
To the Editor,
Microcatheters are essential tools to facilitate guidewire manipulation and exchange, thus enhancing the guidewire penetration force.1 The ReCross over-the-wire dual-lumen microcatheter (DLM) (IMDS, The Netherlands) is the latest evolution among DLM microcatheters. However, no data are available in the medical literature yet. From September 2020 through November 2020 a total of 8 patients undergoing percutaneous coronary intervention (PCI) of chronic total coronary occlusions (CTO) with the ReCross at 5 Italian high-volume PCI-capable centers were retrospectively identified. This study complied with the Declaration of Helsinki, and written informed consent was obtained from all participants.
Case 1. A proximal right coronary artery CTO underwent antegrade approach using the ReCross microcatheter (IMDS, The Netherlands) as a first choice due to the presence of a bifurcation at distal cap level (figure 1). The antegrade wire escalation technique was used with an Ultimate Bros 3 guidewire (Asahi Intecc, Japan) followed by a Gaia Second guidewire (Asahi Intecc, Japan) that was able to cross the CTO body and reach the side branch (right ventricular branch) distal true lumen (figure 1B). The ReCross was advanced over the Gaia Second guidewire through the lesion close to the bifurcation; afterwards, another Gaia Second guidewire was advanced through the blue lumen and easily directed towards the distal main vessel (figure 1C). The ReCross was then advanced as a single-lumen microcatheter (SLM) into the distal right coronary artery true lumen.
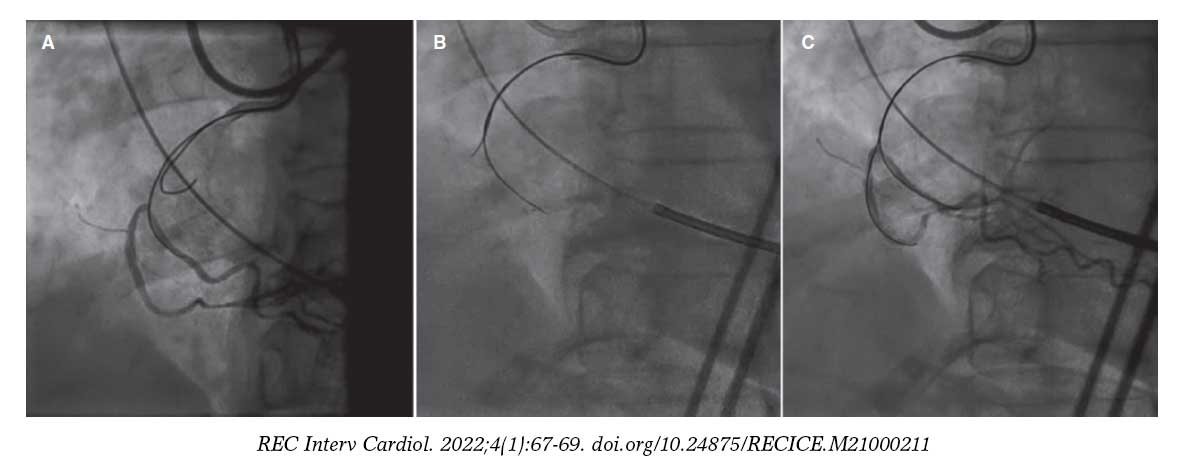
Figure 1. Bifurcation at distal cap level. A: the first chronic total coronary occlusion guidewire (Gaia Second) went into the side branch; B: a second chronic total coronary occlusion guidewire (Gaia Second) was inserted through the hub of the stylet lumen to engage the main vessel; C: a controlateral injection confirmed the correct positioning of the second guidewire into the main distal true lumen.
Case 2. The CTO of a mid-left anterior descending coronary artery (LAD) underwent antegrade approach with the ReCross as the single-lumen microcatheter using the antegrade wire escalation strategy. However, all the guidewires went subintimal and finally the successful recanalization of the occluded artery was achieved using an antegrade dissection and re-entry strategy (ADR). The ReCross microcatheter was advanced over the subintimal guidewire through the white lumen down towards the CTO (figure 2A). Then, a second stiffer guidewire was advanced through the blue lumen and redirected from the subintimal space (figure 2B) into the distal true lumen (figure 2C). The remaining cases are shown on table 1.
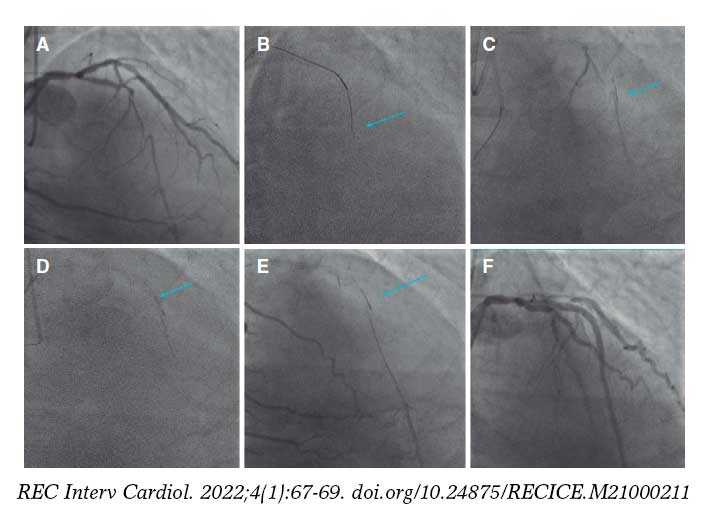
Figure 2. Antegrade dissection and re-entry. A: mid-left anterior descending coronary artery chronic total coronary occlusion; B: unintentional guidewire subintimal tracking (arrow); C: a retrograde superselective tip injection from the septal connection shows the subintimal tracking of the ReCross microcatheter (arrow); D: subintimal guidewire redirection with a stiff guidewire advanced through the stylet lumen to perform a controlled re-entry puncture from the subintimal space into the true lumen (arrow); E: the contralateral injection confirms the correct positioning of the second guidewire into the distal true lumen (arrow); F: final outcome after successful percutaneous coronary intervention of left anterior descending coronary artery chronic total coronary occlusion.
| Artery involved | Approach | Technique used | Anatomical setting | J-CTO score | Fluoroscopy time (min) | Guidewires used | CTO recanalization | |
|---|---|---|---|---|---|---|---|---|
| Case 1 | RCA | Antegrade | DLM | Combination of CTO and bifurcation | 2 | 35 | UB3, Gaia Second | Yes |
| Case 2 | LAD | Antegrade | ADR | Unintentional antegrade guidewire subintimal tracking | 3 | 77 | UB3, Gaia Second, Gaia Third, CP 12 | Yes |
| Case 3 | RCA | Antegrade | Parallel guidewire | Unintentional antegrade guidewire subintimal tracking | 2 | 58 | UB3, Gladius, Gaia Second | Yes |
| Case 4 | RCA | Antegrade | ADR | Hematoma decompression | 3 | 65 | Gladius, Gaia Second, Gaia Third, Hornet 14 | Yes |
| Case 5 | LCX | Antegrade | Parallel guidewire | Unintentional antegrade guidewire subintimal tracking | 3 | 73 | UB3, Gaia Second, Gaia Third, CP 12, Hornet 14 | Yes |
| Case 6 | LAD | Antegrade | Parallel guidewire | Unintentional antegrade guidewire subintimal tracking | 2 | 61 | Gladius, Gaia Second | Yes |
| Case 7 | RCA | Antegrade | DLM | Combination of CTO and bifurcation | 2 | 46 | Fielder XT-R, UB3 | Yes |
| Case 8 | RCA | Retrograde | DLM | Combination of CTO and bifurcation | 3 | 88 | UB3, Suoh 0.3, Gaia Second | Yes |
|
ADR, antegrade dissection and re-entry; CTO, chronic total coronary occlusion; DLM, dual-lumen microcatheter; LAD, left anterior descending coronary artery; LCX, left circumflex artery; RCA, right coronary artery. |
||||||||
The ReCross microcatheter is the new member of the DLM family and its main technological advances are represented by a) the presence of an over-the-wire (OTW) system instead of a monorail system for the tip lumen; b) an additional exit port (the third one) in the tip lumen at a 180° angle of the exit port of the stylet lumen. The second OTW lumen gives the possibility of exchanging and using 2 different guidewires simultaneously and the additional exit port facilitates the redirection of the guidewire (figure 2). In the following paragraphs we detail the versatile use of the ReCross in different anatomical settings during the PCI of a CTO.
Combination of CTOs and bifurcations: the presence of bifurcation lesions in the context of a CTO can be one of the most complex subsets during the PCI.2 In case of a bifurcation close to the proximal cap, the ReCross can be selected as a frontline microcatheter as the procedure is expected to require dual guidewire access. The ReCross is advanced over the workhorse guidewire inside the side branch until the proximal cap. Then, a CTO dedicated guidewire can be advanced through the second OTW lumen to negotiate the occlusion. This technique allows precise manipulations of the CTO guidewire and increases support to be able to penetrate the proximal cap.3 Notably, when the use of intravascular ultrasound-guided puncture is required, the small profile of the ReCross allows the simultaneous use of both devices in a 7-Fr guiding catheter with a large lumen. After successful puncture of the proximal cap the ReCross microcatheter should be removed from the side branch using the trapping technique. Afterwards, it can be re-advanced as a SLM to support the guidewire advance into the distal target true lumen. Finally, when facing a bifurcation inside the CTO body like at distal cap level, the use of the ReCross can be essential for the CTO guidewires to engage the side branch. In this scenario, the ReCross can be advanced at bifurcation level and a second CTO guidewire can be inserted through the second OTW lumen to engage the main distal vessel (case 1).
Unintentional antegrade guidewire subintimal tracking: in many antegrade procedures when the first guidewire goes subintimal, the most useful strategy is to use the parallel guidewire technique. The first guidewire is left in place as a marker occluding the false lumen and modifying the anatomy of the vessel. The first microcatheter must be replaced by a DLM, which is advanced over the subintimal guidewire. Afterwards, a second dedicated CTO guidewire can be used to re-engage the cap for intentional intimal plaque tracking. In those cases in which the parallel guidewire technique is required, the ReCross microcatheter allows the insertion of a second CTO guidewire through the hub of the stylet lumen in order to re-engage the cap. By using the ReCross device operators can advance simultaneously 2 CTO guidewires through 2 different OTW lumens, somehow similar to the pioneering see-saw wiring technique with 2 SLMs.
Antegrade dissection and re-entry (ADR): ADR techniques are characterized by the intentional use of the subintimal space to cross coronary CTOs followed by the subsequent re-entry into the distal true lumen.4 Several devices have been developed to facilitate a controlled ADR (CrossBoss microcatheter and the Stingray balloon; Boston Scientific, United States). The main limitations of these devices are their costs and crossing-profile, which often requires prior balloon dilatation with the corresponding increase of subintimal hematomas. Conversely, the ReCross microcatheter can be advanced into the subintimal space distally to the occlusion often without the need for vessel pre-dilatation to perform a subintimal guidewire redirection. The operator can advance a stiff guidewire through the appropriate lumen to perform a controlled re-entry puncture from the subintimal space towards the true lumen.
Additionally, with the ReCross device it is possible to use 2 CTO guidewires simultaneously to achieve re-entry from the subintimal space towards the true lumen with an high success rate. Moreover, the first lumen can be used for vessel decompression of the subintimal hematoma, thus facilitating the re-entry of the second guidewire. In conclusion, the ReCross device provides a versatile and attractive alternative to standard DLM when performing the PCI of a CTO potentially reducing procedural costs and time.
FUNDING
None reported.
AUTHORS’ CONTRIBUTIONS
R. Garbo, M. Iannaccone, J. Sanz Sánchez, and G.L.Gasparini contributed to the design, analysis, and writing of this manuscript. J.A.Oreglia, and A.Gagnor contributed to the design, and writing of this manuscript too.
CONFLICTS OF INTEREST
None reported.
REFERENCES
1. Oreglia JA, Garbo R, Gagnor A, et al. Dual lumen microcatheters for complex percutaneous coronary interventions. Cardiovasc Revasc Med. 2018;19:298-305.
2. Galassi AR, Boukhris M, Tomasello SD, et al. Incidence, treatment, and in-hospital outcome of bifurcation lesions in patients undergoing percutaneous coronary interventions for chronic total occlusions. Coron Artery Dis. 2015;26:142–149.
3. Arif I, Callihan R, Helmy T. Novel use of twin-pass catheter in successful recanalization of a chronic coronary total occlusion. J Invasive Cardiol. 2008;20:309–311.
4. Danek BA, Karatasakis A, Karmpaliotis D, et al. Use of antegrade dissection re-entry in coronary chronic total occlusion percutaneous coronary intervention in a contemporary multicenter registry. Int J Cardiol. 2016;214:428-437.












