
ABSTRACT
Introduction and objectives: Coronary microcatheters play a key role in contemporary percutaneous coronary intervention (PCI), particularly in complex anatomies such as chronic total coronary occlusions. Under the European Medical Device Regulation (MDR 2017/745), post-market clinical follow-up (PMCF) studies are required to confirm safety and performance. However, PMCF evidence on coronary microcatheters remains limited. Our primary endpoint was to assess device effectiveness, defined as successful lesion or occlusion crossing. Procedural effectiveness was defined as final Thrombolysis in Myocardial Infarction grade-3 flow with < 30% residual percent diameter stenosis. Device safety endpoints included the absence of device-related mechanical failures, including rupture, kinking, or complicated retrieval.
Methods: This prospective, multicenter, multinational, observational PMCF study evaluated the safety and performance of a coronary microcatheter (Navitian, iVascular, Spain) used according to CE-marked indications. Adult patients in whom the use of the device was attempted, usually in combination with other devices, were consecutively included. Clinical outcomes were assessed during in-hospital stay up to discharge.
Results: A total of 102 patients with 115 coronary lesions were included. Lesion complexity was high: 57.4% chronic total coronary occlusions, 87.8% were American Heart Association type B2/C lesions, and 47.0% had significant calcification. Device effectiveness for lesion or occlusion crossing, evaluable in successfully wired lesions, was 95.2%. Procedural success was achieved in 100% of cases in which the device crossed. No device-related safety failures were observed. None of the adverse clinical events observed (4.3%) were adjudicated to the microcatheter.
Conclusions: In this prospective, multinational PMCF study, the Navitian coronary microcatheter demonstrated high effectiveness and an excellent device-related safety profile in a real-world complex PCI, supporting its continued use in routine complex PCIs.
(Clinicaltrials.gov NCT05292118).
Keywords: Microcatheter. Complex PCI. Real-world data. Effectiveness. Safety.
RESUMEN
Introducción y objetivos: Los microcatéteres coronarios desempeñan un papel fundamental en la intervención coronaria percutánea contemporánea, especialmente en anatomías complejas. Según el Reglamento europeo sobre productos sanitarios (MDR 2017/745), se requieren estudios de seguimiento clínico poscomercialización (PMCF) para confirmar la seguridad y el rendimiento. El objetivo principal del presente estudio fue evaluar la eficacia de un dispositivo (cruce exitoso de la lesión u oclusión). La valoración de seguridad incluye la ausencia de fallos mecánicos (rotura, estrangulamiento o retirada complicada).
Métodos: Estudio PMCF observacional, prospectivo, multicéntrico y multinacional para evaluar la seguridad y el rendimiento de un microcatéter coronario (Navitian, iVascular, España) utilizado de acuerdo con las indicaciones aprobadas por el marcado CE. Se incluyeron de forma consecutiva pacientes adultos en los que se intentó utilizar el dispositivo, normalmente en combinación con otros. Los resultados clínicos se evaluaron hasta el alta.
Resultados: Se incluyeron 102 pacientes con 115 lesiones coronarias. La complejidad de las lesiones era alta: 57,4% oclusiones totales, 87,8% lesiones American Heart Association tipo B2/C y 47,0% calcificación significativa. La eficacia del dispositivo, evaluable en las lesiones tras el cruce de la guía, fue del 95,2%. Se logró el éxito del procedimiento (flujo Thrombolysis in Myocardial Infarction 3 final con estenosis residual < 30%) en todos los casos en los que el dispositivo cruzó. No se observaron fallos de seguridad. Ninguno de los eventos clínicos adversos observados (4,3%) se atribuyó al microcatéter.
Conclusiones: En este estudio PMCF prospectivo y multinacional, el microcatéter coronario Navitian demostró una alta eficacia y un excelente perfil de seguridad en intervenciones coronarias percutáneas complejas de la práctica real.
(Clinicaltrials.gov NCT05292118).
Palabras clave: Microcatéter. Intervención coronaria percutánea compleja. Datos de la práctica real. Eficacia. Seguridad.
Abbreviations
CTO: chronic total coronary occlusion. MDR: medical device regulation. PCI: percutaneous coronary intervention. PMCF: post-market clinical follow-up.
INTRODUCTION
Percutaneous coronary intervention (PCI) has progressively expanded to increasingly complex anatomical and clinical scenarios, including chronic total coronary occlusions (CTOs), long and diffuse disease, severe calcification, and tortuous coronary anatomy. In this setting, coronary microcatheters have become indispensable adjunctive devices, facilitating guidewire support and exchange, distal contrast injection, and device delivery.
Despite their widespread use, clinical evidence supporting the safety and performance of coronary microcatheters is largely derived from single-center experiences,1,2 retrospective series,3-5 or extrapolated from broader CTO registries.6-11 Under the current European Medical Device Regulation (MDR 2017/745), manufacturers and sponsors are required to generate post-market clinical follow-up (PMCF) evidence to continuously confirm the safety and clinical performance of CE-marked devices throughout their life cycle. Real-world data, collected prospectively in routine clinical practice, play a central role in fulfilling these regulatory requirements.
The Navitian coronary microcatheter (iVascular, Spain) is a single-lumen, over-the-wire compatible device designed to facilitate guidewire advancement, exchange, and distal infusion during PCI. While its use is well established in daily practice, prospective multinational PMCF evidence evaluating its performance in real-world complex PCI remains limited.
The present study was designed as a prospective, multicenter, multinational PMCF investigation to evaluate the safety and clinical performance of the Navitian coronary microcatheter in routine practice across Spain and Portugal. By focusing on highly complex lesions and contemporary PCI workflows, this study aims to provide clinically relevant and regulatorily robust evidence supporting the real-world use of the device under MDR requirements.
METHODS
Study design
We conducted a prospective, multicenter, multinational observational PMCF study conducted in routine clinical practice in Spain and Portugal (ClinicalTrials.gov ID NCT05292118). The study was designed and performed in full compliance with the European Medical Device Regulation (MDR 2017/745), ISO 14155:2020 for clinical investigations of medical devices, the Declaration of Helsinki, and applicable national regulatory requirements.
The study followed a single-arm design without protocol-mandated additional diagnostic or therapeutic procedures beyond standard clinical care. Device use was limited to its CE-marked indications, and all procedural decisions were left to the discretion of the treating operators.
Study population
Adult patients aged 18 years or older undergoing PCI in whom use of the Navitian coronary microcatheter was attempted, either alone or in combination with other coronary devices, were consecutively included. Eligibility was based on routine clinical practice and operator judgment.
Patients were excluded only if they explicitly declined participation or refused to provide written informed consent, in accordance with local ethical and regulatory requirements.
Participant centers
The study was conducted across 7 high-volume PCI centers in Spain and Portugal, reflecting a broad spectrum of contemporary European practice. This multinational design aimed to enhance the external validity and generalizability of the findings across different healthcare systems and procedural environments.
Device description
The Navitian coronary microcatheter is a single-lumen device compatible with 0.014 in guidewires, designed to provide guidewire support, facilitate wire exchange, and allow distal infusion of contrast or saline. The device features a hydrophilic distal coating to enhance trackability through tortuous and complex coronary anatomy and incorporates a rounded atraumatic distal tip to reduce the risk of arterial damage during advancement, as well as radiopaque markers to aid fluoroscopic visualization (figure 1). The microcatheter was used strictly according to its instructions for use.
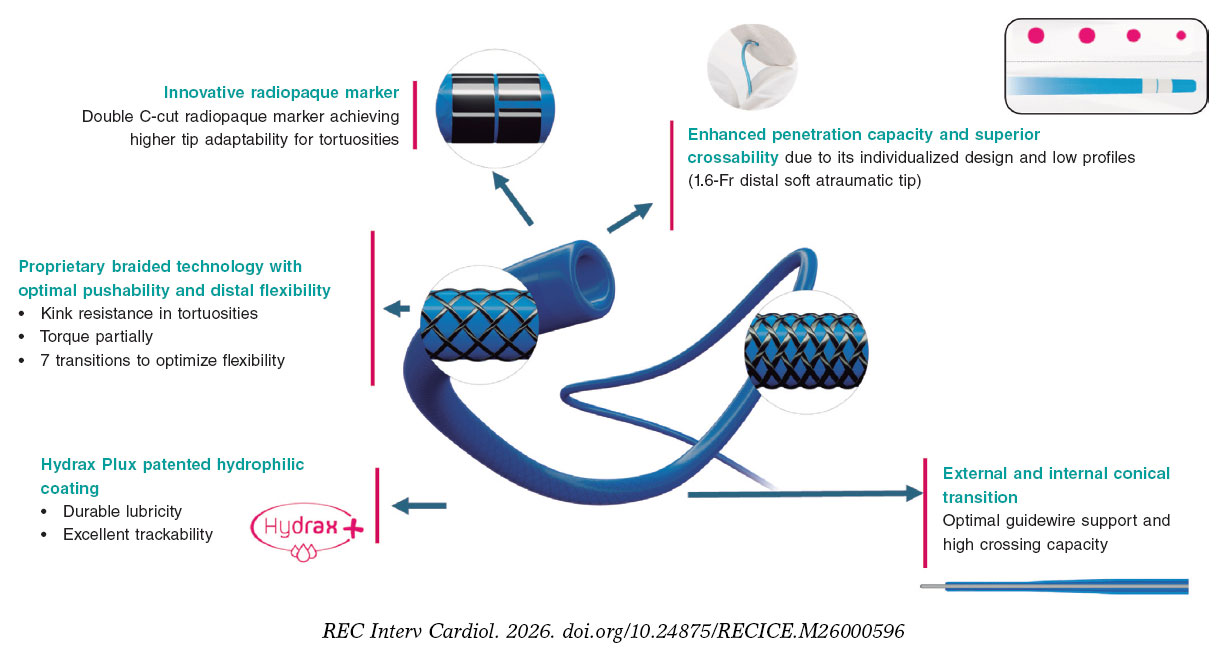
Figure 1. Navitian coronary microcatheter. Schematic representation of the Navitian microcatheter (iVascular, Barcelona, Spain), a rapid-exchange coronary microcatheter designed for use in complex percutaneous coronary intervention. The device features a hydrophilic distal coating to optimize trackability through tortuous and calcified coronary anatomy, a rounded and atraumatic distal tip to reduce the risk of vessel injury during advancement, and radiopaque markers to aid fluoroscopic visualization. The shaft design is intended to provide an optimal balance of pushability, flexibility, and torque transmission for crossing chronic total coronary occlusions and other complex lesions.
Endpoints
The primary device effectiveness endpoint was successful crossing of the target lesion or occlusion with the microcatheter.
Procedural effectiveness was defined as final Thrombolysis in Myocardial Infarction grade-3 flow12 with < 30% residual percent diameter stenosis in the treated segment at the end of the procedure.
Device safety endpoints included the absence of device-related mechanical failures, defined as device rupture, kinking, or complicated device retrieval.
Clinical outcomes were assessed during in-hospital follow-up until discharge and included the occurrence of target lesion failure, defined as the composite of cardiac death, target-vessel myocardial infarction, or clinically driven target lesion revascularization.
Given the sequential dependency inherent to complex PCI and CTO techniques, device effectiveness was assessed only in lesions in which successful guidewire crossing was achieved. Microcatheter performance cannot be meaningfully evaluated in the absence of wire passage; therefore, analyses based on evaluable lesions represent standard practice in CTO and complex PCI studies.
Data collection and monitoring
Data were collected prospectively using a standardized electronic case report form. Remote data monitoring was performed to ensure data completeness and consistency. Cases involving device or procedural failures were subject to targeted review, including source document verification when deemed necessary.
Statistical analysis
Continuous variables are expressed as mean ± standard deviation or median [IQR], as appropriate. Categorical variables are expressed as absolute counts and percentages. The incidence rate of clinical and procedural events is expressed as cumulative incidence during the in-hospital follow-up period.
The planned sample size was based on a noninferiority framework using published benchmarks for device effectiveness,13-15 assuming a reference success rate of 85%, a noninferiority margin of 10%, an alpha level of 0.05, and 80% statistical power.
All analyses were performed using JMP statistical software (version 16; SAS Institute, Cary, NC, United States).
Causality assessment
Causality between adverse events and the study device was assessed based on temporal sequence, inspection of device integrity, procedural context, and operator adjudication. Events occurring after the use of downstream interventional devices, such as balloons or stents, and in the absence of microcatheter malfunction were not considered causally related to the Navitian microcatheter.
RESULTS
Study conduct and population
After approval by the reference ethics committee and local ethics committees, patient enrollment started on 30 September, 2022, and was completed on 11 July, 2024. A total of 102 patients treated across participant centers in Spain and Portugal were included. Overall, 115 coronary lesions were addressed using the Navitian coronary microcatheter.
In 12 patients, the device was used to treat > 1 lesion (11 patients with 2 lesions and 1 patient with 3). Baseline clinical characteristics reflected a population with high cardiovascular risk and complex coronary disease. Table 1 and table 2 summarize the baseline characteristics of patients and lesions.
Table 1. Baseline characteristics
| Variable | Patient-level (n = 102) |
|---|---|
| Age (years) | 68.7 ± 9.9 |
| Male sex | 83 (81.4%) |
| Current/former smokers | 60 (58.9%) |
| Hypertension | 74 (72.5%) |
| Dyslipidemia | 84 (82.4%) |
| Diabetes mellitus | 38 (37.2%) |
| Cerebrovascular/peripheral vascular disease | 15 (14.7%) |
| Chronic kidney disease | 13 (12.7%) |
| Prior percutaneous coronary intervention | 46 (45.1%) |
| Prior coronary artery bypass grafting | 10 (9.8%) |
| Prior myocardial infarction | 37 (36.3%) |
| Multivessel disease | 60 (58.8%) |
| > 1 significant lesion | 60 (58.8%) |
| > 1 lesion treated | 20 (19.6%) |
| Left ventricular ejection fraction (%) | 50.5 [41.2-60] |
| Dual antiplatelet therapy at baseline | 87 (85.3%) |
| Oral anticoagulation at baseline | 22 (21.6%) |
| Clinical presentation | |
| ST-elevation myocardial infarction | 9 (8.8%) |
| Non–ST-elevation myocardial infarction | 34 (33.3%) |
| Stable angina | 44 (43.2%) |
| Silent ischemia | 15 (14.7%) |
|
Data are expressed as No. (%), mean ± standard deviation or median [interquartile range]. |
|
Table 2. Baseline characteristics
| Variable | Lesion-level (n = 115) |
|---|---|
| In-stent restenosis | 8 (11.8%) |
| American Heart Association B2/C lesion | 101 (87.8%) |
| Baseline TIMI grade-0 flow | 56 (48.7%) |
| Ostial lesion | 19 (16.5%) |
| Diffuse disease | 74 (64.3%) |
| Calcified lesion | 54 (47.0%) |
| Bifurcation lesion | 22 (19.1%) |
| Chronic total coronary occlusion | 66 (57.4%) |
| High tortuosity | 19 (16.5%) |
| Reference vessel diameter (mm) | 3.0 [2.5-3.0] |
| Lesion length (mm) | 30 [20-40] |
| Baseline percent diameter stenosis | 100 [90-100] |
| Location | |
| Left anterior descending coronary artery | 47 (40.9%) |
| Left circumflex artery | 15 (13.0%) |
| Right coronary artery | 51 (44.4%) |
| Left main coronary artery | 2 (1.7%) |
|
Data are expressed as No. (%) or median [interquartile range]. |
|
The mean age was 68.7 ± 9.9 years, and 81.4% of patients were male. Relevant comorbidities included diabetes mellitus in 37.2%, chronic kidney disease in 12.7%, and prior myocardial infarction in 36.3%. Previous PCI had been performed in 45.1%, and 21.6% of patients were o chronic oral anticoagulation at the time of the index procedure. Multivessel coronary artery disease was present in 58.8% of patients. Clinical presentation included ST-segment elevation acute coronary syndrome in 8.8% and non–ST-segment elevation acute coronary syndrome in 33.3%.
Lesion and procedural characteristics
Lesion complexity was high. Among the 115 treated lesions, 57.4% were CTOs, 87.8% were classified as American Heart Association type B2/C,16 64.3% showed diffuse disease, and 47.0% exhibited moderate-to-severe calcification. The median lesion length was 30 mm [IQR, 20–40 mm], with a median baseline stenosis of 100%. Lesions with ostial involvement were treated in 16.5% and bifurcation lesions in 19.1%. High vessel tortuosity, considered a key determinant of microcatheter performance, was documented in 16.5% of lesions.
The Navitian microcatheter was used to facilitate guidewire support or advancement in 83.5% of cases, for guidewire exchange after initial wire crossing of very complex lesions in 21.7%, and for distal infusion of contrast, drugs or saline in 6.1%, with overlap of indications in some procedures. Additional support techniques, such as guiding catheter extensions or balloon anchoring, were required in 13.9% of cases.
Device effectiveness and procedural success
Overall, successful crossing of the target lesion or occlusion with the Navitian microcatheter was achieved in 100 of 115 lesions (87.0%). All failed device crossings occurred in CTOs. Among lesions in which guidewire crossing was successfully achieved (n = 105), device effectiveness for lesion or occlusion crossing was 95.2%. In 5 cases, the lesion was successfully wired but the Navitian device could not cross: in 3 cases, no device was able to cross despite multiple attempts; in only 2 cases did another device successfully crossed the lesion, another microcatheter in 1 case and a 1-mm balloon in the other.
All 5 lesions in which the Navitian microcatheter failed to cross were CTOs (100%) located in the right coronary artery (4 of 5) or the first diagonal branch (1 of 5), mostly American Heart Association type C lesions (80%) and de novo (80%). This subgroup showed a high proportion of diffuse disease (80%) and a median lesion length of 32.5 mm [IQR, 28.5–44.75 mm], with moderate- to-severe calcification in 40% and high tortuosity in 40%. In 4 of 5 procedures additional support techniques were required, including a guide catheter extension system in 3 cases, and no device-related technical problems, perforations, dissections or thromboses occurred in this subgroup. Given the small sample size (n = 5), no formal statistical comparison with successfully crossed lesions (n = 100) was performed, but these findings suggest that failures were concentrated in long, diffuse right-coronary CTOs rather than in cases driven by a single identifiable anatomical feature.
In all cases in which the Navitian microcatheter successfully crossed the lesion, procedural success was achieved in 100%, defined as final Thrombolysis in Myocardial Infarction grade-3 flow with < 30% residual percent diameter stenosis in the treated segment.
Device safety and procedural complications
No device-related mechanical failures were observed. Specifically, there were no cases of device rupture, kinking, or complicated device retrieval.
Procedural complications occurred in a limited number of cases and included 3 coronary perforations, all treated with covered stents, 1 coronary dissection of grade C or higher, and 1 probable acute coronary thrombosis. However, the report’s adjudication narrative is important: the 3 perforations occurred after subsequent stent implantation and were managed with covered stents; 1 fatal despite pericardiocentesis and surgery. The probable acute thrombosis occurred after complex left main/left anterior descending coronary artery stenting and drug-coated balloon use, making exclusive attribution to the microcatheter unlikely. The dissection occurred in a failed crossing context in which aggressive CTO wiring, such as with a Pilot 200 guidewire, was used; it had no clinical sequelae.
In-hospital clinical outcomes
The median length of stay was 1 day [IQR, 1–3 days]. Three adverse clinical events were recorded during in-hospital follow-up: 1 target-vessel myocardial infarction and 2 cardiac deaths, 1 following coronary perforation, and 1 following probable acute coronary thrombosis. In all cases, these events occurred after the use of other interventional devices and were not directly attributable to the Navitian microcatheter.
DISCUSSION
In this prospective, multicenter, multinational PMCF study conducted under the requirements of the European Medical Device Regulation (MDR 2017/745), the Navitian coronary microcatheter demonstrated high effectiveness and an excellent device-related safety profile in a real-world population characterized by very high anatomical and clinical complexity. More than half of the treated lesions were CTOs and nearly 90% were classified as American Heart Association type B2/C, closely reflecting contemporary complex PCI practice in high-volume European centers.
Device effectiveness in the context of complex PCI and CTO practice
The primary effectiveness endpoint—successful lesion or occlusion crossing—was achieved in 87% of the total population, and 95.2% of evaluable lesions in which the guidewire successfully crossed, exceeding the 85% benchmark used for PMCF sample size assumptions. Importantly, failure to cross the lesion with the microcatheter was frequently driven by the inability of the guidewire to cross the lesion rather than by microcatheter malfunction. This observation underscores the sequential dependency inherent to complex PCI and CTO interventions and supports the methodological decision to assess device effectiveness only in lesions where guidewire passage was achieved.
When contextualized with published microcatheter experience, these findings appear consistent with contemporary CTO practice (table S1). In the first clinical experience with the NHancer locking microcatheter, Wilson et al.13 reported that the device contributed to at least 1 major procedural step in 85.9% of CTO cases and was the only microcatheter required in 68.4% of successful interventions. While Navitian is not a locking microcatheter, the present PMCF results similarly show that Navitian frequently enabled guidewire support and exchange: it was used for guidewire support in 83.5%, guidewire exchange in 21.7%. Adjunctive backup support, including guide extension or anchor techniques, was required in 13.9% of cases, a figure compatible with escalation patterns described in complex CTO practice.
Sidik et al.15 citer former studies showing procedural success rates in the mid-70% to mid-80% range for CTO-PCI using specialized microcatheters, such as the Corsair series, underscoring that real-world performance depends heavily on lesion complexity, crossing strategy, whether antegrade/retrograde, operator technique, and adjunctive device use.
Registry-based evidence further supports the central role of microcatheters in modern CTO algorithms. Data from contemporary European CTO registries9 indicate overall CTO PCI technical success rates in the range of 85% to 90%, with microcatheter use considered standard practice for wire support, exchange, and escalation strategies. In this context, the performance observed with Navitian aligns with expected outcomes for contemporary coronary microcatheters used in highly complex interventions.
Safety profile and attribution of adverse events
Device safety endpoints were robust: no device fracture, kinking, or difficult withdrawal were reported despite the complexity of the lesions treated. This is a key PMCF reassurance signal for a microcatheter intended for demanding anatomies, particularly in settings in which repeated device exchanges and tortuosity or calcification can increase mechanical stress.
Although 5 procedure-level complications were observed—3 perforations, 1 dissection grade ≥ C, 1 probable acute thrombosis—all the events occurred after the use of additional coronary devices, including guidewires, balloons, and stents, and were not adjudicated as causally related to the microcatheter. These nuances should be explicitly stated in the manuscript because they align with contemporary complex PCI reality: complications often reflect the cumulative risk of the full procedural sequence (wiring, microcatheter manipulation, ballooning, atherectomy/lithotripsy when used, stenting, and optimization), rather than a single device.
Compared with published CTO microcatheter series,13-15 the observed complication profile appears consistent with the underlying risk associated with complex PCI. For example, in an early clinical experience with the NHancer microcatheter,13 Wilson et al. reported a low complication rate, with 1 case of tamponade following guidewire exit that was successfully managed with a covered stent and no reported device failures. Differences compared with the procedural complications observed with Navitian should be interpreted cautiously because a) the Navitian PMCF study included non-CTO complex disease in addition to CTO and reflects broader routine-practice indications, and b) event attribution in the Navitian study points to downstream therapy, particularly stenting, rather than microcatheter malfunction.
Clinical outcomes and regulatory relevance
Three adverse clinical events were recorded during in-hospital follow-up: 1 target-vessel myocardial infarction and 2 cardiac deaths, 1 following coronary perforation, and 1 following probable acute coronary thrombosis. In all cases, these events occurred after the use of other interventional devices and were not directly attributable to the Navitian microcatheter.
Although longer-term clinical outcomes were not assessed, the absence of early device-related safety signals and the favorable procedural success rates provide meaningful evidence supporting the performance of the device under intended-use conditions.
From a regulatory perspective, this study illustrates the value of prospective real-world PMCF investigations in fulfilling MDR 2017/745 requirements.17,18 By generating device-specific evidence in routine clinical practice across multiple centers and countries, such studies complement premarket evaluations and contribute to ongoing benefit–risk assessment throughout the device life cycle. The multinational design further enhances the generalizability of the findings across different European health care environments. Consistent with this approach, prospective multicenter clinical follow-up has recently been applied to other coronary devices for complex PCI, as exemplified by the first-in-man evaluation of the Naviscore scoring balloon for moderate-to-severe calcified lesions.19
Limitations
Some limitations inherent to pragmatic PMCF studies should be acknowledged, such as a) single-arm observational design without a concurrent comparator microcatheter, limiting causal inference; b) heterogeneity of lesion subsets, including CTO and non-CTO complex disease, which enhances generalizability but complicates direct comparison to CTO-only microcatheter series such as NHancer; c) event attribution constraints in complex PCI: complications may be multifactorial and temporally linked to downstream devices or procedural steps, as occurred in this cohort. In addition, angiographic outcomes were site reported and not adjudicated by an independent core laboratory, and formal independent event adjudication was not performed; d) short follow-up and limited to discharge, restricting assessment of longer-term target lesion failure components, particularly repeat revascularization. Clinical follow-up was limited to the in-hospital period. This timeframe reflects the primary endpoint of the present PMCF study, which was to confirm device safety and technical performance under intended-use conditions, in full compliance with MDR 2017/745 requirements, rather than to assess long-term clinical effectiveness; e) standardized definitions for some anatomical features of complex PCI were lacking. No prespecified definition was applied in this study for diffuse disease, significant calcification, or coronary tortuosity; operators classified these characteristics according to their usual angiographic criteria. Several definitions of long or diffuse disease, with lesion length thresholds ranging from 20 mm to ≥ 40 mm have been proposed in the literature, but none was adopted uniformly across centers. This may introduce interobserver variability and should be taken into consideration when interpreting the complexity descriptors of the cohort.
CONCLUSIONS
In a prospective, multicenter, multinational PMCF study conducted under the European MDR framework, the Navitian coronary microcatheter demonstrated high effectiveness, excellent device-related safety, and favorable early clinical outcomes in real-world complex PCI, including CTO interventions. These findings support its continued use in routine practice and provide regulatorily robust evidence of clinical performance across different European health care environments.
FUNDING
This investigator-initiated post-market clinical follow-up study was sponsored by Fundación EPIC, a nonprofit academic organization. An unrestricted grant from the manufacturer of the device, iVascular (Barcelona, Spain) supported the development of the study. However, iVascular had no role in study design, data collection, data analysis, interpretation of the results, or preparation of the manuscript.
ETHICAL CONSIDERATIONS
The study protocol was approved by the Ethics Committee of the Lead Site (Hospital Universitario de León) and by each participant site as required by national regulations. The investigation was conducted in full compliance with the principles outlined in the Declaration of Helsinki, ISO 14155:2020 for clinical investigation of medical devices, the EU Medical Device Regulation (MDR 2017/745), and applicable local laws and regulations for postmarket clinical follow-up studies. Written informed consent was obtained from all participants prior to enrollment. Sex and gender considerations were addressed in accordance with the SAGER (Sex and Gender Equity in Research) guidelines: participants were enrolled consecutively without selection based on sex, and sex-disaggregated baseline characteristics and outcomes are reported where appropriate. The study sample reflects the real-world distribution of patients referred for complex percutaneous coronary intervention during the enrollment period.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
During the preparation of this work the authors used ChatGPT to support language editing and manuscript structuring. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
AUTHORS’ CONTRIBUTIONS
A. Pérez de Prado conceived and designed the study, served as coordinating investigator, supervised data acquisition and analysis, and drafted and critically revised the manuscript. A. Rodrigues, M. Sabaté, I.J. Amat Santos, T. García Camarero, A. Gómez Menchero, and B. García del Blanco served as site principal investigators, contributed to the study design, and participated in patient enrollment, data acquisition, and clinical follow-up. M. López Benito, P. Braga, A. Regueiro, C. Cortés Villar, J. Roa Garrido, and B. Serra Creus participated in patient enrollment, data collection, procedural documentation, and clinical follow-up at the respective sites. J.M. de la Torre-Hernández contributed to the study design, data interpretation, and critical review of the manuscript. All authors reviewed, revised, and approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
CONFLICTS OF INTEREST
J.M. de la Torre-Hernández is editor-in-chief of REC: Interventional Cardiology. A. Pérez de Prado is associate editor of REC: Interventional Cardiology; the journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. A. Pérez de Prado, M. Sabaté, B. García del Blanco, and J.M. de la Torre-Hernández report consulting or speaker fees from iVascular outside the submitted work. The remaining authors declare no conflicts of interest directly related to the subject of this study. The sponsor of the study (Fundación EPIC) received an unrestricted grant from iVascular for the conduct of this postmarket clinical follow-up; iVascular had no role in the study design, collection, analysis or interpretation of data, manuscript preparation, or the decision to submit the manuscript for publication.
WHAT IS KNOWN ABOUT THE TOPIC?
- Microcatheters are essential devices in the current management of complex PCI procedures, such as CTOs or extremely tortuous or calcified anatomies. However, evidence regarding the performance of these devices is currently scarce. With the implementation of the new European Medical Device Regulation (MDR 2017/745), PMCF studies are required to confirm the safety and performance of these products.
WHAT DOES THIS STUDY ADD?
- In a highly complex patient population, the efficacy of the analyzed device, the Navitian microcatheter, as assessed in lesions after guidewire crossing, was > 95%. Procedural success (final Thrombolysis in Myocardial Infarction grade-3 flow with < 30% residual percent diameter stenosis was achieved in all cases in which the device crossed. No safety failures, including rupture, strangulation, or complicated withdrawal, were observed. The rate of adverse clinical events was < 5%; none of the observed events were attributed to the use of the microcatheter.
SUPPLEMENTARY DATA

REFERENCES
1. Achkouty G, Dillinger JG, Sideris G, et al. Microcatheter-Facilitated Primary Angioplasty in ST-Segment Elevation Myocardial Infarction. Can J Cardiol. 2018;34:23–30.
2. Martin-Yuste V, Alvarez-Contreras L, Brugaletta S, Sabate M. Distal side-branch technique:a new use for the Tornus(R) Catheter. Cardiovasc Revasc Med. 2014;15:97–99.
3. Joseph G, Thomson VS, Radhakrishnan S. Corsair microcatheter for retrograde coronary chronic total occlusion recanalization:early experience outside the realm of dedicated recanalization specialists. Indian Heart J. 2012;64:388–393.
4. Mohandes M, Rojas S, Guarinos J, et al. Efficacy and safety of Tornus catheter in percutaneous coronary intervention of hard or balloon-uncrossable chronic total occlusion. ARYA Atheroscler. 2016;12:206–211.
5. Reifart J, Kemala E, Reifart N. Microcatheters for antegrade recanalization of chronic total coronary occlusions:Feasibility and safety of the corsair - A retrospective registry-based single operator experience. Indian Heart J. 2021;73:561–564.
6. Kandzari DE, Grantham JA, Karmpaliotis D, et al. Safety and efficacy of dedicated guidewire and microcatheter technology for chronic total coronary occlusion revascularization:principal results of the Asahi Intecc Chronic Total Occlusion Study. Coron Artery Dis. 2018;29:618–623.
7. Nikolakopoulos I, Choi JW, Alaswad K, et al. Equipment utilization in chronic total occlusion percutaneous coronary interventions:Insights from the PROGRESS-CTO registry. Catheter Cardiovasc Interv. 2021;97: 658–667.
8. Kandzari DE, Alaswad K, Jaffer FA, et al. Safety and efficacy of dedicated guidewire, microcatheter, and guide catheter extension technologies for chronic total coronary occlusion revascularization:Primary results of the Teleflex Chronic Total Occlusion Study. Catheter Cardiovasc Interv. 2022;99:263–270.
9. Vadala G, Galassi AR, Werner GS, et al. Contemporary outcomes of chronic total occlusion percutaneous coronary intervention in Europe:the ERCTO registry. EuroIntervention. 2024;20:e185–e197.
10. Mutlu D, Strepkos D, Ser OS, et al. Traditional Versus Dual Lumen Microcatheter-Assisted Parallel Wiring in Chronic Total Occlusion Percutaneous Coronary Intervention:Insights From the PROGRESS-CTO Registry. Catheter Cardiovasc Interv. 2025;105:1493–1501.
11. Alhusain R, Dayco J, Awadelkarim A, et al. Turnpike Catheter failure, causes and mechanisms:Insights from the MAUDE database. Ann Med Surg (Lond). 2022;78:103923.
12. Chesebro JH, Knatterud G, Roberts R, et al. Thrombolysis in Myocardial Infarction (TIMI) Trial, Phase I:a comparison between intravenous tissue plasminogen activator and intravenous streptokinase. Clinical findings through hospital discharge. Circulation. 1987;76:142–154.
13. Wilson SJ, Maeremans J, Walsh SJ, et al. The first clinical experience with a novel “locking“microcatheter in chronic coronary total occlusions. EuroIntervention. 2017;12:e1883–e1888.
14. Walsh SJ, Dudek D, Bryniarski L, et al. Safety and efficacy of the NovaCross microcatheter in facilitating crossing of chronic total occlusion coronary lesions:a multicenter, single-arm clinical trial. Coron Artery Dis. 2020;31:573–577.
15. Sidik N, McEntegart M, Joshi F, et al. Safety and Effectiveness of a Novel Microcatheter in Coronary Chronic Total Occlusions-The BIOMICS Study. J Soc Cardiovasc Angiogr Interv. 2024;3:102017.
16. Ryan TJ, Faxon DP, Gunnar RM, et al. Guidelines for percutaneous transluminal coronary angioplasty. A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcommittee on Percutaneous Transluminal Coronary Angioplasty). Circulation. 1988;78:486–502.
17. Zubiaur J, Rumoroso Cuevas JR, et al. Medical device research update after the adoption of the EU legislation (MDR). REC Interv Cardiol. 2025; 7:255–263.
18. Spitzer E, de la Torre Hernández JM, Guðmundsdóttir IJ, et al. Use of cardiovascular registries in regulatory pathways:perspectives from the EU-MDR Cardiovascular Collaboratory. REC Interv Cardiol. 2024; 6:213–223.
19. Serra A, Fernández-Peregrina E, Jiménez-Kockar M, et al. New scoring balloon to treat moderate-to-severe calcified coronary lesions. The first-in-man Naviscore study. REC Interv Cardiol. 2025;7:91–98.













