%) in a medicalized ambulance, and 84 (3.6%) outside the health care setting. The initial rhythm was shockable in 158 cases (92.9%). Mortality among patients with pulseless electrical activity (PEA) was 31.2% vs 6.3% in those without PEA (P < .0005). An increase in both unadjusted and adjusted 30-day mortality was observed across groups: non-RCABPA, 6.3%; hospital, 7.5%; primary care, 15.4%; ambulance, 21.2%; and out-of-health care setting, 48.8%; it was only statistically significant when it occurred outside the hospital, both compared with non-RCABPA and in-hospital RCABPA.
Conclusions: RCABPA in STEMI is associated with significantly higher mortality. Prognosis varies according to the location of occurrence. Improvements in cardiopulmonary resuscitation conditions in the out-of-hospital setting may reduce mortality in these patients.
Keywords: Myocardial infarction. Prognosis. Primary angioplasty. Infarction code program.
RESUMEN
Introducción y objetivos: La parada cardiaca recuperada antes de la angioplastia primaria (PCRAAP) empeora notablemente el pronóstico del infarto agudo de miocardio con elevación del segmento ST (IAMCEST). Sin embargo, el efecto del lugar de ocurrencia de la PCRAAP sobre el pronóstico no se ha analizado. El conocimiento de posibles diferencias podría contribuir a mejoras asistenciales que redujeran la mortalidad del IAMCEST.
Métodos: Estudio observacional de una cohorte de pacientes incluidos en un programa regional de código infarto entre el 1 de enero de 2021 y el 31 de diciembre de 2024. Se compararon la mortalidad a 30 días y sus condicionantes según el lugar de ocurrencia de la PCRAAP: en un entorno no sanitario, en atención primaria, en una ambulancia medicalizada o en un hospital.
Resultados: Se incluyeron 2.344 pacientes con IAMCEST. Presentaron PCRAAP 170 (7,3%), 40 (1,7%) en un medio hospitalario, 13 (0,6%) en atención primaria, 33 (1,4%) en una ambulancia medicalizada y 84 (3,6%) fuera del medio sanitario. El ritmo inicial fue desfibrilable en 158 casos (92,9%). La mortalidad de los pacientes con PCRAAP fue del 31,2%, frente al 6,3% en aquellos sin PCRAAP (p < 0,0005). Se observó una mortalidad bruta y ajustada a 30 días creciente: no PCRAAP 6,3%, hospitalaria 7,5%, atención primaria 15,4%, ambulancia 21,2% y extrasanitaria 48,8%; solo fue estadísticamente significativa cuando ocurrió fuera del hospital, tanto en relación con la no PCRAAP como con la PCRAAP hospitalaria.
Conclusiones: La PCRAAP en el IAMCEST se asocia a una significativa mayor mortalidad. Su pronóstico depende del lugar donde ocurre. Mejoras en la atención a la PCRAAP extrahospitalaria, tanto sanitaria-extrahospitalaria como extrasanitaria, podrían reducir la mortalidad del IAMCEST.
Palabras clave: Infarto de miocardio. Pronóstico. Angioplastia primaria. Código infarto.
Abbreviations
CPR: cardiopulmonary resuscitation. PCI: percutaneous coronary intervention. RCABPA: resuscitated cardiac arrest before primary angioplasty. STEMI: ST-segment elevation myocardial infarction.
INTRODUCTION
Acute coronary syndrome, particularly ST-segment elevation myocardial infarction (STEMI), is the leading cause of out-of-hospital cardiac arrest.1 The main underlying mechanism is reversible ischemia, provided that reperfusion is achieved within the first few hours after STEMI.2 Approximately 1 in 20 patients with STEMI presents with cardiac arrest as the initial or early sign of myocardial infarction.3-5 Resuscitated cardiac arrest before primary angioplasty (RCABPA) is an important prognostic marker, and has been associated with 30-day mortality rates of 40% to 60%.3,6 Published studies differ regarding the long-term prognosis of patients who survive the in-hospital phase after RCABPA. Some registries have reported no long-term differences in outcomes,7,8 whereas others have found higher mortality, even after adjustment for the poorer baseline clinical profile of patients with RCABPA.9,10 However, all available studies consistently show that most events occur during the in-hospital phase or within the first 30 days after RCABPA.
“STEMI network” programs are designed to ensure rapid identification of STEMI and timely delivery of the most appropriate reperfusion strategy, preferably primary angioplasty.5 Studies evaluating the characteristics and prognosis of RCABPA have generally paid little attention to the specific point in the STEMI care pathway at which cardiac arrest occurs. Their inclusion criteria have typically included patients with RCABPA occurring outside the hospital setting, without specifying whether the cardiac arrest occurred before or after first medical contact or how close the patient was to resources for advanced cardiopulmonary resuscitation (CPR). In addition, the prognosis of RCABPA occurring in hospitals with CPR capability but without primary angioplasty capability has not been specifically analyzed. The poor short-term prognosis associated with RCABPA may be related to the clinical characteristics and consequences of the STEMI per se or to delays and limitations in CPR when cardiac arrest occurs outside the hospital setting.
Therefore, analyzing the characteristics and consequences of RCABPA based on the place of occurrence may help identify opportunities to improve the care and prognosis of patients with STEMI.
The aim of this study was to analyze short-term mortality in patients with RCABPA, with particular attention to the place where cardiac arrest occurred within the care pathway initiated by activation of the STEMI code after diagnosis.
METHODS
Design
This observational study used a historical cohort of consecutive patients admitted for primary angioplasty with a diagnosis of STEMI and an indication for reperfusion.
Study population
We included all patients who arrived at the cath lab of Hospital Clínico Universitario Virgen de la Arrixaca (El Palmar, Murcia, Spain) between 1 January, 2021, and 31 December, 2024 through the regional STEMI code program and with an indication for primary angioplasty. In patients with > 1 episode during the inclusion period, only the index episode was included. In 2023, the reference population covered by the regional STEMI code program for the study center was 1,132,310 inhabitants. Six non–PCI-capable hospitals referred patients to the study hospital, which served as the reference center. According to the STEMI code protocol, activation must occur at first medical contact, and patients should be transferred directly from the place of activation to the cath lab, without intermediate stops at other hospitals or emergency departments.
Variables
Data were obtained from the prospective patient registry of the cath lab at the reference hospital for primary angioplasty, where demographic characteristics, clinical presentation, procedural data, and follow-up information are systematically recorded. Missing data were completed by reviewing the regional electronic health record or by contacting patients or their relatives by telephone.
RCABPA was defined as cardiac arrest with return of spontaneous circulation after cardiopulmonary resuscitation maneuvers. Cardiac arrests occurring after arrival at the cath lab were excluded. Patients who died before or during transfer to the reference hospital were not included.
Patients were classified into 5 groups according to the location where RCABPA occurred: a) in-hospital RCABPA, occurring in referral hospitals before transfer or at the reference hospital prior to the arrival at the cath lab; b) RCABPA in a medicalized ambulance occurring in an ambulance with defibrillation capability; c) RCABPA in primary care, occurring in a health center or out-of-hospital emergency department with defibrillation capability; d) RCABPA outside the health care setting, occurring at home or in a public place without medical or paramedical personnel present; and e) no RCABPA, used as the control group.
All primary care centers and medicalized ambulances have the capacity to provide advanced CPR. We could not determine the exact number of patients with out-of-hospital RCABPA who may have exceptionally benefited from the proximity of a defibrillation team.
For comparisons by grouped location, groups a, b, and c were classified as RCABPA occurring in a health care setting, whereas groups b and c were classified as RCABPA occurring in an out-of-hospital health care setting.
Vital status at 30 days was obtained from the patients’ electronic health records or, when unavailable, by telephone contact.
The study was conducted in full compliance with the principles outlined in the Declaration of Helsinki. Episodes were collected retrospectively. The study was approved by the local ethics committee.
Statistical analysis
Quantitative variables are expressed as mean and standard deviation or as median and 25th-75th percentiles when they did not meet normality criteria, as assessed with the Shapiro-Wilk test. Quantitative variables that did not meet the normality criteria were compared using the nonparametric Mann-Whitney U test; normally distributed variables were compared using the Student t test for independent samples. Qualitative variables are expressed as absolute frequencies and percentages and were compared using the Pearson chi-square test. As specified in the tables and Results section, patients without RCABPA and those with in-hospital RCABPA were used as reference groups, as appropriate. Thirty-day mortality was assessed using Kaplan-Meier survival analysis. Survival curves were plotted for patients without RCABPA and for those with RCABPA at each individual and grouped location. Survival curves were compared using the log-rank test, with patients without RCABPA and those with in-hospital RCABPA used as reference groups. In all cases, P values < .05 were considered statistically significant.
To determine the contribution of RCABPA to 30-day mortality compared with the absence of RCABPA, as well as the contribution of RCABPA according to its location, logistic regression models were constructed. Models were adjusted for variables that were asymmetrically distributed across the study subgroups in the univariate analysis (P > .1) or that have been associated in the literature with higher mortality: age, diabetes, cardiogenic shock, performance of percutaneous coronary intervention (PCI), anterior infarct location, and delay from symptom onset to first medical contact. The absence of significant multicollinearity among the included variables was confirmed. The predictive performance of each model was assessed using the receiver operating characteristic curve, based on 30-day mortality predicted by the models and observed mortality.
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., United States), and SigmaPlot for Windows, version 11.0 (Systat Software, Inc., United States).
RESULTS
Population description
During the 4-year study period, there were 2463 activations of the STEMI code program with an indication for primary angioplasty. A total of 119 cases (4.9%) were excluded because they had previously been referred for primary angioplasty, leaving a final sample of 2344 patients, 170 of whom (7.3%) experienced RCABPA: 40 (1.7%) in a hospital setting, 13 (0.6%) in primary care, 33 (1.4%) in an advanced life support ambulance, and 84 (3.6%) outside the health care setting. Eight aborted STEMI code activation due to patient death before arrival at the cath lab were recorded, including 3 deaths in an advanced life support ambulance. The final cause of death could not be determined. All these patients had cardiogenic shock at the time of activation and were not included in the study.
The initial rhythm of RCABPA was shockable in 158 cases (92.9%). Baseline characteristics and infarct presentation based on the presence of RCABPA are shown in table 1. Patients with RCABPA underwent PCI less frequently than those without RCABPA (76.5% vs 85.6%; P = .001). PCI was not performed in 2 cases of RCABPA because the patients died before the procedure could be initiated, or in 28 cases because no culprit coronary lesion was identified.
Table 1. Baseline, acute myocardial infarction presentation, and procedural characteristics according to the occurrence or absence of resuscitated cardiac arrest before primary angioplasty
| Variable | No RCABPA (n = 2174) | RCABPA (n = 170) | P |
|---|---|---|---|
| Age, yearsa | 63 (54-74) | 60 (52-69) | .025 |
| Women | 521 (24.0%) | 28 (16.5%) | .026 |
| Age > 80 years | 273 (12.6%) | 17 (10.0%) | .329 |
| Age < 50 years | 320 (14.7%) | 33 (19.4%) | .099 |
| Diabetes | 686 (31.6%) | 41 (24.1%) | .043 |
| Hypertension | 1230 (56.6%) | 92 (54.1%) | .533 |
| Dyslipidemia | 1094 (50.3%) | 66 (38.8%) | .004 |
| Smoking | 1196 (55.0%) | 84 (49.4%) | .158 |
| Previous AMI | 158 (7.3%) | 8 (4.7%) | .210 |
| Previous PCI | 206 (9.5%) | 11 (6.5%) | .193 |
| Shockable rhythm | – | 158 (92.9%) | – |
| PCI performed | 1862 (85.6%) | 130 (76.5%) | .001 |
| Shock | 135 (6.2%) | 47 (27.6%) | < .001 |
| Anterior location | 843 (38.8%) | 78 (45.9%) | .068 |
| Outside working hours | 1685 (77.5%) | 136 (80.0%) | .452 |
| Undetermined location | 82 (3.8%) | 31 (18.2%) | < .001 |
| Symptom-to-FMC time, mina | 60 (30-155) | 20 (10-40) | < .001 |
| FMC-to-reperfusion time, mina | 116 (85-171) | 129 (91-160) | .428 |
| Symptom-to-reperfusion time, mina | 205 (137-355) | 150 (122-210) | < .001 |
|
AMI, acute myocardial infarction; FMC, first medical contact; PCI, percutaneous coronary intervention; RCABPA, resuscitated cardiac arrest before primary angioplasty; SD, standard deviation. a Median (25th-75th percentiles). |
|||
Baseline characteristics and infarct presentation based the presence and location of RCABPA are shown in table 2.
Table 2. Baseline, acute myocardial infarction presentation, and procedural characteristics based on the location of resuscitated cardiac arrest before primary angioplasty
| Variable | No RCABPA (n = 2174) | RCABPA (n = 170) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| In-hospital (n = 40) | Pa | Primary care (n = 13) | Pa | Pb | Advanced life support ambulance (n = 33) | Pa | Pb | Outside the health care setting (n = 84) | Pa | Pb | ||
| Age, yearsc | 63 (54-74) | 60 (52-72) | .397 | 54 (47-80) | .329 | .656 | 59 (54-69) | .436 | .987 | 61 (52-69) | .071 | .761 |
| Women | 521 (24.0%) | 6 (15.0%) | .187 | 4 (30.9%) | .567 | .207 | 4 (12.1%) | .113 | .722 | 14 (16.7%) | .123 | .814 |
| Age > 80 years | 273 (12.6%) | 4 (10.0%) | .628 | 4 (30.8%) | .049 | .069 | 4 (12.1%) | .940 | .773 | 5 (6.0%) | .071 | .417 |
| Age < 50 years | 320 (14.7%) | 7 (17.5%) | .623 | 5 (38.5%) | .016 | .117 | 4 (12.1%) | .676 | .523 | 17 (20.2%) | .164 | .718 |
| Diabetes | 686 (31.6%) | 13 (32.5%) | .899 | 4 (30.8%) | .952 | .908 | 4 (12.1%) | .017 | .040 | 20 (23.8%) | .133 | .306 |
| Hypertension | 1230 (56.6%) | 29 (72.5%) | .044 | 10 (76.9%) | .140 | .753 | 13 (39.4%) | .048 | .004 | 40 (47.6%) | .104 | .009 |
| Dyslipidemia | 1094 (50.3%) | 18 (45.0%) | .505 | 7 (53.8%) | .800 | .579 | 9 (27.3%) | .009 | .118 | 32 (38.1%) | .028 | .464 |
| Smoking | 1196 (55.0%) | 21 (52.5%) | .752 | 7 (53.8%) | .933 | .933 | 24 (72.7%) | .042 | .077 | 32 (38.1%) | .002 | .130 |
| Previous AMI | 158 (7.3%) | 1 (2.5%) | .247 | 0 (0.0%) | .313 | .565 | 2 (6.1%) | .791 | .445 | 5 (6.0%) | .648 | .402 |
| Previous PCI | 206 (9.5%) | 3 (7.5%) | .672 | 0 (0.0%) | .244 | .309 | 2 (6.1%) | .505 | .909 | 6 (7.1%) | .472 | .943 |
| Shockable rhythm | – | 38 (95.0%) | – | 13 (100%) | – | .411 | 31 (93.9%) | – | .352 | 76 (90.5%) | – | .387 |
| PCI performed | 1862 (85.6%) | 28 (70.0%) | .005 | 12 (92.3%) | .494 | .104 | 33 (100%) | .019 | .173 | 57 (67.9%) | < .001 | .810 |
| Shock | 135 (6.2%) | 12 (30.0%) | < .001 | 1 (7.7%) | .825 | .104 | 15 (45.5%) | < .001 | .168 | 19 (22.6%) | < .001 | .375 |
| Anterior location | 843 (38.8%) | 21 (52.5%) | .078 | 10(76.9%) | .005 | .121 | 12 (36.4%) | .778 | .158 | 35 (41.7%) | .594 | .257 |
| Outside working hours | 1685 (77.5%) | 28 (70.0%) | .261 | 10 (76.9%) | .960 | .398 | 25 (75.8%) | .811 | .583 | 73 (86.9%) | .042 | .024 |
| Undetermined location | 82 (3.8%) | 5 (12.5%) | .005 | 2 (15.4%) | .030 | .709 | 2 (6.1%) | .495 | .001 | 22 (26.2%) | < .001 | .084 |
| Symptom-to-FMC time, minc | 60 (30-155) | 13 (0.5-35) | < .001 | 27 (16-55) | .028 | .064 | 30 (21-60) | .003 | .005 | 30 (20-69) | < .001 | .029 |
| FMC-to-reperfusion time, minc | 116 (85-171) | 126 (100-174) | .404 | 116 (95-157) | .993 | .486 | 91 (79-128) | .028 | .030 | 135 (105-164) | .049 | .672 |
| Symptom-to-reperfusion time, minc | 205 (137-355) | 150 (120-225) | .005 | 155 (108-235) | .038 | .857 | 146 (106-206) | < .001 | .387 | 155 (133-208) | < .001 | .469 |
|
AMI, acute myocardial infarction; FMC, first medical contact; PCI, percutaneous coronary intervention; RCABPA, resuscitated cardiac arrest before primary angioplasty. a Comparison with no RCABPA. b Comparison with in-hospital RCABPA. c Median (25th-75th percentiles). |
||||||||||||
A total of 32 patients received mechanical circulatory support, representing 1.4% of the overall population and 17.6% of patients with cardiogenic shock. In this group, the 30-day mortality rate was 47%. Mechanical circulatory support was used in 10 patients with cardiogenic shock and RCABPA (21.2%; 30-day mortality, 70%) and in 22 patients with cardiogenic shock without RCABPA (16.3%; 30-day mortality, 36.4%).
Mortality based on the location of RCABPA
The 30-day all-cause and cardiovascular mortality rates are shown in table 3, and mortality grouped by RCABPA location is shown in figure 1. The 30-day all-cause mortality rate was significantly higher in patients with RCABPA than in those without RCABPA (31.2% vs 6.3%; P < .0005). Mortality increased progressively from in-hospital RCABPA to RCABPA occurring outside the health care setting, where it approached 50% (48.8%). Compared with in-hospital RCABPA, RCABPA occurring outside the hospital was associated with a significantly higher 30-day mortality rate or showed a clear trend toward a higher mortality rate (table 3 and figure 2).
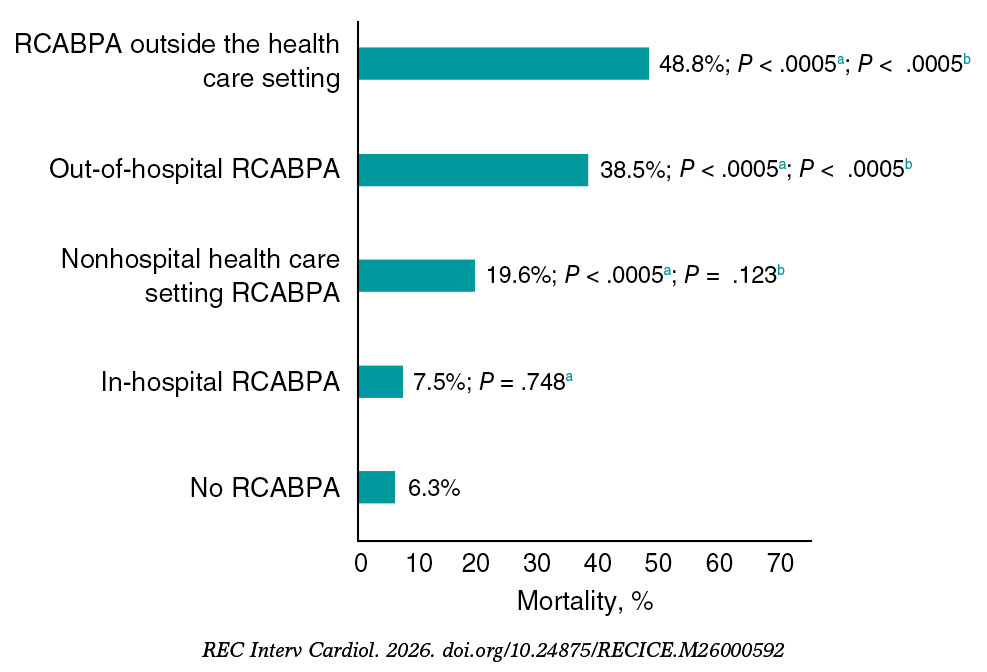
Figure 1. Thirty-day mortality according to the location of resuscitated cardiac arrest before primary angioplasty (RCABPA).
a Comparison with patients without RCABPA.
b Comparison with patients with in-hospital RCABPA.
Table 3. Interventional procedure outcome and 30-day mortality based on the location of resuscitated cardiac arrest before primary angioplasty
| Events | No RCABPA (n = 2174) | Yes RCABPA (n = 170) | P | RCABPA (n = 170) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| In-hospital (n = 40) | Pa | Primary care (n = 13) | Pa | Pb | Advanced life support ambulance (n = 33) | Pa | Pb | Outside the health care setting (n = 84) | Pa | Pb | ||||
| Procedural success | 2135 (98.2%) | 161 (94.7%) | < .001 | 37 (92.5%) | .009 | 13 (100%) | .626 | .309 | 31 (93.9%) | .072 | .809 | 80 (95.2%) | .051 | .537 |
| 30-day mortality | 136 (6.3%) | 53 (31.2%) | < .001 | 3 (7.5%) | .748 | 2 (15.4%) | .177 | .398 | 7 (21.2%) | .001 | .090 | 41 (48.8%) | < .001 | < .001 |
| 30-day cardiovascular mortality | 110 (5.1%) | 25 (14.7%) | < .001 | 2 (5.0%) | .986 | 1 (7.7%) | .667 | .715 | 6 (18.2%) | .001 | .073 | 16 (19.0%) | < .001 | .038 |
|
RCABPA, resuscitated cardiac arrest before primary angioplasty. a Comparison with no RCABPA. a Comparison with in-hospital RCABPA. |
||||||||||||||
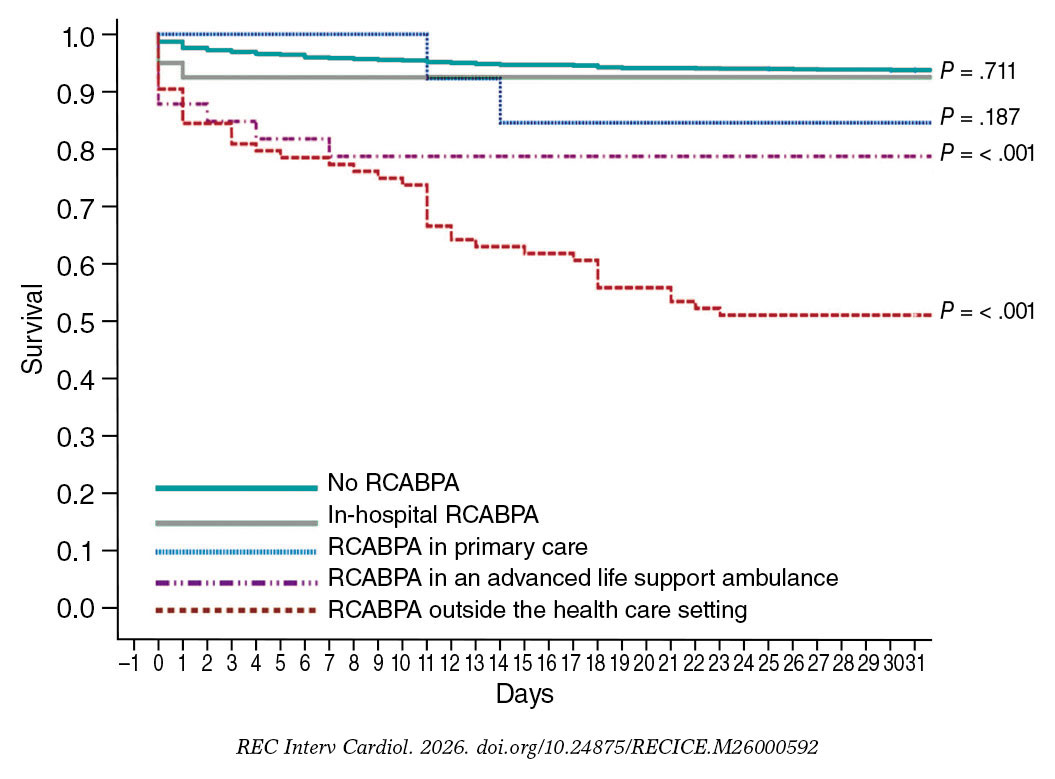
Figure 2. Kaplan-Meier curves for 30-day survival and significance of the log-rank test, using patients without resuscitated cardiac arrest before primary angioplasty (RCABPA) as the reference group.
Patients with RCABPA in a nonhospital health care setting and those with out-of-hospital RCABPA had a significantly higher 30-day mortality rate compared with patients without RCABPA (19.6% vs 6.3%; P < .0005, and 38.5% vs 6.3%; P < .0005, respectively). The 30-day mortality rate among patients with RCABPA in a nonhospital health care setting was numerically much higher than that among patients with in-hospital RCABPA, although the difference did not reach statistical significance (19.6% vs 7.5%; P = .123). When out-of-hospital RCABPA was analyzed as a grouped category, the mortality rate was significantly higher than that observed for in-hospital RCABPA (38.5% vs 7.5%; P < .0005) (figure 2).
After adjustment in logistic regression models, RCABPA was independently associated with a higher 30-day mortality rate, regardless of the presence of cardiogenic shock and other variables associated with poorer prognosis (OR, 5.99; 95%CI, 3.78-9.51; P < .0005). This association was not observed for in-hospital cardiac arrest. Furthermore, the independent predictive value for mortality was observed for out-of-hospital RCABPA (OR, 9.15; 95%CI, 5.59-14.95; P < .0005) and for RCABPA occurring outside the health care setting (OR, 20.9; 95%CI, 11.40-38.30; P < .0005). When in-hospital RCABPA was used as the reference category, the independent predictive value was maintained for virtually all nonhospital RCABPA locations. There was no significant interaction between cardiogenic shock and RCABPA in any of the models. The areas under the receiver operating characteristic curves exceeded 85% for all models (table 4).
Table 4. Adjusted contribution of recovered cardiac arrest before primary angioplasty, based on location, to 30-day mortality. Logistic regression analysis with predictors of 30-day mortality
| Location of RCABPA | n | B | 95%CI | P | Area under the ROC curve | 95%CI | P |
|---|---|---|---|---|---|---|---|
| Compared with no RCABPA (n = 2174) | |||||||
| RCABPA (any location)a | 170 | 5.99 | 3.78-9.51 | < .001 | 0.869 | 0.844-0.894 | < .001 |
| In-hospital RCABPAb | 40 | 0.26 | 0.19-1.77 | .256 | 0.862 | 0.831-0.893 | < .001 |
| RCABPA in primary carec | 13 | 3.26 | 0.63-16.94 | .159 | 0.850 | 0.817-0.883 | < .001 |
| RCABPA in an advanced life support ambulanced | 33 | 2.35 | 0.83-6.68 | .108 | 0.862 | 0.832-0.893 | < .001 |
| RCABPA outside the health care settinge | 84 | 20.90 | 11.40-38.30 | < .001 | 0.875 | 0.848-0.902 | < .001 |
| Nonhospital health care setting RCABPAc | 46 | 2.33 | 0.96-5.63 | .060 | 0.852 | 0.820-0.884 | < .001 |
| Out-of-hospital RCABPAc | 130 | 9.15 | 5.59-14.94 | < .001 | 0.869 | 0.842-0.896 | < .001 |
| Compared with in-hospital RCABPA (n = 40) | |||||||
| RCABPA in primary carec | 13 | 22.48 | 0.61-83.79 | .091 | 0.879 | 0.734-1.00 | .006 |
| RCABPA in an advanced life support ambulancec | 33 | 19.02 | 0.81-445.13 | .067 | 0.950 | 0.902-0.998 | < .001 |
| RCABPA outside the health care settingc | 84 | 35.15 | 6.99-176.65 | < .001 | 0.865 | 0.803-0.927 | < .001 |
| Nonhospital health care setting RCABPAc | 46 | 12.99 | 1.07-157.71 | .044 | 0.908 | 0.824-0.992 | < .001 |
| Out-of-hospital RCABPAc | 130 | 12.52 | 3.16-49.61 | < .001 | 0.809 | 0.745-0.873 | < .001 |
|
RCABPA, recovered cardiac arrest before primary angioplasty. Variables included in the models: a RCABPA, age, female sex, diabetes, dyslipidemia, undetermined location, shock, PCI performed, symptom-to-FMC delay. b RCABPA, age, hypertension, undetermined location, shock, PCI performed, symptom-to-FMC delay. c RCABPA, age, undetermined location, shock, PCI performed, symptom-to-FMC delay. d RCABPA, age, diabetes, hypertension, dyslipidemia, smoking, undetermined location, shock, PCI performed, symptom-to-FMC delay. a RCABPA, age, dyslipidemia, smoking, undetermined location, shock, PCI performed, symptom-to-FMC delay. |
|||||||
DISCUSSION
To our knowledge, this study analyzes the largest series of patients with RCABPA in the setting of STEMI based on the location where cardiac arrest occurred. The main findings were as follows: a) approximately half of RCABPA episodes in patients with STEMI treated within a STEMI code program occurred in a health care setting; b) although STEMI complicated by RCABPA before arrival at the cath lab was associated with a significantly higher 30-day mortality rate, prognosis varied based on RCABPA location; c) patients with in-hospital RCABPA did not have a higher crude or adjusted mortality rate compared with patients without RCABPA; and d) the prognostic differences observed based on RCABPA location may reflect differences in CPR availability and effectiveness, rather than differences in RCABPA per se. These findings suggest that improvements in the STEMI code care pathway could reduce mortality (figure 3).
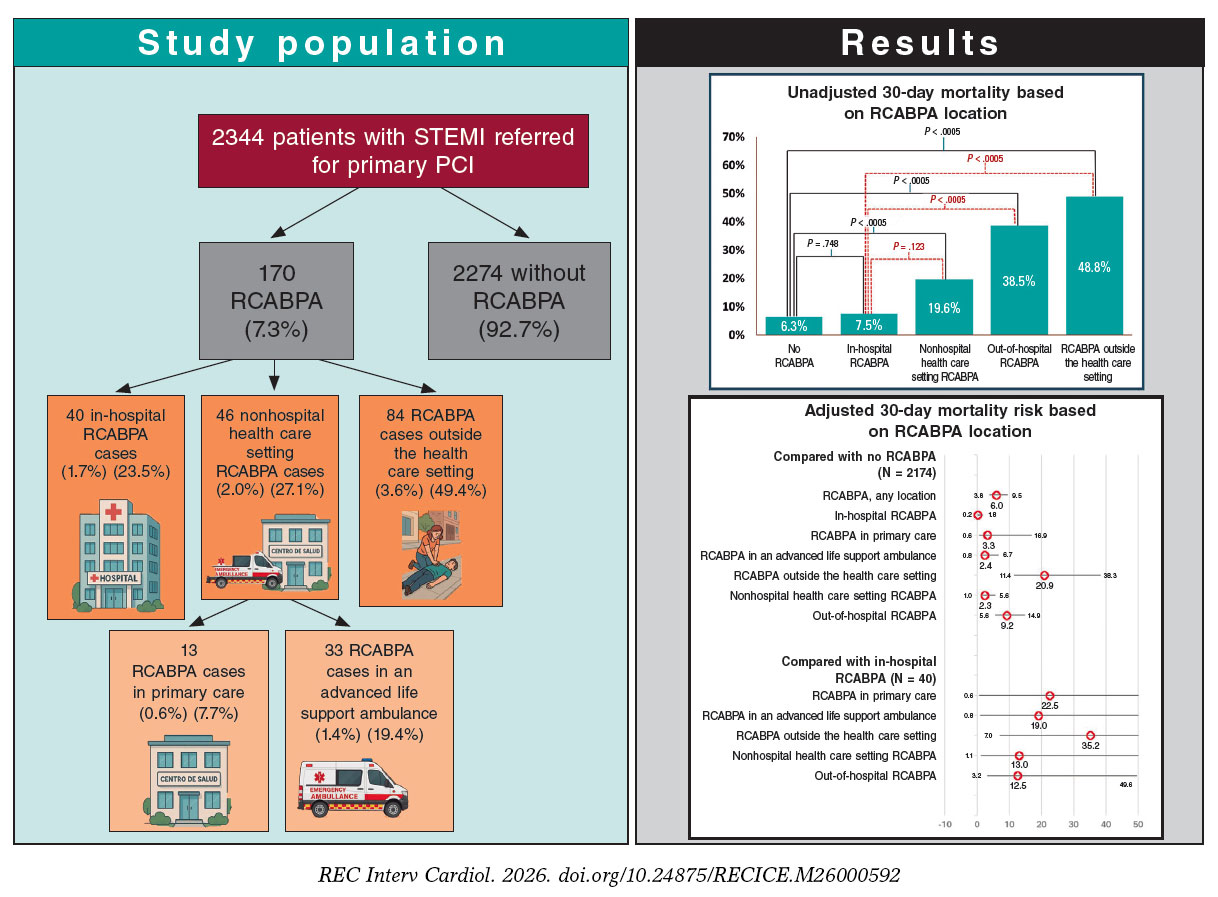
Figure 3. Central illustration. Study design and main results. PCI, percutaneous coronary intervention; RCABPA, resuscitated cardiac arrest before primary angioplasty; STEMI, ST-segment elevation myocardial infarction.
Incidence of cardiac arrest before reperfusion in patients with STEMI
Although it has been estimated that approximately half of sudden deaths are of coronary origin, these cannot be definitely classified because they represent the first sign of ischemic heart disease and patients are not resuscitated.11,12 STEMI code programs have reported an incidence of RCABPA ranging from 2% to 10%,3,6,13-15 with variability depending on inclusion criteria and delays to reperfusion. In our series, the incidence of RCABPA was 7.3%, which is close to the highest reported rates. This may be explained by the comprehensive nature of the registry, its regional coverage, and the median interval from symptom onset to reperfusion, which exceeded 200 minutes. A Danish nationwide case-control study16 including 1901 patients with STEMI reported an 11.6% incidence of ventricular fibrillation before primary angioplasty; although 83% of these episodes occurred outside the hospital, the precise location was not specified.
We found no previous studies that analyzed prognosis based on the location of RCABPA within the STEMI care pathway. This limits comparisons with our series, except for episodes occurring during transfer in an advanced life support ambulance. The first trials showing the superiority of primary angioplasty over thrombolysis in patients requiring transfer for angioplasty reported ventricular fibrillation during ambulance transport in 1.4% of the patients from the DANAMI-2 trial17 and 0.7% of the patients from the PRAGUE-2 trial.18 These figures are similar to the 1.4% observed in our cohort. In an observational study of 7393 patients with myocardial infarction transferred to a tertiary referral center, 5.6% experienced cardiac arrest before hospital arrival.19 In our series, > 35% of RCABPA episodes occurred in the out-of-hospital health care setting, underscoring the importance of appropriate training and the availability of material and human resources to provide high-quality cardiac resuscitation in these settings.
Differences in the prognosis of cardiac arrest in patients with STEMI based on location
Despite its high mortality rate, out-of-hospital cardiac arrest of coronary origin has a better prognosis than cardiac arrest of noncoronary origin.20 Currently, most studies21 assessing the characteristics or prognosis of out-of-hospital RCABPA in patients with or without ST-segment elevation myocardial infarction, have defined it simply as cardiac arrest occurring outside the hospital, without considering the specific setting or whether cardiopulmonary resuscitation was immediately available. In the present study, prognosis differed significantly based on the location of out-of-hospital RCABPA. Mortality increased progressively from RCABPA occurring at the hospital or health care setting to RCABPA occurring in a nonhospital or outside the health care setting (7.5%, 19.6%, and 48.8%, respectively). These differences do not appear to be fully explained by the patients’ baseline clinical characteristics or infarct presentation, because the independent predictive value of RCABPA location for 30-day mortality persisted after adjustment in the different multivariate models. Notably, mortality among patients with in-hospital RCABPA was not significantly different from that observed in patients without RCABPA (7.5% vs 6.3%; P = .748; figure 2). By contrast, mortality was 3 times higher among those with RCABPA occurring in a nonhospital health care setting (19.6% vs 6.3%; P < .0005). In the adjusted model (table 4), RCABPA occurring in a nonhospital health care setting was significantly associated with a higher 30-day mortality rate compared with patients without RCABPA and those with in-hospital RCABPA (OR, 13; P = .044). A previous study analyzing the prognosis of in-hospital cardiac arrest in 40 670 patients with STEMI22 reported an in-hospital mortality rate of 53%, which is substantially higher than that observed in our cohort and significantly higher than that among patients without cardiac arrest. However, unlike in our study, cardiac arrests in that series occurred throughout hospitalization and therefore probably reflected, in many cases, more severe clinical deterioration, including potentially irreversible situations.
Despite the adjustments made, we cannot rule out that patients with RCABPA had location-related characteristics that influenced prognosis. However, our findings suggest that, although health care settings have defibrillation capability and advanced CPR, and although almost all cardiac arrests are caused by shockable rhythms, in-hospital RCABPA is treated more effectively than out-of-hospital RCABPA.
Although in the present study, most RCABPA episodes involved shockable rhythms, RCABPA was associated with poor prognosis regardless of cardiogenic shock. This suggests that most RCABPA episodes were not primarily related to an irreversible hemodynamic condition, but rather that prognosis may have been determined by the consequences of delayed rhythm reversal. This interpretation is supported by the absence of significantly worse prognosis when cardiac arrest occurred in the hospital setting.
The diversity observed in mortality between in-hospital RCABPA and RCABPA occurring in other locations suggests that prognosis may be more closely related to the quality and immediacy of CPR than to cardiac arrest per se. We consider this one of the most important findings of our study, because it identifies potential opportunities to improve survival among patients with RCABPA occurring in out-of-hospital health care setting. Future studies should further explore differences in the clinical presentation and treatment of patients within the health care system outside and inside the hospital to identify actionable areas for improvement.
Prognosis of RCABPA outside the health care setting
Although most studies report in-hospital mortality rates of 55% to 70% among survivors of out-of-hospital cardiac arrest,12 the precise location of arrest is usually not specified. Cause of cardiac arrest, initial rhythm, comorbidity, and socioeconomic status have all been associated with prognosis.23 Rapid initiation of resuscitation, even by the first witness,24,25 is a key determinant of survival.23,26 In our study, mortality among patients with RCABPA occurring outside the health care setting was 6 times higher than that among patients with in-hospital RCABPA and more than twice that among patients with RCABPA occurring in out-of-hospital health care settings. This difference persisted after adjustment for the main variables associated with prognosis. These findings support the importance of population-based campaigns aimed at improving recognition of cardiac arrest and promoting early defibrillation. Current CPR guidelines27 recommend facilitating access to defibrillators in public places and training the general population in CPR maneuvers.
Two studies have analyzed differences in all-cause mortality after out-of-hospital cardiac arrest based on the precise place of occurrence.28,29 In both studies, mortality was highest when cardiac arrest occurred at home, probably because of poorer access to defibrillation and CPR. In our series, the precise location of out-of-hospital RCABPA episodes could not be determined; therefore, differences within this group based on whether they occurred in a public or private place cannot be ruled out.
Limitations
The study design does not allow to determine precisely how many patients with cardiac arrest in the context of STEMI died before STEMI code activation. An undetermined number of patients may have died before the arrival of emergency teams, during first contact, or after unsuccessful resuscitation attempts. Although nonresuscitated cardiac arrest after activation but before arrival at the cath lab is exceptional, this may not be the case for patients who experience sudden death before contact with health care services, without successful circulatory restoration allowing transfer to the cath lab. This may introduce biases that are difficult to control. We believe this limitation is common to most registries of out-of-hospital cardiac arrest and reflects the real-world clinical practice setting of the study. The similarity between our RCABPA rates and those reported in previous studies on primary angioplasty or STEMI suggests that our findings are representative of the routine clinical practice.
Some differences in mortality according to RCABPA location may be explained by clinical characteristics that were not controlled for in the multivariate analyses. Information on the presence of witnesses, availability of a semiautomatic external defibrillator, and qualifications of the first rescuer was not available in our series; therefore, their influence on the observed results could not be assessed. Despite these unmeasured variables, we believe that the observed differences, particularly within the health care setting, suggest important opportunities for improvement in STEMI code programs. The high area under the receiver operating characteristic curve observed in the different models reduces the relevance of these potential uncontrolled variables.
CONCLUSIONS
Cardiac arrest in patients with STEMI before reperfusion occurs in 7.3% of cases referred for primary angioplasty, and approximately half of these events occurred outside the health care setting. Although RCABPA was associated with significantly higher mortality rates, prognosis varied based on the location of the cardiac arrest. In-hospital RCABPA may not adversely affect prognosis, whereas out-of-hospital RCABPA, particularly when occurring outside the health care setting, was associated with significantly higher mortality rates. Improvements in regional STEMI code programs focused on early medical care and out-of-hospital CPR could reduce mortality.
FUNDING
This study received no funding.
ETHICAL CONSIDERATIONS
This study was approved by the local ethics committee, with a waiver of informed consent because it was an anonymized retrospective study. The SAGER guidelines were followed with respect to possible sex/gender bias.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
Artificial intelligence was not used in the preparation of this work.
AUTHORS’ CONTRIBUTIONS
R. López-Palop contributed to the conception and design of the study, data acquisition, analysis, and interpretation, drafting of the original project and final manuscript, and final approval. P. Carrillo Sáez collaborated in data acquisition, analysis, and interpretation, and in drafting, reviewing, and approving the manuscript. R. López-Palop López collaborated in data acquisition, analysis, and interpretation, drafting of the initial project, and review and final approval of the manuscript. M.D. Vallés García collaborated in data acquisition, analysis, and interpretation. N. Fernández Villa collaborated in drafting, reviewing, and final approval of the manuscript. J.R. Gimeno Blanes, J.M. Durán Hernández, F.J. Lacunza Ruiz, J. García de Lara, J.A. Hurtado Martínez, A. Riquelme Pérez, and E. Pinar Bermúdez collaborated in data acquisition and in review and final approval of the manuscript. D. Pascual-Figal participated in reviewing, drafting, editing, and final approval of the manuscript.
CONFLICTS OF INTEREST
None declared.
WHAT IS KNOWN ABOUT THE TOPIC?
- Most studies associate RCABPA with a higher mortality rate in patients with STEMI. In general, virtually all RCABPA episodes are analyzed as occurring outside the hospital setting, without considering possible differences associated with the location where they occur, both in terms of STEMI characteristics and prognosis.
WHAT DOES THIS STUDY ADD?
- We found significant differences in the 30-day mortality rate among patients with RCABPA based on the place of ocurrence.
- The few differences observed between patients with in-hospital RCABPA and those without RCABPA suggest a possibility for improvement in the management of this entity outside the hospital setting, following the STEMI care pathway.
REFERENCES
1. Patterson T, Perkins GD, Hassan Y, et al. Temporal Trends in Identification, Management, and Clinical Outcomes After Out-of-Hospital Cardiac Arrest:Insights From the Myocardial Ischaemia National Audit Project Database. Circ Cardiovasc Interv. 2018;11:e005346.
2. Frampton J, Ortengren AR, Zeitler EP. Arrhythmias After Acute Myocardial Infarction. Yale J Biol Med. 2023;96:83-94.
3. Karam N, Bataille S, Marijon E, et al. Incidence, Mortality, and Outcome-Predictors of Sudden Cardiac Arrest Complicating Myocardial Infarction Prior to Hospital Admission. Circ Cardiovasc Interv. 2019;12:e007081.
4. Kroupa J, Knot J, Ulman J, et al. Characteristics and Survival Determinants in Patients After Out-of-Hospital Cardiac Arrest in The Era of 24/7 Coronary Intervention Facilities. Heart Lung Circ. 2017;26:799-807.
5. Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44: 3720-3826.
6. Machado GP, Theobald AL, de Araujo GN, et al. Pre-percutaneous coronary intervention sudden cardiac arrest in ST-elevation myocardial infarction:Incidence, predictors, and related outcomes. Front Cardiovasc Med. 2023;10: 1100187.
7. Fordyce CB, Wang TY, Chen AY, et al. Long-Term Post-Discharge Risks in Older Survivors of Myocardial Infarction With and Without Out-of-Hospital Cardiac Arrest. J Am Coll Cardiol. 2016;67:1981-1990.
8. DeFilippis EM, Singh A, Gupta A, et al. Long-Term Outcomes After Out-of-Hospital Cardiac Arrest in Young Patients With Myocardial Infarction. Circulation. 2018;138:2855-2857.
9. Ando H, Sawano M, Kohsaka S, et al. Cardiac arrest and post-discharge mortality in patients with myocardial infarction:a large-scale nationwide registry analysis. Resusc Plus. 2024;18:100647.
10. Kosmidou I, Embacher M, McAndrew T, et al. Early Ventricular Tachycardia or Fibrillation in Patients With ST Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention and Impact on Mortality and Stent Thrombosis (from the Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction Trial). Am J Cardiol. 2017;120:1755-1760.
11. Deo R, Albert CM. Epidemiology and genetics of sudden cardiac death. Circulation. 2012;125:620-637.
12. Kosmopoulos M, Bartos JA, Yannopoulos D. ST-Elevation Myocardial Infarction Complicated by Out-of-Hospital Cardiac Arrest. Interv Cardiol Clin. 2021;10:359-368.
13. Rodríguez-Leor O, Cid-Álvarez AB, Pérez de Prado A, et al. Analysis of the management of ST-segment elevation myocardial infarction in Spain. Results from the ACI-SEC Infarction Code Registry. Rev Esp Cardiol. 2022;75:669-680.
14. Siudak Z, Birkemeyer R, Dziewierz A, et al. Out-of-hospital cardiac arrest in patients treated with primary PCI for STEMI. Long-term follow up data from EUROTRANSFER registry. Resuscitation. 2012;83:303-306.
15. Kragholm K, Lu D, Chiswell K, et al. Improvement in Care and Outcomes for Emergency Medical Service-Transported Patients With ST-Elevation Myocardial Infarction (STEMI) With and Without Prehospital Cardiac Arrest:A Mission:Lifeline STEMI Accelerator Study. J Am Heart Assoc. 2017;6:e005717.
16. Jabbari R, Engstrom T, Glinge C, et al. Incidence and risk factors of ventricular fibrillation before primary angioplasty in patients with first ST-elevation myocardial infarction:a nationwide study in Denmark. J Am Heart Assoc. 2015;4:e001399.
17. Andersen HR, Nielsen TT, Rasmussen K, et al. A comparison of coronary angioplasty with fibrinolytic therapy in acute myocardial infarction. N Engl J Med. 2003;349:733-742.
18. Widimsky P, Budesinsky T, Vorac D, et al. Long distance transport for primary angioplasty vs immediate thrombolysis in acute myocardial infarction. Final results of the randomized national multicentre trial —PRAGUE-2. Eur Heart J. 2003;24:94-104.
19. Becker L, Larsen MP, Eisenberg MS. Incidence of cardiac arrest during self-transport for chest pain. Ann Emerg Med. 1996;28:612-616.
20. Matta A, Philippe J, Nader V, et al. Predictors and rate of survival after Out-of-Hospital Cardiac Arrest. Curr Probl Cardiol. 2024;49:102719.
21. Desch S, Freund A, Akin I, et al. Angiography after Out-of-Hospital Cardiac Arrest without ST-Segment Elevation. N Engl J Med. 2021;385:2544-2553.
22. Gong W, Yan Y, Wang X, et al. Risk Factors for In-Hospital Cardiac Arrest in Patients With ST-Segment Elevation Myocardial Infarction. J Am Coll Cardiol. 2022;80:1788-1798.
23. Grasner JT, Herlitz J, Tjelmeland IBM, et al. European Resuscitation Council Guidelines 2021:Epidemiology of cardiac arrest in Europe. Resuscitation. 2021;161:61-79.
24. Baekgaard JS, Viereck S, Moller TP, et al. The Effects of Public Access Defibrillation on Survival After Out-of-Hospital Cardiac Arrest:A Systematic Review of Observational Studies. Circulation. 2017;136:954-965.
25. Kalarus Z, Svendsen JH, Capodanno D, et al. Cardiac arrhythmias in the emergency settings of acute coronary syndrome and revascularization:an European Heart Rhythm Association (EHRA) consensus document, endorsed by the European Association of Percutaneous Cardiovascular Interventions (EAPCI), and European Acute Cardiovascular Care Association (ACCA). Europace. 2019;21:1603-1604.
26. Perkins GD, Handley AJ, Koster RW, et al. European Resuscitation Council Guidelines for Resuscitation 2015:Section 2. Adult basic life support and automated external defibrillation. Resuscitation. 2015;95:81-99.
27. Olasveengen TM, Semeraro F, Ristagno G, et al. European Resuscitation Council Guidelines 2021:Basic Life Support. Resuscitation. 2021;161:98-114.
28. Herlitz J, Eek M, Holmberg M, Engdahl J, Holmberg S. Characteristics and outcome among patients having out of hospital cardiac arrest at home compared with elsewhere. Heart. 2002;88:579-582.
29. Wong RTM. Effect of location on out-of-hospital cardiac arrests involving older adults in Hong Kong:secondary analysis of a territory-wide cohort. Hong Kong Med J. 2023;29:142-9.













