
ABSTRACT
Introduction and objectives: ST-segment elevation myocardial infarction (STEMI) requires early coronary reperfusion to reduce mortality and improve prognosis. In rural areas, timely access to reperfusion therapies, including fibrinolysis or percutaneous coronary intervention (PCI) is frequently constrained by logistical and health care system-related factors.
This study aimed to identify factors associated with delays in reperfusion and those associated with mortality in patients with STEMI code activation in a mountainous European region.
Methods: This is an observational, retrospective, and quantitative study in Alt Pirineu-Aran region (Catalonia, Spain) from 2015 through 2020. Sociodemographic and geographic factors, clinical status, resource management and the treatment provided were analyzed using data from the STEMI code registry and the Catalan emergency medical system.
Results: During the study period, a total of 221 patients with STEMI code were treated in the Alt Pirineu-Aran region. Patients ranged in age from 27 to 96 years, with a mean age of 64.7 years; 72.4% were men. Of these, 47 received fibrinolytic therapy and 173 were transferred to a PCI-capable center, of whom 162 underwent PCI; in 11 cases the code was deactivated. Most patients transferred for PCI experienced delays of > 120 minutes from the diagnostic electrocardiogram. Helicopter transport improved treatment times, with the greatest benefit observed in primary transfers. The 15-day mortality rate was 8.1%.
Conclusions: Most fibrinolysis treatments and PCI were not performed within the times recommended by the European clinical practice guidelines. The study highlights the underutilization of fibrinolysis.
Keywords: ST-segment elevation myocardial infarction. Rural areas. Fibrinolysis. Percutaneous coronary intervention. Mountainous regions. Prehospital care.
RESUMEN
Introducción y objetivos: El infarto agudo de miocardio (IAM) con elevación del segmento ST requiere una reperfusión coronaria precoz para reducir la mortalidad y mejorar el pronóstico. En las zonas rurales, los tiempos de acceso a los tratamientos de reperfusión (fibrinolisis o intervención coronaria percutánea primaria [ICPp]) se ven comprometidos por aspectos logísticos y asistenciales. El objetivo de este estudio es determinar los factores asociados a los retrasos en la reperfusión y los asociados a la mortalidad en pacientes con código IAM en una región montañosa europea.
Métodos: Se realizó un estudio observacional, retrospectivo y cuantitativo en la región del Alt Pirineu-Aran, en Cataluña (España), entre 2015 y 2020. Se analizaron los factores sociodemográficos y geográficos, el estado clínico de los pacientes, la gestión de los recursos y el tratamiento realizado, utilizando los datos del registro del código IAM y del Sistema d’Emergències Mèdiques.
Resultados: Durante el periodo de estudio, 221 pacientes con código IAM fueron atendidos en el Alt Pirineu-Aran. Los pacientes tenían entre 27 y 96 años, con una media de 64,7 años, y el 72,4% eran varones. De ellos, 47 pacientes recibieron fibrinolisis como tratamiento de reperfusión y 173 fueron trasladados a un hospital con unidad de hemodinámica, donde 162 recibieron ICPp; en 11 casos se desactivó el código. La mayoría de los pacientes trasladados para ICPp experimentaron un retraso superior a 120 minutos desde el electrocardiograma diagnóstico. El uso de helicópteros mejoró los tiempos de tratamiento, especialmente en los traslados primarios. La tasa de mortalidad a los 15 días fue del 8,1%.
Conclusiones: La mayoría de las fibrinolisis y de las ICPp no se realizaron dentro de los tiempos recomendados según las guías europeas. Se evidencia una marcada infrautilización de la fibrinolisis.
Palabras clave: Infarto agudo de miocardio con elevación del segmento ST. Zonas rurales. Fibrinolisis. Intervención coronaria percutánea. Zonas montañosas. Atención prehospitalaria.
Abbreviations
AMI: acute myocardial infarction. ECG: electrocardiogram. EMS: Emergency Medical Services of Catalonia. PCI-capable center: percutaneous coronary intervention capable center. pPCI: primary percutaneous coronary intervention. STEMI: ST-segment elevation acute myocardial infarction.
INTRODUCTION
Acute myocardial infarction (AMI) is a medical emergency that requires a rapid response to minimize cardiac damage and improve patient survival. Initial recognition and early treatment based on the optimal reperfusion strategy are key to survival; however, implementing this protocol in rural and mountainous regions is a major challenge.1-4
Primary percutaneous coronary intervention (pPCI) is recommended in all cases provided it can be performed within 120 minutes (ideally in less than 90 minutes).4 If not contraindicated, fibrinolysis is the treatment of choice when this time frame cannot be guaranteed. Contraindications to fibrinolytic therapy may be classified as absolute or relative and should be evaluated on an individual basis. When fibrinolysis is contraindicated, primary angioplasty should be prioritized whenever feasible.1,4 The STEMI code in Catalonia was implemented as a regional health care network in June 2009 designed to organize the management of patients with suspected ST-segment elevation myocardial infarction (STEMI).5,6
Several authors have linked delays in reperfusion treatment to the type of infarction, the timing of symptom onset, and complications.7-9 Other studies suggest that a distance > 50 km to a PCI- capable center is associated with higher mortality rates vs early fibrinolysis.10,11 Other experiences, such as sharing patient data during prehospital care, including electrocardiograms (ECG) and the use of nighttime helicopter transfer to the PCI-capable center have been associated with shorter diagnosis-to-treatment times; however, a reduction in mortality has not been demonstrated.12 However, few studies have analyzed the factors causing delays in mountainous and hard-to-access geographic areas.
The main aim of this study was to determine the factors associated with delays in reperfusion treatment and those associated with mortality in patients treated under the STEMI code in a European mountainous area.
METHODS
Study design
We conducted an observational, retrospective, and quantitative study that included all STEMI code activations in the Alt Pirineu-Aran territory (Catalonia, Spain) from January 2015 through December 2020. The main sources of information were the STEMI code registry of the Department of Health of the Government of Catalonia5,6 and the database of the medical Emergency Medical Services (EMS) of Catalonia, which were cross-referenced to obtain a comprehensive overview. Because the data were derived from preexisting registries and analyzed anonymously, informed consent was deemed unnecessary. The study was approved by the Instituto Universitario de Investigación en Atención Primaria (IDIAP) Jordi Gol Ethics Committee, code CEIm 22/238-P. The SAGER guidelines were followed regarding potential sex and gender bias.
Study setting
Alt Pirineu-Aran is a mountainous region comprising 6 counties and represents 18% of Catalonia’s territory, yet it is home to less than 1% of its population. Population density is extremely low (12.6 inhabitants per km²), and most towns are located between 500 and 800 meters above sea level, far from a specialized hospital center.
This regional health care system faces several challenges. Prehospital care is provided by the EMS, a public service that operates 24 hours per day and provides coverage throughout the entire territory. Each county is served by 1 advanced life support unit, and the region has access to 1 medicalized helicopter, 1 of the 4 operating in Catalonia. Alt Pirineu–Aran includes 4 county hospitals, all of which are non–PCI-capable centers (figure 1).
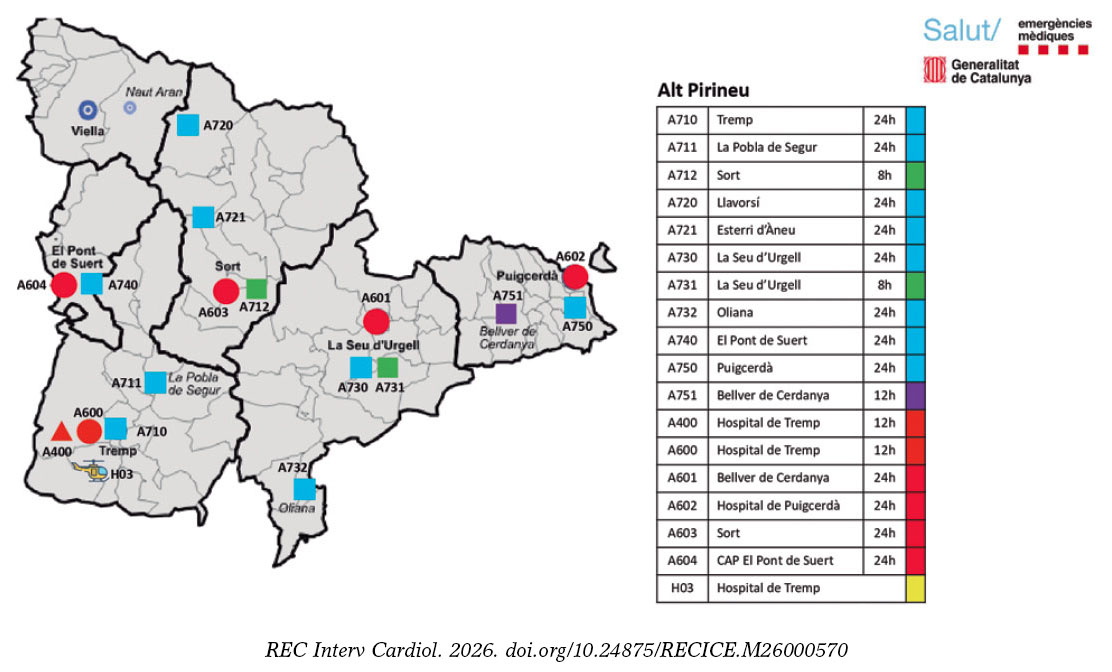
Figure 1. Alt Pirineu-Aran Health Region. H03: Tremp medicalized helicopter. H: county hospitals. Unit call signs are identified with A for Alt Pirineu; 1st number indicates the type of unit (7, basic life support; 4, advanced life support + nurse; and 6, advanced life support + physician); 2nd and 3rd numbers indicate the location of the units on the map.
Hospital Universitario Arnay de Vilanova (Lleida, Spain) serves as the reference center for pPCI for Alt Pirineu-Aran, with the exception of the Cerdanya basic health area, where STEMI code patients are transferred to centers in the Barcelona metropolitan area (table S1).
Definitions and inclusion criteria
The definitions of “delay” used in the study were more than 10 minutes for fibrinolysis administration and more than 120 minutes for pPCI, measured from the time of ECG acquisition. These criteria were established on the basis of former studies and are consistent with current European clinical practice guideline recommendations.1-4
According to EMS protocols, a 90-minute transfer threshold—from ECG acquisition to arrival at the receiving hospital—is used to allow adequate time to perform pPCI and ensure compliance with the 120-minute target. To determine whether patients had a transfer time of less than 90 minutes to a PCI-capable center, a geographic analysis based on distance and estimate travel-time maps was performed.
Patients were included if the STEMI code was activated in Alt Pirineu–Aran and they were attended by EMS during the study period, as well as those who died after prior activation of the STEMI code.
Incomplete cases or those with coding errors were excluded, as were patients transferred to Toulouse (France) from Vall d’Aran.
Study variables
The variables analyzed included demographic, clinical, and logistical data. The primary time intervals assessed were symptom onset to first medical contact, time from first medical contact to ECG, and ECG to initiation of reperfusion treatment. The type of reperfusion strategy (fibrinolysis or pPCI) was recorded as well. Other relevant variables included the location of STEMI code activation, distance to the PCI-capable center, mode of transport to the PCI-capable center (ambulance or helicopter), and type of transfer (primary: direct care and transfer by a medicalized EMS ambulance; secondary: interhospital transfer; or delayed primary: initial assessment by a primary care physician or nurse-staffed ambulance followed by transfer to a medicalized ambulance or medical helicopter). Acute-phase complications and all-cause mortality at first medical contact, and at 24 and 48 hours, and at 15 days were also recorded.
Statistical analysis
The descriptive statistical measures used were absolute and relative frequencies for qualitative variables; mean and standard deviation for quantitative variables with normal distribution; and median and interquartile range for the remaining non-normally distributed quantitative variables, according to the Shapiro-Wilk test.
We analyzed a total of 4 binary outcome variables: use of fibrinolysis as the initial treatment, delays in fibrinolysis (> 10 minutes from ECG acquisition), delays in pPCI (> 120 minutes from ECG acquisition), and mortality. Furthermore, we evaluated associations between each outcome variable and patient- and care-related characteristics using the chi-square test for qualitative variables (or Fisher’s exact test when expected frequencies were < 5), the Mann-Whitney U test for non-normally distributed quantitative variables, and the Student t test otherwise. In addition, we analyzed the importance of variables for treatment delay and mortality using the Boruta algorithm for variable selection. Only variables not rejected by this algorithm were selected for subsequent multivariable analyses to reduce the risk of overfitting. A conditional inference classification tree was constructing using a Monte Carlo test with a minimum terminal node size of 3.
All statistical analyses were performed using R statistical software (R Foundation for Statistical Computing, Austria). P values < .05 were considered statistically significant.
RESULTS
During the study period, a total of 24 125 STEMI codes were activated across Catalonia. The study analyzed 225 cases occurring in Alt Pirineu-Aran, representing less than 1% of the total. Four patients were excluded for not meeting STEMI code criteria (1 pulmonary thromboembolism, 2 coding errors, and 1 duplicate case) (figure 2).
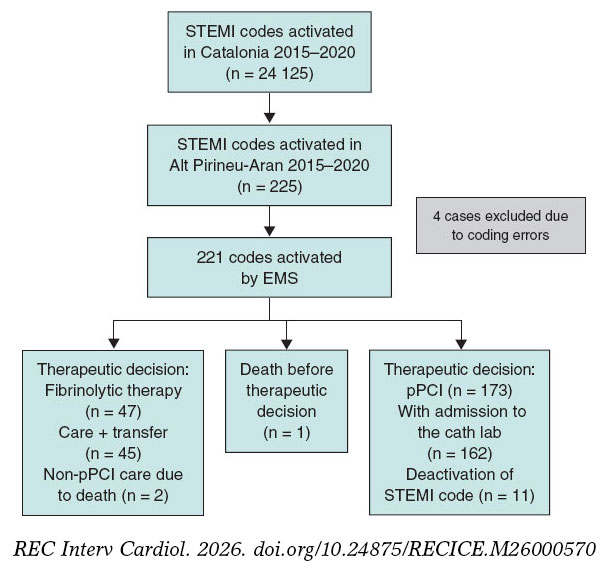
Figure 2. Flow diagram of STEMI codes. AMI, acute myocardial infarction; pPCI, primary percutaneous coronary intervention; EMS, Emergency Medical Services of Catalonia.
The mean age of the 221 included patients was 64.7 years (range, 27–96). Of these, 72.4% were men and 67.4% resided in the study area. All STEMI codes were activated after ECG acquisition at first medical contact, either at a county hospital (51.6%), by EMS at the patient’s home or in a public setting (28.9%), or at a primary care center (19.5%). The median time from first medical contact to ECG acquisition was 6 minutes, and from pain onset to ECG acquisition, 90 minutes (table 1).
Table 1. Clinical characteristics and care times of activated STEMI codes and comparison according to therapeutic decision
| Clinical and care characteristics | Total AMI (n = 221)* | No fibrinolysis (n = 173) | Fibrinolysis (n = 47) | P |
|---|---|---|---|---|
| Female sex | 61 (27.6) | 47 (27.2) | 13 (27.7) | 1 |
| Age (years) | 64.7 (13.7) | 65.7 (13.7) | 60.7 (12.7) | .023 |
| Year | .201 | |||
| 2015 | 30 (13.6) | 25 (14.5) | 5 (10.6) | |
| 2016 | 34 (15.4) | 24 (13.9) | 10 (21.3) | |
| 2017 | 27 (12.2) | 17 (9.83) | 9 (19.1) | |
| 2018 | 35 (15.8) | 27 (15.6) | 8 (17.0) | |
| 2019 | 57 (25.8) | 46 (26.6) | 11 (23.4) | |
| 2020 | 38 (17.2) | 34 (19.7) | 4 (8.51) | |
| Residents in Alt Pirineu i Aran health region | 149 (67.4) | 118 (68.2) | 30 (63.8) | .695 |
| Altitude (m) | 838 [691;1202] | 790 [659;1202] | 974 [691;1202] | .08 |
| Location of first medical contact | .01 | |||
| Primary care center | 65 (29.4) | 57 (32.9) | 8 (17.0) | |
| Home | 20 (9.05) | 18 (10.4) | 2 (4.26) | |
| County hospital | 94 (42.5) | 63 (36.4) | 30 (63.8) | |
| EMS or public setting | 42 (19.0) | 35 (20.2) | 7 (14.9) | |
| Night shift | 56 (25.3) | 34 (19.7) | 22 (46.8) | < .001 |
| Sympton onset–first medical contact time (min) | 80.0 [35.0;193] | 82.0 [39.0;210] | 60.0 [30.0;180] | .292 |
| First medical contact–ECG acquisition time (min) | 6.00 [1.00;12.0] | 6.00 [1.00;12.0] | 5.00 [2.50;12.0] | .807 |
| Sympton onset–ECG acquisition time (min) | 90.0 [45.0;216] | 91.0 [49.0;253] | 80.0 [37.5;192] | .182 |
| Estimated time to PCI-capable center (min) | 106 [93.0;112] | 105 [84.0;109] | 107 [96.0;114] | .061 |
| Estimated time to PCI-capable center ≥ 90 min | 169 (76.5) | 127 (73.4%) | 41 (87.2) | .074 |
| Distance to PCI-capable center (km) | 131 [116;143] | 131 [100;142] | 131 [127;149] | .393 |
| Type of transfer | .036 | |||
| Interhospital | 123 (55.7) | 89 (51.4) | 33 (70.2) | |
| Delayed | 71 (32.1) | 63 (36.4) | 8 (17.0) | |
| Primary | 27 (12.2) | 21 (12.1) | 6 (12.8) | |
| Mode of transport | < .001 | |||
| Ambulance | 106 (48.0) | 69 (39.9) | 36 (76.6) | |
| Helicopter | 56 (25.3) | 49 (28.3) | 7 (14.9) | |
| Ambulance + helicopter | 59 (26.7) | 55 (31.8) | 4 (8.51) | |
| Past medical history | ||||
| Hypertension | 104 (47.1) | 85 (49.1) | 18 (38.3) | .248 |
| Diabetes | 49 (22.2) | 42 (24.3) | 6 (12.8) | .135 |
| Dyslipidemia | 92 (41.6) | 69 (39.9) | 23 (48.9) | .343 |
| Smoking | 63 (28.5) | 47 (27.2) | 16 (34.0) | .458 |
| Previous AMI | 25 (11.3) | 21 (12.1) | 4 (8.51) | .663 |
| Previous pPCI | 25 (11.3) | 22 (12.7) | 3 (6.38) | .34 |
| Stroke | 16 (7.24) | 14 (8.09) | 2 (4.26) | .532 |
| Previous antiplatelet therapy | 40 (18.1) | 35 (20.2) | 5 (10.6) | .194 |
| Treatment and prehospital complications | ||||
| Shock | 8 (3.62) | 5 (2.89) | 2 (4.26) | .643 |
| Ventricular fibrillation | 6 (2.71) | 4 (2.31) | 2 (4.26) | .611 |
| Asystole | 6 (2.71) | 3 (1.73) | 2 (4.26) | .29 |
| Intubation | 7 (3.17) | 4 (2.31) | 2 (4.26) | .611 |
|
AMI, acute myocardial infarction; ECG, electrocardiogram; EMS, Emergency Medical Services of Catalonia; PCI-capable center, percutaneous coronary intervention capable center; pPCI, primary or secondary percutaneous coronary intervention. * Includes 1 patient who died without therapeutic decision. Distribution of totals, no fibrinolysis, and fibrinolysis. Values are expressed as percentage or median. Quantitative variables are expressed as mean (standard deviation) or median [25th percentile; 75th percentile]. |
||||
The incident location had a mean altitude of 838 meters and was located at distances ranging from 81 km to 257 km from the PCI-capable center (median, 131 km). Overall, 76.5% of patients were situated more than 90 minutes from the PCI-capable center (median estimate transfer time, 106 minutes). Air advanced life support was used in 52.5% of the transfers (table 1).
Differences were observed in the time from ECG acquisition to pPCI according to mode of transport (Kruskal-Wallis; P < .001). The median time was 183 minutes for ground ambulance, 138 minutes for helicopter transport, and 140 minutes for combined transport (table 1). Pairwise comparisons using the Mann–Whitney U test showed significant differences compared with ground transport after adjustment for the false discovery rate.
We observed marked variability in the annual frequency of STEMI code cases, with a particularly high number in 2019, and in the proportion of first-assistance fibrinolysis performed from a minimum of 10.5% in 2020 to a maximum of 34.6% in 2017. The number of cases attended in 2020 (the year of the COVID-19 pandemic) was slightly higher than in 2015–2017 (38 cases [17.2%]) but lower than in 2019, which recorded 57 cases (25.8%) (table 1).
Delays in treatment
In 91.5% of patients in whom the therapeutic decision was to perform fibrinolysis at first medical contact, the time between ECG acquisition and treatment exceeded the recommended threshold (> 10 minutes).
When the therapeutic decision was to perform pPCI, the time between ECG acquisition and pPCI exceeded the recommended threshold (> 120 minutes) in 79.6% of cases (table 2).
Table 2. Factors associated with delay in reperfusion treatment
| Clinical and care characteristics | Fibrinolysis (n = 47) | ≤ 10 min | > 10 min | P | pPCI (n = 162) | ≤ 120 min | > 120 min | P |
|---|---|---|---|---|---|---|---|---|
| Female sex | 13 (27.7) | 3 (75.0) | 10 (23.3) | .059 | 45 (27.8) | 6 (18.2) | 39 (30.2) | .245 |
| Age (years) | 60.7 (12.7) | 61.2 (13.8) | 60.7 (12.7) | .943 | 65.3 (13.4) | 65.3 (13.3) | 65.3 (13.5) | 1 |
| Residents in Alt Pirineu i Aran health region | 30 (63.8) | 3 (75.0) | 27 (62.8) | 1 | 109 (67.3) | 22 (66.7) | 87 (67.4) | 1 |
| Altitude (m) | 974 [691;1202] | 946 [649;1202] | 974 [691;1202] | .859 | 692 [640;1202] | 692 [524;957] | 838 [691;1202] | .079 |
| Location of first medical contact | .13 | .014 | ||||||
| Primary care center | 8 (17.0) | 2 (50.0) | 6 (14.0) | 55 (34.0) | 12 (36.4) | 43 (33.3) | ||
| Home | 2 (4.26) | 0 (0.00) | 2 (4.65) | 16 (9.88) | 5 (15.2) | 11 (8.53) | ||
| County hospital | 30 (63.8) | 1 (25.0) | 29 (67.4) | 58 (35.8) | 5 (15.2) | 53 (41.1) | ||
| EMS or public setting | 7 (14.9) | 1 (25.0) | 6 (14.0) | 33 (20.4) | 11 (33.3) | 22 (17.1) | ||
| Night shift | 22 (46.8) | 3 (75.0) | 19 (44.2) | .328 | 31 (19.1) | 1 (3.03) | 30 (23.3) | .017 |
| Symptom onset–first medical contact time (min) | 60.0 [30.0;180] | 190 [180;200] | 57.0 [28.5;152] | .047 | 82.5 [40.0;206] | 60.0 [40.0;116] | 90.0 [40.0;255] | .124 |
| First medical contact–ECG acquisition time (min) | 5.00 [2.50;12.0] | 3.00 [0.75;7.50] | 6.00 [3.00;12.0] | .421 | 6.00 [1.00;11.8] | 6.00 [1.00;10.0] | 6.00 [1.00;12.0] | .75 |
| Symptom onset–ECG acquisition time (min) | 80.0 [37.5;192] | 198 [191;202] | 60.0 [35.0;160] | .05 | 93.5 [50.0;250] | 80.0 [43.0;117] | 115 [57.0;309] | .053 |
| Time to PCI-capable center (min) | 106 (15.9) | 101 (16.2) | 106 (16.0) | .614 | 105 [82.5;110] | 97.0 [71.0;108] | 106 [94.0;111] | .309 |
| Time to PCI-capable center ≥ 90 min | 41 (87.2) | 3 (75.0) | 38 (88.4) | .432 | 118 (72.8) | 19 (57.6) | 99 (76.7) | .047 |
| Distance to PCI-capable center (km) | 131 [127;149] | 132 [123;138] | 131 [127;149] | .969 | 131 [100;143] | 123 [85.0;137] | 131 [123;143] | .085 |
| Type of transfer | .342 | .001 | ||||||
| Interhospital | 33 (70.2) | 2 (50.0) | 31 (72.1) | 83 (51.2) | 8 (24.2) | 75 (58.1) | ||
| Delayed | 8 (17.0) | 1 (25.0) | 7 (16.3) | 59 (36.4) | 18 (54.5) | 41 (31.8) | ||
| Primary | 6 (12.8) | 1 (25.0) | 5 (11.6) | 20 (12.3) | 7 (21.2) | 13 (10.1) | ||
| Mode of transport | 1 | < .001 | ||||||
| Ambulance | 36 (76.6) | 4 (100) | 32 (74.4) | 65 (40.1) | 2 (6.06) | 63 (48.8) | ||
| Helicopter | 7 (14.9) | 0 (0.00) | 7 (16.3) | 48 (29.6) | 18 (54.5) | 30 (23.3) | ||
| Ambulance + helicopter | 4 (8.51) | 0 (0.00) | 4 (9.30) | 49 (30.2) | 13 (39.4) | 36 (27.9) | ||
|
ECG, electrocardiogram; EMS, Emergency Medical Services of Catalonia; PCI-capable center, percutaneous coronary intervention capable center; pPCI, primary or secondary percutaneous coronary intervention. Values are expressed as percentage or median. Quantitative variables are expressed as mean (standard deviation) or median [25th percentile; 75th percentile]. |
||||||||
Among patients located more than 90 minutes from a PCI-capable center who did not receive fibrinolysis at first medical contact, the reason for withholding treatment was not documented in 87 cases (68.5%). Although 76.5% of patients were situated more than 90 minutes from the PCI-capable center, a substantial underuse of fibrinolytic treatment was observed. Of note, patients with a longer time interval from symptom onset to ECG acquisition were more likely to receive fibrinolytic treatment earlier.
Interhospital transfers, incidents without participation of air advanced life support, and nighttime incidents located more than 90 minutes from the PCI-capable center showed greater delays in performing pPCI. Exclusive use of ground ambulance for transfer to the PCI-capable center was associated with a 96.9% rate of delay and emerged as the primary variable in the classification tree for delay between ECG acquisition and pPCI. Among helicopter transfers, delays were more frequent in interhospital transfers (85.4%). In primary or delayed primary transfers, delays were more common when the incident location was more than 90 minutes from the PCI-capable center (65.1%) compared with locations less than 90 minutes away (23.1%) (figure 3).
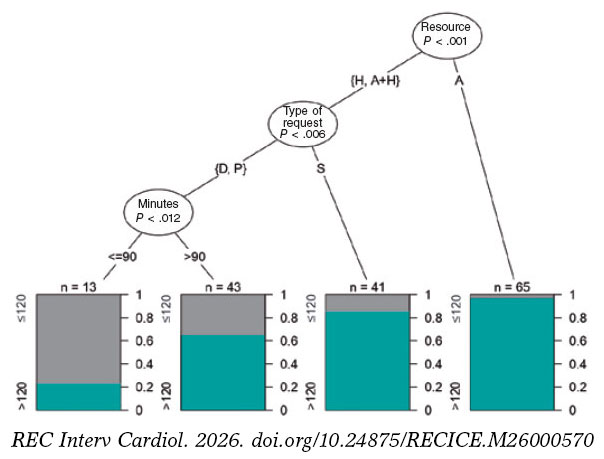
Figure 3. Classification tree for delay in primary percutaneous coronary intervention (pPCI). Three factors were significantly associated with delay: mode of transport (ambulance [A], helicopter [H], or combined use), type of activation (primary [P], delayed [D], or interhospital [S]), and estimated road travel time from the event location to the PCI-capable center in minutes (> 90 minutes < 90 minutes).
Mortality
A total of 18 patients (8.1%) died within the first 15 days. Mortality was significantly higher in patients who experienced a major event (asystole, intubation, shock, or ventricular fibrillation) within the first 24 hours. Age was significantly associated with mortality only at the 48-hour and 15-day follow-up. There were no significant differences in 15-day mortality between patients treated with fibrinolysis and those directly transferred for pPCI. Increased mortality was associated with treatment delays, particularly in the early mortality subgroup (< 24 hours); however, these differences did not reach statistical significance (table 3).
Table 3. Factors associated with mortality according to time from clinical course prior to death
| Clinical and care characteristics | Pre-PCI-capable center (n = 3) | < 24 h (n = 8) | < 48 h (n = 12) | P | ≤ 15 days (n = 18) | P |
|---|---|---|---|---|---|---|
| Female sex | 1 (33.3) | 2 (25.0) | 4 (33.3) | .741 | 6 (33.3) | .587 |
| Age (years) | 67.7 (25.7) | 69.8 (16.0) | 74.4 (15.8) | .047 | 74.1 (14.1) | .008 |
| Residents in Alt Pirineu i Aran health region | 2 (66.7) | 6 (75.0) | 9 (75.0) | .755 | 13 (72.2) | .848 |
| Altitude (m) | 974 [721;1042] | 832 [691;1014] | 691 [468;1014] | .154 | 832 [691;1136] | .625 |
| Location of first medical contact | .337 | .514 | ||||
| Primary care center | 0 (0.00) | 1 (12.5) | 1 (8.33) | 3 (16.7) | ||
| Home | 0 (0.00) | 1 (12.5) | 1 (8.33) | 1 (5.56) | ||
| County hospital | 2 (66.7) | 4 (50.0) | 7 (58.3) | 9 (50.0) | ||
| EMS or public setting | 1 (33.3) | 2 (25.0) | 3 (25.0) | 5 (27.8) | ||
| Night shift | 0 (0.00) | 1 (12.5) | 2 (16.7) | .735 | 4 (22.2) | 1 |
| Symptom onset–first medical contact time (min) | 38.0 [19.0;246] | 64.5 [22.0;488] | 41.0 [22.0;488] | .502 | 65.0 [26.2;413] | .723 |
| First medical contact–ECG acquisition time (min) | 30.0 [17.0;11 542] | 3.00 [0.00;11.2] | 1.50 [0.00;11.2] | .152 | 2.00 [0.00;24.0] | .205 |
| Symptom onset–ECG acquisition time (min) | 42.0 [36.0;11 774] | 66.5 [28.8;682] | 45.0 [30.0;682] | .543 | 81.0 [42.8;518] | .962 |
| Estimated time to PCI-capable center (min) | 96.0 [90.5;113] | 107 [95.8;107] | 96.0 [81.5;107] | .242 | 96.0 [95.0;107] | .432 |
| Estimated time to PCI-capable center ≥ 90 min | 2 (66.7) | 7 (87.5) | 8 (66.7) | .483 | 14 (77.8) | 1 |
| Distance to PCI-capable center (km) | 134 [108;149] | 131 [130;132] | 131 [85.0;131] | .15 | 131 [119;134] | .419 |
| Type of transfer | .911 | .938 | ||||
| Secondary | 2 (66.7) | 4 (50.0) | 8 (66.7) | 11 (61.1) | ||
| Delayed | 1 (33.3) | 3 (37.5) | 3 (25.0) | 5 (27.8) | ||
| Primary | 0 (0.00) | 1 (12.5) | 1 (8.33) | 2 (11.1) | ||
| Mode of transport | .508 | .734 | ||||
| Ambulance | 1 (33.3) | 3 (37.5) | 5 (41.7) | 10 (55.6) | ||
| Helicopter | 1 (33.3) | 1 (12.5) | 2 (16.7) | 3 (16.7) | ||
| Ambulance + helicopter | 1 (33.3) | 4 (50.0) | 5 (41.7) | 5 (27.8) | ||
| Fibrinolytic therapy at first medical contact | 2 (100) | 2 (28.6) | 2 (18.2) | 1 | 4 (23.5) | .764 |
| Delayed fibrinolytic therapy or pPCI | 2 (100) | 7 (100) | 10 (90.9) | .693 | 16 (94.1) | .318 |
| Past medical history | ||||||
| Hypertension | 1 (33.3) | 4 (50.0) | 7 (58.3) | .612 | 11 (61.1) | .317 |
| Diabetes | 1 (33.3) | 2 (25.0) | 3 (25.0) | .731 | 5 (27.8) | .558 |
| Dyslipidemia | 0 (0.00) | 2 (25.0) | 4 (33.3) | .765 | 7 (38.9) | 1 |
| Smoking | 0 (0.00) | 1 (12.5) | 1 (8.33) | .186 | 4 (22.2) | .731 |
| Previous AMI | 0 (0.00) | 1 (12.5) | 2 (16.7) | .631 | 3 (16.7) | .437 |
| Previous pPCI | 0 (0.00) | 1 (12.5) | 2 (16.7) | .631 | 2 (11.1) | 1 |
| Previous stroke | 0 (0.00) | 0 (0.00) | 0 (0.00) | 1 | 1 (5.56) | 1 |
| Prior antiplatelet therapy | 0 (0.00) | 0 (0.00) | 2 (16.7) | 1 | 3 (16.7) | 1 |
| Treatment and prehospital complications | ||||||
| Shock | 2 (66.7) | 3 (37.5) | 4 (33.3) | < .001 | 6 (33.3) | < .001 |
| Ventricular fibrillation | 2 (66.7) | 3 (37.5) | 3 (25.0) | .002 | 3 (16.7) | .008 |
| Asystole | 3 (100) | 5 (62.5) | 5 (41.7) | < .001 | 5 (27.8) | < .001 |
| Intubation | 3 (100) | 4 (50.0) | 4 (33.3) | < .001 | 4 (22.2) | .001 |
|
AMI, acute myocardial infarction; ECG, electrocardiogram; EMS, Emergency Medical Services of Catalonia; PCI-capable center, percutaneous coronary intervention capable center; pPCI, primary or secondary percutaneous coronary intervention. Values are expressed as percentage or median. Quantitative variables are expressed as mean (standard deviation) or median [25th percentile; 75th percentile]. |
||||||
DISCUSSION
In our study, only 20.4% of patients who underwent pPCI received treatment within 120 minutes. Only 4 of the 47 patients treated with fibrinolysis received therapy within 10 minutes.
Several studies, such as the STREAM,13 have shown that prehospital fibrinolysis followed by early pPCI may offer results similar to direct transfer for pPCI if patients are treated within the first 3 hours from symptom onset. In our analysis, we identified underuse of fibrinolytic therapy, along with insufficient documentation of the reasons for withholding treatment.
In contrast to the studies by Stopyra et al.9,14 conducted in North Carolina (United States) in which 60.5% of patients underwent pPCI within ≤ 90 minutes, only 20.4% of patients in our study achieved reperfusion within a broader threshold (< 120 minutes). These findings underscore longer treatment delays in our region and support more frequent consideration of fibrinolytic therapy.
Although Aboal et al.10,11 reported higher mortality rates associated with delayed pPCI, we did not observe a significant association in our study, despite a substantial lower proportion of patients undergoing pPCI within the target time (20.4% vs 42%). In addition, fibrinolysis was more frequently used in patients located more than 50 km from the PCI-capable center (66.7%), reflecting structural and logistical constraints specific to the Alt Pirineu-Aran region that influence treatment selection and reperfusion times.
In line with former evidence regarding mortality, the study results reinforce the clinical importance of time to care as a potential factor associated with worse prognosis, which is particularly relevant in early mortality (< 24 hours).
Compared with the study by Carol et al.,15 in which 58% of patients underwent pPCI after more than 120 minutes, our data show a substantial higher proportion (79.6%). Factors associated with delay, such as intubation, initial shock, and nighttime care, were consistent between the 2 studies; however, other variables, including left bundle branch block, were not. A notable finding of our study is that the care delivered by the EMS was associated with shorter treatment times compared with county hospitals.
Patient origin, geographic location, sex, number of resources involved, time required for therapeutic decision-making, and mode of transport influenced treatment times as well. Hakim et al.16 suggest that helicopter transport is less effective than ground transport, especially for distances of less than 50 km. In our study, 71% of patients transferred by helicopter (all located more than 50 km from the PCI-capable center) received pPCI after more than 120 minutes, which may be associated with the lack of a helipad at the reference PCI-capable center, requiring additional ground transfer, and service hours, mainly daytime during the study period. In constrast to other studies conducted during the COVID-19 pandemic,17,18 our series did not demonstrate a reduction in case volume or prolongation in alert time. However, 2020 was the year with the lowest use of fibrinolysis (4 cases, 10.5%).
Several studies indicate that delays in STEMI recognition and code activation have a direct impact on reperfusion time. One study highlights that training significantly improves these times,19 suggesting that lack of training or skills among professionals may generate delays in care and lower use of fibrinolysis. Our study shows appropriate timing in ECG acquisition and emergency recognition by teams. Delayed primary transfers included the highest percentages of patients with optimal reperfusion times (table 2).
Our findings underscore the need to review and optimize action protocols, particularly in non-PCI-capable centers and geographic areas with greater delays. It is essential to optimize professional response to suspected STEMI, improve therapeutic decision-making time, and explore innovative solutions such as triage systems and STEMI code detection with technological support, optimization of air transport, and greater coordination between PCI and non-PCI capable centers.
Limitations and strengths
This study has limitations due to the small population size in the rural areas studied, which required extending the study period to 6 years to obtain the collected sample. This extension implies that data underwent several changes in record systems (from paper to digitized format) and organizational modifications (implementation of triage in emergency departments and nighttime helicopter flights). The sample of 221 patients remains limited and may have affected the statistical power to detect significant differences between analyzed variables. Similarly, distances from the incident location and estimated average travel times under optimal conditions were used, without accounting for any potential delays due to traffic or other unforeseen factors.
CONCLUSIONS
The results of this study demonstrate the need to increase the use of fibrinolysis in areas distant from a PCI-capable center to reduce reperfusion delays. Documentation of the reasons for not performing fibrinolysis should be improved, as this limits interpretation regarding therapeutic appropriateness. Joint initial care by primary care and emergency teams, as well as delayed primary transfers, reduce reperfusion times and avoid interhospital transfers. Finally, the low number of deaths during the study period prevents multivariate analysis and only allows identification of the variables or characteristics associated with mortality described in the results.
Despite these limitations, the study provides a comprehensive analysis of variables and describes in detail how the investigated population is managed and transferred, something unprecedented in this context. In addition, cross-referencing and thorough review of 2 databases provide valuable information to assess treatment delays. Therefore, this study is a solid basis for future advances in improving STEMI code management in rural areas.
FUNDING
This study was funded by the Provincial Council of Lleida through “The strength of municipalities” project and by IRBLleida through project PP10851 of the Alt Pirineu-Aran Intramural Research Program (IREP).
ETHICAL CONSIDERATIONS
This study was approved by the IDIAP Jordi Gol Ethics Committee, code CEIm 22/238-P. The SAGER guidelines were followed regarding potential sex and gender bias.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
ChatGPT was used to improve the wording of some paragraphs of the article. After using this tool, the authors reviewed and edited the content as necessary and take full responsibility for the final version.
AUTHORS’ CONTRIBUTIONS
M. Navarra Llorens was responsible for study conception and design, overall supervision, and manuscript drafting. M. Martínez Alonso conducted the statistical analysis, interpreted the results, and critically reviewed the content. Y. Azeli was responsible for clinical analysis and critical review. S. Ferrandis Barrés collected data and contributed to the discussion and critical review. M. Canelles Seix collected data and reviewed the manuscript. L. Duch Grau participated in data collection, manuscript review, and final approval. A.M. Forradelles Rey collected data and performed critical review. M.A. Martínez Momblan supervised the project and critically reviewed the manuscript. X. Jiménez-Fàbrega supervised the project and provided intellectual contributions to the discussion. All authors approved the final text.
CONFLICTS OF INTEREST
None declared.
ACKNOWLEDGMENTS
We thank Mar Franch Casanovas and Francisco Iturbe Recasens for their collaboration in data collection, and Isidre Felip for his advice in drafting the manuscript.
WHAT IS KNOWN ABOUT THE TOPIC?
- STEMI requires early coronary reperfusion to reduce mortality and improve prognosis.
- In Catalonia, implementation of the STEMI code has optimized system response; however, in regions such as Alt Pirineu, delays have not been specifically evaluated.
WHAT DOES THIS STUDY ADD?
- This study shows significant underuse of fibrinolytic therapy, even among patients located far from a PCI-capable center. In additions, it highlights the absence of systematic documentation regarding the reasons for withholding fibrinolysis, thereby limiting the evaluation of therapeutic decision-making.
- The study demonstrates that joint initial care by primary care and emergency teams, along with delayed primary transfer, can reduce reperfusion times and avoid interhospital transfers, which are associated with longer delays.
- Similarly, it identifies the mode of transport as the main predictive variable for delay and shows that exclusive use of ground ambulance is the most critical factor.
- Although the low number of deaths prevents a robust multivariate analysis, characteristics associated with mortality are described, and the influence of delays is confirmed, reinforcing the need for adapted strategies.
SUPPLEMENTARY DATA

REFERENCES
1. Ibáñez B, James S, Agewall S, et al. ESC 2017 guidelines on the treatment of acute myocardial infarction in patients with ST segment elevation. Rev Esp Cardiol. 2017;70:1082.e1-1082.e61.
2. Steg G, James SK, Atar D, et al. ESC Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting With ST-Segment Elevation. Rev Esp Cardiol. 2013;66:53.e1-53.e46.
3. Rao SV, O'Donoghue ML, Ruel M, et al. 2025 ACC/AHA/ACEP/NAEMSP/ SCAI Guideline for the Management of Patients With Acute Coronary Syndromes:A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2025;85:2135-2237.
4. Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44:3720-3826.
5. Faixedas MT, Mauri J, Pueyo MJ. The Codi IAM registry:acute myocardial infarction code registry in Catalonia. Rev Esp Cardiol. 2022;75:291-293.
6. Instrucció04/2009, de 12 de maig. Sectoritzacióde l'atencióa les persones malaltes amb infart agut de miocardi (IAM) amb elevaciódel segment ST per tal de portar a terme l'angioplàstia primària. Available at: https:// catsalut.gencat.cat/ca/detalls/articles/instruccio-04-2009-12-maig. Accessed 20 Jan 2026.
7. Rivero F, Bastante T, Cuesta J, et al. Factors Associated With Delays in Seeking Medical Attention in Patients With ST-segment Elevation Acute Coronary Syndrome. Rev Esp Cardiol. 2016;69:279-285.
8. Berga Congost G, Valverde Bernal J, Márquez López A. Factores clínicos predictores de retraso en la actuación del código infarto. Enferm Cardiol. 2017;71:63-71.
9. Stopyra JP, Snavely AC, Ashburn NP, Supples MW, Miller CD, Mahler SA. Delayed first medical contact to reperfusion time increases mortality in rural emergency medical services patients with ST-elevation myocardial infarction. Acad Emerg Med. 2023;30:1101-1109.
10. Aboal J, Núñez M, Bosch D, Tirón C, Brugada R. Angioplastia primaria frente a fibrinolisis en pacientes alejados de un centro con hemodinámica. Emergencias. 2017;29:99-104.
11. Aboal J, Ramos R, Loma-Osorio P, et al. Factores asociados a retrasos de tiempo desde el electrocardiograma diagnóstico hasta el paso de guía en el infarto agudo de miocardio con elevación del segmento ST transferido para angioplastia primaria. Emergencias. 2021;33:195-202.
12. Brunetti ND, Dell'Anno A, Martone A, et al. Prehospital ECG transmission results in shorter door-to-wire time for STEMI patients in a remote mountainous region. Am J Emerg Med. 2020;38:252-257.
13. Van De Werf F, Ristic´AD, Averkov OV, et al. STREAM-2:Half-Dose Tenecteplase or Primary Percutaneous Coronary Intervention in Older Patients With ST-Segment-Elevation Myocardial Infarction:A Randomized, Open-Label Trial. Circulation. 2023;148:753-764.
14. Stopyra JP, Snavely AC, Ashburn NP, et al. Rural EMS STEMI Patients –Why the Delay to PCI?Prehosp Emerg Care. 2024;28:947-954.
15. Carol Ruiz A, Masip Utset J, Ariza-SoléA, et al. Predictors of primary percutaneous coronary intervention delay in cases of myocardial infarction diagnosed in hospitals without hemodynamic support systems. Emergencias. 2021;33:187-194.
16. Hakim R, Revue E, Saint Etienne C, et al. Does helicopter transport delay prehospital transfer for STEMI patients in rural areas?Findings from the CRAC France PCI registry. Eur Heart J Acute Cardiovasc Care. 2020;9:958-965.
17. Romaguera R, Ribera A, Güell-Viaplana F, Tomás-Querol C, Muñoz-Camacho JF, Agudelo V. Decrease in ST-segment elevation myocardial infarction admissions in Catalonia during the COVID-19 pandemic. Rev Esp Cardiol. 2020;73:778-780.
18. Kaddoura R, Salam AM. Thrombosis Management and Challenges in COVID-19 Patients Presenting with Acute Coronary Syndromes. Heart Views. 2020;21:195.
19. Berga Congost G, Brugaletta S, Garcimartin Cerezo P, et al. Effectiveness of a nurse training intervention in the emergency department to improve the diagnosis and treatment of stemi patients:EDUCAMI study. Heart Lung. 2025;70:305-312.












