
ABSTRACT
Introduction and objectives: Drug-coated balloons (DCB) are emerging as a valid alternative for the treatment of coronary bifurcation lesions, particularly in the side branch (SB). Among bifurcation lesions, the left anterior descending (LAD)-diagonal location is the most frequently treated. The aim of this study was to evaluate the long-term effectiveness of a DCB in the SB compared with a conventional strategy in this setting.
Methods: This case-control study compared LAD-diagonal lesions treated in which the SB was treated with a DCB vs a conventional strategy consisting of provisional stenting or a 2-stent technique. The mean follow-up was 3 years. The incidence rates of death, acute myocardial infarction, target lesion revascularization, target vessel revascularization, and the composite of major adverse cardiovascular events were recorded.
Results: A total of 86 patients with LAD-diagonal bifurcation lesions treated with a DCB in the SB were included and compared with a cohort of 88 patients who underwent conventional SB management. The mean follow-up was 1008 days (range, 5-2411 days). In the control group, the strategy consisted of stenting of the main branch only in 76.2% of cases, SB stenting only in 6.8%, and stenting of both branches in 17%. The comparative rate (control vs DCB) of adverse events was as follows: cardiac death, 1.1% vs 2.3% (non-significant); myocardial infarction, 8% vs 0% (P = .014), target lesion revascularization; 9.1% vs 0% (P = .013); target vessel revascularization, 10.2 vs 1.2% (P = .02); and major adverse cardiovascular events, 12.5% vs 3.5% (P = .05).
Conclusions: Treatment of the SB with a DCB in AD-diagonal bifurcation lesions appears to be safe and demonstrates very high long-term effectiveness, with a significantly lower rate of adverse events compared with a conventional strategy. Large randomized clinical trials are needed to confirm these findings.
Keywords: Drug-coated balloon. Coronary bifurcation lesions. Follow-up study.
RESUMEN
Introducción y objetivos: El balón farmacoactivo (BFA) es una alternativa válida en el tratamiento de las lesiones en bifurcación, en especial en la rama lateral (RL). Dentro de las bifurcaciones, la localización descendente anterior (DA)-diagonal es la más frecuente. Nuestro objetivo fue determinar la efectividad a largo plazo del BFA en la RL en dicho escenario, en comparación con una estrategia convencional.
Métodos: Estudio de casos y controles para comparar lesiones en la bifurcación DA-diagonal con las RL tratadas con BFA o con estrategia convencional de stent condicional o 2 stents, con un seguimiento medio de 3 años. Se registró la incidencia de muerte, infarto agudo de miocardio, revascularización de la lesión diana, revascularización del vaso diana y la combinación de eventos cardiovasculares adversos mayores.
Resultados: Se incluyó a 86 pacientes con lesión en la bifurcación DA-diagonal en el grupo de tratamiento con BFA y se compararon con una cohorte de 88 pacientes con abordaje convencional de la RL. El seguimiento medio fue de 1.008 días (rango 5-2.411). La estrategia en el grupo control fue stent solo en la rama principal 76,2%, stent solo en la RL 6,8% y stent en ambas ramas 17%. La incidencia comparativa (control frente a BFA) de eventos adversos fue: muerte cardiaca 1,1 frente a 2, 3% (no significativo); infarto de miocardio 8 frente a 0% (p = 0,014); revascularización de la lesión diana 9,1 frente a 0% (p = 0,013); revascularización del vaso diana 10,2 frente a 1,2% (p = 0,02); y eventos cardiovasculares adversos mayores 12,5 frente a 3,5% (p = 0,05).
Conclusiones: El tratamiento con BFA de la RL en lesiones en la bifurcación DA-diagonal es seguro y presenta una muy alta efectividad a largo plazo, con una incidencia significativamente menor de eventos adversos en comparación con la estrategia convencional. Se requerirían amplios ensayos clínicos aleatorizados para confirmar estos hallazgos.
Palabras clave: Balón farmacoactivo. Lesiones en bifurcación. Estudio de seguimiento.
DCB: drug-coated balloon. MACE: major adverse cardiovascular events. MB: main branch. SB: side branch. TLR: target lesion revascularization. TVR: target vessel revascularization.
INTRODUCTION
Coronary bifurcation lesions represent 20% of all lesions treated in the cath lab; among them, left anterior descending coronary artery (LAD)-diagonal lesions are the most frequent (between 50% and 70% according to published series).1,2 Currently, the most widely accepted strategy is provisional stenting.3-5 The 2-stent strategy is usually reserved for long lesions in the side branch (SB) or as bailout strategy if the SB worsens after main branch (MB) stenting. Drug-coated balloon (DCB) has emerged as a valid strategy for the treatment of these lesions, both in the MB, mainly in Medina 0,1,1 lesions, and in the SB, which is a much more extensively studied scenario.6 Studies have demonstrated significant benefit in angiographic parameters; however, controversy remains regarding clinical benefit, and only recently have studies confirmed significant improvements in clinical events. The theoretical advantages7 of DCB in the management of the SB would mainly be drug delivery at the SB coronary ostium, absence of distortion of its original anatomy, and minimization of strut deformation at the carina if MB stenting is performed.
We present a nonrandomized comparative trial of LAD-diagonal bifurcation lesions with a long-term follow-up (mean 3 years) treated with DCB in the SB vs a control group with conventional SB management.
METHODS
We conducted a comprehensive single-center retrospective registry at Hospital General Dr. Balmis (Alicante, Spain), a high-volume center performing > 1200 angioplasties per year including all consecutive LAD-diagonal bifurcation lesions with SB ≥ 2 mm in which the SB was treated with a paclitaxel-coated SeQuent Please NEO DCB (B. Braun, Germany). Procedures had to conclude successfully (including absence of post-DCB dissection requiring stenting, residual percent diameter stenosis < 50%, and final TIMI grade-3 flow). In our cath lab, the routine clinical practice was to use DCB after MB stenting, recrossing and dilating the cell adjacent to the SB coronary ostium before SB treatment (at the operator’s discretion, the DCB could be used before stenting if recrossing was anticipated to be difficult).
The inclusion period spanned from October 2018 through July 2024. There were no exclusion criteria. The interventional cardiology team was instructed to adhere to device recommendations, including SB predilatation preferably with a noncompliant or scoring balloon at a vessel/balloon diameter ratio of 0.8–1, and DCB use only if acceptable angiographic results were achieved (including TIMI grade-3 flow, no significant dissection, and residual percent diameter stenosis < 30%). The control group included all consecutive procedures performed during the first half of 2021 in which successful LAD-diagonal bifurcation intervention (diagonal diameter ≥ 2 mm) was performed using the provisional or 2-stent technique at operator discretion.
We analyzed clinical patient variables, lesion anatomical characteristics, and procedural data. Mean clinical follow-up was 3 years, conducted via telephone contact or digital health record review. Clinical events were selected according to the Drug Coated Balloon Academic Research Consortium recommendations.8 Recorded events included all-cause mortality (cardiac and noncardiac), acute myocardial infarction (elevation of myocardial injury biomarkers > 99th percentile upper reference limit with clinical evidence of ischemia), lesion thrombosis, target lesion revascularization (TLR), and target vessel revascularization (TVR) (revascularization either of the target lesion included in the study or other segments within the same vessel) at the follow-up. The composite endpoint of mayor adverse cardiovascular events (MACE) included TLR, TVR, hospitalization for acute myocardial infarction, and cardiac death. All patients signed informed consent, and the study was approved by Hospital General Dr. Balmis ethics committee.
Statistical analysis
Continuous variables were expressed as mean and SD and compared using Student t test. Categorical variables were expressed as percentages and were compared using the chi-square test or Fisher’s exact test when expected cell counts were < 5. Variables showing significant differences in univariate analysis between the DCB group and the control group were entered into a logistic regression model to determine independent predictors of higher rates of TLR. Similarly, we constructed event-free survival curves using the Kaplan-Meier method, and the log-rank test to compare the DCB treatment group vs the control group.
RESULTS
A total of 86 patients were included in the DCB group and 88 in the control group. The patients’ clinical and anatomical characteristics are shown in table 1. The rate of true bifurcations (Medina 1,1,1; 1,0,1; or 0,1,1 with SB diameter ≥ 2.5 mm) was 34.9% in the DCB group and 28.4% in the control group (P = .36). Among such variables, significant differences were observed across groups only in multivessel disease and prior coronary intervention, whose incidence rates were both higher in the DCB group. In-stent restenosis lesions were more than twice as frequent in the DCB group, with borderline statistical significance. Procedural variables are shown in table 2.
Table 1. Clinical characteristics of the patients
| Clinical characteristics | DCB group (n = 86) | Control group (n = 88) | P |
|---|---|---|---|
| Age (years) | 67 ± 11 | 65 ± 13 | .28 |
| Male sex | 81.8 | 77.9 | .41 |
| Hypertension | 60.5 | 58 | .73 |
| Dyslipidemia | 75.6 | 67 | .21 |
| Smoking | 25.6 | 31.8 | .36 |
| Diabetes | 24.4 | 34.1 | .16 |
| Prior PTA | 41.9 | 22.7 | < .01 |
| LVEF | 54.3 | 54.4 | .96 |
| Indication for coronary angiography | |||
|
|
|
|
| Multivessel disease | 67.4 | 51.1 | .029 |
| ISR | 15.1 | 6.8 | .079 |
| Medina classification | |||
|
|
|
|
| Lesion in the SB | |||
|
|
|
|
|
DCB, drug-coated balloon; ISR, in-stent restenosis lesion; LV, left ventricle; LVEF, left ventricular ejection fraction; NSTEACS, non–ST-segment elevation acute coronary syndrome; PTA, percutaneous transluminal angioplasty; SB, side branch; STEACS, ST-segment elevation acute coronary syndrome. Data are expressed as No. (%) or mean ± SD. |
|||
Table 2. Procedural characteristics
| Characteristics | DCB group (n = 86) | Control group (n = 88) | P |
|---|---|---|---|
| Radial access | 98.8 | 96.6 | .62 |
| 6-Fr | 96.5 | 90.9 | .78 |
| Predilatation | |||
|
|
|
|
| MB stenting | 84.9 | 93.1 | .079 |
| SB diameter ≥ 2.5 mm | 65.1 | 63.1 | .84 |
| Postdilatation | |||
|
|
|
|
| OCT/IVUS use | 9.3 | 2.3 | .056 |
|
DCB, drug-coated balloon; Fr, French; IVUS, intravascular ultrasound; MB, main branch; OCT, optical coherence tomography; POT, proximal optimization technique; SB, side branch. Data are expressed as percentages. |
|||
In the control group, the predominant strategy was 1 MB stent (76.1%). Stents were implanted in both branches in 17% of the cases and only in the SB in 6.9%. The rates of SB predilatation, MB postdilatation, and use of kissing-balloon or proximal optimization techniques were significantly more frequent in the DCB group. DCB was applied after MB stenting in most cases; pre-stent use occurred in 7 cases (8.1%). The use of intracoronary imaging, such as optical coherence tomography (OCT) or intravascular ultrasound (IVUS) was low in both groups, with a trend toward greater use in the DCB group but remaining < 10%.
The rate of adverse events during follow-up is shown in table 3. After a mean of 3 years, 13 deaths were reported in the DCB group and 11 in the control group, mostly noncardiac. Among the 2 cardiac deaths reported in the DCB group, 1 was due to heart failure progression (after catheterization the patient underwent transfemoral aortic valve implantation and permanent pacemaker implantation), and the other was sudden death at home. No TLR, myocardial infarction, or definite lesion thrombosis occurred in the DCB group. A total of 8 myocardial infarctions were reported in the control group, although only 1 was not target-vessel related (right coronary revascularization in the context of a non-ST-segment elevation acute coronary syndrome). There was 1 case of TVR (figure 1) in the active group in a patient in whom the LAD-diagonal lesion was treated with orbital atherectomy due to severe calcification and who was readmitted 1 year later for unstable angina, without changes on electrocardiogram or echocardiogram and without enzyme elevation. However, repeat catheterization revealed progression of a lesion at the distal margin of the LAD stent, far from the bifurcation treated with DCB. This revascularization was not ischemia-guided, and the result at the bifurcation was optimal. The rate of TLR in the control group was 9.1%, with the MB responsible in 4 of the 8 cases, the SB in 2 cases, and both branches in the remaining 2. The rates of TLR and TVR were significantly lower in the DCB group (TLR, 0 vs 9.1%; P = .013; TVR, 1.2 vs 10.5%; P = .02). The logistic regression model (table 4) showed that none of the analyzed variables were independent predictors of events.
Table 3. Rate of adverse events during follow-up
| Adverse events | DCB group (n = 86) | Control group (n = 88) | P |
|---|---|---|---|
| Follow-up days | 1009 ± 586 | 1028 ± 233 | .66 |
| Cause of death | |||
| Cardiac | 2.3 | 1.1 | .69 |
| Noncardiac | 12.8 | 11.4 | |
| TLR | 0 | 9.1 | .013 |
| TVR | 1.2 | 10.2 | .02 |
| Lesion thrombosis | |||
| Yes | 0 | 3.4 | .15 |
| Possible | 1.2 | 0 | |
| Myocardial infarction | 0 | 8 | .014 |
| Major adverse cardiovascular events | 3.5 | 12.5 | .05 |
|
DCB: drug-coated balloon; TLR: target lesion revascularization; TVR: target vessel revascularization. Data are expressed as No. (%) or mean ± SD. |
|||
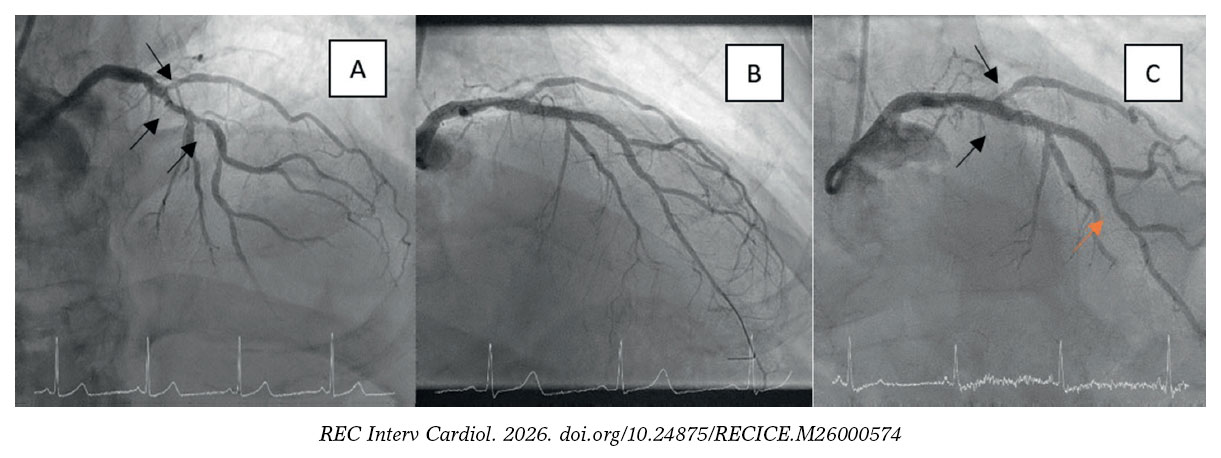
Figure 1. Single case of target vessel revascularization in the drug-coated balloon (DCB) treatment group. A: bifurcation lesion with severe calcification in the main branch. B: optimal result after orbital atherectomy, stent implantation in the left anterior descending coronary artery, and drug-coated balloon in the diagonal branch. C: 1-year follow-up result showing a significant lesion at the distal stent margin (orange arrow), far from the bifurcation treated with DCB (black arrows), which demonstrated sustained procedural success.
Table 4. Logistic regression model for independent predictors of target lesion revascularization
| Factors | P | 95%CI | |
|---|---|---|---|
| Prior PCI | .81 | 0.13-13.2 | |
| Multivessel disease | .45 | 0.11-2.7 | |
| ISR | 1 | 0 – > 30 | |
| SB predilatation | .22 | 0.5-21 | |
| MB stent | 1 | 0 – > 30 | |
| MB postdilatation | .73 | 0.2-8.7 | |
| POT | .85 | 0.09-18.2 | |
| Kissing-balloon | .85 | 0.09-18.2 | |
| OCT/IVUS | 1 | 0 – ≥ 30 | |
|
95%CI, 95% confidence interval; ISR, in-stent restenosis; IVUS, intravascular ultrasound; MB, main branch; OCT, optical coherence tomography; PCI, prior coronary intervention; POT, proximal optimization technique; SB, side branch. |
|||
The rate of MACE was significantly lower in the DCB group (3.5 vs 12.5%; P = .05). Kaplan-Meier curves for primary and secondary endpoints are shown in figure 2.
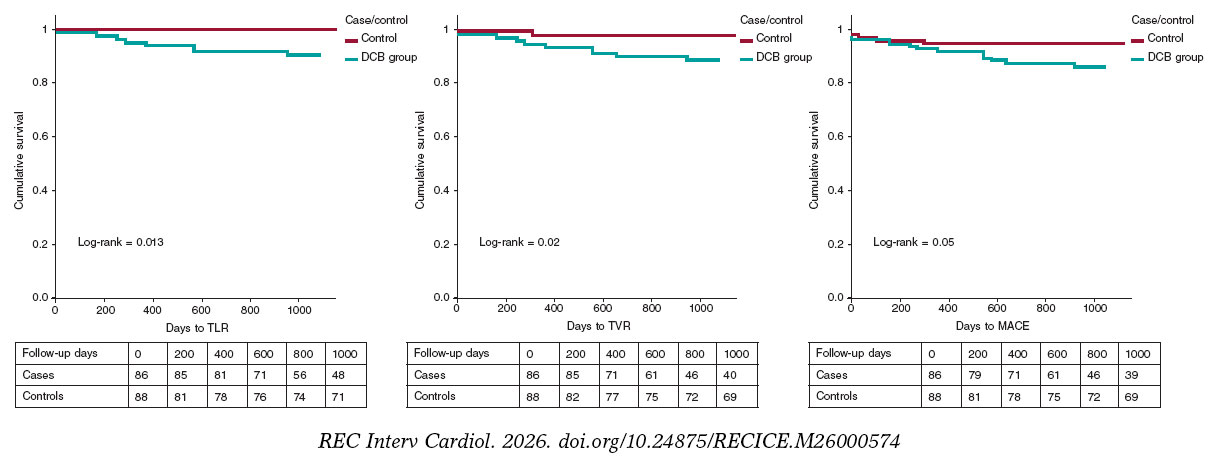
Figure 2. Kaplan-Meier curves for adverse-event–free survival. DCB, drug-coated balloon; MACE, major adverse cardiovascular events; TLR, target lesion revascularization; TVR, target vessel revascularization.
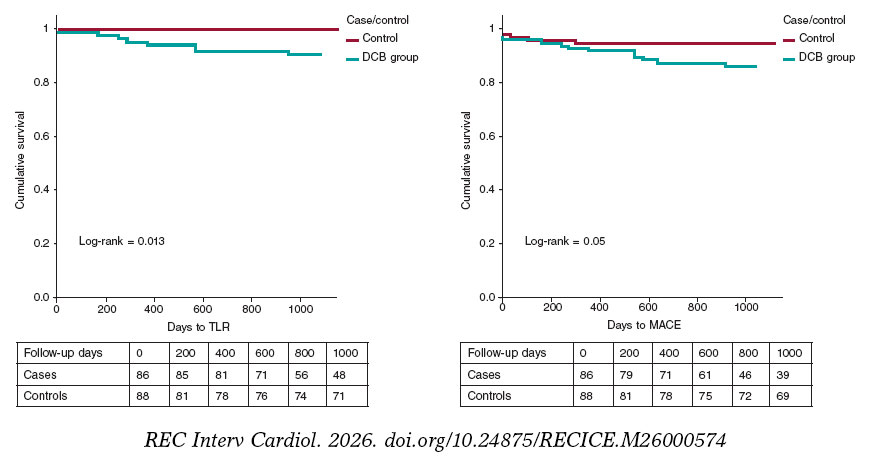
Figure 3. Central illustration. Kaplan-Meier curves for event-free survival. DCB, drug-coated balloon; MACE, major adverse cardiovascular events; TLR, target lesion revascularization.
DISCUSSION
Despite the vast body of literature on coronary bifurcation treatment, the real importance of the SB and its implication in target lesion failure are not well defined; therefore, there are no clear clinical practice guidelines on the optimal therapeutic approach for this branch. Few studies have exclusively analyzed the effectiveness of DCB in SB treatment, although this trend appears to be changing. Early studies published from 2011 onward, such as the DEBIUT,9 the BABILON,10 the DEBSIDE,11 the study by Herrador et al.,12 the PEPCAD V,13 the PEPCAD-BIF,14 and the BEYOND15 showed discrepant data regarding DCB effectiveness, although generally favorable. These studies demonstrated improved quantitative angiographic parameters in terms of restenosis or late lumen loss; however, this was not always accompanied by lower revascularization rates, and there were concerns on a potential increase in late thrombosis, as suggested by some of them. A meta-analysis including 10 studies evaluating the effect of DCB in the SB concluded that this technique resulted in significantly better angiographic outcomes; however, this did not translate into a significant improvement of the outcomes (mainly target lesion failure), according to the authors, due to the low rate of this adverse event and insufficient statistical power because of small sample size.16
The optimal timing for DCB use remains controversial, and no study has demonstrated superiority of its use before or after MB stenting. Although expert consensus recommends its use before stenting, the timing ultimately depends on operator or team experience. Conversely, in the randomized DCB-BIF study17—the most relevant to date—the design required DCB application after stenting.
In the present registry, although not randomized, we consider both groups comparable when interpreting differences in the rate of adverse event, which favored the DCB treatment group. Clinical and anatomical differences were unfavorable to the DCB group (higher rate of in-stent restenosis lesions and multivessel disease), and some procedural differences may be explained by the intrinsic characteristics of each approach in each of the groups (such as a higher SB predilatation rate in the DCB group, considered practically mandatory). Furthermore, multivariate analysis including all these factors did not identify any independent predictor of events, thereby minimizing the likelihood of confounding. Despite this, in the study by Oh et al.,18 treatment of the SB with either a conventional balloon or a stent in 1089 patients with true LAD-diagonal bifurcation lesions, compared with no SB treatment, was associated with a lower rate of target vessel failure. However, this difference did not reach statistical significance overall, although it became significant in the low-risk subgroup.
Very few studies have demonstrated clinical, not only angiographic, benefit after DCB use in the SB. The most relevant one is the 2025 study by Gao et al.,17 in which DCB in the SB after provisional stenting resulted in a significant reduction of the composite adverse event driven by fewer myocardial infarctions, although without significant differences in TLR. The cause of these findings remains controversial.19
Another study published in 2022 randomized 219 true de novo bifurcation lesions to SB treatment with conventional balloon vs DCB.20 At the 12-month clinical and angiographic follow-up, significant improvements were observed both in angiographic parameters (lower late lumen loss and greater late minimum lumen diameter) and clinical outcomes, with a lower rate of MACE; however, this improvement did not translate into significant reductions in new revascularizations or target vessel failure.
In the present study, the rate of adverse events at the 3-year follow-up in the DCB group was exceptionally low, with 0% TLR and 1.2% TVR. The 9% TLR rate in the control group is similar to that reported in former studies of high-risk coronary lesions such as bifurcations. In the abovementioned study by Oh et al.,17 the 3-year rates of TLR went from 6.6% to 9% among > 1000 LAD- diagonal lesions. In another study comparing conventional vs DCB approaches in various complex lesions (including bifurcations: 36% in the first group and 24% in the second), the 2-year rate of TVR was 7.6% in the DCB group and 8.1% in the stent group.21
In a very recent Swedish study, the rate of adverse events was compared in nearly 6800 LAD-diagonal bifurcation lesions treated with a simple (MB only) vs complex strategy (both branches, both with balloon and stent).22 At the 1-year follow-up, the rate of MACE was lower in the complex strategy group (6.2% vs 7.9%; HR, 0.74; 95%CI, 0.59–0.93; P = .010), driven by a lower all-cause mortality rate, without differences in TLR. This benefit persisted at 5 years (17% vs 19.8%; HR, 0.83; 95%CI, 0.72–0.96; P = .010).
The relative importance of the SB in repeat revascularizations remains controversial. Although some studies, such as the BABILON10 showed that new revascularizations originated in the MB, in our registry, in the control group, up to 50% of the cases originated in the SB. This supports the need for exhaustive SB treatment during provisional stenting, both with DCB (as suggested by our results) and any other technique (conventional balloon or stent), particularly if significant SB ostial stenosis persists even without flow limitation.
Our group recently published a study analyzing adverse predictors after DCB use in SB bifurcation lesions regardless of location.23 Only the presence of long SB lesions (> 10 mm) was identified as a negative prognostic factor. Our findings suggest that in the LAD-diagonal location this factor may be less relevant than in other locations, although adequately powered randomized trials are needed to confirm or refute this hypothesis.
Limitations
The main limitations of this study are the lack of randomization, absence of perioperative myocardial infarction recording due to its retrospective design, inability to extract relevant IVUS/OCT data given low usage, relatively small sample size, and lack of systematic angiographic reevaluation, which may have identified subclinical events.
CONCLUSIONS
These results correspond to a single center with a very low long-term rate of adverse events in patients with LAD-diagonal bifurcation lesions whose SB was treated with DCB, significantly lower than in the control group. Currently, this is the first study demonstrating a significant improvement in an important endpoint such as TLR. Therefore, proper lesion selection (possibly those without long SB lesions), meticulous lesion preparation technique, and greater use of IVUS and OCT are essential. Randomized clinical trials with sufficient statistical power are needed to confirm these promising results and definitively establish the superiority of DCB for SB treatment in bifurcation lesions, particularly in the most frequent location, LAD-diagonal.
WHAT IS KNOWN ABOUT THE TOPIC?
- There is a limited number of studies analyzing the role of DCB in SB treatment of coronary bifurcation lesions, particularly in LAD-diagonal.
- Although DCB appears beneficial in angiographic parameters, this has not consistently translated into significant clinical improvement such as target vessel failure or need for repeat revascularization.
WHAT DOES THIS STUDY ADD?
- Experience from a high-volume center with very long-term follow-up representative of real-world practice.
- The favorable results may support DCB as a useful tool to improve long-term outcomes in LAD-diagonal bifurcation intervention.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
The study followed the Helsinki Declaration guidelines and was approved by Hospital General Dr. Balmis ethics committee (Alicante, Spain). Informed consent was obtained. SAGER guidelines regarding sex/gender bias were followed.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence was used in the preparation of this work or manuscript.
AUTHORS’ CONTRIBUTIONS
J. Valencia: patient treatment, data collection, manuscript drafting and revision. F. Torres-Mezcua and M. Herrero-Brocal: patient treatment, data collection and revision. P. Bordes, F. Torres-Saura, J. Pineda and J.M. Ruiz-Nodar: patient treatment and revision. All authors approved the final version.
CONFLICTS OF INTEREST
None declared.
REFERENCES
1. Valencia J, Torres-Mezcua F, Herrero-Brocal M, et al. Long-term effectiveness of drug-coated balloon in the side branch treatment of bifurcation lesions. REC Interv Cardiol. 2023;5:7-13.
2. Kurt M, Tanboga IH, Karakas MF, et al. Clinical and morphological evaluation of coronary bifurcation lesions. Arch Turk Soc Cardiol. 2013;41:207-211.
3. Albiero R, Burzotta F, Lassen JF, et al. Treatment of coronary bifurcation lesions, part I:implanting the first stent in the provisional pathway. The 16th expert consensus document of the European Bifurcation Club. EuroIntervention. 2022;18:e362-e376.
4. Burzotta F, Lassen JF, Louvard Y, et al. European Bifurcation Club white paper on stenting techniques for patients with bifurcated coronary artery lesions. Catheter Cardiovasc Interv. 2020;96:1067-1079.
5. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. 2019;40:87-165.
6. Jeger RV, Eccleshall S, Wan Ahmad WA, et al. Drug-Coated Balloons for Coronary Artery Disease:Third Report of the International DCB Consensus Group. JACC Cardiovasc Interv. 2020;13:1391-1402.
7. Sawaya FJ, Lefèvre T, Chevalier B, et al. Contemporary Approach to Coronary Bifurcation Lesion Treatment. JACC Cardiovasc Interv. 2016;9:1861-1878.
8. Fezzi S, Scheller B, Cortese B, et al. Definitions and standardized endpoints for the use of drug-coated balloon in coronary artery disease:consensus document of the Drug Coated Balloon Academic Research Consortium. Eur Heart J. 2025;46:2498-2519.
9. Stella PR, Belkacemi A, Dubois C, et al. A multicenter randomized comparison of drug-eluting balloon plus bare-metal stent versus bare-metal stent versus drug-eluting stent in bifurcation lesions treated with a single-stenting technique:six-month angiographic and 12-month clinical results of the drug-eluting balloon in bifurcations trial. Catheter Cardiovasc Interv. 2012;80:1138-1146.
10. López Mínguez JR, Nogales Asensio JM, Doncel Vecino LJ, et al. A prospective randomised study of the paclitaxel-coated balloon catheter in bifurcated coronary lesions (BABILON trial):24-month clinical and angiographic results. EuroIntervention. 2014;10:50-57.
11. Berland J, Lefèvre T, Brenot P, et al. DANUBIO —a new drug-eluting balloon for the treatment of side branches in bifurcation lesions:six-month angiographic follow-up results of the DEBSIDE trial. EuroIntervention. 2015;11:868-876.
12. Herrador JA, Fernandez JC, Guzman M, Aragon V. Drug-eluting vs. conventional balloon for side branch dilation in coronary bifurcations treated by provisional T stenting. J Interv Cardiol. 2013;26:454-462.
13. Mathey DG, Wendig I, Boxberger M, Bonaventura K, Kleber FX. Treatment of bifurcation lesions with a drug-eluting balloon:the PEPCAD V (Paclitaxel Eluting PTCA Balloon in Coronary Artery Disease) trial. EuroIntervention. 2011;7 (Suppl K):K61-65.
14. Kleber FX, Rittger H, Ludwig J, et al. Drug eluting balloons as stand alone procedure for coronary bifurcational lesions:results of the randomized multicenter PEPCAD-BIF trial. Clin Res Cardiol. 2016;105:613-621.
15. Jing QM, Zhao X, Han YL, et al. A drug-eluting Balloon for the trEatment of coronarY bifurcatiON lesions in the side branch:a prospective multicenter ranDomized (BEYOND) clinical trial in China. Chin Med J. 2020;133:899-908.
16. Zheng Y, Li J, Wang L, et al. Effect of Drug-Coated Balloon in Side Branch Protection for de novo Coronary Bifurcation Lesions:A Systematic Review and Meta-Analysis. Front Cardiovasc Med. 2021;8:758560.
17. Gao X, Tian N, Kan J, et al. Drug-Coated Balloon Angioplasty of the Side Branch During Provisional Stenting:The Multicenter Randomized DCB-BIF Trial. J Am Coll Cardiol. 2025;85:1-15.
18. Oh GC, Park KW, Kang J, et al. Association of Side-Branch Treatment and Patient Factors in Left Anterior Descending Artery True Bifurcation Lesions:Analysis from the GRAND-DES Pooled Registry. J Interv Cardiol. 2020;2020:8858642.
19. Ali Z, Yong CM. Drug-coated balloons to keep interventions of the side branch simple (KISS):KISS or be KISS'd?J Am Coll Cardiol. 2025;85:16-18.
20. Li Y, Mao Q, Liu H, Zhou D, Zhao J. Effect of Paclitaxel-Coated Balloon Angioplasty on Side Branch Lesion and Cardiovascular Outcomes in Patients with De Novo True Coronary Bifurcation Lesions Undergoing Percutaneous Coronary Intervention. Cardiovasc Drugs Ther. 2022;36:859-866.
21. Joh HS, Kwon W, Shin D, et al. Efficacy of drug-coated-balloon and drug-eluting stent in percutaneous coronary intervention for complex lesions. JACC Asia. 2024;4:519-531.
22. Katona A, von Koch S, Andell P, et al. Long-term prognosis after coronary bifurcation PCI-A nationwide observational study. PLoS One.2025;20:e0317628.
23. Valencia J, Torres-Mezcua F, Herrero M, et al. Prognostic factors in drug-coated balloon interventions for treating the side branch of coronary bifurcation lesions. REC Interv Cardiol. 2025;7:57-59.












