
ABSTRACT
Introduction and objectives: Transcatheter aortic valve implantation (TAVI) for pure aortic regurgitation is challenging due to inadequate device anchoring and increased risks of device embolization and paravalvular regurgitation (PVR). This study aimed to review the safety and efficacy of TAVI for aortic regurgitation with devices specifically designed for this indication.
Methods: A comprehensive search of PubMed, Web of Science, Cochrane Library, and major conference archives up to April 2024 identified 143 unique results based on predefined criteria.
Results: Fifteen studies (n = 788 patients) were included, with J-Valve used in 357 patients and JenaValve in 431. Men represented 51% of the cohort, with a mean age of 74.7 ± 8.8 years and an STS-PROM score of 5.8 ± 4.9%. Transapical and transfemoral access routes were used in 62.7% and 37.3% of patients, respectively. Overall, procedural success was achieved in 95.9% of cases; surgical conversion was required in 1.8%, device migration/embolization occurred in 3.2%, and a second valve (in-valve) was required in 2.0% of patients. At 30 days, 95.5% of patients were alive, and device success was reported in 93.3% of cases. Mild PVR was observed in 18.0% of patients, moderate-to-severe PVR in 1.7%, and permanent pacemaker implantation (PPI) was required in 13.0%. In studies focusing on transfemoral procedures (all using JenaValve), the pooled estimates showed a procedural success rate of 97.8% (95%CI, 94.4-100), device success of 97.0% (95%CI, 94.8-99.2), 30-day mortality of 1.96% (95%CI, 0.20-3.72), moderate-to-severe PVR of 0.47% (95%CI, 0.00-1.47), and PPI requirement of 18.7% (95%CI, 13.9-23.4)
Conclusions: This systematic review of relatively small observational studies demonstrates the safety and favorable early outcomes of TAVI using J-Valve and JenaValve in patients with pure aortic regurgitation, especially when the transfemoral approach is used. Nevertheless, the need for PPI remains frequent.
Keywords: Aortic regurgitation. Transcatheter aortic valve implantation. Outcome. Systematic review. J-Valve. JenaValve.
RESUMEN
Introducción y objetivos: El implante percutáneo de válvula aórtica (TAVI) para la insuficiencia aórtica pura es un reto debido al anclaje inadecuado del dispositivo y al mayor riesgo de su embolización y de fuga periprotésica (FPP). Nuestro objetivo fue revisar la seguridad y la eficacia del TAVI para la insuficiencia aórtica con dispositivos dedicados a esta indicación.
Métodos: Una búsqueda exhaustiva mediante criterios predefinidos en PubMed, Web of Science y Cochrane Library, así como en los principales archivos de congresos hasta abril de 2024, identificó 143 resultados únicos.
Resultados: Se incluyeron 15 estudios (n = 788 pacientes), en los que se utilizó J-Valve en 357 pacientes y JenaValve en 431. El 51% eran varones, la edad media fue de 74,7 ± 8,8 años y la puntuación STS-PROM fue de 5,8 ± 4,9%. Se utilizaron accesos transapicales y transfemorales en el 62,7 y el 37,3% de los casos respectivamente. En general, la intervención fue satisfactoria en el 95,9% de los casos; se requirió conversión quirúrgica en el 1,8%, se produjo migración/embolización del dispositivo en el 3,2% y fue necesaria una segunda válvula (in-valve) en el 2%. A los 30 días, el 95,5% de los pacientes estaban vivos y el éxito del dispositivo se alcanzó en el 93,3%. Se observó una FPP leve en el 18,0% y una FPP moderada-grave en el 1,7%, mientras que en el 13,0% fue necesario implantar un marcapasos permanente. En los estudios de intervenciones transfemorales (todas con JenaValve), la estimación conjunta del éxito de la intervención fue del 97,8% (IC95%, 94,4-100), del éxito del dispositivo fue del 97,0% (IC95%, 94,8-99,2), de la mortalidad a 30 días fue del 1,96% (IC95%, 0,20-3,72), de la FPP moderada-grave fue del 0,47% (IC95%, 0,0-1,47) y del implante de marcapasos permanente fue del 18,7% (IC95%, 13,9-23,4).
Conclusiones: Esta revisión sistemática de estudios observacionales relativamente pequeños demuestra la seguridad y los resultados precoces favorables del TAVI con J-Valve y JenaValve en pacientes con insuficiencia aórtica pura, en especial cuando se utiliza el abordaje transfemoral. No obstante, la necesidad de marcapasos permanente sigue siendo frecuente.
Palabras clave: Insuficiencia aórtica. Válvula aórtica percutánea. Resultados. Revisión sistemática. J-Valve. JenaValve.
Abbreviations
AoR: aortic regurgitation. NYHA: New York Heart Association. PPI: permanent pacemaker implantation. PVR: paravalvular regurgitation. TAVI: transcatheter aortic valve implantation.
INTRODUCTION
Aortic regurgitation (AR) results from abnormalities in the valve cusps or the structures supporting them (ie, the aortic root and annulus).1 The prevalence of AR increases with age, affecting 2% of people older than 70 years.2,3 Patients with severe AR have impaired functional capacity and increased mortality compared with the general population.2,4
If left untreated, severe AR leads to left ventricular dysfunction and heart failure in approximately 50% of patients.2 Although surgical aortic valve replacement is the recommended treatment for symptomatic severe AR,5 many elderly patients with this condition are refused surgery due to high operative risk.6
Since the introduction of transcatheter aortic valve implantation (TAVI) in 2002, it has demonstrated good safety and efficacy in various patient groups and several anatomical contexts.7-13 However, due to the high stroke volume, the lack of aortic annular calcification, and the frequent dilatation of the aortic root/annulus, TAVI for pure native AR is associated with an increased risk of adverse events including device dislocation and paravalvular regurgitation (PVR).14 The J-Valve(J.C. Medical, United States) and the JenaValve (JenaValve Technology GmbH, United States) are dedicated, next-generation, self-expanding transcatheter valves designed to address the challenges associated with native pure AR.15,16
To date, the evidence on the safety and efficacy of these technologies in native pure AR is limited. We conducted a systematic review of the current data on the safety and efficacy of TAVI using the J-Valve or JenaValve in patients with native pure AR.
METHODS
This systematic review and associated meta-analysis were conducted in accordance with the standards outlined in the PRISMA statement and the Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0).17,18 The study protocol was prospectively registered (PROSPERO registration number: CRD42023460306).
Data collection
We included studies that involved a minimum of 10 patients who underwent TAVI with the J-Valve or JenaValve for native pure or predominant AR. Studies were excluded if they involved mixed aortic valve disease (moderate to severe stenosis and regurgitation) or prior aortic valve replacement (valve-in-valve procedures).
Information sources, search strategy, and study selection
Three online databases (PubMed, Web of Science, and Cochrane Library) were searched up to March 2024 using the following search terms: ((aortic valve insufficiency OR aortic regurgitation OR regurgitant aortic valve OR aortic incompetency OR incompetent aortic valve OR NAVR OR noncalcific aortic valve) AND (transcatheter aortic valve replacement OR transcatheter aortic valve OR transfemoral aortic valve OR transaortic aortic valve OR transapical aortic valve OR transcutaneous aortic valve OR percutaneous aortic valve OR TAVI OR TAVR) AND (J-Valve OR JenaValve)). Additional relevant studies were identified through a manual search of secondary sources, including references of initially identified articles, reviews, commentaries, and archives of major cardiology conferences.
Endnote software (Clarivate Analytics, United States) was used to remove duplicates. The retrieved references were screened in 2 steps: first, all authors independently screened the titles and abstracts to determine their relevance, and second, the full-text articles of the identified abstracts were reviewed for final eligibility in the quantitative analysis. The Rayyan website was used in the selection process.19 For overlapping study populations, the most recent publication was chosen for inclusion.
Data extraction and outcomes
The data were extracted into a standardized data extraction sheet, which included: a) study characteristics, b) the patients’ baseline characteristics, c) echocardiographic and computed tomographic data, d) procedural data, and e) short-term clinical outcomes.
The main endpoints of the current investigation were device success, procedural success, and 30-day all-cause mortality. Additional outcomes of interest included bleeding, vascular complications, stroke, permanent pacemaker implantation (PPI), and PVR within 30 days.
Assessing the risk of bias
The quality of the retrieved studies was evaluated according to the Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0, updated March 2011). The risk of bias was assessed using appropriate tools based on the study design: the National Institutes of Health (NIH) tool for single-arm observational studies, the Newcastle-Ottawa Scale (NOS) for comparative observational studies, and the NIH tool for case-series studies. The individual studies were classified as ‘Low risk’ or ‘Good,’ ‘High risk’ or ‘Poor,’ and ‘Unclear risk’ or ‘Fair’ of bias.
Assessment of heterogeneity
The statistical heterogeneity among the studies was assessed using the chi-square test, specifically the Cochrane Q test. The chi-square statistic, known as Cochrane Q, was used to compute the I-squared value using the following formula: I2 = ([Q – df] / Q) × 100%. Significant heterogeneity was defined as a chi-square P value < .1. An I-squared value equal to or more than 40% was considered indicative of a significant level of heterogeneity.
Quantitative analysis
The DerSimonian and Laird meta-analysis approach was used to obtain the pooled effect size for all outcomes. Proportions and 95% confidence intervals (95%CI) were computed using R software (version 4.3.1 for Windows) and the Meta package.
A random-effects model, which gives relatively higher weight to smaller studies to account for heterogeneity, was used when heterogeneity was deemed significant. A fixed-effects model was chosen when heterogeneity was lower. Consequently, the predicted effects in our meta-analysis are conservative estimates that account for potential inconsistencies.
Certainty assessment
A certainty evaluation was performed using sensitivity analysis (leave-one-out meta-analysis) to test the robustness of the evidence. This analysis was conducted using R software (version 4.3.1 for Windows) with the Meta package and Metainf function. Sensitivity analyses were was run in several scenarios for each outcome in the meta-analysis, eliminating one study in each scenario, to ensure that the overall effect size was not dependent on any single study.
RESULTS
Literature search
Our search identified 143 results after duplicates were removed. Following title and abstract screening, 29 articles were selected for full-text review. Of these, 15 studies6,14,20-32 were included in the systematic review, with 5 studies of transfemoral TAVI being included in the quantitative meta-analysis. No further articles were included after manually searching the references of the included studies. The selection process is illustrated in a PRISMA flow diagram (figure 1). According to the NIH and NOS scales for quality assessment, the overall quality of the included studies was rated as good for all investigations, as shown in the supplementary data.
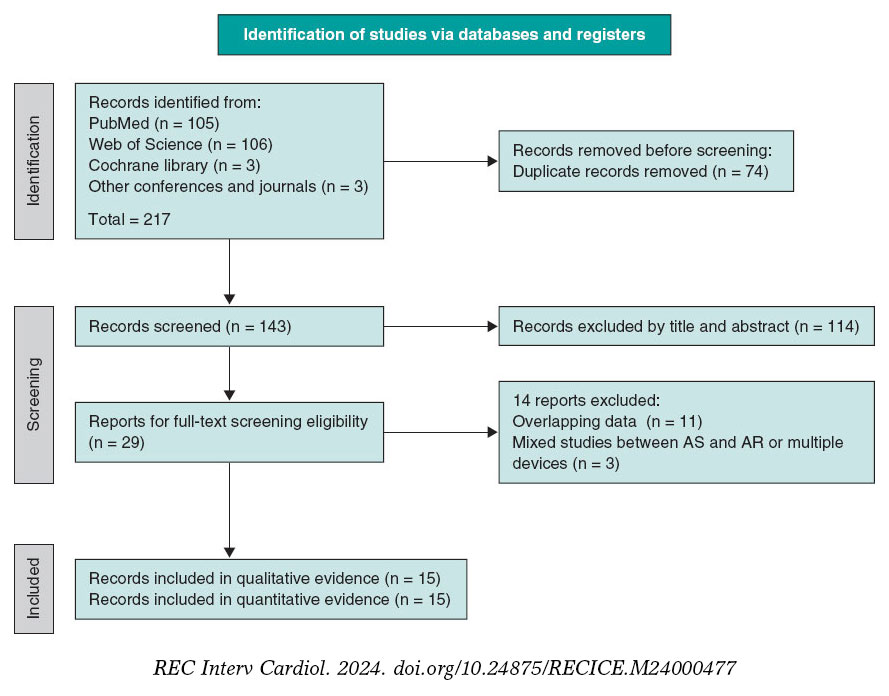
Figure 1. PRISMA flow diagram of the study.
Patient and procedural characteristics
Overall, 788 patients underwent TAVI for native pure or predominant AR (J-Valve, 357 patients; JenaValve, 431 patients). Most J-Valve procedures were performed in China, while most JenaValve procedures were conducted in Europe and North America. The average surgical risk was elevated but showed significant variability, with Log EuroSCORE at 22.8 ± 12.3, EuroSCORE II at 7.1 ± 6.6, and Society of Thoracic Surgeons - Predicted Risk of Mortality (STS-PROM) at 5.9 ± 4.7.
The mean age was 73.6 ± 7.3 years for J-Valve recipients and 75.9 ± 10.0 years for JenaValve recipients. Males comprised 61.9% of J-Valve recipients and 42.0% of JenaValve recipients. The body mass index (BMI) was 22.6 ± 3.0 for J-Valve recipients and 25.3 ± 5.7 for JenaValve recipients. The STS-PROM score was 6.7 ± 5.9 for J-Valve recipients and 4.4 ± 3.5 for JenaValve recipients. Most patients had severe symptoms, with New York Heart Association (NYHA) class III/IV dyspnea present in 75.9% of J-Valve recipients and 57.3% of JenaValve recipients. Demographic, clinical, echocardiographic, and computed tomography data from the individual studies are summarized in table 1 and table 2.
Most J-Valve implantations were performed via the transapical approach (92.4%), whereas JenaValve implantations were transapical in 36.7% of cases and transfemoral in 63.3%. The annulus diameter was 26.0 ± 2.4 mm for J-Valve and 25.6 ± 2.3 mm for JenaValve. The device size was 27.2 ± 1.9 mm for J-Valve and 26.1 ± 0.2 mm for JenaValve. The most frequently used device size was 27 mm. Further procedural data from the individual studies are summarized in table 3.
Table 1. Baseline characteristics of patients included in 15 unique studies
| Study ID | Countries | Recruitment | Device | Approach | Patient n | Male | Age | BMI (kg/m2) | EuroSCORE I | EuroSCORE II | STS-PROM | NYHA III/IV | HTN |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Garcia et al.20 2023 | USA, Canada | May 2018 - Oct 2022 | J-Valve | TFa | 27 | 16 (59) | 79.3 ± 9.6 | - | - | - | 4.1 ± 2.0 | 26 (96.3) | 24 (89) |
| Kong et al.21 2022 | China | Sept 2016 - Sept 2022 | J-Valve | TA | 69 | 52 (75.4) | 71.5 ± 7.9 | 22.70 ± 3.15 | - | - | 3.8 ± 3.9 | 53 (76.8) | 48 (69.6) |
| Liu et al.b22 2022 | China | March 2014 - June 2019 | J-Valve | TA | 161 | 119 (73.9) | 72.5 ± 6.2 | - | - | - | 9.9 ± 5.7 | 157 (98.1) | 107 (66.5) |
| Huan Liu et al.23 2020 | China | May 2014 - October 2018 | J-Valve | TA | 47 | 34 (72.3) | 73.7 ± 7.9 | 22.6 ± 2.9 | 24.3 ± 5.1 | - | 35 (74.5) | 31 (66.0) | |
| W. Liu et al.24 2019 | China | June 2017 - December 2018 | J-Valve | TA | 53 | - | 76.4 ± 5.2 | - | - | - | 6.3 ± 1.8 | - | - |
| Vahl et al.32 2024 | USA (20 sites) | June 8, 2018 - Aug 29, 2022 | JenaValve | TF | 180 | 95 (53) | 75.5 ± 10.8 | 25.3 ± 6.1 | - | - | 4.1 ± 3.4 | 122 (68) | 149 (83) |
| Adamet al.25 2023 | Germany (6 centers) | Sept 2021 - July 2022 | JenaValve | TF | 58 | 37 (63.8) | 76.5 ± 9.0 | 26.19 ± 4.36 | - | 6.10 ± 6.60 | 4.2 ± 4.3 | 43 (74) | 53 (91) |
| Baumbach et al.26 2023 | UK | - | JenaValve | TF | 12 | 7 (58) | 83.3 ± 6.7 | - | - | - | 4.6 [4.1-6.6] | 11 (92) | 8 (67) |
| Ranard et al.27 2022 | USA | July 2018 - March 2020 | JenaValve | TF | 11 | - | 77.6 ± 8.9 | - | - | - | - | - | - |
| Baldus et al.28 2019 | Germany and Netherlands (7 centers) | - | JenaValve | TF | 12 | 4 (33.3) | 75 ± 7.2 | - | - | - | 3.5 ± 2.1 | 8 (67) | - |
| Silaschi et al.29 2018 | Germany (15 center) | 2012 - 2015 | JenaValve | TA | 30 | 12 (40.0) | 74.4 ± 9.3 | - | 17.7 ± 14.8 | 6.9 ± 6.5 | 4.9 ± 3.5 | 27 (90) | 24 (80.0) |
| Sawaya et al.14 2017 | Europe, North America, and Asia Middle East (18 center) | July 2007 - Sept 2016 | JenaValvec | TA | 23/146 | - | - | - | - | - | - | - | - |
| Yoon et al.6 2017 | Europe, North America, and Asia | Sept 2007 - Feb 2017 | JenaValved | TAe | 64/212 | - | - | - | - | - | - | - | - |
| Seiffert et al.30 2014 | 9 centers, Germany | April 2012 - October 2013 | JenaValve | TA | 31 | 20 (64.5) | 73.8 ± 9.1 | 24.0 ± 4.5 | 23.6 ± 14.5 | 9.3 ± 6.4 | 5.4 ± 3.6 | 28 (90.3) | 26 (83.9) |
| Schlingloff et al.31 2014 | Hamburg, Germany | December 2012 - Sept 2013 | JenaValve | TA | 10 | 6 (60) | 79.1 ± 9.3 | - | 28.3 ± 17.1 | - | 7.0 ± 1.0 | 9 (90) | - |
| Garcia et al.20 2023 | 5 (19) | 7 (26) | 12 (44) | 4 (15) | NA | 3 (11) | 4 (15) | - | - | 4 (15) | 13 (48) | 4 (15) | |
| Kong et al.21 2022 | 9 (13.0) | 14 (20.3) | 18 (26.1) | 7 (10.1) | 5 (7.2) | 2 (2.9) | 6 (8.7) | - | 19 (27.5) | 0 | 4 (5.8) | 1(1.4) | |
| Liu et al.b22 2022 | 24 (14.9%) | 50 (31.1) | 36 (22.4)f | - | 34 (21.1) | 5 (3.1) | 51 (31.7) | 53 (32.9) | 52 (32.3) | - | 4 (2.5) | - | |
| Huan Liu et al.23 2020 | 4 (8.5) | 9 (19.1) | 9 (19.1) | 10 (21.3) | - | 1 (2.1) | 15 (31.9) | - | 11 (23.4) | 0 (0) | 2 (4.3) | 2 (4.3) | |
| W. Liu et al.24 2019 | - | - | - | - | - | - | - | - | - | - | - | - | |
| Vahl et al.32 2024 | 26 (14) | 32 (18) | 72 (40) | 21 (12) | 58 (33) | 30 (16) | 19 (11) | - | - | - | 37 (23) | 20 (12) | |
| Adamet al.25 2023 | 14 (24) | 9 (16) | 34 (59) | 7 (12) | - | 7 (12) | 8 (14) | - | 25 (43) | 5 (8.6) | 17 (29) | - | |
| Baumbach et al.26 2023 | 1 (8) | 2 (17) | 7 (58) | - | 4 (33) | - | 2 (17) | - | - | - | 2 (17) | ||
| Ranard et al27 2022 | - | - | - | - | - | - | - | - | - | - | - | - | |
| Baldus et al.28 2019 | - | - | 5 (42) | - | - | - | - | 3 (25) | - | - | 2 (17) | - | |
| Silaschi et al.29 2018 | 5 (16.7) | 5 (16.7) | 9 (30.0) | 3 (10.0) | 11 (36.7) | 4 (13.3) | 2 (6.7) | 10 (33.3) | 14 (46.7) | 1 (3.3) | 8 (26.7) | 5 (16.7) | |
| Sawaya et al.14 2017 | - | - | - | - | - | - | - | - | - | - | - | - | |
| Yoon et al.6 2017 | - | - | - | - | - | - | - | - | - | - | - | - | |
| Seiffert et al.30 2014 | 4 (12.9) | 9 (29.0) | 6 (19.3) | 6 (19.3) | - | 3 (9.7) | 6 (19.3) | 6 (20) | 20 (64.5) | 11 (35.5) | 10 (32.2) | 7 (22.6) | |
| Schlingloff et al.31 2014 | - | - | - | - | - | - | - | - | - | - | - | - | |
|
AF, atrial fibrillation; AS, aortic stenosis; BMI, body mass index; CABG, coronary artery bypass grafting; CAD, coronary artery disease; COPD, chronic (obstructive) pulmonary disease; DM, diabetes mellitus; EuroSCORE, European System for Cardiac Operative Risk Evaluation; HTN, hypertension; MI, myocardial infarction; NYHA, New York Heart Association; PVD, peripheral vascular disease; PCI, percutaneous coronary intervention; STS-PROM, Society of Thoracic Surgeons Predicted Risk Of Mortality; TA, transapical; TF, transfemoral. The data are presented as mean ± standard deviation, median [IQR], or No. (%). a F in 21. Other access: 1 carotid, 4 subclavian, 1 transcaval. b Liu et al. 22 (2022) included 29 (18.0%) patients with concomitant mild AS and 1 patient (0.6%) with bioprosthetic valve failure. c Sawaya et al. 14 (2017) included different devices; the number of JenaValve recipients was 23. d Yoon et al. 6 (2017) included different devices, but number of JenaValve patients was 64. e Yoon et al. 6 (2017) included 63 transapical implantations. f Atrial fibrillation/flutter. |
|||||||||||||
Table 2. Echocardiographic and computed tomographic data
| Study ID | LVEF (%) | LVEDD (mm) | MR, ≥ moderate | Aortic regurgitation grade | Bicuspid AV | Ascending aorta diameter | Aortic annulus diameter | Aortic annulus perimeter | |
|---|---|---|---|---|---|---|---|---|---|
| Moderate | Severe | ||||||||
| Garcia et al.20 2023 | 54 [37–60] | 55 ± 90 | - | 5 (19) | 22 (81) | 1 (4) | - | 25.6 ± 3 | 81 ± 10.5 |
| Kong et al.21 2022 | 50.8 ± 12.4 | - | - | 69 (100) | - | - | - | - | |
| Liu et al.b22 2022 | 52.3 ± 12.8 | 65.1 ± 9.3 | - | - | 161 (100) | 13 (8.1) | 41.4 ± 5.2 | 26.2 ± 2.4 | - |
| Huan Liu et al.23 2020 | 52.3 ± 12.4 | 59.2 ± 8.4 | 5 (10.6) | 0 | 47 (100) | 3 (6.4) | 40.1 ± 4.9 | 27.1 ± 2.2a | - |
| W. Liu et al.24 2019 | - | - | - | 0 | 53 (100) | - | - | - | - |
| Vahl et al.32 2024 | 53.8 ± 11.4 | - | - | 5 (3) | 116 (64) | - | 37·3 ± 5·0 | - | 79·1 ± 6·1 |
| Adamet al.25 2023 | - | - | 25 (43.1)b | 2 (3.4) | 56 (96.6)c | - | - | - | 80.3 ± 9.7 |
| Baumbach et al.26 2023 | 47 [39–56] | 60 [59–66] | - | - | 12 (100) | - | - | 27 × 24d | - |
| Ranard et al27 2022 | 44.6 ± 10.4 | 64 ± 8 | - | 11 (100) | - | - | - | - | |
| Baldus et al.28 2019 | 53.0 ± 8.5 | - | 10 (83) | - | 12 (100) | - | - | 25 ± 2.3 | - |
| Silaschi et al.29 2018 | 49.6 ± 13.3 | - | 15 (50) | 1 (3.3) | 29 (96.7) | - | - | 24.3 ± 1.9 | - |
| Sawaya et al.14 2017 | - | - | - | - | - | - | - | - | - |
| Yoon et al.6 2017 | - | - | - | - | - | - | - | - | - |
| Seiffert et al.30 2014 | 46.8 ± 16.1 | - | 8 (25.8) | 1 (3.2) | 30 (96.8) | - | 36.6 ± 7.0 | 24.7 ± 1.5 | - |
| Schlingloff et al.31 2014 | 48.2 ± 15.8 | 62 ± 2.2 | 3 (30) | - | 10 (100) | - | - | - | - |
|
AR, aortic regurgitation; Bicuspid AV, bicuspid aortic valve; LVEF, left ventricular ejection fraction; LVEDD, left ventricular end-diastolic diameter; MR, mitral regurgitation. The data are presented as mean ± standard deviation, No. (%), or median [IQR]. a Perimeter-derived diameter. b Including mild to moderate MR. c Including moderately-severe and severe AR. d Data presented as median. |
|||||||||
Table 3. Procedural characteristics
| Study ID | Device | Access | Valve prosthesis size (mm) | Average prosthesis size, mm | BPostD | ||||
|---|---|---|---|---|---|---|---|---|---|
| 21 mm | 23 mm | 25 mm | 27 mm | 29 mm | |||||
| Garcia et al.20 2023 | J-Valve | TFa | - | - | - | - | - | 26.9 ± 1.8 | 0 (0) |
| Kong et al.21 2022 | J-Valve | TA | - | - | - | - | 59 (85.9) | 29c | - |
| Liu et al.b22 2022 | J-Valve | TA | 4 (2.5) | 15 (9.3) | 35 (21.7) | 64 (39.75) | 43 (26.7) | 26.6 ± 2.0 | - |
| Huan Liu et al.23 2020 | J-Valve | TA | - | 1 (2.1) | 7 (14.9) | 26 (55.3) | 13 (27.7) | 27.2 ± 1.4 | 0 (0) |
| W. Liu et al.24 2019 | J-Valve | TA | - | - | - | - | - | - | - |
| Vahl et al.32 2024 | JenaValve | TF | - | 40 (23) | 35 (20) | 102 (58) | - | 25.7 ± 1.6 | 7 (4) |
| Adamet al.25 2023 | JenaValve | TF | - | 4 (6.9) | 16 (27.6) | 38 (65.5) | - | 26.2 ± 1.2 | 2 (3.4) |
| Baumbach et al.26 2023 | JenaValve | TF | - | - | 3 (25) | 9 (75) | - | 26.5 ± 0.9 | - |
| Ranard et al27 2022 | JenaValve | TF | - | - | - | - | - | - | - |
| Baldus et al.28 2019 | JenaValve | TF | - | 2 (16.7) | 2 (16.7) | 8 (66.7) | - | 26 ± 1.6 | 0 (0) |
| Silaschi et al.29 2018 | JenaValve | TA | - | 4 (13.3) | 11 (36.7) | 15 (50.0) | - | 25.7 ± 1.4 | 1 (3.3) |
| Sawaya et al.14 2017 | JenaValve | TA | - | - | - | - | - | - | - |
| Yoon et al.6 2017 | JenaValve | TAb | - | - | - | - | - | - | - |
| Seiffert et al.30 2014 | JenaValve | TA | - | 4 (12.9) | 7 (22.6) | 20 (64.5) | - | 26.3 ± 1.5 | 2 (6.4) |
| Schlingloff et al.31 2014 | JenaValve | TA | - | 1 (10) | 2 (20) | 7(70) | - | 26.2 ± 1.4 | - |
|
BPostD, balloon postdilatation; TA, transapical; TF, transfemoral. The data are presented as mean ± standard deviation or No. (%). a Transfemoral in 21. Other access: 1 carotid, 4 subclavian, 1 transcaval. b Transapical in 63/64. c Data presented as mean. |
|||||||||
In-hospital outcomes
Overall, in-hospital outcomes were favorable. Procedural success was achieved in 95.9% (n = 518/540). Surgical conversion was required in 1.8% (n = 12/678), device migration or embolization occurred in 3.2% (n = 17/540), and a second valve (in-valve) was required in 2.0% (n = 13/651). Only 1 patient (out of 502) experienced coronary obstruction, and no patients developed annular rupture (among 449). Details of in-hospital outcomes from the individual studies are summarized in table 4.
| Study ID | Procedural success | Conversion to surgery | Coronary obstruction | Annulus rupture | Device migration/embolization | Need for second valve | Bleeding, major or life-threatening | Vascular and access-related complications | Acute kidney injury | In-hospital mortality | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Event | Total | Event | Total | Event | Total | Event | Total | Event | Total | Event | Total | Event | Total | Event | Total | Event | Total | Event | Total | |
| Garcia et al.20 2023 | 22 (81) | 27 | 2 (7) | 27 | - | - | - | - | 3 (11.1) | 27 | 3 (11.1) | 27 | - | - | 5(18.5) | 27 | - | - | 1 (3.7) | - |
| Kong et al.21 2022 | 67 (98.5) | 68 | 1 (1.4) | 69 | - | - | - | - | 1(1.4) | 68 | - | - | 5 (7.4) | 68 | - | - | - | - | 0 (0) | 68 |
| Liu et al.b22 2022 | - | - | 4 (2.5) | 161 | 1 (0.6) | 161 | 0 (0) | 161 | 4 (2.5) | 161 | 0 (0) | 161 | 1 (0.6) | 161 | - | - | - | - | 3 (1.9) | 161 |
| Huan Liu et al.23 2020 | 46 (97.9) | 47 | 0 (0) | 47 | 0 (0) | 47 | 0 (0) | 47 | 1(2.1) | - | 1 (2.1) | 47 | 0 | 47 | 0 (0) | 47 | 8(17.0) | 47 | - | - |
| W. Liu et al.24 2019 | 51 (96.2) | 53 | 2 (3.8) | 53 | 0 (0) | 53 | - | - | 2 (3.8) | 53 | 1 (1.9) | 53 | 5 (14.3) | 53 | - | - | - | - | - | - |
| Vahl et al.32 2024 | 171 (95) | 180 | 1 (< 1) | 180 | 0 (0) | 180 | 0 (0) | 180 | 4(2.2) | 180 | 1 (< 1) | 180 | 8 (4) | 180 | 7 (4) | 180 | 2 (1) | 180 | 0 (0) | 180 |
| Adamet al.25 2023 | 58 (100) | 58 | 0 (0) | 58 | - | - | - | - | 0 (0) | 58 | 0 (0) | 58 | 0 (0) | 58 | 4 (6.9) | 58 | 7 (12) | 58 | 0 (0) | 58 |
| Baumbach et al.26 2023 | 12 (100) | 12 | - | - | - | - | - | - | - | - | - | - | 1 (8.3) | 12 | 5(41.7) | 12 | 1 (8.3) | 12 | - | - |
| Ranard et al.27 2022 | 11 (100) | 11 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Baldus et al.28 2019 | 11 (92) | 12 | 1 (8.3) | 12 | - | - | - | - | - | - | - | - | - | - | 1 (8.3) | 12 | - | - | 0 (0) | 12 |
| Silaschi et al.29.2018 | 29 (96.7) | 30 | 1 (3.7) | 27 | 0 (0) | 30 | 0 (0) | 30 | 1 (3.3) | 30 | 0 | 30 | 1 (3.3) | 30 | 1 (3.3) | 30 | 0 (0) | 30 | - | - |
| Sawaya et al.14 2017 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 2(8.7) | 23 | - | - | - | - |
| Yoon et al.6 2017 | - | - | - | - | - | - | - | - | - | - | 6 (9.4) | 64 | 5 (7.8) | 64 | 1 (1.6) | 64 | 4 (9.4) | 47 | - | - |
| Seiffert et al.30 2014 | 30 (96.8) | 31 | 0 (0) | 31 | 0 (0) | 31 | 0 (0) | 31 | 1 (3.2) | 31 | 1 (3.2) | 31 | 3 (9.7) | 31 | 4 (13) | 31 | 7 (22.5) | 31 | - | - |
| Schlingloff et al.31 2014 | 10 (100) | 10 | 0 (0) | 10 | - | - | - | - | - | - | - | - | 0 (0) | 10 | - | - | - | - | 0 (0) | 10 |
|
The data are presented as No (%). |
||||||||||||||||||||
Thirty-day outcomes
At 30 days, 95.5% of patients were alive (n = 716/750), and device success was achieved in 93.3% (n = 498/534). Mild PVR was observed in 18.0% (n = 86/478), while moderate-to-severe PVR occurred in 1.7% (n = 12/703; including 10 patients with J-Valve and 2 patients with JenaValve). PPI was required in 13.0% (n = 86/711; with 25 patients receiving J-Valve and 61 receiving JenaValve). Further 30-day outcomes from the individual studies are summarized in table 5.
| Study ID | Device success | 30-day all-cause mortality | 30-day Stroke | 30-day PPI | 30-day mild PVR | 30-day PVR ≥ moderate | 30-day EOA (cm2) | 30-day mean AVPG | 30-day repeat procedure for valve-related dysfunction | NYHA class III/ IV | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Event | Total | Event | Total | Event | Total | Event | Total | Event | Total | Event | Total | Event | Total | Event | Total | |||
| Garcia et al.20 2023 | - | - | 1 (4) | 24 | 1 (4) | 24 | 3 (13) | 24 | 8 (33) | 24 | 0 (0) | 24 | 2.1 ± 0.6 | 7 ± 4 | - | - | 3 (12) | 24 |
| Kong et al.21 2022 | - | - | 1 (1.5) | 68 | 2 (2.9) | 68 | 5 (7.5) | 67 | 19 (28) | 68 | 4 (5.9) | 68 | - | - | - | - | 7 (10) | 68 |
| Liu et al.b22 2022 | 153 (95.0) | 161 | 3 (1.9) | 161 | 1 (0.6) | 161 | 13 (8.3) | 155 | - | - | 4 (1.9) | 161 | - | 8.5 ± 2.9 | 1 (0.6) | 161 | 1 (0.6) | 161 |
| Huan Liu et al.23 2020 | - | - | 1 (2.1) | 47 | 0 (0) | 47 | 2 (4.3) | 46 | 14(30.4) | 47 | 1 (2.1) | 47 | - | 7.9 ± 2.4 | 0 (0) | 47 | 2 (4.5) | 44 |
| W. Liu et al.24 2019 | - | - | 5 (9.2) | 53 | 0 (0) | 53 | 2 (5.7) | 53 | 3 (5.6) | 53 | 1 (1.9) | 53 | - | - | - | - | - | - |
| Vahl et al.32 2024 | 174 (96.7)b | 180 | 4 (2) | 180 | 4 (2) | 180 | 36 (24) | 180a | 31 (19) | 180 | 1 (0.6) | 180 | 2.8 ± 0.6e | 3·9 ± 1·6 | - | - | 16 (9) | 180 |
| Adamet al.25 2023 | 47 (98) | 48 | 1 (1.7) | 58 | 0 (0) | 57 | 10 (19.6) | 51 | 2 (4.1) | 49 | 0 (0) | 49 | 2.65 ± 0.6c | 4.5 ± 2.0 | - | - | 4 (7.7) | 52 |
| Baumbach et al.26 2023 | - | - | 0 (0) | 12 | - | - | 2 (17) | 12 | 3 (33) | 12 | 0 | 12 | - | - | - | - | 3 (25) | 12 |
| Ranard et al.27 2022 | - | - | - | - | - | - | - | - | 0 (0) | 11 | 0 (0) | 11 | 2.7 ± 0.4 | 4.1 ± 1.7 | - | - | - | - |
| Baldus et al.28 2019 | - | - | 0 (0) | 12 | 0 (0) | 12 | 1 (8.3) | 12 | 2 (20) | 10 | 0 (0) | 10 | 2.4 ± 0.5 | 4.3 ± 1.7 | - | - | 0 (0) | 9 |
| Silaschi et al.29 2018 | 24 (88.9) | 27 | 3 (10.0) | 30 | 1 (3.3) | 30 | 1 (3.8) | 26 | 4 (15.4) | 26 | 0 (0) | 26 | - | 11.4 ± 3.7d | 1 (3.3) | 30 | 11 (41) | 27 |
| Sawaya et al.14 2017 | 18 (78.2) | 23 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Yoon et al.6 2017 | 52 (82.8) | 64 | 8 (12.5) | 64 | 5 (7.8) | 64 | 7 (15.8) | 47 | - | - | 1 (1.6) | 64 | - | - | - | - | - | - |
| Seiffert et al.30 2014 | 30 (96.8) | 31 | 4 (12.9) | 31 | 0 (0) | 31 | 2 (71.4) | 28 | - | - | - | - | - | 7.9 ± 4.0d | - | - | 4 (15.3) | 26 |
| Schlingloff et al.31 2014 | - | - | 3 (30) | 10 | - | - | 2 (20) | 10 | 0 (0) | 6 | 0 (0) | 6 | - | 7.2 ± 4.3 | - | - | 0 (0) | 10 |
|
AVPG, aortic valve pressure gradient; EOA, effective orifice area; NYHA, New York Heart Association; PPI, permanent pacemaker; PVR, prosthetic valve regurgitation. The data are presented as No. (%). a 30 patients had a previous pacemaker. b Data of device success reported in the abstract presented in TCT 2023. Makkar et al.33 2023. c Assessed at discharge. d Immediate postprocedural measurement. e Data of EOA mentioned in the abstract published in JAAC. Reference: Hamid et al.342024. |
||||||||||||||||||
Quantitative analysis of the outcomes of transfemoral TAVI for aortic regurgitation
A meta-analysis of 5 studies25-28,32 of transfemoral TAVI for AR (all with the JenaValve) included 273 patients (mean age, 77.6 years; 52.4% male). Pooled estimates were as follows: procedural success was 97.8% (95%CI, 94.4%-100%, I2 = 43%, P value = .13) (figure 2A), conversion to surgery was 0.49% (95%CI, 0.0%-1.5%, I2 = 0%, P value = .56) (figure 2B), device migration/embolization was 1.2% (95%CI, 0.0-3.3%, I2 = 47%, P value = .17) (figure 2C), and the need for a second valve was 0.46% (95%CI, 0.0%-1.44%, I2 = 0%, P value = .67) (figure 2D). Further details of in-hospital outcomes are summarized in table 6 and in the supplementary data.
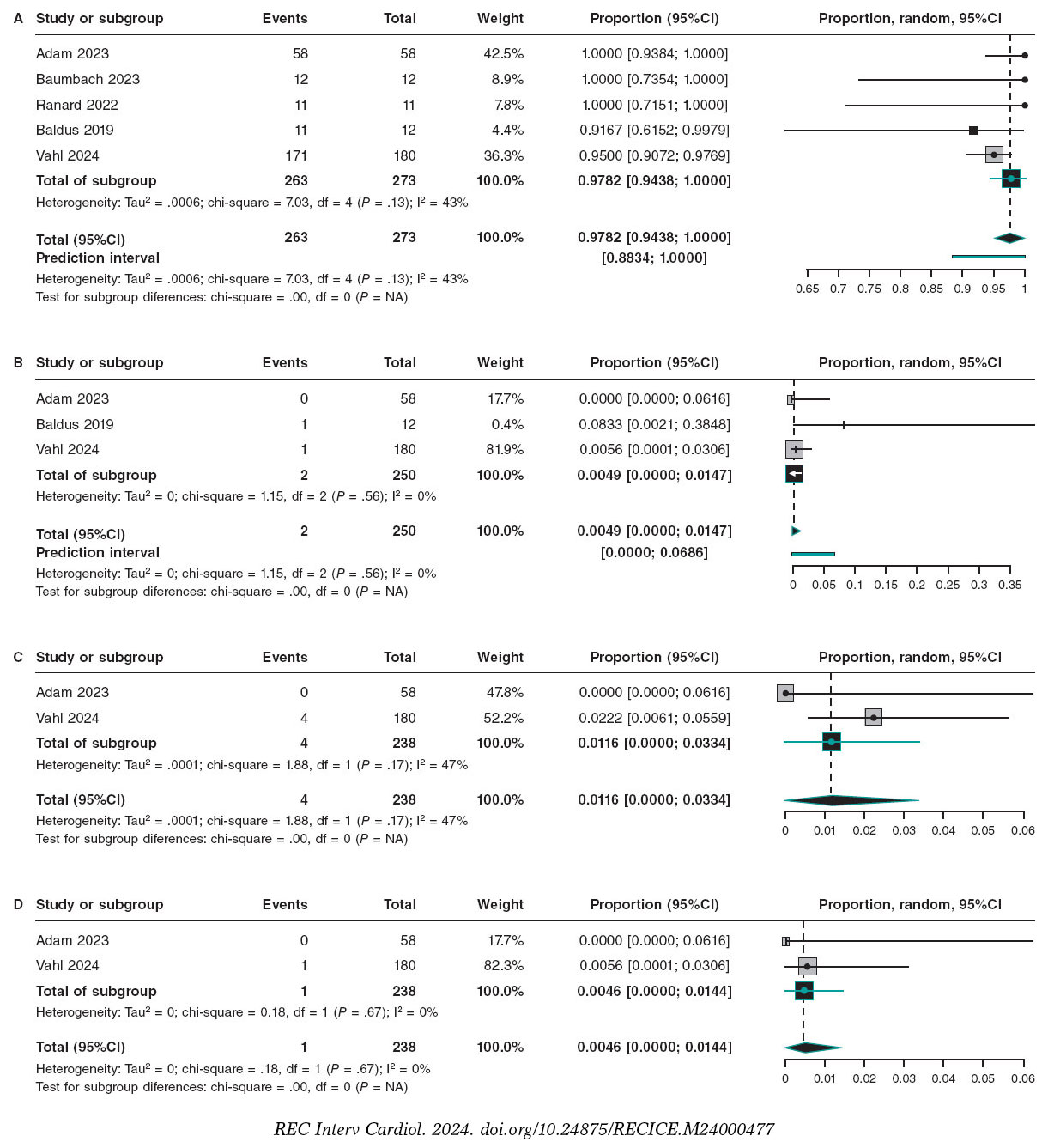
Figure 2. A. Forest plot of procedural success of TF JenaValve. The bibliographical references mentioned in this figure correspond to: Adam et al.25 2023, Baumbach et al.26 2023, Ranard et al.27 2022, Baldus et al.28 2019, Vahl et al.32 2024; B. Forest plot of conversion to surgery TF JenaValve. The bibliographical references mentioned in this figure correspond to: Adam et al.25 2023, Baldus et al.28 2019, Vahl et al.32 2024; C. Forest plot of device migration/embolization TF JenaValve. The bibliographical references mentioned in this figure correspond to: Adam et al.25 2023, Vahl et al.32 2024; D. Forest plot of need for a second valve TF JenaValve. The bibliographical references mentioned in this figure correspond to: Adam et al.25 2023, Vahl et al.32 2024. 95%CI, 95% confidence interval.
Table 6. Quantitative analysis of in-hospital outcomes of transfemoral transcatheter aortic valve implantation for aortic regurgitation
| Variables | Reporting studies (n) | Total patients (n) | Proportion with the endpoint (95%CI) | Heterogeneity |
|---|---|---|---|---|
| Procedural success | 5 | 273 | 0.9782 (0.9438-1.000) | I2 = 43%, P = .13 |
| Device success | 2 | 228 | 0.9704 (0.9484-0.9924) | I2 = 0%, P = .61 |
| Conversion to surgery | 3 | 250 | 0.0049 (0.0000-0.0147) | I2 = 0%, P = .56 |
| Device migration/ embolization | 2 | 238 | 0.0116 (0.0000-0.0334) | I2 = 47%, P = .17 |
| Need for a second Valve | 2 | 238 | 0.0046 (0.0000-0.0144) | I2 = 0%, P = .67 |
| Bleeding, major or life-threatening | 3 | 250 | 0.0249 (0.0000-0.0656) | I2 = 66%, P = .05 |
| Vascular complications | 4 | 262 | 0.0572 (0.0174-0.0969) | I2 = 61%, P = .05 |
| Acute kidney injury | 3 | 250 | 0.0592 (0.000-0.1386) | I2 = 72%, P = .03 |
| In-hospital mortality | 3 | 250 | 0.0000 (0.0000-0.0073) | I2 = 0%, P = 1.00 |
|
95%CI, 95% confidence interval. |
||||
At 30 days, the pooled estimate of device success was 97.0% (95%CI, 94.8%-99.2%, I2 = 0%, P value = .61) (figure 3A), and the pooled estimate of all-cause mortality was 2.0% (95%CI, 0.2%-3.7%, I2 = 0%, P value = .95) (figure 3B). The rate of PPI was 18.7% (95%CI, 13.9%-23.4%, I2 = 0%, P value = .58) (figure 3C). Mild PVR rate was 10.6% (95%CI, 1.7%-19.4%, I2 = 75%, P < .01) (figure 4A) with statistically significant heterogeneity resolved by omitting Vahl et al.32 yielding a rate of 4.7% (95%CI, 0.0%-9.5%, I2 = 38%) (supplementary data), while the rate of moderate-severe PVR was 0.47% (95%CI, 0.0%-1.47%, I2 = 0%, P- = 1.00) (figure 4B). Further 30-day outcomes are summarized in table 7 and in the supplementary data.
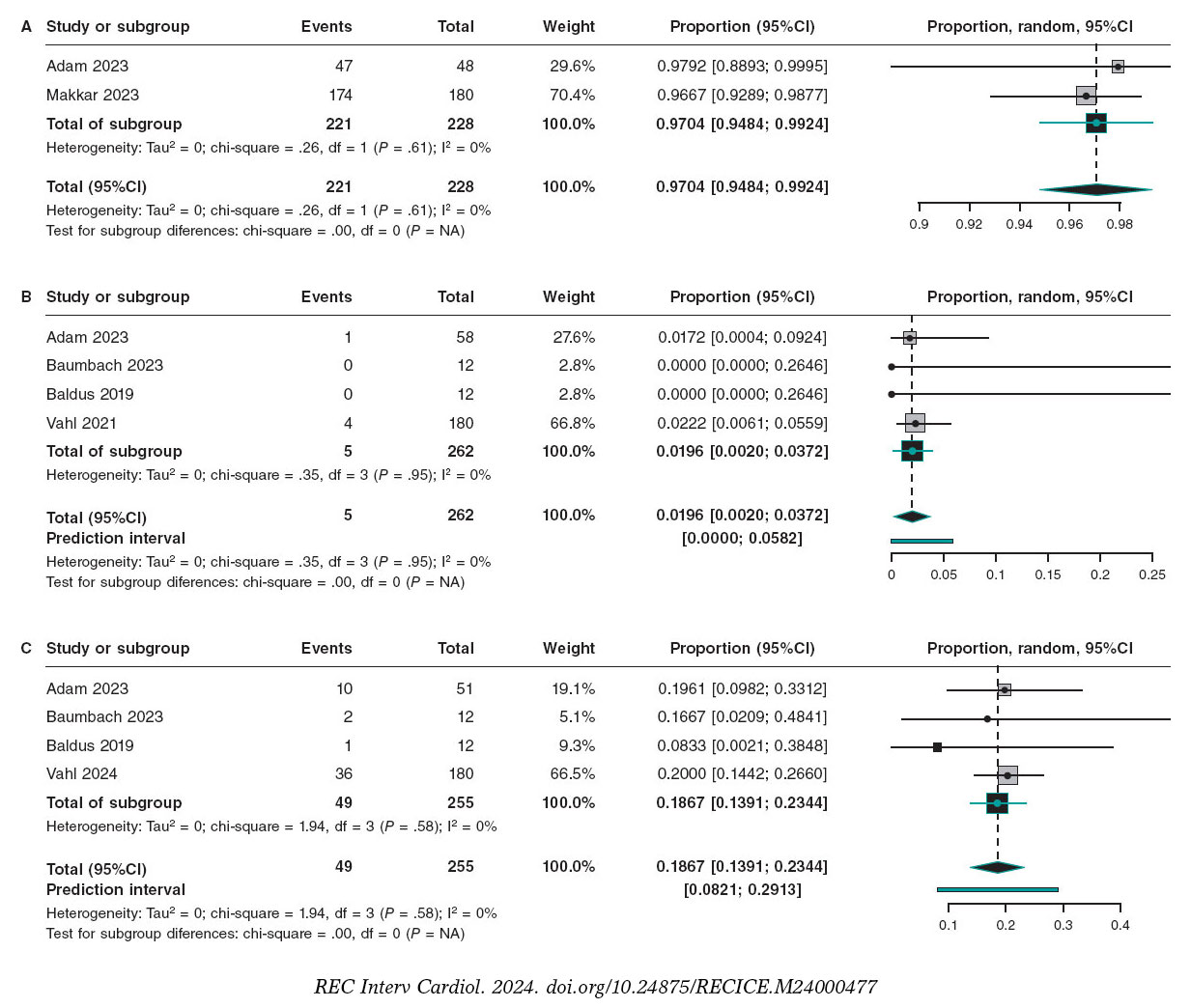
Figure 3. A. Forest plot of device success TF JenaValve. The bibliographical references mentioned in this figure correspond to: Adam et al.25 2023, Makkar et al.33 2023; B. Forest plot of 30-day all-cause mortality TF JenaValve. The bibliographical references mentioned in this figure correspond to: Adam et al.25 2023, Baumbach et al.26 2023, Baldus et al.28 2019, Vahl et al.32 2024; C. Forest plot of 30-day permanent pacemaker implantation TF JenaValve. The bibliographical references mentioned in this figure correspond to: Adam et al.25 2023, Baumbach et al.26 2023, Baldus et al.28 2019, Vahl et al.32 2024.
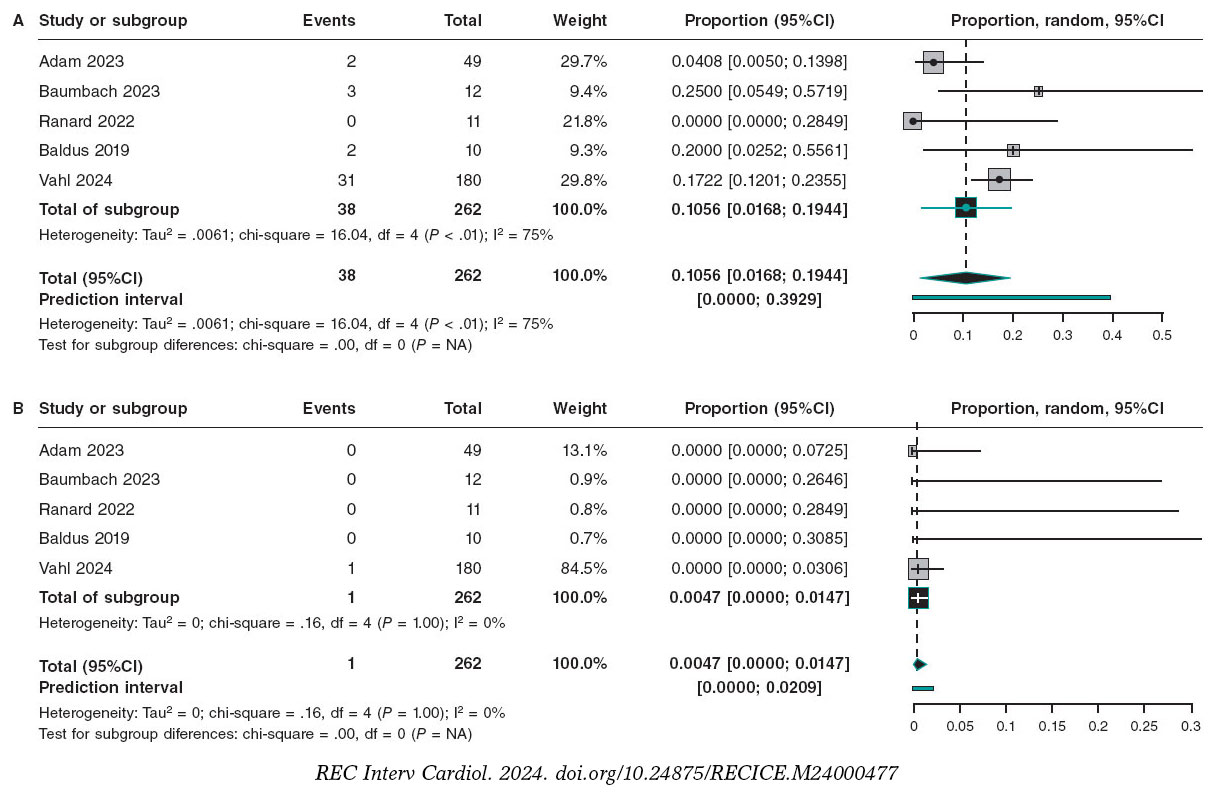
Figure 4. A. Forest plot of 30-day of mild prosthetic valve regurgitation TF JenaValve. The bibliographical references mentioned in this figure correspond to: Adam et al.25 2023, Baumbach et al.26 2023, Ranard et al.27 2022, Baldus et al.28 2019, Vahl et al.32 2024; B. Forest plot of 30-day of greater than mild prosthetic valve regurgitation TF JenaValve. The bibliographical references mentioned in this figure correspond to: Adam et al.25 2023, Baumbach et al.26 2023, Ranard et al.27 2022, Baldus et al.28 2019, Vahl et al.32 2024.
Table 7. Quantitative analysis of 30-day outcomes of transfemoral transcatheter aortic valve implantation for aortic regurgitation
| Variables | Reporting studies (n) | Total patients (n) | Proportion with the endpoint (95%CI) | Heterogeneity |
|---|---|---|---|---|
| 30-day all-cause mortality | 4 | 262 | 0.0196 (0.0020-0.0372) | I2 = 0%, P = .95 |
| 30-day stroke | 3 | 250 | 0.0112 (0.0000-0.0316) | I2= 0%, P = .38 |
| 30-day PPM implantation | 4 | 255 | 0.1867 (0.1391-0.2344) | I2 = 0%, P = .58 |
| 30-day mild PVR | 5 | 262 | 0.1056 (0.0168-0.1944) | I2 = 75%, P < .01 |
| 30-day moderate PVR | 5 | 262 | 0.0047 (0.0000-0.0147) | I2 = 0%, P = 1.00 |
|
95%CI, 95% confidence interval; PPM, permanent pacemaker; PVR, prosthetic valve regurgitation. |
||||
DISCUSSION
In this study, we included data from 788 patients who underwent TAVI using 1 of the 2 dedicated devices specifically designed for use in pure/predominant AR: the J-Valve and the JenaValve (figure 5). Studies published up to April 2024 were included, providing a contemporary and comprehensive analysis of published data in this field to date. Overall, 357 patients received the J-Valve (in 5 studies), while 431 received the JenaValve (in 10 studies). These patients were generally at increased surgical risk. J-Valve recipients were predominantly Chinese, tended to be slightly younger, had a smaller BMI, wand showed a clear male predominance compared with JenaValve recipients.
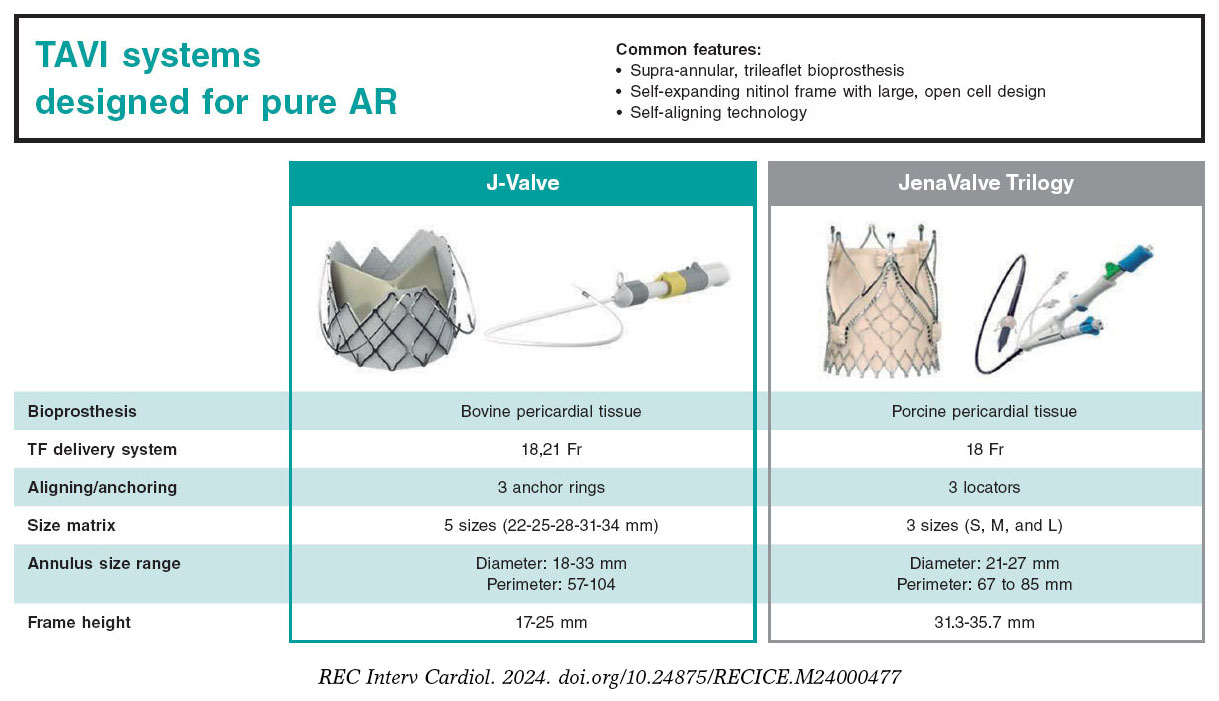
Figure 5. Central illustration. Features of the contemporary generations of 2 TAVI systems dedicated to aortic regurgitation.
The use of the 2 technologies (J-Valve and JenaValve) was influenced by their geographical availability, leading to differences between the populations treated with each device. Moreover, as mentioned earlier, the 2 groups differed in age, sex, and STS-PROM scores. Additionally, most of the transfemoral implantations involved the JenaValve, while the vast majority of J-Valve implantations were transapical. Consequently, direct statistical comparison between the 2 devices and the 2 access routes was deemed inappropriate. For similar reasons, we avoided pooling data from all JenaValve procedures (mixing transapical and transfemoral implantations) and from all transapical procedures (mixing J-Valves and JenaValves). This approach minimized the risk of drawing invalid conclusions by mixing heterogeneous data or comparing outcomes without accounting for important independent confounders. Patients receiving the JenaValve via the transfemoral approach constituted a homogeneous subgroup, allowing for pooled/quantitative analysis. The findings of this latter analysis are particularly important, as transfemoral access currently dominates the TAVI field.
Our systematic review combines prospective and retrospective studies, which share common limitations such as small sample sizes and nonrandomized designs. Therefore, the findings should be regarded as preliminary and require validation in larger randomized studies. From the available data, our major observations can be summarized as follows: first, TAVI using AR-dedicated devices demonstrated a high success rate with a reassuring early safety profile. Second, the rates of surgical conversion, device dislocation, and second valve implantation were low (2%-3%). Third, both dedicated devices effectively eliminated or reduced AR, with only 1% to 2% of patients having ≥ moderate residual AR. Fourth, the results of transfemoral TAVI for AR using the JenaValve were particularly encouraging, although the PPI rate was still relatively high. Taken together, these initial findings suggest that transcatheter treatment of AR, especially through transfemoral access, may be a safe and effective alternative to surgery in appropriately selected patients.
Treating AR with TAVI using the first/older generations of transcatheter heart valves has been associated with suboptimal results.35,36 However, subsequent studies showed that next/newer generation transcatheter heart valves can improve outcomes, bringing them closer to those achieved in patients with AS.13 With the introduction of dedicated devices, several key outcomes have shown further improvement, yielding very high procedural and device success rates and low rates of conversion to surgery, device migration or embolization, the need for a second valve, and PVR. Although annular injury is a concern given the frequent association of AR with aortopathy, no cases of annular rupture were reported with the 2 self-expanding dedicated devices. We also observed low rates of acute kidney injury, bleeding, vascular complications, and in-hospital mortality. Whether this low rate of early complications will translate into improved long-term clinical outcomes remains to be determined and should be explored in longitudinal prospective studies.
A major challenge associated with TAVI for native pure/predominant AR is the risk of device migration/embolization and paravalvular leakage. This risk arises from the absence of calcification in the landing zone, the large size of the aortic annulus, and the high stroke volume in AR patients. The design of the 2 AR-dedicated TAVI devices aims is to mitigate this risk (figure 5).
The JenaValve device features an natomically-oriented design with ‘supporting arms’ that can be positioned in the sinuses of the aortic root, ensuring precise placement of the valve stent. Additionally, the fixation of the oriented device to the native valve leaflet through clip attachment provides an extra axial expansion force, enabling secure fixation even in the absence of leaflet calcifications.37
The J-Valve device is characterized by its U-shaped grasper that captures the aortic valve leaflets, achieving ‘axial’ fixation, which complements the ‘radial’ fixation, which is less reliable in the absence of calcification. Furthermore, the dual-phase release mechanism of this device (the graspers are initially released, followed by the valve) can aid in precise placement of the graspers prior to valve deployment and decrease the likelihood of damage to the native valve.38
Our data suggest that these innovative designs are associated with very low rates of device dislocation and paravalvular leakage, which in turn results in low rates of second valve requirement and surgical conversion. Importantly, these benefits did not come at the expense of increased risk of annular injury or coronary obstruction. However, a relatively high rate of PPI was observed with JenaValve, reaching nearly 19% in 5 studies of its updated transfemoral version. This may reflect a tendency for a relatively deeper implantation, a common issue with early experience of nearly all TAVI systems that tends to improve over time and typically portends a decline in PPI rates.39-42
While the current review includes preliminary single-arm, observational, small-scale studies, several randomized trials are have been conducted on J-Valve and JenaValve.43-47 While the results of these trials are pending, our data suggest a positive outcome.
In the currently available data, there is a dominance of transapical access procedures among J-Valve implantations. However, with the trend toward more minimalistic TAVI procedures, the transapical approach may only be a precursor, with the transfemoral approach expected to eventually become the standard, as already observed with the JenaValve. The most recent data, presented in 2023, on transfemoral J-Valve procedures (from the compassionate use experience in North America) is particularly reassuring.20
Study limitations
The scope of our investigation was restricted to observational studies, abstracts, and conference presentations;, none of which were randomized controlled trials. This inherently limits the quality of the evidence produced. Additionally, the present findings may have been influenced by publication bias favoring TAVI for native pure or predominant AR, which was mitigated by our. However, we sought to mitigate this bias through an exhaustive review of the available literature and the meticulous exclusion of overlapping or duplicate data. The total patient population remained relatively small, and follow-up was restricted to 30-day outcomes, so the findings should be interpreted with these limitations in mind.
CONCLUSIONS
This systematic review provides a comprehensive and up-to-date analysis of data on TAVI with dedicated devices for native pure/predominant AR. The initial experience discussed in the present review demonstrates the safety and favorable early outcomes of TAVI using J-Valve and JenaValve in patients with pure/predominant AR, especially when the transfemoral approach is used. Nevertheless, PPI requirement remains frequent.
FUNDING
None.
ETHICAL CONSIDERATIONS
The present article is a literature review and, as such, ethics approval was not required. The study did not involve patient recruitment or access to disaggregated information on individuals and therefore informed consent was not required. Possible sex/gender biases have been taken into account in the preparation of this article.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence was used in the preparation of this article.
AUTHORS’ CONTRIBUTIONS
A. Hassan, M. Abdelshafy, and R.A. Diab performed the literature review, data analysis, and initial manuscript drafting. H. Wienemann, M. Adam, S. García, and M. Saad critically reviewed the manuscript. M. Abdelghani conceived the idea, designed and supervised data collection and analysis, and finalized the manuscript.
CONFLICTS OF INTEREST
M. Adam reports personal fees and speaker honoraria from Abbott, Boston Scientific, Edwards Lifesciences, JenaValve, and Medtronic. S. Garcia reports institutional grants from J.C. Medical and JenaValve. All other authors have no conflict of interest to report.
WHAT IS KNOWN ABOUT THE TOPIC?
- The off-label use of the next-generation nondedicated TAVI devices to treat pure AR is associated with an increased risk of device embolization and PVR.
WHAT DOES THIS STUDY ADD?
- TAVI for AR with devices specifically designed for this indication (J-Valve and JenaValve) shows favorable early safety and efficacy, especially when the transfemoral approach is used. Nevertheless, the need for PPI remains frequent.
SUPPLEMENTARY DATA

REFERENCES
1. Flint N, Wunderlich NC, Shmueli H, Ben-Zekry S, Siegel RJ, Beigel R. Aortic Regurgitation. Curr Cardiol Rep. 2019;21:65.
2. Maurer G. Aortic regurgitation. Heart. 2006;92:994-1000.
3. Singh JP, Evans JC, Levy D, et al. Prevalence and clinical determinants of mitral, tricuspid, and aortic regurgitation (the Framingham Heart Study). Am J Cardiol. 1999;83:897-902.
4. Dujardin KS, Enriquez-Sarano M, Schaff HV, Bailey KR, Seward JB, Tajik AJ. Mortality and morbidity of aortic regurgitation in clinical practice. A long-term follow-up study. Circulation. 1999;99:1851-1857.
5. Bonow RO, Carabello BA, Chatterjee K, et al. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease:a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease):endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. 2008;118:523-661.
6. Yoon S-H, Schmidt T, Bleiziffer S, et al. Transcatheter Aortic Valve Replacement in Pure Native Aortic Valve Regurgitation. J Am Coll Cardiol. 2017;70:2752-2763.
7. Adams DH, Popma JJ, Reardon MJ, et al. Transcatheter aortic-valve replacement with a self-expanding prosthesis.N Engl J Med. 2014;370:1790-1798.
8. Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187-2198.
9. Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597-1607.
10. Reardon MJ, Van Mieghem NM, Popma JJ, et al. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2017;376:1321-1331.
11. Leon MB, Smith CR, Mack MJ, et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2016;374:1609-1620.
12. Dvir D, Webb JG, Bleiziffer S, et al. Transcatheter aortic valve implantation in failed bioprosthetic surgical valves. JAMA. 2014;312:162-170.
13. Yoon S-H, Bleiziffer S, De Backer O, et al. Outcomes in transcatheter aortic valve replacement for bicuspid versus tricuspid aortic valve stenosis. J Am Coll Cardiol. 2017;69:2579-2589.
14. Sawaya FJ, Deutsch M-A, Seiffert M, et al. Safety and efficacy of transcatheter aortic valve replacement in the treatment of pure aortic regurgitation in native valves and failing surgical bioprostheses:results from an international registry study. JACC Cardiovasc Interv. 2017;10:1048-1056.
15. Zhu D, Chen Y, Zhang J, Hu J, Guo Y. Transapical implantation of a new second-generation transcatheter heart valve in patients with pure aortic regurgitation:a preliminary report. Interact Cardiovasc Thorac Surg. 2015;20:860-862.
16. Treede H, Rastan A, Ferrari M, Ensminger S, Figulla H-R, Mohr F-W. JenaValve. EuroIntervention. 2012;8 Suppl Q:Q88-93.
17. Page M, McKenzie J, Bossuyt P, et al. The PRISMA 2020 statement:an updated guideline for reporting systematic reviews. BMJ. 2021;372:71.
18. Cochrane Handbook for Systematic Reviews of Interventions(5.1.0). Available at: https://handbook-5-1.cochrane.org. Accessed 19 July 2024.
19. Systematic review screening tool/software. Available at: https://www.rayyan.ai/. Accessed 19 July 2024.
20. Garcia S, Ye J, Webb J, et al. Transcatheter treatment of native aortic valve regurgitation:the north american experience with a novel device. JACC Cardiovasc Interv. 2023;16:1953-1960.
21. Kong M, Hong Z, Liu X, Zhu X, Wang J, Dong A. 30-Day Outcomes after Surgical or Transapical Aortic Valve Replacement in Symptomatic Aortic Regurgitation. J Cardiovasc Dev Dis. 2022;9:224.
22. Liu L, Peng Y, Shi J, Qian H, Guo Y. Initial experience with repositionable J-Valve for severe aortic regurgitation:a single-center experience. J Cardiovasc Surg (Torino). 2022;63:521-528.
23. Liu H, Liu S, Lu Y, et al. Transapical transcatheter aortic valve implantation for predominant aortic regurgitation with a self-expandable valve. J Thorac Dis. 2020;12:538-549.
24. Liu W, Zhou YJ, Zhang HB, Meng XU, Gao YN. P1852The clinical experience of J valve transapical transcatheter aortic valve replacement system in high-risk patients with severe pure aortic regurgitation. Eur Heart J. 2019;40(Supplement_1):ehz748.0603.
25. Adam M, Tamm AR, Wienemann H, et al. Transcatheter Aortic Valve Replacement for Isolated Aortic Regurgitation Using a New Self-Expanding TAVR System. JACC Cardiovasc Interv. 2023;16:1965-1973.
26. Baumbach A, Patel KP, Kennon S, et al. A heart valve dedicated for aortic regurgitation:Review of technology and early clinical experience with the transfemoral Trilogy system. Catheter Cardiovasc Interv. 2023;102:766-771.
27. Ranard LS, Gogia S, Hamid N, et al. Left ventricular remodeling after jenavalve trilogy transcatheter aortic valve replacement in patients with pure aortic regurgitation. J Am Coll Cardiol. 2022;79:647.
28. Baldus S, Treede H, Kempfert J, Kim WK, Rudolph T and Bleiziffer S, Mieghem NV. A Feasibility Study to Assess Safety and Effectiveness of the JenaValve Transfemoral TAVR System in the Treatment of Patients With Severe Aortic Regurgitation. Euro PCR 2019. Paris, France.
29. Silaschi M, Conradi L, Wendler O, S et al. The JUPITER registry:One-year outcomes of transapical aortic valve implantation using a second generation transcatheter heart valve for aortic regurgitation. Catheter Cardiovasc Interv. 2018;91:1345-1351.
30. Seiffert M, Bader R, Kappert U, et al. Initial German experience with transapical implantation of a second-generation transcatheter heart valve for the treatment of aortic regurgitation. JACC Cardiovasc Interv. 2014;7:1168-1174.
31. Schlingloff F, Schäfer U, Frerker C, Schmoeckel M, Bader R. Transcatheter aortic valve implantation of a second-generation valve for pure aortic regurgitation:procedural outcome, haemodynamic data and follow-up. Interact Cardiovasc Thorac Surg. 2014;19:388-393.
32. Vahl TP, Thourani VH, Makkar RR, et al. Transcatheter aortic valve implantation in patients with high-risk symptomatic native aortic regurgitation (ALIGN-AR):a prospective, multicentre, single-arm study. Lancet. 2024;403:1451-1459.
33. Makkar R. Valve Hemodynamics and Device Performance:A New Era in Safety and Technical Success for TAVR in AR [video]. TCT 2023. Available at: https://www.crfconnect.com/episode/valve-hemodynamics-and-device-performance-a-new-era-in-safety-and-technical-success-for-tavr-in-ar-1700.
34. Hamid, N, Vahl, T, Thourani, V. al. Hemodynamic performance of the JenaValve Trilogy™system from the ALIGN-AR trial - the first dedicated transcatheter aortic valve for aortic regurgitation. J Am Coll Cardiol. 2024;83(Suppl 13):803.
35. Ullah W, Suleiman A-RM, Osman H, et al. Trends and outcomes of transcatheter aortic valve implantation in aortic insufficiency:A nationwide readmission database analysis. Curr Probl Cardiol. 202449(1 Pt A):102012.
36. Haddad A, Arwani R, Altayar O, Sawas T, Murad MH, de Marchena E. Transcatheter aortic valve replacement in patients with pure native aortic valve regurgitation:A systematic review and meta-analysis. Clin Cardiol. 2019;42:159-166.
37. Seiffert M, Diemert P, Koschyk D, et al. Transapical implantation of a second-generation transcatheter heart valve in patients with noncalcified aortic regurgitation. JACC Cardiovasc Interv. 2013;6:590-597.
38. Zhu D, Hu J, Meng W, Guo Y. Successful transcatheter aortic valve implantation for pure aortic regurgitation using a new second generation self-expanding J-Valve(TM) system - the first in-man implantation. Heart Lung Circ. 2015;24:411-414.
39. Sammour Y, Banerjee K, Kumar A, et al. Systematic Approach to High Implantation of SAPIEN-3 Valve Achieves a Lower Rate of Conduction Abnormalities Including Pacemaker Implantation. Circ Cardiovasc Interv. 2021;14:009407.
40. Eliav R, Elitzur Y, Planer D, et al. Predictors for permanent pacemaker implantation following transcatheter aortic valve implantation:trends over the past decade. J Interv Card Electrophysiol. 2021;62:299-307.
41. Vora AN, Gada H, Manandhar P, et al. National variability in pacemaker implantation rate following TAVR:insights from the STS/ACC TVT registry. JACC Cardiovasc Interv. 2024;17:391-401.
42. Mauri V, Abdel-Wahab M, Bleiziffer S, et al. Temporal trends of TAVI treatment characteristics in high volume centers in Germany 2013-2020. Clin Res Cardiol. 2022;111:881-888.
43. J-Valve Compassionate Use. Available at: https://clinicaltrials.gov/study/NCT03876964. Accessed 15 July 2024.
44. Clinical Trial in China. Available at: https://clinicaltrials.gov/study/NCT05580952?tab=results. Accessed 15 July 2024.
45. Safety &Efficacy of the J-Valve Ausper System in Patients With Severe Aortic Stenosis and/or Aortic Regurgitation. Available at: https://clinicaltrials.gov/study/NCT03025971. Accessed 15 July 2024.
46. THE ALIGN-AR EFS TRIAL:JenaValve Pericardial TAVR Aortic Regurgitation Study. Available at: https://clinicaltrials.gov/study/NCT02732704. Accessed 15 July 2024.
47. JUPITER Study:Transapical Aortic Valve Implantation for Aortic Regurgitation (JUPITER). Available at: https://clinicaltrials.gov/study/NCT01598844. Accessed 15 July 2024.










