
Coronary artery vasculitis is a cause of coronary artery disease especially in young patients. Certain inflammatory conditions, such as Kawasaki disease, can trigger this entity. Histological confirmation is challenging, as coronary artery biopsy is not feasible. However, tissue characterization can be achieved using optical coherence tomography (OCT).
In 2014, a 25-years-old male with a past medical history of hypereosinophilic syndrome was referred to our center after an incidental finding of right coronary artery calcification on a computed tomography scan. A coronary angiography revealed the presence of aneurysmal lesions in the right coronary artery (RCA) (figure 1). OCT imaging showed mixed arterial wall abnormalities: a calcified aneurysm (figure 1A), fibrotic intimal thickening with medial disruption and prominent vasa vasorum (figure 1B), calcification (figure 1C), and a less diseased distal vessel (figure 1D). Treatment with acetylsalicylic acid 100 mg daily was initiated.
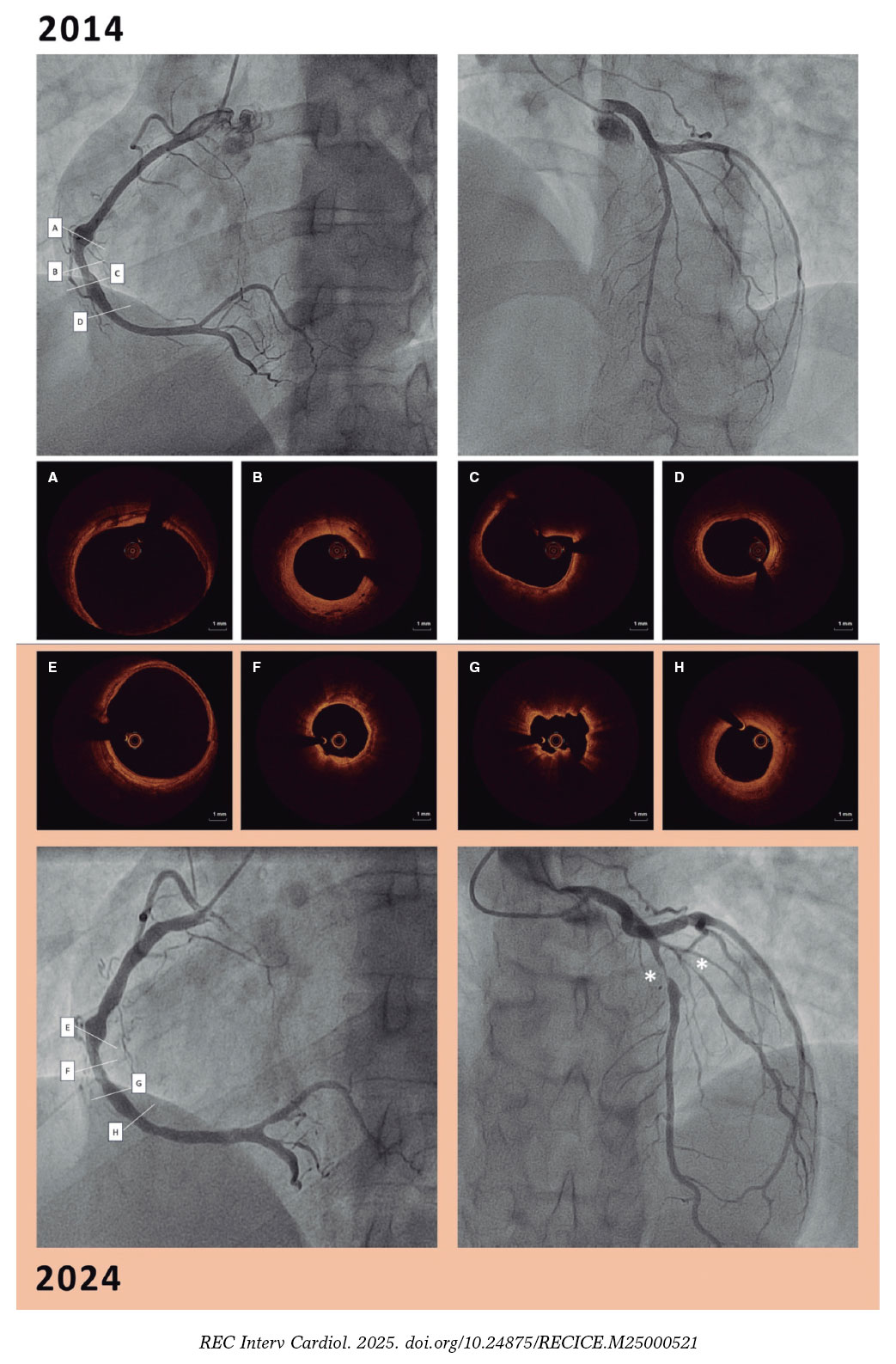
Figure 1.
In 2024, repeat coronary angiography for exertional angina showed RCA disease progression with larger mid-RCA calcification, confirmed by OCT of the same artery segment. Furthermore, the distal segment showed disease progression with intima thickening and medial disruption (figure 1; figure 1E-1H). A new critical stenosis was found in the left anterior descending coronary artery. Furthermore, a biopsy was obtained from an aneurysmal segment of the temporal artery (figure 2). Histopathological findings were similar to those seen on the OCT of coronary arteries. The thickened arterial wall was characterized by fibrous/myofibroblastic intimal hyperplasia, acute inflammatory infiltrate, necrosis, and fibrinoid changes (figure 2A-arrow). Moreover, a loss of the internal elastic lamina (figure 2B-arrow and figure 2A- asterisk) and adventitial vessels confirmed the presence of perivascular chronic inflammation.
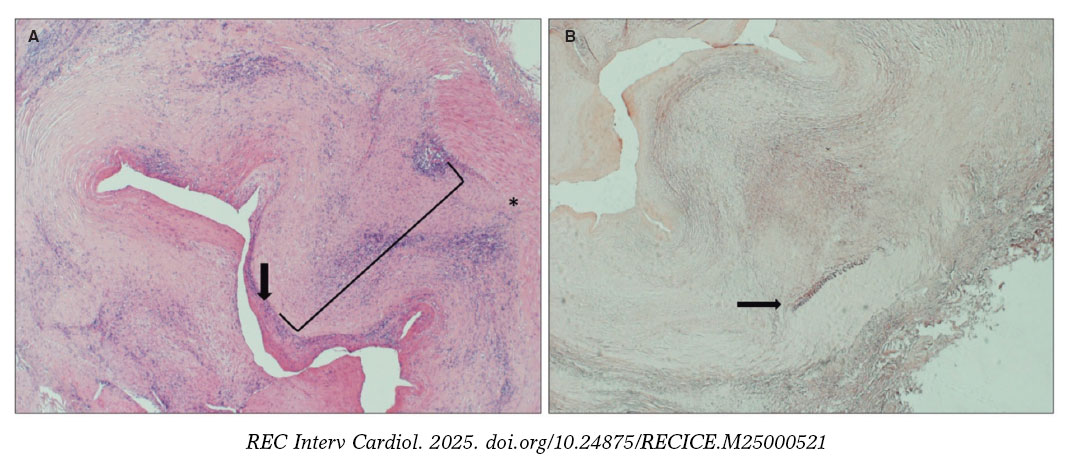
Figure 2.
Based on the symptoms and left anterior descending coronary artery findings (intimal thickening and medial disruption, suggestive of vasculitis; figure 3A, asterisk and arrow), with a healthy distal vessel (figure 3A, double asterisk). A transcatheter coronary intervention with drug-coated balloon was performed (figure 3B).
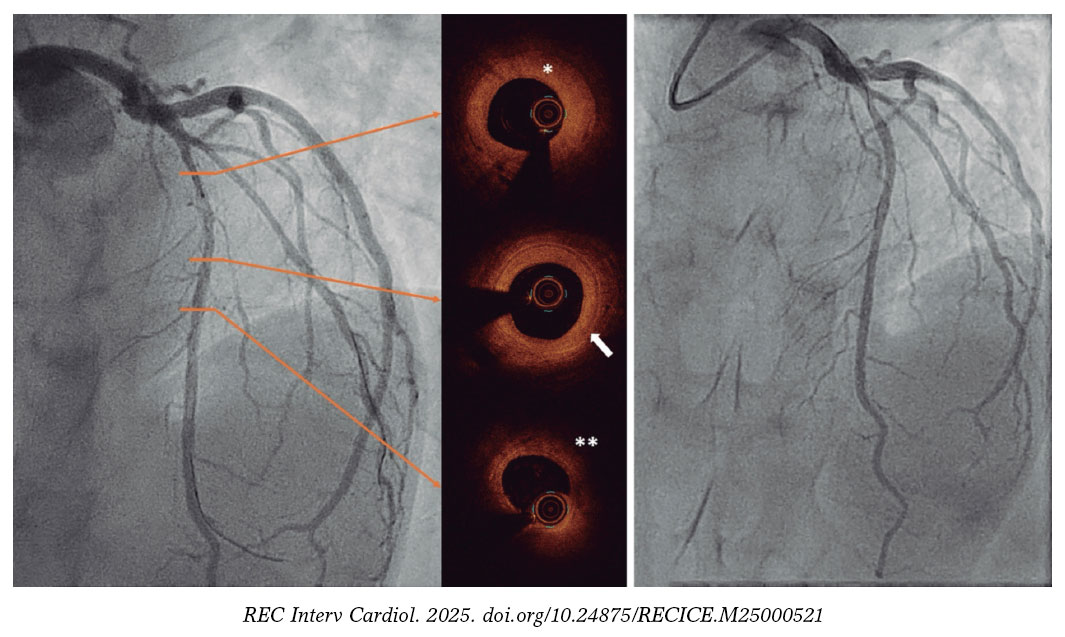
Figure 3.
FUNDING
This was an investigator-initiated study with no funding.
ETHICAL CONSIDERATIONS
The Ethics Committee approval was deemed unnecessary. The patient’s prior written informed consent was obtained for publication of this case report and accompanying images. Variables of sex and gender have been taken into consideration in full compliance with the SAGER guidelines.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
Artificial intelligence was not used in the present manuscript.
AUTHORS’ CONTRIBUTIONS
C. Tejada and J.M. de Alba were the patient’s treating physicians. C. Real, P. Salinas and J.F. Chávez-Solsol were the interventional cardiologists who performed the procedures. Y. Castro analyzed the pathological findings. C. Tejada and C. Real drafted the initial version of this manuscript, which was subsequently revised by P. Salinas. All the authors critically reviewed and approved the final version of the manuscript.
CONFLICTS OF INTEREST
None declared.













