


Original article
Transcatheter mitral edge-to-edge repair vs optimal medical therapy in secondary mitral regurgitation: a meta-analysis
Reparación mitral percutánea de borde a borde frente a tratamiento médico óptimo en regurgitación mitral secundaria: un metanálisis
aFacultad de Medicina, Universidad Autónoma Metropolitana, Mexico City, Mexico bDepartamento de Urgencias y Unidad Coronaria, Instituto Nacional de Cardiología Ignacio Chávez, Mexico City, Mexico cEscuela Superior de Medicina, Instituto Politécnico Nacional, Mexico City, Mexico dFacultad de Medicina, Universidad Católica Boliviana, Santa Cruz, Bolivia eDepartment of Medicine, Indiana University School of Medicine, IN, United States
ABSTRACT
Introduction and objectives: Drug-coated balloons are an emerging stentless therapeutic option for the treatment of de novo coronary artery disease. Although paclitaxel-coated balloons remain the current standard, concerns regarding delayed vascular healing and potential local toxicity have driven the development of sirolimus-eluting balloons (SEB). This study aimed to compare the safety and efficacy profile of the novel SELUTION SLR SEB with the established Pantera Lux paclitaxel-coated balloon in a real-world cohort of patients with de novo coronary artery disease.
Methods: We conducted a prospective, single-center registry included 257 patients with 316 de novo coronary lesions treated with drug-coated balloon–only percutaneous coronary intervention from 2023 through 2024. Patients were treated with either the SELUTION SLR sirolimus-eluting balloon or the Pantera Lux paclitaxel-coated balloon. A 1-year follow-up was conducted to assess major adverse cardiovascular events, target lesion failure (TLF), and target lesion revascularization (TLR), which were descriptively compared across groups.
Results: Baseline clinical and angiographic characteristics were well balanced. At the 1-year follow-up, the overall rate of major adverse cardiovascular events was 5.8%, with no significant differences across treatment groups. The rates of TLF and TLR were low and comparable. However, patients treated with the SELUTION SLR experienced fewer procedural complications, including a lower rate of mild coronary dissections (6.7% vs 14.7%; P = .043) and no-reflow events (0.0% vs 2.7%; P = .036).
Conclusions: The SELUTION SLR SEB demonstrated efficacy vs the Pantera Lux, with fewer procedural complications. These findings support the selective use of SELUTION SLR as a stentless treatment strategy and highlight the need for larger randomized trials to confirm long-term comparative outcomes.
Keywords: Coronary artery disease. Drug-coated balloon. Percutaneous coronary intervention.
RESUMEN
Introducción y objetivos: Los balones farmacoactivos representan una alternativa emergente sin stent para el tratamiento de la enfermedad coronaria de novo. Aunque los balones recubiertos de paclitaxel constituyen el estándar actual, las preocupaciones sobre el retraso en la cicatrización y la toxicidad vascular han favorecido el desarrollo de balones liberadores de sirolimus. El objetivo fue comparar la seguridad y la eficacia del balón liberador de sirolimus SELUTION SLR frente al balón recubierto de paclitaxel Pantera Lux en pacientes con enfermedad coronaria de novo en la práctica clínica real.
Métodos: Registro prospectivo y unicéntrico que incluye 257 pacientes con 316 lesiones de novo tratados mediante intervención coronaria percutánea exclusivamente con balón farmacoactivo entre 2023 y 2024. Los pacientes recibieron SELUTION SLR (sirolimus) o Pantera Lux (paclitaxel). El seguimiento a 1 año evaluó los eventos cardiacos adversos mayores, el fracaso de la lesión diana y la revascularización de la lesión diana, analizados de forma descriptiva.
Resultados: Las características clínicas y angiográficas basales fueron comparables entre los grupos. Al año, la tasa global de eventos cardiacos adversos mayores fue del 5,8%, sin diferencias significativas. El fracaso de la lesión diana y la revascularización de la lesión diana fueron bajos y similares. Sin embargo, el grupo con SELUTION SLR presentó menos complicaciones intraprocedimiento, incluidas disecciones coronarias leves (6,7% frente a 14,7 %, p = 0,043) y fenómenos de no reflujo (0,0 % frente a 2,7 %, p = 0,036).
Conclusiones: El balón liberador de sirolimus SELUTION SLR mostró una eficacia comparable al Pantera Lux, con menos complicaciones intraprocedimiento, lo que apoya su uso selectivo como estrategia sin stent y señala la necesidad de ensayos aleatorizados de mayor tamaño.
Palabras clave: Enfermedad coronaria. Balón farmacoactivo. Intervención coronaria percutánea.
Abbreviations
CAD: coronary artery disease. DCB: drug-coated balloon. DES: drug-eluting stent. PCB: paclitaxel-coated balloon. PCI: percutaneous coronary intervention. SEB: sirolimus-eluting balloon.
INTRODUCTION
Percutaneous coronary intervention (PCI) has revolutionized the treatment of coronary artery disease (CAD), particularly with the advent of drug-eluting stents (DES). However, restenosis, late thrombosis, and very late thrombosis, and the need for prolonged dual antiplatelet therapy have increased interest in no-footprint percutaneous coronary intervention (PCI) strategies like drug-coated balloons (DCBs).1 Initially developed and widely adopted for treating in-stent restenosis, DCBs have more recently gained acceptance for the management of de novo coronary lesions, particularly in small-vessel disease and in patients at high risk of hemorrhage.2,3
Paclitaxel-coated balloons (PCBs) have dominated the field due to drug lipophilicity and potent antiproliferative effect.4 However, concerns regarding delayed vascular healing, cytotoxicity, and downstream embolization have encouraged the development of newer DCB technologies. Sirolimus, by being cytostatic rather than cytotoxic, offers several theoretical advantages over paclitaxel, including a wider therapeutic window, improved endothelial healing, and reduced inflammatory response. However, its low lipophilicity (making tissue retention difficult) and slow onset of action has limited its use in DCB platforms.
The SELUTION SLR (Cordis, United States) aimed to overcome the unfavorable pharmacodynamics of sirolimus by incorporating microreservoirs and a phospholipid coating designed for controlled, sustained release of sirolimus over 90 days. Preclinical and early clinical evidence suggests favorable vessel healing, drug retention, and patency.5 However, comparative data vs paclitaxel-based DCBs in de novo lesions remain limited. Given the evolving landscape of interventional cardiology and increasing interest in no-footprint PCI, a direct head-to-head evaluation of the safety and efficacy profiles of these 2 DCB platforms is warranted.
This study provides a real-world comparison between the SELUTION SLR SEB and the Pantera Lux (Biotronik, Germany) PCB in the management of de novo coronary lesions. By analyzing clinical and angiographic outcomes, we aim to determine whether the novel SEB platform offers a feasible and potentially superior alternative to the current standard of care.
METHODS
Study population
We conducted an analysis of a single-center prospective registry of 257 patients and 316 de novo coronary lesions treated with DCBs from January 2023 through December 2024. Patients presenting with chronic or acute coronary syndrome were eligible if at least 1 lesion was treated with either the SELUTION SLR or the Pantera Lux. The selection of the DCB platform was left to the operator’s discretion. We excluded patients with cardiac arrest or cardiogenic shock and those in whom > 1 brand of DCB was used. In patients with acute coronary syndrome and multivessel disease, complete revascularization was preferably performed in staged procedures to allow for opportunistic angiographic reevaluation of previously treated lesions. Patients were clinically monitored for 1 year and the rates of all-cause mortality, cardiac death, myocardial infarction (MI), unplanned revascularization, target lesion restenosis, and target lesion revascularization (TLR) were compared between the 2 groups. Target lesion failure (TLF) was determined as a composite endpoint of cardiac death, target lesion MI and TLR. Major adverse cardiovascular events (MACE) were defined as a composite endpoint of cardiac death, any MI and any unplanned revascularization. In patients undergoing opportunistic angiographical follow-up, positive vessel remodeling was defined by a ≥ 50% increment in lumen diameter and restenosis as a ≥ 50% lumen reduction. The protocol of the study was revised and approved by the local ethics committee.
Lesion preparation and DCB deployment
All types of coronary lesions were included and aggressive plaque preparation techniques (using scoring or cutting balloons) were incentivized, as was the use of intracoronary imaging to guide balloon size selection and deployment. Only lesions with residual percent diameter stenosis < 30% after optimal preparation and without significant recoil or flow impairment were eligible for DCB inflation. DCBs were selected according to target vessel reference diameter in a 1:1 ratio and had to be inflated for at least 60 seconds. Only 1 inflation per DCB was allowed. Use of multiple DCB was allowed only if the same brand was used. In lesions with persistent residual percent diameter ≥ 30% after aggressive preparation, PCI with DES was recommended. Although post-PCB bailout stenting was recommended only in the presence of flow limiting dissections or persistent contrast staining, the final decision was left to the operator’s discretion.
Statistical analysis
Continuous variables with normal distribution were expressed as mean ± standard deviation, and categorical ones as absolute count and respective percentages. The 95% confidence intervals (95%CI) of the means of continuous variables and percentages of categorical variables were calculated using t tests and Clopper-Pearson (exact) approaches, respectively. The Student t and Mann Whitney U tests were used to compare variables with normal and non-normal distribution, respectively, while the chi-square test was used to compare prevalences across groups. A subgroup analysis stratified by target vessel diameter was performed using a 3-mm lumen diameter cutoff. Kaplan-Meier survival curves were generated for descriptive time-to-event assessment. Due to the low number of events, propensity score weighting, adjusted Cox proportional hazards models, and other multivariable approaches were not performed, as these approaches would be underpowered and potentially yield unreliable or misleading estimates. All analyses used SPSS v30 (IBM, United States). Although statistical significance was defined as P < .05, findings should be interpreted as exploratory.
RESULTS
Study population
A total of 257 patients with 316 coronary lesions were included: 104 patients (133 lesions) treated with SELUTION SLR and 153 patients (183 lesions) treated with Pantera Lux. Baseline demographics and clinical characteristics were balanced across the groups (table 1). There were no significant differences in target vessel location or lesion complexity according to ACC/AHA lesion classification. True bifurcation lesions represented 44.0% of all treated lesions, reflecting the real-world nature and complexity of the cohort (table 2).
Table 1. General characteristics of the study population (per patient analysis)
| Baseline characteristics | Population (N = 257) | SELUTION SLR (n = 104) | Pantera Lux (n = 153) | P |
|---|---|---|---|---|
| Baseline demographics | ||||
| Age (years) | 67.3 ± 11.1 | 67.3 ± 11.4 | 67.3 ± 10.0 | .994 |
| Male | 224 (83.7) | 91 (87.5) | 133 (86.9) | .771 |
| BMI (kg/m2) | 27.0 [22.9-29.4] | 26.2 [24.5-29.2] | 27.0 [24.9-29.6] | .409 |
| Past medical history | ||||
| Prior MI | 138 (53.7) | 54 (51.9) | 84 (54.9) | .678 |
| Prior PCI | 128 (49.8) | 51 (49.0) | 77 (50.3) | .839 |
| Prior CABG | 9 (3.5) | 6 (5.8) | 3 (2.0) | .103 |
| Hypertension | 192 (74.7) | 80 (76.9) | 112 (73.2) | .501 |
| Dyslipidemia | 200 (77.8) | 79 (75.9) | 121 (79.1) | .201 |
| Smoker | 74 (28.8) | 32 (30.8) | 42 (27.5) | .564 |
| Congestive heart failure | 51 (19.8) | 22 (21.2) | 29 (18.9) | .512 |
| Diabetes mellitus | 102 (39.7) | 40 (38.5) | 62 (40.5) | .740 |
| Renal dysfunction | 52 (20.2) | 23 (22.1) | 29 (19.0) | .532 |
| Pulmonary disease | 12 (4.7) | 7 (6.7) | 5 (3.3) | .197 |
| Peripheral arterial disease | 30 (11.7) | 11 (10.6) | 19 (12.4) | .652 |
| Atrial fibrillation/flutter | 18 (7.0) | 7 (6.7) | 11 (7.2) | .888 |
| Family history of CAD | 21 (8.2) | 6 (5.8) | 15 (9.8) | .246 |
| Clinical presentation | ||||
| STEMI | 57 (22.2) | 23 (22.1) | 34 (22.2) | .984 |
| NSTEMI | 77 (30.0) | 26 (25.0) | 51 (33.3) | .152 |
| Unstable angina | 9 (3.5) | 3 (2.9) | 6 (3.9) | .657 |
| CCS | 114 (44.3) | 52 (50.0) | 62 (40.5) | .113 |
| Procedural characteristics | ||||
| Multivessel/segment disease | 205 (79.7) | 86 (82.7) | 119 (77.8) | .650 |
| > 1 lesion treated | 181 (70.4) | 79 (75.9) | 102 (66.7) | .109 |
| No. of treated lesions | 1.0 [1.0-2.0] | 2.0 [1.0-2.0] | 1.0 [1.0-2.0] | .201 |
|
BMI, body mass index; CABG, coronary artery bypass grafting; CAD, coronary artery disease; CCS, chronic coronary syndrome; MI, myocardial infarction; NSTEMI, non-ST segment myocardial infarction; PCI, percutaneous coronary interventions; STEMI, ST-segment elevation myocardial infarction. Data are express as No. (%), mean ± standard deviation or median [interquartile range]. |
||||
Table 2. General characteristics of the target lesion treated (per lesion analysis)
| Vessel/segment | Population (N = 316) | SELUTION SLR (n = 133) | Pantera Lux (n = 183) | P |
|---|---|---|---|---|
| LAD | 141 (44.6) | 56 (42.1) | 85 (46.4) | .331 |
| Proximal LAD | 25 (7.9) | 10 (7.5) | 15 (8.2) | - |
| Mid LAD | 15 (4.7) | 6 (4.5) | 9 (4.9) | - |
| Distal LAD | 31 (9.8) | 11 (8.3) | 20 (10.9) | - |
| First diagonal | 59 (18.7) | 24 (18.0) | 35 (19.1) | - |
| Second or third diagonal | 11 (3.5) | 5 (3.8) | 6 (3.3) | - |
| LCx | 93 (29.4) | 44 (33.1) | 49 (26.7) | .109 |
| Proximal LCx | 20 (6.3) | 8 (6.0) | 12 (6.6) | - |
| Distal LCx | 23 (7.3) | 12 (9.0) | 11 (6.0) | - |
| First obtuse marginal | 37 (11.7) | 16 (12.0) | 21 (11.5) | - |
| Second obtuse marginal | 11 (3.5) | 6 (4.5) | 5 (2.7) | - |
| Third obtuse marginal | 2 (0.6) | 2 (1.5) | 0 (0.0) | - |
| Intermediate branch | 9 (2.8) | 3 (2.3) | 6 (3.3) | .743 |
| RCA | 70 (22.2) | 29 (21.8) | 41 (22.4) | .828 |
| Proximal RCA | 8 (2.5) | 3 (2.3) | 5 (2.7) | - |
| Mid RCA | 9 (2.8) | 2 (1.5) | 7 (3.8) | - |
| Distal RCA | 15 (4.7) | 6 (4.5) | 9 (4.9) | - |
| PDA | 21 (6.6) | 10 (7.5) | 11 (6.0) | - |
| Postero-lateral branch | 17 (5.4) | 8 (6.0) | 9 (4.9) | - |
| CABG | 3 (0.9) | 1 (0.8) | 2 (1.0) | .901 |
| Arterial graft | 1 (0.3) | 0 (0.0) | 1 (0.5) | - |
| Venous graft | 2 (0.6) | 1 (0.8) | 1 (0.5) | - |
| Lesion characteristics | ||||
| Target vessel diameter ≥ 3 mm | 59 (18.7) | 23 (17.2) | 36 (19.7) | .384 |
| AHA class A | 93 (29.4) | 39 (29.3) | 54 (29.5) | .911 |
| AHA class B1/B2 | 195 (61.7) | 83 (62.4) | 112 (61.2) | .873 |
| AHA class C | 28 (8.9) | 11 (8.3) | 17 (9.3) | .795 |
| CTO | 29 (9.2) | 14 (10.5) | 15 (8.2) | .479 |
| True bifurcation | 139 (44.0) | 61 (45.9) | 78 (42.6) | .559 |
|
AHA, American Heart Association; CABG, coronary artery bypass graft; CTO, chronic total coronary occlusion; LAD, left anterior descending coronary artery; LCx, left circumflex artery; PDA, posterior descending artery; RCA, right coronary artery. Data are expressed as No. (%). |
||||
Procedural characteristics
Lesion preparation details are shown in table 3. Most lesions were prepared with non-compliant (NC) balloons (82.0%). Intracoronary imaging to guide PCI was used in 25.9% of cases. There were no differences in mean DCB diameter (2.25 [2.00-2.50] vs 2.25 [2.00-2.50] for SELUTION SLR and Pantera Lux, respectively, P = .205) and the mean DCB length (20.0 [15.0-25.0] vs 20.0 [15.0-29.0], for SELUTION SLR and Pantera Lux, respectively, P = .432). Nearly one-third (n = 100, 31.6%) of all DCB utilization occurred in the setting of hybrid bifurcation PCI (DES in the main branch plus DCB in the side branch), reflecting the increasing adoption of this strategy to avoid 2-stent PCI technique outside of the left main coronary artery. SELUTION SLR was used more frequently than Pantera Lux in pure DCB bifurcation PCI (DCB in both the main and side branches) (15.7% vs 9.8%, for SELUTION SLR and Pantera Lux, respectively; P = .012).
Table 3. Lesion preparation, devices used for PCI and procedural results (per lesion analysis)
| Devices used and procedural results | Population (N = 316) | SELUTION SLR (n = 133) | Pantera Lux (n = 183) | P |
|---|---|---|---|---|
| Predilatation | ||||
| SC balloon | 66 (20.9) | 29 (21.8) | 37 (20.2) | .732 |
| NC balloon | 259 (82.0) | 110 (82.7) | 149 (81.4) | .769 |
| Plaque preparation/calcium modification | ||||
| Cutting/scoring balloon | 62 (19.6) | 27 (20.3) | 35 (19.1) | .907 |
| Rotational atherectomy | 2 (0.6) | 1 (0.8) | 1 (0.5) | .820 |
| Orbital atherectomy | 9 (2.8) | 4 (3.0) | 5 (2.7) | .885 |
| IVL | 7 (2.2) | 3 (2.3) | 4 (2.2) | .898 |
| Intracoronary imaging | ||||
| IVUS | 70 (22.2) | 28 (21.1) | 42 (23.0) | .792 |
| OCT | 12 (3.8) | 6 (4.5) | 6 (3.3) | .789 |
| PCI | ||||
| DCB diameter | 2.25 [2.00-2.50] | 2.25 [2.00-2.50] | 2.25 [2.00-2.50] | .205 |
| DCB length | 20.0 [15.0-25.0] | 20.0 [15.0-25.0] | 20.0 [15.0-29.0] | .432 |
| PCI with DES in a different lesion | 181 (57.3) | 76 (57.1) | 105 (59.7) | .480 |
| Hybrid bifurcation PCI (DES + DCB) | 100 (31.6) | 43 (32.3) | 57 (31.1) | .703 |
| DCB-only bifurcation PCI | 39 (12.3) | 21 (15.7) | 18 (9.8) | .012 |
| Procedural results | ||||
| Post-DCB residual percent diameter stenosis > 30% | 19 (6.0) | 11 (8.4) | 8 (4.8) | .201 |
| Mild dissection (type A-B) | 36 (11.4) | 9(6.7) | 27 (14.7) | .043 |
| Severe dissection (type C-F) | 3 (0.9) | 0 (0.0) | 3 (1.6) | .370 |
| Coronary perforation | 2 (0.6) | 1 (0.8) | 1 (0.5) | .820 |
| Coronary rupture | 2 (0.6) | 1 (0.8) | 1 (0.5) | .820 |
| No-reflow | 5 (1.6) | 0 (0.0) | 5 (2.7) | .036 |
| Bailout DES | 31 (9.8) | 9 (6.8) | 22 (12.0) | .121 |
| Procedural mortality | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
|
DCB, drug-coated balloon; DES, drug eluting stent; IVL, intravascular lithotripsy; IVUS, intravascular ultrasound; NC, non-compliant; OCT, optical coherence tomography; PCI, percutaneous coronary intervention; SC, semi-compliant. Data are expressed as No. (%), mean ± standard deviation or median [interquartile range]. |
||||
Several important differences emerged in procedural findings. Mild coronary dissections, defined as non–flow-limiting dissections of types A–B and considered expected angiographic findings after preparation or DCB inflation, occurred significantly more often in the Pantera Lux than in the SELUTION SLR group (14.7% vs 6.7%; P = .043). Severe dissections were rare. There were no-reflow phenomena exclusively in the Pantera Lux group, with 5 cases being reported overall, corresponding to 1.6% of all lesions (0.0% vs 2.7% within each respective treatment group; P = .036). There were no periprocedural deaths in either arm.
1-year clinical outcomes
Clinical follow-up at 12 months was available for all patients, whereas angiographic follow-up was performed in 35.4% of lesions (n = 91) at the operator’s discretion and was not protocol mandated. At the patient level, the overall rates of adverse clinical events were low (table 4). All-cause mortality occurred in 2.3% of patients, cardiovascular mortality in 1.6%, and myocardial infarction in 2.3%. The composite MACE rate was 5.8% overall, with no statistically significant difference between SELUTION SLR and Pantera Lux (2.9% vs 7.8%; P = .168). At the lesion level, TLF occurred in 3.8% of lesions, again without significant differences being reported across groups (2.3% vs 5.8%; P = .252). TLR was rare, recorded in 0.9% of lesions, with no difference across devices. Figure 1 illustrates the respective Kaplan-Meier survival curves for MACE, cardiac death and MI.
Table 4. Events at the follow-up
| Outcomes | Population | SELUTION SLR | Pantera Lux | P |
|---|---|---|---|---|
| Patient oriented outcomes | N = 257 | n = 104 | n = 153 | |
| All-cause mortality | 6 (2.3) | 1 (0.9) | 5 (3.2) | .574 |
| Cardiac death | 4 (1.6) | 1 (0.9) | 3 (1.9) | .410 |
| Myocardial infarction | 6 (2.3) | 1 (0.9) | 5 (3.2) | .574 |
| UR for angina | 5 (1.9) | 1 (0.9) | 4 (2.6) | .630 |
| MACE (cardiac death + MI + UR) | 15 (5.8) | 3 (2.9) | 12 (7.8) | .168 |
| Lesion oriented outcomes | N = 316 | n = 133 | n = 183 | |
| TLF (CV death + target vessel MI + TLR) | 12 (3.8) | 3 (2.3) | 9 (5.8) | .252 |
| Target lesion revascularization | 3 (0.9) | 1 (0.8) | 2 (1.1) | .721 |
| Angiographic control | N = 91 | n = 34 | n = 57 | |
| Restenosis (> 50% diameter) | 7 (7.7) | 1 (2.9) | 6 (10.5) | .229 |
| Positive remodeling (> 50% lumen gain) | 22 (24.2) | 12 (35.3) | 10 (17.5) | .097 |
|
MACE: major adverse cardiovascular events; MI, myocardial infarction; TLR, target lesion revascularization; UR: unplanned revascularization. Data are expressed as No. (%). |
||||
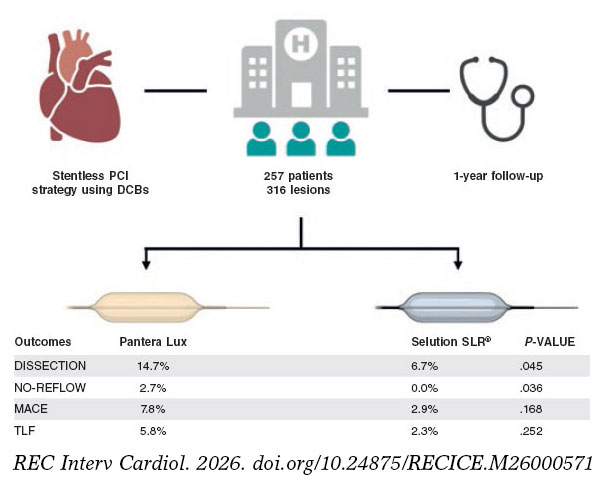
Figure 1. Kaplan Meier survival curves for MACE (A), CV death (B) and MI (C) after 1 year follow-up. CV, cardiovascular; DCB, drug-coated balloon; MACE, major adverse cardiac events; MI, myocardial infarction.
Among the lesions that underwent repeat angiography, restenosis was diagnosed in 7.7% of cases, with no meaningful differences across the different balloon types. Positive vessel remodeling was numerically more common in SELUTION SLR-treated lesions (35.3% vs 17.5%; P = .097), although the sample was limited due to the opportunistic nature of follow-up.
A subgroup analysis according to reference vessel diameter showed that 18.7% of lesions were treated in vessels ≥ 3 mm (table S1). From a procedural standpoint, large arteries did not exhibit higher rates of mild (types A and B) dissections (18.6% vs 10.1%; P = .066) but higher rates of bailout stenting (18.6% vs 7.8%; P = .011) (reasons for stent bailout are summarized in table S2). Despite this, there were no differences in safety outcomes such as severe dissection, coronary rupture, or no-reflow. Moreover, lesion-oriented outcomes, including TLF and TLR rates, were low and comparable across groups. Of note, only 1 TVF event was registered in the large artery group, in 1 patient treated with Pantera Lux. These subgroup observations should be interpreted as exploratory because the study was not powered for interaction testing and event rates were low.
DISCUSSION
In this prospective, real-world registry comparing the SELUTION SLR sirolimus-eluting balloon with the Pantera Lux paclitaxel-coated balloon for the treatment of de novo coronary lesions, the 2 devices demonstrated low and comparable clinical event rates at 12 months (figure 2). The study population included complex, all-comer patients, and despite the inherent limitations of a single-center observational design, the findings contribute to the growing body of evidence supporting DCB strategies for selected de novo lesions.
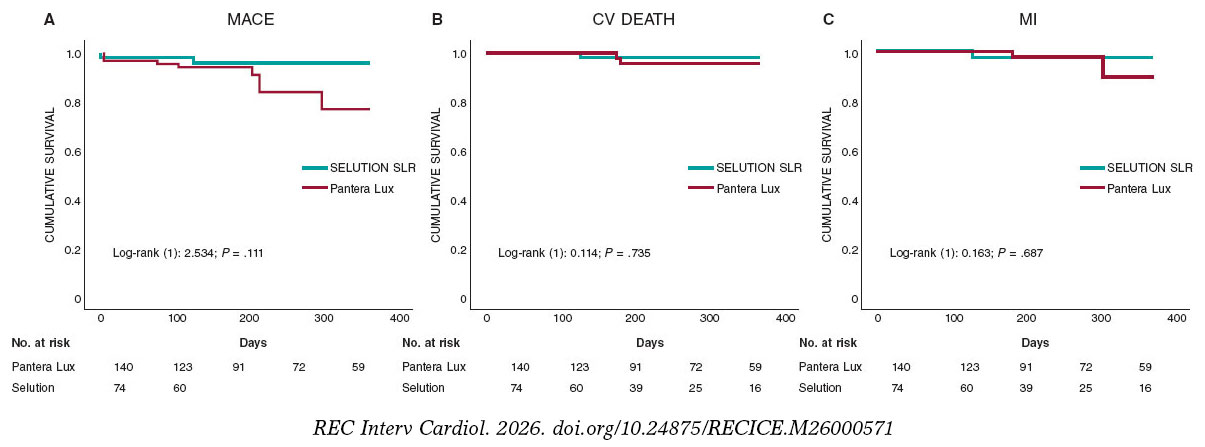
Figure 2. Central illustration. Study design and main outcomes. A total of 257 patients with 316 de novo coronary lesions were treated using a stentless percutaneous coronary intervention strategy with paclitaxel-coated balloon and 1-year follow-up. Outcomes were compared between the Pantera Lux paclitaxel-coated balloon and SELUTION SLR sirolimus-eluting balloon. SELUTION SLR was associated with fewer procedural complications, including lower rates of coronary dissection and no-reflow, with comparable clinical outcomes at follow-up. CV, cardiovascular; MI, myocardial infarction; MACE, major adverse cardiovascular events; PCI, percutaneous coronary intervention; TLF, target lesion failure.
The results of our study offer important insights into the real-world performance of sirolimus-DCB, particularly the novel SELUTION SLR platform, in the management of de novo coronary lesions. The findings are 2-fold: first, the SELUTION SLR demonstrated a safety and efficacy profile comparable to that of an established PCB; and second, overall, outcomes were consistent across vessel diameters, with no significant reduction in performance observed between small- and large-caliber arteries.
The principal observation of the present analysis is that SELUTION SLR yielded clinical outcomes similar to those obtained with the Pantera Lux, while being associated with fewer procedural findings such as mild, non–flow-limiting dissections, and no-reflow phenomena. This finding may reflect differences in mechanical interaction or coating characteristics between the 2 platforms. However, because factors such as lesion preparation, severity of calcification, balloon-to-artery ratio, and operator technique strongly influence dissection rates—and were neither controlled nor adjusted for in this analysis—this interpretation remains speculative. Furthermore, mild angiographic type A–B dissections are widely regarded as expected and benign features of DCB angioplasty, provided TIMI grade-3 flow is maintained and no significant recoil is present. Recent consensus documents indicate that such dissections rarely require stenting and may even facilitate drug transfer. Of note, all 5 cases of no-reflow occurred in Pantera Lux–treated lesions, an observation consistent with prior preclinical and clinical work documenting the embolic behavior of crystalline paclitaxel particles.6 Although this mechanistic explanation is biologically plausible, further studies in humans are required to confirm this association. Given the small number of events observed in both groups, the clinical relevance of these findings remains uncertain.
Paclitaxel has remained the backbone of DCB therapy for CAD for over a decade, primarily due to its lipophilic properties, rapid tissue uptake, and strong antiproliferative effects.7 However, emerging concerns regarding delayed healing, potential toxicity, and long-term safety have prompted the development of balloons with alternative antiproliferative agents.8 Sirolimus, although more hydrophilic and requiring innovative delivery systems to ensure sustained arterial wall absorption, has demonstrated superior biocompatibility, endothelial healing properties, and reduced inflammatory responses in both preclinical and early clinical settings. Nonetheless, the results from the TRANSFORM I trial were disappointing.9 By not being as cytotoxic, it became clear from this trial that platforms using sirolimus had to ensure sustained drug delivery to the artery over a long period of time and become a “drug-eluting balloon” rather than a “drug-coated balloon”. Hence, the SELUTION SLR incorporates a proprietary micro-reservoir technology with biodegradable polymers to facilitate sustained sirolimus release over 60–90 days, aiming to mimic the drug release kinetics of second-generation DES, and ensure drug activity over the traditional restenosis cycle period of coronary arteries after balloon barotrauma9,10.
In our study cohort comprising both small and large vessels, the procedural success and short-term lesion-oriented outcomes, namely TLF and TLR, were low and statistically similar between the SELUTION SLR and the Pantera Lux platforms. These observations are consistent with data from the PRESTIGE trial, which have demonstrated non-inferior late lumen loss (LLL) and binary restenosis rates with SELUTION SLR vs a paclitaxel DCB in a smaller cohort of patients including de novo lesions and in-stent restenosis.11 We reported very low rates of TLR (0.9% of treated lesions). We believe this finding is likely multifactorial. First, this was a selected population in which most treated vessels were small (< 3.0 mm). In small vessels, the amount of myocardium at risk is limited, and both procedural failures and late vessel occlusions may remain clinically silent and therefore undetected. In our subgroup analysis, we did not find any differences in TLR between small and larger vessels, however, our sample size is underpow- ered to detect such differences. Notably, in the REC-CAGEFREE I trial, the higher event rates observed in larger vessels ultimately drove the trial results.12 Second, angiographic follow-up was not mandated by protocol, and we acknowledge that asymptomatic restenosis or late vessel occlusion may have gone undetected and may or may not be equally distributed across treatment groups.
The bulk of the existing evidence favoring PCB comes from large randomized trials such as the PEPCAD II, the FEMPAC, and the BELLO, which provided robust comparative data across various lesion subsets and anatomical territories.13-15 However, PCB are not without limitations, including concerns regarding late thrombotic events, dose-dependent cytotoxicity, and secondary vasomotor and endothelial dysfunction.16 In fact, the toxicity profile of PCB was made evident in patients who were treated for chronic total coronary occlusions (CTO) and demonstrated post-PCI late coronary aneurysms, either due to > 1 PCB being applied in the same territory, as paclitaxel has a very narrow therapeutic window, or by having the drug delivered in false lumen segments and being directly applied to the vascular smooth muscle cell layer.17 Moreover, animal studies have shown that, while PCB and SEB have been shown to equally reduce neointimal formation, medial muscle cell layer loss was greater with PCB, underscoring their higher toxicity profile.16 Furthermore, various reports have noted the occurrence of paclitaxel crystal embolization into distal vascular territories after balloon inflation both in peripheral and myocardial tissues.18,19 This phenomenon might help explain the increased occurrence of no-reflow in the PCB group in our study.
The differential performance of DCBs in small vs large coronary arteries is another critical consideration. Traditionally, small vessels have posed a greater challenge for DES due to increased risk of restenosis, higher neointimal proliferation, and limited expansion capacity.20 By avoiding permanent implants and associated foreign body responses, DCBs are ideally suited for small vessel interventions. Our analysis confirms this advantage, with low rates of TLF and TLR being reported in small arteries, and no significant increase in procedural complications vs larger vessels. In fact, the overall MACE rate at the 1-year follow-up was 5.8%, which is well within the margins of current DES platforms, with 1 exception being the FireBird stent in the REC-CAGEFREE I trial. In this trial, patients with de novo coronary lesions treated with PCB (Swide, Shenqi Medical, China) exhibited a 2-year MACE rate of 6.4%, while patients treated with the FireBird stent, a sirolimus eluting stent, exhibited a 2-year MACE rate of 3.4%, well under the expected rate for DES platforms.12 The good performance of DES in this study was likely due to the inclusion of simple lesions and high rates of plaque modification techniques before stenting (scoring and cutting balloons being used in > 60% of cases), suggesting that good plaque preparation not only is fundamental for DCB PCI outcomes, but also seems to improve them in the context of DES PCI.
Interestingly, the large vessel subgroup in our cohort demonstrated a higher rate of bailout DES implantation (18.6% vs 7.8%; P = .011), despite comparable pre-treatment angiographic severity and lesion characteristics. This finding may reflect either a procedural bias—operators may be more inclined to stent larger vessels when faced with apparently suboptimal DCB results—or true differences in biomechanical response and vessel wall compliance between vessel calibers. Nevertheless, these findings did not translate into differences in safety endpoints or short-term clinical outcomes, highlighting the procedural adaptability and safety of the DCB-only approach in larger arteries when managed judiciously.
In the SELUTION DeNovo trial (NCT04859985),21 a strategy using the SELUTION SLR sirolimus-eluting balloon with provisional stenting achieved a 1-year TVF rate of approximately 5.3% vs 4.4% in the systematic DES arm, meeting the prespecified non-inferiority margin. Notably, nearly 80% of patients randomized to the SELUTION arm were successfully treated without any stenting, reinforcing the feasibility of a “leave-nothing-behind” approach in appropriately prepared de novo lesions. These results are consistent with the observations of our registry, where SELUTION SLR demonstrated comparable clinical outcomes to its direct PCB comparator, Pantera Lux, along with fewer procedural disturbances such as mild dissections and no-reflow. While the SELUTION DeNovo findings support the safety and efficacy profile of SELUTION in a controlled randomized environment,21 it is important to note that the trial included carefully selected patients—excluding left main disease, STEMI, CTO, and other high-risk anatomies—whereas our registry reflects real-world lesion complexity and operator-driven device selection. Consequently, although the procedural and clinical performance of SELUTION in this study appears directionally consistent with DeNovo, extrapolation should remain cautious given differences in inclusion criteria, lesion profiles, and the non-randomized nature of our dataset. Together, both datasets reinforce the potential of SELUTION SLR as a viable stentless strategy, while highlighting the need for further randomized clinical trials with broader inclusion criteria and extended follow-up to determine long-term durability > 1 year. Larger, randomized trials with extended clinical endpoints are essential to confirm the long-term efficacy and durability of SEB, particularly in complex anatomical settings such as bifurcations, diffuse disease, and high-risk diabetic or chronic kidney disease populations.
Limitations
Interpretation of the present results must balance the strengths of an all-comers design with the inherent weaknesses of observational registries. The absence of randomization introduces the possibility of confounding by indication, particularly regarding device selection and bailout stenting decisions. Notably, clinical event rates in this analysis were low across the 2 devices, limiting statistical power to detect small or moderate differences and rendering subgroup analyses descriptive rather than inferential. Given the observational nature of the study and the low number of clinical events, formal propensity score adjustment was not performed, which limits causal inference despite comparable baseline prevalence of key complexity markers. Furthermore, angiographic follow-up was opportunistic rather than protocol-mandated, which may introduce verification bias, as patients returning for angiography may differ meaningfully from those who did not. Despite these constraints, the consistency of the clinical findings, together with the observed procedural advantages, lends support to the feasibility of a sirolimus-eluting balloon strategy in well-prepared de novo lesions. Finally, given the nature of our study, our results are mainly hypothesis generating rather than hypothesis testing and larger studies are required to validate our observations.
CONCLUSIONS
In conclusion, the SELUTION SLR demonstrated comparable 12-month clinical outcomes to the Pantera Lux while showing fewer procedural disturbances and numerically favorable angiographic trends. These results reinforce the role of DCB as a viable stentless strategy in appropriately selected de novo lesions and support continued evaluation of sirolimus-based DCB technologies in larger randomized clinical trials.
ETHICAL CONSIDERATIONS
Ethical approval was obtained from our institutional review board. The study was conducted in full compliance with the principles outlined in the Declaration of Helsinki and follows the SAGER guidelines
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
A large language model was used to improve text readability and fluency.
AUTHORS’ CONTRIBUTIONS
D. Faria was responsible for the study design, data collection, statistical analysis and drafting. D. Neves was responsible for review and drafting. L. Hamann was responsible for data collection. J. Guedes, J. Bispo, F. Soares and H. Vinhas were responsible for manuscript review.
CONFLICTS OF INTEREST
D. Faria has received speaker fees from Cordis. H. Vinhas declared to have received speaker fees from Cordis. F. Soares declared to have received consultant fees from Cordis and Biotronik. The remaining authors declared no conflicts of interest whatsoever.
FUNDING
None declared.
WHAT IS KNOWN ABOUT THE TOPIC?
- DCBs are an established stentless treatment option for selected coronary lesions, with PCB being supported by extensive clinical evidence.
- More recently, SEB technologies have been developed to address potential limitations of paclitaxel-based platforms, but comparative real-world data in de novo coronary lesions remain limited.
WHAT DOES THIS STUDY ADD?
- In this prospective cohort of 257 patients with de novo coronary artery disease, the SELUTION SLR SEB demonstrated similar 1-year clinical outcomes vs the Pantera Lux paclitaxel-coated balloon, with fewer procedural complications.
- These findings support the safety and feasibility of SEB as a stentless treatment strategy, while underscoring the need for confirmation in randomized clinical trials.
SUPPLEMENTARY DATA

REFERENCES
1. Alfonso F, Byrne RA, Scheller B, van Belle E, Mehilli J. Drug-coated balloon angioplasty for in-stent restenosis:pros and cons. EuroIntervention. 2025;21:e102-e104.
2. Cortese B, Di Palma G, Guimaraes MG, et al. Drug-Coated Balloon Versus Drug-Eluting Stent for Small Coronary Vessel Disease:PICCOLETO II Randomized Clinical Trial. JACC Cardiovasc Interv. 2020;13:2840-2849.
3. Jeger RV, Farah A, Ohlow MA, et al. BASKET-SMALL 2 Investigators. Drug-coated balloons for small coronary artery disease (BASKET-SMALL 2):an open-label randomised non-inferiority trial. Lancet. 2018;392:849-856.
4. Sedhom R, Hamed M, Elbadawi A, et al. Outcomes With Limus- vs Paclitaxel-Coated Balloons for Percutaneous Coronary Intervention:Meta-Analysis of Randomized Controlled Trials. JACC Cardiovasc Interv. 2024;17:1533-1543.
5. Madanchi M, Cioffi GM, Attinger-Toller A, et al. Metal free percutaneous coronary interventions in all-comers:First experience with a novel sirolimus-coated balloon. Cardiol J. 2022;29:906-916.
6. Kawai K, Kolodgie FD, Kawakami R, et al. Vascular Response, Downstream Effect, and Pharmacokinetics After Sirolimus- and Paclitaxel-Coated Balloons in Porcine Coronary Arteries. Catheter Cardiovasc Interv. 2025;105:1434-1444.
7. Loh JP, Waksman R. Paclitaxel drug-coated balloons:a review of current status and emerging applications in native coronary artery de novo lesions. JACC Cardiovasc Interv. 2012;5:1001-1012.
8. Shin D, Singh M, Shlofmitz E, et al. Paclitaxel-coated versus sirolimus-coated balloon angioplasty for coronary artery disease:A systematic review and meta-analysis. Catheter Cardiovasc Interv. 2024;104:425-436.
9. Ninomiya K, Serruys PW, Colombo A, et al. A Prospective Randomized Trial Comparing Sirolimus-Coated Balloon With Paclitaxel-Coated Balloon in De Novo Small Vessels. JACC Cardiovasc Interv. 2023;16:2884-2896.
10. Costa MA, Simon DI. Molecular basis of restenosis and drug-eluting stents. Circulation. 2005;111:2257-2273.
11. Costa RA, Mandal SC, Hazra PK, et al. Sirolimus-Coated Balloon With a Microsphere-Based Technology for the Treatment of De novo or Restenotic Coronary Lesions. Cardiovasc Revasc Med. 2022;45:18-25.
12. Gao C, He X, Ouyang F, et al. Drug-coated balloon angioplasty with rescue stenting versus intended stenting for the treatment of patients with de novo coronary artery lesions (REC-CAGEFREE I):an open-label, randomised, non-inferiority trial. Lancet. 2024;404:1040-1050.
13. Unverdorben M, Vallbracht C, Cremers B, et al. Paclitaxel-coated balloon catheter versus paclitaxel-coated stent for the treatment of coronary in-stent restenosis:the three-year results of the PEPCAD II ISR study. EuroIntervention. 2015;11:926-34.
14. Latib A, Colombo A, Castriota F, et al. A randomized multicenter study comparing a paclitaxel drug-eluting balloon with a paclitaxel-eluting stent in small coronary vessels:the BELLO (Balloon Elution and Late Loss Optimization) study. J Am Coll Cardiol. 2012;60:2473-2480.
15. Werk M, Langner S, Reinkensmeier B, et al. Inhibition of restenosis in femoropopliteal arteries:paclitaxel-coated versus uncoated balloon:femoral paclitaxel randomized pilot trial. Circulation. 2008;118:1358-1365.
16. Nakamura T, Brott BC, Brants I, et al. Vasomotor function after paclitaxel-coated balloon post-dilation in porcine coronary stent model. JACC Cardiovasc Interv. 2011;4:247-255.
17. Jun EJ, Shin ES, Kim B, et al. Coronary artery aneurysm formation after paclitaxel-coated balloon-only intervention for de novo coronary chronic total occlusion. Front Cardiovasc Med. 2023;9:1039316.
18. Kawai K, Kolodgie FD, Kawakami R, et al. Vascular Response, Downstream Effect, and Pharmacokinetics After Sirolimus- and Paclitaxel-Coated Balloons in Porcine Coronary Arteries. Catheter Cardiovasc Interv. 2025;105:1434-1444.
19. Boitet A, Grassin-Delyle S, Louedec L, et al. An Experimental Study of Paclitaxel Embolisation During Drug Coated Balloon Angioplasty. Eur J Vasc Endovasc Surg. 2019;57:578-586.
20. Giustino G, Colombo A, Camaj A, et al. Coronary In-Stent Restenosis:JACC State-of-the-Art Review. J Am Coll Cardiol. 2022;80:348-372.
21. Spaulding C, Krackhardt F, Bogaerts K, et al. Comparing a strategy of sirolimus-eluting balloon treatment to drug-eluting stent implantation in de novo coronary lesions in all-comers: Design and rationale of the SELUTION DeNovo Trial. Am Heart J. 2023;258:77-84.
ABSTRACT
Introduction and objectives: ST-segment elevation myocardial infarction (STEMI) requires early coronary reperfusion to reduce mortality and improve prognosis. In rural areas, timely access to reperfusion therapies, including fibrinolysis or percutaneous coronary intervention (PCI) is frequently constrained by logistical and health care system-related factors.
This study aimed to identify factors associated with delays in reperfusion and those associated with mortality in patients with STEMI code activation in a mountainous European region.
Methods: This is an observational, retrospective, and quantitative study in Alt Pirineu-Aran region (Catalonia, Spain) from 2015 through 2020. Sociodemographic and geographic factors, clinical status, resource management and the treatment provided were analyzed using data from the STEMI code registry and the Catalan emergency medical system.
Results: During the study period, a total of 221 patients with STEMI code were treated in the Alt Pirineu-Aran region. Patients ranged in age from 27 to 96 years, with a mean age of 64.7 years; 72.4% were men. Of these, 47 received fibrinolytic therapy and 173 were transferred to a PCI-capable center, of whom 162 underwent PCI; in 11 cases the code was deactivated. Most patients transferred for PCI experienced delays of > 120 minutes from the diagnostic electrocardiogram. Helicopter transport improved treatment times, with the greatest benefit observed in primary transfers. The 15-day mortality rate was 8.1%.
Conclusions: Most fibrinolysis treatments and PCI were not performed within the times recommended by the European clinical practice guidelines. The study highlights the underutilization of fibrinolysis.
Keywords: ST-segment elevation myocardial infarction. Rural areas. Fibrinolysis. Percutaneous coronary intervention. Mountainous regions. Prehospital care.
RESUMEN
Introducción y objetivos: El infarto agudo de miocardio (IAM) con elevación del segmento ST requiere una reperfusión coronaria precoz para reducir la mortalidad y mejorar el pronóstico. En las zonas rurales, los tiempos de acceso a los tratamientos de reperfusión (fibrinolisis o intervención coronaria percutánea primaria [ICPp]) se ven comprometidos por aspectos logísticos y asistenciales. El objetivo de este estudio es determinar los factores asociados a los retrasos en la reperfusión y los asociados a la mortalidad en pacientes con código IAM en una región montañosa europea.
Métodos: Se realizó un estudio observacional, retrospectivo y cuantitativo en la región del Alt Pirineu-Aran, en Cataluña (España), entre 2015 y 2020. Se analizaron los factores sociodemográficos y geográficos, el estado clínico de los pacientes, la gestión de los recursos y el tratamiento realizado, utilizando los datos del registro del código IAM y del Sistema d’Emergències Mèdiques.
Resultados: Durante el periodo de estudio, 221 pacientes con código IAM fueron atendidos en el Alt Pirineu-Aran. Los pacientes tenían entre 27 y 96 años, con una media de 64,7 años, y el 72,4% eran varones. De ellos, 47 pacientes recibieron fibrinolisis como tratamiento de reperfusión y 173 fueron trasladados a un hospital con unidad de hemodinámica, donde 162 recibieron ICPp; en 11 casos se desactivó el código. La mayoría de los pacientes trasladados para ICPp experimentaron un retraso superior a 120 minutos desde el electrocardiograma diagnóstico. El uso de helicópteros mejoró los tiempos de tratamiento, especialmente en los traslados primarios. La tasa de mortalidad a los 15 días fue del 8,1%.
Conclusiones: La mayoría de las fibrinolisis y de las ICPp no se realizaron dentro de los tiempos recomendados según las guías europeas. Se evidencia una marcada infrautilización de la fibrinolisis.
Palabras clave: Infarto agudo de miocardio con elevación del segmento ST. Zonas rurales. Fibrinolisis. Intervención coronaria percutánea. Zonas montañosas. Atención prehospitalaria.
Abbreviations
AMI: acute myocardial infarction. ECG: electrocardiogram. EMS: Emergency Medical Services of Catalonia. PCI-capable center: percutaneous coronary intervention capable center. pPCI: primary percutaneous coronary intervention. STEMI: ST-segment elevation acute myocardial infarction.
INTRODUCTION
Acute myocardial infarction (AMI) is a medical emergency that requires a rapid response to minimize cardiac damage and improve patient survival. Initial recognition and early treatment based on the optimal reperfusion strategy are key to survival; however, implementing this protocol in rural and mountainous regions is a major challenge.1-4
Primary percutaneous coronary intervention (pPCI) is recommended in all cases provided it can be performed within 120 minutes (ideally in less than 90 minutes).4 If not contraindicated, fibrinolysis is the treatment of choice when this time frame cannot be guaranteed. Contraindications to fibrinolytic therapy may be classified as absolute or relative and should be evaluated on an individual basis. When fibrinolysis is contraindicated, primary angioplasty should be prioritized whenever feasible.1,4 The STEMI code in Catalonia was implemented as a regional health care network in June 2009 designed to organize the management of patients with suspected ST-segment elevation myocardial infarction (STEMI).5,6
Several authors have linked delays in reperfusion treatment to the type of infarction, the timing of symptom onset, and complications.7-9 Other studies suggest that a distance > 50 km to a PCI- capable center is associated with higher mortality rates vs early fibrinolysis.10,11 Other experiences, such as sharing patient data during prehospital care, including electrocardiograms (ECG) and the use of nighttime helicopter transfer to the PCI-capable center have been associated with shorter diagnosis-to-treatment times; however, a reduction in mortality has not been demonstrated.12 However, few studies have analyzed the factors causing delays in mountainous and hard-to-access geographic areas.
The main aim of this study was to determine the factors associated with delays in reperfusion treatment and those associated with mortality in patients treated under the STEMI code in a European mountainous area.
METHODS
Study design
We conducted an observational, retrospective, and quantitative study that included all STEMI code activations in the Alt Pirineu-Aran territory (Catalonia, Spain) from January 2015 through December 2020. The main sources of information were the STEMI code registry of the Department of Health of the Government of Catalonia5,6 and the database of the medical Emergency Medical Services (EMS) of Catalonia, which were cross-referenced to obtain a comprehensive overview. Because the data were derived from preexisting registries and analyzed anonymously, informed consent was deemed unnecessary. The study was approved by the Instituto Universitario de Investigación en Atención Primaria (IDIAP) Jordi Gol Ethics Committee, code CEIm 22/238-P. The SAGER guidelines were followed regarding potential sex and gender bias.
Study setting
Alt Pirineu-Aran is a mountainous region comprising 6 counties and represents 18% of Catalonia’s territory, yet it is home to less than 1% of its population. Population density is extremely low (12.6 inhabitants per km²), and most towns are located between 500 and 800 meters above sea level, far from a specialized hospital center.
This regional health care system faces several challenges. Prehospital care is provided by the EMS, a public service that operates 24 hours per day and provides coverage throughout the entire territory. Each county is served by 1 advanced life support unit, and the region has access to 1 medicalized helicopter, 1 of the 4 operating in Catalonia. Alt Pirineu–Aran includes 4 county hospitals, all of which are non–PCI-capable centers (figure 1).
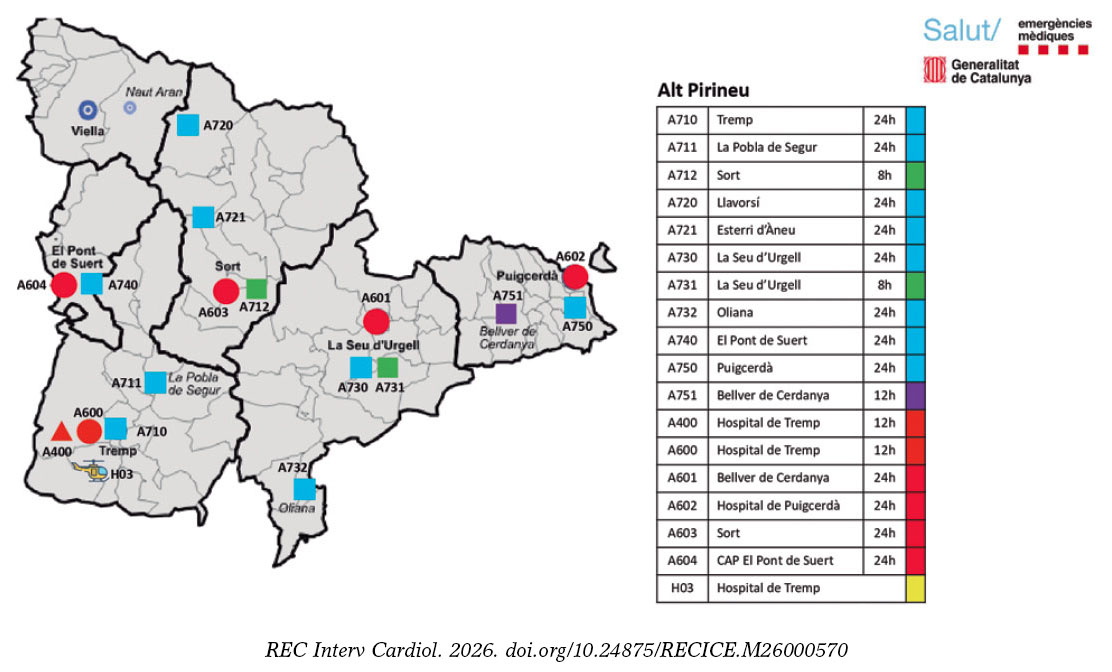
Figure 1. Alt Pirineu-Aran Health Region. H03: Tremp medicalized helicopter. H: county hospitals. Unit call signs are identified with A for Alt Pirineu; 1st number indicates the type of unit (7, basic life support; 4, advanced life support + nurse; and 6, advanced life support + physician); 2nd and 3rd numbers indicate the location of the units on the map.
Hospital Universitario Arnay de Vilanova (Lleida, Spain) serves as the reference center for pPCI for Alt Pirineu-Aran, with the exception of the Cerdanya basic health area, where STEMI code patients are transferred to centers in the Barcelona metropolitan area (table S1).
Definitions and inclusion criteria
The definitions of “delay” used in the study were more than 10 minutes for fibrinolysis administration and more than 120 minutes for pPCI, measured from the time of ECG acquisition. These criteria were established on the basis of former studies and are consistent with current European clinical practice guideline recommendations.1-4
According to EMS protocols, a 90-minute transfer threshold—from ECG acquisition to arrival at the receiving hospital—is used to allow adequate time to perform pPCI and ensure compliance with the 120-minute target. To determine whether patients had a transfer time of less than 90 minutes to a PCI-capable center, a geographic analysis based on distance and estimate travel-time maps was performed.
Patients were included if the STEMI code was activated in Alt Pirineu–Aran and they were attended by EMS during the study period, as well as those who died after prior activation of the STEMI code.
Incomplete cases or those with coding errors were excluded, as were patients transferred to Toulouse (France) from Vall d’Aran.
Study variables
The variables analyzed included demographic, clinical, and logistical data. The primary time intervals assessed were symptom onset to first medical contact, time from first medical contact to ECG, and ECG to initiation of reperfusion treatment. The type of reperfusion strategy (fibrinolysis or pPCI) was recorded as well. Other relevant variables included the location of STEMI code activation, distance to the PCI-capable center, mode of transport to the PCI-capable center (ambulance or helicopter), and type of transfer (primary: direct care and transfer by a medicalized EMS ambulance; secondary: interhospital transfer; or delayed primary: initial assessment by a primary care physician or nurse-staffed ambulance followed by transfer to a medicalized ambulance or medical helicopter). Acute-phase complications and all-cause mortality at first medical contact, and at 24 and 48 hours, and at 15 days were also recorded.
Statistical analysis
The descriptive statistical measures used were absolute and relative frequencies for qualitative variables; mean and standard deviation for quantitative variables with normal distribution; and median and interquartile range for the remaining non-normally distributed quantitative variables, according to the Shapiro-Wilk test.
We analyzed a total of 4 binary outcome variables: use of fibrinolysis as the initial treatment, delays in fibrinolysis (> 10 minutes from ECG acquisition), delays in pPCI (> 120 minutes from ECG acquisition), and mortality. Furthermore, we evaluated associations between each outcome variable and patient- and care-related characteristics using the chi-square test for qualitative variables (or Fisher’s exact test when expected frequencies were < 5), the Mann-Whitney U test for non-normally distributed quantitative variables, and the Student t test otherwise. In addition, we analyzed the importance of variables for treatment delay and mortality using the Boruta algorithm for variable selection. Only variables not rejected by this algorithm were selected for subsequent multivariable analyses to reduce the risk of overfitting. A conditional inference classification tree was constructing using a Monte Carlo test with a minimum terminal node size of 3.
All statistical analyses were performed using R statistical software (R Foundation for Statistical Computing, Austria). P values < .05 were considered statistically significant.
RESULTS
During the study period, a total of 24 125 STEMI codes were activated across Catalonia. The study analyzed 225 cases occurring in Alt Pirineu-Aran, representing less than 1% of the total. Four patients were excluded for not meeting STEMI code criteria (1 pulmonary thromboembolism, 2 coding errors, and 1 duplicate case) (figure 2).
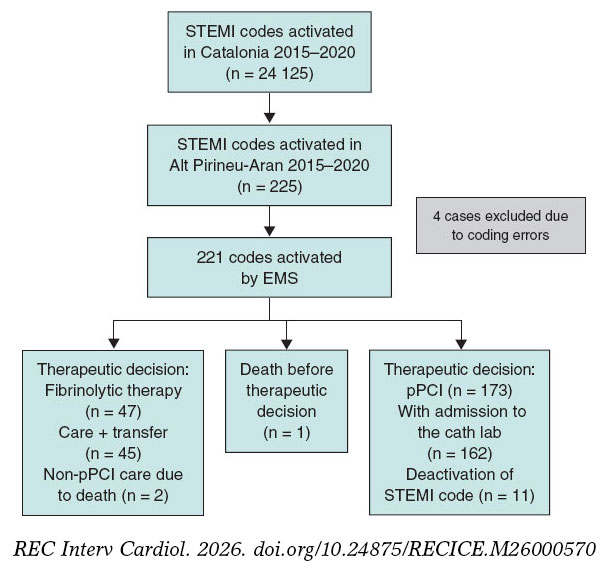
Figure 2. Flow diagram of STEMI codes. AMI, acute myocardial infarction; pPCI, primary percutaneous coronary intervention; EMS, Emergency Medical Services of Catalonia.
The mean age of the 221 included patients was 64.7 years (range, 27–96). Of these, 72.4% were men and 67.4% resided in the study area. All STEMI codes were activated after ECG acquisition at first medical contact, either at a county hospital (51.6%), by EMS at the patient’s home or in a public setting (28.9%), or at a primary care center (19.5%). The median time from first medical contact to ECG acquisition was 6 minutes, and from pain onset to ECG acquisition, 90 minutes (table 1).
Table 1. Clinical characteristics and care times of activated STEMI codes and comparison according to therapeutic decision
| Clinical and care characteristics | Total AMI (n = 221)* | No fibrinolysis (n = 173) | Fibrinolysis (n = 47) | P |
|---|---|---|---|---|
| Female sex | 61 (27.6) | 47 (27.2) | 13 (27.7) | 1 |
| Age (years) | 64.7 (13.7) | 65.7 (13.7) | 60.7 (12.7) | .023 |
| Year | .201 | |||
| 2015 | 30 (13.6) | 25 (14.5) | 5 (10.6) | |
| 2016 | 34 (15.4) | 24 (13.9) | 10 (21.3) | |
| 2017 | 27 (12.2) | 17 (9.83) | 9 (19.1) | |
| 2018 | 35 (15.8) | 27 (15.6) | 8 (17.0) | |
| 2019 | 57 (25.8) | 46 (26.6) | 11 (23.4) | |
| 2020 | 38 (17.2) | 34 (19.7) | 4 (8.51) | |
| Residents in Alt Pirineu i Aran health region | 149 (67.4) | 118 (68.2) | 30 (63.8) | .695 |
| Altitude (m) | 838 [691;1202] | 790 [659;1202] | 974 [691;1202] | .08 |
| Location of first medical contact | .01 | |||
| Primary care center | 65 (29.4) | 57 (32.9) | 8 (17.0) | |
| Home | 20 (9.05) | 18 (10.4) | 2 (4.26) | |
| County hospital | 94 (42.5) | 63 (36.4) | 30 (63.8) | |
| EMS or public setting | 42 (19.0) | 35 (20.2) | 7 (14.9) | |
| Night shift | 56 (25.3) | 34 (19.7) | 22 (46.8) | < .001 |
| Sympton onset–first medical contact time (min) | 80.0 [35.0;193] | 82.0 [39.0;210] | 60.0 [30.0;180] | .292 |
| First medical contact–ECG acquisition time (min) | 6.00 [1.00;12.0] | 6.00 [1.00;12.0] | 5.00 [2.50;12.0] | .807 |
| Sympton onset–ECG acquisition time (min) | 90.0 [45.0;216] | 91.0 [49.0;253] | 80.0 [37.5;192] | .182 |
| Estimated time to PCI-capable center (min) | 106 [93.0;112] | 105 [84.0;109] | 107 [96.0;114] | .061 |
| Estimated time to PCI-capable center ≥ 90 min | 169 (76.5) | 127 (73.4%) | 41 (87.2) | .074 |
| Distance to PCI-capable center (km) | 131 [116;143] | 131 [100;142] | 131 [127;149] | .393 |
| Type of transfer | .036 | |||
| Interhospital | 123 (55.7) | 89 (51.4) | 33 (70.2) | |
| Delayed | 71 (32.1) | 63 (36.4) | 8 (17.0) | |
| Primary | 27 (12.2) | 21 (12.1) | 6 (12.8) | |
| Mode of transport | < .001 | |||
| Ambulance | 106 (48.0) | 69 (39.9) | 36 (76.6) | |
| Helicopter | 56 (25.3) | 49 (28.3) | 7 (14.9) | |
| Ambulance + helicopter | 59 (26.7) | 55 (31.8) | 4 (8.51) | |
| Past medical history | ||||
| Hypertension | 104 (47.1) | 85 (49.1) | 18 (38.3) | .248 |
| Diabetes | 49 (22.2) | 42 (24.3) | 6 (12.8) | .135 |
| Dyslipidemia | 92 (41.6) | 69 (39.9) | 23 (48.9) | .343 |
| Smoking | 63 (28.5) | 47 (27.2) | 16 (34.0) | .458 |
| Previous AMI | 25 (11.3) | 21 (12.1) | 4 (8.51) | .663 |
| Previous pPCI | 25 (11.3) | 22 (12.7) | 3 (6.38) | .34 |
| Stroke | 16 (7.24) | 14 (8.09) | 2 (4.26) | .532 |
| Previous antiplatelet therapy | 40 (18.1) | 35 (20.2) | 5 (10.6) | .194 |
| Treatment and prehospital complications | ||||
| Shock | 8 (3.62) | 5 (2.89) | 2 (4.26) | .643 |
| Ventricular fibrillation | 6 (2.71) | 4 (2.31) | 2 (4.26) | .611 |
| Asystole | 6 (2.71) | 3 (1.73) | 2 (4.26) | .29 |
| Intubation | 7 (3.17) | 4 (2.31) | 2 (4.26) | .611 |
|
AMI, acute myocardial infarction; ECG, electrocardiogram; EMS, Emergency Medical Services of Catalonia; PCI-capable center, percutaneous coronary intervention capable center; pPCI, primary or secondary percutaneous coronary intervention. * Includes 1 patient who died without therapeutic decision. Distribution of totals, no fibrinolysis, and fibrinolysis. Values are expressed as percentage or median. Quantitative variables are expressed as mean (standard deviation) or median [25th percentile; 75th percentile]. |
||||
The incident location had a mean altitude of 838 meters and was located at distances ranging from 81 km to 257 km from the PCI-capable center (median, 131 km). Overall, 76.5% of patients were situated more than 90 minutes from the PCI-capable center (median estimate transfer time, 106 minutes). Air advanced life support was used in 52.5% of the transfers (table 1).
Differences were observed in the time from ECG acquisition to pPCI according to mode of transport (Kruskal-Wallis; P < .001). The median time was 183 minutes for ground ambulance, 138 minutes for helicopter transport, and 140 minutes for combined transport (table 1). Pairwise comparisons using the Mann–Whitney U test showed significant differences compared with ground transport after adjustment for the false discovery rate.
We observed marked variability in the annual frequency of STEMI code cases, with a particularly high number in 2019, and in the proportion of first-assistance fibrinolysis performed from a minimum of 10.5% in 2020 to a maximum of 34.6% in 2017. The number of cases attended in 2020 (the year of the COVID-19 pandemic) was slightly higher than in 2015–2017 (38 cases [17.2%]) but lower than in 2019, which recorded 57 cases (25.8%) (table 1).
Delays in treatment
In 91.5% of patients in whom the therapeutic decision was to perform fibrinolysis at first medical contact, the time between ECG acquisition and treatment exceeded the recommended threshold (> 10 minutes).
When the therapeutic decision was to perform pPCI, the time between ECG acquisition and pPCI exceeded the recommended threshold (> 120 minutes) in 79.6% of cases (table 2).
Table 2. Factors associated with delay in reperfusion treatment
| Clinical and care characteristics | Fibrinolysis (n = 47) | ≤ 10 min | > 10 min | P | pPCI (n = 162) | ≤ 120 min | > 120 min | P |
|---|---|---|---|---|---|---|---|---|
| Female sex | 13 (27.7) | 3 (75.0) | 10 (23.3) | .059 | 45 (27.8) | 6 (18.2) | 39 (30.2) | .245 |
| Age (years) | 60.7 (12.7) | 61.2 (13.8) | 60.7 (12.7) | .943 | 65.3 (13.4) | 65.3 (13.3) | 65.3 (13.5) | 1 |
| Residents in Alt Pirineu i Aran health region | 30 (63.8) | 3 (75.0) | 27 (62.8) | 1 | 109 (67.3) | 22 (66.7) | 87 (67.4) | 1 |
| Altitude (m) | 974 [691;1202] | 946 [649;1202] | 974 [691;1202] | .859 | 692 [640;1202] | 692 [524;957] | 838 [691;1202] | .079 |
| Location of first medical contact | .13 | .014 | ||||||
| Primary care center | 8 (17.0) | 2 (50.0) | 6 (14.0) | 55 (34.0) | 12 (36.4) | 43 (33.3) | ||
| Home | 2 (4.26) | 0 (0.00) | 2 (4.65) | 16 (9.88) | 5 (15.2) | 11 (8.53) | ||
| County hospital | 30 (63.8) | 1 (25.0) | 29 (67.4) | 58 (35.8) | 5 (15.2) | 53 (41.1) | ||
| EMS or public setting | 7 (14.9) | 1 (25.0) | 6 (14.0) | 33 (20.4) | 11 (33.3) | 22 (17.1) | ||
| Night shift | 22 (46.8) | 3 (75.0) | 19 (44.2) | .328 | 31 (19.1) | 1 (3.03) | 30 (23.3) | .017 |
| Symptom onset–first medical contact time (min) | 60.0 [30.0;180] | 190 [180;200] | 57.0 [28.5;152] | .047 | 82.5 [40.0;206] | 60.0 [40.0;116] | 90.0 [40.0;255] | .124 |
| First medical contact–ECG acquisition time (min) | 5.00 [2.50;12.0] | 3.00 [0.75;7.50] | 6.00 [3.00;12.0] | .421 | 6.00 [1.00;11.8] | 6.00 [1.00;10.0] | 6.00 [1.00;12.0] | .75 |
| Symptom onset–ECG acquisition time (min) | 80.0 [37.5;192] | 198 [191;202] | 60.0 [35.0;160] | .05 | 93.5 [50.0;250] | 80.0 [43.0;117] | 115 [57.0;309] | .053 |
| Time to PCI-capable center (min) | 106 (15.9) | 101 (16.2) | 106 (16.0) | .614 | 105 [82.5;110] | 97.0 [71.0;108] | 106 [94.0;111] | .309 |
| Time to PCI-capable center ≥ 90 min | 41 (87.2) | 3 (75.0) | 38 (88.4) | .432 | 118 (72.8) | 19 (57.6) | 99 (76.7) | .047 |
| Distance to PCI-capable center (km) | 131 [127;149] | 132 [123;138] | 131 [127;149] | .969 | 131 [100;143] | 123 [85.0;137] | 131 [123;143] | .085 |
| Type of transfer | .342 | .001 | ||||||
| Interhospital | 33 (70.2) | 2 (50.0) | 31 (72.1) | 83 (51.2) | 8 (24.2) | 75 (58.1) | ||
| Delayed | 8 (17.0) | 1 (25.0) | 7 (16.3) | 59 (36.4) | 18 (54.5) | 41 (31.8) | ||
| Primary | 6 (12.8) | 1 (25.0) | 5 (11.6) | 20 (12.3) | 7 (21.2) | 13 (10.1) | ||
| Mode of transport | 1 | < .001 | ||||||
| Ambulance | 36 (76.6) | 4 (100) | 32 (74.4) | 65 (40.1) | 2 (6.06) | 63 (48.8) | ||
| Helicopter | 7 (14.9) | 0 (0.00) | 7 (16.3) | 48 (29.6) | 18 (54.5) | 30 (23.3) | ||
| Ambulance + helicopter | 4 (8.51) | 0 (0.00) | 4 (9.30) | 49 (30.2) | 13 (39.4) | 36 (27.9) | ||
|
ECG, electrocardiogram; EMS, Emergency Medical Services of Catalonia; PCI-capable center, percutaneous coronary intervention capable center; pPCI, primary or secondary percutaneous coronary intervention. Values are expressed as percentage or median. Quantitative variables are expressed as mean (standard deviation) or median [25th percentile; 75th percentile]. |
||||||||
Among patients located more than 90 minutes from a PCI-capable center who did not receive fibrinolysis at first medical contact, the reason for withholding treatment was not documented in 87 cases (68.5%). Although 76.5% of patients were situated more than 90 minutes from the PCI-capable center, a substantial underuse of fibrinolytic treatment was observed. Of note, patients with a longer time interval from symptom onset to ECG acquisition were more likely to receive fibrinolytic treatment earlier.
Interhospital transfers, incidents without participation of air advanced life support, and nighttime incidents located more than 90 minutes from the PCI-capable center showed greater delays in performing pPCI. Exclusive use of ground ambulance for transfer to the PCI-capable center was associated with a 96.9% rate of delay and emerged as the primary variable in the classification tree for delay between ECG acquisition and pPCI. Among helicopter transfers, delays were more frequent in interhospital transfers (85.4%). In primary or delayed primary transfers, delays were more common when the incident location was more than 90 minutes from the PCI-capable center (65.1%) compared with locations less than 90 minutes away (23.1%) (figure 3).
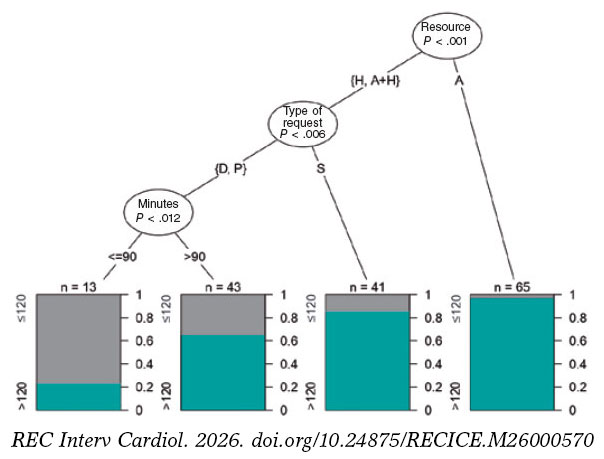
Figure 3. Classification tree for delay in primary percutaneous coronary intervention (pPCI). Three factors were significantly associated with delay: mode of transport (ambulance [A], helicopter [H], or combined use), type of activation (primary [P], delayed [D], or interhospital [S]), and estimated road travel time from the event location to the PCI-capable center in minutes (> 90 minutes < 90 minutes).
Mortality
A total of 18 patients (8.1%) died within the first 15 days. Mortality was significantly higher in patients who experienced a major event (asystole, intubation, shock, or ventricular fibrillation) within the first 24 hours. Age was significantly associated with mortality only at the 48-hour and 15-day follow-up. There were no significant differences in 15-day mortality between patients treated with fibrinolysis and those directly transferred for pPCI. Increased mortality was associated with treatment delays, particularly in the early mortality subgroup (< 24 hours); however, these differences did not reach statistical significance (table 3).
Table 3. Factors associated with mortality according to time from clinical course prior to death
| Clinical and care characteristics | Pre-PCI-capable center (n = 3) | < 24 h (n = 8) | < 48 h (n = 12) | P | ≤ 15 days (n = 18) | P |
|---|---|---|---|---|---|---|
| Female sex | 1 (33.3) | 2 (25.0) | 4 (33.3) | .741 | 6 (33.3) | .587 |
| Age (years) | 67.7 (25.7) | 69.8 (16.0) | 74.4 (15.8) | .047 | 74.1 (14.1) | .008 |
| Residents in Alt Pirineu i Aran health region | 2 (66.7) | 6 (75.0) | 9 (75.0) | .755 | 13 (72.2) | .848 |
| Altitude (m) | 974 [721;1042] | 832 [691;1014] | 691 [468;1014] | .154 | 832 [691;1136] | .625 |
| Location of first medical contact | .337 | .514 | ||||
| Primary care center | 0 (0.00) | 1 (12.5) | 1 (8.33) | 3 (16.7) | ||
| Home | 0 (0.00) | 1 (12.5) | 1 (8.33) | 1 (5.56) | ||
| County hospital | 2 (66.7) | 4 (50.0) | 7 (58.3) | 9 (50.0) | ||
| EMS or public setting | 1 (33.3) | 2 (25.0) | 3 (25.0) | 5 (27.8) | ||
| Night shift | 0 (0.00) | 1 (12.5) | 2 (16.7) | .735 | 4 (22.2) | 1 |
| Symptom onset–first medical contact time (min) | 38.0 [19.0;246] | 64.5 [22.0;488] | 41.0 [22.0;488] | .502 | 65.0 [26.2;413] | .723 |
| First medical contact–ECG acquisition time (min) | 30.0 [17.0;11 542] | 3.00 [0.00;11.2] | 1.50 [0.00;11.2] | .152 | 2.00 [0.00;24.0] | .205 |
| Symptom onset–ECG acquisition time (min) | 42.0 [36.0;11 774] | 66.5 [28.8;682] | 45.0 [30.0;682] | .543 | 81.0 [42.8;518] | .962 |
| Estimated time to PCI-capable center (min) | 96.0 [90.5;113] | 107 [95.8;107] | 96.0 [81.5;107] | .242 | 96.0 [95.0;107] | .432 |
| Estimated time to PCI-capable center ≥ 90 min | 2 (66.7) | 7 (87.5) | 8 (66.7) | .483 | 14 (77.8) | 1 |
| Distance to PCI-capable center (km) | 134 [108;149] | 131 [130;132] | 131 [85.0;131] | .15 | 131 [119;134] | .419 |
| Type of transfer | .911 | .938 | ||||
| Secondary | 2 (66.7) | 4 (50.0) | 8 (66.7) | 11 (61.1) | ||
| Delayed | 1 (33.3) | 3 (37.5) | 3 (25.0) | 5 (27.8) | ||
| Primary | 0 (0.00) | 1 (12.5) | 1 (8.33) | 2 (11.1) | ||
| Mode of transport | .508 | .734 | ||||
| Ambulance | 1 (33.3) | 3 (37.5) | 5 (41.7) | 10 (55.6) | ||
| Helicopter | 1 (33.3) | 1 (12.5) | 2 (16.7) | 3 (16.7) | ||
| Ambulance + helicopter | 1 (33.3) | 4 (50.0) | 5 (41.7) | 5 (27.8) | ||
| Fibrinolytic therapy at first medical contact | 2 (100) | 2 (28.6) | 2 (18.2) | 1 | 4 (23.5) | .764 |
| Delayed fibrinolytic therapy or pPCI | 2 (100) | 7 (100) | 10 (90.9) | .693 | 16 (94.1) | .318 |
| Past medical history | ||||||
| Hypertension | 1 (33.3) | 4 (50.0) | 7 (58.3) | .612 | 11 (61.1) | .317 |
| Diabetes | 1 (33.3) | 2 (25.0) | 3 (25.0) | .731 | 5 (27.8) | .558 |
| Dyslipidemia | 0 (0.00) | 2 (25.0) | 4 (33.3) | .765 | 7 (38.9) | 1 |
| Smoking | 0 (0.00) | 1 (12.5) | 1 (8.33) | .186 | 4 (22.2) | .731 |
| Previous AMI | 0 (0.00) | 1 (12.5) | 2 (16.7) | .631 | 3 (16.7) | .437 |
| Previous pPCI | 0 (0.00) | 1 (12.5) | 2 (16.7) | .631 | 2 (11.1) | 1 |
| Previous stroke | 0 (0.00) | 0 (0.00) | 0 (0.00) | 1 | 1 (5.56) | 1 |
| Prior antiplatelet therapy | 0 (0.00) | 0 (0.00) | 2 (16.7) | 1 | 3 (16.7) | 1 |
| Treatment and prehospital complications | ||||||
| Shock | 2 (66.7) | 3 (37.5) | 4 (33.3) | < .001 | 6 (33.3) | < .001 |
| Ventricular fibrillation | 2 (66.7) | 3 (37.5) | 3 (25.0) | .002 | 3 (16.7) | .008 |
| Asystole | 3 (100) | 5 (62.5) | 5 (41.7) | < .001 | 5 (27.8) | < .001 |
| Intubation | 3 (100) | 4 (50.0) | 4 (33.3) | < .001 | 4 (22.2) | .001 |
|
AMI, acute myocardial infarction; ECG, electrocardiogram; EMS, Emergency Medical Services of Catalonia; PCI-capable center, percutaneous coronary intervention capable center; pPCI, primary or secondary percutaneous coronary intervention. Values are expressed as percentage or median. Quantitative variables are expressed as mean (standard deviation) or median [25th percentile; 75th percentile]. |
||||||
DISCUSSION
In our study, only 20.4% of patients who underwent pPCI received treatment within 120 minutes. Only 4 of the 47 patients treated with fibrinolysis received therapy within 10 minutes.
Several studies, such as the STREAM,13 have shown that prehospital fibrinolysis followed by early pPCI may offer results similar to direct transfer for pPCI if patients are treated within the first 3 hours from symptom onset. In our analysis, we identified underuse of fibrinolytic therapy, along with insufficient documentation of the reasons for withholding treatment.
In contrast to the studies by Stopyra et al.9,14 conducted in North Carolina (United States) in which 60.5% of patients underwent pPCI within ≤ 90 minutes, only 20.4% of patients in our study achieved reperfusion within a broader threshold (< 120 minutes). These findings underscore longer treatment delays in our region and support more frequent consideration of fibrinolytic therapy.
Although Aboal et al.10,11 reported higher mortality rates associated with delayed pPCI, we did not observe a significant association in our study, despite a substantial lower proportion of patients undergoing pPCI within the target time (20.4% vs 42%). In addition, fibrinolysis was more frequently used in patients located more than 50 km from the PCI-capable center (66.7%), reflecting structural and logistical constraints specific to the Alt Pirineu-Aran region that influence treatment selection and reperfusion times.
In line with former evidence regarding mortality, the study results reinforce the clinical importance of time to care as a potential factor associated with worse prognosis, which is particularly relevant in early mortality (< 24 hours).
Compared with the study by Carol et al.,15 in which 58% of patients underwent pPCI after more than 120 minutes, our data show a substantial higher proportion (79.6%). Factors associated with delay, such as intubation, initial shock, and nighttime care, were consistent between the 2 studies; however, other variables, including left bundle branch block, were not. A notable finding of our study is that the care delivered by the EMS was associated with shorter treatment times compared with county hospitals.
Patient origin, geographic location, sex, number of resources involved, time required for therapeutic decision-making, and mode of transport influenced treatment times as well. Hakim et al.16 suggest that helicopter transport is less effective than ground transport, especially for distances of less than 50 km. In our study, 71% of patients transferred by helicopter (all located more than 50 km from the PCI-capable center) received pPCI after more than 120 minutes, which may be associated with the lack of a helipad at the reference PCI-capable center, requiring additional ground transfer, and service hours, mainly daytime during the study period. In constrast to other studies conducted during the COVID-19 pandemic,17,18 our series did not demonstrate a reduction in case volume or prolongation in alert time. However, 2020 was the year with the lowest use of fibrinolysis (4 cases, 10.5%).
Several studies indicate that delays in STEMI recognition and code activation have a direct impact on reperfusion time. One study highlights that training significantly improves these times,19 suggesting that lack of training or skills among professionals may generate delays in care and lower use of fibrinolysis. Our study shows appropriate timing in ECG acquisition and emergency recognition by teams. Delayed primary transfers included the highest percentages of patients with optimal reperfusion times (table 2).
Our findings underscore the need to review and optimize action protocols, particularly in non-PCI-capable centers and geographic areas with greater delays. It is essential to optimize professional response to suspected STEMI, improve therapeutic decision-making time, and explore innovative solutions such as triage systems and STEMI code detection with technological support, optimization of air transport, and greater coordination between PCI and non-PCI capable centers.
Limitations and strengths
This study has limitations due to the small population size in the rural areas studied, which required extending the study period to 6 years to obtain the collected sample. This extension implies that data underwent several changes in record systems (from paper to digitized format) and organizational modifications (implementation of triage in emergency departments and nighttime helicopter flights). The sample of 221 patients remains limited and may have affected the statistical power to detect significant differences between analyzed variables. Similarly, distances from the incident location and estimated average travel times under optimal conditions were used, without accounting for any potential delays due to traffic or other unforeseen factors.
CONCLUSIONS
The results of this study demonstrate the need to increase the use of fibrinolysis in areas distant from a PCI-capable center to reduce reperfusion delays. Documentation of the reasons for not performing fibrinolysis should be improved, as this limits interpretation regarding therapeutic appropriateness. Joint initial care by primary care and emergency teams, as well as delayed primary transfers, reduce reperfusion times and avoid interhospital transfers. Finally, the low number of deaths during the study period prevents multivariate analysis and only allows identification of the variables or characteristics associated with mortality described in the results.
Despite these limitations, the study provides a comprehensive analysis of variables and describes in detail how the investigated population is managed and transferred, something unprecedented in this context. In addition, cross-referencing and thorough review of 2 databases provide valuable information to assess treatment delays. Therefore, this study is a solid basis for future advances in improving STEMI code management in rural areas.
FUNDING
This study was funded by the Provincial Council of Lleida through “The strength of municipalities” project and by IRBLleida through project PP10851 of the Alt Pirineu-Aran Intramural Research Program (IREP).
ETHICAL CONSIDERATIONS
This study was approved by the IDIAP Jordi Gol Ethics Committee, code CEIm 22/238-P. The SAGER guidelines were followed regarding potential sex and gender bias.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
ChatGPT was used to improve the wording of some paragraphs of the article. After using this tool, the authors reviewed and edited the content as necessary and take full responsibility for the final version.
AUTHORS’ CONTRIBUTIONS
M. Navarra Llorens was responsible for study conception and design, overall supervision, and manuscript drafting. M. Martínez Alonso conducted the statistical analysis, interpreted the results, and critically reviewed the content. Y. Azeli was responsible for clinical analysis and critical review. S. Ferrandis Barrés collected data and contributed to the discussion and critical review. M. Canelles Seix collected data and reviewed the manuscript. L. Duch Grau participated in data collection, manuscript review, and final approval. A.M. Forradelles Rey collected data and performed critical review. M.A. Martínez Momblan supervised the project and critically reviewed the manuscript. X. Jiménez-Fàbrega supervised the project and provided intellectual contributions to the discussion. All authors approved the final text.
CONFLICTS OF INTEREST
None declared.
ACKNOWLEDGMENTS
We thank Mar Franch Casanovas and Francisco Iturbe Recasens for their collaboration in data collection, and Isidre Felip for his advice in drafting the manuscript.
WHAT IS KNOWN ABOUT THE TOPIC?
- STEMI requires early coronary reperfusion to reduce mortality and improve prognosis.
- In Catalonia, implementation of the STEMI code has optimized system response; however, in regions such as Alt Pirineu, delays have not been specifically evaluated.
WHAT DOES THIS STUDY ADD?
- This study shows significant underuse of fibrinolytic therapy, even among patients located far from a PCI-capable center. In additions, it highlights the absence of systematic documentation regarding the reasons for withholding fibrinolysis, thereby limiting the evaluation of therapeutic decision-making.
- The study demonstrates that joint initial care by primary care and emergency teams, along with delayed primary transfer, can reduce reperfusion times and avoid interhospital transfers, which are associated with longer delays.
- Similarly, it identifies the mode of transport as the main predictive variable for delay and shows that exclusive use of ground ambulance is the most critical factor.
- Although the low number of deaths prevents a robust multivariate analysis, characteristics associated with mortality are described, and the influence of delays is confirmed, reinforcing the need for adapted strategies.
SUPPLEMENTARY DATA
REFERENCES
1. Ibáñez B, James S, Agewall S, et al. ESC 2017 guidelines on the treatment of acute myocardial infarction in patients with ST segment elevation. Rev Esp Cardiol. 2017;70:1082.e1-1082.e61.
2. Steg G, James SK, Atar D, et al. ESC Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting With ST-Segment Elevation. Rev Esp Cardiol. 2013;66:53.e1-53.e46.
3. Rao SV, O'Donoghue ML, Ruel M, et al. 2025 ACC/AHA/ACEP/NAEMSP/ SCAI Guideline for the Management of Patients With Acute Coronary Syndromes:A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2025;85:2135-2237.
4. Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44:3720-3826.
5. Faixedas MT, Mauri J, Pueyo MJ. The Codi IAM registry:acute myocardial infarction code registry in Catalonia. Rev Esp Cardiol. 2022;75:291-293.
6. Instrucció04/2009, de 12 de maig. Sectoritzacióde l'atencióa les persones malaltes amb infart agut de miocardi (IAM) amb elevaciódel segment ST per tal de portar a terme l'angioplàstia primària. Available at: https:// catsalut.gencat.cat/ca/detalls/articles/instruccio-04-2009-12-maig. Accessed 20 Jan 2026.
7. Rivero F, Bastante T, Cuesta J, et al. Factors Associated With Delays in Seeking Medical Attention in Patients With ST-segment Elevation Acute Coronary Syndrome. Rev Esp Cardiol. 2016;69:279-285.
8. Berga Congost G, Valverde Bernal J, Márquez López A. Factores clínicos predictores de retraso en la actuación del código infarto. Enferm Cardiol. 2017;71:63-71.
9. Stopyra JP, Snavely AC, Ashburn NP, Supples MW, Miller CD, Mahler SA. Delayed first medical contact to reperfusion time increases mortality in rural emergency medical services patients with ST-elevation myocardial infarction. Acad Emerg Med. 2023;30:1101-1109.
10. Aboal J, Núñez M, Bosch D, Tirón C, Brugada R. Angioplastia primaria frente a fibrinolisis en pacientes alejados de un centro con hemodinámica. Emergencias. 2017;29:99-104.
11. Aboal J, Ramos R, Loma-Osorio P, et al. Factores asociados a retrasos de tiempo desde el electrocardiograma diagnóstico hasta el paso de guía en el infarto agudo de miocardio con elevación del segmento ST transferido para angioplastia primaria. Emergencias. 2021;33:195-202.
12. Brunetti ND, Dell'Anno A, Martone A, et al. Prehospital ECG transmission results in shorter door-to-wire time for STEMI patients in a remote mountainous region. Am J Emerg Med. 2020;38:252-257.
13. Van De Werf F, Ristic´AD, Averkov OV, et al. STREAM-2:Half-Dose Tenecteplase or Primary Percutaneous Coronary Intervention in Older Patients With ST-Segment-Elevation Myocardial Infarction:A Randomized, Open-Label Trial. Circulation. 2023;148:753-764.
14. Stopyra JP, Snavely AC, Ashburn NP, et al. Rural EMS STEMI Patients –Why the Delay to PCI?Prehosp Emerg Care. 2024;28:947-954.
15. Carol Ruiz A, Masip Utset J, Ariza-SoléA, et al. Predictors of primary percutaneous coronary intervention delay in cases of myocardial infarction diagnosed in hospitals without hemodynamic support systems. Emergencias. 2021;33:187-194.
16. Hakim R, Revue E, Saint Etienne C, et al. Does helicopter transport delay prehospital transfer for STEMI patients in rural areas?Findings from the CRAC France PCI registry. Eur Heart J Acute Cardiovasc Care. 2020;9:958-965.
17. Romaguera R, Ribera A, Güell-Viaplana F, Tomás-Querol C, Muñoz-Camacho JF, Agudelo V. Decrease in ST-segment elevation myocardial infarction admissions in Catalonia during the COVID-19 pandemic. Rev Esp Cardiol. 2020;73:778-780.
18. Kaddoura R, Salam AM. Thrombosis Management and Challenges in COVID-19 Patients Presenting with Acute Coronary Syndromes. Heart Views. 2020;21:195.
19. Berga Congost G, Brugaletta S, Garcimartin Cerezo P, et al. Effectiveness of a nurse training intervention in the emergency department to improve the diagnosis and treatment of stemi patients:EDUCAMI study. Heart Lung. 2025;70:305-312.
ABSTRACT
Introduction and objectives: There is limited data on territorial longitudinal strain (TLS) as an echocardiographic marker in stable coronary artery disease (CAD). We evaluated the predictive role of TLS in stable CAD for identifying the location and severity of significant coronary artery stenosis.
Methods: We included patients presenting with chest pain, whereas those with myocardial infarction, arrhythmia, normal coronary angiography, previous percutaneous coronary intervention or coronary artery bypass grafting, and inadequate echocardiographic window were excluded. Among the 738 patients enrolled, a total of 199 study participants with stable CAD were selected and underwent speckle tracking echocardiography.
Results: Regional longitudinal strain (RLS) identified significant stenosis in at least 1 of the coronary arteries with sensitivity and specificity rates of 89.4% and 87.8%, respectively, and an area under curve (AUC) of 0.947 (P < .001). Receiver operating characteristic curve comparison demonstrated RLS had the highest predictive value for identifying significant stenosis with an optimal cutoff of ≥ -16% compared with regional radial strain (RRS) (AUC difference, 0.149; 95%CI, 0.132-0.167; P ≤ .0001), regional wall motion abnormality (RWMA) (AUC difference, 0.277; 95%CI, 0.262-0.293; P ≤ .0001), and regional circumferential strain (RCS) (AUC difference, 0.348; 95%CI, 0.327-0.368; P ≤ .0001).
TLS predicted significant proximal left anterior descending coronary artery stenosis when ≥ 4 of 7 territorial segments were impaired, significant proximal left circumflex artery stenosis when ≥ 3 of 5 territorial segments were impaired, and significant proximal right coronary artery stenosis when ≥ 3 of 5 territorial segments were impaired.
Conclusions: TLS predicted the location and severity of significant coronary artery stenosis in patients with stable CAD.
[Trial registration No. Md 110/2021].
Keywords: Coronary artery disease. Echocardiography. Ventricular dysfunction. Global longitudinal strain.
RESUMEN
Introducción y objetivos: Existen pocos datos sobre la deformación longitudinal territorial (DLT) como marcador ecocardiográfico en la enfermedad arterial coronaria (EAC) estable. El objetivo fue evaluar el valor predictivo de la DLT en la EAC estable para identificar la localización y el grado de estenosis coronaria significativa.
Métodos: Se incluyó a pacientes con dolor torácico y se excluyó a aquellos con infarto de miocardio, arritmia, angiografía coronaria normal, intervención coronaria percutánea o cirugía de revascularización aortocoronaria previas, o ventana ecocardiográfica deficiente. De los 738 pacientes incluidos se seleccionó a 199 con EAC estable, a los que se realizó una ecocardiografía con rastreo de marcas.
Resultados: La deformación longitudinal regional (DLR) identificó estenosis significativa en al menos 1 de las arterias coronarias, con una sensibilidad del 89,4%, una especificidad del 87,8% y un área bajo la curva (AUC) de 0,947 (p < 0,001). La comparación de las curvas ROC mostró que la DLR tenía el mejor valor predictivo para identificar estenosis significativa con un punto de corte ≥ –16% en comparación con la deformación radial regional (DRR) (la diferencia entre las AUC de la DLR y la DRR es 0,149; IC95%, 0,132-0,167; p ≤ 0,0001), la alteración de la contractilidad segmentaria (ACS) (la diferencia entre las AUC de la DLR y la ACS es de 0,277; IC95%, 0,262-0,293; p ≤ 0,0001) y la deformación circunferencial regional (la diferencia entre las AUC de la DLR y de la deformación circunferencial regional es de 0,348; IC95%, 0,327-0,368; p ≤ 0,0001). La DLT predijo una estenosis significativa de la arteria descendente anterior izquierda proximal si al menos 4 de los 7 segmentos territoriales estaban afectados, una estenosis significativa de la arteria circunfleja izquierda proximal si al menos 3 de los 5 segmentos territoriales estaban afectados, y una estenosis significativa de la arteria coronaria derecha proximal si al menos 3 de los 5 segmentos territoriales estaban afectados.
Conclusiones: La DLT predijo la ubicación y el grado de estenosis coronaria significativa en pacientes con EAC estable.
[Número de registro del estudio: Md 110/2021].
Palabras clave: Enfermedad arterial coronaria. Ecocardiografía. Disfunción ventricular. Deformación longitudinal global.
Abbreviations
CAD: coronary artery disease. GCS: global circumferential strain. GLS: global longitudinal strain. RLS: regional longitudinal strain. RRS: regional radial strain. RWMA: regional wall motion abnormality.
INTRODUCTION
Coronary artery disease (CAD) is a significant national and global public health concern. In 2021, more than 254 million cases of CAD were diagnosed worldwide, with an incidence rate of 403.89 new cases per 100,000 people and a mortality rate of 113.94 deaths per 100,000. In Egypt, CAD is the most prevalent cardiovascular disease among men and women, with an overall prevalence of 4.27%.1 Key risk factors for CAD include smoking, gender, diabetes, hypertension, and dyslipidemia, with men experiencing a 2-fold higher rate than women.2 Computed tomography is the standard diagnostic imaging modality for stable CAD, while high sensitivity C-reactive protein is recommended for predicting stable CAD. Although regional wall motion abnormality (RWMA) is the gold standard echocardiographic marker for stable CAD, it is not effective in detecting subclinical myocardial damage.3
Two-dimensional (2D) speckle tracking echocardiography (STE) strain analysis measures myocardial deformation providing a more reliable evaluation of myocardial mechanics and addressing the limitation of RWMA in identifying subtle myocardial damage.4 Real-world evidence suggests that global (GLS) and regional longitudinal strain (RLS) offer better diagnostic accuracy and reproducibility in detecting stable CAD.5-7 GLS assesses ventricular shortening from base to apex to estimate overall strain in the left ventricle (LV), whereas RLS focuses on strain in specific LV segments. Other strain analysis methods include global radial strain (GRS), global circumferential strain (GCS), territorial longitudinal strain (TLS), regional radial strain (RRS), and regional circumferential strain (RCS), each measuring different aspects of myocardial strain.8 Our study aimed to evaluate the predictive role of TLS in stable CAD for identifying significant coronary artery lesions with ≥ 70% diameter stenosis.
METHODS
Study design
We conducted a 24-month cross-sectional, open-label, single-cohort, single-center study was at the cath lab of a tertiary care teaching hospital. Investigators were not blinded to the study group. Prior to conducting the study, its design and protocol were reviewed, approved, and registered with Ain Shams University Hospital Human Ethics Committee on 1 July 2021 under trial registration No. Md 110/2021.
Written informed consents was obtained from all human research subjects and study participants. Participant privacy rights were strictly protected, data were anonymized, and study procedures were conducted in accordance with the Egyptian National Commission for Bioethics statement on ethical conduct in human research. Furthermore, the study adhered to the SAGER guidelines to address potential sex- and gender-related bias.
Study participants
Patients with typical or atypical anginal chest pain evaluated at the outpatient clinic and cath lab of a single tertiary care center between August 2021 and August 2023 were included in the study. Patients with acute coronary syndrome, myocardial infarction, non-sinus rhythm, normal coronary angiography (CAG), prior percutaneous coronary intervention or coronary artery bypass grafting, inadequate echocardiographic window, or valvular or myocardial disease were excluded.
Study procedures
A total of 738 patients were enrolled and undewent history taking and data collection for gender, age, diabetes mellitus, hypertension, smoking, dyslipidemia, chronic kidney disease, peripheral arterial disease, stroke, sedentary lifestyle, myocardial infarction, and family history of CAD. Furthermore, patients undewent blood pressure measurements and comprehensive cardiac examination, including assessment for abnormal auscultatory findings, prior cardiac surgery, cardiomegaly, and heart failure. Moreover, all patients underwent 12-lead electrocardiogram, 2D echocardiography and 2D STE using an IE 33 ultrasound system (Philips, The Netherlands) with an X5-1 phased-array transducer; CAG with digital image acquisition and storage, complete blood count; lipid profile; liver and kidney function tests; coagulation studies (prothrombin time, activated partial thromboplastin time, and international normalized ratio); and serial cardiac enzyme measurements. The 2D echocardiography was conducted before the CAG and the 2D STE after the CAG. The cardiologists performing 2D echocardiography and 2D STE were specialized in echocardiography, held level III competency according to the European Society of Cardiology Core Curriculum, and were blinded to the coronary angiographic data.9 Furthermore, the interventional cardiologists, who analyzed the CAGs were blinded to the results of the echocardiographic evaluation. Data documented with CAG included the severity of coronary artery stenosis according to the Coronary Artery Disease-Reporting and Data System and the regional distribution of the area supplied with the epicardial coronary artery according to the 17 LV segment model. A coronary lesion of ≥ 70% diameter stenosis was considered significant, and such patients were classified as having severe stable CAD.10 A consecutive sample of 199 eligible participants with severe stable CAD was selected, assigned, and allocated to a single group (figure 1). Operators performing 2D echocardiography and 2D STE were blinded to the coronary angiographic data. Data documented with 2D echocardiography and 2D STE included RWMA, wall motion score index (WMSI), and strain analysis. RWMA was categorized into normal with an assigned score of 1, hypokinetic with an assigned score of 2, akinetic with an assigned score of 3, and dyskinetic with an assigned score of 4. The WMSI represents the average RWMA of the 17 analyzed segments in a 17 LV segment model.11 Myocardial function by strain imaging was evaluated on a frame-by-frame basis by automatic tracking of acoustic markers (speckles) throughout the cardiac cycle in a 17 LV segment model, and GLS was obtained by averaging the myocardial function of all 17 segments. The endocardial borders were traced in the end-systolic frame of the 2D images from the 3 apical views for analyses of longitudinal strains. RCS analysis was obtained from the 3 parasternal short-axis views. RRS analysis from the 3 apical views was conducted manually by tracking the average peak systolic radial excursion for each segment between 2 points (endocardial and epicardial) of 3 levels for each of the 17 segments. Peak systolic strains were obtained for 17 longitudinal, 17 radial, and 16 circumferential LV segments. All segmental values were averaged to GLS and GCS for each study participant and automatically displayed in a bull’s-eye plot. TLS measured the number of impaired territories based on the cutoff results of the RLS analysis from the segments supplied with the corresponding coronary arteries in a 17 segment LV model as follows: 7 segments for the left anterior descending coronary artery (LAD), 5 for the right coronary artery (RCA), and 5 for the left circumflex artery (LCx).12
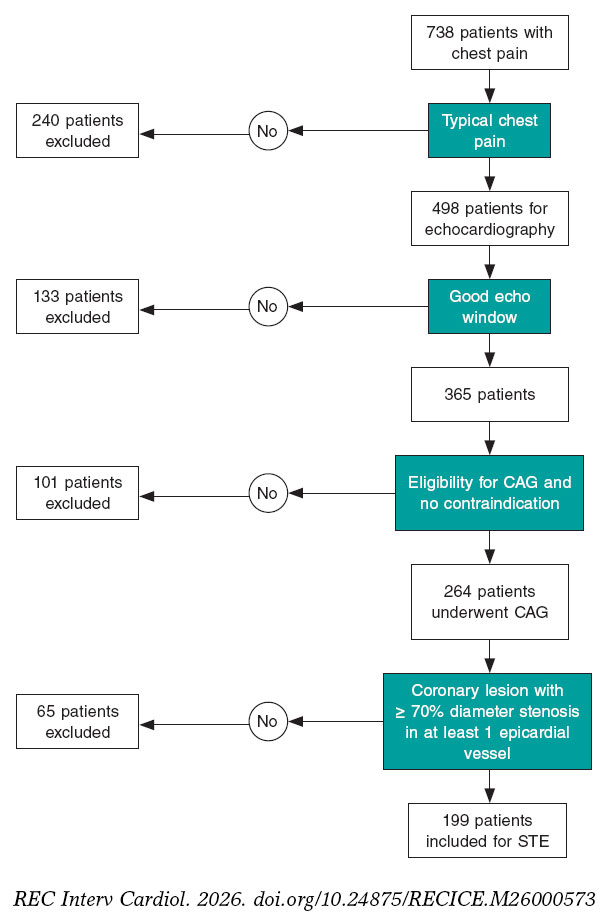
Figure 1. Flow chart of stable coronary artery disease cohort selection. CAG, coronary angiography; STE, speckle tracking echocardiography.
Endpoints
The endpoint of the study was the predictive role of TLS in stable CAD for identifying the location and severity of significant coronary artery lesion with ≥ 70% diameter stenosis.
Statistical analysis
Our study was a cross-sectional, open-label, single cohort, single center study. The echocardiographic assessment outcomes were coded, and data were analyzed with the SPSS v29 software package (IBM, United States). Shapiro-Wilks test was used to assess normality of data. Qualitative data was expressed as frequencies (number of cases) and relative frequencies (percentages), and quantitative data as means, standard deviations, medians, and interquartile ranges. Comparisons of parametrically distributed quantitative variables were performed using the Student t test or analysis of variance (ANOVA), whereas nonparametrically distributed quantitative variables were compared using the Mann-Whitney test, and between qualitative variables using the chi-square test or Fishers exact test, as appropriate.13,14 Inter- and intra-observer variability was assessed by reanalyzing the data of 18 randomly selected study participants and reported as intraclass correlation coefficient (ICC), whose scale ranges from 0 to 1 where 1 represents perfect reliability with no measurement error and 0, no reliability. An ICC value < 0.5 indicates poor reliability; 0.5-0.75, moderate reliability; 0.75-0.9, good reliability; and > 0.90, excellent reliability.15 The area under the curve (AUC) was constructed to detect the cutoff for optimal sensitivity and specificity of regional strains. Receiver operating characteristic (ROC) curve comparison was performed using MedCalc version 10.3.1.0 (MedCalc Software, United States). Confidence interval was set to 95% and the accepted margin of error at 5%. 01. A P value <05 was considered statistically significant, and a P value < .01 was considered highly significant. Final analyses were conducted according to the per-protocol approach.
RESULTS
Baseline characteristics and sociodemographic features
The baseline characteristics and sociodemographic features of the study cohort are shown in table 1. Male predominance was the pivotal sociodemographic characteristic of the enrolled participants (56.5%), and the mean age was 60.4 ± 9.9years. Baseline risk factors and comorbidities of the study cohort included hypertension in 68.5%, diabetes mellitus in 70%, dyslipidemia in 66%, and smoking in 47%, respectively. There were no withdrawals, and all participants completed the study.
Table 1. Baseline characteristics and sociodemographic features of stable coronary artery disease cohort
| Variable | Stable coronary artery disease cohort (No. = 199) | |
|---|---|---|
| Mean ± SD | Range | |
| Age, (years) | 60.4 ± 9.9 | 38 – 81 |
| Left ventricular ejection fraction | 53.9 ± 6.5 | 40 – 66 |
| Hypertension | 137 | 68.5 |
| Diabetes mellitus | 140 | 70 |
| Dyslipidemia | 132 | 66 |
| Current smoker | 94 | 47 |
| Gender | ||
| Male | 112 (56.6) | – |
| Female | 87 (43.5) | – |
|
Unless otherwise indicated, data are expressed as number (No.) and percentage (%) or mean ± standard deviation (SD). |
||
Coronary angiographic characteristics of stable coronary artery disease cohort
The location and severity of significant coronary lesions with ≥ 70% diameter stenosis is shown in table 2. Most study participants had single-vessel disease (68%). Among significant lesions, 63 (22%) were located in the LCx, 121 (43%) in the LAD, and 98 (35%) in the RCA.
Table 2. Coronary angiographic characteristics of stable coronary artery disease cohort
| Variable | Stable coronary artery disease cohort (No. = 199) | |||||
|---|---|---|---|---|---|---|
| Site of significant coronary lesions with ≥ 70% diameter stenosis (No., %) | Single-vessel disease | 2-vessel disease | 3-vessel disease | |||
| No. | % | No. | % | No. | % | |
| 135 | 68 | 45 | 23 | 19 | 10 | |
| Level of significant coronary lesions with ≥ 70% diameter stenosis (No., %) | LAD | LCX | RCA | |||
| No. | % | No. | % | No. | % | |
| Proximal | 74 | 61 | 40 | 63 | 51 | 52 |
| Mid | 42 | 35 | 0 | 0 | 16 | 16 |
| Distal | 5 | 4 | 23 | 37 | 31 | 32 |
| Total | 121 | 100 | 63 | 100 | 98 | 100 |
|
LAD, left anterior descending coronary artery; LCx, left circumflex artery; RCA, right coronary artery. |
||||||
Strain analysis of stable coronary artery disease cohort
The global strain analysis showed a GLS range of -26% to -8%, with a mean value of -16.4 ± 3.6%, and a GCS range of -35% to -10%, with a mean value of -18.4 ± 4.9%. The regional strain analysis (RSA) of 3383 segments showed RWMA in 3378 segments (99.8%), a mean WMSI of 1.3 ± 0.2 with sensitivity and specificity rates of 88% and 61%, respectively, GLS in 3365 segments (99.5%), GCS in 3184 segments (100%), global radial strain in 3352 segments (99%), significant hypoperfusion (coronary lesions with ≥ 70% diameter stenosis) in 1472 segments (43%), and normal perfusion to mild-to-moderate hypoperfusion (coronary lesions with < 70% diameter stenosis) in 1911 segments (57%). The medians and the interquartile ranges of the regional strain parameters for coronary lesions with ≥ 70% diameter stenosis demonstrated significant differences vs the corresponding parameters for coronary lesions with < 70% diameter stenosis. The median RLS was -20% (IQR, -23% to -17%) for lesions < 70% diameter stenosis vs -12% (IQR, -14% to -9%) for lesions ≥ 70% diameter stenosis (P < .001). The median RRS was 40% (IQR, 38%-43%) for lesions < 70% diameter stenosis vs 33% (IQR, 21%-39%) for lesions ≥ 70% diameter stenosis (P < .001) (figure 2). The median RCS was -19% (IQR, -24% to -14%) for lesions < 70% diameter stenosis vs -17% (IQR, -22% to -12%) for lesions ≥ 70% diameter stenosis (P < .001). RWMA were detected in 38% of the segments supplied by significant coronary lesions with ≥ 70% diameter stenosis compared with 6% of the segments supplied by non-significant coronary lesions with < 70% diameter stenosis (P < .001).
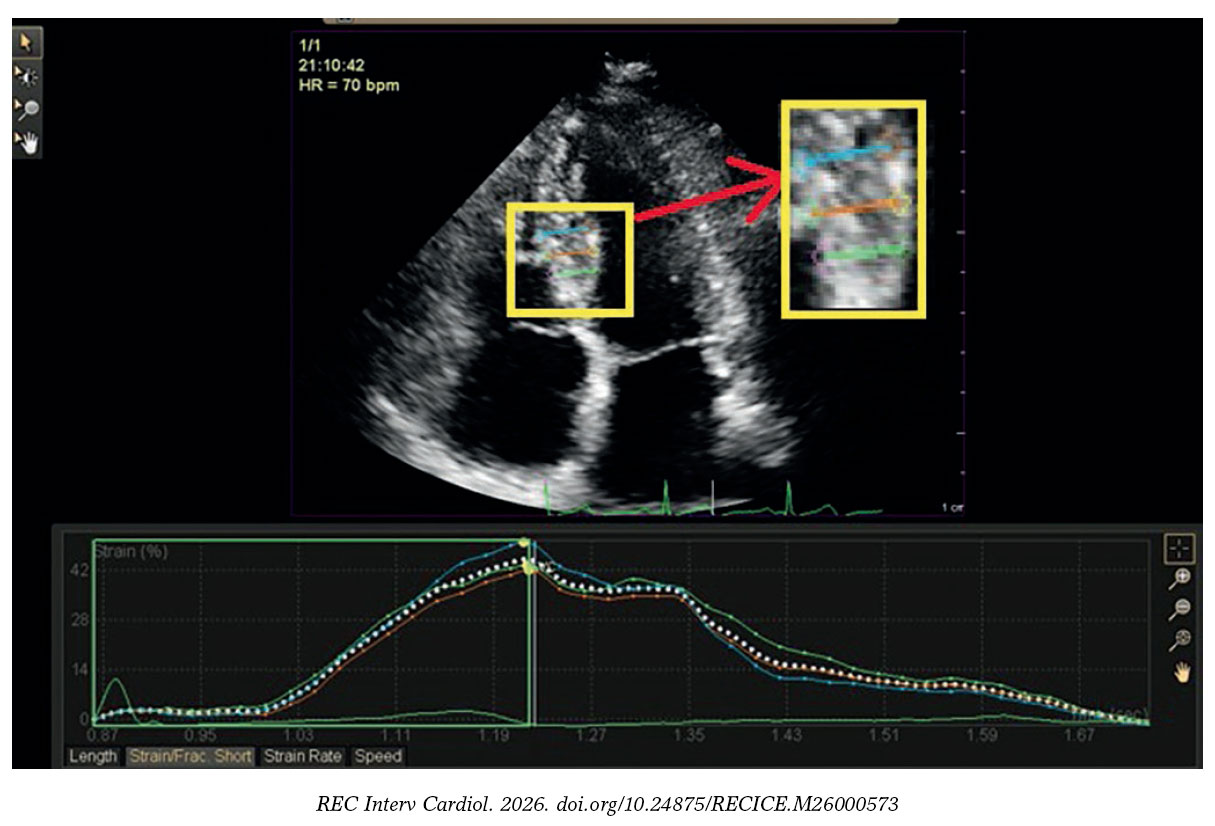
Figure 2. Regional radial strain analysis of a study participant with stable coronary artery disease showing 42% strain of the mid inferoseptal segment.
Feasibility and reproducibility of stable coronary artery disease cohort
The ICC for inter- and intra-observer variability of segmental strains were measured in 21 of the 199 patients study cohort (11%). The results of the ICC for inter- and intra-observer variability of segmental strains were 0.91 and 0.96 for GLS, 0.94 and 0.97 for GCS, and 0.86 and 0.92 for GRS.
ROC curve and area under the curve analysis in patients with stable coronary artery disease
AUC was constructed to detect the cutoff for optimal sensitivity and specificity of regional strains (table 3). The AUC for RLS was 0.947 (P < .001) which detected a cutoff of ≥ -16% for optimal sensitivity and specificity of RLS. ROC curve comparison showed that RLS exhibited the highest predictive value for identifying significantly hypoperfused segments (with ≥ 70% diameter stenosis) at a cutoff of ≥ -16% vs the RRS (AUC difference, 0.149; 95%CI, 0.132-0.167; P ≤ .0001), RWMA (AUC difference, 0.277; 95%CI, 0.262-0.293; P ≤ .0001), and RCS (AUC differ- ence, 0.348; 95%CI, 0.327-0.368; P ≤ .0001), respectively (figure 3).
Table 3. Area under curve for detection of cutoff for optimal sensitivity and specificity of the regional strains
| Variable | Cutoff | AUC | 95%CI | Sensitivity (%) | Specificity (%) | P-value |
|---|---|---|---|---|---|---|
| RLS | ≥ -16 | 0.947 | 0.938-0.953 | 89.4 | 87.8 | < .001* |
| RCS | ≥ -19 | 0.599 | 0.582-0.617 | 60.7 | 54.4 | < .001* |
| RRS | ≤ 35 | 0.8 | 0.786-0.813 | 57.8 | 92.3 | < .001* |
|
Data is presented as percentages. 95%CI, 95% confidence interval; AUC, area under the curve; RCS, regional circumferential strain; RLS, regional longitudinal strain; RRS, regional radial strain. * Statistically significant P value. |
||||||
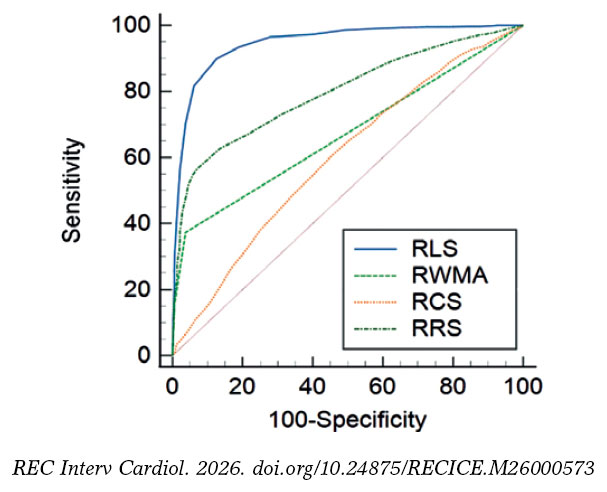
Figure 3. Receiving operating characteristic curve comparison of stable coronary artery disease cohort comparing regional longitudinal strain, regional radial strain, regional circumferential strain, and regional wall motion abnormalities in predicting significant ≥ 70% diameter stenosis. RCS, regional circumferential strain; RLS, regional longitudinal strain; RRS, regional radial strain; RWMA, regional wall motion abnormality.
ROC curve analysis of regional longitudinal strain in patients with stable coronary artery disease
Guided by the detected cutoff of ≥ -16% for the optimal sensitivity and specificity of RLS, the predictive role of TLS in stable CAD for identifying the location and severity of significant coronary artery lesions with ≥ 70% diameter stenosis was explored (table 4). The ROC curve analysis of the RLS at a cutoff of ≥ -16% demonstrated that the optimal number of impaired segments that could predict the location and severity of significant coronary lesions with ≥ 70% diameter stenosis was ≥ 3 impaired segments out of the 7 territorial segments of LAD to predict proximal or significant lesion in the mid-LAD and ≥ 3 impaired segments among the 5 territorial segments of either the LCx or RCA to predict proximal significant lesion in the LCx or RCA (figure 4).
Table 4. Receiving operating characteristic curve analysis of regional longitudinal strain
| Vessel | Level | No. | AUC | Sensitivity (%) | Specificity (%) | 95%CI | P-value |
|---|---|---|---|---|---|---|---|
| LAD (7 segments) | Proximal | ≥ 4 | 0.952 | 93.20 | 83.30 | 0.913-0.977 | < .001* |
| Mid | ≥ 3 | 0.911 | 92.20 | 73.80 | 0.862-0.946 | < .001* | |
| Distal | ≥ 2 | 0.902 | 95.80 | 68.30 | 0.852-0.939 | < .001* | |
| LCx (5 segments) | Proximal | ≥ 3 | 0.897 | 87.50 | 85 | 0.846-0.935 | < .001* |
| Distal | ≥ 2 | 0.87 | 92 | 70.80 | 0.815-0.913 | < .001* | |
| RCA (5 segments) | Proximal | ≥ 3 | 0.928 | 88.20 | 83.90 | 0.883-0.960 | < .001* |
| Mid | ≥ 3 | 0.942 | 88 | 92.50 | 0.9-0.970 | < .001* | |
| Distal | ≥ 2 | 0.932 | 91.80 | 80.40 | 0.888-0.963 | < .001* | |
|
Receiving operating characteristic curve analysis of regional longitudinal strain in stable coronary artery disease to explore the role of territorial longitudinal strain in predicting the site and level of significant ≥ 70% diameter stenosis. 95%CI, 95% confidence interval; AUC, area under the curve; LAD, left anterior descending coronary artery; LCx, left circumflex artery; RCA, right coronary artery. * Statistically significant P value. |
|||||||
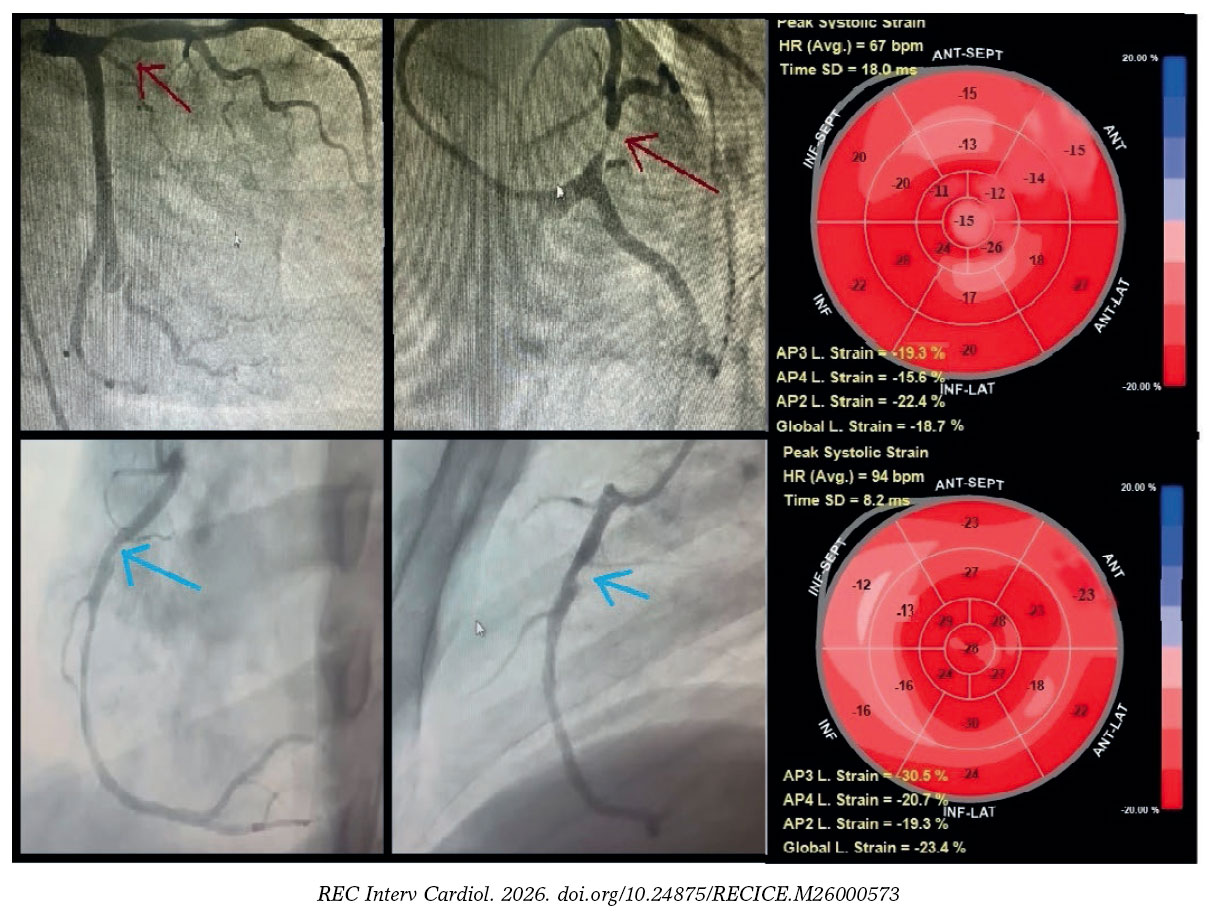
Figure 4. Territorial longitudinal strain of study participants with stable coronary artery disease. Top row: representative study participant with significant proximal left anterior descending coronary artery lesion (≥ 70% diameter stenosis; red arrow). Global longitudinal (L) strain was -18.7%. Seven segments within the left anterior descending coronary artery territory (anteroseptal, anterior regions, and apex) demonstrated impaired strain (≥ -16%), consistent with a true-positive finding, whereas left circumflex and right coronary artery territories showed preserved strain (< -16%), consistent with true-negative findings. Bottom row: representative of a study participant with a significant proximal right coronary artery lesion (≥ 70% diameter stenosis; blue arrow). Global longitudinal strain was -23.3%. Four segments within the right coronary artery territory (mid, basal inferior, and inferoseptal) demonstrated impaired strain (≥ -16%), consistent with a true-positive finding, whereas left anterior descending artery and left circumflex artery territories showed preserved strain (< -16%), consistent with true-negative findings.
DISCUSSION
Despite being the gold standard echocardiographic marker for stable CAD, RWMA is ineffective at detecting subclinical myocardial damage.3 Our study aimed to evaluate the predictive capability of TLS in identifying the location and severity of significant coronary lesions with ≥ 70% diameter stenosis.
Participants in our study had a mean age of 60.4 ± 9.9 years (range, 38-81 years), with 112 men (56.5%). Most participants had single-vessel disease (68%); 45 (23%), 2-vessel disease; and 19 (10%), 3-vessel disease. Significant coronary lesions with ≥ 70% diameter stenosis were located in the LCx, LAD, and RCA in 63 (22%), 121 (43%), and 98 cases (35%), respectively. Similarly, Koulaouzidis et al. found that 57% of their participants had single-vessel disease with ≥ 50% diameter stenosis.16 Observational studies suggest that most single-vessel coronary occlusions occur in the proximal LAD.17,18
In our cross-sectional study, GLS ranged from -26% to -8%, averaging -16.4 ± 3.6%, while RLS for lesions < 70% diameter stenosis was -20% (IQR, -23% to -17%) vs -12% (IQR, -14% to -9%) for lesions ≥ 70% diameter stenosis (P < .001). Norum et al. concluded that a GLS cutoff of -17.4% to -20.3% could predict CAD in patients with chest pain, with sensitivity rates between 51% and 81% and specificity rates between 58% and 81%.19 There is limited real-world data on RSA in stable CAD. Montgomery et al. found that summed LAD segmental strain demonstrated a sensitivity and specificity of 66% at a cutoff of -20.3% for predicting LAD lesions ≥ 50% diameter stenosis.20 Shimoni et al. demonstrated that segmental analysis using the least 10-percentile peak systolic strain (PSS) outperformed global PSS and GLS.21 Biering-Sørensen et al. observed that significant left main stenosis (≥ 70%) affected apical longitudinal strain (ALS) more than significant lesions did in the LAD or LCx, despite similar GLS results.22 Carstensen et al. studied asymptomatic CAD in patients with aortic stenosis using an 18-segment LV model, finding that only ALS and mid-longitudinal strain were significant independent predictors of asymptomatic CAD, which is consistent with other studies indicating that proximal lesions impact all defined regions.23-25 Liu et al. showed that a cutoff of ≥ -23.5% for endocardial RLS and GLS of the LAD was higher in identifying significant LAD stenosis (≥ 50%) vs strain values from other layers.26
Our findings indicate that at a cutoff of ≥ -16%, TLS can predict the location and severity of significant coronary lesions with ≥ 70% diameter stenosis. Specifically, impairment of ≥ 3 of 7 in the LAD predicted significant proximal or mid lesions, whereas impairment of ≥ 3 of 5 segments in either the LCx or RCA predicted significant proximal lesions. TLS has not been extensively studied in stable CAD. Eek et al. found that at a cutoff of ≥ -14%, impaired blood supply in ≥ 4 segments predicted acute coronary occlusion with improved sensitivity (85%) and specificity (70%) vs the left ventricular ejection fraction.12 Sarvari et al. noted that although TLS, GLS, and GCS were affected in patients with non-ST-segment elevation myocardial infarction, the differences between GLS and TLS were not statistically significant.24 Caspar et al. demonstrated that TLS has high predictive value for significant lesions with ≥ 50% diameter stenosis across the 3 major coronary territories.25
The takeaway from our study is that TLS enhances the diagnostic capacity of RLS, accurately predicting both the location and severity of significant coronary lesions with ≥ 70% diameter stenosis. While several non-invasive methods show acceptable sensitivity and specificity,27 they usually face limitations regarding availability and cost. Echocardiography is widely accessible, and strain analysis can be performed offline, making it beneficial for patients with chest pain, allowing for assessment prior to invasive procedures or costly imaging modalities. Further studies are needed to clarify the diagnostic and prognostic significance of TLS in patients with chest pain.
Strengths and limitations
Our study was conducted on a well-balanced cohort with regards to the risk factors and baseline characteristics and did not have missing data allowing robust per protocol analysis, the interventional cardiologists who analyzed the CAGs were blinded to the results of the echocardiographic evaluation, whereas the investigators who performed the 2D echocardiography and the 2D STE were blinded to the coronary angiographic data, hence observer bias was minimized. Despite its strengths, the limitations of the study require consideration. It was a single centre cross-sectional study which didn’t allow us to investigate the chronological relationship between the echocardiographic and the coronary angiographic data in stable patients with CAD. There was no invasive functional assessment of the coronary blood flow with fractional flow reserve, RRS was assessed manually, and 36 study participants (18%) with impaired myocardial function (left ventricular ejection fraction ≤ 50%) were selected for the study. Patients with stable CAD patients and coronary microvascular disease (microvascular angina) and normal CAG and patients with stable CAD and abnormal CAG with coronary lesions with < 70% diameter stenosis were excluded from the study cohort overestimating the RLS of the study cohort. Inclusion of patints with stable CAD and abnormal CAG with coronary lesions with ≥ 70% diameter stenosis could only limit the generalizability of the study results to the population with stable CAD. Ultimately, ROC curve analysis of RLS in stable CAD, used to explore the role of TLS in predicting the location and severity of significant ≥ 70% diameter stenosis relied on clinically limited metrics, namely sensitivity and specificity. As a result, the high RLS performance estimate (0.947) may be biased, and the cutoff of ≥ -16% potentially misleading. Consequently, WMSI was not included in the analyss, and no incremental diagnostic value for RLS over WMSI could be established.
CONCLUSIONS
RLS indicated potential clinical relevance in the diagnosis of stable CAD and TLS demonstrated a significant ability to predict the site and level of significant coronary lesion with ≥ 70% diameter stenosis in patients with stable CAD.
DATA AVAILABILITY
Data are available from the corresponding author upon request.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
The study design and protocol were approved by the human ethics committee of the Ain Shams University Hospital before study initiation on 1 July, 2021. The study was registered and assigned trial registration No. Md 110 / 2021. Written informed consent was obtained from all human research subjects and study participants, including consent for publication. Participant privacy was strictly protected, and all data were anonymized, informed consents were signed by study participants for publication, and the study procedures were conducted in full compliance with the Egyptian National Commission for Bioethics statement on ethical conduct in human research, and SAGER guidelines have been followed with respect to possible sex/gender bias.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
The authors declare that they have not used any type of generative artificial intelligence for the drafting of this manuscript, nor for the creation of images, graphics, tables, or their corresponding captions.
AUTHORS’ CONTRIBUTIONS
The study was designed by A. Rezq and H. Shaalan, the data was collected, analyzed, and interpreted by M.A. Hashem and A.E. Nayel, the manuscript was drafted by M.A. Hashem and critically reviewed by A. Rezq, A.K. Araquib, A.E. Nayel, and H. Shaalan, and A. Rezq, A.E. Nayel, A.K. Araquib, and H. Shaalan approved the final manuscript. The authors take full responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
CONFLICTS OF INTEREST
None declared.
WHAT IS KNOWN ABOUT THE TOPIC?
- CAD is the most prevalent cardiovascular condition among Egyptian men and women, with an overall prevalence of 4.27%. Computed tomography is the standard diagnostic imaging modality for stable CAD, while high sensitivity C-reactive protein is the recommended test for predicting stable CAD.
- Although RWMA is the gold standard echocardiographic marker for stable CAD, it is not effective in detecting subclinical myocardial damage.
- Real-world evidence shows that myocardial strain analysis methods with 2D STE, including RLS, GLS, GCS, TLS, and RRS, offer better diagnostic accuracy and reproducibility in detecting stable CAD, provide a more reliable evaluation of myocardial mechanics in stable CAD, and address the limitation of RWMA in identifying subtle myocardial damage.
WHAT DOES THIS STUDY ADD?
- Our study showed that, at a cutoff of ≥ -16%, RLS is the optimal imaging biomarker for predicting significant ≥ 70% diameter stenosis in stable CAD.
- Our study showed that TLS is a promising imaging biomarker for predicting the site and level of significant ≥ 70% diameter stenosis in stable CAD.
REFERENCES
1. GBD Results. Institute for Health Metrics and Evaluation. 2025. Available at:https://vizhub.healthdata.org/gbd-results. Consulted 15 May 2025.
2. Gao Z, Chen Z, Sun A, Deng X. Gender differences in cardiovascular disease. Med Nov Technol Devices. 2019;4:100025.
3. Bansal M, Kasliwal RR. How do I do it?Speckle-tracking echocardiography. Indian Heart J. 2013;65:117-123.
4. Muraru D, Niero A, Rodriguez-Zanella H, Cherata D, Badano L. Three-dimensional speckle-tracking echocardiography:benefits and limitations of integrating myocardial mechanics with three-dimensional imaging. Cardiovasc Diagn Ther. 2018;8:101-117.
5. Reant P, Labrousse L, Lafitte S, et al. Experimental validation of circumferential, longitudinal, and radial 2-dimensional strain during dobutamine stress echocardiography in ischemic conditions. J Am Coll Cardiol. 2008; 51:149-157.
6. Bajracharya P, Acharya KP, Banerjee SK, et al. Correlation between Myocardial Strain by 2-D Speckle-Tracking Echocardiography and Angiographic findings by Coronary Angiogram in Stable Angina. Maedica (Bucur). 2020; 15:365-372.
7. Norum IB, Otterstad JE, Ruddox V, Bendz B, Edvardsen T. Novel regional longitudinal strain by speckle tracking to detect significant coronary artery disease in patients admitted to the emergency department for chest pain suggestive of acute coronary syndrome. J Echocardiogr. 2022;20:166-177.
8. Cerqueira MD, Weissman NJ, Dilsizian V, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation. 2002;105:539-542.
9. Popescu BA, Andrade MJ, Badano LP, et al. European Association of Echocardiography recommendations for training, competence, and quality improvement in echocardiography. Eur J Echocardiogr. 2009;10:893-905.
10. Knipe H, Martínez Juárez D, Silverstone L, et al. Coronary artery disease. Radiology Reference Article. Radiopaedia. 2026. https://doi.org/10.53347/rID-43406
11. Steeds RP, Wheeler R, Bhattacharyya S, et al. Stress echocardiography in coronary artery disease:a practical guideline from the British Society of Echocardiography. Echo Res Pract. 2019;6:G17-G33.
12. Eek C, Grenne B, Brunvand H, et al. Strain echocardiography predicts acute coronary occlusion in patients with non-ST-segment elevation acute coronary syndrome. Eur J Echocardiogr. 2010;11:501-508.
13. Chan YH. Biostatistics 102:quantitative data - Parametric &non-parametric Tests. Singap Med J. 2003;44:391–396.
14. Chan YH. Biostatistics 103:qualitative data –tests of Independence. Singap Med J. 2003;44:498–503
15. Koo TK, Li MY. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J Chiropr Med. 2016;15:155-163.
16. Koulaouzidis G, Kleitsioti P, Kalaitzoglou M, et al. Left Ventricular Longitudinal Strain Detects Ischemic Dysfunction at Rest, Reflecting Significant Coronary Artery Disease. Diagnostics (Basel). 2025;15:1102.
17. Ahmed IAM, Khalid NHM, Abd-Elmagid AEM, Abdullah MAM, Musa AMI, Al-Qarni NO. Common coronary artery occlusions in patients with myocardial infarction. Pan Afr Med J. 2022;42:254.
18. Wang TY, Zhang M, Fu Y, et al. Incidence, distribution, and prognostic impact of occluded culprit arteries among patients with non-ST-elevation acute coronary syndromes undergoing diagnostic angiography. Am Heart J. 2009;157:716-723.
19. Norum IB, Ruddox V, Edvardsen T, Otterstad JE. Diagnostic accuracy of left ventricular longitudinal function by speckle tracking echocardiography to predict significant coronary artery stenosis. A systematic review. BMC Med Imaging. 2015;15:25.
20. Montgomery DE, Puthumana JJ, Fox JM, Ogunyankin KO. Global longitudinal strain aids the detection of non-obstructive coronary artery disease in the resting echocardiogram. Eur Heart J Cardiovasc Imaging. 2012; 13:579-587.
21. Shimoni S, Gendelman G, Ayzenberg O, et al. Differential effects of coronary artery stenosis on myocardial function:the value of myocardial strain analysis for the detection of coronary artery disease. J Am Soc Echocardiogr. 2011;24:748-757.
22. Biering-Sørensen T, Hoffmann S, Mogelvang R, et al. Myocardial strain analysis by 2-dimensional speckle tracking echocardiography improves diagnostics of coronary artery stenosis in stable angina pectoris. Circ Cardiovasc Imaging. 2014;7:58-65.
23. Carstensen HG, Larsen LH, Hassager C, Kofoed KF, Jensen JS, Mogelvang R. Association of ischemic heart disease to global and regional longitudinal strain in asymptomatic aortic stenosis. Int J Cardiovasc Imaging. 2015; 31:485-495.
24. Sarvari SI, Haugaa KH, Zahid W, et al. Layer-specific quantification of myocardial deformation by strain echocardiography may reveal significant CAD in patients with non-ST-segment elevation acute coronary syndrome. JACC Cardiovasc Imaging. 2013;6:535-544.
25. Caspar T, Samet H, Ohana M, et al. Longitudinal 2D strain can help diagnose coronary artery disease in patients with suspected non-ST-elevation acute coronary syndrome but apparent normal global and segmental systolic function. Int J Cardiol. 2017;236:91-94.
26. Liu C, Li J, Ren M, et al. Multilayer longitudinal strain at rest may help to predict significant stenosis of the left anterior descending coronary artery in patients with suspected non-ST-elevation acute coronary syndrome. Int J Cardiovasc Imaging. 2016;32:1675-1685.
27. Danad I, Szymonifka J, Twisk JWR, et al. Diagnostic performance of cardiac imaging methods to diagnose ischaemia-causing coronary artery disease when directly compared with fractional flow reserve as a reference standard:a meta-analysis. Eur Heart J. 2017;38:991-998.
ABSTRACT
Introduction and objectives: Rapid ventricular pacing is essential to ensure accurate valve deployment during transcatheter aortic valve implantation (TAVI). Although it is traditionally performed via right ventricular (RV) pacing using a temporary pacemaker, left ventricular (LV) pacing with pre-shaped guidewires has emerged as an effective alternative, associated with shorter procedural and fluoroscopy times. There are no data available on the use of the Abbott Circulo guidewire. The aim of this study was to evaluate its safety and efficacy profile for LV pacing during TAVI.
Methods: This was a prospective, multicenter, observational study with patients undergoing transfemoral TAVI with LV pacing using the Circulo guidewire. The primary endpoint was pacing efficacy, defined as a reduction in systolic blood pressure < 60 mmHg. Secondary endpoints included the pacing threshold, crossover to RV pacing, and perioperative complications.
Results: A total of 50 patients were enrolled from March through June 2025 (mean age, 80.56 ± 6.26 years; 62% women). Rapid LV pacing was successful in 100% of cases, with a mean pacing threshold of 7.00 ± 3.48 mV. A total of 3 patients required crossover to RV pacing due to atrioventricular block after balloon predilatation. The overall rate of complications was 14%, with rhythm disturbances being the most common adverse events. There were no complications associated with the use of the Circulo guidewire.
Conclusions: LV pacing using the Circulo guidewire during TAVI is safe and effective, and avoids the routine use of temporary transvenous pacemakers.
Keywords: Transcatheter aortic valve implantation. Left ventricular pacing. Pre-shaped guidewire. Rapid pacing. Pacemaker. Structural heart procedure.
RESUMEN
Introducción y objetivos: La estimulación ventricular rápida es esencial para la correcta colocación de la prótesis durante el implante percutáneo de válvula aórtica (TAVI). Aunque clásicamente se realiza mediante estimulación del ventrículo derecho (VD) con marcapasos transitorio, la estimulación del ventrículo izquierdo (VI) con guías preformadas es una alternativa eficaz, asociada a menor tiempo de procedimiento y de fluoroscopia. No existen estudios publicados sobre el uso de la guía Circulo de Abbott. El objetivo fue evaluar su eficacia y seguridad para la estimulación del VI durante el TAVI.
Métodos: Estudio observacional, prospectivo y multicéntrico que incluyó pacientes sometidos a TAVI transfemoral con estimulación del VI mediante la guía Circulo. El objetivo primario fue la eficacia de la estimulación, definida como una reducción de la presión arterial sistólica por debajo de 60 mmHg. Los objetivos secundarios incluyeron el umbral de estimulación, la conversión a estimulación del VD y las complicaciones periprocedimiento.
Resultados: Entre marzo y junio de 2025 se incluyó a 50 pacientes (edad media 80,56 ± 6,26 años; 62% mujeres). La estimulación rápida del VI fue efectiva en el 100% de los casos, con un umbral medio de 7,00 ± 3,48 mV. Un total de 3 pacientes requirieron estimulación del VD por bloqueo auriculoventricular tras la predilatación con balón. La tasa global de complicaciones fue del 14%, principalmente trastornos de la conducción, sin complicaciones atribuibles a la guía Circulo.
Conclusiones: La estimulación del VI con la guía Circulo durante el TAVI es eficaz y segura, y evita el implante sistemático de un marcapasos transitorio.
Palabras clave: Implante percutáneo de válvula aórtica. Estimulación ventricular izquierda. Guía preformada. Estimulación rápida. Marcapasos. Intervención estructural cardiaca.
Abbreviations
AVB: atrioventricular block. LV: left ventricle. RV: right ventricle. TAVI: transcatheter aortic valve implantation.
INTRODUCTION
Transcatheter aortic valve implantation (TAVI) is one of the treatments that has been shown to improve prognosis and reduce mortality in patients with symptomatic severe aortic stenosis.1 Currently, according to the clinical practice guidelines outlined by the European Society of Cardiology (ESC),2 TAVI is the treatment of choice in patients aged ≥ 70 years, while the American Heart Association and the American College of Cardiology (AHA/ACC) clinical practice guidelines indicate that it may be considered from the age of 65 years.3,4.
Although TAVI is considered a safe procedure, complications may occur;5 however, their incidence has declined over the years owing, among other factors, to advances in preoperative cardiac imaging, the development of improved models of transcatheter heart valves and delivery sheaths, and the increasing experience of the teams performing the procedure.6 However, not all complications are directly associated with valve implantation, and some are due to auxiliary devices used perioperatively. One example is the temporary transvenous pacemaker traditionally used for rapid right ventricular (RV) pacing, which requires an additional puncture (generally in the femoral, jugular, subclavian, or brachial vein) and the insertion of a catheter into the RV.
A meta-analysis published in 2019 reported that, even today, despite the availability of imaging modalities that facilitate implantation, transvenous temporary pacing remains associated with complications in 22.9% of patients.7 Many of these complications could be avoided by performing left ventricular (LV) pacing using the pre-shaped guidewire during TAVI, which eliminates the need for any additional vascular accesses or specific devices.8 In 2019, the randomized clinical trial EASY TAVI compared both techniques showing a similar safety and efficacy profile, resulting in lower costs and shorter procedural and fluoroscopy times with LV pacing.9 Although the utility of the SAFARI 2 (Boston Scientific, United States), Confida (Medtronic, United States), Lunderquist (Cook Medical Inc., United States), Amplatz Extra-Stiff (Cook Medical Inc.), Amplatz Super Stiff (Boston Scientific), and SavvyWire (OpSens Inc., Canada) guidewires has already been demonstrated10,11, there are no studies on the Circulo guidewire (Abbott, United States).12
The aim of this study was to evaluate the performance of the pre-shaped Circulo guidewire for LV pacing during TAVI (figure 1A).
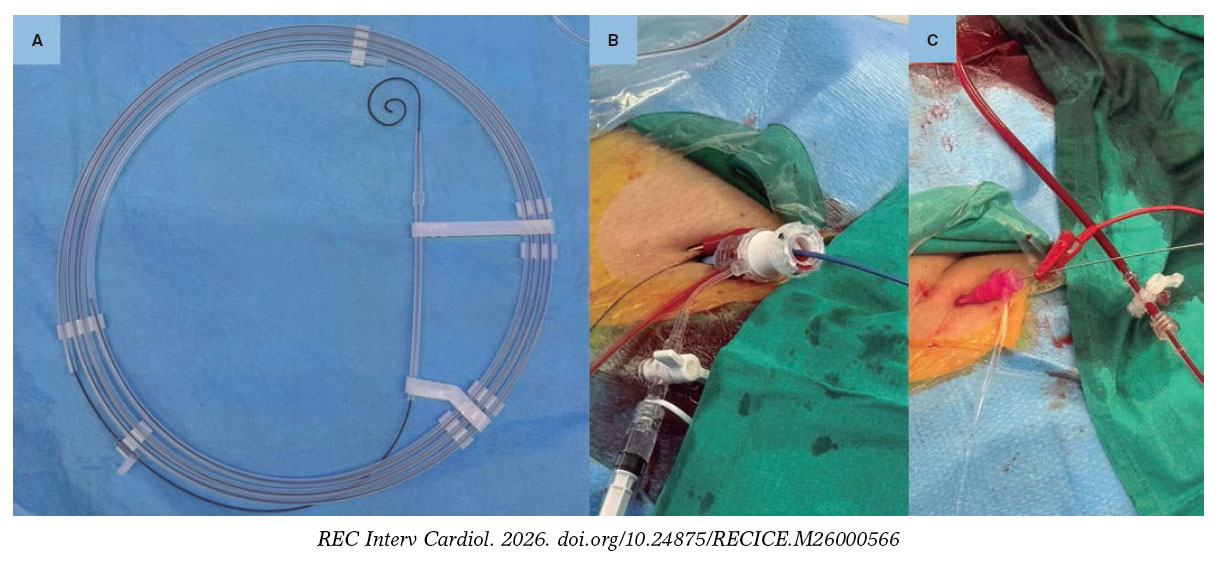
Figure 1. A: pre-shaped Circulo guidewire. B: grounding for left ventricular pacing through the skin. C: grounding for left ventricular pacing through a guidewire.
METHODS
We conducted an observational, prospective, multicenter study. The primary endpoint was to demonstrate the efficacy of rapid LV pacing, defined as a decrease in systemic systolic pressure < 60 mmHg. Secondary endpoints included pacing threshold, the need for conversion to RV pacing, and safety.
The Circulo guidewire
Circulo is a 275-cm–long polytetrafluoroethylene–coated guidewire. It features a double curve at its distal end, with a circular configuration slightly different from that of other guidewires, which reduces ventricular compression. This characteristic is particularly notable in the smaller curve.
Study population
The study protocol was approved by Hospital Clínic de Barcelona Ethics Committee (Barcelona, Spain) in full compliance with the ethical principles outlined in the Declaration of Helsinki. A total of 50 consecutive patients with severe aortic stenosis or regurgitation undergoing TAVI in 8 Spanish centers with the pre-shaped Circulo guidewire for LV pacing were prospectively included. Patients were excluded if, in the investigators’ judgment, they required RV pacing, lacked femoral access, or underwent TAVI without the need for rapid pacing.
Baseline characteristics were collected, including sex, age, weight, height, surgical risk, history of pacemaker implantation, atrial fibrillation, ischemic heart disease, or bundle branch block. Echocardiographic characteristics included LV size, LV ejection fraction, and the presence of severe valvular heart disease.
TAVI with left ventricular pacing
TAVI was performed according to the clinical practice of each center. The grounding configuration for LV pacing and the type of TAVI were decided by each center based on patient characteristics (figure 1B-C). During LV pacing, systemic blood pressure and pacing threshold were measured. To determine the LV pacing threshold, pacemaker output was initially increased to the maximum and then gradually reduced until loss of capture was observed. The lowest voltage capable of capturing the ventricle on all beats was selected. Systemic blood pressure was measured using an arterial catheter.
Procedural characteristics were recorded, including venous access, grounding configuration for LV pacing, LV pacing threshold, systemic blood pressure during rapid LV pacing, conversion to pacing using a different LV guidewire or RV pacing, type and size of the transcatheter heart valve, need for balloon pre- or postdilatation, and complications according to the Valve Academic Research Consortium-3 (VARC-3) criteria, including vascular and access-related complications, hemorrhages, neurological events, new conduction disturbances and arrhythmias, acute kidney injury, structural heart complications, length of stay, and mortality.5
Follow-up
Follow-up was conducted 30 days after TAVI, either by telephone or in person. Complications were adjudicated according to VARC-3 criteria.5
Statistical analysis
Quantitative variables are expressed as mean and standard deviation or median and interquartile range (IQR), depending on whether distribution was normal, as previously assessed using the Kolmogorov–Smirnov test. The qualitative ones are expressed as total number and percentage. Statistical analyses were performed using IBM SPSS Statistics (version 27) and RStudio (version 4.5.1). Depending on the variable, Fisher’s exact test, the Kruskal–Wallis test, or ANOVA was applied.
RESULTS
Baseline characteristics
Baseline characteristics are shown in table 1. A total of 50 patients were included in the study, 31 (62%) women and 19 (38%) men. The mean age of the cohort was 80.56 ± 6.26 years. In terms of past medical history, the mean body mass index was 27.38 ± 4.6 kg/m2; 17 patients (34%) had ischemic heart disease; 12 (24%), atrial fibrillation; 3 (6%), a previously implanted pacemaker; 4 (11.8%), first-degree atrioventricular block (AVB); and 6 (12%), bundle branch block (4 patients had left bundle branch block and 2, right bundle branch block). The PR interval ranged from 140 ms to 240 ms, with a median of 170 ms (IQR, 158-190), and QRS duration ranged from 72 ms to 170 ms, with a median of 90 ms (IQR, 80-110). Median surgical risk, assessed using the EuroSCORE II, was 2.06% (IQR, 1.62-3.36).
Table 1. Baseline characteristics of the patients
| Variable | Total (n = 50) |
|---|---|
| Demographic data | |
| Age (years) | 80.56 ± 6.26 |
| Women | 31 (62) |
| Past medical history | |
| Body mass index (kg/m2) | 27.38 ± 4.6 |
| Ischemic heart disease | 17 (34) |
| Atrial fibrillation | 12 (24) |
| Previous pacemaker | 3 (6) |
| PR duration (ms) | 170 [158-190] |
| QRS duration (ms) | 90 [80-110] |
| First-degree AVB | 4 (11.8) |
| LBBB | 4 (8) |
| RBBB | 2 (4) |
| Surgical risk | |
| EuroSCORE II (%) | 2.06 [1.62-3.36] |
| Echocardiographic characteristics | |
| LV ejection fraction (%) | 58.48 ± 8.63 |
| LV end-diastolic diameter (mm) | 45.28 ± 7.83 |
| Mean gradient (mmHg) | 47.24 ± 19.25 |
| Severe aortic regurgitation | 6 (12) |
| Severe tricuspid regurgitation | 0 (0) |
|
AVB, atrioventricular block; RBBB, right bundle branch block; LBBB, left bundle branch block; LV, left ventricle. Data express n (%), mean ± standard deviation, or median [interquartile range]. |
|
Baseline echocardiographic evaluation demonstrated a mean LV end-diastolic diameter of 45.28 ± 7.83 mm, a mean LV ejection fraction of 58.48 ± 8.63%, and a mean transaortic gradient of 47.24 ± 19.25 mmHg. Severe aortic regurgitation was present in 6 patients (12%) and was the primary valvular heart disease in 2 cases (4%). There were no patients with severe tricuspid regurgitation.
Procedural characteristics and performance of the pre-shaped guidewire
LV pacing avoided venous access in nearly half of the patients (n = 24; 48%). Among those requiring venous access, the femoral vein was the most widely used site (n = 20; 77%), followed by the brachial (n = 4; 15%) and jugular veins (n = 2; 8%). Grounding methods for LV pacing varied, with skin grounding being the one most frequently used (n = 22; 44%), followed by grounding to a guidewire via venous access (n = 19; 38%), and needle-based grounding methods (n = 9; 18%) (table 2).
Table 2. Procedural characteristics and perioperative complications and 30-day follow-up
| Procedural characteristics | Total (n = 50) |
|---|---|
| Venous access | |
| None | 24 (48%) |
| Femoral | 20 (40%) |
| Jugular | 2 (4%) |
| Brachial | 4 (8%) |
| Grounding for LV pacing | |
| Needle | 9 (18%) |
| Guidewire | 19 (38%) |
| Skin | 22 (44%) |
| Predilatation | 71 (82%) |
| Systolic blood pressure < 60 mmHg during rapid LV pacing | 50 (100%) |
| LV pacing threshold (mV) | 7.00 ± 3.48 |
| Conversion to RV pacing | 3 (6%) |
| Conversion to a different LV guidewire | 0 (0%) |
| Type of transcatheter heart valve | |
| Navitor | 28 (56%) |
| Evolut | 5 (10%) |
| ACURATE | 5 (10%) |
| SAPIEN | 6 (12%) |
| Myval | 6 (12%) |
| Transcatheter heart valve size | 25 [23-27] |
| Pacing during TAVI | |
| None | 21 (42%) |
| LV | 27 (54%) |
| RV | 2 (4%) |
| Postdilatation | 10 (20%) |
| Length of stay | 3 (2-5) |
| Total complications | 7 (14%) |
| Stroke | 0 (0%) |
| Vascular | 1 (2%) |
| Bleeding | 0 (0%) |
| Coronary obstruction | 0 (0%) |
| Cardiac tamponade | 0 (0%) |
| Device embolization | 0 (0%) |
| Perioperative AVB | 6 (12%) |
| Permanent pacemaker | 4 (8%) |
| In-hospital mortality | 0 (0%) |
| 30-day readmission | 0 (0%) |
| 30-day mortality | 0 (0%) |
|
AVB, atrioventricular block; LV, left ventricle; RV, right ventricle. |
|
The Navitor valve (Abbott, United States) was the most frequently used transcatheter heart valve (n = 28; 56%), followed by the SAPIEN (Edwards Lifesciences, United States) and the Myval (Meril Life Sciences, India) valves (n = 6; 12%). The least frequently used ones were the Evolut (Medtronic, United States) and the ACURATE (Boston Scientific, United States) (n = 5; 10%). Self-expanding valves accounted for 76% of all implanted transcatheter heart valves. Valve sizes ranged from 23 mm to 34 mm, with a median of 25 mm (IQR, 23-27). Predilatation was performed in most patients (n = 41; 82%), whereas postdilatation was required in only 20% (n = 10) (table 2). The mean LV pacing threshold was 7 ± 3.48 mV, and in 100% of patients (n = 50), a decrease in systolic blood pressure < 60 mmHg was achieved without loss of capture during rapid LV pacing. Comparative data across the different guidewires are presented in table 3. No patient required conversion to an alternative LV pacing guidewire, and only 3 (6%) required RV pacing, all due to AVB following balloon predilatation or during advancement of the valve into the LV. No guidewire exchange was required to advance the TAVI delivery system (table 2).
Table 3. Performance of the preformed left ventricular pacing guidewire
| Study and guidewire | LV pacing threshold (mV) | Procedural success | |||
|---|---|---|---|---|---|
| Mean | SD | Median | IQR | n (%) | |
| Circulo (n = 50) | 7.00 | 3.48 | 7 | 3.8-9.25 | 50 (100) |
| Tamura et al. (2022)10 (n = 204) | 202 (99.02) | ||||
| CONFIDA (n = 34) | 3.36 | 1.66 | 3 | 2-5 | 34 (100) |
| SAFARI (n = 163) | 5.85 | 2.68 | 5 | 4-7 | 161 (98.8) |
| SAFARI Small (n = 110) | 5.97 | 3.01 | 5 | 4-7 | 108 (98.2) |
| SAFARI Extra Small (n = 53) | 5.62 | 1.96 | 6 | 4-7 | 53 (100) |
| Lunderquist (n = 7) | 7.5 | 5.94 | 5 | 3.25-10.5 | 7 (100) |
|
IQR, interquartile range; LV, left ventricle; SD, standard deviation. |
|||||
Complications
The overall rate of complications was 14% (n = 7), with conduction disturbances being the most frequent. Perioperative AVB requiring temporary pacemaker implantation occurred in 6 patients (12%), 4 of whom (8%) exhibited postoperative persistent complete AVB and eventually required permanent pacemaker implantation. One patient experienced a minor vascular complication in the form of vascular occlusion, which was successfully treated by transcatheter procedure and resolved without sequelae. There were no strokes or other major adverse events. The median length of stay from TAVI to discharge was 3 days (IQR, 2-5). The in-hospital survival rate was 100%, and no readmissions or deaths were recorded at the 1-month follow-up. Perioperative complications and those occurring within 1 month after the procedure are shown in table 2.
DISCUSSION
The main findings of the study were these: a) LV pacing using the pre-shaped Circulo guidewire was effective, achieving a reduction in systolic blood pressure < 60 mmHg in 100% of patients; b) no patient required switching to an alternative LV pacing guidewire; c) only 3 patients required conversion to RV pacing, all due to AVB following predilatation; d) the procedural success rate of TAVI was 100%; and e) there were no complications related to the Circulo guidewire. These results demonstrate the safety and efficacy profile of LV pacing using the Circulo guidewire and support its usefulness during transfemoral TAVI.
In this study, the success rate of LV pacing with the Circulo guidewire was comparable to that reported in former studies using other guidewires.8-11,13,14 Only 4% of patients presented right bundle branch block on baseline electrocardiography, indicating a cohort with a low risk of developing conduction disturbances. No patient required switching to an alternative LV pacing guidewire, and only 3 (6%) required conversion to RV pacing due to the onset of AVB after balloon predilatation or during valve advancement into the LV. In 2 of these 3 cases, LV pacing had been effective, with adequate pacing thresholds of 2.5 mV and 3.0 mV; however, although the procedure could have been continued using LV pacing, the operators decided to implant a transvenous temporary pacemaker before valve implantation, anticipating the need for pacing support after the procedure. In the third case, LV pacing was attempted, but due to the absence of adequate capture, conversion to RV pacing with implantation of a transvenous temporary pacemaker was performed. These patients did not present notable clinical differences, and aside from predilatation, no additional predictive factors were identified. The pacing thresholds recorded were slightly higher than those observed in former studies (7 mV vs 3.36 mV-7.5 mV);10 however, these discrepancies were not clinically relevant and are plausibly explained by inter-operator variability inherent to the technique.
Because transvenous temporary pacemaker implantation was only required in patients who developed AVB during or after the procedure, LV pacing with the Circulo guidewire avoided the implantation of 44 temporary pacemakers among 50 cases (88%). In former studies, this approach has been shown to reduce both procedural and fluoroscopy times.9,15,16 Therefore, although LV pacing can be performed in all patients, it is most beneficial in those at low risk of AVB and subsequent pacing requirements. In such cases, transvenous temporary pacemaker implantation can be avoided, a procedure associated with potential complications, such as inadvertent arterial puncture (0.3%), major hemorrhage (2.7%), deep vein thrombosis (0.3%), pulmonary thromboembolism (0.1%), pneumothorax (0.1%), cardiac perforation (0.7%), lead dislodgement (3.4%), pacing failure (7.7%), and the need for multiple placement attempts (0.9%).7
Although it is evident that LV pacing reduces most complications associated with transvenous RV temporary pacemaker implantation, the main concerns regarding LV pacing have focused on the risk of aortic bioprosthesis embolization due to loss of capture and the risk of perforation related to advancing the guidewire inside the LV during pacing. However, multiple studies have shown no significant differences in valve embolization rates between the 2 techniques, with some reporting a trend toward a lower risk of cardiac tamponade with LV pacing, likely attributable to the greater myocardial thickness of the LV vs the RV.9,14,15 In our study, there were no cases of device embolization or cardiac tamponade or LV pacing-related complications.
Study limitations
One limitation of the present study is that guidewire selection was left to the operator’s discretion, which may have introduced selection bias. In the cohort presented, only 4% of patients exhibited right bundle branch block on baseline electrocardiography, which is representative of a population at a low risk of developing arrhythmic complications. However, the operator-dependent choice of guidewire enhances the external validity of the results, as it more accurately reflects real-world clinical decision-making. Another limitation is the absence of a comparison group undergoing RV or LV pacing with other guidewires, which limits the ability to directly compare outcomes between techniques. Instead, results were compared with those of previously published studies.
CONCLUSIONS
The use of the Circulo guidewire for LV pacing during TAVI proved to be safe and effective, with a low overall rate of TAVI-related complications and no guidewire-related complications. This approach avoids the need for transvenous temporary pacemaker implantation in most patients at low risk of arrhythmic complications, thus potentially reducing procedural risks and simplifying perioperative management.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
The study protocol was approved by Hospital Clínic de Barcelona Clinical Research Ethics Committee in full compliance with the ethical principles outlined in the Declaration of Helsinki. All participants signed informed consent prior to inclusion in the study. No sex-based subgroup analysis was performed, as this could compromise the statistical power of the study and both sexes were adequately represented in the cohort; furthermore, there is no prior evidence suggesting sex-related differences in response to LV pacing using a pre-shaped guidewire.
DECLARATION ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence was used in the development of this article.
AUTHORS’ CONTRIBUTIONS
A. Regueiro designed the protocol, database, and study framework, and coordinated statistical analysis, data interpretation, and manuscript drafting. I. Anduaga contributed to protocol design, database development, and study framework, performed statistical analysis and data interpretation, and drafted the manuscript. A. Ruberti, V. Vilalta, I.J. Amat-Santos, F. Díez-Delhoyo, L.L. Gheorghe, J.A. Baz, J.F. Díaz Fernández, L. Gutiérrez-Alonso, and X. Carrillo participated in data collection and critically reviewed the manuscript. All authors approved the final published version.
CONFLICTS OF INTEREST
A. Regueiro is a consultant for Abbott, Edwards, Haemonetics, Medtronic, and Meril. J.F. Díaz Fernández is a consultant for Abbott, Boston Scientific, and Medtronic. I.J. Amat-Santos is a proctor for Boston Scientific, Medtronic, Meril, and MicroPort. The remaining authors declared no conflicts of interest whatsoever.
WHAT IS KNOWN ABOUT THE TOPIC?
- LV pacing using pre-shaped guidewires has emerged as an effective alternative to RV pacing with transvenous temporary pacemaker implantation.
- LV pacing has been associated with shorter procedural and fluoroscopy times.
- Although LV pacing has proven safe and effective with several guidewires, not all guidewires currently used in TAVI have proven useful for this purpose.
WHAT DOES THIS STUDY ADD?
- The pre-shaped Circulo guidewire, with its circular design, proved to be a highly effective option for LV pacing during transfemoral TAVI.
- The overall TAVI complication rate was low, and no complications attributable to the Circulo guidewire were observed.
- The Circulo guidewire avoids the need for transvenous temporary pacemaker implantation in a considerable proportion of patients and is particularly useful in those at low risk of perioperative conduction disturbances.
REFERENCES
1. Toff WD, Hildick-Smith D, Kovac J, et al. Effect of Transcatheter Aortic Valve Implantation vs Surgical Aortic Valve Replacement on All-Cause Mortality in Patients With Aortic Stenosis:A Randomized Clinical Trial. JAMA. 2022;327:1875-1887.
2. Praz F, Borger MA, Lanz J, et al. 2025 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2025;46:4635-4736.
3. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease:A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227.
4. Ando T, Onishi T, Kuno T, et al. Transcatheter Versus Surgical Aortic Valve Replacement in the United States (From the Nationwide Readmission Database). Am J Cardiol. 2021;148:110-115.
5. Généreux P, Piazza N, Alu MC, et al. Valve Academic Research Consortium 3:Updated Endpoint Definitions for Aortic Valve Clinical Research. J Am Coll Cardiol. 2021;77:2717-2746.
6. Ludman PF. UK TAVI registry. Heart. 2019;105(Suppl 2):s2-s5.
7. Tjong FVY, de Ruijter UW, Beurskens NEG, Knops RE. A comprehensive scoping review on transvenous temporary pacing therapy. Neth Heart J. 2019;27:462-473.
8. Faurie B, Abdellaoui M, Wautot F, et al. Rapid pacing using the left ventricular guidewire:Reviving an old technique to simplify BAV and TAVI procedures. Catheter Cardiovasc Interv. 2016;88:988-993.
9. Faurie B, Souteyrand G, Staat P, et al. Left Ventricular Rapid Pacing Via the Valve Delivery Guidewire in Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2019;12:2449-2459.
10. Tamura Y, Tamura Y, Konami Y, et al. Comparison of left ventricular pacing performance among pre-shaped guidewires designed for transfemoral-approach transcatheter aortic valve implantation. Heart Vessels. 2022;37:460-466.
11. Regueiro A, Alperi A, Vilalta V, et al. Safety and Efficacy of TAVR With a Pressure Sensor and Pacing Guidewire:SAFE-TAVI Trial. JACC Cardiovasc Interv. 2023;16:3016-3023.
12. Blusztein D, Raney A, Walsh J, Nazif T, Woods C, Daniels D. Best Practices in Left Ventricular Pacing for Transcatheter Aortic Valve Replacement. Struct Heart. 2023;7:100213.
13. Hilling-Smith R, Cockburn J, Dooley M, et al. Rapid pacing using the 0.035-in. Retrograde left ventricular support wire in 208 cases of transcatheter aortic valve implantation and balloon aortic valvuloplasty. Catheter Cardiovasc Interv. 2017;89:783-786.
14. Sta˛pór M, Tre˛bacz J, Wiewiórka Ł, et al. Direct left ventricular wire pacing during transcatheter aortic valve implantation. Kardiol Pol. 2020;78:882-888.
15. Hokken TW, de Ronde M, Wolff Q, et al. Insights in a restricted temporary pacemaker strategy in a lean transcatheter aortic valve implantation program. Catheter Cardiovasc Interv. 2022;99:1197-1205.
16. Savvoulidis P, Mechery A, Lawton E, et al. Comparison of left ventricular with right ventricular rapid pacing on tamponade during TAVI. Int J Cardiol. 2022;360:46-52.
ABSTRACT
Introduction and objectives: To compare clinical outcomes of immediate vs staged multivessel percutaneous coronary intervention (PCI) for non-culprit lesions in hemodynamically stable patients with ST-segment elevation myocardial infarction and multivessel coronary artery disease.
Methods: We conducted this systematic review and meta-analysis according to PRISMA guidelines. PubMed, Embase, and Cochrane databases were searched throughout September 2025. Outcomes included cardiac death, all-cause mortality, reinfarction, acute kidney injury, and stroke. Risk ratios were calculated, and trial sequential analysis, incidence rate ratio (IRR) analyses, and meta-regression were conducted.
Results: Six randomized controlled trials including 4267 patients were analyzed. At the 1-year follow-up, there were no significant differences between immediate and staged PCI regarding cardiac death (RR, 1.26; 95%CI, 0.89-1.79), all-cause mortality (RR, 1.18; 95%CI, 0.93-1.50), acute kidney injury (RR, 0.91; 95%CI, 0.64-1.31), or stroke (RR, 1.17; 95%CI, 0.66-2.05). Immediate PCI was associated with a lower risk of reinfarction (RR, 0.63; 95%CI, 0.40-0.98), a finding confirmed by IRR analysis (IRR, 0.60; 95%CI, 0.39-0.94; I2 = 0%). Exploratory meta-regression analyses did not identify procedural timing or baseline comorbidities as significant effect modifiers.
Conclusions: In patients with ST-segment elevation myocardial infarction and multivessel disease, immediate PCI was associated with a lower risk of reinfarction, without any significant differences being reported in cardiac death or all-cause mortality compared with staged PCI. Although trial sequential analysis indicates that current evidence remains underpowered for certain outcomes, the consistency of findings across multiple analytical approaches supports the safety profile of immediate complete revascularization, pending confirmation in adequately powered randomized trials. (PROSPERO: CRD42023485163.I).
Keywords: Coronary artery disease. ST-segment elevation myocardial infarction. Multivessel disease. Immediate percutaneous coronary intervention. Staged percutaneous coronary intervention.
RESUMEN
Introducción y objetivos: Esta revisión sistemática con metanálisis evalúa si una estrategia de intervención coronaria percutánea (ICP) multivaso por etapas o inmediata proporciona resultados clínicos superiores en pacientes hemodinámicamente estables con infarto agudo de miocardio con elevación del segmento ST y enfermedad coronaria multivaso sometidos a revascularización de lesiones no culpables.
Métodos: Se realizaron búsquedas en PubMed, Embase y Cochrane hasta septiembre de 2025 según las directrices PRISMA. Los resultados incluyeron muerte por causa cardiaca, muerte por cualquier causa, reinfarto, lesión renal aguda y accidente vascular cerebral. Se estimaron los riesgos relativos y se realizó un análisis secuencial de ensayos en desenlaces seleccionados. Además, se calcularon las tasas de incidencia relativa (IRR) y se realizó una metarregresión.
Resultados: Se incluyeron 6 ensayos clínicos aleatorizados con 4.267 pacientes. En el seguimiento al año no se encontraron diferencias significativas entre la ICP por etapas y la inmediata en el riesgo de muerte por causa cardiaca (RR = 1,26; IC95%, 0,89-1,79), muerte por cualquier causa (RR = 1,18; IC95%, 0,93-1,50), lesión renal aguda (RR = 0,91; IC95%, 0,64-1,31) o accidente vascular cerebral (RR = 1,17; IC95%, 0,66-2,05). La ICP inmediata se asoció con un menor riesgo de reinfarto (RR = 0,63; IC95%, 0,40-0,98), confirmado por el análisis de tasa de incidencia relativa (IRR = 0,60; IC95%, 0,39-0,94; I² = 0%). La metarregresión no mostró asociación significativa entre el riesgo de reinfarto y el momento de la ICP por etapas o la comorbilidad basal.
Conclusiones: La ICP inmediata en pacientes con infarto agudo de miocardio con elevación del segmento ST y enfermedad multivaso se asoció con un menor riesgo de reinfarto, sin diferencias significativas en la mortalidad por causa cardiaca ni en la mortalidad por cualquier causa frente a la ICP por etapas. Aunque el análisis secuencial de ensayos indicó que la evidencia actual aún carece de suficiente poder estadístico, la consistencia en la dirección del efecto a través de múltiples enfoques analíticos respalda la seguridad y la posible ventaja clínica de la revascularización completa inmediata, lo que justifica su confirmación en futuros ensayos aleatorizados adecuadamente dimensionados. (PROSPERO: CRD42023485163.I).
Palabras clave: Enfermedad coronaria. Infarto agudo de miocardio con elevación del segmento ST. Enfermedad multivaso. Intervención coronaria percutánea inmediata. Intervención coronaria percutánea por etapas.
Abbreviations
AKI: acute kidney injury; PCI: percutaneous coronary intervention. STEMI: ST-segment elevation myocardial infarction.
INTRODUCTION
Multivessel coronary artery disease is defined as the presence of ≥ 70% luminal stenosis in at least 2 major epicardial coronary arteries due to atherosclerotic plaque. Approximately 40% of patients with ST-segment elevation myocardial infarction (STEMI) exhibit multivessel coronary disease, which is associated with an increased risk of recurrent myocardial infarction and mortality.1-3 Evidence from randomized controlled trials has underscored the advantages of comprehensive revascularization with multivessel percutaneous coronary intervention (PCI) over culprit-lesion-only PCI, notably reducing the risks of cardiac death, myocardial infarction, and ischemia-driven revascularization at 1 year.4-6 There are 2 strategies to approach non-culprit lesions: immediate PCI which involves the revascularization of both culprit and non-culprit lesions during the index procedure, and staged PCI, where the treatment of non-culprit lesions is deferred to a later stage.
The 2021 clinical practice guidelines outlined by the American College of Cardiology/American Heart Association (ACC/AHA) acknowledge non-culprit vessel revascularization as a class IIb recommendation for patients with STEMI.7 However, determining the optimal timing for revascularization of non-culprit lesions remains a clinical challenge7,8 While PCI for non-culprit lesions has demonstrated superiority over a strategy of treating the culprit lesion alone,4-6 the timing of intervention, whether immediate or staged, lacks conclusive evidence.8,9
The objective of this meta-analysis was to compare staged vs immediate PCI for non-culprit lesions in hemodynamically stable patients with STEMI and multivessel disease. We hypothesize that both the staged and immediate PCI targeting non-culprit vessels will demonstrate comparable levels of safety, efficacy, and rate of complications.
METHODS
We conducted the present study following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.10 All steps were conducted in full compliance with the Cochrane Handbook of Systematic Reviews and Meta-analysis of Interventions (version 6.3).11 This meta-analysis protocol was registered on PROSPERO on 4 December, 2023, under protocol ID: CRD42023485163.l. During the peer-review process, the literature search was updated using the same search strategy, databases, and eligibility criteria described in supplementary data S1 to identify newly published randomized evidence.
Criteria of the included studies
We evaluated randomized controlled trials comparing immediate vs staged PCI for non-culprit lesions in adults with STEMI and multivessel coronary artery disease. Eligible studies were required to report extractable numerical data for at least 1 prespecified outcome of interest, as defined below. Trials reporting outcomes exclusively as Kaplan-Meier curves without corresponding event counts or effect estimates or reporting outcomes only as composite endpoints without separate data, were excluded from quantitative synthesis. No publication time limit was applied; however, the search was restricted to studies published in Spanish, English, or German. Case-control and cross-sectional studies, systematic reviews, meta-analyses, case reports, basic science research, conference abstracts, and letters to the editor were excluded.
Literature search strategy
We conducted a comprehensive and systematic search across 3 databases (PubMed, EMBASE, and COCHRANE) from their inception until 28 September, 2025. Keywords used for the search included “coronary artery disease”, “immediate multivessel percutaneous coronary intervention”, “staged multivessel percutaneous coronary intervention”, “acute coronary syndrome”, “multivessel disease”, “myocardial infarction”, “major adverse cardiovascular events”, “ST-segment elevation myocardial infarction”. These keywords were combined using Boolean operators AND and OR. The search details for each database are available in the supplementary data S1.
Screening of literature search results
All duplicates were removed using Zotero reference manager software. Records were initially screened by title and abstract by one author (E. Andrade-Arbaiza), followed by full-text assessment when potentially eligible. Two independent authors (D. Paulino-González, and L.H. García-Mena) reviewed full-text articles for inclusion and methodological quality, with disagreements being resolved by consensus or third-party adjudication (D. A. Navarro-Martínez). Studies were excluded at the full-text stage if they lacked extractable numerical data for prespecified outcomes or did not report outcomes separately, precluding quantitative synthesis. A detailed list of excluded studies with reasons for exclusion is provided in table S1. References cited in included studies were also manually screened for eligibility.
Data extraction
Data extraction was performed using standardized Excel spreadsheets to collect baseline population characteristics, key study features, outcome measures expressed as risk ratios, and domains for quality assessment. Outcome data were included only when numerical information was directly available or could be reliably derived without reconstruction from survival curves.
Assessing the risk of bias
The risk of bias of included randomized controlled trials was assessed usingvVersion 2 of the Cochrane risk-of-bias tool for randomized trials (ROB 2), in accordance with the Cochrane Handbook of Systematic Reviews of Interventions.11
Endpoints
The prespecified endpoints of this meta-analysis were cardiac death, all-cause mortality, stroke, reinfarction, and acute kidney injury (AKI). Given minor variations in endpoint definitions across trials, detailed outcome definitions as reported by each study are summarized in table S2. Outcomes were analyzed as dichotomous variables using event counts and percentages, and risk ratios with 95% confidence intervals (95%CI) were calculated.
Data analysis
Dichotomous outcomes were analyzed using pooled event data from the included studies and are reported as risk ratios with 95%CI. P values < .05 were considered statistically significant. Associations between outcomes and immediate vs staged PCI were evaluated using a random-effects model (DerSimonian–Laird method) to account for between-study heterogeneity.12 Statistical analyses and forest plots were generated using RevMan version 5.4.1 (Cochrane Collaboration) for MacOs.
Statistical analysis
Pooled risk ratios (RR) and incidence rate ratios (IRR) were estimated using random-effects models with appropriate adjustments, and heterogeneity was assessed using the I2 statistic. Sensitivity analyses, trial sequential analysis, and meta-regression were performed to evaluate the robustness of findings and explore potential effect modifiers. Detailed methodological procedures are shown in the supplementary data S2.
Assessment of heterogeneity
Heterogeneity was assessed using Cochran’s Q test (P < .10) and quantified with the I2 statistic, with values > 50% indicating substantial heterogeneity.
RESULTS
A total of 6 studies13-18 met the predefined inclusion criteria and were included in the analysis. The study selection process is summarized in the PRISMA flow diagram shown in figure 1. All included studies evaluated staged or immediate PCI in non-culprit arteries of patients with STEMI and multivessel disease.
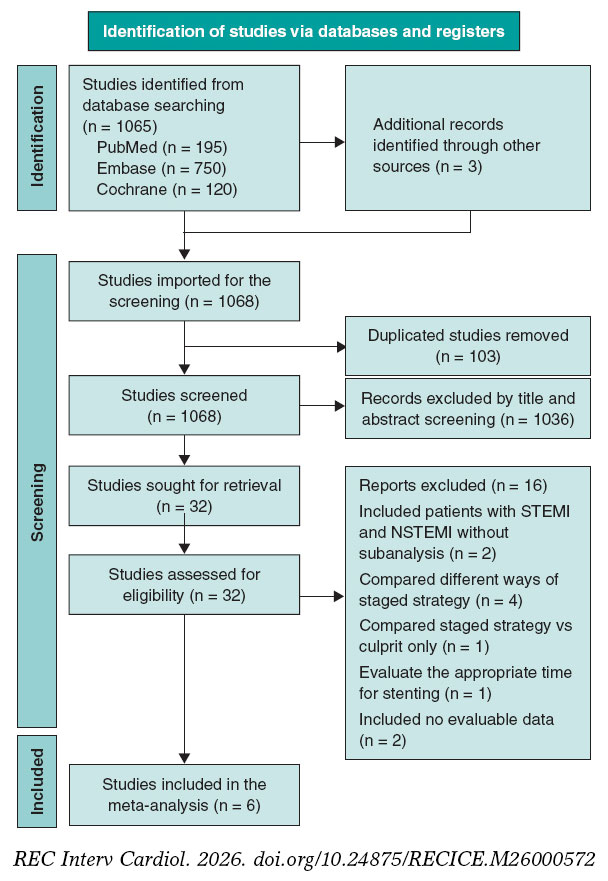
Figure 1. PRISMA flow diagram. The diagram reflects the initial search and the updated search performed during peer review using the same strategy and eligibility criteria (supplementary data S1). NSTEMI, non-ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction.
In the staged strategy, PCI of nonculprit lesions was performed a mean of 18.6 days (IQR, 7-34) after the index procedure. The total patient population included in our meta-analysis was 4267 patients, of whom 2479 underwent immediate PCI and 1788, staged PCI. Summary and baseline characteristics are shown in table 1. The characteristics of the included studies are summarized in table 2.
Table 1. Baseline characteristics and treatment of the included studies’ populations
| Study information | Baseline characteristics | Treatments and following intervention | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study ID | Country | Total population size | Intervention | Population size | Median [IQR] Age | Gender | Comorbidities | Culprit artery | Non-culprit artery | Access site index | Access site index + staged | Stent used index | Stent used index + staged | Volume of contrast index | Volume of contrast index + staged | Length of stay index | Length of stay index + staged | ||
| Kim et al.182025 | Multicenter | 994 | Immediate | 498 | 66 IQR [57-76] | F: 102 M: 396 |
Yes | Left main coronary artery | NR | Left main coronary artery | NR | Radial:371 Femoral: NR | Radial: 379 Femoral: NR | 2 | NR | 180 (140-225) | NR | 4 (3-6) | NR |
| NR | NR | ||||||||||||||||||
| Left anterior descending coronary artery | 221 | Left anterior descending coronary artery | 222 | ||||||||||||||||
| 234 | 212 | ||||||||||||||||||
| Staged | 496 | 65 IQR [58-76] | F: 103 M: 393 |
Left circumflex artery | 62 | Left circumflex artery | 218 | 1 | 2 | 130 (100-180) | 220 (170-298) | NR | 5 (4-8) | ||||||
| 67 | 215 | ||||||||||||||||||
| Right coronary artery | 215 | Right coronary artery | 162 | ||||||||||||||||
| 195 | 167 | ||||||||||||||||||
| Stähli et al.132023 | Multicentric | 840 | Immediate | 418 | 66 IQR [58-74] | F: 97 M:321 | Yes | Left main coronary artery | 0 | Left main coronary artery | 1 | Radial: 301 Femoral 117 | Radial: -- Femoral 296 | 3 (2-4) | NR | 250 (199-320) | NR | 4 (3-6) | NR |
| 1 | 4 | ||||||||||||||||||
| Left anterior descending coronary artery | 163 | Left anterior descending coronary artery | 205 | ||||||||||||||||
| 176 | 180 | ||||||||||||||||||
| Staged | 422 | 64 IQR [55-73] | F:81 M:341 | Left circumflex artery | 67 | Left circumflex artery | 196 | Radial: 311 Femoral 111 | Radial: -- Femoral 90 | 1 (1-2) | 3 (2-4) | 170 (130-220) | 333 (258-411) | 4 (3-6) | 5 (4-7) | ||||
| 77 | 152 | ||||||||||||||||||
| Right coronary artery | 188 | Right coronary artery | 134 | ||||||||||||||||
| 169 | 124 | ||||||||||||||||||
| Politi et al.142010 | Italy | 130 |
Immediate | 65 | 64.5 ± 11.7 | F: 15 M: 50 |
Yes | Left main coronary artery | NR | Left main coronary artery | NR | NR | NR | NR | NR | NR | NR | 4.8 ±2.6 | NR |
| NR | NR | ||||||||||||||||||
| Left anterior descending coronary artery | NR | Left anterior descending coronary artery | NR | ||||||||||||||||
| NR | NR | ||||||||||||||||||
| Staged | 65 | 64.5 ± 11.1 | F:13 M: 52 |
Left circumflex artery | NR | Left circumflex artery | NR | NR | NR | NR | NR | NR | NR | 5.4±3.1 | NR | ||||
| NR | NR | ||||||||||||||||||
| Right coronary artery | NR | Right coronary artery | NR | ||||||||||||||||
| NR | NR | ||||||||||||||||||
| Park et al.152023 | Multicentric | 209*Analysis of a subgroup | Immediate | 103 | 63.3 ± 10.4 | F:21 M:82 | Yes | Left main coronary artery | 1 | Left main coronary artery | 4 | Radial: 27 | -- | 2.58 ± 0.86 | -- | NR | -- | NR | NR |
| 1 | 3 | ||||||||||||||||||
| Left anterior descending coronary artery | 45 | Left anterior descending coronary artery | 79 | ||||||||||||||||
| 48 | 82 | ||||||||||||||||||
| Staged | 106 | 62.2 ± 10.9 | F 18 M: 88 |
Left circumflex artery | 12 | Left circumflex artery | 60 | Radial:25 | NR | 2.62 ± 1.00 | NR | NR | NR | NR | NR | ||||
| 17 | 55 | ||||||||||||||||||
| Right coronary artery | 46 | Right coronary artery | 78 | ||||||||||||||||
| 42 | 80 | ||||||||||||||||||
| 228 | 65 | ||||||||||||||||||
| Maamoun et al.162011 | Yemen | 78 | Immediate | 36 | 52.33 ± 7.1 | M: 32 F: 4 |
Yes | NR | NR | NR | NR | Femoral | Femoral | 2.38 ± 0.49 | 2.31 ± 0.47 | NR | NR | NR | NR |
| Staged | 42 | 54.52 ± 10.3 | M: 40 F: 2 |
||||||||||||||||
| Wood et al.172019 | Canada | 4041* | Immediate | 1353 | 61.8 ± 10.5 | M: 1079 F: 274 |
Yes | NR | NR | Left main coronary artery | 4 | Radial | Radial | NR | NR | NR | NR | NR | NR |
| 6 | |||||||||||||||||||
| Left anterior descending coronary artery | 683 | ||||||||||||||||||
| 384 | |||||||||||||||||||
| Staged | 663 | 61.2 ± 11.0 | M: 544 F: 119 |
Left circumflex artery | 654 | ||||||||||||||
| 294 | |||||||||||||||||||
| Right coronary artery | 463 | ||||||||||||||||||
| 207 | |||||||||||||||||||
|
F, female; IQR, interquartile range; M, male; NR, not reported. |
|||||||||||||||||||
Table 2. Summary of included studies.
| Author & year | Journal | Country | Study design | Population size (included) | Compared interventions | Timeframe by staged PCI | Mean follow-up | Key findings |
|---|---|---|---|---|---|---|---|---|
| Kim et al.182025 | South Korea | Ramdomized controlled trial | 994 | Immediate vs staged revascularization | 3 days | 1 year |
| |
| Stähli et al.132023 | Europe | Randomized controlled trial | 840 | Immediate vs staged revascularization | 19-45 days | 30 days (± 7 days), 6 months (± 14 days), 1 year (± 14 days) |
| |
| Park et al.152023 | South Korea | Randomized controlled trial | 209 | Immediate vs staged revascularization | 14 days | 7 days 1 month 1 year |
|
|
| Wood et al.172019 | Canada | Randomized controlled trial | 4041 (2016) | Immediate vs staged revascularization | 23 (12.5-33.5) days | 3 years |
|
|
| Maamoun et al.162011 | Yemen | Randomized controlled trial | 78 | Immediate vs staged revascularization | 7 days | 1 year |
|
|
| Politi et al.142010 | Italy | Randomized controlled trial | 263 (130) | Immediate vs staged revascularization | 56.8 ± 12.9 days | 2.5 ± 1.4 years |
|
|
|
95%CI, 95% confidence interval; CR, complete revascularization; HR, hazard ratio; IRA, infarct-related artery; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction; MACE, major adverse cardiovascular events; MI, myocardial infarction; RR, risk ratio; SR, staged revascularization. |
||||||||
Cardiac death
There were no significant difference between staged and immediate PCI regarding the risk of cardiac death (RR, 1.26; 95%CI, 0.89-1.79; P = .19). No heterogeneity was observed among the included studies (I2 = 0%). These findings are shown in figure 2A.
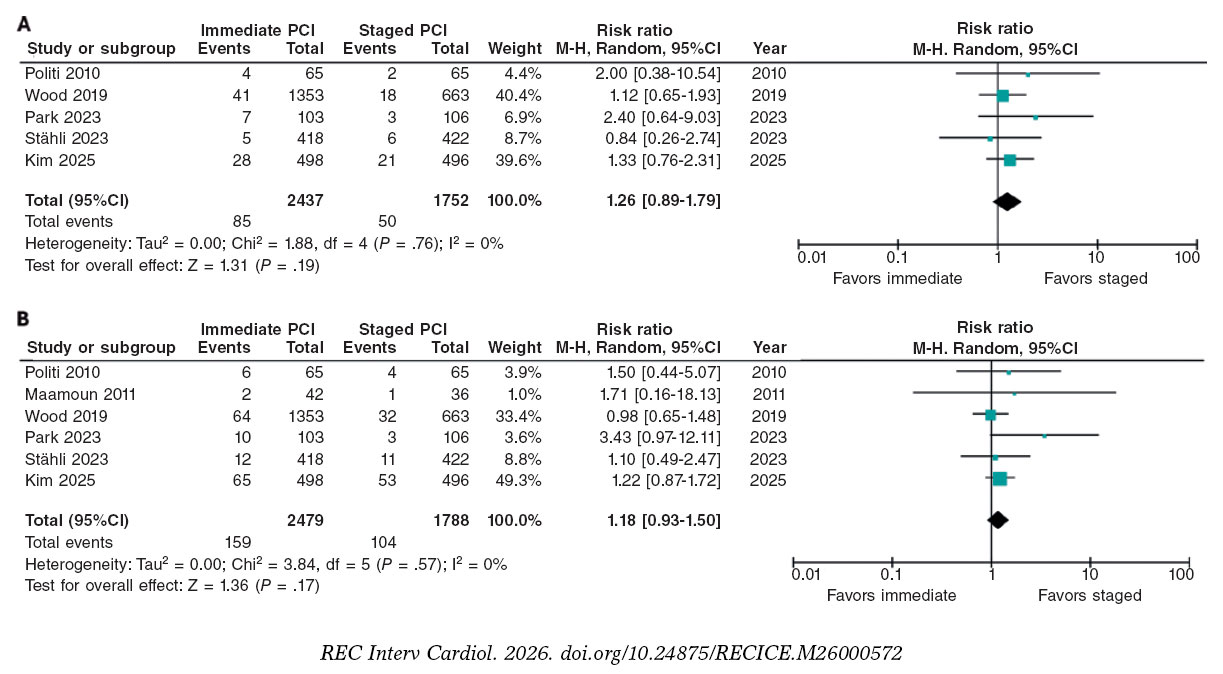
Figure 2. Risk Ratios of cardiac death and all-cause mortality. A: cardiac death: risk ratio (RR) across the included trials are represented by solid squares, with horizontal lines indicating 95% confidence intervals (95%CI). B: all-cause mortality: RR across trials are shown by solid squares, with 95%CI indicated by horizontal lines. The bibliographical references cited in this figure correspond to the following studies: Politi et al.14 (2010), Maamoun et al.16 (2011), Wood et al.17 (2019), Park et al.15 (2023), Stähli et al.13 (2023), and Kim et al.18 (2025).
All-cause mortality
There were no significant differences in the risk of all-cause mortality between patients undergoing staged PCI and those treated with immediate PCI (RR, 1.18; 95%CI, 0.93-1.50; P = .17), with no heterogeneity detected among studies (I2 = 0%) (figure 2B).
Reinfarction
The analysis demonstrated a statistically significant lower risk of reinfarction with immediate vs staged PCI (RR, 0.63; 95%CI, 0.40-0.98; P = .04), which amounts to an approximately 37% relative risk reduction with the former. There was no heterogeneity across trials (I2 = 0%). These findings are shown in figure 3A.
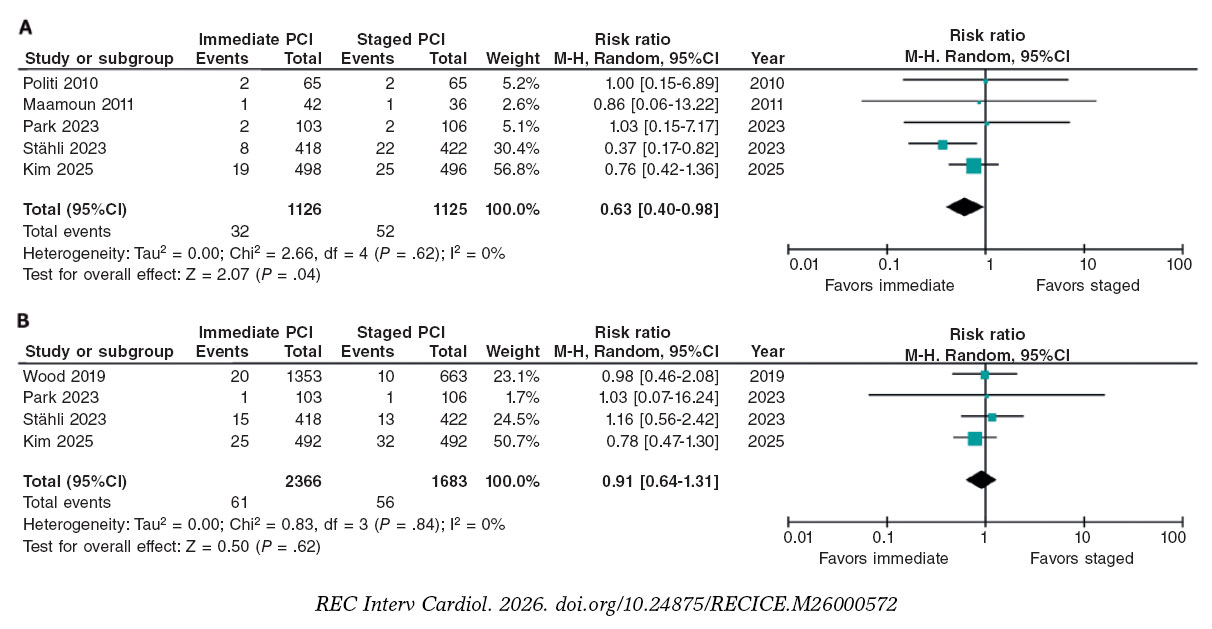
Figure 3. Risk ratios for reinfarction and acute kidney injury. A: reinfarction: risk ratio (RR) across the included trials are represented by solid squares, with horizontal lines indicating 95% confidence intervals (95%CI). B: acute kidney injury: RR across trials are shown by solid squares, with 95%CI indicated by horizontal lines. The bibliographical references cited in this figure correspond to the following studies: Politi et al.14 (2010), Maamoun et al.16 (2011), Wood et al.17 (2019), Park et al.15 (2023), Stähli et al.13 (2023), and Kim et al.18 (2025).
Acute kidney injury
There were no significant differences between the 2 strategies (RR, 0.91; 95%CI, 0.64-1.31; P = .62), indicating no clear association between the revascularization strategy and the risk of AKI. There was no heterogeneity among the included studies (I2 = 0%). These results are shown in figure 3B.
Stroke
Stroke was reported in only 3 of the studies included, and our analysis showed no significant differences between staged and immediate PCI for this outcome (RR, 1.17; 95%CI, 0.66-2.05; P = .59). There was no heterogeneity among the included studies (I2 = 0%). These results are shown in figure S1.
Publication bias was assessed using funnel plots, Egger’s regression, and trim-and-fill analyses for reinfarction, cardiac death, and all-cause mortality. There was no visual evidence of funnel-plot asymmetry (figure S2). For reinfarction, trim-and-fill imputed 1 potentially missing study, with the pooled effect remained statistically significant (IRR, 0.59; 95%CI, 0.38-0.90). For cardiac death and all-cause mortality, 2 studies were imputed in each analysis; however, pooled effects remained non-significant, with no heterogeneity detected (I2 = 0%). Overall, these results suggest no substantial publication bias, although the limited number of included trials reduces the power of formal tests for funnel plot asymmetry.
Sensitivity analyses
Leave-one-out sensitivity analyses confirmed the robustness of the pooled estimates across all primary endpoints (figure S3). For all-cause mortality and cardiac death, exclusion of individual studies did not materially alter the results, with pooled RRs remaining within the confidence intervals of the main models and I2 = 0% in all scenarios. For reinfarction, estimates consistently favored immediate PCI (RR range, 0.46-0.75), with I2 = 0% supporting the internal consistency of the findings.
Incidence rate ratios
At the 1-year follow-up, IRR analysis showed that immediate PCI was associated with a lower rate of reinfarction vs staged PCI. Under the random-effects model, the pooled IRR was 0.60 (95%CI, 0.39-0.94; I2 = 0%), which is consistent with the common-effect model (IRR, 0.59; 95%CI, 0.38-0.92), supporting the robustness of this finding (figure S4). In contrast, there were no significant differences between the strategies regarding cardiac death (IRR, 1.26; 95%CI, 0.90-1.77; I2 = 0%) or all-cause mortality (IRR, 1.17; 95%CI, 0.84-1.64; I2 = 0%), indicating stable estimates with negligible heterogeneity across studies (figures S5, S6).
Trial sequential analyses
Trial sequential analysis were conducted for cardiac death, all-cause mortality, and reinfarction (figure 4A-C). For cardiac death and all-cause mortality, the accrued sample represented 33% and 58% of the required information size, respectively; in both analysis, the cumulative Z-curves remained within nonsignificant boundaries, indicating insufficient evidence to confirm or exclude a 30% relative risk reduction. For reinfarction, only 3.4% of the required information size was reached, and the Z-curve remained well within the futility zone, showing a non-significant trend favoring immediate PCI. Collectively, these results demonstrate that current data remain underpowered to establish definitive conclusions across outcomes, despite a consistent numerical pattern supporting immediate revascularization.
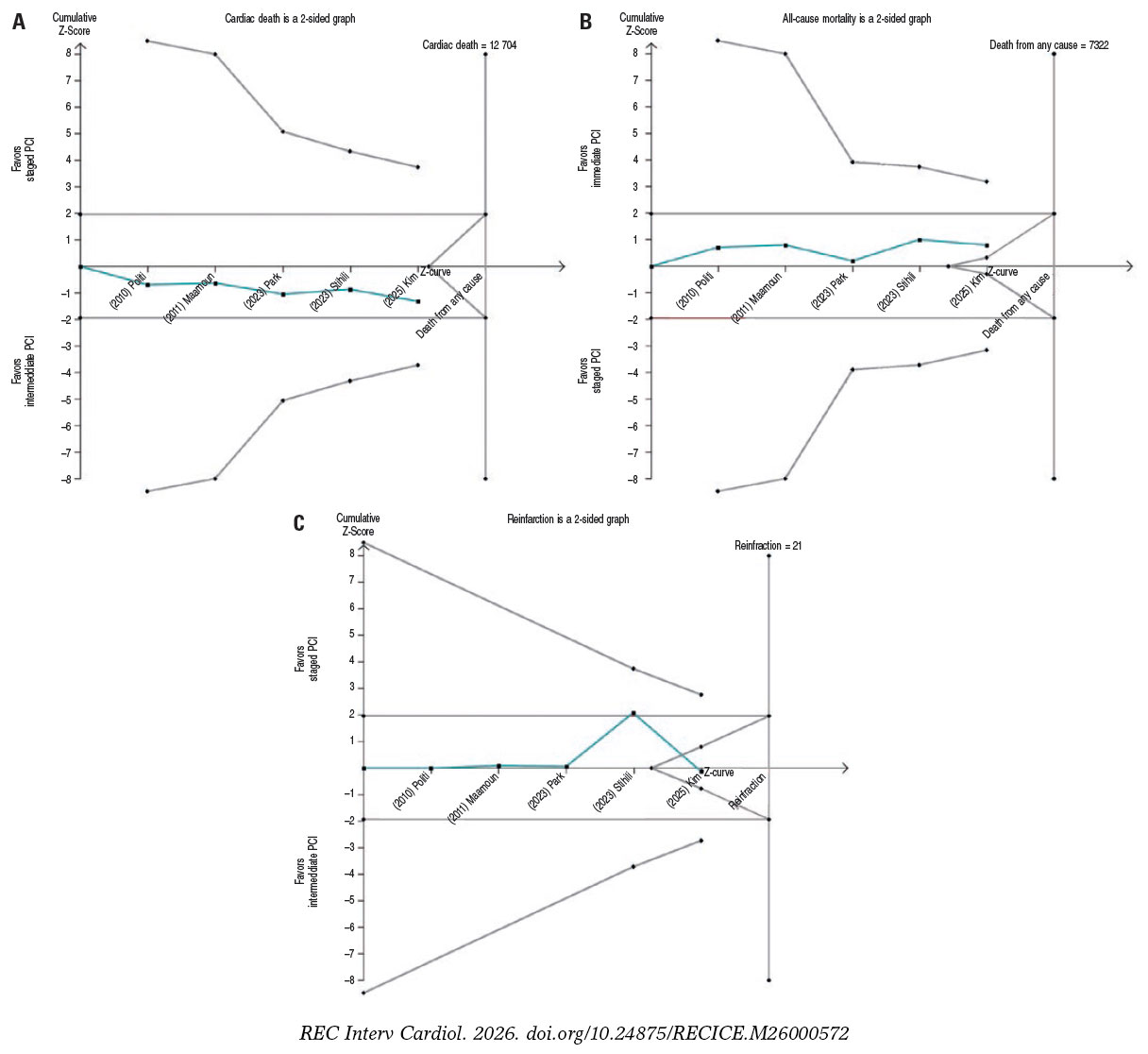
Figure 4. Trial sequential analysis. Trial sequential analysis for (A) cardiac death, (B) all-cause mortality, and (C) reinfarction. In all panels, the cumulative Z-curve is shown in blue, trial sequential monitoring boundaries in red, and conventional significance thresholds as horizontal magenta lines. PCI, percutaneous coronary intervention. The bibliographical references cited in this figure correspond to the following studies: Politi et al.14 (2010), Maamoun et al.16 (2011), Wood et al.17 (2019), Park et al.15 (2023), Stähli et al.13 (2023), and Kim et al.18 (2025).
Meta-regression
Exploratory meta-regression analyses were conducted to assess whether procedural timing or baseline comorbidities influenced reinfarction outcomes. The association between time to staged PCI and reinfarction risk showed a negative but non-significant slope (β = –0.016 per day; 95%CI, –0.042-0.010; P = .22), with no residual heterogeneity (I2 = 0%), indicating consistent effects across studies (figure S7). Similarly, diabetes prevalence (β = 0.021 per 1% increase; 95%CI, –0.017 to 0.058; P = .22) and hypertension prevalence (β = –0.064 per 1% increase; 95%CI, –0.214 to 0.085; P = .40) were not significantly associated with reinfarction risk, with no evidence of residual heterogeneity (I2 = 0% for both) (figures S8-S9). Collectively, these findings suggest that neither procedural timing nor comorbidity burden materially modified the comparative risk of reinfarction between immediate and staged PCI; however, given the study-level and exploratory design of these analyses, results should be interpreted with caution.
Risk of bias assessment
Risk of bias assessment was assessed using version 2 of the Cochrane risk-of-bias tool for randomized trials (ROB 2), as outlined in the Cochrane Handbook of Systematic Reviews of Interventions.11 Four clinical trials were judged to have a low overall risk of bias, whereas the study by Maamoun et al.16 was rated as the only clinical trial having some concerns (table 3).
Table 3. Risk of bias summary for randomized studies (RoB 2)
| Study | Bias arising from randomization process | Bias due to deviations from intended interventions | Bias due to missing outcome data | Bias in measurement of the outcomes | Bias in selection of the reported results | Overall risk of bias |
|---|---|---|---|---|---|---|
| Politi et al.142010 | Low | Low | Low | Low | Low | Low |
| Maamoun et al.162011 | Low | Some concerns | Low | Some concerns | Low | Some concerns |
| Wood et al.172019 | Low | Low | Low | Low | Low | Low |
| Park et al.152023 | Low | Low | Low | Low | Low | Low |
| Stähli et al.132023 | Low | Low | Low | Low | Low | Low |
| Kim et al.182025 | Low | Low | Low | Low | Low | Low |
DISCUSSION
The present meta-analysis provides a focused comparison of immediate vs staged PCI in patients with STEMI and multivessel disease. By integrating randomized evidence using complementary analytical approaches, our findings offer an updated and clinically relevant synthesis of the safety and efficacy profile of these 2 revascularization strategies in a well-defined population.
Although cardiac death and all-cause mortality are clinically relevant, they are relatively rare outcomes in contemporary STEMI populations undergoing multivessel revascularization. In the present analysis, there were no statistically significant differences between immediate and staged PCI for either endpoint. These neutral findings should be interpreted in the context of limited statistical power, as reflected by the low cumulative incidence of events and trial sequential analysis indicating that the required information size has not yet been reached.19,20 Additional IRR analyses yielded consistent results, further supporting the absence of a clinically meaningful survival difference between strategies. Accordingly, mortality outcomes do not appear to discriminate between immediate and staged PCI, and treatment selection should instead be guided by patient-specific clinical stability and procedural considerations rather than isolated mortality endpoints alone.
Regarding reinfarction risk, immediate PCI was consistently associated with a significantly lower rate of reinfarction vs staged PCI. Exploratory meta-regression analyses did not identify procedural timing, diabetes, or hypertension prevalence as significant modifiers of this association. Trial sequential and sensitivity analyses showed consistent results across the models, with no evidence of heterogeneity. Although the required information size was not fully reached, the consistency of findings across multiple analytical approaches supports a robust association between immediate PCI and reduced recurrent ischemic events.
Regarding AKI, there were no significant differences between immediate and staged PCI, with low event rates and no heterogeneity across trials. The limited number of events precluded meaningful trial sequential analysis, highlighting insufficient power to detect small differences. Although post-PCI AKI is influenced by multiple factors, including contrast exposure and procedural complexity,21 current evidence does not support the assumption that staged PCI reduces renal risk by distributing contrast load.22 None of the included trials were specifically powered for renal outcomes, and AKI definitions varied across studies. Therefore, until adequately powered trials with standardized definitions become available, PCI timing decisions should remain individualized, taking into account baseline renal function and overall procedural risk.23
There were no significant differences in the rates of stroke between staged and immediate PCI, with few events being reported across trials, limiting statistical power. Available evidence suggests that stroke risk after PCI in STEMI is more closely related to procedural factors than to the timing of non-culprit revascularization.15 Accordingly, stroke does not appear to represent a clinically discriminative endpoint when comparing immediate and staged revascularization strategies in this population.
Historically, international clinical practice guidelines favored a staged approach to complete revascularization in STEMI with multivessel disease, largely due to concerns regarding procedural complexity, contrast exposure, and hemodynamic instability during the index intervention. However, cumulative randomized evidence has challenged this paradigm, showing that immediate complete PCI can be performed safely in hemodynamically stable patients, with outcomes comparable or superior to staged strategies.13,17,24,25 Notably, most prior trials primarily enrolled clinically stable patients following successful reperfusion, which may limit the generalizability of their findings to higher-risk STEMI populations. In this context, the OPTION-STEMI trial extends the available evidence by including patients with transient or mild hemodynamic instability, thereby providing contemporary data that better reflect real-world clinical complexity.18
Consistent with our primary findings, immediate and staged PCI did not differ in cardiac death or all-cause mortality at 1 year, while immediate PCI was associated with a lower risk of reinfarction. Beyond clinical outcomes, immediate complete revascularization may offer economic advantages by reducing the length of stay, avoiding repeat cardiac catheterizations, and optimizing resource utilization. In contrast, staged PCI often requires a second procedure and hospitalization, increasing cumulative costs by up to 50% in some analyses,26,27 and mirroring the additional expenses associated with unplanned readmissions for recurrent ischemia. In this context, a single-session revascularization strategy may provide both clinical and economic value, particularly in health care systems with constrained resources, where contemporary PCI costs remain substantial.28
From a safety and efficacy perspective, both staged and immediate PCI represent acceptable revascularization strategies in appropriately selected patients with STEMI and multivessel disease. In the present analysis, immediate PCI was primarily associated with a reduction in recurrent ischemic events, while major adverse cardiovascular events, including cardiac death and all-cause mortality did not differ significantly across strategies. Accordingly, the choice between immediate and staged PCI may increasingly be guided by patient-specific clinical characteristics and logistical considerations rather than concerns regarding procedural safety.
Although not directly assessed in this meta-analysis, emerging evidence suggests that systemic biological factors—such as inflammation, hypercoagulability, and sympathetic activation—may influence recurrent ischemic risk beyond angiographic severity alone.29,30 In addition, features of plaque vulnerability have been associated with future ischemic events in non-culprit lesions, even when angiographically mild.31 Integrating biological risk markers and clinical stability into revascularization decision-making, therefore, represents a relevant direction for future research aimed at refining individualized strategies in patients with STEMI and multivessel disease.
Limitations
Several limitations should be acknowledged. First, only 6 randomized controlled trials were included, resulting in limited statistical power, particularly for rare outcomes. Second, this analysis was restricted to patients with STEMI and multivessel disease; therefore, the findings should not be extrapolated to other acute coronary syndrome populations, and the limited number of trials reporting all prespecified outcomes may reduce the robustness of certain estimates. Third, the use of aggregate study-level data precluded adjustment for individual patient characteristics and limited the assessment of patient-level effect modification; accordingly, meta-regression analyses were exploratory and should be interpreted with caution given the small number of included studies and the potential for ecological bias. Finally, variability in the timing of staged PCI across trials may have introduced residual clinical heterogeneity, and formal assessments of publication bias were underpowered due to the limited number of studies.
CONCLUSIONS
This meta-analysis, integrating additional analytical approaches, provides a focused comparison of immediate vs staged PCI in patients with STEMI and multivessel disease. Immediate PCI was consistently associated with a lower risk of reinfarction, without significant differences being reported in cardiac death or all-cause mortality, stroke, or renal injury. Although the cumulative evidence remains below the required information size for certain hard endpoints, the consistency of findings across multiple analyses supports the robustness of the observed reduction in reinfarction events. From a clinical perspective, these results suggest that immediate complete revascularization can be performed safely in appropriately selected patients and may reduce the burden of reinfarction. Accordingly, the choice between immediate and staged strategies should increasingly be guided by patient-specific clinical stability and practical considerations rather than by concerns regarding procedural safety alone. Future research incorporating biological risk markers may further refine individualized revascularization strategies in this population.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
This meta-analysis was based exclusively on data from previously published studies and involved secondary analyses of publicly available information. Therefore, approval by an Ethics Committee or institutional review board was deemed unnecessary. As no individual patient data or case reports were included, informed consent was not applicable. All the studies included were conducted in full compliance with the ethical standards of the respective institutions at the time of their original publication.
In line with the SAGER guidelines, we assessed sex and gender reporting in the included randomized trials. While sex was generally reported at baseline, sex-disaggregated outcome data and gender-related variables were rarely available, precluding analyses by sex or gender. This limitation should be considered when interpreting the results.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
During the preparation of this work the authors used ChatGPT 5.2 to review the syntaxis and grammar of this document. After using this tool/service, the authors reviewed and edited the content as needed and took full responsibility for the content of the published article.
AUTHORS’ CONTRIBUTIONS
D. Paulino-González: conceptualization, formal analysis, drafting – review and editing. L.H. García-Mena: formal analysis, investigation, drafting – review and editing. E. Andrade-Arbaiza: methodology, investigation, drafting – review and editing. D.A. Navarro-Martínez: methodology, formal analysis; J.L. Maldonado-García: formal analysis, drafting – review and editing; S.A. Xiloj-López: investigation. C.J. Palomino-Ojeda: investigation, drafting – review and editing, R.M. Arellano-Sánchez: data curating, formal analysis. N.E. Antonio-Villa: data curating, formal analysis, drafting – review and editing. A. Ricalde-Alcocer: drafting – review and editing, supervision. D. Araiza-Garaygordobil: drafting – review and editing, supervision.
CONFLICTS OF INTEREST
None declared.
ACKNOWLEDGEMENTS
The authors respectfully honor, in memory, a beloved family member of one of the coauthors, and gratefully acknowledge the support of Dr. Pavel Pichardo-Rojas.
SUPPLEMENTARY DATA
WHAT IS KNOWN ABOUT THE TOPIC?
- Multivessel disease is present in approximately 40% of patients with ST-segment elevation myocardial infarction and is associated with an increased risk of recurrent myocardial infarction and mortality. Complete revascularization, including both culprit and non-culprit lesions, reduces adverse cardiovascular events compared with culprit-lesion-only PCI. Non-culprit lesions may be treated either during the index procedure or in a staged approach; however, the optimal timing of revascularization remains uncertain.
WHAT DOES THIS STUDY ADD?
- This meta-analysis of 6 randomized controlled trials provides a comprehensive comparison of immediate vs staged PCI for non-culprit lesions in STEMI with multivessel disease. Immediate PCI was associated with a lower risk of reinfarction, without significant differences being reported in cardiac death, all-cause mortality, stroke, or AKI. Exploratory meta-regression analyses did not identify procedural timing or baseline comorbidities as effect modifiers. Overall, these findings support the safety of immediate complete revascularization and suggest a potential clinical and economic advantage by reducing recurrent ischemic events and repeat procedures.
REFERENCES
1. Pimor A, Auffret V, Didier R, et al. Immediate complete revascularization in patients with ST-segment elevation myocardial infarction and multivessel disease treated by primary percutaneous coronary intervention:Insights from the ORBI registry. Arch Cardiovasc Dis. 2018;111:656-665.
2. Muller DWM, Topol EJ, Ellis SG, Sigmon KN, Lee K, Califf RM. Multivessel coronary artery disease:a key predictor of short-term prognosis after reperfusion therapy for acute myocardial infarction. Thrombolysis and Angioplasty in Myocardial Infarction (TAMI) Study Group. Am Heart J. 1991;121(4 Pt 1):1042-1049.
3. Jaski BE, Cohen JD, Trausch J, et al. Outcome of urgent percutaneous transluminal coronary angioplasty in acute myocardial infarction:comparison of single-vessel vs multivessel coronary artery disease. Am Heart J. 1992;124:1427-1433.
4. Wald DS, Morris JK, Wald NJ, et al. Randomized trial of preventive angioplasty in myocardial infarction. N Engl J Med. 2013;369:1115-1123.
5. Gershlick AH, Khan JN, Kelly DJ, et al. Randomized trial of complete vs lesion-only revascularization in patients undergoing primary percutaneous coronary intervention for STEMI and multivessel disease:the CvLPRIT trial. J Am Coll Cardiol. 2015;65:963-972.
6. Mehta SR, Wood DA, Storey RF, et al. Complete Revascularization with Multivessel PCI for Myocardial Infarction. N Engl J Med. 2019;381:1411-1421.
7. O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction:a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:362-425.
8. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation:The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119-177.
9. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40:87-165.
10. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement:an updated guideline for reporting systematic reviews. BMJ. 2021;372:71.
11. Higgins JPT, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.5 (updated August 2024). Cochrane. Available at www.cochrane.org/handbook. Accessed 11 Dec 2025.
12. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177-188.
13. Stähli BE, Varbella F, Linke A, et al. Timing of Complete Revascularization with Multivessel PCI for Myocardial Infarction. N Engl J Med. 2023;389:1368-1379.
14. Politi L, Sgura F, Rossi R, et al. A randomised trial of target-vessel vs multi-vessel revascularisation in ST-elevation myocardial infarction:major adverse cardiac events during long-term follow-up. Heart. 2010;96:662-667.
15. Park S, Rha SW, Choi BG, et al. Immediate versus staged complete revascularization in patients with ST-segment elevation myocardial infarction and multivessel coronary artery disease:results from a prematurely discontinued randomized multicenter trial. Am Heart J. 2023;259:58-67.
16. Maamoun W, Elkhaeat N, Elarasy R. Safety and feasibility of complete simultaneous revascularization during primary PCI in patients with STEMI and multi-vessel disease. Egypt Heart J. 2011;63:39-43.
17. Wood DA, Cairns JA, Wang J, et al. Timing of Staged Nonculprit Artery Revascularization in Patients With ST-Segment Elevation Myocardial Infarction:COMPLETE Trial. J Am Coll Cardiol. 2019;74:2713-2723.
18. Kim MC, Ahn JH, Hyun DY, et al. Immediate versus staged complete revascularisation during index admission in patients with ST-segment elevation myocardial infarction and multivessel disease (OPTION–STEMI):a multicentre, non-inferiority, open-label, randomised trial. Lancet. 2025;406:1032-1043.
19. Schoenfeld DA. Sample-Size Formula for the Proportional-Hazards Regression Model. Biometrics. 1983;39:499.
20. Olivier CB, StrußL, Sünnen N, et al. Accuracy of Event Rate and Effect Size Estimation in Major Cardiovascular Trials:A Systematic Review. JAMA Netw Open. 2024;7:248818-248818.
21. Mehran R, Dangas GD, Weisbord SD. Contrast-Associated Acute Kidney Injury. N Engl J Med. 2019;380:2146-2155.
22. Almendarez M, Gurm HS, Mariani J, et al. Procedural Strategies to Reduce the Incidence of Contrast-Induced Acute Kidney Injury During Percutaneous Coronary Intervention. JACC Cardiovasc Interv. 2019;12:1877-1888.
23. Nakamura T, Watanabe M, Sugiura J, et al. Prognostic impact and predictors of persistent renal dysfunction in acute kidney injury after percutaneous coronary intervention for acute myocardial infarction. Scientific Reports. 2024;14:1-9.
24. Rao S V, O'Donoghue ML, Ruel M, et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes:A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2025;151:771-862.
25. Diletti R, den Dekker WK, Bennett J, et al. Immediate versus staged complete revascularisation in patients presenting with acute coronary syndrome and multivessel coronary disease (BIOVASC):a prospective, open-label, non-inferiority, randomised trial. Lancet. 2023;401:1172-1182.
26. Virani SS, Newby LK, Arnold SV, et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients With Chronic Coronary Disease:A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2023;148:E9-E119.
27. Kim LK, Yeo I, Cheung JW, et al. Thirty?Day Readmission Rates, Timing, Causes, and Costs after ST?Segment–Elevation Myocardial Infarction in the United States:A National Readmission Database Analysis 2010-2014. J Am Heart Assoc. 2018;7:009863.
28. Hsia RY, Antwi YA, Weber E, Nath JB. A Cross-Sectional Analysis of Variation in Charges and Prices across California for Percutaneous Coronary Intervention. PLoS One. 2014;9:103829.
29. Seropian IM, Toldo S, Van Tassell BW, Abbate A. Anti-inflammatory strategies for ventricular remodeling following ST-segment elevation acute myocardial infarction. J Am Coll Cardiol. 2014;63:1593-1603.
30. Klingenberg R, Brokopp CE, Grivès A, et al. Clonal restriction and predominance of regulatory T cells in coronary thrombi of patients with acute coronary syndromes. Eur Heart J. 2015;36:1041-1048.
31. Spagnolo M, Giacoppo D, Laudani C, et al. Advances in the Detection and Management of Vulnerable Coronary Plaques. Circ Cardiovasc Interv. 2025;18:015529.
- Design of the LUDICO study: effectiveness and safety of coronary laser in undilatable or uncrossable lesions
- Clinical utility of thrombus aspiration using the Hunter catheter in patients with acute myocardial infarction: the Hunted registry
- Out-of-hours presentation and 30-day myocardial infarction mortality in Mexico: a 2014-2023 retrospective study
- Transcatheter mitral edge-to-edge repair vs optimal medical therapy in secondary mitral regurgitation: a meta-analysis







Review Articles

Interviews

An interview with Bruno Scheller
aServicio de Cardiología, Hospital Universitario de La Princesa, Instituto de Investigación Sanitaria de La Princesa (IIS-IP), Universidad Autónoma de Madrid, Spain
bCentro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain



