
To the Editor,
Chronic total occlusion (CTO) percutaneous coronary intervention (PCI) is among the most radiation-intensive coronary procedures, owing to high lesion complexity, use of dual injections, and prolonged wire manipulation and/or retrograde techniques, all of which increase fluoroscopy time and cine acquisition. Contemporary data indicate that median patient radiation exposure, measured as air kerma (AK) remains substantial in CTO PCI (median, 2.3 Gy); however, this has been in decline recently due to improvements in equipment and procedural techniques.1 From the patient standpoint, transient tissue reactions usually occur when absorbed radiation skin dose exceeds 2 Gy while permanent effects occur in absorbed doses > 5 Gy.2 For operators, cumulative scatter radiation exposure to the eyes, head, and torso underscores the need to improve shielding and workflow to reduce occupational exposure.3 Importantly, a large multicenter analysis showed that education, equipment optimization, and procedural discipline can significantly decrease radiation exposure without compromising procedural success.4 Similarly, a previously published report from our research group showed that an ultra-low-dose (ULD) fluoroscopy protocol significantly reduces radiation exposure during CTO PCI.5 Accordingly, we sought to evaluate the feasibility of implementing a ULD fluoroscopy workflow during CTO PCI procedures at a single-center institution.
We conducted a retrospective analysis of 88 consecutive patients referred to our single-center catheterization laboratory for elective PCI CTO over a 3-year period (January 2021 to October 2023). Because of the use of solely retrospective and anonymized data for this manuscript, Ethical Committee approval was deemed unnecessary as per our local institutional practices. All procedures were performed by the single operator, and in all patient cases we employed an ULD fluoroscopy workflow featuring routine fluoroscopy at 3.75 frames per second (FPS) and cine acquisition limited to 7.5 FPS. In addition to reduced frame rates, the workflow routinely emphasized tight collimation, minimation of magnification, preferential use of stored fluoroscopy in place of cine acquisition when clinically appropriate, avoidance of unnecessary repeat acquisitions, and attention to shielding and operator positioning. The equipment used in the study was a single-plane suspended C-arm angiographic system (Shimadzu Corporation, Trinias C8, Model DAR 9500f). As this was a retrospective analysis, detailed dose-escalation logs, dose-area product (DAP), and vendor-specific radiation output variables such as pulse width and tube current were not systematically available for all cases and are therefore not reported.
Most patients were male (81.8%) with a mean body mass index of 28.9 ± 5.4 kg/m². The median J-CTO score was 2.0 (interquartile range [IQR], 1-3) points while nearly 40% of cases had a J-CTO score of 0 to 1 (N = 35). Median CTO length per QCA analysis was 15 mm [IQR, 10-20], interventional CTO approach was primarily antegrade in 83% of cases (N = 73), and target CTO vessel was approached via radial access in most cases (94.3%). Median CTO crossing time was 6.5 [2.0-15.0] minutes with a mean of 10.9 ± 16 minutes. The most widely affected CTO artery in our dataset was the right coronary artery (59%), followed by the left circumflex (22%) and left anterior descending coronary arteries (19%). Ten out of 88 patients (10.2%) had a previous CTO recanalization attempt while the mean eGFR at baseline was 70.6 ± 23.1 mL/min/1.73 m². The median contrast volume used was 210 mL (152-260), the median total procedural time was 70 minutes (45-120), and procedural success and Thrombolysis in Myocardial Infarction grade-3 flow were achieved in 75 out of 88 patients (85.2%). No adverse events were observed including death, perioperative myocardial infarction, stroke, coronary perforation, flow-limiting dissection, or bleeding.
Importantly, our data show that median AK at the interventional reference point was 715 mGy (369-1116) with a total fluoroscopy time of only 27 minutes (16-41), as shown in figure 1. This yielded a normalized AK/fluoroscopy-time ratio of approximately 26.5 mGy/min. Within this cohort, the low-frame-rate workflow was feasible and adopted as a routine practice without apparent compromise in procedural conduct. However, given the absence of a contemporary control group and the lack of formal image quality assessment, no comparative inference can be made regarding procedural time, contrast volume, or visualization relative to standard fluoroscopy settings.
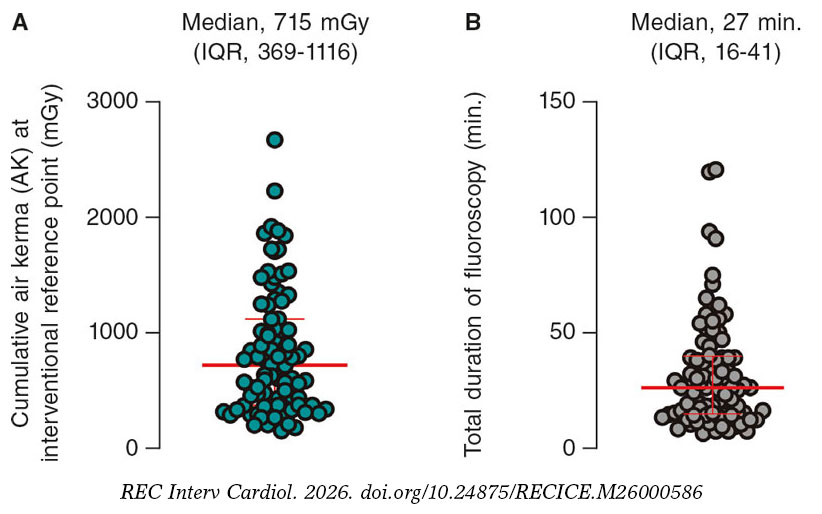
Figure 1. A: median cumulative air kerma at interventional reference point (in mGy); B: median total fluoroscopy time (minutes). IQR, interquartile range.
This feasibility study bears important implications for clinical practice since it demonstrates that, in a cohort with a median J-CTO score of 2 and predominantly antegrade procedures, CTO PCI can often be performed with cumulative radiationa exposure < 1 Gy and total fluoroscopy times < 30 minutes. These absolute AK values are directionally similar to those reported with other structured protocol- based approaches and lower than those described in standard CTO practice, including multicenter PROGRESS-CTO data; however, such cross-study comparisons should be interpreted with caution.1,6 Given that most cases procedures were antegrade, median lesion length was modest, and re-attempts were infrequent, this workflow may be easiest to implement initially in lower- to intermediate- complexity CTO before broader adoption in more complex retrograde or reattempt cases. Importantly, the use of normalized radiation metrics, such as AK per minute of fluoroscopy, may facilitate benchmarking across centers and offer better comparability among institutions employing similar radiation-reduction protocols.
Several limitations should be acknowledged. First, our results may not be generalized to other CTO centers with different operator experience, case selection, or equipment-specific programming because this work is limited to a single center. Furthermore, no standardized universal definition of ULD fluoroscopy currently exists; for this study we used a cumulative procedural AK < 1 Gy as a pragmatic descriptive benchmark rather than a universally accepted threshold. More broadly, our ULD protocol reflects a combination of low frame-rate acquisition (3.75 frames/s fluoroscopy and 7.5 frames/s cine) and systematic dose-reduction strategies, including collimation, minimal magnification, and restriction of cine acquisitions. Our analysis also lacks a contemporary non-ULD comparator cohort. In addition, several potentially relevant variables relevant for external benchmarking— including operator experience, frequency of temporary dose escalation, dose-area product, and vendor-specific radiation output parameters—were not systematically captured in this retrospective dataset. Accordingly, comparison with PROGRESS-CTO1 or other observational series should be considered contextual only rather than a formal control analysis. The protocol described in this report remains in routine use at our center; however, larger datasets and prospective comparative analyses are warranted.
In conclusion, reducing radiation exposure during CTO PCI is essential both for patient safety and operator occupational exposure, especially in CTO. We suggest that interventional cardiologists performing CTO procedures should consider adopting structured radiation-sparing workflows tailored to local expertise and equipment, particularly as part of broader dose-optimization programs. This protocol might be particularly feasible for non-overly complex CTO lesions. Larger comparative studies are needed to define which CTO subsets derive the greatest benefit and to validate these findings across operators, centers, and imaging platforms.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
Under the applicable institutional framework governing this type of research (HR-OBC-71023-2016-04-18), this study was exempt from local ethics committee approval and did not require formal institutional review board oversight. The study was conducted in full compliance with institutional requirements and with the principles outlined in the Declaration of Helsinki. Informed consent was waived due to the retrospective design of the study and the use of fully anonymized data, where applicable. SAGER guidelines were followed with respect to possible sex/gender bias.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence software or services were used while drafting this manuscript.
AUTHORS’ CONTRIBUTIONS
M. Kovacic and J.A. Borovac conceived the idea and wrote the original first draft. M. Ostricki, G.L. Gasparini contributed with important intellectual content, as well as with manuscript drafting and revision. All authors reviewed and approved the final version of the manuscript for publication.
CONFLICTS OF INTEREST
None declared.
REFERENCES
1. Vemmou E, Alaswad K, Khatri JJ, et al. Patient radiation dose during chronic total occlusion percutaneous coronary intervention:insights from the PROGRESS-CTO registry. Circ Cardiovasc Interv. 2020;13:009412.
2. Fisher RF, Applegate KE, Berkowitz LK, et al. AAPM Medical Physics Practice Guideline 12.a:Fluoroscopy dose management. J Appl Clin Med Phys. 2022;23:13526.
3. Roguin A, Wu P, Cohoon T, et al. Update on radiation safety in the cath lab—moving toward a “lead-free“environment. J Soc Cardiovasc Angiogr Interv. 2023;2:101040.
4. Werner GS, Avran A, Boudou N, et al. Improvement of radiation management in percutaneous interventions of chronic total occlusions in a multicenter registry. JACC Cardiovasc Interv. 2025;18425-435.
5. Bacci E, Chiarito M, Sanz-Sanchez J, et al. Safety and efficacy of an ultra low dose fluoroscopic protocol for chronic total occlusion recanalization. Catheter Cardiovasc Interv. 2023;101:911-917.
6. Werner GS, Yaginuma K, Koch M, et al. Modulated radiation protocol achieves marked reduction of radiation exposure for chronic total coronary occlusion intervention. Catheter Cardiovasc Interv. 2021;97:1196-1206.













