
Coronary involvement of mycotic pseudoaneurysms is rare but has increased with the widespread use of percutaneous coronary intervention (PCI). Although surgery has traditionally been recommended, PCI has emerged as a feasible alternative, particularly in patients with prohibitive surgical risk.
We present the case of an 84-year-old man with very high cardiovascular risk (hypertension, diabetes mellitus, dyslipidemia, former smoking) and chronic ischemic heart disease, previously treated with drug-eluting stents. One month earlier, he had been hospitalized for pulmonary bacteremia due to Klebsiella pneumoniae. He was readmitted with dyspnea, chest pain and fever; blood cultures again yielded grew K. pneumoniae. Chest computed tomography (CT) showed pneumonia and an aneurysmal dilatation (figure 1A, blue arrow) at the site of the prior circumflex stent (figure 1A,C, red arrow), with associated soft-tissue thickening suggestive of a contained pseudoaneurysm rupture (figure 1A, asterisk). Transthoracic echocardiography showed concordant findings (figure 1B, asterisk). Given the high risk of rupture and the patient’s prohibitive surgical risk, the heart team decided on percutaneous exclusion after blood cultures tested negative following initiation of ceftriaxone according to the antibiogram.
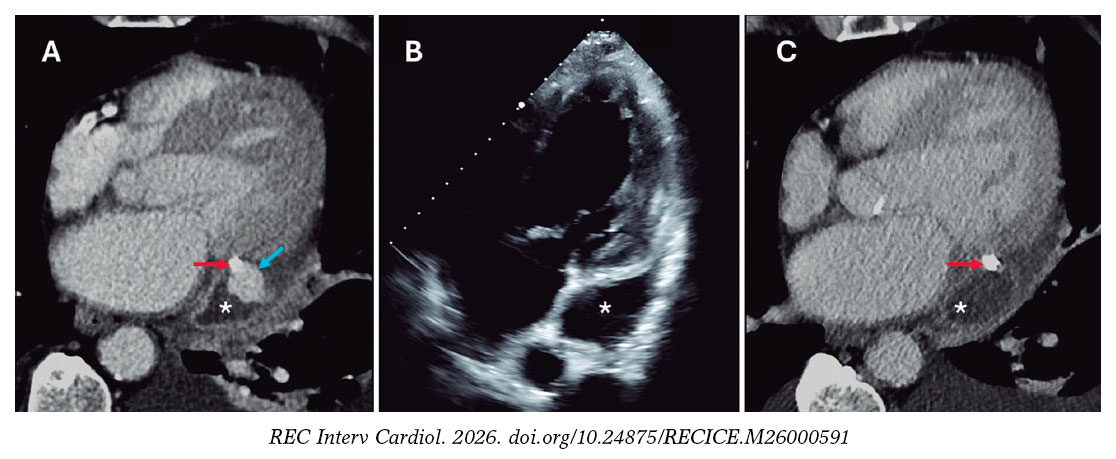
Figure 1.
Via radial access, 2 covered stents were implanted within the prior stent, achieving complete pseudoaneurysm sealing (figure 2A, arrow) and restoration of distal flow (figure 2A-B, video S1). The risk associated with the use of covered stents in this context was considered acceptable. The patient had an uneventful recovery and, at the 2-month follow-up, remained asymptomatic with complete pseudoaneurysm exclusion confirmed by CT (figure 1C, asterisk).
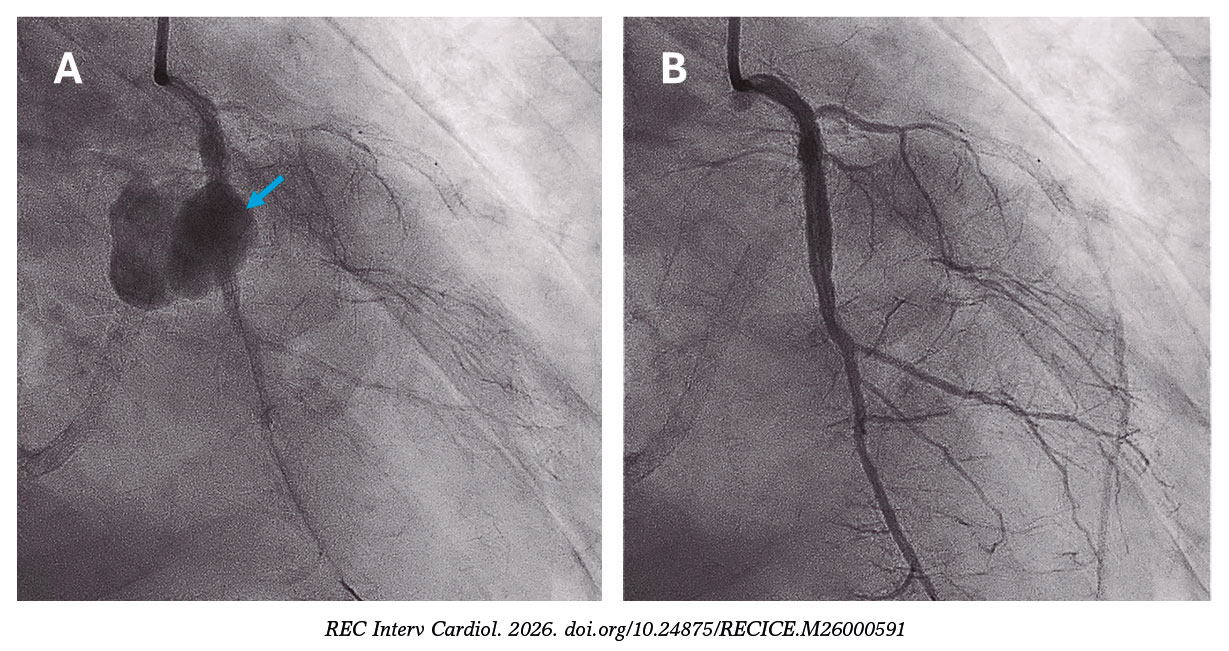
Figure 2.
Despite the rarity of this condition, similar cases have been reported, supporting percutaneous management as a safe and effective therapeutic option.
FUNDING
This work has not received funding.
ETHICAL CONSIDERATIONS
The present clinical case was conducted in full compliance with the ethical principles outlined in the Declaration of Helsinki. Ethics committee approval was deemed unnecessary; however, prior written informed consent for publication of the case and accompanying images was obtained from the patient. The authors adhered to the SAGER guidelines for sex and gender equity in research.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence tools or software were used in the preparation of this manuscript.
AUTHORS’ CONTRIBUTIONS
F. Torres-Mezcua and J. Valencia were the interventional cardiologists who performed the coronary intervention. J. Arenas analyzed the radiological findings of the CT scan. E. Blanco-López and M. Herrero-Brocal conducted the literature review and drafted the manuscript, which was critically revised by J.M. Ruiz-Nodar. All authors reviewed and approved the final version of the manuscript.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest in relation to this manuscript.
SUPPLEMENTARY DATA
Vídeo 1. Blanco-López E. DOI: 10.24875/RECICE.M26000591













