

Original article
Transcatheter mitral edge-to-edge repair vs optimal medical therapy in secondary mitral regurgitation: a meta-analysis
Reparación mitral percutánea de borde a borde frente a tratamiento médico óptimo en regurgitación mitral secundaria: un metanálisis
aFacultad de Medicina, Universidad Autónoma Metropolitana, Mexico City, Mexico bDepartamento de Urgencias y Unidad Coronaria, Instituto Nacional de Cardiología Ignacio Chávez, Mexico City, Mexico cEscuela Superior de Medicina, Instituto Politécnico Nacional, Mexico City, Mexico dFacultad de Medicina, Universidad Católica Boliviana, Santa Cruz, Bolivia eDepartment of Medicine, Indiana University School of Medicine, IN, United States
ABSTRACT
Introduction and objectives: Coronary microcatheters play a key role in contemporary percutaneous coronary intervention (PCI), particularly in complex anatomies such as chronic total coronary occlusions. Under the European Medical Device Regulation (MDR 2017/745), post-market clinical follow-up (PMCF) studies are required to confirm safety and performance. However, PMCF evidence on coronary microcatheters remains limited. Our primary endpoint was to assess device effectiveness, defined as successful lesion or occlusion crossing. Procedural effectiveness was defined as final Thrombolysis in Myocardial Infarction grade-3 flow with < 30% residual percent diameter stenosis. Device safety endpoints included the absence of device-related mechanical failures, including rupture, kinking, or complicated retrieval.
Methods: This prospective, multicenter, multinational, observational PMCF study evaluated the safety and performance of a coronary microcatheter (Navitian, iVascular, Spain) used according to CE-marked indications. Adult patients in whom the use of the device was attempted, usually in combination with other devices, were consecutively included. Clinical outcomes were assessed during in-hospital stay up to discharge.
Results: A total of 102 patients with 115 coronary lesions were included. Lesion complexity was high: 57.4% chronic total coronary occlusions, 87.8% were American Heart Association type B2/C lesions, and 47.0% had significant calcification. Device effectiveness for lesion or occlusion crossing, evaluable in successfully wired lesions, was 95.2%. Procedural success was achieved in 100% of cases in which the device crossed. No device-related safety failures were observed. None of the adverse clinical events observed (4.3%) were adjudicated to the microcatheter.
Conclusions: In this prospective, multinational PMCF study, the Navitian coronary microcatheter demonstrated high effectiveness and an excellent device-related safety profile in a real-world complex PCI, supporting its continued use in routine complex PCIs.
(Clinicaltrials.gov NCT05292118).
Keywords: Microcatheter. Complex PCI. Real-world data. Effectiveness. Safety.
RESUMEN
Introducción y objetivos: Los microcatéteres coronarios desempeñan un papel fundamental en la intervención coronaria percutánea contemporánea, especialmente en anatomías complejas. Según el Reglamento europeo sobre productos sanitarios (MDR 2017/745), se requieren estudios de seguimiento clínico poscomercialización (PMCF) para confirmar la seguridad y el rendimiento. El objetivo principal del presente estudio fue evaluar la eficacia de un dispositivo (cruce exitoso de la lesión u oclusión). La valoración de seguridad incluye la ausencia de fallos mecánicos (rotura, estrangulamiento o retirada complicada).
Métodos: Estudio PMCF observacional, prospectivo, multicéntrico y multinacional para evaluar la seguridad y el rendimiento de un microcatéter coronario (Navitian, iVascular, España) utilizado de acuerdo con las indicaciones aprobadas por el marcado CE. Se incluyeron de forma consecutiva pacientes adultos en los que se intentó utilizar el dispositivo, normalmente en combinación con otros. Los resultados clínicos se evaluaron hasta el alta.
Resultados: Se incluyeron 102 pacientes con 115 lesiones coronarias. La complejidad de las lesiones era alta: 57,4% oclusiones totales, 87,8% lesiones American Heart Association tipo B2/C y 47,0% calcificación significativa. La eficacia del dispositivo, evaluable en las lesiones tras el cruce de la guía, fue del 95,2%. Se logró el éxito del procedimiento (flujo Thrombolysis in Myocardial Infarction 3 final con estenosis residual < 30%) en todos los casos en los que el dispositivo cruzó. No se observaron fallos de seguridad. Ninguno de los eventos clínicos adversos observados (4,3%) se atribuyó al microcatéter.
Conclusiones: En este estudio PMCF prospectivo y multinacional, el microcatéter coronario Navitian demostró una alta eficacia y un excelente perfil de seguridad en intervenciones coronarias percutáneas complejas de la práctica real.
(Clinicaltrials.gov NCT05292118).
Palabras clave: Microcatéter. Intervención coronaria percutánea compleja. Datos de la práctica real. Eficacia. Seguridad.
Abbreviations
CTO: chronic total coronary occlusion. MDR: medical device regulation. PCI: percutaneous coronary intervention. PMCF: post-market clinical follow-up.
INTRODUCTION
Percutaneous coronary intervention (PCI) has progressively expanded to increasingly complex anatomical and clinical scenarios, including chronic total coronary occlusions (CTOs), long and diffuse disease, severe calcification, and tortuous coronary anatomy. In this setting, coronary microcatheters have become indispensable adjunctive devices, facilitating guidewire support and exchange, distal contrast injection, and device delivery.
Despite their widespread use, clinical evidence supporting the safety and performance of coronary microcatheters is largely derived from single-center experiences,1,2 retrospective series,3-5 or extrapolated from broader CTO registries.6-11 Under the current European Medical Device Regulation (MDR 2017/745), manufacturers and sponsors are required to generate post-market clinical follow-up (PMCF) evidence to continuously confirm the safety and clinical performance of CE-marked devices throughout their life cycle. Real-world data, collected prospectively in routine clinical practice, play a central role in fulfilling these regulatory requirements.
The Navitian coronary microcatheter (iVascular, Spain) is a single-lumen, over-the-wire compatible device designed to facilitate guidewire advancement, exchange, and distal infusion during PCI. While its use is well established in daily practice, prospective multinational PMCF evidence evaluating its performance in real-world complex PCI remains limited.
The present study was designed as a prospective, multicenter, multinational PMCF investigation to evaluate the safety and clinical performance of the Navitian coronary microcatheter in routine practice across Spain and Portugal. By focusing on highly complex lesions and contemporary PCI workflows, this study aims to provide clinically relevant and regulatorily robust evidence supporting the real-world use of the device under MDR requirements.
METHODS
Study design
We conducted a prospective, multicenter, multinational observational PMCF study conducted in routine clinical practice in Spain and Portugal (ClinicalTrials.gov ID NCT05292118). The study was designed and performed in full compliance with the European Medical Device Regulation (MDR 2017/745), ISO 14155:2020 for clinical investigations of medical devices, the Declaration of Helsinki, and applicable national regulatory requirements.
The study followed a single-arm design without protocol-mandated additional diagnostic or therapeutic procedures beyond standard clinical care. Device use was limited to its CE-marked indications, and all procedural decisions were left to the discretion of the treating operators.
Study population
Adult patients aged 18 years or older undergoing PCI in whom use of the Navitian coronary microcatheter was attempted, either alone or in combination with other coronary devices, were consecutively included. Eligibility was based on routine clinical practice and operator judgment.
Patients were excluded only if they explicitly declined participation or refused to provide written informed consent, in accordance with local ethical and regulatory requirements.
Participant centers
The study was conducted across 7 high-volume PCI centers in Spain and Portugal, reflecting a broad spectrum of contemporary European practice. This multinational design aimed to enhance the external validity and generalizability of the findings across different healthcare systems and procedural environments.
Device description
The Navitian coronary microcatheter is a single-lumen device compatible with 0.014 in guidewires, designed to provide guidewire support, facilitate wire exchange, and allow distal infusion of contrast or saline. The device features a hydrophilic distal coating to enhance trackability through tortuous and complex coronary anatomy and incorporates a rounded atraumatic distal tip to reduce the risk of arterial damage during advancement, as well as radiopaque markers to aid fluoroscopic visualization (figure 1). The microcatheter was used strictly according to its instructions for use.
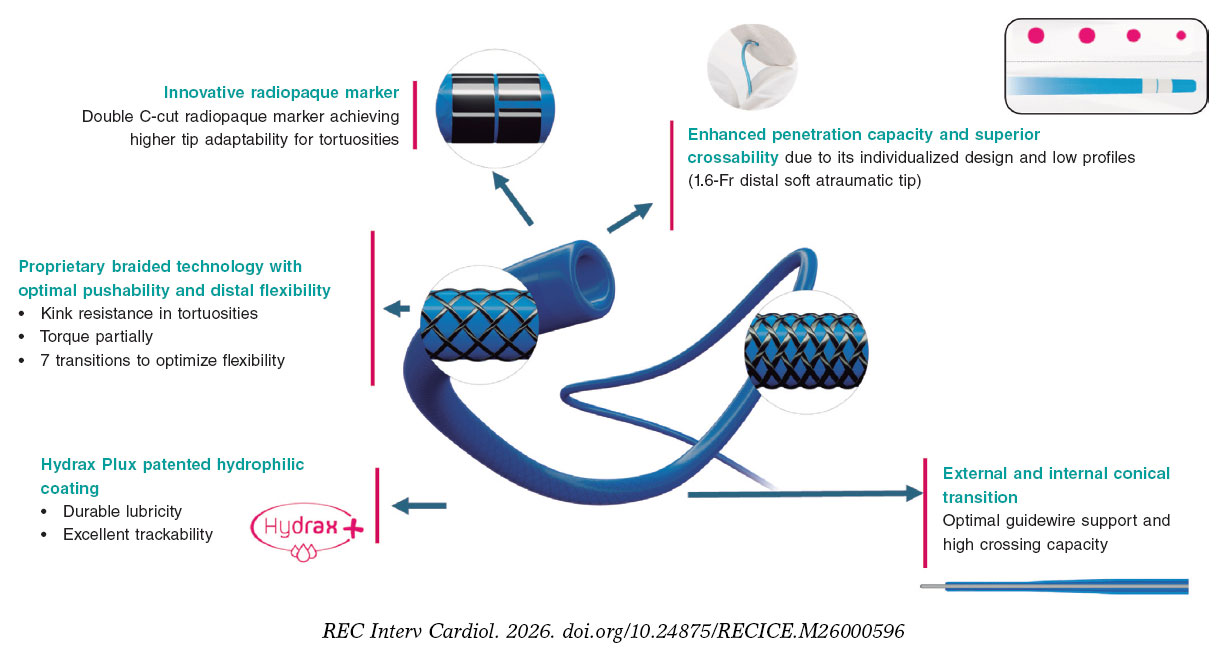
Figure 1. Navitian coronary microcatheter. Schematic representation of the Navitian microcatheter (iVascular, Barcelona, Spain), a rapid-exchange coronary microcatheter designed for use in complex percutaneous coronary intervention. The device features a hydrophilic distal coating to optimize trackability through tortuous and calcified coronary anatomy, a rounded and atraumatic distal tip to reduce the risk of vessel injury during advancement, and radiopaque markers to aid fluoroscopic visualization. The shaft design is intended to provide an optimal balance of pushability, flexibility, and torque transmission for crossing chronic total coronary occlusions and other complex lesions.
Endpoints
The primary device effectiveness endpoint was successful crossing of the target lesion or occlusion with the microcatheter.
Procedural effectiveness was defined as final Thrombolysis in Myocardial Infarction grade-3 flow12 with < 30% residual percent diameter stenosis in the treated segment at the end of the procedure.
Device safety endpoints included the absence of device-related mechanical failures, defined as device rupture, kinking, or complicated device retrieval.
Clinical outcomes were assessed during in-hospital follow-up until discharge and included the occurrence of target lesion failure, defined as the composite of cardiac death, target-vessel myocardial infarction, or clinically driven target lesion revascularization.
Given the sequential dependency inherent to complex PCI and CTO techniques, device effectiveness was assessed only in lesions in which successful guidewire crossing was achieved. Microcatheter performance cannot be meaningfully evaluated in the absence of wire passage; therefore, analyses based on evaluable lesions represent standard practice in CTO and complex PCI studies.
Data collection and monitoring
Data were collected prospectively using a standardized electronic case report form. Remote data monitoring was performed to ensure data completeness and consistency. Cases involving device or procedural failures were subject to targeted review, including source document verification when deemed necessary.
Statistical analysis
Continuous variables are expressed as mean ± standard deviation or median [IQR], as appropriate. Categorical variables are expressed as absolute counts and percentages. The incidence rate of clinical and procedural events is expressed as cumulative incidence during the in-hospital follow-up period.
The planned sample size was based on a noninferiority framework using published benchmarks for device effectiveness,13-15 assuming a reference success rate of 85%, a noninferiority margin of 10%, an alpha level of 0.05, and 80% statistical power.
All analyses were performed using JMP statistical software (version 16; SAS Institute, Cary, NC, United States).
Causality assessment
Causality between adverse events and the study device was assessed based on temporal sequence, inspection of device integrity, procedural context, and operator adjudication. Events occurring after the use of downstream interventional devices, such as balloons or stents, and in the absence of microcatheter malfunction were not considered causally related to the Navitian microcatheter.
RESULTS
Study conduct and population
After approval by the reference ethics committee and local ethics committees, patient enrollment started on 30 September, 2022, and was completed on 11 July, 2024. A total of 102 patients treated across participant centers in Spain and Portugal were included. Overall, 115 coronary lesions were addressed using the Navitian coronary microcatheter.
In 12 patients, the device was used to treat > 1 lesion (11 patients with 2 lesions and 1 patient with 3). Baseline clinical characteristics reflected a population with high cardiovascular risk and complex coronary disease. Table 1 and table 2 summarize the baseline characteristics of patients and lesions.
Table 1. Baseline characteristics
| Variable | Patient-level (n = 102) |
|---|---|
| Age (years) | 68.7 ± 9.9 |
| Male sex | 83 (81.4%) |
| Current/former smokers | 60 (58.9%) |
| Hypertension | 74 (72.5%) |
| Dyslipidemia | 84 (82.4%) |
| Diabetes mellitus | 38 (37.2%) |
| Cerebrovascular/peripheral vascular disease | 15 (14.7%) |
| Chronic kidney disease | 13 (12.7%) |
| Prior percutaneous coronary intervention | 46 (45.1%) |
| Prior coronary artery bypass grafting | 10 (9.8%) |
| Prior myocardial infarction | 37 (36.3%) |
| Multivessel disease | 60 (58.8%) |
| > 1 significant lesion | 60 (58.8%) |
| > 1 lesion treated | 20 (19.6%) |
| Left ventricular ejection fraction (%) | 50.5 [41.2-60] |
| Dual antiplatelet therapy at baseline | 87 (85.3%) |
| Oral anticoagulation at baseline | 22 (21.6%) |
| Clinical presentation | |
| ST-elevation myocardial infarction | 9 (8.8%) |
| Non–ST-elevation myocardial infarction | 34 (33.3%) |
| Stable angina | 44 (43.2%) |
| Silent ischemia | 15 (14.7%) |
|
Data are expressed as No. (%), mean ± standard deviation or median [interquartile range]. |
|
Table 2. Baseline characteristics
| Variable | Lesion-level (n = 115) |
|---|---|
| In-stent restenosis | 8 (11.8%) |
| American Heart Association B2/C lesion | 101 (87.8%) |
| Baseline TIMI grade-0 flow | 56 (48.7%) |
| Ostial lesion | 19 (16.5%) |
| Diffuse disease | 74 (64.3%) |
| Calcified lesion | 54 (47.0%) |
| Bifurcation lesion | 22 (19.1%) |
| Chronic total coronary occlusion | 66 (57.4%) |
| High tortuosity | 19 (16.5%) |
| Reference vessel diameter (mm) | 3.0 [2.5-3.0] |
| Lesion length (mm) | 30 [20-40] |
| Baseline percent diameter stenosis | 100 [90-100] |
| Location | |
| Left anterior descending coronary artery | 47 (40.9%) |
| Left circumflex artery | 15 (13.0%) |
| Right coronary artery | 51 (44.4%) |
| Left main coronary artery | 2 (1.7%) |
|
Data are expressed as No. (%) or median [interquartile range]. |
|
The mean age was 68.7 ± 9.9 years, and 81.4% of patients were male. Relevant comorbidities included diabetes mellitus in 37.2%, chronic kidney disease in 12.7%, and prior myocardial infarction in 36.3%. Previous PCI had been performed in 45.1%, and 21.6% of patients were o chronic oral anticoagulation at the time of the index procedure. Multivessel coronary artery disease was present in 58.8% of patients. Clinical presentation included ST-segment elevation acute coronary syndrome in 8.8% and non–ST-segment elevation acute coronary syndrome in 33.3%.
Lesion and procedural characteristics
Lesion complexity was high. Among the 115 treated lesions, 57.4% were CTOs, 87.8% were classified as American Heart Association type B2/C,16 64.3% showed diffuse disease, and 47.0% exhibited moderate-to-severe calcification. The median lesion length was 30 mm [IQR, 20–40 mm], with a median baseline stenosis of 100%. Lesions with ostial involvement were treated in 16.5% and bifurcation lesions in 19.1%. High vessel tortuosity, considered a key determinant of microcatheter performance, was documented in 16.5% of lesions.
The Navitian microcatheter was used to facilitate guidewire support or advancement in 83.5% of cases, for guidewire exchange after initial wire crossing of very complex lesions in 21.7%, and for distal infusion of contrast, drugs or saline in 6.1%, with overlap of indications in some procedures. Additional support techniques, such as guiding catheter extensions or balloon anchoring, were required in 13.9% of cases.
Device effectiveness and procedural success
Overall, successful crossing of the target lesion or occlusion with the Navitian microcatheter was achieved in 100 of 115 lesions (87.0%). All failed device crossings occurred in CTOs. Among lesions in which guidewire crossing was successfully achieved (n = 105), device effectiveness for lesion or occlusion crossing was 95.2%. In 5 cases, the lesion was successfully wired but the Navitian device could not cross: in 3 cases, no device was able to cross despite multiple attempts; in only 2 cases did another device successfully crossed the lesion, another microcatheter in 1 case and a 1-mm balloon in the other.
All 5 lesions in which the Navitian microcatheter failed to cross were CTOs (100%) located in the right coronary artery (4 of 5) or the first diagonal branch (1 of 5), mostly American Heart Association type C lesions (80%) and de novo (80%). This subgroup showed a high proportion of diffuse disease (80%) and a median lesion length of 32.5 mm [IQR, 28.5–44.75 mm], with moderate- to-severe calcification in 40% and high tortuosity in 40%. In 4 of 5 procedures additional support techniques were required, including a guide catheter extension system in 3 cases, and no device-related technical problems, perforations, dissections or thromboses occurred in this subgroup. Given the small sample size (n = 5), no formal statistical comparison with successfully crossed lesions (n = 100) was performed, but these findings suggest that failures were concentrated in long, diffuse right-coronary CTOs rather than in cases driven by a single identifiable anatomical feature.
In all cases in which the Navitian microcatheter successfully crossed the lesion, procedural success was achieved in 100%, defined as final Thrombolysis in Myocardial Infarction grade-3 flow with < 30% residual percent diameter stenosis in the treated segment.
Device safety and procedural complications
No device-related mechanical failures were observed. Specifically, there were no cases of device rupture, kinking, or complicated device retrieval.
Procedural complications occurred in a limited number of cases and included 3 coronary perforations, all treated with covered stents, 1 coronary dissection of grade C or higher, and 1 probable acute coronary thrombosis. However, the report’s adjudication narrative is important: the 3 perforations occurred after subsequent stent implantation and were managed with covered stents; 1 fatal despite pericardiocentesis and surgery. The probable acute thrombosis occurred after complex left main/left anterior descending coronary artery stenting and drug-coated balloon use, making exclusive attribution to the microcatheter unlikely. The dissection occurred in a failed crossing context in which aggressive CTO wiring, such as with a Pilot 200 guidewire, was used; it had no clinical sequelae.
In-hospital clinical outcomes
The median length of stay was 1 day [IQR, 1–3 days]. Three adverse clinical events were recorded during in-hospital follow-up: 1 target-vessel myocardial infarction and 2 cardiac deaths, 1 following coronary perforation, and 1 following probable acute coronary thrombosis. In all cases, these events occurred after the use of other interventional devices and were not directly attributable to the Navitian microcatheter.
DISCUSSION
In this prospective, multicenter, multinational PMCF study conducted under the requirements of the European Medical Device Regulation (MDR 2017/745), the Navitian coronary microcatheter demonstrated high effectiveness and an excellent device-related safety profile in a real-world population characterized by very high anatomical and clinical complexity. More than half of the treated lesions were CTOs and nearly 90% were classified as American Heart Association type B2/C, closely reflecting contemporary complex PCI practice in high-volume European centers.
Device effectiveness in the context of complex PCI and CTO practice
The primary effectiveness endpoint—successful lesion or occlusion crossing—was achieved in 87% of the total population, and 95.2% of evaluable lesions in which the guidewire successfully crossed, exceeding the 85% benchmark used for PMCF sample size assumptions. Importantly, failure to cross the lesion with the microcatheter was frequently driven by the inability of the guidewire to cross the lesion rather than by microcatheter malfunction. This observation underscores the sequential dependency inherent to complex PCI and CTO interventions and supports the methodological decision to assess device effectiveness only in lesions where guidewire passage was achieved.
When contextualized with published microcatheter experience, these findings appear consistent with contemporary CTO practice (table S1). In the first clinical experience with the NHancer locking microcatheter, Wilson et al.13 reported that the device contributed to at least 1 major procedural step in 85.9% of CTO cases and was the only microcatheter required in 68.4% of successful interventions. While Navitian is not a locking microcatheter, the present PMCF results similarly show that Navitian frequently enabled guidewire support and exchange: it was used for guidewire support in 83.5%, guidewire exchange in 21.7%. Adjunctive backup support, including guide extension or anchor techniques, was required in 13.9% of cases, a figure compatible with escalation patterns described in complex CTO practice.
Sidik et al.15 citer former studies showing procedural success rates in the mid-70% to mid-80% range for CTO-PCI using specialized microcatheters, such as the Corsair series, underscoring that real-world performance depends heavily on lesion complexity, crossing strategy, whether antegrade/retrograde, operator technique, and adjunctive device use.
Registry-based evidence further supports the central role of microcatheters in modern CTO algorithms. Data from contemporary European CTO registries9 indicate overall CTO PCI technical success rates in the range of 85% to 90%, with microcatheter use considered standard practice for wire support, exchange, and escalation strategies. In this context, the performance observed with Navitian aligns with expected outcomes for contemporary coronary microcatheters used in highly complex interventions.
Safety profile and attribution of adverse events
Device safety endpoints were robust: no device fracture, kinking, or difficult withdrawal were reported despite the complexity of the lesions treated. This is a key PMCF reassurance signal for a microcatheter intended for demanding anatomies, particularly in settings in which repeated device exchanges and tortuosity or calcification can increase mechanical stress.
Although 5 procedure-level complications were observed—3 perforations, 1 dissection grade ≥ C, 1 probable acute thrombosis—all the events occurred after the use of additional coronary devices, including guidewires, balloons, and stents, and were not adjudicated as causally related to the microcatheter. These nuances should be explicitly stated in the manuscript because they align with contemporary complex PCI reality: complications often reflect the cumulative risk of the full procedural sequence (wiring, microcatheter manipulation, ballooning, atherectomy/lithotripsy when used, stenting, and optimization), rather than a single device.
Compared with published CTO microcatheter series,13-15 the observed complication profile appears consistent with the underlying risk associated with complex PCI. For example, in an early clinical experience with the NHancer microcatheter,13 Wilson et al. reported a low complication rate, with 1 case of tamponade following guidewire exit that was successfully managed with a covered stent and no reported device failures. Differences compared with the procedural complications observed with Navitian should be interpreted cautiously because a) the Navitian PMCF study included non-CTO complex disease in addition to CTO and reflects broader routine-practice indications, and b) event attribution in the Navitian study points to downstream therapy, particularly stenting, rather than microcatheter malfunction.
Clinical outcomes and regulatory relevance
Three adverse clinical events were recorded during in-hospital follow-up: 1 target-vessel myocardial infarction and 2 cardiac deaths, 1 following coronary perforation, and 1 following probable acute coronary thrombosis. In all cases, these events occurred after the use of other interventional devices and were not directly attributable to the Navitian microcatheter.
Although longer-term clinical outcomes were not assessed, the absence of early device-related safety signals and the favorable procedural success rates provide meaningful evidence supporting the performance of the device under intended-use conditions.
From a regulatory perspective, this study illustrates the value of prospective real-world PMCF investigations in fulfilling MDR 2017/745 requirements.17,18 By generating device-specific evidence in routine clinical practice across multiple centers and countries, such studies complement premarket evaluations and contribute to ongoing benefit–risk assessment throughout the device life cycle. The multinational design further enhances the generalizability of the findings across different European health care environments. Consistent with this approach, prospective multicenter clinical follow-up has recently been applied to other coronary devices for complex PCI, as exemplified by the first-in-man evaluation of the Naviscore scoring balloon for moderate-to-severe calcified lesions.19
Limitations
Some limitations inherent to pragmatic PMCF studies should be acknowledged, such as a) single-arm observational design without a concurrent comparator microcatheter, limiting causal inference; b) heterogeneity of lesion subsets, including CTO and non-CTO complex disease, which enhances generalizability but complicates direct comparison to CTO-only microcatheter series such as NHancer; c) event attribution constraints in complex PCI: complications may be multifactorial and temporally linked to downstream devices or procedural steps, as occurred in this cohort. In addition, angiographic outcomes were site reported and not adjudicated by an independent core laboratory, and formal independent event adjudication was not performed; d) short follow-up and limited to discharge, restricting assessment of longer-term target lesion failure components, particularly repeat revascularization. Clinical follow-up was limited to the in-hospital period. This timeframe reflects the primary endpoint of the present PMCF study, which was to confirm device safety and technical performance under intended-use conditions, in full compliance with MDR 2017/745 requirements, rather than to assess long-term clinical effectiveness; e) standardized definitions for some anatomical features of complex PCI were lacking. No prespecified definition was applied in this study for diffuse disease, significant calcification, or coronary tortuosity; operators classified these characteristics according to their usual angiographic criteria. Several definitions of long or diffuse disease, with lesion length thresholds ranging from 20 mm to ≥ 40 mm have been proposed in the literature, but none was adopted uniformly across centers. This may introduce interobserver variability and should be taken into consideration when interpreting the complexity descriptors of the cohort.
CONCLUSIONS
In a prospective, multicenter, multinational PMCF study conducted under the European MDR framework, the Navitian coronary microcatheter demonstrated high effectiveness, excellent device-related safety, and favorable early clinical outcomes in real-world complex PCI, including CTO interventions. These findings support its continued use in routine practice and provide regulatorily robust evidence of clinical performance across different European health care environments.
FUNDING
This investigator-initiated post-market clinical follow-up study was sponsored by Fundación EPIC, a nonprofit academic organization. An unrestricted grant from the manufacturer of the device, iVascular (Barcelona, Spain) supported the development of the study. However, iVascular had no role in study design, data collection, data analysis, interpretation of the results, or preparation of the manuscript.
ETHICAL CONSIDERATIONS
The study protocol was approved by the Ethics Committee of the Lead Site (Hospital Universitario de León) and by each participant site as required by national regulations. The investigation was conducted in full compliance with the principles outlined in the Declaration of Helsinki, ISO 14155:2020 for clinical investigation of medical devices, the EU Medical Device Regulation (MDR 2017/745), and applicable local laws and regulations for postmarket clinical follow-up studies. Written informed consent was obtained from all participants prior to enrollment. Sex and gender considerations were addressed in accordance with the SAGER (Sex and Gender Equity in Research) guidelines: participants were enrolled consecutively without selection based on sex, and sex-disaggregated baseline characteristics and outcomes are reported where appropriate. The study sample reflects the real-world distribution of patients referred for complex percutaneous coronary intervention during the enrollment period.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
During the preparation of this work the authors used ChatGPT to support language editing and manuscript structuring. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
AUTHORS’ CONTRIBUTIONS
A. Pérez de Prado conceived and designed the study, served as coordinating investigator, supervised data acquisition and analysis, and drafted and critically revised the manuscript. A. Rodrigues, M. Sabaté, I.J. Amat Santos, T. García Camarero, A. Gómez Menchero, and B. García del Blanco served as site principal investigators, contributed to the study design, and participated in patient enrollment, data acquisition, and clinical follow-up. M. López Benito, P. Braga, A. Regueiro, C. Cortés Villar, J. Roa Garrido, and B. Serra Creus participated in patient enrollment, data collection, procedural documentation, and clinical follow-up at the respective sites. J.M. de la Torre-Hernández contributed to the study design, data interpretation, and critical review of the manuscript. All authors reviewed, revised, and approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
CONFLICTS OF INTEREST
J.M. de la Torre-Hernández is editor-in-chief of REC: Interventional Cardiology. A. Pérez de Prado is associate editor of REC: Interventional Cardiology; the journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. A. Pérez de Prado, M. Sabaté, B. García del Blanco, and J.M. de la Torre-Hernández report consulting or speaker fees from iVascular outside the submitted work. The remaining authors declare no conflicts of interest directly related to the subject of this study. The sponsor of the study (Fundación EPIC) received an unrestricted grant from iVascular for the conduct of this postmarket clinical follow-up; iVascular had no role in the study design, collection, analysis or interpretation of data, manuscript preparation, or the decision to submit the manuscript for publication.
WHAT IS KNOWN ABOUT THE TOPIC?
- Microcatheters are essential devices in the current management of complex PCI procedures, such as CTOs or extremely tortuous or calcified anatomies. However, evidence regarding the performance of these devices is currently scarce. With the implementation of the new European Medical Device Regulation (MDR 2017/745), PMCF studies are required to confirm the safety and performance of these products.
WHAT DOES THIS STUDY ADD?
- In a highly complex patient population, the efficacy of the analyzed device, the Navitian microcatheter, as assessed in lesions after guidewire crossing, was > 95%. Procedural success (final Thrombolysis in Myocardial Infarction grade-3 flow with < 30% residual percent diameter stenosis was achieved in all cases in which the device crossed. No safety failures, including rupture, strangulation, or complicated withdrawal, were observed. The rate of adverse clinical events was < 5%; none of the observed events were attributed to the use of the microcatheter.
SUPPLEMENTARY DATA

REFERENCES
1. Achkouty G, Dillinger JG, Sideris G, et al. Microcatheter-Facilitated Primary Angioplasty in ST-Segment Elevation Myocardial Infarction. Can J Cardiol. 2018;34:23–30.
2. Martin-Yuste V, Alvarez-Contreras L, Brugaletta S, Sabate M. Distal side-branch technique:a new use for the Tornus(R) Catheter. Cardiovasc Revasc Med. 2014;15:97–99.
3. Joseph G, Thomson VS, Radhakrishnan S. Corsair microcatheter for retrograde coronary chronic total occlusion recanalization:early experience outside the realm of dedicated recanalization specialists. Indian Heart J. 2012;64:388–393.
4. Mohandes M, Rojas S, Guarinos J, et al. Efficacy and safety of Tornus catheter in percutaneous coronary intervention of hard or balloon-uncrossable chronic total occlusion. ARYA Atheroscler. 2016;12:206–211.
5. Reifart J, Kemala E, Reifart N. Microcatheters for antegrade recanalization of chronic total coronary occlusions:Feasibility and safety of the corsair - A retrospective registry-based single operator experience. Indian Heart J. 2021;73:561–564.
6. Kandzari DE, Grantham JA, Karmpaliotis D, et al. Safety and efficacy of dedicated guidewire and microcatheter technology for chronic total coronary occlusion revascularization:principal results of the Asahi Intecc Chronic Total Occlusion Study. Coron Artery Dis. 2018;29:618–623.
7. Nikolakopoulos I, Choi JW, Alaswad K, et al. Equipment utilization in chronic total occlusion percutaneous coronary interventions:Insights from the PROGRESS-CTO registry. Catheter Cardiovasc Interv. 2021;97: 658–667.
8. Kandzari DE, Alaswad K, Jaffer FA, et al. Safety and efficacy of dedicated guidewire, microcatheter, and guide catheter extension technologies for chronic total coronary occlusion revascularization:Primary results of the Teleflex Chronic Total Occlusion Study. Catheter Cardiovasc Interv. 2022;99:263–270.
9. Vadala G, Galassi AR, Werner GS, et al. Contemporary outcomes of chronic total occlusion percutaneous coronary intervention in Europe:the ERCTO registry. EuroIntervention. 2024;20:e185–e197.
10. Mutlu D, Strepkos D, Ser OS, et al. Traditional Versus Dual Lumen Microcatheter-Assisted Parallel Wiring in Chronic Total Occlusion Percutaneous Coronary Intervention:Insights From the PROGRESS-CTO Registry. Catheter Cardiovasc Interv. 2025;105:1493–1501.
11. Alhusain R, Dayco J, Awadelkarim A, et al. Turnpike Catheter failure, causes and mechanisms:Insights from the MAUDE database. Ann Med Surg (Lond). 2022;78:103923.
12. Chesebro JH, Knatterud G, Roberts R, et al. Thrombolysis in Myocardial Infarction (TIMI) Trial, Phase I:a comparison between intravenous tissue plasminogen activator and intravenous streptokinase. Clinical findings through hospital discharge. Circulation. 1987;76:142–154.
13. Wilson SJ, Maeremans J, Walsh SJ, et al. The first clinical experience with a novel “locking“microcatheter in chronic coronary total occlusions. EuroIntervention. 2017;12:e1883–e1888.
14. Walsh SJ, Dudek D, Bryniarski L, et al. Safety and efficacy of the NovaCross microcatheter in facilitating crossing of chronic total occlusion coronary lesions:a multicenter, single-arm clinical trial. Coron Artery Dis. 2020;31:573–577.
15. Sidik N, McEntegart M, Joshi F, et al. Safety and Effectiveness of a Novel Microcatheter in Coronary Chronic Total Occlusions-The BIOMICS Study. J Soc Cardiovasc Angiogr Interv. 2024;3:102017.
16. Ryan TJ, Faxon DP, Gunnar RM, et al. Guidelines for percutaneous transluminal coronary angioplasty. A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcommittee on Percutaneous Transluminal Coronary Angioplasty). Circulation. 1988;78:486–502.
17. Zubiaur J, Rumoroso Cuevas JR, et al. Medical device research update after the adoption of the EU legislation (MDR). REC Interv Cardiol. 2025; 7:255–263.
18. Spitzer E, de la Torre Hernández JM, Guðmundsdóttir IJ, et al. Use of cardiovascular registries in regulatory pathways:perspectives from the EU-MDR Cardiovascular Collaboratory. REC Interv Cardiol. 2024; 6:213–223.
19. Serra A, Fernández-Peregrina E, Jiménez-Kockar M, et al. New scoring balloon to treat moderate-to-severe calcified coronary lesions. The first-in-man Naviscore study. REC Interv Cardiol. 2025;7:91–98.
ABSTRACT
Introduction and objectives: Resuscitated cardiac arrest before primary angioplasty (RCABPA) in ST-segment elevation myocardial infarction (STEMI) is associated with a worse prognosis. Mortality according to the place of occurrence has not been previously analyzed. Assessment of potential differences depending on where RCABPA occurs may lead to improvements in care and, consequently, reductions in STEMI-related mortality.
Methods: Observational study of a cohort of patients included in a regional infarction code program between 1 January 2021, and 31 December 2024. Thirty-day mortality and its determinants were compared according to the location of RCABPA occurrence: out-of-hospital, primary care, medicalized ambulance, or hospital.
Results: A total of 2344 patients with STEMI were included, 170 (7.3%) with RCABPA, 40 (1.7%) in the hospital setting, 13 (0.6%) in primary care, 33 (1.4%) in a medicalized ambulance, and 84 (3.6%) outside the health care setting. The initial rhythm was shockable in 158 cases (92.9%). Mortality among patients with pulseless electrical activity (PEA) was 31.2% vs 6.3% in those without PEA (P < .0005). An increase in both unadjusted and adjusted 30-day mortality was observed across groups: non-RCABPA, 6.3%; hospital, 7.5%; primary care, 15.4%; ambulance, 21.2%; and out-of-health care setting, 48.8%; it was only statistically significant when it occurred outside the hospital, both compared with non-RCABPA and in-hospital RCABPA.
Conclusions: RCABPA in STEMI is associated with significantly higher mortality. Prognosis varies according to the location of occurrence. Improvements in cardiopulmonary resuscitation conditions in the out-of-hospital setting may reduce mortality in these patients.
Keywords: Myocardial infarction. Prognosis. Primary angioplasty. Infarction code program.
RESUMEN
Introducción y objetivos: La parada cardiaca recuperada antes de la angioplastia primaria (PCRAAP) empeora notablemente el pronóstico del infarto agudo de miocardio con elevación del segmento ST (IAMCEST). Sin embargo, el efecto del lugar de ocurrencia de la PCRAAP sobre el pronóstico no se ha analizado. El conocimiento de posibles diferencias podría contribuir a mejoras asistenciales que redujeran la mortalidad del IAMCEST.
Métodos: Estudio observacional de una cohorte de pacientes incluidos en un programa regional de código infarto entre el 1 de enero de 2021 y el 31 de diciembre de 2024. Se compararon la mortalidad a 30 días y sus condicionantes según el lugar de ocurrencia de la PCRAAP: en un entorno no sanitario, en atención primaria, en una ambulancia medicalizada o en un hospital.
Resultados: Se incluyeron 2.344 pacientes con IAMCEST. Presentaron PCRAAP 170 (7,3%), 40 (1,7%) en un medio hospitalario, 13 (0,6%) en atención primaria, 33 (1,4%) en una ambulancia medicalizada y 84 (3,6%) fuera del medio sanitario. El ritmo inicial fue desfibrilable en 158 casos (92,9%). La mortalidad de los pacientes con PCRAAP fue del 31,2%, frente al 6,3% en aquellos sin PCRAAP (p < 0,0005). Se observó una mortalidad bruta y ajustada a 30 días creciente: no PCRAAP 6,3%, hospitalaria 7,5%, atención primaria 15,4%, ambulancia 21,2% y extrasanitaria 48,8%; solo fue estadísticamente significativa cuando ocurrió fuera del hospital, tanto en relación con la no PCRAAP como con la PCRAAP hospitalaria.
Conclusiones: La PCRAAP en el IAMCEST se asocia a una significativa mayor mortalidad. Su pronóstico depende del lugar donde ocurre. Mejoras en la atención a la PCRAAP extrahospitalaria, tanto sanitaria-extrahospitalaria como extrasanitaria, podrían reducir la mortalidad del IAMCEST.
Palabras clave: Infarto de miocardio. Pronóstico. Angioplastia primaria. Código infarto.
Abbreviations
CPR: cardiopulmonary resuscitation. PCI: percutaneous coronary intervention. RCABPA: resuscitated cardiac arrest before primary angioplasty. STEMI: ST-segment elevation myocardial infarction.
INTRODUCTION
Acute coronary syndrome, particularly ST-segment elevation myocardial infarction (STEMI), is the leading cause of out-of-hospital cardiac arrest.1 The main underlying mechanism is reversible ischemia, provided that reperfusion is achieved within the first few hours after STEMI.2 Approximately 1 in 20 patients with STEMI presents with cardiac arrest as the initial or early sign of myocardial infarction.3-5 Resuscitated cardiac arrest before primary angioplasty (RCABPA) is an important prognostic marker, and has been associated with 30-day mortality rates of 40% to 60%.3,6 Published studies differ regarding the long-term prognosis of patients who survive the in-hospital phase after RCABPA. Some registries have reported no long-term differences in outcomes,7,8 whereas others have found higher mortality, even after adjustment for the poorer baseline clinical profile of patients with RCABPA.9,10 However, all available studies consistently show that most events occur during the in-hospital phase or within the first 30 days after RCABPA.
“STEMI network” programs are designed to ensure rapid identification of STEMI and timely delivery of the most appropriate reperfusion strategy, preferably primary angioplasty.5 Studies evaluating the characteristics and prognosis of RCABPA have generally paid little attention to the specific point in the STEMI care pathway at which cardiac arrest occurs. Their inclusion criteria have typically included patients with RCABPA occurring outside the hospital setting, without specifying whether the cardiac arrest occurred before or after first medical contact or how close the patient was to resources for advanced cardiopulmonary resuscitation (CPR). In addition, the prognosis of RCABPA occurring in hospitals with CPR capability but without primary angioplasty capability has not been specifically analyzed. The poor short-term prognosis associated with RCABPA may be related to the clinical characteristics and consequences of the STEMI per se or to delays and limitations in CPR when cardiac arrest occurs outside the hospital setting.
Therefore, analyzing the characteristics and consequences of RCABPA based on the place of occurrence may help identify opportunities to improve the care and prognosis of patients with STEMI.
The aim of this study was to analyze short-term mortality in patients with RCABPA, with particular attention to the place where cardiac arrest occurred within the care pathway initiated by activation of the STEMI code after diagnosis.
METHODS
Design
This observational study used a historical cohort of consecutive patients admitted for primary angioplasty with a diagnosis of STEMI and an indication for reperfusion.
Study population
We included all patients who arrived at the cath lab of Hospital Clínico Universitario Virgen de la Arrixaca (El Palmar, Murcia, Spain) between 1 January, 2021, and 31 December, 2024 through the regional STEMI code program and with an indication for primary angioplasty. In patients with > 1 episode during the inclusion period, only the index episode was included. In 2023, the reference population covered by the regional STEMI code program for the study center was 1,132,310 inhabitants. Six non–PCI-capable hospitals referred patients to the study hospital, which served as the reference center. According to the STEMI code protocol, activation must occur at first medical contact, and patients should be transferred directly from the place of activation to the cath lab, without intermediate stops at other hospitals or emergency departments.
Variables
Data were obtained from the prospective patient registry of the cath lab at the reference hospital for primary angioplasty, where demographic characteristics, clinical presentation, procedural data, and follow-up information are systematically recorded. Missing data were completed by reviewing the regional electronic health record or by contacting patients or their relatives by telephone.
RCABPA was defined as cardiac arrest with return of spontaneous circulation after cardiopulmonary resuscitation maneuvers. Cardiac arrests occurring after arrival at the cath lab were excluded. Patients who died before or during transfer to the reference hospital were not included.
Patients were classified into 5 groups according to the location where RCABPA occurred: a) in-hospital RCABPA, occurring in referral hospitals before transfer or at the reference hospital prior to the arrival at the cath lab; b) RCABPA in a medicalized ambulance occurring in an ambulance with defibrillation capability; c) RCABPA in primary care, occurring in a health center or out-of-hospital emergency department with defibrillation capability; d) RCABPA outside the health care setting, occurring at home or in a public place without medical or paramedical personnel present; and e) no RCABPA, used as the control group.
All primary care centers and medicalized ambulances have the capacity to provide advanced CPR. We could not determine the exact number of patients with out-of-hospital RCABPA who may have exceptionally benefited from the proximity of a defibrillation team.
For comparisons by grouped location, groups a, b, and c were classified as RCABPA occurring in a health care setting, whereas groups b and c were classified as RCABPA occurring in an out-of-hospital health care setting.
Vital status at 30 days was obtained from the patients’ electronic health records or, when unavailable, by telephone contact.
The study was conducted in full compliance with the principles outlined in the Declaration of Helsinki. Episodes were collected retrospectively. The study was approved by the local ethics committee.
Statistical analysis
Quantitative variables are expressed as mean and standard deviation or as median and 25th-75th percentiles when they did not meet normality criteria, as assessed with the Shapiro-Wilk test. Quantitative variables that did not meet the normality criteria were compared using the nonparametric Mann-Whitney U test; normally distributed variables were compared using the Student t test for independent samples. Qualitative variables are expressed as absolute frequencies and percentages and were compared using the Pearson chi-square test. As specified in the tables and Results section, patients without RCABPA and those with in-hospital RCABPA were used as reference groups, as appropriate. Thirty-day mortality was assessed using Kaplan-Meier survival analysis. Survival curves were plotted for patients without RCABPA and for those with RCABPA at each individual and grouped location. Survival curves were compared using the log-rank test, with patients without RCABPA and those with in-hospital RCABPA used as reference groups. In all cases, P values < .05 were considered statistically significant.
To determine the contribution of RCABPA to 30-day mortality compared with the absence of RCABPA, as well as the contribution of RCABPA according to its location, logistic regression models were constructed. Models were adjusted for variables that were asymmetrically distributed across the study subgroups in the univariate analysis (P > .1) or that have been associated in the literature with higher mortality: age, diabetes, cardiogenic shock, performance of percutaneous coronary intervention (PCI), anterior infarct location, and delay from symptom onset to first medical contact. The absence of significant multicollinearity among the included variables was confirmed. The predictive performance of each model was assessed using the receiver operating characteristic curve, based on 30-day mortality predicted by the models and observed mortality.
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., United States), and SigmaPlot for Windows, version 11.0 (Systat Software, Inc., United States).
RESULTS
Population description
During the 4-year study period, there were 2463 activations of the STEMI code program with an indication for primary angioplasty. A total of 119 cases (4.9%) were excluded because they had previously been referred for primary angioplasty, leaving a final sample of 2344 patients, 170 of whom (7.3%) experienced RCABPA: 40 (1.7%) in a hospital setting, 13 (0.6%) in primary care, 33 (1.4%) in an advanced life support ambulance, and 84 (3.6%) outside the health care setting. Eight aborted STEMI code activation due to patient death before arrival at the cath lab were recorded, including 3 deaths in an advanced life support ambulance. The final cause of death could not be determined. All these patients had cardiogenic shock at the time of activation and were not included in the study.
The initial rhythm of RCABPA was shockable in 158 cases (92.9%). Baseline characteristics and infarct presentation based on the presence of RCABPA are shown in table 1. Patients with RCABPA underwent PCI less frequently than those without RCABPA (76.5% vs 85.6%; P = .001). PCI was not performed in 2 cases of RCABPA because the patients died before the procedure could be initiated, or in 28 cases because no culprit coronary lesion was identified.
Table 1. Baseline, acute myocardial infarction presentation, and procedural characteristics according to the occurrence or absence of resuscitated cardiac arrest before primary angioplasty
| Variable | No RCABPA (n = 2174) | RCABPA (n = 170) | P |
|---|---|---|---|
| Age, yearsa | 63 (54-74) | 60 (52-69) | .025 |
| Women | 521 (24.0%) | 28 (16.5%) | .026 |
| Age > 80 years | 273 (12.6%) | 17 (10.0%) | .329 |
| Age < 50 years | 320 (14.7%) | 33 (19.4%) | .099 |
| Diabetes | 686 (31.6%) | 41 (24.1%) | .043 |
| Hypertension | 1230 (56.6%) | 92 (54.1%) | .533 |
| Dyslipidemia | 1094 (50.3%) | 66 (38.8%) | .004 |
| Smoking | 1196 (55.0%) | 84 (49.4%) | .158 |
| Previous AMI | 158 (7.3%) | 8 (4.7%) | .210 |
| Previous PCI | 206 (9.5%) | 11 (6.5%) | .193 |
| Shockable rhythm | – | 158 (92.9%) | – |
| PCI performed | 1862 (85.6%) | 130 (76.5%) | .001 |
| Shock | 135 (6.2%) | 47 (27.6%) | < .001 |
| Anterior location | 843 (38.8%) | 78 (45.9%) | .068 |
| Outside working hours | 1685 (77.5%) | 136 (80.0%) | .452 |
| Undetermined location | 82 (3.8%) | 31 (18.2%) | < .001 |
| Symptom-to-FMC time, mina | 60 (30-155) | 20 (10-40) | < .001 |
| FMC-to-reperfusion time, mina | 116 (85-171) | 129 (91-160) | .428 |
| Symptom-to-reperfusion time, mina | 205 (137-355) | 150 (122-210) | < .001 |
|
AMI, acute myocardial infarction; FMC, first medical contact; PCI, percutaneous coronary intervention; RCABPA, resuscitated cardiac arrest before primary angioplasty; SD, standard deviation. a Median (25th-75th percentiles). |
|||
Baseline characteristics and infarct presentation based the presence and location of RCABPA are shown in table 2.
Table 2. Baseline, acute myocardial infarction presentation, and procedural characteristics based on the location of resuscitated cardiac arrest before primary angioplasty
| Variable | No RCABPA (n = 2174) | RCABPA (n = 170) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| In-hospital (n = 40) | Pa | Primary care (n = 13) | Pa | Pb | Advanced life support ambulance (n = 33) | Pa | Pb | Outside the health care setting (n = 84) | Pa | Pb | ||
| Age, yearsc | 63 (54-74) | 60 (52-72) | .397 | 54 (47-80) | .329 | .656 | 59 (54-69) | .436 | .987 | 61 (52-69) | .071 | .761 |
| Women | 521 (24.0%) | 6 (15.0%) | .187 | 4 (30.9%) | .567 | .207 | 4 (12.1%) | .113 | .722 | 14 (16.7%) | .123 | .814 |
| Age > 80 years | 273 (12.6%) | 4 (10.0%) | .628 | 4 (30.8%) | .049 | .069 | 4 (12.1%) | .940 | .773 | 5 (6.0%) | .071 | .417 |
| Age < 50 years | 320 (14.7%) | 7 (17.5%) | .623 | 5 (38.5%) | .016 | .117 | 4 (12.1%) | .676 | .523 | 17 (20.2%) | .164 | .718 |
| Diabetes | 686 (31.6%) | 13 (32.5%) | .899 | 4 (30.8%) | .952 | .908 | 4 (12.1%) | .017 | .040 | 20 (23.8%) | .133 | .306 |
| Hypertension | 1230 (56.6%) | 29 (72.5%) | .044 | 10 (76.9%) | .140 | .753 | 13 (39.4%) | .048 | .004 | 40 (47.6%) | .104 | .009 |
| Dyslipidemia | 1094 (50.3%) | 18 (45.0%) | .505 | 7 (53.8%) | .800 | .579 | 9 (27.3%) | .009 | .118 | 32 (38.1%) | .028 | .464 |
| Smoking | 1196 (55.0%) | 21 (52.5%) | .752 | 7 (53.8%) | .933 | .933 | 24 (72.7%) | .042 | .077 | 32 (38.1%) | .002 | .130 |
| Previous AMI | 158 (7.3%) | 1 (2.5%) | .247 | 0 (0.0%) | .313 | .565 | 2 (6.1%) | .791 | .445 | 5 (6.0%) | .648 | .402 |
| Previous PCI | 206 (9.5%) | 3 (7.5%) | .672 | 0 (0.0%) | .244 | .309 | 2 (6.1%) | .505 | .909 | 6 (7.1%) | .472 | .943 |
| Shockable rhythm | – | 38 (95.0%) | – | 13 (100%) | – | .411 | 31 (93.9%) | – | .352 | 76 (90.5%) | – | .387 |
| PCI performed | 1862 (85.6%) | 28 (70.0%) | .005 | 12 (92.3%) | .494 | .104 | 33 (100%) | .019 | .173 | 57 (67.9%) | < .001 | .810 |
| Shock | 135 (6.2%) | 12 (30.0%) | < .001 | 1 (7.7%) | .825 | .104 | 15 (45.5%) | < .001 | .168 | 19 (22.6%) | < .001 | .375 |
| Anterior location | 843 (38.8%) | 21 (52.5%) | .078 | 10(76.9%) | .005 | .121 | 12 (36.4%) | .778 | .158 | 35 (41.7%) | .594 | .257 |
| Outside working hours | 1685 (77.5%) | 28 (70.0%) | .261 | 10 (76.9%) | .960 | .398 | 25 (75.8%) | .811 | .583 | 73 (86.9%) | .042 | .024 |
| Undetermined location | 82 (3.8%) | 5 (12.5%) | .005 | 2 (15.4%) | .030 | .709 | 2 (6.1%) | .495 | .001 | 22 (26.2%) | < .001 | .084 |
| Symptom-to-FMC time, minc | 60 (30-155) | 13 (0.5-35) | < .001 | 27 (16-55) | .028 | .064 | 30 (21-60) | .003 | .005 | 30 (20-69) | < .001 | .029 |
| FMC-to-reperfusion time, minc | 116 (85-171) | 126 (100-174) | .404 | 116 (95-157) | .993 | .486 | 91 (79-128) | .028 | .030 | 135 (105-164) | .049 | .672 |
| Symptom-to-reperfusion time, minc | 205 (137-355) | 150 (120-225) | .005 | 155 (108-235) | .038 | .857 | 146 (106-206) | < .001 | .387 | 155 (133-208) | < .001 | .469 |
|
AMI, acute myocardial infarction; FMC, first medical contact; PCI, percutaneous coronary intervention; RCABPA, resuscitated cardiac arrest before primary angioplasty. a Comparison with no RCABPA. b Comparison with in-hospital RCABPA. c Median (25th-75th percentiles). |
||||||||||||
A total of 32 patients received mechanical circulatory support, representing 1.4% of the overall population and 17.6% of patients with cardiogenic shock. In this group, the 30-day mortality rate was 47%. Mechanical circulatory support was used in 10 patients with cardiogenic shock and RCABPA (21.2%; 30-day mortality, 70%) and in 22 patients with cardiogenic shock without RCABPA (16.3%; 30-day mortality, 36.4%).
Mortality based on the location of RCABPA
The 30-day all-cause and cardiovascular mortality rates are shown in table 3, and mortality grouped by RCABPA location is shown in figure 1. The 30-day all-cause mortality rate was significantly higher in patients with RCABPA than in those without RCABPA (31.2% vs 6.3%; P < .0005). Mortality increased progressively from in-hospital RCABPA to RCABPA occurring outside the health care setting, where it approached 50% (48.8%). Compared with in-hospital RCABPA, RCABPA occurring outside the hospital was associated with a significantly higher 30-day mortality rate or showed a clear trend toward a higher mortality rate (table 3 and figure 2).
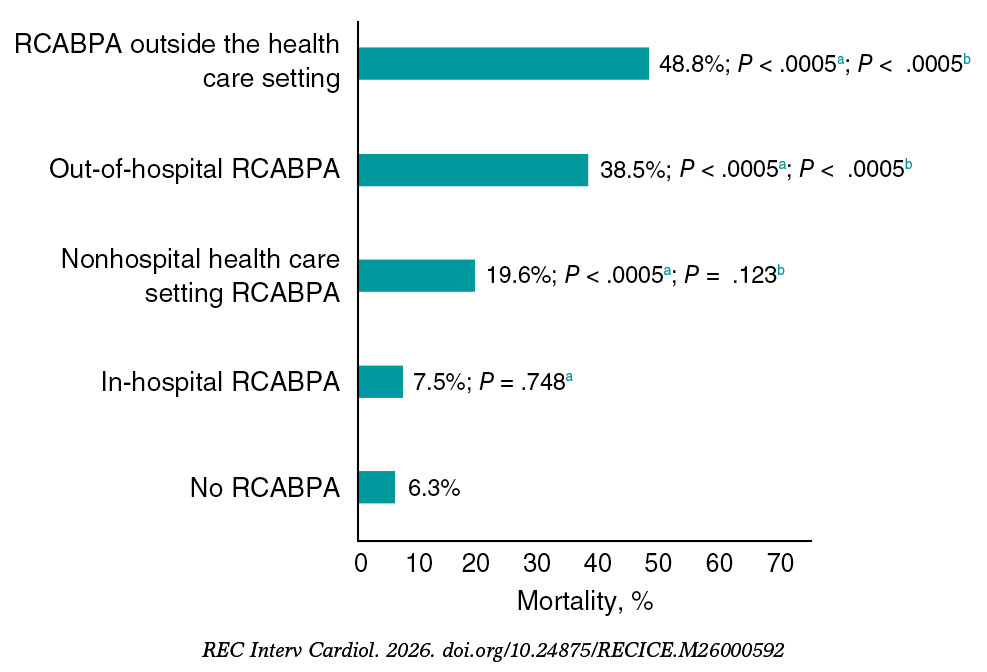
Figure 1. Thirty-day mortality according to the location of resuscitated cardiac arrest before primary angioplasty (RCABPA).
a Comparison with patients without RCABPA.
b Comparison with patients with in-hospital RCABPA.
Table 3. Interventional procedure outcome and 30-day mortality based on the location of resuscitated cardiac arrest before primary angioplasty
| Events | No RCABPA (n = 2174) | Yes RCABPA (n = 170) | P | RCABPA (n = 170) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| In-hospital (n = 40) | Pa | Primary care (n = 13) | Pa | Pb | Advanced life support ambulance (n = 33) | Pa | Pb | Outside the health care setting (n = 84) | Pa | Pb | ||||
| Procedural success | 2135 (98.2%) | 161 (94.7%) | < .001 | 37 (92.5%) | .009 | 13 (100%) | .626 | .309 | 31 (93.9%) | .072 | .809 | 80 (95.2%) | .051 | .537 |
| 30-day mortality | 136 (6.3%) | 53 (31.2%) | < .001 | 3 (7.5%) | .748 | 2 (15.4%) | .177 | .398 | 7 (21.2%) | .001 | .090 | 41 (48.8%) | < .001 | < .001 |
| 30-day cardiovascular mortality | 110 (5.1%) | 25 (14.7%) | < .001 | 2 (5.0%) | .986 | 1 (7.7%) | .667 | .715 | 6 (18.2%) | .001 | .073 | 16 (19.0%) | < .001 | .038 |
|
RCABPA, resuscitated cardiac arrest before primary angioplasty. a Comparison with no RCABPA. a Comparison with in-hospital RCABPA. |
||||||||||||||
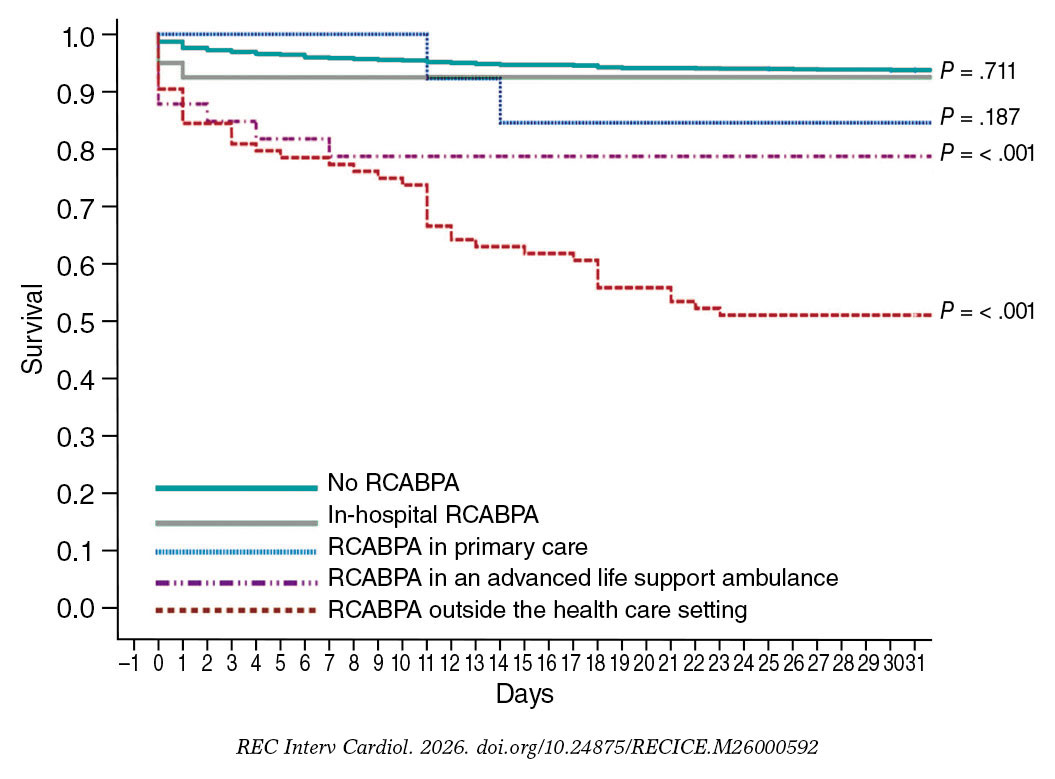
Figure 2. Kaplan-Meier curves for 30-day survival and significance of the log-rank test, using patients without resuscitated cardiac arrest before primary angioplasty (RCABPA) as the reference group.
Patients with RCABPA in a nonhospital health care setting and those with out-of-hospital RCABPA had a significantly higher 30-day mortality rate compared with patients without RCABPA (19.6% vs 6.3%; P < .0005, and 38.5% vs 6.3%; P < .0005, respectively). The 30-day mortality rate among patients with RCABPA in a nonhospital health care setting was numerically much higher than that among patients with in-hospital RCABPA, although the difference did not reach statistical significance (19.6% vs 7.5%; P = .123). When out-of-hospital RCABPA was analyzed as a grouped category, the mortality rate was significantly higher than that observed for in-hospital RCABPA (38.5% vs 7.5%; P < .0005) (figure 2).
After adjustment in logistic regression models, RCABPA was independently associated with a higher 30-day mortality rate, regardless of the presence of cardiogenic shock and other variables associated with poorer prognosis (OR, 5.99; 95%CI, 3.78-9.51; P < .0005). This association was not observed for in-hospital cardiac arrest. Furthermore, the independent predictive value for mortality was observed for out-of-hospital RCABPA (OR, 9.15; 95%CI, 5.59-14.95; P < .0005) and for RCABPA occurring outside the health care setting (OR, 20.9; 95%CI, 11.40-38.30; P < .0005). When in-hospital RCABPA was used as the reference category, the independent predictive value was maintained for virtually all nonhospital RCABPA locations. There was no significant interaction between cardiogenic shock and RCABPA in any of the models. The areas under the receiver operating characteristic curves exceeded 85% for all models (table 4).
Table 4. Adjusted contribution of recovered cardiac arrest before primary angioplasty, based on location, to 30-day mortality. Logistic regression analysis with predictors of 30-day mortality
| Location of RCABPA | n | B | 95%CI | P | Area under the ROC curve | 95%CI | P |
|---|---|---|---|---|---|---|---|
| Compared with no RCABPA (n = 2174) | |||||||
| RCABPA (any location)a | 170 | 5.99 | 3.78-9.51 | < .001 | 0.869 | 0.844-0.894 | < .001 |
| In-hospital RCABPAb | 40 | 0.26 | 0.19-1.77 | .256 | 0.862 | 0.831-0.893 | < .001 |
| RCABPA in primary carec | 13 | 3.26 | 0.63-16.94 | .159 | 0.850 | 0.817-0.883 | < .001 |
| RCABPA in an advanced life support ambulanced | 33 | 2.35 | 0.83-6.68 | .108 | 0.862 | 0.832-0.893 | < .001 |
| RCABPA outside the health care settinge | 84 | 20.90 | 11.40-38.30 | < .001 | 0.875 | 0.848-0.902 | < .001 |
| Nonhospital health care setting RCABPAc | 46 | 2.33 | 0.96-5.63 | .060 | 0.852 | 0.820-0.884 | < .001 |
| Out-of-hospital RCABPAc | 130 | 9.15 | 5.59-14.94 | < .001 | 0.869 | 0.842-0.896 | < .001 |
| Compared with in-hospital RCABPA (n = 40) | |||||||
| RCABPA in primary carec | 13 | 22.48 | 0.61-83.79 | .091 | 0.879 | 0.734-1.00 | .006 |
| RCABPA in an advanced life support ambulancec | 33 | 19.02 | 0.81-445.13 | .067 | 0.950 | 0.902-0.998 | < .001 |
| RCABPA outside the health care settingc | 84 | 35.15 | 6.99-176.65 | < .001 | 0.865 | 0.803-0.927 | < .001 |
| Nonhospital health care setting RCABPAc | 46 | 12.99 | 1.07-157.71 | .044 | 0.908 | 0.824-0.992 | < .001 |
| Out-of-hospital RCABPAc | 130 | 12.52 | 3.16-49.61 | < .001 | 0.809 | 0.745-0.873 | < .001 |
|
RCABPA, recovered cardiac arrest before primary angioplasty. Variables included in the models: a RCABPA, age, female sex, diabetes, dyslipidemia, undetermined location, shock, PCI performed, symptom-to-FMC delay. b RCABPA, age, hypertension, undetermined location, shock, PCI performed, symptom-to-FMC delay. c RCABPA, age, undetermined location, shock, PCI performed, symptom-to-FMC delay. d RCABPA, age, diabetes, hypertension, dyslipidemia, smoking, undetermined location, shock, PCI performed, symptom-to-FMC delay. a RCABPA, age, dyslipidemia, smoking, undetermined location, shock, PCI performed, symptom-to-FMC delay. |
|||||||
DISCUSSION
To our knowledge, this study analyzes the largest series of patients with RCABPA in the setting of STEMI based on the location where cardiac arrest occurred. The main findings were as follows: a) approximately half of RCABPA episodes in patients with STEMI treated within a STEMI code program occurred in a health care setting; b) although STEMI complicated by RCABPA before arrival at the cath lab was associated with a significantly higher 30-day mortality rate, prognosis varied based on RCABPA location; c) patients with in-hospital RCABPA did not have a higher crude or adjusted mortality rate compared with patients without RCABPA; and d) the prognostic differences observed based on RCABPA location may reflect differences in CPR availability and effectiveness, rather than differences in RCABPA per se. These findings suggest that improvements in the STEMI code care pathway could reduce mortality (figure 3).
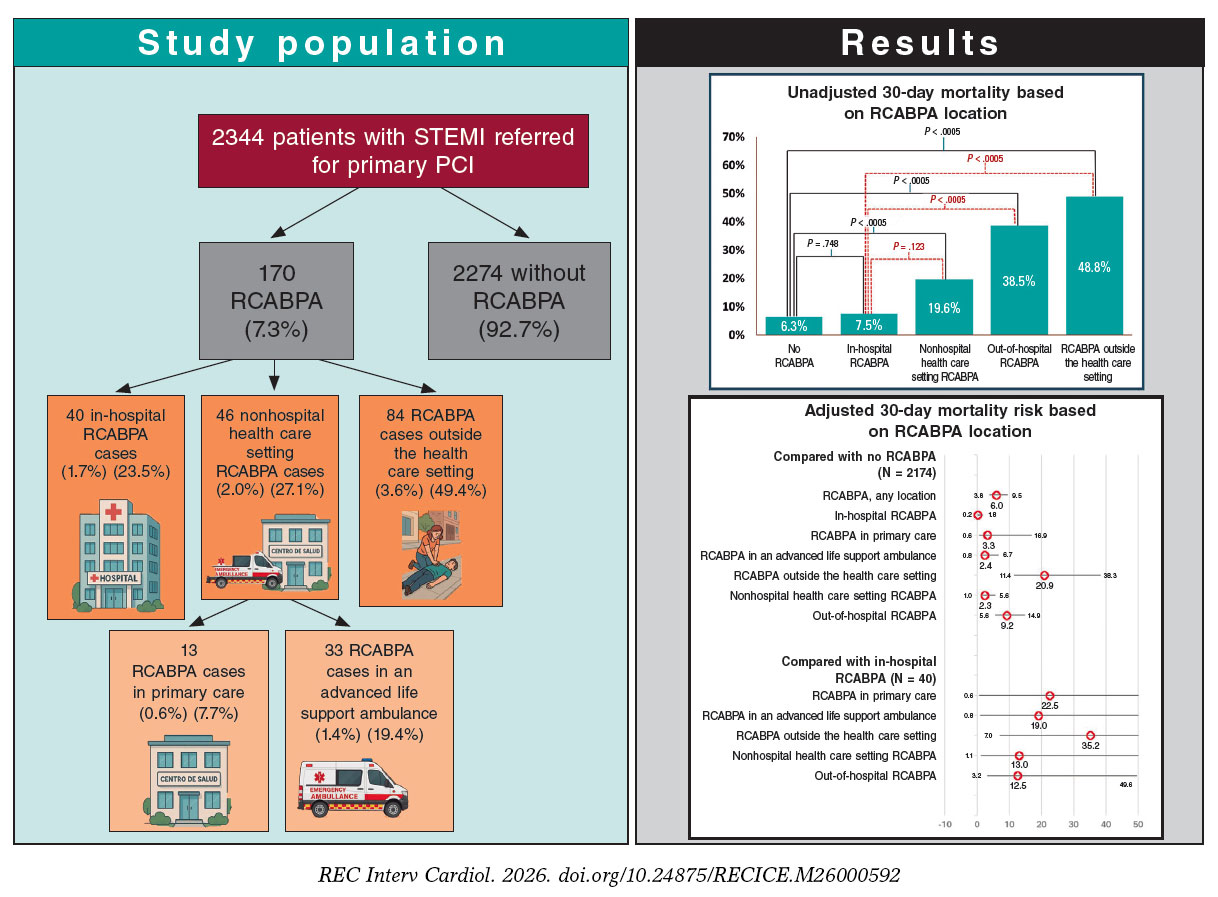
Figure 3. Central illustration. Study design and main results. PCI, percutaneous coronary intervention; RCABPA, resuscitated cardiac arrest before primary angioplasty; STEMI, ST-segment elevation myocardial infarction.
Incidence of cardiac arrest before reperfusion in patients with STEMI
Although it has been estimated that approximately half of sudden deaths are of coronary origin, these cannot be definitely classified because they represent the first sign of ischemic heart disease and patients are not resuscitated.11,12 STEMI code programs have reported an incidence of RCABPA ranging from 2% to 10%,3,6,13-15 with variability depending on inclusion criteria and delays to reperfusion. In our series, the incidence of RCABPA was 7.3%, which is close to the highest reported rates. This may be explained by the comprehensive nature of the registry, its regional coverage, and the median interval from symptom onset to reperfusion, which exceeded 200 minutes. A Danish nationwide case-control study16 including 1901 patients with STEMI reported an 11.6% incidence of ventricular fibrillation before primary angioplasty; although 83% of these episodes occurred outside the hospital, the precise location was not specified.
We found no previous studies that analyzed prognosis based on the location of RCABPA within the STEMI care pathway. This limits comparisons with our series, except for episodes occurring during transfer in an advanced life support ambulance. The first trials showing the superiority of primary angioplasty over thrombolysis in patients requiring transfer for angioplasty reported ventricular fibrillation during ambulance transport in 1.4% of the patients from the DANAMI-2 trial17 and 0.7% of the patients from the PRAGUE-2 trial.18 These figures are similar to the 1.4% observed in our cohort. In an observational study of 7393 patients with myocardial infarction transferred to a tertiary referral center, 5.6% experienced cardiac arrest before hospital arrival.19 In our series, > 35% of RCABPA episodes occurred in the out-of-hospital health care setting, underscoring the importance of appropriate training and the availability of material and human resources to provide high-quality cardiac resuscitation in these settings.
Differences in the prognosis of cardiac arrest in patients with STEMI based on location
Despite its high mortality rate, out-of-hospital cardiac arrest of coronary origin has a better prognosis than cardiac arrest of noncoronary origin.20 Currently, most studies21 assessing the characteristics or prognosis of out-of-hospital RCABPA in patients with or without ST-segment elevation myocardial infarction, have defined it simply as cardiac arrest occurring outside the hospital, without considering the specific setting or whether cardiopulmonary resuscitation was immediately available. In the present study, prognosis differed significantly based on the location of out-of-hospital RCABPA. Mortality increased progressively from RCABPA occurring at the hospital or health care setting to RCABPA occurring in a nonhospital or outside the health care setting (7.5%, 19.6%, and 48.8%, respectively). These differences do not appear to be fully explained by the patients’ baseline clinical characteristics or infarct presentation, because the independent predictive value of RCABPA location for 30-day mortality persisted after adjustment in the different multivariate models. Notably, mortality among patients with in-hospital RCABPA was not significantly different from that observed in patients without RCABPA (7.5% vs 6.3%; P = .748; figure 2). By contrast, mortality was 3 times higher among those with RCABPA occurring in a nonhospital health care setting (19.6% vs 6.3%; P < .0005). In the adjusted model (table 4), RCABPA occurring in a nonhospital health care setting was significantly associated with a higher 30-day mortality rate compared with patients without RCABPA and those with in-hospital RCABPA (OR, 13; P = .044). A previous study analyzing the prognosis of in-hospital cardiac arrest in 40 670 patients with STEMI22 reported an in-hospital mortality rate of 53%, which is substantially higher than that observed in our cohort and significantly higher than that among patients without cardiac arrest. However, unlike in our study, cardiac arrests in that series occurred throughout hospitalization and therefore probably reflected, in many cases, more severe clinical deterioration, including potentially irreversible situations.
Despite the adjustments made, we cannot rule out that patients with RCABPA had location-related characteristics that influenced prognosis. However, our findings suggest that, although health care settings have defibrillation capability and advanced CPR, and although almost all cardiac arrests are caused by shockable rhythms, in-hospital RCABPA is treated more effectively than out-of-hospital RCABPA.
Although in the present study, most RCABPA episodes involved shockable rhythms, RCABPA was associated with poor prognosis regardless of cardiogenic shock. This suggests that most RCABPA episodes were not primarily related to an irreversible hemodynamic condition, but rather that prognosis may have been determined by the consequences of delayed rhythm reversal. This interpretation is supported by the absence of significantly worse prognosis when cardiac arrest occurred in the hospital setting.
The diversity observed in mortality between in-hospital RCABPA and RCABPA occurring in other locations suggests that prognosis may be more closely related to the quality and immediacy of CPR than to cardiac arrest per se. We consider this one of the most important findings of our study, because it identifies potential opportunities to improve survival among patients with RCABPA occurring in out-of-hospital health care setting. Future studies should further explore differences in the clinical presentation and treatment of patients within the health care system outside and inside the hospital to identify actionable areas for improvement.
Prognosis of RCABPA outside the health care setting
Although most studies report in-hospital mortality rates of 55% to 70% among survivors of out-of-hospital cardiac arrest,12 the precise location of arrest is usually not specified. Cause of cardiac arrest, initial rhythm, comorbidity, and socioeconomic status have all been associated with prognosis.23 Rapid initiation of resuscitation, even by the first witness,24,25 is a key determinant of survival.23,26 In our study, mortality among patients with RCABPA occurring outside the health care setting was 6 times higher than that among patients with in-hospital RCABPA and more than twice that among patients with RCABPA occurring in out-of-hospital health care settings. This difference persisted after adjustment for the main variables associated with prognosis. These findings support the importance of population-based campaigns aimed at improving recognition of cardiac arrest and promoting early defibrillation. Current CPR guidelines27 recommend facilitating access to defibrillators in public places and training the general population in CPR maneuvers.
Two studies have analyzed differences in all-cause mortality after out-of-hospital cardiac arrest based on the precise place of occurrence.28,29 In both studies, mortality was highest when cardiac arrest occurred at home, probably because of poorer access to defibrillation and CPR. In our series, the precise location of out-of-hospital RCABPA episodes could not be determined; therefore, differences within this group based on whether they occurred in a public or private place cannot be ruled out.
Limitations
The study design does not allow to determine precisely how many patients with cardiac arrest in the context of STEMI died before STEMI code activation. An undetermined number of patients may have died before the arrival of emergency teams, during first contact, or after unsuccessful resuscitation attempts. Although nonresuscitated cardiac arrest after activation but before arrival at the cath lab is exceptional, this may not be the case for patients who experience sudden death before contact with health care services, without successful circulatory restoration allowing transfer to the cath lab. This may introduce biases that are difficult to control. We believe this limitation is common to most registries of out-of-hospital cardiac arrest and reflects the real-world clinical practice setting of the study. The similarity between our RCABPA rates and those reported in previous studies on primary angioplasty or STEMI suggests that our findings are representative of the routine clinical practice.
Some differences in mortality according to RCABPA location may be explained by clinical characteristics that were not controlled for in the multivariate analyses. Information on the presence of witnesses, availability of a semiautomatic external defibrillator, and qualifications of the first rescuer was not available in our series; therefore, their influence on the observed results could not be assessed. Despite these unmeasured variables, we believe that the observed differences, particularly within the health care setting, suggest important opportunities for improvement in STEMI code programs. The high area under the receiver operating characteristic curve observed in the different models reduces the relevance of these potential uncontrolled variables.
CONCLUSIONS
Cardiac arrest in patients with STEMI before reperfusion occurs in 7.3% of cases referred for primary angioplasty, and approximately half of these events occurred outside the health care setting. Although RCABPA was associated with significantly higher mortality rates, prognosis varied based on the location of the cardiac arrest. In-hospital RCABPA may not adversely affect prognosis, whereas out-of-hospital RCABPA, particularly when occurring outside the health care setting, was associated with significantly higher mortality rates. Improvements in regional STEMI code programs focused on early medical care and out-of-hospital CPR could reduce mortality.
FUNDING
This study received no funding.
ETHICAL CONSIDERATIONS
This study was approved by the local ethics committee, with a waiver of informed consent because it was an anonymized retrospective study. The SAGER guidelines were followed with respect to possible sex/gender bias.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
Artificial intelligence was not used in the preparation of this work.
AUTHORS’ CONTRIBUTIONS
R. López-Palop contributed to the conception and design of the study, data acquisition, analysis, and interpretation, drafting of the original project and final manuscript, and final approval. P. Carrillo Sáez collaborated in data acquisition, analysis, and interpretation, and in drafting, reviewing, and approving the manuscript. R. López-Palop López collaborated in data acquisition, analysis, and interpretation, drafting of the initial project, and review and final approval of the manuscript. M.D. Vallés García collaborated in data acquisition, analysis, and interpretation. N. Fernández Villa collaborated in drafting, reviewing, and final approval of the manuscript. J.R. Gimeno Blanes, J.M. Durán Hernández, F.J. Lacunza Ruiz, J. García de Lara, J.A. Hurtado Martínez, A. Riquelme Pérez, and E. Pinar Bermúdez collaborated in data acquisition and in review and final approval of the manuscript. D. Pascual-Figal participated in reviewing, drafting, editing, and final approval of the manuscript.
CONFLICTS OF INTEREST
None declared.
WHAT IS KNOWN ABOUT THE TOPIC?
- Most studies associate RCABPA with a higher mortality rate in patients with STEMI. In general, virtually all RCABPA episodes are analyzed as occurring outside the hospital setting, without considering possible differences associated with the location where they occur, both in terms of STEMI characteristics and prognosis.
WHAT DOES THIS STUDY ADD?
- We found significant differences in the 30-day mortality rate among patients with RCABPA based on the place of ocurrence.
- The few differences observed between patients with in-hospital RCABPA and those without RCABPA suggest a possibility for improvement in the management of this entity outside the hospital setting, following the STEMI care pathway.
REFERENCES
1. Patterson T, Perkins GD, Hassan Y, et al. Temporal Trends in Identification, Management, and Clinical Outcomes After Out-of-Hospital Cardiac Arrest:Insights From the Myocardial Ischaemia National Audit Project Database. Circ Cardiovasc Interv. 2018;11:e005346.
2. Frampton J, Ortengren AR, Zeitler EP. Arrhythmias After Acute Myocardial Infarction. Yale J Biol Med. 2023;96:83-94.
3. Karam N, Bataille S, Marijon E, et al. Incidence, Mortality, and Outcome-Predictors of Sudden Cardiac Arrest Complicating Myocardial Infarction Prior to Hospital Admission. Circ Cardiovasc Interv. 2019;12:e007081.
4. Kroupa J, Knot J, Ulman J, et al. Characteristics and Survival Determinants in Patients After Out-of-Hospital Cardiac Arrest in The Era of 24/7 Coronary Intervention Facilities. Heart Lung Circ. 2017;26:799-807.
5. Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44: 3720-3826.
6. Machado GP, Theobald AL, de Araujo GN, et al. Pre-percutaneous coronary intervention sudden cardiac arrest in ST-elevation myocardial infarction:Incidence, predictors, and related outcomes. Front Cardiovasc Med. 2023;10: 1100187.
7. Fordyce CB, Wang TY, Chen AY, et al. Long-Term Post-Discharge Risks in Older Survivors of Myocardial Infarction With and Without Out-of-Hospital Cardiac Arrest. J Am Coll Cardiol. 2016;67:1981-1990.
8. DeFilippis EM, Singh A, Gupta A, et al. Long-Term Outcomes After Out-of-Hospital Cardiac Arrest in Young Patients With Myocardial Infarction. Circulation. 2018;138:2855-2857.
9. Ando H, Sawano M, Kohsaka S, et al. Cardiac arrest and post-discharge mortality in patients with myocardial infarction:a large-scale nationwide registry analysis. Resusc Plus. 2024;18:100647.
10. Kosmidou I, Embacher M, McAndrew T, et al. Early Ventricular Tachycardia or Fibrillation in Patients With ST Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention and Impact on Mortality and Stent Thrombosis (from the Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction Trial). Am J Cardiol. 2017;120:1755-1760.
11. Deo R, Albert CM. Epidemiology and genetics of sudden cardiac death. Circulation. 2012;125:620-637.
12. Kosmopoulos M, Bartos JA, Yannopoulos D. ST-Elevation Myocardial Infarction Complicated by Out-of-Hospital Cardiac Arrest. Interv Cardiol Clin. 2021;10:359-368.
13. Rodríguez-Leor O, Cid-Álvarez AB, Pérez de Prado A, et al. Analysis of the management of ST-segment elevation myocardial infarction in Spain. Results from the ACI-SEC Infarction Code Registry. Rev Esp Cardiol. 2022;75:669-680.
14. Siudak Z, Birkemeyer R, Dziewierz A, et al. Out-of-hospital cardiac arrest in patients treated with primary PCI for STEMI. Long-term follow up data from EUROTRANSFER registry. Resuscitation. 2012;83:303-306.
15. Kragholm K, Lu D, Chiswell K, et al. Improvement in Care and Outcomes for Emergency Medical Service-Transported Patients With ST-Elevation Myocardial Infarction (STEMI) With and Without Prehospital Cardiac Arrest:A Mission:Lifeline STEMI Accelerator Study. J Am Heart Assoc. 2017;6:e005717.
16. Jabbari R, Engstrom T, Glinge C, et al. Incidence and risk factors of ventricular fibrillation before primary angioplasty in patients with first ST-elevation myocardial infarction:a nationwide study in Denmark. J Am Heart Assoc. 2015;4:e001399.
17. Andersen HR, Nielsen TT, Rasmussen K, et al. A comparison of coronary angioplasty with fibrinolytic therapy in acute myocardial infarction. N Engl J Med. 2003;349:733-742.
18. Widimsky P, Budesinsky T, Vorac D, et al. Long distance transport for primary angioplasty vs immediate thrombolysis in acute myocardial infarction. Final results of the randomized national multicentre trial —PRAGUE-2. Eur Heart J. 2003;24:94-104.
19. Becker L, Larsen MP, Eisenberg MS. Incidence of cardiac arrest during self-transport for chest pain. Ann Emerg Med. 1996;28:612-616.
20. Matta A, Philippe J, Nader V, et al. Predictors and rate of survival after Out-of-Hospital Cardiac Arrest. Curr Probl Cardiol. 2024;49:102719.
21. Desch S, Freund A, Akin I, et al. Angiography after Out-of-Hospital Cardiac Arrest without ST-Segment Elevation. N Engl J Med. 2021;385:2544-2553.
22. Gong W, Yan Y, Wang X, et al. Risk Factors for In-Hospital Cardiac Arrest in Patients With ST-Segment Elevation Myocardial Infarction. J Am Coll Cardiol. 2022;80:1788-1798.
23. Grasner JT, Herlitz J, Tjelmeland IBM, et al. European Resuscitation Council Guidelines 2021:Epidemiology of cardiac arrest in Europe. Resuscitation. 2021;161:61-79.
24. Baekgaard JS, Viereck S, Moller TP, et al. The Effects of Public Access Defibrillation on Survival After Out-of-Hospital Cardiac Arrest:A Systematic Review of Observational Studies. Circulation. 2017;136:954-965.
25. Kalarus Z, Svendsen JH, Capodanno D, et al. Cardiac arrhythmias in the emergency settings of acute coronary syndrome and revascularization:an European Heart Rhythm Association (EHRA) consensus document, endorsed by the European Association of Percutaneous Cardiovascular Interventions (EAPCI), and European Acute Cardiovascular Care Association (ACCA). Europace. 2019;21:1603-1604.
26. Perkins GD, Handley AJ, Koster RW, et al. European Resuscitation Council Guidelines for Resuscitation 2015:Section 2. Adult basic life support and automated external defibrillation. Resuscitation. 2015;95:81-99.
27. Olasveengen TM, Semeraro F, Ristagno G, et al. European Resuscitation Council Guidelines 2021:Basic Life Support. Resuscitation. 2021;161:98-114.
28. Herlitz J, Eek M, Holmberg M, Engdahl J, Holmberg S. Characteristics and outcome among patients having out of hospital cardiac arrest at home compared with elsewhere. Heart. 2002;88:579-582.
29. Wong RTM. Effect of location on out-of-hospital cardiac arrests involving older adults in Hong Kong:secondary analysis of a territory-wide cohort. Hong Kong Med J. 2023;29:142-9.
s
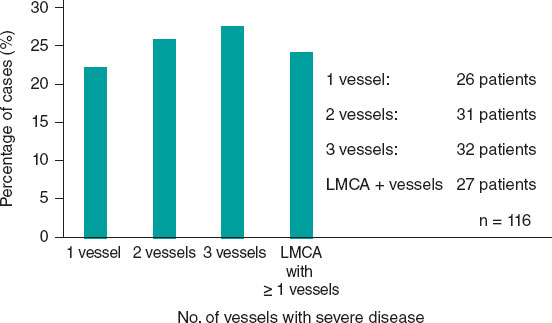
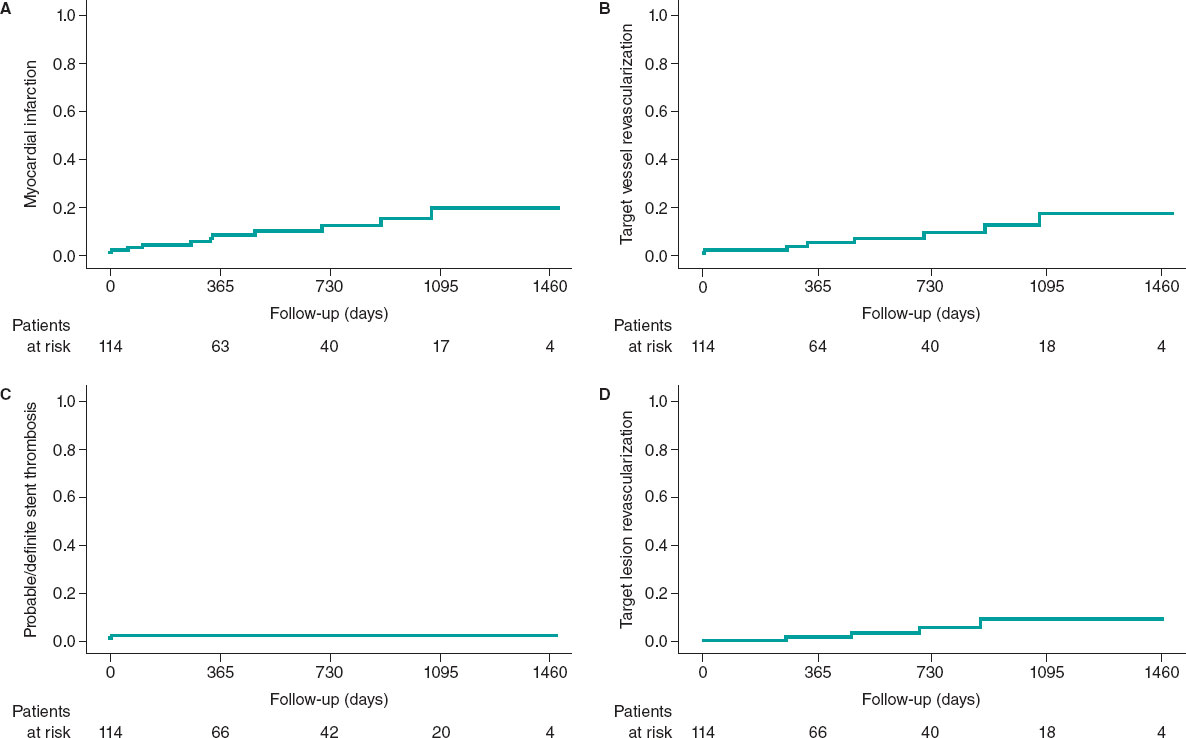
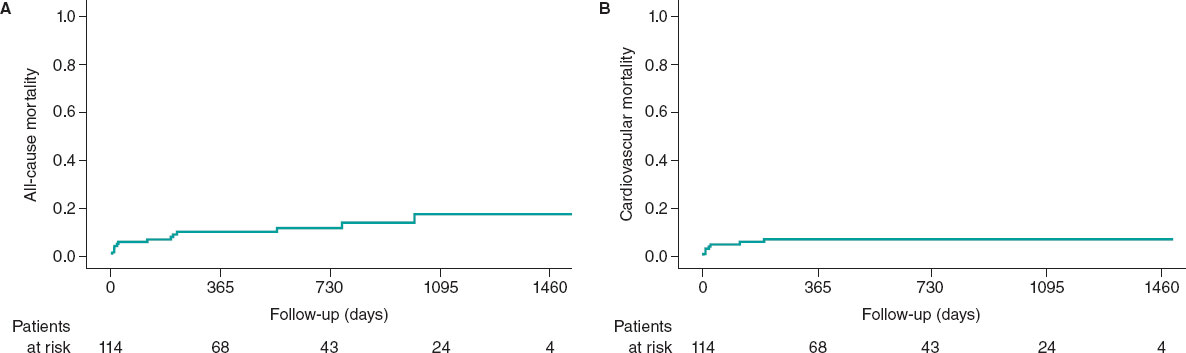
ABSTRACT
Introduction and objectives: Plaque modification techniques are important for the percutaneous treatment of severely calcified coronary lesions. The aim of this study was to retrospectively analyze patients who underwent orbital atherectomy for calcified coronary lesions at a hospital without on-site cardiac surgery.
Methods: Patients treated with orbital atherectomy between April 2021 and April 2025 were included. Procedural success was analyzed, defined as treatment of the target vessel with < 20% residual percent diameter stenosis and final TIMI grade-3 flow, as well as the composite endpoint of target vessel failure (TVF) at 12 months.
Results: A total of 116 patients were included, with a mean age of 73.24 years; 82.2% were male and 77 cases (66.4%) were admitted for acute coronary syndrome. The procedural success rate with adequate angiographic results was 98.3%. Regarding immediate complications, 1 patient died during the procedure (0.9%), 2 patients presented coronary dissection (1.7%), 3 presented coronary perforation (2.6%), and 2 experienced slow-flow or no reflow phenomena (1.7%). Mean clinical follow-up was 1.63 ± 1.2 years. The cumulative incidence rate of acute myocardial infarction was 19.3% (95%CI, 11.7-26.9); target vessel revascularization (TVR), 16.3% (95%CI, 3.7-28.9); stent thrombosis, 1.8% (95%CI, 0-4.3); and symptom-guided target lesion revascularization (TLR), 8.7% (95%CI, 0.1-16.3). All-cause mortality rate was 16.7% (95%CI,7.2–26.2), and cardiovascular mortality was 5.4% (95%CI, 1.3-9.5). Target vessel failure showed a cumulative incidence rate at the 12-month follow-up of 10% (95%CI, 3.8-16.2).
Conclusions: We present a large real-world registry of patients with calcified coronary lesions treated with orbital atherectomy (OA), showing a high procedural success rate and a low complication rate during long-term follow-up.
Keywords: Coronary artery calcification. Orbital atherectomy. Coronary plaque modification.
RESUMEN
Introducción y objetivos: Las técnicas de modificación de la placa son importantes para el tratamiento percutáneo de las lesiones coronarias con calcificación grave. El objetivo de este estudio fue analizar de forma retrospectiva los pacientes sometidos a aterectomía orbitacional en lesiones coronarias calcificadas en un hospital sin cirugía cardiaca.
Métodos: Se incluyeron pacientes tratados con aterectomía orbitacional desde abril de 2021 hasta abril de 2025. Se analizaron el éxito del procedimiento, definido como tratamiento del vaso diana con estenosis residual menor del 20% y flujo TIMI 3 final, y la variable combinada denominada fallo del vaso diana a 12 meses.
Resultados: Del total de 116 pacientes, con una edad media de 73,24 años y el 82,2% varones, 77 (66,4%) ingresaron por síndrome coronario agudo. La tasa de éxito con adecuado resultado angiográfico fue del 98,3%. Respecto a las complicaciones inmediatas: 1 paciente falleció durante el procedimiento (0,9%), 2 presentaron disección coronaria (1,7%), 3 tuvieron perforación coronaria (2,6%) y 2 mostraron reflujo lento o nulo (1,7%). El seguimiento clínico fue de 1,63 ± 1,2 años, con una incidencia acumulada de infarto agudo de miocardio del 19,3% (IC95%, 11,7-26,9), revascularización del vaso diana en el 16,3% (IC95%, 3,7-28,9), trombosis del stent en el 1,8% (IC95%, 0-4,3) y revascularización de la lesión diana guiada por síntomas en el 8,7% (IC95% 0,1-16,3). La mortalidad por todas las causas fue del 16,7% (IC95%, 7,2-26,2) y por causa cardiovascular del 5,4% (IC95%, 1,3-9,5). El fallo del vaso diana a 12 meses tuvo una tasa de incidencia acumulada a los 12 meses de seguimiento del 10% (IC95%, 3,8-16,2).
Conclusiones: Presentamos un amplio registro de la vida real de pacientes con lesiones coronarias calcificadas tratados con aterectomía orbitacional, con una alta tasa de éxito del procedimiento y una baja tasa de complicaciones en el seguimiento a largo plazo.
Palabras clave: Calcificación arterial coronaria. Aterectomía orbitacional. Modificación de placa coronaria.
Abbreviations
CAC: coronary artery calcification. OA: orbital atherectomy. TLR: target lesion revascularization. TVR: target vessel revascularization. TVF: target vessel failure.
INTRODUCTION
Coronary artery calcification (CAC) is a consequence of the progression of atherosclerotic disease, as well as an independent predictor of major adverse cardiovascular events (MACE).1,2 The etiology of CAC is multifactorial, and, among other clinical conditions, is associated with conventional cardiovascular risk factors, ethnicity, and chronic kidney disease.3-6
Patients with CAC have worse short- and long-term follow-up outcomes after percutaneous coronary intervention (PCI), including lower rates of complete revascularization and higher risks of stent underexpansion, coronary dissection, coronary perforation, and stent deformation or loss.7-10 Furthermore, CAC has been associated with a higher risk of in-stent restenosis and a greater long-term need for target lesion revascularization (TLR). In addition, approximately 50% of stents implanted in calcified lesions show asymmetric expansion, which increases the risk of stent thrombosis or in-stent restenosis.11-14 Adequate lesion preparation before stent implantation is therefore essential to reduce procedural difficulty and prevent complications. Dedicated techniques for calcified lesion modification, including calcium ablation or fracture, can improve vascular compliance. Among these techniques, orbital atherectomy (OA) has shown favorable results in the treatment of CAC and is the focus of the present study.15
METHODS
We conducted a retrospective observational study including all patients with significant calcified coronary lesions treated with OA. The aim of the study was to assess the safety and efficacy profile of OA for the treatment of patients with CAC in a hospital without on-site cardiac surgery in Spain.
The primary endpoint was procedural success, defined as treatment of the target vessel with residual percent diameter stenosis < 20% and final TIMI grade-3 flow. A composite endpoint, defined as target vessel failure (TVF) at 12 months, included cardiac death, target vessel myocardial infarction, and target vessel revascularization (TVR).
Procedure-related secondary safety endpoints included acute or subacute stent thrombosis, slow-flow or no-reflow phenomena, type C-F coronary dissections, and coronary perforations.
Clinical follow-up of the patients was performed by telephone consultation at 6 months and an in-person visit at 12 months.
The OA clinical database was approved by the Ethics Committee of the Servicio Gallego de Salud, with waiver of informed consent because of the characteristics of the study. Sex and gender variables were considered in full compliance with the SAGER guidelines.
Orbital atherectomy technique
OA is an ablative coronary technique performed using a 1.25-mm diamond-coated crown (Diamondback 360, Abbott, United States), a dedicated guidewire (ViperWire Advance, Abbott, United States), and a lubricant infused during ablation (ViperSlide, Abbott, United States). Driven by centrifugal force, the crown orbits at 2 rotational speeds (80 000 rpm or 120 000 rpm), sanding the calcium within the arterial wall and causing deep calcium fractures.16,17
Statistical analysis
Qualitative variables are expressed as number and percentage, and the quantitative ones as mean and SD. Survival curves were generated using the Kaplan-Meier method, and statistical differences in events between patients undergoing scheduled procedures and those admitted for acute coronary syndrome (ACS) were assessed using the log-rank test. A multivariate Cox regression analysis was performed to identify factors independently associated with TVF at 1 year. Variables associated with TVF in the univariable analysis at P < .1 were entered into the regression. Afterwards, the least associated variables were removed one by one using backward stepwise regression until a parsimonious model was obtained in which all variables were associated with TVF. Statistically significant difference was set at P < .05. Analyses were performed using SPSS statistical software version 17 (IBM, United States).
RESULTS
From April 2021 through April 2025, a total of 116 patients with CAC were treated with OA. Regarding the patients’ clinical charac- teristics, their mean age was 73.24 years, most were men (82.8%), and exhibited multiple classic cardiovascular risk factors. The mean left ventricular ejection fraction (LVEF) was 50.3 ± 11.9%, and up to 37.1% of patients had LVEF < 50%. Chronic kidney disease, defined as glomerular filtration rate < 60 mL/min, was present in 38.8% of patients; in 10 patients (8.6%) glomerular filtration rate was < 20 mL/min. Approximately one third of patients (30.2%) had chronic ischemic heart disease; of these, 25 (21.6%) had previously undergone revascularization by PCI and 16 (13.8%) by coronary artery bypass grafting (table 1).
Table 1. Baseline characteristics of patients treated with orbital atherectomy
| Characteristics | n = 116 |
|---|---|
| Age, years | 73.24 ± 8.23 |
| Men | 96 (82.8) |
| Height, m | 1.64 ± 0.09 |
| Weight, kg | 77.37 ± 15.59 |
| Body mass index | 28.67 ± 4.82 |
| Hypertension | 97 (83.6) |
| Dyslipidemia | 90 (77.6) |
| Diabetes mellitus | 58 (50) |
| Smoking status | |
| Nonsmokers | 62 (53.4) |
| Smokers | 13 (11.2) |
| Former smokers | 41 (35.3) |
| LVEF, % | 50.29 ± 11.93 |
| Creatinine, mg/dL | 1.41 ± 1.51 |
| GFR, mL/min/1.73 m2 | |
| < 15 | 5 (4.3) |
| 15-59 | 40 (34.5) |
| 60-89 | 53 (45.7) |
| > 90 | 18 (15.5) |
| History of coronary revascularization | 35 (30.2) |
| Previous PCI | 25 (21.6) |
| Previous CABG | 16 (13.8) |
|
CABG, coronary artery bypass grafting; GFR, glomerular filtration rate; LVEF, left ventricular ejection fraction; PCI, percutaneous coronary intervention. Data are expressed as No. (%) or mean ± SD. |
|
Regarding clinical presentation, 77 patients (66.4%) were admitted with ACS, 61 (52.1%) with non-ST-segment elevation acute coronary syndrome (NSTEACS) and 16 (13.8%) with ST-segment elevation acute coronary syndrome (STEACS). Among the latter, the artery treated with OA was the infarct-related artery in 5 cases (4.3%) (table 2). Regarding the extent of coronary artery disease, 32 patients (27.6%) had 3-vessel disease and 27 (23.3%) had left main coronary artery disease (figure 1).
Table 2. Distribution of cases based on clinical presentation
| Presentación clínica | n = 116 |
|---|---|
| Acute coronary syndrome | 77 (66.4) |
| Unstable angina | 7 (6.0) |
| NSTEACS | 54 (46.6) |
| STEACS (second-stage nonculprit lesion) | 11 (9.5) |
| STEACS (culprit lesion) | 5 (4.3) |
| Chronic ischemic heart disease | 39 (33.6) |
|
NSTEACS, non-ST-segment elevation acute coronary syndrome; STEACS, ST-segment elevation acute coronary syndrome. Data are expressed as No. (%). |
|
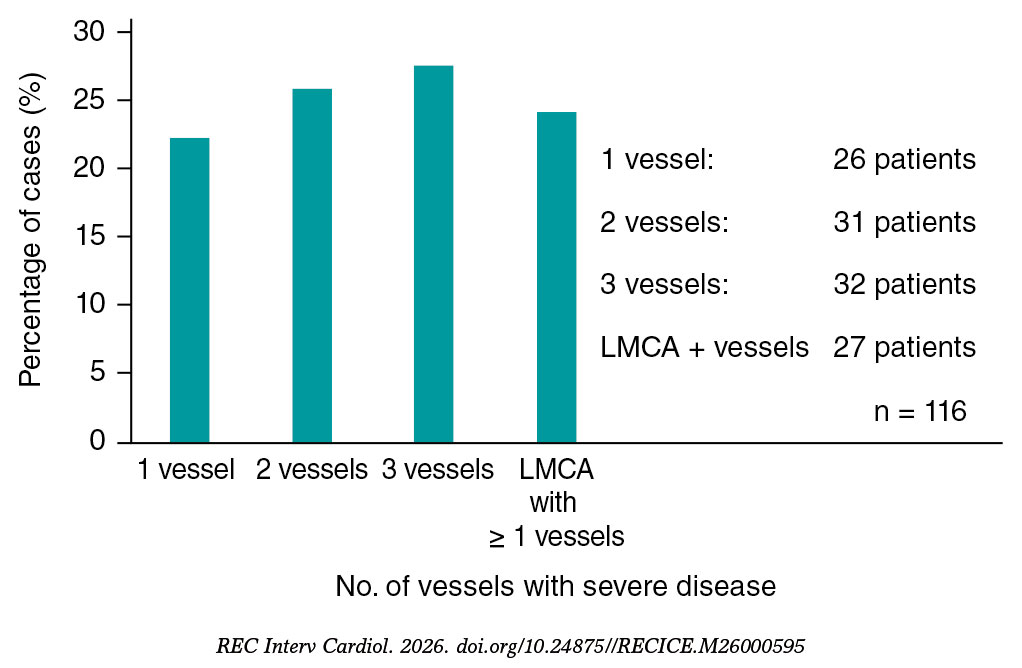
Figure 1. Distribution of cases treated with orbital atherectomy based on the number of coronary arteries with severe disease (n = 116). LMCA, left main coronary artery.
Regarding procedural characteristics, radial access was the most widely used vascular approach (77.2%). The vessel most frequently treated with OA was the left anterior descending coronary artery, in 57 cases (49.1%), followed by the right coronary artery in 34 cases (29.3%) and the left main coronary artery in 18 cases (15.5%). Intravascular imaging was used before the PCI in 42 cases (37.2%), mainly intravascular ultrasound, and after the PCI in 18 cases (15.4%). As an adjunctive plaque-modification technique to OA, a cutting balloon was used in 61 cases (52.6%), excimer laser atherectomy in 2 cases (1.7%), and intravascular lithotripsy in 1 case (0.9%). Rotational atherectomy was not used in any patient. In most patients, 1 or 2 stents were implanted (35.3% and 28.4%, respectively), with a mean stent length of 23.3 ± 6.4 mm and a mean stent diameter of 3.3 ± 0.6 mm. The mean procedure duration was 85 ± 29.5 minutes; mean fluoroscopy time, 28.7 ± 17 minutes; and mean contrast volume, 179.3 ± 65.2 mL. Procedural success rate, with an adequate angiographic result and final TIMI grade-3 flow was achieved in 98.3% of cases. Immediate complications included 1 intraprocedural death (0.9%), and in 1 case the device failed to cross the lesion (0.9%). Regarding the secondary safety endpoint, 1 patient had acute or subacute stent thrombosis (0.9%), 2 had type C-F coronary dissections (1.7%), 3 had coronary perforations (2.6%), and 2 had slow-flow or no-reflow phenomena (1.7%). Of note, all complications occurred in the subgroup of patients with ACS (table 3).
Table 3. Characteristics and materials of percutaneous coronary intervention with orbital atherectomy
| Orbital atherectomy procedure | n = 116 |
|---|---|
| Radial | 88 (77.2) |
| Femoral | 19 (16.7) |
| Other | 7 (6.1) |
| Target vessel | |
| Left anterior descending coronary artery | 57 (49.1) |
| Right coronary artery | 34 (29.3) |
| Left circumflex artery | 7 (6.0) |
| Left main coronary artery | 18 (15.5) |
| Initial TIMI grade flow | |
| 0 | 1 (0.9) |
| I | 4 (3.4) |
| II | 6 (5.2) |
| III | 105 (90.5) |
| Lesion length, mm | 36.89 ± 21.31 |
| Lesion reference diameter, mm | 3.68 ± 1.59 |
| Chronic total coronary occlusion | 1 (0.9) |
| Bifurcation | 25 (21.6) |
| Tortuosity | |
| No | 108 (93.1) |
| Mild | 4 (3.4) |
| Moderate | 3 (2.6) |
| Severe | 1 (0.9) |
| Intravascular imaging before OA | |
| IVUS | 27 (23.9) |
| OCT | 15 (13.3) |
| Intravascular imaging after OA | |
| IVUS | 9 (7.8) |
| OCT | 9 (7.8) |
| Use of other devices associated with OA | |
| Semicompliant balloon | 45 (38.8) |
| Noncompliant balloon | 63 (54.3) |
| Scoring balloon | 61 (52.6) |
| Very-high-pressure balloon | 4 (3.4) |
| Laser | 2 (1.7) |
| Intravascular lithotripsy | 1 (0.9) |
| No. of stents implanted | |
| 1 | 41 (35.3) |
| 2 | 33 (28.4) |
| 3 | 24 (20.7) |
| 4 | 9 (7.8) |
| 5 | 7 (6.0) |
| 6 | 2 (1.7) |
| Stent length, mm | 23.31 ± 6.39 |
| Stent diameter, mm | 3.34 ± 0.61 |
| Treatment with drug-coated balloon | 3 (2.6) |
| Final TIMI grade flow | |
| 0 | 1 (0.9) |
| I | 0 (0) |
| II | 2 (1.7) |
| III | 113 (98.3) |
| Procedural time, min | 85.03 ± 29.49 |
| Fluoroscopy time, min | 28.77 ± 17.03 |
| Contrast volume used, mL | 179.32 ± 65.25 |
| Procedural success | 114 (98.3) |
| Immediate complications | |
| Acute stent thrombosis | 1 (0.9) |
| Coronary dissection | 2 (1.7) |
| Coronary perforation | 3 (2.6) |
| No-flow phenomenon | 2 (1.7) |
| Intraprocedural death | 1 (0.9) |
|
IVUS, intravascular ultrasound; OA, orbital atherectomy; OCT, optical coherence tomography; TIMI, Thrombolysis in Myocardial Infarction. Data are expressed as No. (%) or mean ± SD. |
|
Mean follow-up was 1.63 ± 1.2 years, with a median of 1.48 years, Q1 of 0.53 years, and Q3 of 2.58 years. Out-of-hospital follow-up was lost in 2 cases (1.7%).
During follow-up, 11 patients had acute myocardial infarction, with a 4-year cumulative incidence rate of 19.3% (95%CI, 11.7-26.9) (figure 2A); 8 required TVR, with a 4-year cumulative incidence rate of 16.3% (95%CI, 3.7-28.9) (figure 2B); 2 had stent thrombosis, with a 4-year cumulative incidence rate of 1.8% (95%CI, 0-4.3) (figure 2C); and 4 required symptom-guided TLR, with a 4-year cumulative incidence rate of 8.7% (95%CI, 0.1-16.3) (figure 2D). There were no admissions for STEACS.
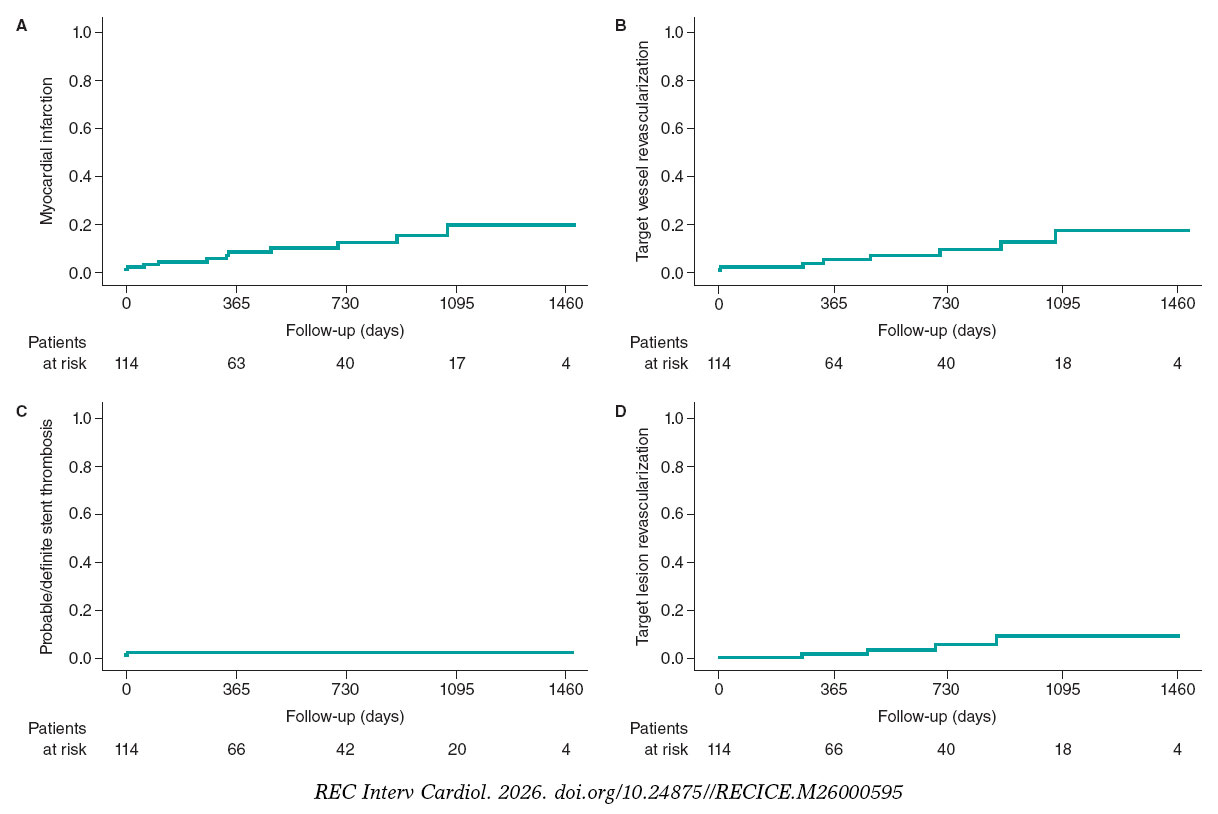
Figure 2. Cumulative incidence curves for events during follow-up: myocardial infarction (A), target vessel revascularization (B), stent thrombosis (C), and symptom-guided target lesion revascularization (D).
During follow-up, 13 patients died, with a 4-year cumulative incidence rate of 16.7% (95%CI, 7.2-26.2) (figure 3A). Cardiovascular mortality occurred in 7 cases, with a 4-year cumulative incidence rate of 5.4% (95%CI, 1.3-9.5) (figure 3B). When noncardiovascular mortality was analyzed, 3 patients died of severe infection or septic shock, 2 of cancer, and 1 of an accidental cause.
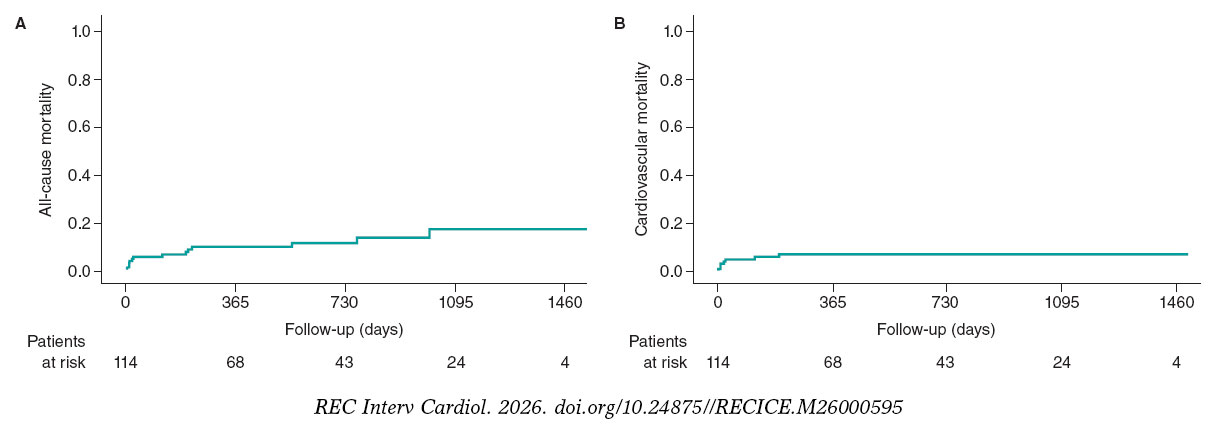
Figure 3. Kaplan-Meier mortality curves during follow-up: all-cause (A) and cardiovascular mortality (B).
The composite endpoint occurred in 10 patients, with a 12-month cumulative incidence rate of 10% (95%CI, 3.8-16.2).
Multivariable analysis showed that age < 70 years (HR, 0.35; 95%CI, 0.14-0.92), LVEF as a continuous variable (HR, 0.92; 95%CI, 0.88-0.96), and presentation as ACS (HR, 3.95; 95%CI, 1.12-13.97) were independent predictors of TVF during follow-up.
DISCUSSION
CAC is associated with an increase in adverse clinical events related to percutaneous revascularization procedures.18 OA has emerged as a safe and effective technology for the percutaneous treatment of CAC across its entire clinical spectrum. Although robust scientific evidence exists for uncrossable lesions remains limited, favorable clinical experiences with its use have been reported.19
In the registry by Lee et al.,18 stent implantation was successful in 99.1% of patients, with low rates of angiographic complications. The 30-day MACE rate, defined as a composite of cardiac death, myocardial infarction, target vessel revascularization, and stroke, was 1.7%, and the 30-day all-cause mortality rate was low, at 1.3%. Although our registry included a smaller sample, the proportions of patients with acute myocardial infarction, a past medical history of chronic ischemic heart disease, and chronic kidney disease were higher, reflecting a greater burden of high-risk clinical features. Despite this, our procedural success and immediate complication rates were comparable.
The ORBIT I study evaluated OA for the treatment of de novo calcified coronary lesions and showed sustained favorable outcomes at 5 years. Procedural success was achieved in 94% of cases. The cumulative MACE rate, defined as a composite of cardiac death, myocardial infarction, and target vessel revascularization, was 4% during hospitalization, 6% at 30 days, 8% at 6 months, 18.2% at 3 years, and 21.2% at 5 years. The rate of cardiovascular mortality was 6.1% at 2 years, 9.1% at 3 years, and 12.1% at 5 years.20-22 Of note, compared with the ORBIT I study, our registry included more than twice as many patients and a population at higher cardiovascular risk. Even so, procedural success was higher in our series (98%), and cardiovascular mortality at a mean follow-up of 1.6 years was lower than that reported in the ORBIT I beyond 2 years (5.4% vs 6.1%).
The ORBIT II study evaluated OA for de novo calcified lesions, with successful stent implantation in 97.7% and residual percent diameter stenosis < 50% in 98.6% of patients. Regarding complications, immediate and 30-day cardiovascular mortality rate was 0.2%, with low rates of severe coronary dissection, coronary perforation, slow-flow phenomenon, and acute coronary occlusion.23 These rates were similar to or lower than those reported in previous studies of rotational atherectomy, such as the ROTAXUS.24,25 The MACE rate in the ORBIT II, defined as a composite of cardiac death, myocardial infarction, and target vessel revascularization, was 16.4% at the 1-year follow-up, 19.4% at 2 years, and 23.5% at 3 years. The cardiovascular mortality at 1, 2, and 3 years was 3%, 4.3%, and 6.7%, respectively.26-28 In our registry, with a mean follow-up of 1.6 years, the rate of cardiovascular mortality was slightly higher than that reported in the ORBIT II study at 2 years (5.4% vs 4.3%). A factor that could have possibly influenced our results is that > 60% of patients in our series presented with ACS, whereas this population was excluded from the ORBIT II. In addition, the ORBIT II study excluded patients with chronic kidney disease, except those receiving dialysis, patients with serum creatinine levels > 2.5 mg/dL, and those with LVEF ≤ 25%, whereas our study included a higher-risk cardiovascular population. The ROLLER COASTR-EPIC2229 study compared rotational atherectomy, intravascular lithotripsy, and excimer laser atherectomy for the treatment of patients with CAC. The study showed that intravascular lithotripsy is noninferior to rotational atherectomy in terms of stent expansion, whereas excimer laser atherectomy did not meet the criterion for noninferiority compared with rotational atherectomy. In this context, we believe that a clinical trial including OA would be necessary and of substantial practical value to compare the optimal strategy for the treatment of CAC.
The ECLIPSE study compared OA with balloon angioplasty in severely calcified lesions and concluded that the ideal scenario for OA use would be lesions with severe superficial or nodular calcification that are nondilatable or cannot be crossed with a balloon.30 In the ECLIPSE study, 12-month TVF in the OA group was 11.5%, compared with 10% in our series, and procedural success was 86%, compared with 98% in our series. Compared with our registry, the ECLIPSE population had lower cardiovascular risk characteristics: 44% of patients had diabetes compared with 50% in our study, 24% had chronic kidney disease compared with 38.8% in our study, and the mean age was 70 years compared with 73 years in our study. In addition, the ECLIPSE study only included 13.7% of patients with ACS, including 1.3% with STEACS, compared with 66.4% with ACS (13.8% with STEACS) in our study. Thus, despite including a higher-risk population, our registry showed a higher stent implantation success rate and a slightly lower 12-month TVF rate.
Limitations
This study has several limitations. First, it is a retrospective observational registry from a single hospital; therefore, the findings may not be generalizable of other centers. Second, the OA technique is associated with a learning curve, and the results cannot be extrapolated to hospitals without experience in this technique. Third, the use of intravascular imaging was relatively low, at approximately 40% of cases, which may have led to underestimation of the severity of coronary lesion calcification. However, the use of intravascular imaging in this registry was slightly higher than that reported in previous real-world registries.
CONCLUSIONS
This large real-world registry of patients with CAC treated with OA showed a high procedural success rate and a low complication rate during long-term follow-up.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
The orbital atherectomy care database was approved by the Ethics Committee of the SERGAS of Hospital Universitario Lucus Augusti, and the requirement for informed consent was waived because of the characteristics of the study. Sex and gender variables were considered in full compliance with the SAGER guidelines.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
Artificial intelligence was not used in the preparation of the article.
AUTHORS’ CONTRIBUTIONS
J. Bayón drafted the manuscript and prepared the images. R.A. Mori-Junco reviewed the manuscript. A. Negrete-Marcolongo and A. López-Pena participated in the literature search. C. González- Juanatey performed the final review of the manuscript. All authors approved the final version.
CONFLICTS OF INTEREST
J. Bayón is a proctor for Abbott Diamondback 360 orbital atherectomy. The remaining authors declared no conflicts of interest whatsoever.
WHAT IS KNOWN ABOUT THE TOPIC?
- Orbital atherectomy is a plaque-modification technique for calcified coronary lesions, with safety and efficacy data in patients with stable coronary artery disease.
WHAT DOES THIS STUDY ADD?
- Our registry provides real-world data on a large series of patients with calcified coronary artery disease treated with orbital atherectomy, two thirds of whom presented with acute coronary syndrome. The stent implantation rate was approximately 98%, comparable to that reported in previous studies, with relatively low rates of complications and mortality during follow-up beyond 12 months.
REFERENCES
1. Mohan J, Shams P, Bhatti K, Zelster R. Coronary Artery Calcification. [Internet]. Treasure Island (FL):StatPearls Publishing;2026. Available at:https://www.ncbi.nlm.nih.gov/books/NBK519037/.
2. Onnis C, Virmani R, Kawai K, et al. Coronary Artery Calcification:Current Concepts and Clinical Implications. Circulation. 2024;149:251-266.
3. Mori H, Torii S, Kutyna M, et al. Coronary Artery Calcification and its Progression:What Does it Really Mean?JACC Cardiovasc Imaging. 2018;11:127-142.
4. Vervloet M, Cozzolino M. Vascular calcification in chronic kidney disease:different bricks in the wall?Kidney Int. 2017;91:808-817.
5. Carson AP, Steffes MW, Carr JJ, et al. Hemoglobin a1c and the progression of coronary artery calcification among adults without diabetes. Diabetes Care. 2015;38:66-71.
6. Bild DE, Detrano R, Peterson D, et al. Ethnic differences in coronary calcification:the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2005;111:1313-1320.
7. Genereux P, Madhavan MV, Mintz GS, et al. Ischemic outcomes after coronary intervention of calcified vessels in acute coronary syndromes. Pooled analysis from the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) and ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) trials. J Am Coll Cardiol. 2014;63:1845-1854.
8. Kawashima H, Serruys PW, Hara H, et al. 10-Year All-Cause Mortality Following Percutaneous or Surgical Revascularization in Patients With Heavy Calcification. JACC Cardiovasc Interv. 2022;15:193-204.
9. Kobayashi Y, Okura H, Kume T, et al. Impact of target lesion coronary calcification on stent expansion. Circ J. 2014;78:2209-2214.
10. Genereux P, Madhavan MV, Mintz GS, et al. Relation between coronary calcium and major bleeding after percutaneous coronary intervention in acute coronary syndromes (from the Acute Catheterization and Urgent Intervention Triage Strategy and Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction Trials). Am J Cardiol. 2014;113:930-935.
11. Bourantas CV, Zhang YJ, Garg S, et al. Prognostic implications of coronary calcification in patients with obstructive coronary artery disease treated by percutaneous coronary intervention:a patient-level pooled analysis of 7 contemporary stent trials. Heart. 2014;100:1158-1164.
12. Konigstein M, Madhavan MV, Ben-Yehuda O, et al. Incidence and predictors of target lesion failure in patients undergoing contemporary DES implantation-Individual patient data pooled analysis from 6 randomized controlled trials. Am Heart J. 2019;213:105-111.
13. Guedeney P, Claessen BE, Mehran R, et al. Coronary Calcification and Long-Term Outcomes According to Drug-Eluting Stent Generation. JACC Cardiovasc Interv. 2020;13:1417-1428.
14. Kawashima H, Serruys PW, Hara H, et al. 10-Year All-Cause Mortality Following Percutaneous or Surgical Revascularization in Patients With Heavy Calcification. JACC Cardiovasc Interv. 2022;15:193-204.
15. Jurado-Román A, Gómez-Menchero A, Gonzalo N, et al. Plaque modification techniques to treat calcified coronary lesions. Position paper from the ACI-SEC. REC Interv Cardiol. 2023;5:46-61.
16. Shlofmitz E, Martinsen BJ, Lee M, et al. Orbital atherectomy for the treatment of severely calcified coronary lesions:evidence, technique, and best practices. Expert Rev Med Devices. 2017;14:867-879.
17. Kirtane AJ, Ribichini F. Atherectomy for calcified plaques:orbital for most?Pros and cons. EuroIntervention. 2024;20:e627-e629.
18. Lee MS, Shlofmitz E, Kaplan B, et al. Real-World Multicenter Registry of Patients with Severe Coronary Artery Calcification Undergoing Orbital Atherectomy. J Interv Cardiol. 2016;29:357-362.
19. Bayón J, Mori-Junco RA, JuskováM, et al. Feasibility and safety of orbital atherectomy in uncrossable lesions. REC Interv Cardiol. 2025;7:269-271.
20. Parikh K, Chandra P, Choksi N, et al. Safety and feasibility of orbital atherectomy for the treatment of calcified coronary lesions:the ORBIT I trial. Catheter Cardiovasc Interv. 2013;81:1134-1139.
21. Bhatt P, Parikh P, Patel A, et al. Orbital atherectomy system in treating calcified coronary lesions:3-Year follow-up in first human use study (ORBIT I trial). Cardiovasc Revasc Med. 2014;15:204-208.
22. Bhatt P, Parikh P, Patel A, et al. Long-term safety and performance of the orbital atherectomy system for treating calcified coronary artery lesions:5-Year follow-up in the ORBIT I trial. Cardiovasc Revasc Med. 2015;16: 213-216.
23. Chambers JW, Feldman RL, Himmelstein SI, et al. Pivotal trial to evaluate the safety and efficacy of the orbital atherectomy system in treating de novo, severely calcified coronary lesions (ORBIT II). JACC Cardiovasc Interv. 2014;7:510-518.
24. Abdel-Wahab M, Richardt G, Joachim Büttner H, et al. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions:the randomized ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) trial. JACC Cardiovasc Interv. 2013;6:10-19.
25. de Waha S, Allali A, Büttner HJ, et al. Rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions:two-year clinical outcome of the randomized ROTAXUS trial. Catheter Cardiovasc Interv. 2016;87:691-700.
26. Généreux P, Lee AC, Kim CY, et al. Orbital Atherectomy for Treating De Novo Severely Calcified Coronary Narrowing (1-Year Results from the Pivotal ORBIT II Trial). Am J Cardiol. 2015;115:1685-1690.
27. Généreux P, Bettinger N, Redfors B, et al. Two-year outcomes after treatment of severely calcified coronary lesions with the orbital atherectomy system and the impact of stent types:Insight from the ORBIT II trial. Catheter Cardiovasc Interv. 2016;88:369-377.
28. Lee M, Généreux P, Shlofmitz R, et al. Orbital atherectomy for treating de novo, severely calcified coronary lesions:3-year results of the pivotal ORBIT II trial. Cardiovasc Revasc Med. 2017;18:261-264.
29. Jurado-Román A, Gómez-Menchero A, Rivero-Santana B, et al. Rotational Atherectomy, Lithotripsy, or Laser for Calcified Coronary Stenosis:The ROLLER COASTR-EPIC22 Trial. JACC Cardiovasc Interv. 2025;18: 606-618.
30. Kirtane AJ, Généreux P, Lewis B, et al. Orbital atherectomy versus balloon angioplasty before drug-eluting stent implantation in severely calcified lesions eligible for both treatment strategies (ECLIPSE):a multicentre, open-label, randomised trial. Lancet. 2025;405:1240-1251.
ABSTRACT
Introduction and objectives: The ROLLER COASTR-EPIC22 trial randomized 171 patients with moderate-to-severe calcified coronary lesions to undergo percutaneous coronary intervention with rotational atherectomy, intravascular lithotripsy, or excimer laser. This trial and its 1-year follow-up demonstrated no significant differences among the 3 arms in terms of procedural success, complications and clinical outcomes. This subanalysis aimed to describe age-related outcomes among patients undergoing percutaneous coronary intervention with plaque-modification techniques.
Methods: Of 171 patients (118 < 75 years; 53 ≥ 75 years), we compared final stent expansion by optical coherence tomography using an intention-to-treat analysis. Secondary endpoints included minimum stent area, angiographic, procedural, and clinical success, in-hospital complications, 1-year all-cause mortality, and major adverse cardiovascular events (MACE), including cardiac death, target vessel myocardial infarction, target lesion revascularization, and stent thrombosis.
Results: Baseline characteristics and treatment allocation were similar among groups. Final stent expansion was 85 ± 17.1 % in patients < 75 vs 84 ± 18.9 % in those ≥ 75 (P = .76). Minimum stent area, procedural success, and in-hospital complications were comparable. At 1 year, the ≥ 75 cohort had significantly higher MACE (11.3% vs 1.7%; P = .01) and all-cause mortality (9.4% vs 0.9%; P = .01).
Conclusions: Elderly patients achieved similar procedural outcomes as younger patients, but higher rates of MACE and all-cause mortality at 1-year follow-up.
Keywords: Rotational atherectomy. Intravascular lithotripsy. Excimer laser coronary angioplasty. Coronary calcification. Optical coherence tomography. Elderly patients.
RESUMEN
Introducción y objetivos: En el ensayo ROLLER COASTR-EPIC22 se aleatorizó a 171 pacientes con lesiones coronarias con calcificación moderada a grave para ser tratados con intervención coronaria percutánea mediante aterectomía rotacional, litotricia intravascular o láser de excímeros (ELCA). El ensayo fundamental y su seguimiento a 1 año demostraron que no había diferencias significativas entre los 3 grupos en cuanto a éxito del procedimiento, complicaciones y eventos clínicos. Este subanálisis tuvo como objetivo describir los resultados estratificados por edad en pacientes sometidos a intervención coronaria percutánea con técnicas de modificación de placa.
Métodos: En un total de 171 pacientes (118 < 75 años y 53 ≥ 75 años) se comparó la expansión final del stent mediante tomografía de coherencia óptica utilizando un análisis por intención de tratar. Los objetivos secundarios fueron el área mínima del stent, el éxito angiográfico, de procedimiento y clínico, las complicaciones intrahospitalarias, la mortalidad por cualquier causa al año y los eventos cardiovasculares adversos mayores (MACE), incluida la muerte de causa cardiovascular, el infarto de miocardio del vaso tratado, la revascularización de la lesión tratada y la trombosis del stent.
Resultados: Las características basales y la asignación del tratamiento fueron similares entre los grupos. La expansión final del stent fue del 85 ± 17,1% en los pacientes < 75 años y del 84 ± 18,9% en aquellos ≥ 75 años (p = 0,76). Al año, la cohorte ≥ 75 años presentó una tasa de MACE significativamente más alta (11,3 frente a 1,7%; p = 0,01), así como de mortalidad por todas las causas (9,4 frente a 0,85%; p = 0,01).
Conclusiones: Los pacientes ancianos lograron resultados procedimentales similares a los más jóvenes, pero con tasas más altas de MACE y de mortalidad por cualquier causa en el seguimiento a 1 año.
Palabras clave: Aterectomía rotacional. Litotricia intravascular. Aterectomía coronaria con láser de excímeros. Calcificación coronaria. Tomografía de coherencia óptica. Pacientes ancianos.
Abbreviations
ELCA: excimer laser coronary atherectomy. IVL: intravascular lithotripsy. MACE: major adverse cardiovascular events. OCT: optical coherence tomography. PCI: percutaneous coronary intervention. PMT: plaque modification technique.
INTRODUCTION
Coronary artery calcification constitutes a major challenge during percutaneous coronary intervention (PCI), as it reduces procedural success and increases the risk of complications. It limits optimal stent expansion, which predicts restenosis, stent thrombosis, and the need of target lesion revascularization.1-3 Several plaque modification techniques (PMT) have been developed to improve clinical outcomes in this setting. Rotational atherectomy has long been considered the standard approach for managing resistant calcified lesions. However, the development of newer technologies such as intravascular lithotripsy (IVL), together with increasing interest in excimer laser coronary atherectomy (ELCA), has expanded the range of available therapeutic options.4-7
The ROLLER COASTR-EPIC22 trial was the first randomized trial comparing rotational atherectomy, IVL, and ELCA in patients with moderate-to-severe calcified coronary lesions. Procedural success, safety and 1-year clinical outcomes were similar across all techniques.8
Elderly patients (≥ 75 years), who often present with increased comorbidity and complex coronary anatomy, remain underrepresented in clinical trials and may experience higher procedural risk and higher long-term mortality.9 In this post-hoc analysis of the ROLLER COASTR-EPIC22 trial, we assessed the impact of age on outcomes of PCI for moderately to severely calcified coronary stenosis treated with contemporary plaque-modification techniques. Specifically, we compared stent expansion, procedural success, in-hospital complications and 1-year clinical outcomes between patients < 75 and ≥ 75 years of age. Exploratory analyses of individual PMT within age strata were performed but were not powered for formal between-technique comparisons.
METHODS
Study design and population
ROLLER COASTR-EPIC22 trial was a multicenter randomized trial (NCT04181268) conducted at 8 high-volume centers in Spain.10 Complete inclusion and exclusion criteria, as well as the randomization process and procedural details, have been previously described.11 Briefly, eligible patients had moderate-to-severe calcification estimated by coronary angiography, and culprit lesions of ST-segment elevation acute coronary syndromes were excluded. All patients gave therir prior written informed consent before participation. Included patients were randomized 1:1:1 to rotational atherectomy, IVL, or ELCA from July 2019 through December 2023.10,11
Stratification and endpoints
This study is a post-hoc age-stratified analysis. Patients were stratified by age in 2 groups: < 75 years (n = 118) and ≥ 75 years (n = 53). Comparisons within age subgroups are exploratory and should be viewed as descriptive rather than confirmatory.
The primary endpoint was stent expansion assessed by optical coherence tomography (OCT), calculated as minimal stent area divided by the mean reference lumen area, analyzed according to the intention-to-treat principle.11
The secondary endpoints included angiographic success (final Thrombolysis in Myocardial Infarction grade-3 flow, assessed at both < 20% and < 30% residual stenosis), procedural success (angiographic success without major perioperative complications), clinical success (procedural success without in-hospital major adverse cardiovascular events [MACE]), device success (defined as achievement of adequate plaque modification with the initial device without the need for a second advanced PMT), minimal stent area by OCT, and in-hospital complications.11
Major perioperative complications were defined as death, perforation, flow-limiting dissection, abrupt vessel closure, or stent thrombosis. MACE was defined as the composite of cardiac death, target vessel myocardial infarction, target lesion revascularization, and definite/probable stent thrombosis.11
Procedures and imaging
Procedures have been previously described and followed latest European guideline recommendations.10 Pre- and post-PMT OCT imaging were recommended to characterize the lesion. Predilation with low-profile balloons was permitted to allow OCT catheter crossing prior to PMT. After plaque modification, drug-eluting stent implantation and optimization were performed, followed by the final mandatory OCT. OCT image acquisition and stent optimization protocols have been previously described.11
Rotational atherectomy, IVL and ELCA were performed according to current recommendations and device instructions, as previously described.6,12,13
Statistical analysis
The principal analyses were conducted in the intention-to-treat population. An additional analysis was performed in an as-treated fashion, based on the last PMT used. Continuous variables are expressed as mean ± standard deviation if normally distributed or median [IQR] otherwise, and categorical variables as counts and percentages. Between-group comparisons used the chi-square test or Fisher’s exact test for categorical variables and Student t test or Mann–Whitney U test for continuous variables. Noninferiority of IVL and ELCA vs rotational atherectomy for stent expansion was tested with a 1-sided t test against a prespecified noninferiority margin of −7%. This margin was adopted from the pivotal ROLLER COASTR-EPIC22 trial and was defined a priori by the steering committee as the smallest absolute difference in stent expansion considered clinically relevant, based on previous studies.11,14,15 Statistical significance was set at P < .05.10,11
Because this was an exploratory, post-hoc age-stratified analysis with a relatively small sample size in the elderly subgroup, no formal adjustment for multiple comparisons was applied. Given the large number of comparisons (2 age groups, 3 PMT and several procedural and clinical endpoints), conservative corrections such as Bonferroni would have markedly reduced statistical power and increased the risk of type II error. Instead, all effect estimates, 95% confidence intervals and exact P values are reported to allow readers to interpret the results with appropriate caution, and all subgroup findings are considered hypothesis-generating rather than confirmatory.
Given the low number of events, survival was assessed with Kaplan–Meier curves and log-rank tests. All statistical analyses were conducted using R version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Patient allocation and baseline characteristics
A total of 171 patients were enrolled, of whom 118 (69%) were younger than 75 years (mean age, 66.8 ± 6.4 years; 79.5% male) and 53 (31%) were aged ≥ 75 years (mean age, 79.7 ± 3.7 years; 73.6% male). In patients < 75 years (n = 118), age was 66.8 ± 6.4 years (median, 68; IQR 64–71; range, 44–74), whereas in those ≥ 75 years (n = 53) age was 79.7 ± 3.7 years (median, 79; IQR 77–82; range, 75–89) (table S1 and figure S1).
Baseline clinical characteristics were broadly comparable between age groups, including rates of diabetes, hypertension, and prior revascularization. However, older patients had a lower prevalence of active smoking (15.1% vs 33.6%; P = .02), lower body mass index (27.0 ± 3.8 vs 28.5 ± 4.3 kg/m²; P = .04), and lower haemoglobin (12.8 ± 1.8 vs 13.5 ± 2.0 g/L; P = .04). No significant differences were observed in left ventricular ejection fraction, basal creatinine or clinical presentation, although elderly patients showed a trend towards a more frequent presentation as acute coronary syndrome (table 1).
Table 1. Baseline clinical characteristics
| Variable | < 75 years (n = 118) | ≥ 75 years (n = 53) | P |
|---|---|---|---|
| Age | 66.8 ± 6.4 | 79.7 ± 3.7 | < .01 |
| Male | 93 (79.5) | 39 (73.6) | .51 |
| BMI (kg/m2) | 28.5 ± 4.3 | 27.0 ± 3.8 | .04 |
| Current smoker | 39 (33.1) | 8 (15.1) | .02 |
| Diabetes mellitus | 57 (48.3) | 27 (50.9) | 92 |
| Hypertension | 93 (78.8) | 43 (81.1) | .97 |
| Dyslipidemia | 86 (72.9) | 40 (75.5) | .93 |
| Prior PCI | 40 (33.9) | 16 (30.2) | .73 |
| Prior CABG | 4 (3.4) | 2 (3.8) | 1 |
| LVEF | 54.8 ± 10.9 | 54.9 ± 10.7 | .96 |
| Serum creatinine (mg/dL) | 1.2 ± 1.2 | 1.2 ± 1.0 | .95 |
| Hemoglobin (g/L) | 13.5 ± 2.0 | 12.8 ± 1.8 | .04 |
| Clinical presentation | .08 | ||
| CCS | 77 (65.3) | 29 (54.7) | |
| Unstable angina | 12 (10.2) | 10 (18.8) | |
| NSTEMI | 18 (15.2) | 12 (22.6) | |
| STEMI | 8 (6.8) | 0 (0) | |
|
BMI, body mass index; CABG, coronary artery bypass graft; CCS, chronic coronary syndrome; LVEF, left ventricular ejection fraction; NSTEMI, non-ST-segment elevation myocardial infarction; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction. Data are expressed as No. (%) or mean ± standard deviation. All angiographic parameters were measured at a central core laboratory blinded to the treatment arm. |
|||
Angiographic and procedural data
Target vessels and lesion characteristics, including severity and length of calcification, were comparable across age strata and treatment arms. Most procedures were performed via radial access (> 80%), and treatment allocation was well balanced across age strata. Procedural duration, sheath size, and use of ad hoc PCI did not differ by age. Angiographic and procedural details are summarized in table S2.
OCT findings
The optional pre-plaque modification OCT was performed in 39 of 118 patients < 75 years (33.1%) and in 20 of 53 patients ≥ 75 years (37.7%), with no significant difference between age groups (P = .67).
Final OCT runs were obtained in more than 75% of patients. OCT parameters of calcification, assessed by an independent central core laboratory, consistently demonstrated a heavy calcium burden across all cases, with no significant differences between age groups or treatment modalities. OCT findings are presented in table S3.
Primary and secondary endpoints
No significant differences in terms of final stent expansion, minimal stent area, or final residual stenosis were observed between groups (table 2, figure S2). Angiographic, procedural, and clinical success rates exceeded 90% (considering < 30% residual percent diameter stenosis) in both age groups and did not differ by technique (table 2, figure 1).
Table 2. Procedural outcomes and complications
| Procedural outcomes | < 75 years (n = 118) | ≥ 75 years (n = 53) | P |
|---|---|---|---|
| Success considering < 30% residual percent diameter stenosis | |||
| Angiographic | 112 (94.9%) | 49 (92.5%) | .78 |
| Procedural | 108 (91.5%) | 49 (92.5%) | 1.00 |
| Clinical | 108 (91.5%) | 48 (90.6%) | 1.00 |
| Success considering < 20% residual percent diameter stenosis | |||
| Angiographic | 87 (73.7) | 42 (79.2) | .56 |
| Procedural | 83 (70.3) | 42 (79.2) | .30 |
| Clinical | 83 (70.3) | 41 (77.4) | .44 |
| Final TIMI grade flow | .63 | ||
| 0 | 1 (0.8) | 0 | |
| 1 | 0 | 0 | |
| 2 | 1 (0.8) | 0 | |
| 3 | 116 (98.3) | 53 (100) | |
| Final diameter diameter stenosis (%) | 14.7 ± 11.5 | 12.8 ± 10.9 | .30 |
| Final SE (%) | 85.0 ± 17.1 | 84.0 ± 18.9 | .76 |
| Severe procedural complications | 4 (3.4) | 0 (0) | .42 |
| Death | 0 (0) | 0 (0) | – |
| Perforation | 4 (3.4) | 0 (0) | .42 |
| Flow-limiting dissection | 0 (0) | 0 (0) | – |
| Abrupt vessel closure | 0 (0) | 0 (0) | – |
| Stent thrombosis | 0 (0) | 0 (0) | – |
| Dissection | |||
| A | 3 (2.5) | 1 (1-9) | 1.00 |
| B | 0 (0) | 2 (3.8) | .18 |
| D | 1 (0.8) | 1 (1.9) | 1.00 |
| Slow flow/No-reflow | 1 (0.8) | 1 (1.9) | 1.00 |
| Side branch occlusion | 0 (0) | 1 (1.9) | .68 |
| Complications during admission | 0 (0) | 2 (3.8) | .18 |
| Mortality | 0 (0) | 1 (1.9) | .68 |
| Cardiac death | 0 (0) | 1 (1.9) | .68 |
| Target lesion revascularization | 0 (0) | 0 (0) | – |
| Stent thrombosis | 0 (0) | 0 (0) | – |
| Stroke | 0 (0) | 0 (0) | – |
| BARC grade ≥ 3b bleeding | 0 (0) | 1 (1.9) | .68 |
|
BARC, Bleeding Academic Research Consortium; SE, stent expansion; TIMI, Thrombolysis in Myocardial Infarction. Data are expressed as No. (%) or mean ± standard deviation. Severe procedural complications were defined as death, perforation, flow-limiting dissection, abrupt vessel closure or stent thrombosis. |
|||
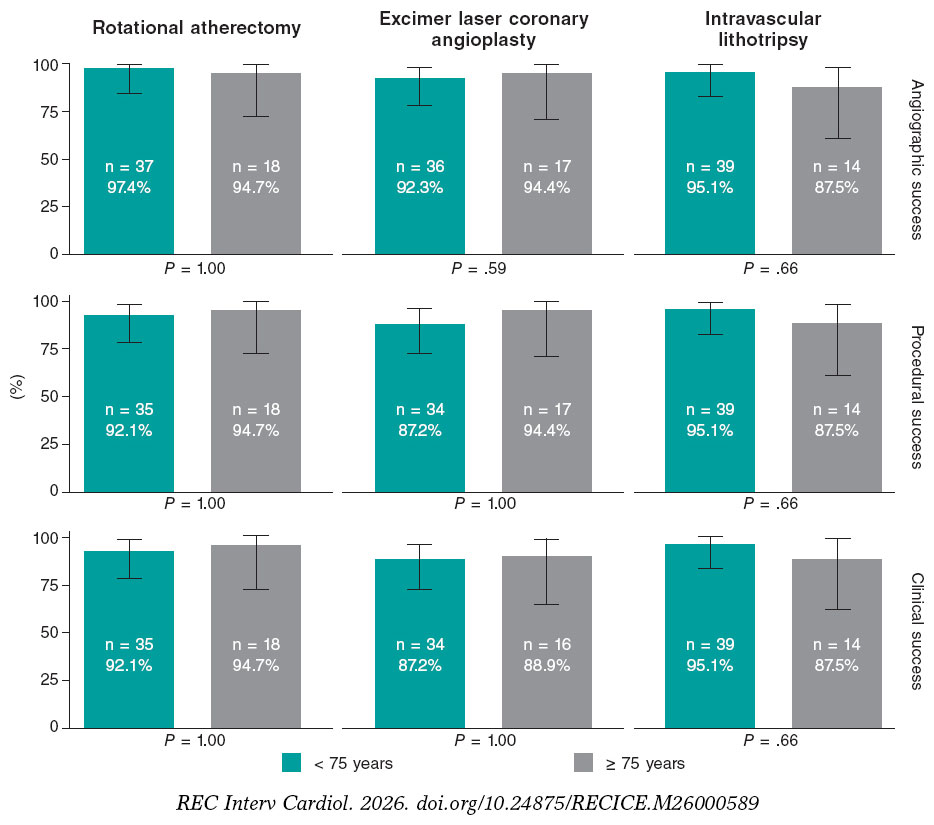
Figure 1. Angiographic, procedural, and clinical success of each technique. Angiographic success defined as final Thrombolysis in Myocardial Infarction grade-3 flow with < 30% residual percent diameter stenosis. Procedural success was considered angiographic success without major perioperative complications. Clinical success was defined as procedural success without in-hospital major adverse cardiovascular events.
Among patients ≥ 75 years, mean stent expansion values were broadly similar across the 3 PMT, and no statistically significant between-technique differences were detected; however, 95%CI, were wide because of the small sample size in each subgroup (table S3). Exploratory analyses of mean differences in stent expansion between techniques yielded results that were directionally consistent with the overall ROLLER COASTR-EPIC22 trial but were clearly underpowered in this age-stratified cohort and should be interpreted as hypothesis-generating only (figure 2 and table S4).
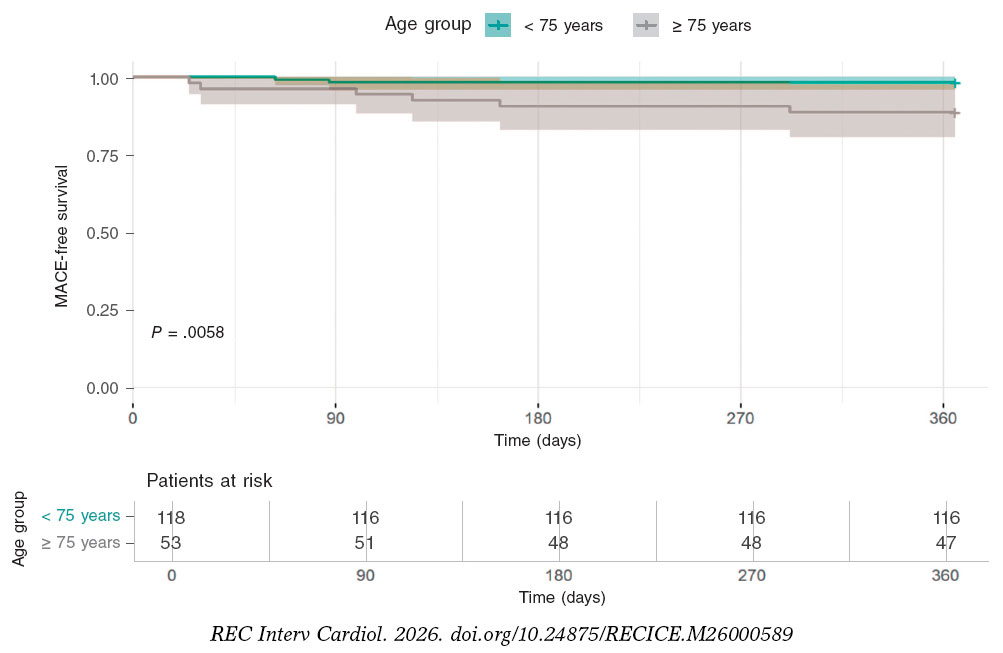
Figure 2. One-year MACE-free survival. Kaplan-Meier curves showing 1-year freedom from MACE in the intention to-treat population. MACE was defined as the composide endpoing of cardiac death, target vessel myocardial infarction, target lesion revascularization, stent thrombosis. MACE, major adverse cardiovascular events.
Overall, device success rate was 88.3% overall and was similar by age: < 75 (89.7%) vs ≥ 75 years (85.7%); P = .76. The causes of crossover differed by device: as in the pivotal trial, in the rotational atherectomy arm most crossovers were prompted by inadequate lesion dilation after atherectomy, whereas in the IVL and ELCA arms the primary driver was inability to cross the lesion with the dedicated balloon or laser catheter (figure S3 and table S5). In-hospital complication rates (perforations, bleeding, death) were low and balanced by age (table 2).
In 1-year follow-up (table 3, figure 2), patients aged ≥ 75 years had a markedly higher rate of MACE than those < 75 years (11.3% vs 1.7%; P = .01). All-cause mortality was also greater in the older cohort (9.4% vs 0.9%; P = .01).
Table 3. One-year event rates
| Event | < 75 years | ≥ 75 years | P |
|---|---|---|---|
| MACE | 2 (1.7%) | 6 (11.3%) | .01 |
| All-cause mortality | 1 (0.9%) | 5 (9.4%) | .01 |
| Cardiac death | 0 (0.00%) | 2 (3.8%) | .10 |
| TVMI | 0 (0.00%) | 2 (3.8%) | .10 |
| TLR | 1 (0.9%) | 2 (3.8%) | .23 |
| TVR | 2 (1.7%) | 4 (7.6%) | .08 |
| ST | 0 (0.00%) | 2 (3.8%) | .10 |
|
MACE, major adverse cardiovascular events; ST, stent thrombosis; TLR, target lesion revascularization; TVMI, target vessel myocardial infarction; TVR, target vessel revascularization. Data are expressed as No. (%). MACE was defined as a composite endpoint of cardiac death, target vessel acute myocardial infarction, target lesion revascularization, and stent thrombosis. P values have been calculated as log-rank p-values from Kaplan-Meier comparisons. |
|||
Although less frequent, each individual component of the composite endpoint was numerically higher in patients ≥ 75 years without reaching statistical significance: cardiac death (11.3% vs 0%; P = .1), target vessel myocardial infarction (3.8% vs 0%; P = .1), target lesion revascularization (3.8% vs 0.8%; P = .23), target vessel revascularization (7.5% vs 1.7%; P = .08) and stent thrombosis (3.8% vs 0%; P = .10).
In a multivariable logistic regression including age ≥ 75 years, anemia, acute coronary syndrome presentation and renal dysfunction, age ≥ 75 years remained the strongest predictor of 1-year endpoints. For MACE, age ≥ 75 years was associated with an adjusted OR, 7.4 (95%CI, 1.5–53.9; P = .02), whereas none of the other covariates showed a clear independent association with the composite endpoint. For all-cause mortality, the adjusted OR for age ≥ 75 years was 10.7 (95%CI, 1.5–218.7; P = .04) and none of the other covariates demonstrated a clear independent effect. These findings are presented in table S6 and figure S4.
DISCUSSION
In this post-hoc age-stratified analysis of the ROLLER COASTR-EPIC22 trial and its 1-year follow-up, we observed that the overall safety and efficacy of PMT appeared consistent across age groups. However, at 1 year older patients experienced significantly higher rates of MACE (11.3% vs 1.7%; P = .01) and all-cause mortality (9.4% vs 0.9%; P = .01) despite comparable in-hospital complication rates.
After adjustment for anemia, acute coronary syndrome presentation, and renal dysfunction, age ≥ 75 years remained associated with higher adjusted odds of both 1-year MACE and all-cause mortality. None of the adjustment covariates demonstrated a clear independent effect, suggesting that unmeasured factors closely related to aging, such as frailty, are likely to account for much of the excess risk observed in older patients.
Randomized evidence directly comparing contemporary PMT in calcified coronary disease remains scarce. The ROLLER COASTR-EPIC22 trial was the first trial to randomize patients among rotational atherectomy, IVL, and ELCA.10 Previous device-specific studies and registries have demonstrated the feasibility of each technique, but none had evaluated all 3 within a single randomized framework.16-18
Coronary calcium is independently associated with long-term mortality risk, and age is not only a key predictor of coronary calcification but also an independent predictor of MACE, regardless of calcium burden.19 Nevertheless, elderly patients are underrepresented in PMT studies, leaving limited evidence to guide the choice of the optimal PMT strategy. Regarding rotational atherectomy, there is little evidence in elderly patients, but retrospective data suggests similar success and in-hospital complication rates compared with younger individuals.20 Similarly, the BENELUX-IVL prospective registry demonstrated the safety profile and technical success of IVL in patients aged ≥ 80 years.21 ELCA, however, has not been specifically studied in the elderly population.
Selecting elderly patients for revascularization requires balancing benefits and risks. Comorbidities (anemia, chronic kidney disease, acute coronary syndrome) and limitations in physiological reserve increase complexity and may reduce revascularization uptake in this population.22,23 Our findings support that chronological age alone should not preclude revascularization, as PMT appeared effective and safe when performed by experienced operators, regardless of age. These results, however, should be interpreted cautiously given the limited sample size and exploratory, post-hoc nature of the age-stratified analysis. The importance of operator experience in PMT for complex scenarios has been highlighted by the CRATER trial program, which evaluated rotational atherectomy in patients with chronic kidney disease and severely calcified lesions and reported high procedural success but also substantial perioperative and long-term event rates, largely reflecting the extreme baseline risk of this population.24,25
Notably, our analysis suggests no excess perioperative complications in older adults, although the study was not powered for subgroup comparisons and 95%CI, were wide, particularly in the elderly ELCA subgroup. We advocate for meticulous patient selection, based on preoperative risks and comorbidities; however, PMT should be used when necessary for adequate lesion preparation to maximize stent expansion and avoid suboptimal implantation, a known driver of adverse clinical events.
In our cohort, elderly patients achieved similar procedural success, stent expansion and in-hospital safety outcomes vs younger patients yet experienced a markedly higher rate of 1-year MACE and all- cause mortality. This pattern is consistent with the e-ULTIMASTER and MOSCA FRAIL trials, in which frailty, rather than age per se, emerged as the main determinant of adverse outcomes in older adults undergoing PCI.26,27 Taken together, these data support that revascularization decisions in elderly patients should not rely exclusively on chronological age, but should incorporate assessment of frailty, functional capacity and comorbidity to individualize the benefit–risk balance of an invasive strategy. The lack of formal frailty indices in our study therefore represents an important limitation. Future trials in elderly patients undergoing complex PCI should prospectively integrate standardized frailty tools to better guide patient selection and tailor treatment.
In the subset of patients with available baseline OCT, we did not observe relevant differences in calcium burden or morphology nor in angiographic severity or extent of disease, between patients < 75 and ≥ 75 years. This suggests that the underlying calcific process is biologically similar across age groups, even if it becomes clinically manifest at different ages, and is consistent with the comparable postoperative stent expansion and minimal stent area observed in both strata. Nevertheless, despite similar stent optimization, the ≥ 75-year group showed a numerically higher rate of definite/probable stent thrombosis and cardiovascular death at 1 year (3.8%), which is clinically meaningful in this context. As underexpansion alone is unlikely to fully explain these events, age-related factors such as greater comorbidity and frailty, a prothrombotic milieu and a reduced myocardial reserve, may have contributed to the excess risk observed in older patients, even after apparently adequate angiographic and OCT-guided results.
Contemporary randomized PMT trials (such as ROTAXUS, PREPARE-CALC, ISAR-CALC 2 or ECLIPSE ) enrolled patients with a mean age around 70 years, but none of them reported age-specific outcomes for those ≥ 75 years, limiting its applicability to older populations.28-32 Our analysis contributes to fill this knowledge gap suggesting procedural success and safety of PMT in the elderly. However, due to the nonprespecified nature of our analysis, these results should be considered hypothesis-generating. Future randomized studies should integrate objective frailty and functional measures and include sufficient follow-up to assess both procedural and long-term outcomes in this growing population.
Study limitations
This study has several limitations to consider. First, it was a post-hoc analysis and the findings should be regarded as hypothesis- generating rather than definitive. Second, because age stratification was not prespecified in the trial design, the study was not statistically powered for subgroup comparisons based on age, and the relatively small number of patients aged ≥ 75 years may limit the generalizability of the results.
Third, frailty status and functional capacity –both known to strongly influence outcomes in elderly patients– were not assessed, which limits the clinical granularity of the findings.
Fourth, the study was not powered to detect differences in clinical events and results should be interpreted cautiously due to the limited number of events.
Fifth, posttreatment OCT images were not available in slightly more than 20% of patients, with a higher proportion of missing studies in the ≥ 75-year group. This pattern of missing data may introduce selection bias, as patients without analyzable postoperative OCT could differ systematically from those with complete imaging, potentially limiting the internal validity and generalizability of the stent expansion findings, particularly in the elderly subgroup.
Sixth, randomization was based on angiographic calcification alone, without prior evaluation of lesion crossability or balloon dilatability, which could have impacted the need for secondary PMT. Indeed, some patients required a second PMT, complicating the interpretation of the intention-to-treat analysis, although complementary as-treated and per-protocol analyses were performed to mitigate this limitation. Additionally, not all patients underwent complete pre- and post-PCI OCT, which may have influenced both device selection and the assessment of stent expansion metrics.
Seventh, the 1-year follow-up provides only mid-term outcome data and does not address long-term endpoints such as stent durability or the need for target lesion revascularization. Lastly, the trial was conducted in high-volume centres by experienced operators, which may limit the applicability of these results to lower-volume settings or institutions with less experience in complex PCI and PMT.
CONCLUSIONS
In this age-stratified analysis of the ROLLER COASTR-EPIC22 trial, elderly patients undergoing PCI for calcified coronary lesions achieved similar procedural success, stent expansion, and in-hospital safety outcomes as younger patients. However, patients aged ≥ 75 years experienced significantly higher rates of MACE and all-cause mortality at 1 year (figure 3).
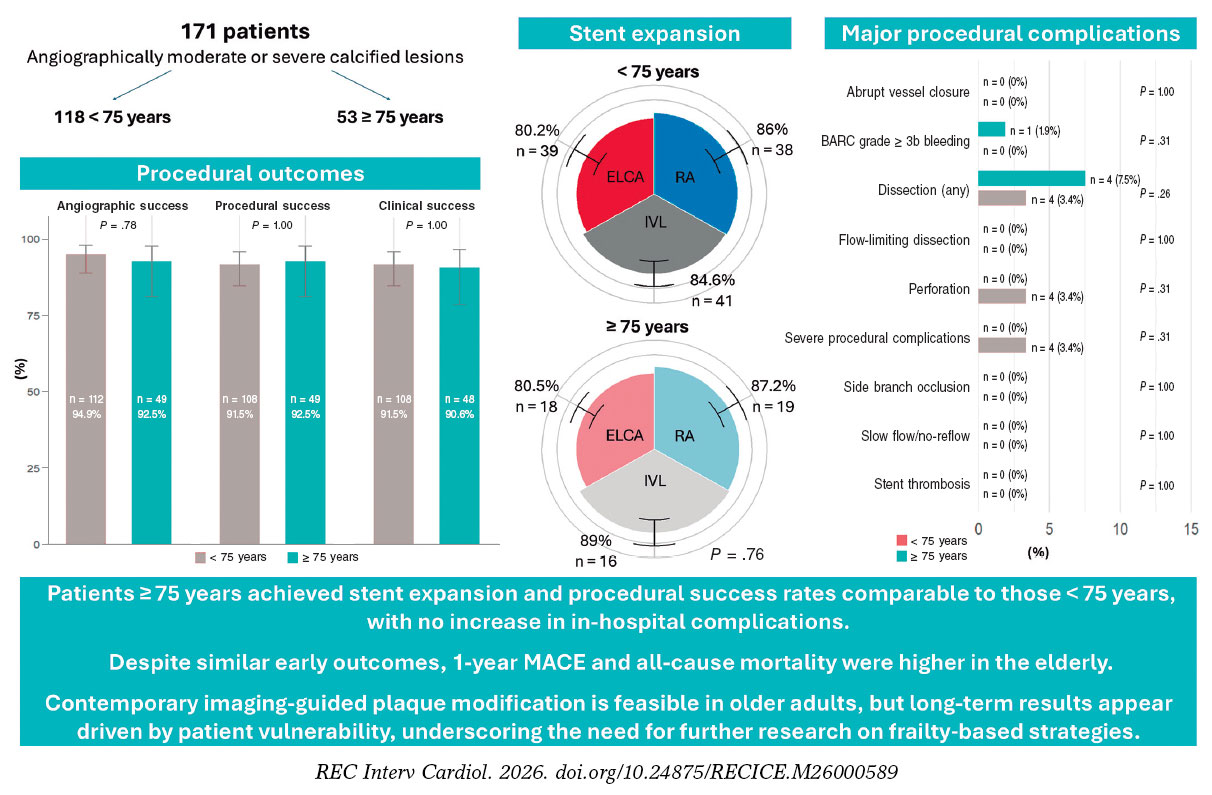
Figure 3. Central illustration. Senior-ROLLER: age-related outcomes of plaque modification in coronary stenosis. Procedural success, stent expansion, and major procedural complications were similar in patients < 75 and those ≥ 75 years; however, the 1-year MACE and all-cause mortality rates were higher in the elderly, which highlights the need for careful patient selection and individualized treatment strategies. BARC, Bleeding Academic Research Consortium; ELCA, excimer laser coronary atherectomy; IVL, intravascular lithotripsy; MACE, major adverse cardiovascular events; RA, rotational atherectomy.
DATA AVAILABILITY
The data that support the findings of this study are available from the corresponding author upon reasonable request.
FUNDING
The ROLLER COASTR-EPIC22 trial was supported by an unrestricted grant from Fundación EPIC.
ETHICAL CONSIDERATIONS
This is a subanalysis of the ROLLER COASTR-EPIC22 trial (NCT04181268), which was approved by the institutional ethics committee at each participant center and conducted in full compliance with the principles outlined in the Declaration of Helsinki. The authors confirm that written informed consent was obtained from all participants before enrolment.
Sex and gender aspects were considered according to the Sex and Gender Equity in Research (SAGER) guidelines.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
Artificial intelligence was not used in this manuscript.
AUTHORS’ CONTRIBUTIONS
J. Vila-García and M. Basile contributed equally to the manuscript and share first authorship. J. Vila-García and M. Basile contributed equally to several phases of the study, including conception and design, and acquisition, analysis and interpretation of the data. In addition, J. Vila-García contributed to the drafting of the original manuscript and to the writing and revision of the final version, while M. Basile was primarily responsible for the critical review of the article. A. Gómez-Menchero, J. Caballero-Borrego, B. Rivero- Santana, G. Galeote, I.J. Amat-Santos, S. Jiménez-Valero, G. Miñana, S. Ojeda, A. Gonzálvez-García, D. Tébar-Márquez, S. Camacho- Freire, J. Zubiaur, R. Ocaranza-Sánchez and A. Domínguez participated in the acquisition of the data and in the review and editing of the final text. A. Jurado-Román and R. Moreno participated in the conception and design of the study, in the acquisition, analysis and interpretation of the data, in the drafting, review, editing and approval of the final manuscript, and in the overall supervision of the project. A. Jurado-Román was responsible for funding and administration. All authors approved the final version of the manuscript.
CONFLICTS OF INTEREST
S. Ojeda and R. Moreno are associate editors of REC: Interventional Cardiology; the journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. A. Jurado-Román is a proctor for Abbott, Boston Scientific, World Medica, and Philips; has received consulting fees from Boston Scientific and Philips; and has received speaker fees from Abbott, Boston Scientific, Shockwave Medical, Philips, and World Medica. S. Ojeda has received consulting fees from Medtronic and Edwards Lifesciences; and has received speaker fees from Abbott, Boston Scientific, Philips, and World Medical. All other authors report no relationships relevant to the contents of this article to disclose.
ACKNOWLEDGMENTS
We thank the ROLLER COASTR-EPIC22 trial investigators, coordinators, and participating patients for their dedication.
SUPPLEMENTARY DATA
WHAT IS KNOWN ABOUT THE TOPIC?
- Contemporary PMT (rotational atherectomy, IVL, and ELCA) have demonstrated efficacy in managing heavily calcified coronary lesions across all age groups. However, elderly patients remain significantly underrepresented in randomized controlled trials of interventional cardiology, limiting the evidence base for clinical decision-making in this growing population. The ROLLER COASTR-EPIC22 Trial trial was the first randomized study to directly compare all 3 main PMT in a single cohort, establishing their procedural safety and efficacy profile in younger patients. Prior data suggest that age alone may not be an absolute contraindication to contemporary interventional strategies; however, age-stratified outcomes for elderly patients specifically remain sparse in the literature.
WHAT DOES THIS STUDY ADD?
- This analysis provides the first randomized age-stratified evaluation of PMT. Our findings demonstrate that procedural success and stent expansion are comparable between elderly and younger cohorts, with no excess in-hospital complications in older adults. Despite similar early procedural outcomes, elderly patients experienced significantly higher rates of MACE and all-cause mortality at 1-year follow-up, highlighting the importance of patient vulnerability and frailty over chronological age alone. These results suggest that age should not be an exclusion criterion for contemporary PMT when clinically indicated, but rather that individualized risk assessment and targeted follow-up strategies are essential for optimizing outcomes in elderly populations undergoing complex percutaneous coronary intervention.
REFERENCES
1. Généreux P, Madhavan MV, Mintz GS, et al. Ischemic outcomes after coronary intervention of calcified vessels in acute coronary syndromes: Pooled analysis from the HORIZONS-AMI (Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction) and ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) trials. J Am Coll Cardiol. 2014;63:1845-1854.
2. Ma W, Wang Q, Wang B, et al. Novel predictors of stent under-expansion regarding calcified coronary lesions assessed by optical coherence tomography. Catheter Cardiovasc Interv. 2022;99(S1):1473-1481.
3. Ng P, Maehara A, Kirtane AJ, et al. Management of Coronary Stent Underexpansion. J Am Coll Cardiol. 2025;85:625-644.
4. Shah M, Najam O, Bhindi R, Silva KD. Calcium Modification Techniques in Complex Percutaneous Coronary Intervention. Circ Cardiovasc Interv. 2021;14:E009870.
5. Barbato E, Gallinoro E, Abdel-Wahab M, et al. Management strategies for heavily calcified coronary stenoses: an EAPCI clinical consensus statement in collaboration with the EURO4C-PCR group. Eur Heart J. 2023;44:4340-4356.
6. Barbato E, CarriéD, Dardas P, et al. European expert consensus on rotational atherectomy. EuroIntervention. 2015;11:30-36.
7. Cobarro L, Jurado-Román A, Tébar-Márquez D, et al. Excimer laser coronary atherectomy in severely calcified lesions: time to bust the myth. REC Interv Cardiol. 2023;6:33-40.
8. Basile M, Gómez-Menchero A, Rivero-Santana B, et al. Rotational Atherectomy, Lithotripsy, or Laser for Calcified Coronary Stenosis: One-Year Outcomes From the ROLLER COASTER-EPIC22 Trial. Catheter Cardiovasc Interv. 2025;106:702-710.
9. Kuna C, Bradaric C, Koch T, et al. Age-related ten-year outcomes after percutaneous coronary intervention of in-stent restenosis. Int J Cardiol. 2025;428:133109.
10. Jurado-Román A, Gómez-Menchero A, Rivero-Santana B, et al. Rotational Atherectomy, Lithotripsy, or Laser for Calcified Coronary Stenosis: The ROLLER COASTR-EPIC22 Trial. JACC Cardiovasc Interv. 2025;18:606-618.
11. Jurado-Román A, Gómez-Menchero A, Amat-Santos IJ, et al. Design of the ROLLERCOASTR trial: rotational atherectomy, lithotripsy or laser for the management of calcified coronary stenosis. REC Interv Cardiol. 2023;5:279-286.
12. Rawlins J, Din JN, Talwar S, O'Kane P. Coronary Intervention with the Excimer Laser: Review of the Technology and Outcome Data. Interv Cardiol Rev. 2016;11:27.
13. Riley RF, Patel MP, Abbott JD, et al. SCAI Expert Consensus Statement on the Management of Calcified Coronary Lesions. J Soc Cardiovasc Angiogr Interv. 2024;3:101259.
14. de Waha S, Allali A, Büttner HJ, et al. Rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions: Two-year clinical outcome of the randomized ROTAXUS trial. Catheter Cardiovasc Interv. 2016;87:691-700.
15. Maehara A, Ben-Yehuda O, Ali Z, et al. Comparison of Stent Expansion Guided by Optical Coherence Tomography Vs Intravascular Ultrasound: The ILUMIEN II Study (Observational Study of Optical Coherence Tomography [OCT] in Patients Undergoing Fractional Flow Reserve [FFR] and Percutaneous Coronary Intervention). JACC Cardiovasc Interv. 2015;8:1704-1714.
16. Jurado-Román A, Gonzálvez A, Galeote G, Jiménez-Valero S, Moreno R. RotaTripsy: Combination of Rotational Atherectomy and Intravascular Lithotripsy for the Treatment of Severely Calcified Lesions. JACC Cardiovasc Interv. 2019;12:e127-e129.
17. Hill JM, Kereiakes DJ, Shlofmitz RA, et al. Intravascular Lithotripsy for Treatment of Severely Calcified Coronary Artery Disease. J Am Coll Cardiol. 2020;76:2635-2646.
18. Shibui T, Tsuchiyama T, Masuda S, Nagamine S. Excimer laser coronary atherectomy prior to paclitaxel-coated balloon angioplasty for de novo coronary artery lesions. Lasers Med Sci. 2021;36:111-117.
19. McClelland RL, Chung H, Detrano R, Post W, Kronmal RA. Distribution of coronary artery calcium by race, gender, and age: Results from the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2006;113:30-37.
20. Sharma V, Abdul F, Haider ST, et al. Rotablation in the Very Elderly –Safer than We Think?Cardiovasc Revasc Med. 2021;22:36-41.
21. Oliveri F, García PV, Oort MJH van, et al. Intravascular lithotripsy for the treatment of calcified coronary lesions in individuals of advanced age: a post-hoc analysis of the multicentre, prospective BENELUX-IVL study. eClinicalMedicine. 2025;85:103342.
22. Tisminetzky M, Miozzo R, Gore JM, et al. Trends in the magnitude of chronic conditions in patients hospitalized with a first acute myocardial infarction. J Multimorb Comorbidity. 2021;11:2633556521999570.
23. Nanna MG, Sutton NR, Kochar A, et al. Assessment and Management of Older Adults Undergoing PCI, Part 1: A JACC: Advances Expert Panel. JACC Adv. 2023;2:100389.
24. Galeote G, Zubiaur J, Jurado?Román A, et al. Coronary Rotational Atherectomy Elective Vs Bailout in Patients With Severely Calcified Lesions and Chronic Renal Failure (CRATER) Trial. Catheter Cardiovasc Interv. 2025;106:1702-1712.
25. Zubiaur J, Galeote G, Jurado-Román A, et al. Coronary Rotational ATherectomy Elective Vs Bailout in Patients With Severely Calcified Lesions and Chronic Renal Failure: Long-Term Outcomes of CRATER Trial. Catheter Cardiovasc Interv. 2026;107:431-438.
26. Saada M, Kobo O, Kauer F, et al. Prognosis of PCI in the Older Adult Population: Outcomes From the Multicenter Prospective e-ULTIMASTER Registry. J Soc Cardiovasc Angiogr Interv. 2022;1:100442.
27. Sanchis J, Bueno H, Miñana G, et al. Effect of Routine Invasive vs Conservative Strategy in Older Adults With Frailty and Non–ST-Segment Elevation Acute Myocardial Infarction: A Randomized Clinical Trial. JAMA Intern Med. 2023;183:407-415.
28. Abdel-Wahab M, Richardt G, Büttner HJ, et al. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions: The randomized ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) trial. JACC Cardiovasc Interv. 2013;6:10-19.
29. Mankerious N, Richardt G, Allali A, et al. Lower revascularization rates after high-speed rotational atherectomy compared to modified balloons in calcified coronary lesions: 5-year outcomes of the randomized PREPARE-CALC trial. Clin Res Cardiol. 2024;113:1051-1059.
30. Rheude T, Rai H, Richardt G, et al. Super high-pressure balloon vs scoring balloon to prepare severely calcified coronary lesions: the ISAR-CALC randomised trial: Balloon-based techniques for calcific CAD. EuroIntervention. 2021;17:481.
31. Abdel-Wahab M, Toelg R, Byrne RA, et al. High-speed rotational atherectomy vs modified balloons prior to drug-eluting stent implantation in severely calcified coronary lesions: The randomized prepare-CALC trial. Circ Cardiovasc Interv. 2018;11:e007415.
32. Kirtane AJ, Généreux P, Lewis B, et al. Orbital atherectomy vs balloon angioplasty before drug-eluting stent implantation in severely calcified lesions eligible for both treatment strategies (ECLIPSE): a multicentre, open-label, randomised trial. Lancet. 2025;405:1240-1251.
ABSTRACT
Background and objectives: Percutaneous coronary intervention for chronic total occlusion (CTO PCI) is a prolonged and technically demanding procedure often associated with patient anxiety and discomfort. We evaluated whether intraoperative audiovisual distraction via virtual reality (VR) goggles reduces procedural anxiety vs usual care.
Methods: The ReViCTO trial was a prospective, single-center, randomized, open-label study enrolling 59 patients undergoing elective CTO PCI. Participants were randomized to receive intraoperative audiovisual distraction via VR goggles (n = 31) or usual care (n = 28). The primary endpoint was maximum patient-reported procedural anxiety assessed immediately after theprocedure using a visual analogue scale (VAS; range, 0-10). Secondary endpoints included procedural pain, intraoperative sedative/analgesic requirements, and patient satisfaction.
Results: Baseline clinical characteristics were similar between groups. There was no significant difference in the primary endpoint of maximum procedural anxiety between the VR and control groups (mean VAS, 3.23 ± 2.78 vs 3.75 ± 2.77; mean difference, –0.52; P = .472). Similarly, no significant differences were observed regarding maximum procedural pain (P = .964) or the use and dosage of intraoperative morphine or midazolam. The intervention was safe, and 80.6% of patients in the VR group reported willingness to use the device during a future procedure.
Conclusions: Among patients undergoing elective CTO PCI, the use of immersive VR was feasible and well-tolerated but did not significantly reduce patient-reported peak anxiety, pain, or intraoperative pharmacologic requirements vs contemporary usual care.
[ClinicalTrials.gov: NCT05458999].
Keywords: Virtual reality. Percutaneous coronary intervention. Chronic total occlusion. Anxiety. Pain.
RESUMEN
Introducción y objetivos: La intervención coronaria percutánea (ICP) para las oclusiones coronarias totales crónicas (OTC) es un procedimiento prolongado y técnicamente exigente, a menudo asociado a ansiedad y malestar del paciente. Se evalúa si la distracción audiovisual durante el procedimiento mediante gafas de realidad virtual (RV) reduce la ansiedad procedimental en comparación con la atención habitual.
Métodos: El ensayo ReViCTO es un estudio prospectivo, unicéntrico, aleatorizado y abierto que incluyó 59 pacientes sometidos a ICP electiva de OTC. Los participantes se asignaron al azar para recibir distracción audiovisual durante el procedimiento con gafas de RV (n = 31) o atención habitual (n = 28). El objetivo principal fue la ansiedad máxima percibida por el paciente durante el procedimiento, evaluada inmediatamente después con una escala visual analógica (EVA; rango 0-10). Los objetivos secundarios fueron el dolor procedimental, las necesidades de sedación o analgesia durante el procedimiento, y la satisfacción del paciente.
Resultados: Las características clínicas basales fueron comparables entre los grupos. No hubo diferencias significativas en el objetivo principal de ansiedad máxima entre el grupo de RV y el grupo control (EVA media 3,23 ± 2,78 frente a 3,75 ± 2,77; diferencia media −0,52; p = 0,472). Tampoco se encontraron diferencias significativas en el dolor máximo (p = 0,964) ni en el uso y la dosis de morfina o midazolam durante el procedimiento. La intervención fue segura y el 80,6% de los pacientes del grupo de RV manifestaron que estarían dispuestos a utilizar el dispositivo en una intervención futura.
Conclusiones: En los pacientes sometidos a ICP electiva de OTC, el uso de RV inmersiva, en comparación con la atención habitual contemporánea, fue factible y bien tolerado, pero no redujo de manera significativa la ansiedad máxima ni el dolor percibidos por el paciente, y tampoco los requerimientos farmacológicos durante el procedimiento.
[ClinicalTrials.gov: NCT05458999].
Palabras clave: Realidad virtual. Intervención coronaria percutánea. Oclusión total crónica. Ansiedad. Dolor.
Abbreviations
CTO: chronic total occlusion. PCI: percutaneous coronary intervention. VASa: visual analogue scale for anxiety. VASp: visual analogue scale for pain. VR: virtual reality.
INTRODUCTION
Chronic total occlusions (CTO) are common among patients undergoing coronary angiography and represent one of the most technically demanding scenarios for percutaneous coronary intervention (PCI). Although contemporary CTO PCI programs achieve high success rates,1 these procedures frequently require prolonged fluoroscopy time, dual arterial access,2,3 and sustained patient immobility. In addition, ischemia-related chest discomfort may occur during complex procedural strategies.4,5
Anxiety is common in patients undergoing coronary procedures in the cath lab and may contribute to procedural discomfort and the need for pharmacologic sedation or analgesia.6-8 In routine practice, premedication and intraoperative administration of benzodiazepines or opioids are often used to mitigate anxiety and pain; however, their benefits are modest, and pharmacologic strategies and their use varies across centers.9 CTO PCI may be particularly associate with anxiety due to its typical duration, access strategy, and potential for procedural chest pain.
Virtual reality (VR) is an immersive audiovisual distraction strategy that can reduce procedural pain and anxiety across clinical settings. A systematic review demonstrated that VR-based distraction is effective for pain reduction in multiple procedural contexts.10
In interventional cardiology, early evidence suggests feasibility and potential benefit of VR during procedures performed under conscious sedation, including transcatheter aortic valve implantation and atrial fibrillation ablation.11,12 However, there are no randomized data evaluating VR during CTO PCI, a setting in which nonpharmacologic anxiolysis could be particularly valuable.
The ReViCTO trial was designed to test whether VR use during elective CTO PCI reduces the maximum level of patient-reported procedural anxiety vs usual care. Secondary endpoints included procedural pain, the use and dose of intraoperative anxiolytic or analgesic drugs, and patient satisfaction with the VR intervention. Figure 1 summarizes the main findings.
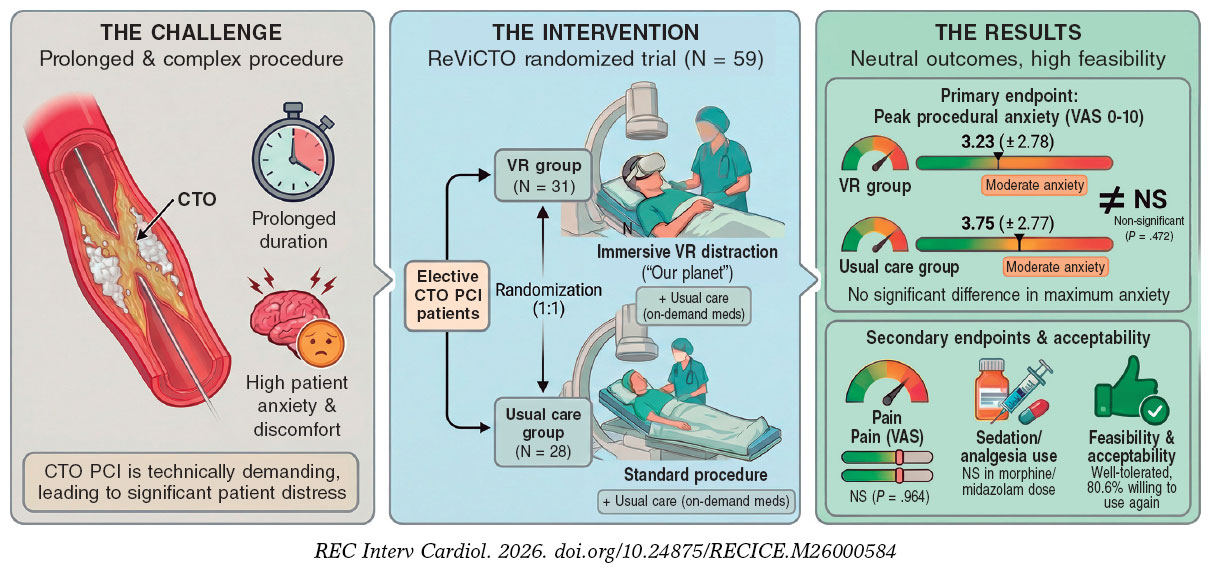
Figure 1. Central illustration. ReViCTO trial overview and main findings. Elective CTO PCI is a prolonged, technically complex procedure frequently associated with patient anxiety and discomfort. In the ReViCTO randomized trial (N = 59), patients were assigned to immersive audiovisual distraction using VR goggles (n = 31) or usual care (n = 28). VR use was feasible and well tolerated but did not significantly reduce peak procedural anxiety (VAS 0–10) or pain or intraoperative sedative or analgesic requirements vs usual care; 80.6% of VR patients reported willingness to use VR again in a future intervention. CTO, chronic total occlusion; PCI, percutaneous coronary intervention; VAS, visual analogue scale; VR, virtual reality.
METHODS
Trial design and oversight
The ReViCTO trial is an investigator-initiated, single-center, randomized, controlled, open-label, superiority trial with 2 parallel groups comparing immersive VR goggles vs usual care during elective CTO PCI. The study received no external funding. The rationale and full trial design have been published previously.13
The trial was conducted in accordance with the Declaration of Helsinki and International Conference on Harmonization Good Clinical Practice guidelines. The protocol was approved by the Clinical Research Ethics Committee of Hospital Clínico Universitario de València on 28 February, 2022, and all patients gave their prior written informed consent. The trial was registered at ClinicalTrials.gov (NCT05458999).
Participants
Adults (age > 18 years) scheduled for elective CTO PCI at Hospital Clínico Universitario de València were screened for eligibility. Key exclusion criteria were any condition precluding VR use, such as significant visual impairment, dementia, language barrier (inability to communicate fluently in Spanish or English), or other circumstances preventing safe use of the headset. Eligibility criteria were prespecified in the protocol publication.13
Randomization and trial procedures
Patients were randomized in a 1:1 ratio to the VR group or the control group using computer-generated permuted blocks to reduce the risk of imbalance in group sizes in a small trial.14 Allocation concealment was implemented via a web-based application that generated a unique trial identification number and assigned treatment arm after enrollment, preventing post-randomization modification or deletion. Due to the nature of the intervention, no blinding was applied to participants, operators, or outcome assessors.
CTO PCI was performed according to contemporary clinical practice by an experienced CTO team. Pharmacologic management of anxiety and pain was not protocolized and was left to the discretion of the primary operator in both groups. Specifically, morphine chloride and/or midazolam could be administered on demand during the procedure according to observed or reported anxiety or pain, in accordance with the trial protocol.
Interventions
Virtual reality group
A commercially available head-mounted display (Oculus Quest 2, Meta Platforms, United States) was used. Participants viewed the documentary series Our Planet via a video-streaming application (Netflix) in a virtual “theater” environment, starting with episode 1 with sequential autoplay thereafter, as specified in the protocol. The headset was applied before arterial puncture and was maintained throughout the intervention unless the patient requested removal or a serious complication occurred. Patient status was monitored at regular intervals during the procedure.
Control group
Participants assigned to control underwent CTO PCI under usual care without VR goggles.
Outcomes
The prespecified primary endpoint was the maximum level of anxiety perceived by the patient during the procedure, assessed immediately after the procedure and before leaving the cath lab using a visual analogue scale for anxiety (VASa). Secondary endpoints included maximum patient-perceived pain during the procedure (VASp), the use and total dose of intraoperative anxiolytic or analgesic drugs (midazolam and morphine chloride), procedure-related nausea or dizziness, and patient satisfaction with the VR intervention, including willingness to use VR again. Endpoint definitions and timing of assessment followed the protocol publication.
For analysis, VAS scores were treated as numeric ratings ranging from 0 (none) to 10 (worst), consistent with the trial questionnaires and the observed data range. Baseline angina-related health status was measured using the Seattle Angina Questionnaire (SAQ) to contextualize symptom burden.15
Data collection and management
Demographic characteristics, medical history, comorbidities, baseline symptom status (including SAQ), and procedural characteristics (arterial access strategy, procedure duration, fluoroscopy time, and radiation dose metrics) were collected from institutional electronic health records and procedure reports, supplemented by direct patient interview when necessary. Immediately after completion of CTO PCI, a trained study nurse administered the postoperative questionnaire and recorded VAS anxiety and pain, as well as nausea, dizziness, and satisfaction items. Intraoperative administration of morphine and midazolam and their total doses were recorded contemporaneously by the study nurse.
Data were entered into a dedicated electronic database incorporating range checks for numeric variables and duplicate checks for hospital identifiers and stored on a restricted-access workstation as described in the protocol.
Sample size estimation
The target sample size (58 patients, 29 per group) was calculated based on the primary endpoint, assuming a common standard deviation of 2.7 points for VAS anxiety and aiming to detect an absolute between-group difference of at least 2 points with a 2-sided alpha of 0.05 and 80% power. The standard deviation assumption was informed by prior cath lab anxiety studies.9,16
Statistical analysis
Continuous variables are expressed as mean (standard deviation, SD) or median (interquartile range, IQR) as appropriate (for the primary endpoint and Japan Chronic Total Occlusion (J-CTO) score, both measures are reported to allow comparison with sample size assumptions and to account for non-normal distribution). Categorical variables as counts and percentages. Between-group comparisons were performed using the Student t test for normally distributed continuous variables and the Mann–Whitney U test otherwise; categorical variables were compared using Fisher’s exact test or the chi-square test, as appropriate. Post hoc, we performed an analysis of covariance (ANCOVA) model with VASa as the dependent variable and treatment group as the main effect, adjusting for baseline anxiety. As a sensitivity analysis, we additionally adjusted for intraoperative opioid and benzodiazepine administration. Finally, to address the randomization imbalance in angiographic complexity, a multivariable linear regression analysis was conducted with maximum procedural anxiety as the dependent variable, adjusting for baseline anxiety and the J-CTO score. All tests were 2-sided, with a significance threshold of P < .05. Analyses were performed using R (V. 4.3.2, R Foundation for Statistical Computing, Austria). Reporting followed CONSORT guidelines for trial conduct and prespecified analyses (checklist in the supplementary data).17
RESULTS
Patients
Between 1 March 2022 and 23 October 2025, a total of 119 scheduled CTO PCI were performed. Fifteen patients declined the use of the headset, and in 44 cases the VR device was not available. One patient was excluded due to visual impairment (blindness). Overall, 59 patients were randomized to VR goggles (n = 31) or usual care (n = 28), as shown in figure 2.
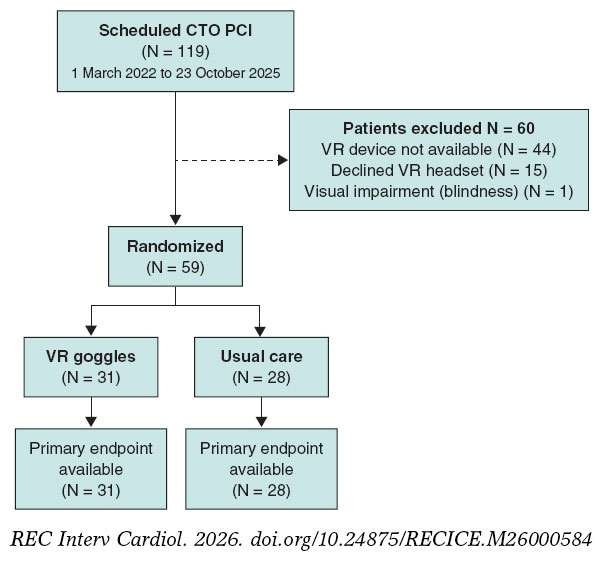
Figure 2. Study flow diagram. CTO PCI, percutaneous coronary intervention for chronic total occlusion; VR, virtual reality.
Enrolment was prospective; however, randomization was contingent on operational availability of the VR system. Early in the study, a single trained investigator was responsible for device preparation and operation, so randomization could only occur when this investigator was present in the cath lab (eg, during vacations or other clinical/research commitments). From June 2023 onward, a second investigator was trained, increasing coverage. In addition, the VR system was out of service for approximately 2 months due to changes in the required internet infrastructure. Importantly, nonrandomization during these periods was driven by logistical constraints rather than patient characteristics.
Baseline characteristics
Baseline clinical characteristics were broadly similar between groups. Median age was 67 [60;70] years in the VR group and 60 [58;66] years in the control group, and most participants were men (29 [93.5%] vs 26 [92.9%]). The prevalence of hypertension (51.6% vs 60.7%) and diabetes (41.9% vs 46.4%) was comparable; dyslipidemia was numerically less frequent in the VR group (58.1% vs 82.1%). Baseline anxiety assessed before entering the cath lab was moderate and did not differ significantly between groups (VAS anxiety: mean ± SD, 3.35 ± 3.10 vs 4.21 ± 3.05; P = .289; median [IQR], 2 [0; 6] vs 5 [2; 6]). Baseline pain was minimal in both groups (VAS pain baseline: 0.06 ± 0.36 vs 0.00 ± 0.00; P = .346; median [IQR], 0 [0 to 0] in both). Baseline angina-related health status was similar. The SAQ score was 52.4 [36.3; 64.3] in the VR group and 50.0 [44.0; 64.3] in the control group (P = .475), as shown in table 1.
Angiographic complexity differed between groups. The J-CTO score was higher in the VR group (mean ± SD, 3.10 ± 1.11; median [IQR], 3 [2; 4]) than in the control group (2.32 ± 1.36; median [IQR], 2 [1; 3]) (Student t test P = .019; Mann-Whitney U test P = .040).
Procedural characteristics and clinical outcomes
The distribution of procedural approach (antegrade, retrograde, or hybrid) was similar between groups (P = .826). Procedural duration, fluoroscopy time, radiation dose-area product, and contrast volume were not significantly different between groups, although radiation exposure tended to be higher in the VR group.
Technical success was achieved in 25 of 31 patients (80.6%) in the VR and 25 of 28 patients (89.3%) in the usual care group (P = .477). Procedural complications occurred in 4 of 31 patients (12.9%) in the VR group and 4 of 28 patients (14.3%) in the control group (P = 1.00) (table 1).
Table 1. Baseline characteristics, lesion and procedural characteristics
| Characteristic | VR goggles (n = 31) | Usual care (n = 28) | P |
|---|---|---|---|
| Age, years | 67 [60; 70] | 60 [58; 66] | .191 |
| Male sex | 29/31 (93.5%) | 26/28 (92.9%) | 1.000 |
| Hypertension | 16/31 (51.6%) | 17/28 (60.7%) | .482 |
| Dyslipidemia | 18/31 (58.1%) | 23/28 (82.1%) | .045 |
| Diabetes mellitus | 13/31 (41.9%) | 13/28 (46.4%) | .728 |
| Chronic kidney disease | 2/31 (6.5%) | 3/28 (10.7%) | .661 |
| Peripheral arterial disease | 5/31 (16.1%) | 4/28 (14.3%) | 1.000 |
| Current smoker | 5/31 (16.1%) | 10/28 (35.7%) | .084 |
| Former smoker | 15/31 (48.4%) | 6/28 (21.4%) | .031 |
| Previous myocardial infarction | 16/31 (51.6%) | 15/28 (53.6%) | .880 |
| Previous PCI | 19/31 (61.3%) | 17/28 (60.7%) | .966 |
| Previous CABG | 4/31 (12.9%) | 0/28 (0.0%) | .118 |
| Previous CTO-PCI attempt | 5/31 (16.1%) | 4/28 (14.3%) | 1.000 |
| Number of previous CTO attempts | 0 [0; 1] | 0 [0; 1] | .917 |
| NYHA class | 1 [1; 2] | 1 [1; 2] | .742 |
| Left ventricular ejection fraction, % | 50.4 ± 15.1 | 51.6 ± 14.0 | .742 |
| Hemoglobin, g/dL | 14.30 ± 1.79 | 14.33 ± 1.81 | .955 |
| Creatinine, mg/dL | 0.94 [0.80; 1.10] | 0.92 [0.81; 1.10] | .911 |
| NT-proBNP, pg/mL | 432 [186; 1406] | 390 [213; 1002] | .765 |
| Seattle Angina Questionnaire summary score (0-100) | 52.4 [36.3; 64.3] | 50.0 [44.0; 64.3] | .475 |
| Baseline anxiety (VAS 0-10) (mean) | 3.35 ± 3.10 | 4.21 ± 3.05 | .289 |
| Baseline anxiety (VAS 0-10) (IQR) | 2 [0; 6] | 5 [2; 6] | .289 |
| Baseline pain (VAS 0-10) (mean) | 0.06 ± 0.36 | 0.00 ± 0.00 | .346 |
| Baseline pain (VAS 0-10) (IQR) | 0 [0; 0] | 0 [0; 0] | .346 |
| Familiarity with technology: no | 4/31 (12.9%) | 2/28 (7.1%) | .389 |
| Familiarity with technology: cell phone | 10/31 (32.3%) | 11/28 (39.3%) | |
| Familiarity with technology: cell phone + personal computer | 15/31 (48.4%) | 15/28 (53.6%) | |
| Familiarity with technology: missing | 2/31 (6.5%) | 0/28 (0.0%) | |
| Previous VR experience: no | 25/31 (80.6%) | 24/28 (85.7%) | .103 |
| Previous VR experience: yes | 4/31 (12.9%) | 3/28 (10.7%) | |
| Previous VR experience: unknown | 0/31 (0.0%) | 1/28 (3.6%) | |
| Previous VR experience: missing | 2/31 (6.5%) | 0/28 (0.0%) | |
| Belief that video could relax: no | 7/31 (22.6%) | 1/28 (3.6%) | .103 |
| Belief that video could relax: yes | 23/31 (74.2%) | 26/28 (92.9%) | |
| Belief that video could relax: unknown | 1/31 (3.2%) | 1/28 (3.6%) | |
| SYNTAX score | 12 [9; 21] | 13 [11; 18] | .451 |
| J-CTO score (median) | 3 [2; 4] | 2 [1; 3] | .040 |
| J-CTO score (mean) | 3.10 ± 1.11 | 2.32 ± 1.36 | .019 |
| In-stent CTO | 1/30 (3.3%) | 3/28 (10.7%) | .344 |
| Occlusion length, mm | 30 [20; 40] | 30 [15; 40] | .209 |
| Blunt proximal cap | 21/31 (67.7%) | 22/28 (78.6%) | .350 |
| Moderate/severe calcification | 26/31 (83.9%) | 15/28 (53.6%) | .012 |
| Bending > 45° | 17/31 (54.8%) | 7/28 (25.0%) | .020 |
| Collateral pattern: ipsilateral | 4/31 (12.9%) | 2/28 (7.1%) | .346 |
| Collateral pattern: contralateral | 20/31 (64.5%) | 15/28 (53.6%) | |
| Collateral pattern: ipsi- and contralateral | 7/31 (22.6%) | 11/28 (39.3%) | |
| Approach: antegrade | 25/31 (80.6%) | 22/28 (78.6%) | .826 |
| Approach: retrograde | 4/31 (12.9%) | 3/28 (10.7%) | |
| Approach: hybrid | 2/31 (6.5%) | 3/28 (10.7%) | |
| Any femoral access used | 4/31 (12.9%) | 4/28 (14.3%) | 1.000 |
| Procedure duration, min | 123 ± 38 | 107 ± 55 | .216 |
| Fluoroscopy time, min | 48 [35; 63] | 40 [20; 67] | .370 |
| Dose-area product, Gy · cm2 | 218 [183; 321] | 178 [103; 281] | .052 |
| Contrast volume, mL | 145 [106; 220] | 150 [112; 198] | .967 |
| No. of stents | 2 [1; 3] | 1 [1; 2] | .030 |
| Total stent length, mm | 80 ± 40 | 52 ± 28 | .006 |
| Technical success | 25/31 (80.6%) | 25/28 (89.3%) | .477 |
| Procedural complications | 4/31 (12.9%) | 4/28 (14.3%) | 1.000 |
|
Data are expressed as mean (SD), median [interquartile range], or n/N (%). P values were calculated using the Student t test for normally distributed variables, the Mann–Whitney U test for non-normally distributed variables, and the chi-square or Fisher exact test for categorical variables, according to the prespecified analysis plan. NT-proBNP available in 13 VR and 12 control patients; SAQ available in 30 VR and 27 control patients; NYHA available in 30 VR and 28 control patients. For baseline VAS anxiety and pain, both mean ± SD and median [Q1; Q3] are reported. CABG, coronary artery bypass grafting; CTO, chronic total occlusion; J-CTO, Japanese Chronic Total Occlusion score; NT-proBNP, N-terminal pro-B-type natriuretic peptide; NYHA, New York Heart Association; PCI, percutaneous coronary intervention; SAQ, Seattle Angina Questionnaire; SD, standard deviation; SYNTAX, Synergy Between PCI With TAXUS and Cardiac Surgery score; VAS, visual analogue scale; VR, virtual reality. |
|||
Primary endpoint
The primary endpoint (maximum procedural anxiety; [VASa]) and key secondary endpoints (maximum procedural pain [VASp] and intraoperative drug administration) were available for all randomized participants.
Maximum procedural anxiety did not differ significantly between groups. Mean VASa was 3.23 ± 2.78 with VR and 3.75 ± 2.77 with usual care (mean difference, −0.52 points; 95% confidence interval (95%CI), −1.97 to 0.92; Student t test P = .472). Median [IQR] values were 4 [0; 5] and 4 [2; 6], respectively. Because the VASa distribution was skewed, results were consistent using the Mann–Whitney U test (P = .379) (figure 3, table 2 and table S1).
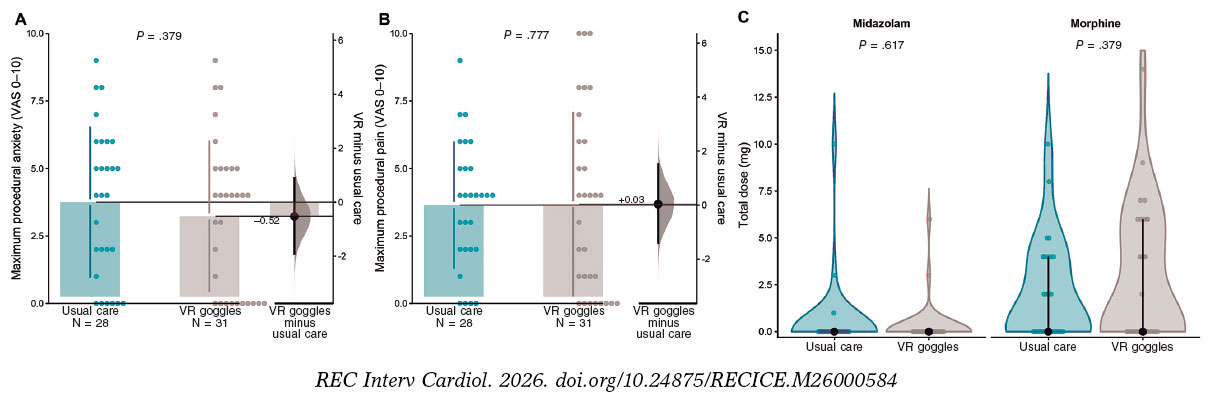
Figure 3. Patient-reported procedural anxiety and pain, and intraoperative drug use. A: maximum procedural anxiety assessed immediately after the procedure using a visual analogue scale for anxiety (VASa; 0–10). B: maximum procedural pain assessed using a visual analogue scale for pain (VASp; 0–10). C: total intraoperative dose (mg) of midazolam and morphine by treatment group; zero values indicate no drug administration. In panels A and B, dots represent individual patients; the right-side estimation plot shows the mean between-group difference (VR minus usual care) with its 95% confidence interval. P values correspond to prespecified between-group comparisons. VAS, visual analogue scale; VR, virtual reality.
Table 2. Endpoints and safety
| Variable | VR goggles | Usual care | P |
|---|---|---|---|
| Maximum procedural anxiety* | 3.23 ± 2.78 | 3.75 ± 2.77 | .472 |
| Maximum procedural anxiety* | 4 [0; 5] | 4 [2 to 6] | .379 |
| Maximum procedural pain* | 3.68 ± 3.39 | 3.64 ± 2.33 | .964 |
| Maximum procedural pain* | 4 [1; 6] | 4 [2;5] | .777 |
| Morphine administered | 14/31 (45.2) | 13/28 (46.4) | 1.000 |
| Total morphine dose, mg | 2.74 ± 3.61 | 2.00 ± 2.71 | .379 |
| Midazolam administered | 2/31 (6.5) | 3/28 (10.7) | .661 |
| Total midazolam dose, mg | 0.29 ± 1.19 | 0.50 ± 1.95 | .617 |
| Nausea during procedure | 1/31 (3.2) | 0/28 (0.0) | 1.000 |
| Dizziness during procedure | 1/31 (3.2) | 0/28 (0.0) | 1.000 |
|
Values are mean ± SD, median [Q1; Q3], or n/N (%). For visual analogue scale (VAS) anxiety and pain, both mean ± SD and median [Q1; Q3] are reported due to skewness of the distributions. P values for rows reporting mean ± SD are from Student’s t test; P values for rows reporting median [Q1; Q3] are from Mann–Whitney U tests. Categorical variables were compared using Fisher’s exact test. Total morphine and midazolam doses (mg) include zeros for patients not receiving the drug. SD, standard deviation; VR, virtual reality. * VAS 0-10. |
|||
In a post hoc ANCOVA adjusting for baseline anxiety, VR was not associated with lower peak procedural anxiety (adjusted mean difference, −0.21; 95%CI, −1.62-1.20; P = .773). Results remained consistent after additional adjustment for intraoperative morphine and midazolam dose (table S1 and table S2).
Given the significantly higher angiographic complexity in the VR group, a sensitivity analysis was conducted using multivariable linear regression. After adjusting for J-CTO score and baseline anxiety, the effect of VR on procedural anxiety remained non-significant (adjusted coefficient -0.40; 95%CI, -1.81 to 1.02; P = .576). In this model, procedural complexity was not independently associated with patient-reported anxiety (P = .370); see table S1.
Secondary endpoints
VASp was similar in the 2 groups: 3.68 ± 3.39 with VR and 3.64 ± 2.33 with usual care (mean difference, 0.03; 95%CI, −1.50-1.57; P = .964). Median [IQR] values were 4 [1; 6] and 4 [2; 5], respectively (P = .777).
Intraoperative pharmacologic treatment did not differ between groups. Morphine was administered to 14 of 31 patients (45.2%) in the VR group and 13 of 28 (46.4%) in the control group (P = 1.00). Total morphine dose (including zero valus for nonuse) was 2.74 ± 3.61 mg and 2.00 ± 2.71 mg, respectively (P = .379). Midazolam was administered to 2 of 31 patients (6.5%) in the VR group and 3 of 28 (10.7%) in the control group (P = .661), with total midazolam doses of 0.29 ± 1.19 mg and 0.50 ± 1.95 mg, respectively (P = .617) (figure 3 and table 2).
Safety and acceptability
Symptoms potentially attributable to VR were uncommon. Nausea occurred in 1 patient (3.2%) in the VR group and in no patients in the control group (P = 1.00). Dizziness occurred in 1 patient (3.2%) in the VR group and in no patients in the control group (P = 1.00).
Among patients assigned to VR, 25 of 31 (80.6%) reported that they would be willing to use a relaxation video again during a future intervention; 5 (16.1%) would not, and 1 (3.2%) was uncertain.
DISCUSSION
We conducted a randomized trial to evaluate whether VR-based audiovisual distraction during elective CTO PCI can improve the patient experience. Several key findings emerge. First, VR did not meaningfully reduce patient-reported peak procedural anxiety, and pain outcomes were similarly neutral, arguing against a clinically relevant anxiolytic or analgesic effect with the intervention as delivered. Second, VR did not reduce the use of intraoperative opioid or benzodiazepine requirements, suggesting limited incremental benefit beyond contemporary usual care in the cath lab. Third, VR implementation appeared feasible and was not associated with signals of procedural harm, with overall procedural outcomes remaining comparable despite an imbalance toward greater angiographic complexity in the VR group. Finally, acceptability was generally high among patients assigned to VR, supporting its role as a patient-centered option for selected individuals even when average effects on anxiety are modest.
Interpreting the neutral result in the context of prior interventional cardiology VR trials
Several factors may explain the absence of a measurable anxiolytic effect in ReViCTO. First, peak procedural anxiety levels were relatively low, leaving limiting the potential for improvement and increasing the likelihood of a floor effect. A similar pattern has been observed in contemporary minimally sedated structural interventions, in which overall anxiety burden is modest and VR has not consistently produced detectable differences on global assessments.18
Second, anxiety and pain were assessed immediately after the procedure as a single recalled measure of peak intensity. Although pragmatic and consistent with the study protocol, this approach relies on retrospective recall and may underestimate brief, procedure-specific peaks of discomfort that are particularly relevant in CTO PCI, such as arterial puncture, prolonged immobility, complex device manipulation, or episodes of ischemic chest pain.19 Consequently, any benefit limited to these discrete high-stress intervals may have been diluted when summarized as a single postprocedural peak value.
Third, the VR content in the ReViCTO consisted of passive content (documentary viewing). Across procedural settings, the magnitude of VR’s effect appears to depend on how strongly the experience captures attention and induces relaxation. Interventions incorporating guided relaxation, hypnosis-based modules, or interactive elements have more consistently demonstrated larger and more reproducible effects than passive viewing alone.20-22
In the context of the broader interventional cardiology literature, the neutral effect of VR on peak intraoperative anxiety in ReViCTO is therefore less surprising. Existing cath lab and structural heart studies suggest that observable benefit depends on when VR is delivered, which patients are targeted, particularly those with higher baseline anxiety, and how outcomes are measured. In transcatheter aortic valve implantation (TAVI), early randomized studies reported lower VAS-based procedural anxiety, supporting feasibility and a potential anxiolytic effect.11 In contrast, a larger minimalistic TAVI randomized study found improvements in state anxiety (State-Trait Anxiety Inventory, state scale [STAI-S]) and perceived procedure duration, yet less consistent effects on VAS-based anxiety or pain, underscoring the influence of measurement instruments on signal detection.23 Evidence from coronary procedures is similarly nuanced. In the VR InCard program, which targeted patients with elevated preoperative anxiety and incorporated structured preprocedural sessions, the primary analysis was neutral but adjusted analyses suggested modest reductions, with heterogeneity by clinical context.24,25 Similarly, a randomized trial conducted before coronary angiography reported anxiety reduction using questionnaire-based assessments rather than a single recalled postoperative peak rating.26 Collectively, these data support the interpretation that VR may be most effective when targeted to patients with higher baseline anxiety, delivered during anticipatory or discrete high-stress phases, and evaluated using instruments sensitive to global state anxiety, rather than relying solely on a single recalled peak score.22,27
Pharmacologic co-intervention and post hoc adjustment
A key pragmatic feature of ReViCTO was that background anxiolysis and analgesia were not protocolized, reflecting real-world practice in the cath lab where conscious sedation and intraoperative comfort measures are typically individualized. This approach is consistent with contemporary cath lab randomized studies evaluating patient comfort under usual care conditions.28,29 In the final dataset, intraoperative morphine and midazolam use were similar, and dose distributions did not differ materially. To align with current analytic recommendations, we performed a post hoc ANCOVA adjusting peak anxiety for baseline anxiety, an approach that can improve precision when baseline values are prognostic.30 Baseline anxiety was strongly associated with peak anxiety, while VR assignment was not (adjusted VR effect approximately -0.32 VAS points; P = .64). Adding opioid and benzodiazepine doses did not materially change the VR estimate, supporting that the neutral primary result is unlikely to be explained by baseline imbalance or differential pharmacologic rescue. Baseline anxiety was higher in the usual care group; adjusted analyses yielded consistent findings.
Feasibility, tolerability, and patient-center implementation
From a feasibility standpoint, VR use in CTO PCI appeared safe and compatible with the cath lab environment, with nausea and dizziness reported rarely and no signal suggesting increased procedural instability. The practical challenge was tolerability during long procedures: early discontinuation of the headset occurred in 9 VR patients, which is consistent with broader evidence that fully immersive head-mounted displays can trigger discomfort or cybersickness in a minority of users, particularly with extended exposure.31 Implementation studies further indicate that device-related factors—such as physical interference, usability barriers, and the need for individual tailoring—can influence both uptake and sustained use, supporting a selective rather than universal deployment strategy.32 These observations support a patient-center approach: VR may be most useful when offered to patients with higher baseline anxiety, a clear preference for audiovisual distraction, or anticipated prolonged immobility, and when focused around discrete high-stress phases. Preoperative counseling remains essential with VR serving as a complementary, rather than substitutive, strategy.
Limitations
This trial has limitations that should be considered. First, it was a single-center, open-label study and subjective outcomes may be susceptible to reporting buas; however, randomization, standardized outcome collection, and consistently neutral findings across patient-reported outcomes and medication use make a major bias-driven effect unlikely. Second, recruitment was not consecutive and 12.6% of eligible patients declined participation, which may limit generalizability; nonetheless, this also reflects real-world acceptability of a wearable intervention, and the decliner rate is transparently reported. Third, anxiety and pain were assessed as a single postoperative peak rating rather than repeated measures during predefined high-stress phases; this approach was identical in both groups, and recalled peak experience remains clinically relevant for satisfaction and willingness to undergo future procedures. Fourth, anxiolysis and analgesia were not protocolized and were operator-directed, potentially attenuating any incremental benefit of VR. Nevertheless, this pragmatic design improves applicability and bailout medication was systematically recorded. Fifth, VR content was passive and exposure time likely varied due to early discontinuation; the intention-to-treat analysis therefore estimates the real-world effect of offering VR. Finally, although angiographic complexity (J-CTO score) was higher in the VR group, multivariable analyses indicated this imbalance did not explain the neutral anxiety results and complexity was not a significant predictor of distress in this cohort. Benzodiazepine amnesia may attenuate recall; midazolam use was low and balanced.
CONCLUSIONS
In this randomized trial of patients undergoing elective CTO PCI, although immersive VR was feasible and well tolerated, it did not reduce patient-reported peak intraoperative anxiety or pain, or the need for intraoperative morphine or midazolam vs usual care.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
The protocol was approved by the Clinical Research Ethics Committee of Hospital Clínico Universitario de València (28 February, 2022), and all participants gave their prior written informed consent. Sex distribution is reported, and reporting adhered to SAGER guidelines to mitigate potential sex- and gender-related bias.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
Generative artificial intelligence was used to support language editing and formatting of the revised manuscript. No artificial intelligence tools were used to analyze study data. All content was reviewed and approved by the authors, who take full responsibility for the manuscript.
AUTHORS’ CONTRIBUTIONS
A. Fernández-Cisnal and B. Silla conceived the study and designed the trial. A. Fernández-Cisnal, B. Silla, C.E. Vergara-Uzcategui, J.M. Ramón, E. Valero, and C. Romero Menor contributed to patient inclusion and data acquisition. A. Fernández-Cisnal performed the statistical analyses and drafted the manuscript. B. Silla, C.E. Vergara- Uzcategui, J.M. Ramón, E. Valero, C. Romero Menor, J. Núñez, V. Bodí, and G. Miñana critically revised the manuscript for important intellectual content. All authors approved the final version and agreed to be accountable for all aspects of the work.
CONFLICTS OF INTEREST
None declared.
WHAT IS KNOWN ABOUT THE TOPIC?
- CTO PCI is a long, technically complex cath lab procedure that can cause anxiety and discomfort for patients.
- Patient anxiety during coronary procedures may worsen perceived discomfort and can increase the need for intraoperative sedatives or analgesics, although pharmacological strategies show modest and variable benefits in routine practice.
- VR provides immersive audiovisual distraction and has been shown to reduce pain and anxiety in several procedural and clinical settings.
- Early studies in interventional cardiology suggest VR can be feasible during procedures performed under conscious sedation, but evidence is mixed and randomized data in CTO PCI were lacking.
WHAT DOES THIS STUDY ADD?
- In the prospective, single-center randomized ReViCTO trial with 59 patients undergoing elective CTO PCI, intraoperative VR goggles were feasible, safe, and generally well tolerated.
- VR did not significantly reduce patient-reported peak procedural anxiety vs usual care and similarly showed no reduction in peak pain.
- VR did not decrease the use or total dose of intraoperative morphine or midazolam, suggesting limited incremental benefit over contemporary usual care.
- Despite a higher angiographic complexity in the VR group, procedural outcomes and complication rates were comparable, and most VR patients reported they would consider using the device again in future interventions.
SUPPLEMENTARY DATA
REFERENCES
1. Patel VG, Brayton KM, Tamayo A, et al. Angiographic Success and Procedural Complications in Patients Undergoing Percutaneous Coronary Chronic Total Occlusion Interventions. JACC Cardiovasc Interv. 2013;6:128-136.
2. Brilakis ES, Grantham JA, Rinfret S, et al. A Percutaneous Treatment Algorithm for Crossing Coronary Chronic Total Occlusions. JACC Cardiovasc Interv. 2012;5:367-379.
3. Christopoulos G, Karmpaliotis D, Alaswad K, et al. Application and outcomes of a hybrid approach to chronic total occlusion percutaneous coronary intervention in a contemporary multicenter US registry. Int J Cardiol. 2015;198:222-228.
4. Fefer P, Knudtson ML, Cheema AN, et al. Current Perspectives on Coronary Chronic Total Occlusions. J Am Coll Cardiol. 2012;59:991-997.
5. Tajti P, Burke MN, Karmpaliotis D, et al. Update in the Percutaneous Management of Coronary Chronic Total Occlusions. JACC Cardiovasc Interv. 2018;11:615-625.
6. Delewi R, Vlastra W, Rohling WJ, et al. Anxiety levels of patients undergoing coronary procedures in the catheterization laboratory. Int J Cardiol. 2017;228:926-930.
7. Trotter R, Gallagher R, Donoghue J. Anxiety in patients undergoing percutaneous coronary interventions. Heart Lung. 2011;40:185-192.
8. Astin F, Jones K, Thompson DR. Prevalence and patterns of anxiety and depression in patients undergoing elective percutaneous transluminal coronary angioplasty. Heart Lung. 2005;34:393-401.
9. Vlastra W, Delewi R, Rohling WJ, et al. Premedication to reduce anxiety in patients undergoing coronary angiography and percutaneous coronary intervention. Open Heart. 2018;5:000833.
10. Teh JJ, Pascoe DJ, Hafeji S, et al. Efficacy of virtual reality for pain relief in medical procedures:a systematic review and meta-analysis. BMC Med. 2024;22:64.
11. Bruno RR, Lin Y, Wolff G, et al. Virtual reality-assisted conscious sedation during transcatheter aortic valve implantation:a randomised pilot study. EuroIntervention. 2020;16:1014-1020.
12. Roxburgh T, Li A, Guenancia C, et al. Virtual Reality for Sedation During Atrial Fibrillation Ablation in Clinical Practice:Observational Study. J Med Internet Res. 2021;23:26349.
13. Fernández-Cisnal A, Silla B, María Ramón J, et al. Efficacy of virtual reality reducing anxiety during CTO revascularization:the ReViCTO trial design. REC Interv Cardiol. 2023;5:203-209.
14. Schulz KF, Grimes DA. Unequal group sizes in randomised trials:guarding against guessing. Lancet. 2002;359:966-970.
15. Spertus JA, Winder JA, Dewhurst TA, et al. Development and evaluation of the Seattle Angina questionnaire:A new functional status measure for coronary artery disease. J Am Coll Cardiol. 1995;25:333-341.
16. Delewi R, Vlastra W, Rohling WJ, et al. Anxiety levels of patients undergoing coronary procedures in the catheterization laboratory. Int J Cardiol. 2017;228:926-930.
17. Chan AW, Boutron I, Hopewell S, et al. SPIRIT 2025 statement:updated guideline for protocols of randomised trials. BMJ. 2025;389:081477.
18. Chatterjee S, Ooms J, De Ronde M, et al. Anxiety during transcatheter aortic valve replacement under local anesthesia - the ART-VR trial. Cardiovasc Revasc Med. 2025;79:71-77.
19. Brilakis ES, Banerjee S, Karmpaliotis D, et al. Procedural Outcomes of Chronic Total Occlusion Percutaneous Coronary Intervention. JACC Cardiovasc Interv. 2015;8:245-253.
20. Bekelis K, Calnan D, Simmons N, MacKenzie TA, Kakoulides G. Effect of an Immersive Preoperative Virtual Reality Experience on Patient Reported Outcomes:A Randomized Controlled Trial. Ann Surg. 2017;265:1068-1073.
21. Gullo G, Rotzinger DC, Colin A, et al. Virtually Augmented Self-Hypnosis in Peripheral Vascular Intervention:A Randomized Controlled Trial. Cardiovasc Intervent Radiol. 2023;46:786-793.
22. El Mathari S, Hoekman A, Kharbanda RK, et al. Virtual Reality for Pain and Anxiety Management in Cardiac Surgery and Interventional Cardiology. JACC:Advances. 2024;3:100814.
23. Lind A, Ahsan M, Totzeck M, et al. Virtual reality-assisted distraction during transcatheter aortic valve implantation under local anaesthesia:A randomised study. Int J Cardiol. 2023;387:131130.
24. Groenveld TD, Breunissen EHW, Bonnes JL, et al. Virtual Reality to Reduce Preprocedural Anxiety During Invasive Coronary Angiography. JACC:Advances. 2025;4:101976.
25. Breunissen EHW, Groenveld TD, Garms L, Bonnes JL, Van Goor H, Damman P. Virtual reality to reduce periprocedural anxiety during invasive coronary angiography:rationale and design of the VR InCard trial. Open Heart. 2024;11:002628.
26. Keshvari M, Yeganeh MR, Paryad E, Roushan ZA, Pouralizadeh M. The effect of virtual reality distraction on reducing patients'anxiety before coronary angiography:a randomized clinical trial study. Egypt Heart J. 2021;73:98.
27. Micheluzzi V, Burrai F, Casula M, et al. Effectiveness of virtual reality on pain and anxiety in patients undergoing cardiac procedures:A systematic review and meta-analysis of randomized controlled trials. Curr Probl Cardiol. 2024;49:102532.
28. Boukantar M, Chiaroni PM, Gallet R, et al. A Randomized Controlled Trial of Nonfasting vs Fasting Before Interventional Coronary Procedures. JACC Cardiovasc Interv. 2024;17:1200-1210.
29. Ferreira D, Hardy J, Meere W, et al. Fasting >no fasting prior to catheterization laboratory procedures:the SCOFF trial. Eur Heart J. 2024;45:4990-4998.
30. Tackney MS, Morris T, White I, Leyrat C, Diaz-Ordaz K, Williamson E. A comparison of covariate adjustment approaches under model misspecification in individually randomized trials. Trials. 2023;24:14.
31. Cossio S, Chiappinotto S, Dentice S, et al. Cybersickness and discomfort from head-mounted displays delivering fully immersive virtual reality:A systematic review. Nurse Educ Pract. 2025;85:104376.
32. Kouijzer MMTE, Kip H, Bouman YHA, Kelders SM. Implementation of virtual reality in healthcare:a scoping review on the implementation process of virtual reality in various healthcare settings. Implement Sci Commun. 2023;4:67.
- Design of the ORBIT-SHOCK pilot study: orbital atherectomy vs intravascular lithotripsy for calcified coronary nodules
- Drug-coated balloons versus drug-eluting stents for de novo coronary lesions: a systematic review and meta-analysis
- Drug-coated balloon for the side branch compared with conventional strategy in left anterior descending-diagonal bifurcation lesions
- SELUTION SLR sirolimus-eluting balloon compared with the Pantera Lux paclitaxel drug-coated balloon in the management of de novo coronary lesions







Interviews

An interview with Bruno Scheller
aServicio de Cardiología, Hospital Universitario de La Princesa, Instituto de Investigación Sanitaria de La Princesa (IIS-IP), Universidad Autónoma de Madrid, Spain
bCentro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain




