
Article
Ischemic heart disease and acute cardiac care
REC Interv Cardiol. 2019;1:21-25
Access to side branches with a sharply angulated origin: usefulness of a specific wire for chronic occlusions
Acceso a ramas laterales con origen muy angulado: utilidad de una guía específica de oclusión crónica
Servicio de Cardiología, Hospital de Cabueñes, Gijón, Asturias, España
ABSTRACT
Introduction and objectives: In elderly and frail patients, there is limited evidence on the therapeutic management of left main coronary artery (LM) disease. The objective of this study was to evaluate mid-term clinical outcomes in older adults undergoing percutaneous coronary intervention (PCI) of LM.
Methods: We conducted a retrospective study including all older patients (≥ 75 years) undergoing LM-PCI at a high-volume center between 2017 and 2021. The primary endpoint was a composite of major adverse cardiovascular events (MACE). Patients were grouped according to the presence of frailty based on the FRAIL scale. Inverse probability of treatment weighting was used to account for clinical differences between the 2 groups.
Results: A total of 140 patients were included in the study (median age 80 [78-84]; 36% women). Of them, 49% met the criteria for frailty. After a median follow-up of 19 [5-35] months, 40 MACE (29%) were recorded. The all-cause death rate was 32%. There were no differences in the risk of MACE between frailty groups, but patients with frailty had an increased risk of all-cause mortality (HRadj, 1.95 [1.02-3.75]; P = .046).
Conclusions: LM-PCI in older adults with multiple associated comorbidities could be considered a feasible option in this special population. The rate of MACE at follow-up was acceptable. Frailty was associated with a worse prognosis in terms of all-cause mortality at follow-up.
Keywords: Coronary artery disease. Left main coronary artery. Percutaneous coronary intervention. Elderly. Frailty.
RESUMEN
Introducción y objetivos: La evidencia sobre el abordaje terapéutico de la enfermedad del tronco coronario izquierdo (TCI) en pacientes ancianos y frágiles es limitada. El objetivo de este estudio fue evaluar los resultados clínicos a medio plazo en ancianos que recibieron una intervención coronaria percutánea (ICP) del TCI.
Métodos: Estudio retrospectivo en el que se incluyeron todos los pacientes ancianos (≥ 75 años) tratados con ICP del TCI en un centro de alto volumen entre 2017 y 2021. El objetivo principal fue un compuesto de eventos adversos cardiovasculares mayores (MACE). Los pacientes fueron agrupados en función de su fragilidad según la escala FRAIL. Se utilizó la ponderación de probabilidad inversa de tratamiento para tener en cuenta las diferencias clínicas entre los 2 grupos.
Resultados: Se incluyeron 140 pacientes (mediana de edad: 80 años [78-84]; 36% mujeres), de los cuales el 49% cumplían los criterios de fragilidad. Tras una mediana de seguimiento de 19 meses (5-35) se registraron 40 MACE (29%). La tasa de mortalidad por todas las causas fue del 32%. No se observaron diferencias en el riesgo de MACE entre los grupos, aunque los pacientes frágiles presentaron una mayor mortalidad por todas las causas (HRa = 1,95 [1,02-3,75]; p = 0,046).
Conclusiones: La ICP del TCI en pacientes ancianos con comorbilidad podría considerarse una opción factible en esta población especial. La tasa de MACE en el seguimiento resulta aceptable. La fragilidad se asoció con un peor pronóstico en términos de mortalidad por todas las causas durante el seguimiento.
Palabras clave: Enfermedad arterial coronaria. Tronco coronario izquierdo. Intervención coronaria percutánea. Paciente anciano. Fragilidad.
Abbreviations
CABG: coronary artery bypass grafting. LM: left main coronary artery. PCI: percutaneous coronary intervention.
INTRODUCTION
The left main coronary artery (LM) supplies 84% of the blood flow to the left ventricle in patients with right dominance,1 making LM disease the coronary lesion with the worst prognosis. The prevalence of this disease is not negligible, as it is found in 4.8% of coronary angiograms,2 highlighting the prognostic importance of these lesions. Conservative treatment is a rarely a feasible option due to the high rate of cardiac adverse events during short-term follow-up, with a mortality rate exceeding 50%.3
Coronary artery bypass grafting (CABG) has traditionally been the most widely accepted revascularization strategy.4 In recent years, there have been significant pharmacological and technological improvements in percutaneous revascularization techniques, such as drug-eluting stents and intracoronary diagnostic techniques.5 These improvements, together with comparative studies, have prompted discussion on the various alternatives.6 Presently, the choice of revascularization strategy should be based on the complexity of the coronary anatomy and surgical risk.7
However, evidence is limited in older adults who are scarcely represented in classic studies. Furthermore, in these patients, frailty is a frequent and unstudied characteristic that can influence their prognosis. In this special population, CABG is usually ruled out due to high-surgical risk. On the other hand, percutaneous coronary intervention (PCI) could be a potential therapeutic option, although with little evidence to date.8 Consequently, we postulated that PCI of the LM might be feasible and safe in older patients, with a low incidence of associated complications and an acceptable rate of major adverse cardiac events (MACE) during follow-up.
METHODS
Study design
We conducted a retrospective, single-center study of older patients diagnosed with LM disease who underwent PCI. The study aimed to evaluate mid-term clinical outcomes and examine the prognostic significance of frailty in these patients. The study protocol was approved by the local clinical research ethics committee according to institutional and good clinical practice guidelines. Recruitment took place from January 2017 to December 2021 at Hospital Universitario Reina Sofía (Cordoba, Spain). Patients were eligible if they were aged ≥ 75 years at the time of LM disease diagnosis, and PCI was chosen as the treatment after deliberation by heart team discussion, or due to instability requiring emergent revascularization. Exclusion criteria consisted of end-stage chronic diseases, patients under palliative care, contraindications to dual antiplatelet therapy, and incomplete follow-up data. Included patients were grouped according to frailty status, determined by the FRAIL scale, with patients scoring 3 or more points considered frail.9 Definitions are shown in the supplementary data.
Outcomes
The main objective of the study was to describe mid-term clinical outcomes in older patients undergoing LM-PCI. We also aimed to compare clinical events according to the presence of frailty. The primary endpoint was a composite of MACE, defined as a composite of cardiovascular death (including death of uncertain cause), nonfatal myocardial infarction, the need for new revascularization, and stroke. Secondary outcomes were the individual components of MACE and all-cause mortality.
Angiographic analysis
Quantitative analysis of the coronary arteries was performed using the validated CAAS system (Pie Medica Imaging, the Netherlands). The basal anatomy of the LM bifurcation with the anterior descending artery and the circumflex artery was classified according to the Medina classification.10 The measurements analyzed included the reference diameter of the LM and its percentage of stenosis. The complexity of the coronary anatomy was studied using the SYNTAX scale.6
Statistical analysis
Categorical data are presented as counts (percentages), while continuous data are expressed as mean ± standard deviation or median [interquartile range]. Between-group comparisons were performed using the chi-square test or the Fisher exact test for categorical variables and the Student t-test or the Mann-Whitney U test for continuous variables. Kaplan-Meier curves and Cox regression models were used to analyze clinical events according to frailty. Inverse probability of treatment weighting (IPTW) was used to account for clinical differences between the 2 groups.11 Propensity scores were calculated using a logistic regression model that included the following covariates: age, sex, left ventricular ejection fraction, atrial fibrillation, chronic kidney disease, anemia, and chronic obstructive pulmonary disease. Standardized mean differences before and after weighting were used to evaluate the balance of the groups regarding the covariates. A difference of < 10% was considered to indicate a satisfactory balance. The distributions of the propensity scores before and after weighting were plotted to assess the degree of overlap between the 2 groups. Confidence intervals for the IPTW coefficients were obtained using robust sandwich-type variance estimators (figure 1 of the supplementary data).12 All tests were 2-tailed and significance was set at P < .05. Statistical analyses were performed using SPSS software (V 24; IBM Corp., United States) and R software (V4.0.3; R Foundation for Statistical Computing, Austria).
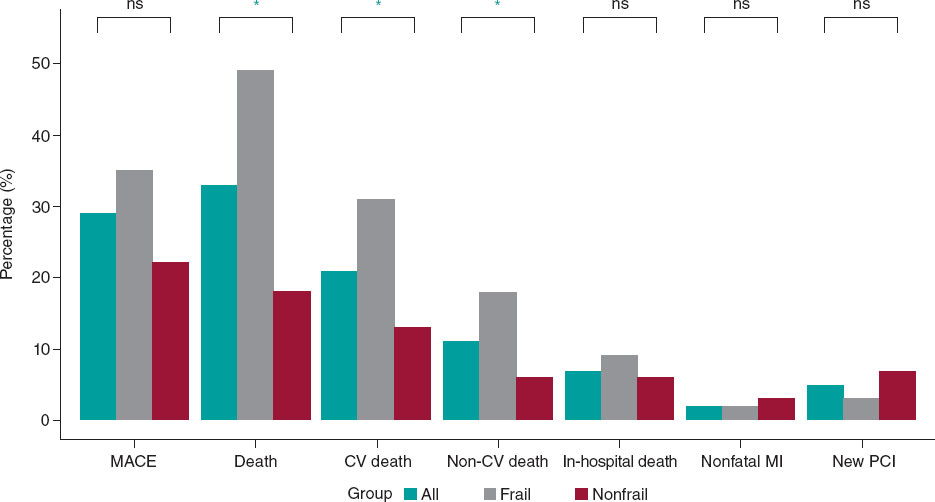
Figure 1. Main events to follow-up. CV, cardiovascular; MACE, mayor adverse cardiovascular events; MI, myocardial infarction; NS, nonsignificant; PCI, percutaneous coronary intervention. * P < .005.
RESULTS
During the study period, our hospital treated 437 patients with significant LM lesions percutaneously. Of them, a total of 140 patients met the inclusion criteria and were included in the analysis (figure 2 of the supplementary data).
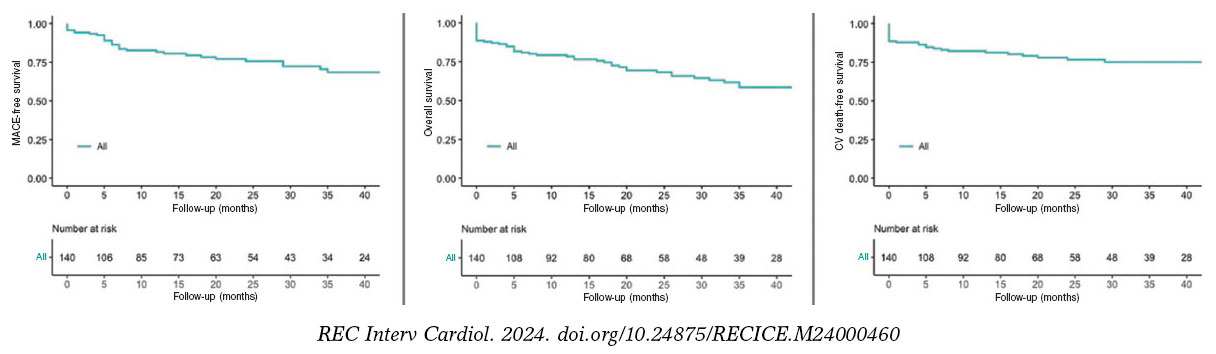
Figure 2. Kaplan-Meier Curves of the primary outcome and mortality. CV, cardiovascular; MACE, major adverse cardiovascular events.
Baseline characteristics
The baseline clinical characteristics, clinical presentation and antithrombotic treatment administered are detailed in table 1. The median age of the patients was 80 [78-84] years and 36% (51 patients) were women. Most of the patients had a history of hypertension (84%, 118 patients) and 58% (81 patients) were diabetic. More than a third of the patient cohort had a previous personal history of ischemic heart disease (37%, 52 patients) and 33% (46 patients) had chronic kidney disease. Among noncardiovascular comorbidities, active cancer was present in 11 patients (8%) and prior blood transfusions had been required in 16 patients (11%). The mean EuroSCORE II was 3.07 [1.96-5.7] to assess surgical risk. Forty-eight patients (34%) had left ventricular systolic dysfunction at the time of revascularization.
Table 1. Patients’ baseline characteristics
| Characteristics | Total n = 140 | Nonfrail n = 72 (51) | Frail n = 68 (49) | P |
|---|---|---|---|---|
| Baseline clinical characteristics | ||||
| Age, years | 80 [78-84] | 80 [77-84] | 80 [78-84] | .090 |
| Female sex | 51 (36) | 18 (25) | 33 (49) | .004 |
| Hypertension | 118 (84) | 61 (85) | 57 (84) | .884 |
| Diabetes | 81 (58) | 36 (50) | 45 (66) | .053 |
| Hypercholesterolemia | 112 (80) | 56 (78) | 56 (82) | .999 |
| Smoking history | 7 (5) | 5 (7) | 2 (3) | .442 |
| Previous ischemic heart disease | 52 (37) | 31 (43) | 21 (31) | .136 |
| Chronic kidney disease | 46 (33) | 22 (33) | 24 (39) | .481 |
| Atrial fibrillation | 22 (16) | 7 (10) | 15 (22) | .041 |
| Peripheral artery disease | 20 (14) | 14 (20) | 6 (9) | .073 |
| COPD | 17 (12) | 6 (8) | 11 (16) | .156 |
| Previous stroke | 16 (11) | 10 (14) | 6 (9) | .073 |
| Valve disease | 15 (11) | 7 (7) | 10 (15) | .114 |
| Anemia | 29 (21) | 10 (14) | 19 (28) | .040 |
| Active cancer | 11 (8) | 7 (10) | 4 (6) | .399 |
| Liver disease | 4 (3) | 3 (4) | 1 (2) | .339 |
| Previous blood transfusions | 16 (11) | 5 (7) | 11 (16) | .086 |
| Recent surgery or trauma | 38 (27) | 19 (26) | 19 (28) | .836 |
| EuroScore II | 3.07 [1.96-5.7] | 2.76 [1.83-4.18] | 3.80 [2.04-7.85] | .010 |
| Glomerular filtration rate (mL/min) | 71.4 [48.4-87.3] | 76.71 [51.01-87.51] | 61.40 [41.40-81.85] | .072 |
| Creatinine (mg/dL) | 1.02 [0.87-1.30] | 1.00 [0.80-1.85] | 1.03 [0.90-1.50] | .109 |
| Hemoglobin (mg/dL) (mean, ±SD) | 12.6 (± 2) | 13.02 (± 2) | 12.16 (± 1.9) | .017 |
| Hematocrit | 38.6 [34.6-43.0] | 39.6 [36.0-44.7] | 36.6 [33.9-42.1] | .031 |
| Platelets (× 109/L) | 208 [171-246] | 211 [182-244] | 196 [160-250] | .340 |
| Hs-cTnI (ng/L) | 954 [40-7352] | 2250 [30-10 000] | 650 [40-5600] | .245 |
| LVEF | 60 [39-67] | 60 [45-68] | 58 [35-63] | .245 |
| LV systolic dysfunction | 48 (34) | 20 (32) | 28 (46) | .106 |
| Clinical presentation | ||||
| Acute coronary syndrome | 85 (61) | 45 (63) | 40 (59) | .656 |
| NSTEMI | 61 (44) | 28 (39) | 33 (49) | .250 |
| STEMI | 9 (6) | 6 (8) | 3 (4) | .495 |
| Unstable angina | 15 (11) | 11 (15) | 4 (6) | .101 |
| Chronic coronary syndrome | 55 (39) | 27 (38) | 28 (41) | .656 |
| Antiplatelet therapy | ||||
| Dual antiplatelet therapy | 104 (74) | 57 (79) | 47 (69) | .174 |
| Aspirin + clopidogrel | 61 (43) | 31 (43) | 30 (44) | .899 |
| Aspirin + ticagrelor | 43 (31) | 26 (36) | 17 (25) | .154 |
| Triple antiplatelet therapy | ||||
| Aspirin + clopidogrel + anticoagulant | 36 (26) | 15 (2) | 21 (31) | .174 |
|
COPD, chronic obstructive pulmonary disease; Hs-cTnI, high sensitivity cardiac troponin I; LV, left ventricle; LVEF, left ventricular ejection fraction; NSTEMI, non-ST-elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction. Data are expressed as No. (%), mean ± standard deviation or median [interquartile range]. |
||||
The most common clinical presentation was acute coronary syndrome (85 patients, 61% of cases). Among these, onset consisted of ST-segment elevation myocardial infarction (STEMI) in 9 patients (6%), non-ST-segment elevation myocardial infarction in 61 patients (44%), and unstable angina in 15 patients (10%). The remaining patients (55, 39%) presented with chronic coronary syndrome.
A total of 104 patients (74%) were discharged with dual antiplatelet therapy. The main combination was aspirin and clopidogrel (61 patients, 43%). In 36 patients (26%), initial triple therapy (anticoagulation and dual antiplatelet therapy) was chosen due to concurrent conditions requiring chronic oral anticoagulation.
Based on the FRAIL scale, almost half of the patients (68 patients, 49%) met clinical criteria for frailty at the time of revascularization. The baseline characteristics of frail and nonfrail patients are shown in table 1. No statistically significant differences were found in terms of age, main cardiovascular risk factors or noncardiovascular comorbidities between the 2 groups. However, compared with nonfrail patients, those with frailty were more likely to be female (49% vs 25%; P = .004), to have atrial fibrillation (22% vs 10%; P = .041), a higher EuroSCORE level (3.80 vs 2.76; P = .010), and anemia (28% vs 14%; P = .040), and consequently a lower hematocrit and hemoglobin value (36.6% vs 39.6%; P = .031 and 12.16 mg/dL vs 13.02 mg/dL; P = .017, respectively).
Angiographic and procedural characteristics
Angiographic and procedural data are shown in table 2. The arterial access of choice was radial access (81% of procedures, 113 patients). A median SYNTAX score of 21 [15-29.5] was observed in 96 patients (68%) with multivessel disease, and 62 patients (44%) had a SYNTAX score > 22. The most common angiographic involvement of the LM was the distal segment (61%, 86 patients), while the most common plaque distribution according to the Medina classification was “1,1,1” (35 patients, 41% of LM bifurcation lesions). The strategy of choice for the treatment of the bifurcation was the provisional stent strategy (85% of LM bifurcation lesions, 73 patients), while the upfront 2-stent strategy was used in only 13 patients (15% of the LM bifurcation lesions). The mean diameter of the LM was 4.1 [± 3.5-4.5] mm with a mean angiographic stenosis of 62% (± 7). In 59 patients (42%), the procedure was guided using intravascular imaging techniques (58 patients using intracoronary ultrasound and 1 patient using coherence tomography). Coronary physiology was used in 5 patients (4%) to guide the need for revascularization or to check the result after percutaneous treatment. In 7 (5%) patients, mechanical support was required, either due to cardiogenic shock, or as a preventive measure in high-risk angioplasty (5 patients with an intra-aortic balloon pump and 2 with an Impella CP device [Abiomed, United States]). Intraprocedural complications occurred in 8 patients (6%), including a major complication in 4 patients (3 intraprocedural deaths and 1 cardiogenic shock), and a minor complication in 4 patients (1 coronary dissection with Thrombolysis in Myocardial Infarction (TIMI) grade 3 distal flow, 1 pseudoaneurysm, and 2 bleeding events from the femoral access resolved by stent implantation). The LM diameter was larger in patients with frailty than in those without (4 mm [4-4.5] vs 3.5 mm [3.5-4.5]; P = .023), a paradoxical finding since the percentage of women was higher in the group with frailty percentage of women. However, this information did not seem to be clinically relevant. No other clinically relevant differences were found between the 2 groups (table 2).
Table 2. Patients’ angiographic and procedural characteristics
| Characteristics | Total n = 140 | Nonfrail n = 72 (51) | Frail n = 68 (49) | P |
|---|---|---|---|---|
| Angiographic characteristics | ||||
| Multivessel disease | 96 (68) | 50 (69) | 46 (68) | .819 |
| SYNTAX score | 21 [15-29,5] | 21 [17-28.5] | 21.5 [14-30.6] | .752 |
| SYNTAX score > 22 | 62 (44) | 25 (39) | 31 (46) | .463 |
| LM diameter (mm) | 4 [3.5-4.5] | 3.5 [3.5-4.5] | 4 [4-4.5] | .023 |
| LM stenosis | 62 (± 7) | 64 (± 6) | 61 (± 5) | .342 |
| LM bifurcation | 86 (61) | 39 (54) | 47 (69) | .069 |
| Medina (1,1,1) | 35 (41) | 20 (51) | 15 (32) | .690 |
| Medina (1,1,0) | 33 (39) | 10 (26) | 23 (49) | .027 |
| Medina (1,0,1) | 8 (9) | 3 (8) | 5 (11) | .724 |
| Medina (0,1,1) | 3 (3) | 2 (5) | 1 (2) | .588 |
| Medina (1,0,0) | 4 (5) | 1 (3) | 3 (6) | .623 |
| Medina (0,1,0) | 0 (0) | 0 (0) | 0 (0) | - |
| Medina (0,0,1) | 3 (3) | 3 (8) | 0 (0) | .089 |
| Intracoronary diagnostic technique | ||||
| Intravascular imaging | 59 (42) | 28 (39) | 31 (46) | .422 |
| IVUS | 58 (41) | 28 (39) | 30 (44) | .530 |
| OCT | 0 (0) | 0 (0) | 1 (2) | .486 |
| Intracoronary physiology test | 5 (4) | 4 (6) | 1 (2) | .367 |
| Procedure characteristics | ||||
| Radial access | 113 (81) | 60 (83) | 53 (78) | .253 |
| Contrast (mL) | 200 [160-255] | 215 [150-259] | 200 [160-250] | .553 |
| Temporary pacemakers | 6 (4) | 3 (4) | 3 (4) | 1.000 |
| LV assist devices | 7 (5) | 4 (6) | 3 (4) | 1.000 |
| Intra-aortic balloon pump | 5 (4) | 4 (6) | 1 (2) | .367 |
| Impella | 2 (1) | 0 (0) | 2 (3) | .239 |
| One-stent bifurcation technique | 73 (85) | 34 (87) | 39 (83) | .588 |
| Stent MB + kissing | 20 (27) | 12 (35) | 7 (18) | .077 |
| Two-stent bifurcation technique | 13 (15) | 5 (13) | 8 (17) | .636 |
| T stenting | 3 (23) | 2 (40) | 1 (12.5) | .498 |
| TAP | 2 (15) | 0 (0) | 2 (25) | .498 |
| Culotte | 5 (39) | 1 (20) | 4 (50) | .371 |
| DK-Crush | 2 (15) | 1 (20) | 1 (12.5) | 1.000 |
| SKS | 1 (8) | 1 (20) | 0 (0) | .413 |
| MB stent diameter (mm) | 3.5 [3-3.5] | 3.5 [3-3.5] | 3.5 [3-3.5] | .877 |
| MB stent length (mm) | 18 [15-18] | 18 [15-18] | 18 [15-18] | .896 |
| SB stent diameter (mm) | 3.5 [3-3.5] | 3.25 [2.8-3.5] | 3.5 [3-3.6] | .371 |
| SB stent length (mm) | 15 [12-18] | 15.5 [15-21] | 15 [11-18] | .342 |
| Complications | ||||
| Intraprocedural complications | 8 (6) | 6 (8) | 2 (3) | .157 |
| Major | 4 (3) | 3 (4) | 1 (2) | .356 |
| Minor | 4 (3) | 3 (4) | 1 (2) | .356 |
|
DK, double kissing; IVUS, intravascular ultrasound; LM, left main; LV, left ventricle; MB, main branch; OCT, optical coherence tomography; SB, side branch; SKS, simultaneous kissing stents. TAP, T and small protrusion. Data are expressed as No. (%), mean ± standard deviation or median [interquartile range]. |
||||
Clinical results at follow-up
After a median follow-up of 19 months [5-35], a total of 40 (29%) MACE were recorded: 3 (2%) patients had a nonfatal myocardial infarction, 7 (5%) patients required repeat revascularization (3 for restenosis of the LM, and 4 in a different vessel), and 30 patients (21%) died of cardiac and/or uncertain causes. No strokes were reported during follow-up. Sixteen patients (11%) died of noncardiac causes during follow-up.
Clinical outcomes are presented in figure 1 and figure 2. No independent predictor of MACE was identified. The independent predictors of all-cause mortality were left ventricular ejection fraction (hazard ratio [HR], 0.90 [0.96-0.99]; P = .014), chronic kidney disease (HR, 2.26 [1.16-4.42]; P = .017), and particularly the presence of frailty (HR, 2.42 [1.17-5.02]; P = .018) (table 1 of the supplementary data). The primary endpoint of MACE occurred in 24 (35%) patients in the frail group and in 16 (22%) patients in the nonfrail group (HR, 1.61 [0.79-3.28]; P = .193). Frail patients had an increased risk of cardiovascular mortality: 21 (31%) vs 9 (13%); HR, 2.64 (1.21-5.77); P = .015. All-cause mortality was also more frequent in the frail group: 33 (49%) vs 13 (18%); HR, 2.94 (1.55-5.59); P = .001). The events during follow-up are presented in table 2 of the supplementary data. After IPTW adjustment, only the difference in all-cause mortality remained significant (HR, 1.95 [1.02-3.75]; P = .046). Survival analysis of the weighted population is shown in figure 3.
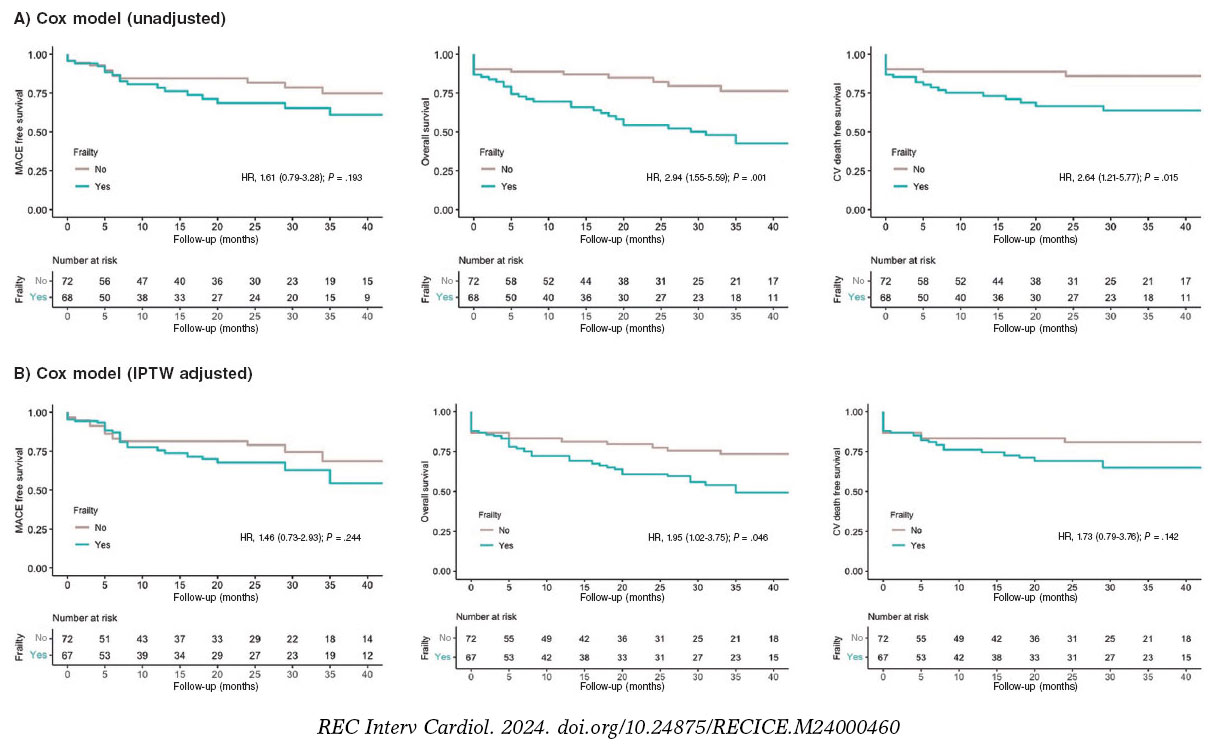
Figure 3. Kaplan-Meier Curves of the secondary outcomes. CV, cardiovascular; IPTW, inverse probability of treatment weighting; MACE, major adverse cardiovascular events.
DISCUSSION
The present study describes the feasibility of LM-PCI in a cohort of older patients. The main results were as follows: a) the rate of MACE at mid-term follow-up was 29%, mainly driven by cardiovascular and/or uncertain cause death; b) a high percentage of frailty was found in our population (49%); c) frail patients had a 2-fold increased risk of all-cause mortality during follow-up (HR, 1.95 [1.02-3.75]; P = .046) (figure 4).
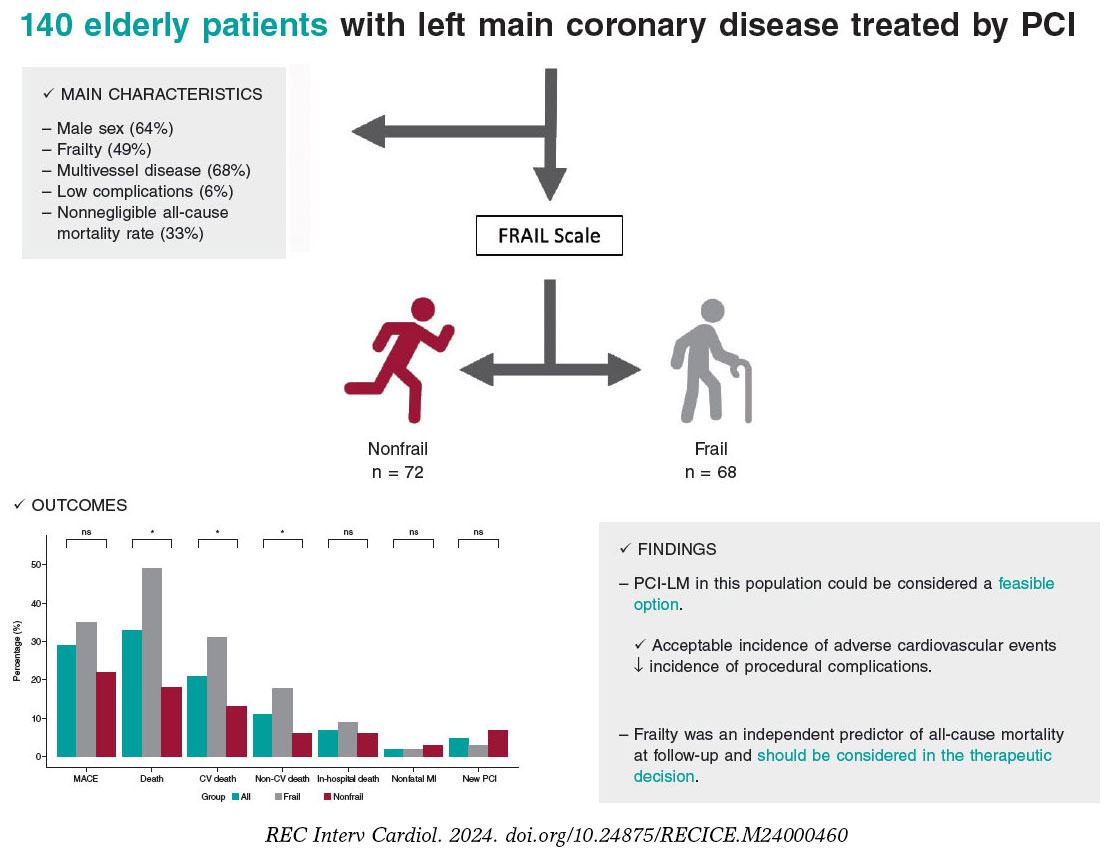
Figure 4. Central illustration. Results of percutaneous treatment of LM in elderly patients and impact of frailty. CV, cardiovascular; LM, left main coronary artery; MACE, major adverse cardiovascular events; MI, myocardial infarction; NS, non-significant; PCI, percutaneous coronary intervention.
The treatment of LM disease has traditionally been surgical, given the complexity involved and significant prognostic impact.13 However, the marked advances in interventional cardiology in recent decades have modified the approach.14,15 Contrasting evidence from clinical trials and meta-analyses shows that percutaneous treatment has similar results to surgical approaches in terms of mortality, acute myocardial infarction, and stroke at 5 years of follow-up.16 This shift has is reflected in the evolving recommendations in clinical practice guidelines, and the current European revascularization guidelines assign a grade of recommendation IA to both surgical and percutaneous strategies for the treatment of LM disease when the anatomy is not complex (SYNTAX < 22), and a class IIa recommendation for cases of intermediate complexity (SYNTAX 23-32).7
Nevertheless, the population analyzed in the study has specific clinical characteristics, and is not usually represented in large clinical trials (older patients and those with frailty and a high burden of associated comorbidities). These variables are not systematically included in surgical risk scores but are generally taken into account in routine clinical practice and often influence heart team decisions on the treatment strategy.17 Therefore, because this particular patient cohort is often excluded from research, there are no conclusive data on the benefit of percutaneous revascularization.
Our results are in line with those of previous registries in terms of MACE and all-cause mortality, as well as the association between age and a marked incidence of mortality due to noncardiac causes during follow-up. However, unlike earlier studies, we observed no differences in cardiovascular mortality, despite these patients having a more complex coronary anatomy than younger patients.18 In this regard, our study cohort had a median SYNTAX score of 21, and 44% of the patients had a score above 22. Like previous studies, this SYNTAX index score was not associated with a higher probability of cardiac events during follow-up in this special population.
In the present study, rates of acute myocardial infarction and new revascularization of the target lesion were lower than in other cohorts. Although it is difficult to make direct comparisons, we postulate that the use of new-generation drug-eluting stents and a higher proportion of revascularization guided by intracoronary diagnostic techniques may have influenced this finding. However, the use of intracoronary imaging techniques in our study was relatively low (42%) considering their benefit in patients with complex coronary lesions.19
In recent years, there has been growing interest in understanding the impact of comorbidities and frailty in older patients with cardiovascular disease.20,21 Several studies have compared invasive strategies with conservative approaches in older patients, demonstrating benefits for revascularization.22,23 However, the MOSCA-FRAIL trial compared both strategies in frail patients and observed that an invasive strategy did not confer additional benefit compared with conservative management of these patients, despite a fairly low percentage of LM disease.24 In our study, we observed a 2-fold increase in the risk of all-cause mortality in patients with frailty, suggesting the need to add systematic evaluation of frailty in older patients undergoing LM-PCI. Such assessment can aid in selecting the optimal therapeutic strategy, taking into account the likelihood of mortality during follow-up, irrespective of the application of an invasive strategy in coronary disease. These results, moreover, are consistent with other cardiovascular diseases with significant prevalence and mortality, such as heart failure.25
Study limitations
The present study has several limitations. First, it has the limitations inherent to its observational and retrospective design. Although the sample size is relatively small, it represents the largest study specifically focused on LM-PCI in older patients and analyses associated comorbidities and their impact on cardiovascular adverse events. Second, the absence of a control group receiving conservative treatment hinders the ability to draw more robust conclusions on the safety and efficacy of LM-PCI in these patients. In addition, the selection of cutoff points (age ≥ 75 years) to define this cohort of older patients was arbitrarily based on the exclusion criteria of the main clinical trials previously published. A high percentage of patients with frailty may not have undergone revascularization and would therefore have been excluded from the study. Regarding the prognostic significance of frailty, although we used IPTW to reduce confounding bias, we cannot rule out the possibility of residual confounding due to unmeasured covariables. Furthermore, there are no data on bleeding events during follow-up, which is an important concern given the impact of antiplatelet therapy in these patients. Finally, the percentage of intracoronary imaging use was lower than expected.
CONCLUSIONS
In real-life patients with advanced age and multiple associated comorbidities, percutaneous treatment of LM could be considered a feasible option, with an acceptable incidence of adverse cardiovascular events during follow-up and a low incidence of complications associated with the procedure. Frailty was an independent predictor of all-cause mortality during follow-up. When weighing the risks of LM-PCI in older patients, frailty should be taken into account in the therapeutic decision-making process.
FUNDING
None.
ETHICAL CONSIDERATIONS
The study protocol was approved by the Local Clinical Research Ethics Committee according to institutional and Good Clinical Practice guidelines. All patients signed the informed consent for publication. The authors confirm that sex and gender variables have been considered in accordance with the SAGER guidelines.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence was used in the preparation of the study.
AUTHORS’ CONTRIBUTIONS
I. Gallo, M. Alvarado and J. Perea contributed to data collection. R. González-Manzanares performed the statistical analysis. J. Suárez de Lezo and M. Romero contributed to the interpretation of the results. I. Gallo and F. Hidalgo wrote the manuscript. S. Ojeda and M. Pan reviewed the manuscript.
CONFLICTS OF INTEREST
S. Ojeda is associate editor of REC: Interventional Cardiology. The journal’s editorial procedure to ensure impartial processing of the manuscript has been followed. S. Ojeda has received consulting fees from Medtronic and Edwards and speaker fees from Philips, World Medical and Boston Scientific and is holder of a research grant (PI21/00949) from the Spanish Ministry of Science and Innovation (Instituto de Salud Carlos III). M. Pan has received speaker fees from Abbott, Boston Scientific, World Medical and Philips and holds a research grant (PI21/00949) from the Spanish Ministry of Science and Innovation (Instituto de Salud Carlos III). The remaining authors declare no conflicts of interest.
WHAT IS KNOWN ABOUT THE TOPIC?
- Coronary artery disease is closely related to age and the aging process.
- The prognosis of LM disease is uncertain and, due to due to advances in interventional cardiology in recent years, there is a need for further evidence on treatment options.
- Frailty is associated with a worse prognosis in various diseases.
WHAT DOES THIS STUDY ADD?
- LM-PCI in older adults is a feasible option in high-volume centers.
- Frailty is prevalent in older patients with LM disease and is associated with increased all-cause mortality.
SUPPLEMENTARY DATA

REFERENCES
1. Collet C, Capodanno D, Onuma Y, et al. Left main coronary artery disease:pathophysiology, diagnosis, and treatment. Nat Rev Cardiol.2018;15:321-331.
2. Giannoglou GD, Antoniadis AP, Chatzizisis YS, et al. Prevalence of narrowing >or=50% of the left main coronary artery among 17,300 patients having coronary angiography. Am J Cardiol. 2006;98:1202-1205.
3. Ramadan R, Boden WE, Kinlay S. Management of Left Main Coronary Artery Disease. J Am Heart Assoc. 2018;7:008151.
4. Yusuf S, Zucker D, Peduzzi P, et al. Effect of coronary artery bypass graft surgery on survival:overview of 10-year results from randomized trials by the Coronary Artery Bypass Graft Surgery Trialists Collaboration. Lancet. 1994;344:563-570.
5. Suárez de Lezo J, Medina A, Pan M, et al. Rapamycin-eluting stents for the treatment of unprotected left main coronary disease. Am Heart J. 2004;148:481-485.
6. Thuijs DJFM, Kappetein AP, Serruys PW, et al. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with three-vessel or left main coronary artery disease:10-year follow-up of the multicentre randomised controlled SYNTAX trial.Lancet. 2019;394:1325-1334.
7. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40:87-165.
8. Ono M, Serruys PW, Hara H, et al. 10-Year Follow-Up After Revascularization in Elderly Patients With Complex Coronary Artery Disease. J Am Coll Cardiol. 2021;77:2761-2773.
9. Abellan van Kan G, Rolland Y, Bergman H, et al. The I.A.N.A. Task Force on frailty assessment of older people in clinical practice. J Nutr Health Aging. 2008;12:29-37.
10. Medina A, Suárez de Lezo J, Pan M. Una clasificación simple de las lesiones coronarias en bifurcación [A new classification of coronary bifurcation lesions]. Rev Esp Cardiol. 2006;59:183.
11. Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW. the propensity score to estimate causal treatment effects in observational studies. Stat Med. 2015;34:3661-3679.
12. Austin PC. Variance estimation when using inverse probability of treatment weighting (IPTW. survival analysis. Stat Med.2016;35:5642-5655.
13. Baydoun H, Jabbar A, Nakhle A, et al. Revascularization of Left Main Coronary Artery. Cardiovasc Revasc Med.2019;20:1014-1049.
14. Stone GW, Sabik JF, Serruys PW, et al. Everolimus-Eluting Stents or Bypass Surgery for Left Main Coronary Artery Disease. N Engl J Med. 2016;375:2223-2235.
15. Mäkikallio T, Holm NR, Lindsay M, et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in treatment of unprotected left main stenosis (NOBLE):a prospective, randomised, open-label, non-inferiority trial. Lancet. 2016;388:2743-2752.
16. Sabatine MS, Bergmark BA, Murphy SA, et al. Percutaneous coronary intervention with drug-eluting stents versus coronary artery bypass grafting in left main coronary artery disease:an individual patient data meta-analysis. Lancet. 2021;398:2247-2257.
17. Gach O, Louis O, Martinez C, et al. Predictors of early and late outcome of percutaneous coronary intervention in octogenarians. Acta Cardiol. 2003;58:289-294.
18. Gómez-Hospital JA, Gomez-Lara J, Rondan J, et al. Long-term follow-up after percutaneous treatment of the unprotected left main stenosis in high-risk patients not suitable for bypass surgery. Rev Esp Cardiol. 2012;65:530-537.
19. Lee JM, Choi KH, Song YB, et al. Intravascular Imaging-Guided or Angiography-Guided Complex PCI. N Engl J Med. 2023;388:1668-1679.
20. Díez-Villanueva P, Arizá-SoléA, Vidán MT et al. Recomendaciones de la Sección de Cardiología Geriátrica de la Sociedad Española de Cardiología para la valoración de la fragilidad en el anciano con cardiopatía. Rev Esp Cardiol. 2019;72:63–71.
21. Pernias V, García Acuña JM, Raposeiras-Roubín S, et al. Influencia de las comorbilidades en la decisión del tratamiento invasivo en ancianos con SCASEST. REC Interv Cardiol. 2021;3:15-20.
22. Kaura A, Sterne JAC, Trickey A, et al. Invasive versus non-invasive management of older patients with non-ST elevation myocardial infarction (SENIOR-NSTEMI):a cohort study based on routine clinical data. Lancet. 2020;396:623-634.
23. Tegn N, Abdelnoor M, Aaberge L, et al. Invasive versus conservative strategy in patients aged 80 years or older with non-ST-elevation myocardial infarction or unstable angina pectoris (After Eighty study):an open-label randomised controlled trial. Lancet.2016;387:1057-1065.
24. Sanchis J, Bueno H, Miñana G, et al. Effect of Routine Invasive vs Conservative Strategy in Older Adults With Frailty and Non-ST-Segment Elevation Acute Myocardial Infarction:A Randomized Clinical Trial. JAMA Intern Med. 2023;183:407-415.
25. Jiménez-Méndez C, Díez-Villanueva P, Bonanad C, et al. Frailty and prognosis of older patients with chronic heart failure. Rev Esp Cardiol. 2022;75:1011-1019.
* Corresponding author.
 @NachoGalloFer;
@FranJHidalgo;
@rafaelglezm;
@MarcoA1788;
@PereaJorge5;
@cardiojsl;
@OjedaOjeda18;
@MPAOSS;
@Cardio_HURS
@NachoGalloFer;
@FranJHidalgo;
@rafaelglezm;
@MarcoA1788;
@PereaJorge5;
@cardiojsl;
@OjedaOjeda18;
@MPAOSS;
@Cardio_HURS
ABSTRACT
Introduction and objectives: Functional assessment of coronary stenosis severity with the piezo-electric sensor pressure wire has shown a discrepancy of up to 20% between hyperemic and nonhyperemic indexes. No data are available with fiber-optic pressure wires. The aim of this study was to evaluate the incidence and factors related to the diagnostic discordance between these indexes with a fiber-optic pressure wire. Secondary aims were to assess diagnostic reproducibility in 2 consecutive measurements of fractional flow reserve (FFR) and diastolic pressure ratio (dPR) and evaluate the drift rate.
Methods: We conducted a prospective, observational multicenter study in patients undergoing functional assessment with a fiber-optic pressure wire. We took 2 consecutive measurements of the dPR (cutoff point 0.89) and FFR (cut-off point 0.80) in each lesion analyzed. The diagnostic correlation between 2 measurements with the same technique and between the 2 techniques (dPR and FFR) was assessed. Clinical and angiographic factors associated with discordance (FFR−/dPR+ and FFR+/dPR−) between the 2 techniques were analyzed.
Results: We included 428 cases of stenosis (361 patients). Diagnostic reproducibility was 95.8% for the dPR, with a correlation coefficient between the 2 measurements (dPR1 and dPR2) of 0.974 (P < .0001). For FFR, the diagnostic reproducibility was 94.9% with a correlation coefficient (FFR1 and FFR2) of 0.942 (P < .0001). The diagnostic discordance was 18.2% (FFR+/dPR− 8.2% and FFR−/dPR+ 10%). Among the variables analyzed, the factors significantly associated with FFR−/dPR+ discordance in the multivariate analysis were hypertension and intracoronary adenosine. The only factors significantly associated with FFR+/dPR− discordance were age < 75 years and stenosis > 60%. The drift rate was 5.7%.
Conclusions: Although FFR and dPR measurements with a fiber-optic pressure wire have excellent reproducibility and a low drift rate, the discordance rate remains similar to those in previous studies with a piezo-electric pressure wire. FFR−/dPR+ discordance is associated with intracoronary adenosine and hypertension. FFR+/dPR− discordance is related to age < 75 years old and stenosis > 60%.
Keywords: Coronary physiology. Fractional flow reserve. Nonhyperemic index. Discordance. Drift.
RESUMEN
Introducción y objetivos: La valoración funcional de las estenosis coronarias con guías de presión de sensor piezoeléctrico ha mostrado hasta un 20% de discordancia entre los índices hiperémico y no hiperémico. No hay datos disponibles con guía de presión de sensor óptico. El objetivo del estudio es evaluar la incidencia y los factores relacionados con la discordancia diagnóstica entre estos índices con guía de presión de sensor óptico. Como objetivos secundarios se evaluó la reproducibilidad diagnóstica en dos determinaciones consecutivas de la reserva fraccional de flujo (RFF) y la diastolic pressure ratio (dPR). También se evaluó la tasa de drift.
Métodos: Estudio observacional, prospectivo, multicéntrico, en pacientes a quienes se realiza una valoración funcional con guía de presión de sensor óptico. Se hicieron dos mediciones consecutivas de dPR (umbral 0,89) y RFF (umbral 0,80) en cada lesión analizada. Se valoró la correlación diagnóstica entre dos mediciones con la misma técnica y entre ambas técnicas (dPR y RFF). Se analizaron factores clínicos y angiográficos asociados a la discordancia (RFF−/dPR+ y RFF+/dPR−) entre ambas técnicas.
Resultados: Se incluyeron 428 estenosis (361 pacientes). La reproducibilidad diagnóstica fue del 95,8% para dPR, con un coeficiente de correlación entre ambas mediciones (dPR1 y dPR2) de 0,974 (p < 0,0001). Para RFF la reproducibilidad diagnóstica fue del 94,9%, con un coeficiente de correlación (RFF1 y RFF2) de 0,942 (p < 0,0001). La discordancia diagnóstica fue del 18,2% (RFF+/dPR− 8,2% y RFF−/dPR+ 10%). Entre las variables analizadas, en el análisis multivariado, la hipertensión arterial y la administración intracoronaria de adenosina se asociaron de manera significativa con la discordancia RFF−/dPR+. Solo la edad < 75 años y la estenosis > 60% se asociaron de manera significativa con la discordancia RFF+/dPR−. La tasa de drift fue del 5,7%.
Conclusiones: Aunque las mediciones de RFF y dPR con guía de presión de sensor óptico tienen una excelente reproducibilidad y una baja incidencia de drift, la tasa de discordancia permanece similar a la de estudios previos con guía de presión de sensor piezoeléctrico. La adenosina intracoronaria y la hipertensión arterial se asocian con la discordancia RFF−/dPR+. La edad < 75 años y la estenosis > 60% se asocian a discordancia RFF+/dPR−.
Palabras clave: Fisiología coronaria. Reserva fraccional de flujo. Índice no hiperémico. Discordancia. Drift.
Abbreviations
dPR: diastolic pressure ratio. FFR: fractional flow reserve. FOSW: fiber-optic sensor wire. iFR: instantaneous wave-free ratio: PPSW: piezoelectric pressure sensor wire.
INTRODUCTION
Fractional flow reserve (FFR) measurement is an invasive procedure performed during coronary angiography to determine the functional significance of coronary stenoses.
In recent years, the instantaneous wave-free ratio (iFR) resting index has been developed to assess the functional significance of coronary stenoses without the need for adenosine administration. The optimal iFR cutoff value—equivalent to 0.80 in FFR—was initially established at 0.89.1 In 2017, 2 clinical studies comparing FFR with iFR found no significant differences in clinical outcomes at follow-up.2-3 After the publication of these 2 studies, the European Society of Cardiology guidelines on myocardial revascularization4 assigned resting indices the same grade of recommendation as FFR for the functional assessment of coronary lesions.
Despite the validation of these 2 techniques in clinical trials and their inclusion in clinical practice guidelines, up to 20% discordance has been reported between iFR+/FFR− or iFR−/FFR+5 Several clinical factors, such as diabetes,6 and anatomical factors, such as lesion location in the left main or proximal left anterior descending coronary arteries, have been identified in association with this discordance.7
Previous studies comparing FFR with iFR using a piezoelectric pressure sensor wire (PPSW) calculated the mean distal-to-aortic pressure ratio beginning 25% into diastole and ending 5 ms before end diastole.1
Recently, a new resting index—the diastolic pressure ratio (dPR)—has been developed to calculate the mean distal-to-aortic pressure ratio over the entire diastolic phase (from the lowest point of the dicrotic notch up to 50 ms before the onset of the upstroke of the next beat)8 using a fiber-optic sensor wire (FOSW).
A study that compared the values of different resting indices (iFR, dPR, dPR25-75, dPRmid, iFRmatlab, iFR50ms, and iFR100ms) revealed that all were numerically identical,8 meaning that the results obtained with the iFR can be extrapolated to other resting indices.
To date, no study has compared the agreement between dPR and FFR measured using a FOSW. One advantage of the FOSW over the PPSW is the lower loss of mean pressure matching in the wire compared with the measurement obtained in the guide catheter (drift).9 Although various iFR studies state that drifts < ± 0.02 are considered acceptable, the drifts reported with the FOSW were even lower at < ± 0.01.10
The diagnostic reproducibility of PPSW decreases significantly when close to the threshold value of 0.80 and is approximately 80% when measurements are < 0.77 or > 0.83, and around 90% with values < 0.76 or > 0.84.11 Since the FOSW is less sensitive to changes in humidity and temperature, greater reproducibility of results can be expected when the measurement is repeated.
Considering that most discordant measurements have been associated with cutoff values, the better reproducibility of measurements and practically nonexistent drift of the FOSW can more accurately determine FFR and dPR measurements and reduce discrepancies.
METHODS
Study design
In this prospective, observational, and multicenter registry of consecutive coronary stenoses, we conducted a study with FOSW based on our routine clinical practice.
We included consecutive patients with clinical signs and coronary angiography findings suggesting the need for a functional study with a pressure wire. We excluded patients with cardiogenic shock, heart failure, severe anemia (hemoglobin < 10 mg/dL), heart rate < 50 or > 100 bpm, baseline systolic blood pressure < 90 mmHg or > 160 mmHg, severe coronary artery lesions in distal segments, and contraindications for the administration of adenosine.
Objective
The aim of this study was to evaluate the incidence and factors related to diagnostic discrepancies between these indices using the FOSW. Secondary aims consisted of assessing the diagnostic reproducibility of FOSW in 2 consecutive measurements of FFR and dPR and evaluating the drift rate.
Procedure
The study was approved by the Drugs Research Ethics Committee of the Basque Country (internal code PS 2019039). All patients received information on the study and were asked to sign a written informed consent form prior to their participation in the study.
We performed coronary angiography using standard methods, with visual estimation of severity after intracoronary nitroglycerin administration. We included lesions with up to 50% to 75% percent diameter stenosis and collected data on the reference luminal diameter, minimum luminal diameter, lesion length, calcification, and vessel tortuosity for each studied lesion.
We performed 2 consecutive measurements of dPR (threshold, 0.89) and FFR (threshold, 0.80) for each studied lesion and analyzed the clinical and angiographic factors to determine their correlation with discordance (FFR−/dPR+ and FFR+/dPR−). We took dPR1 and FFR1 as reference values for discrepancy analysis.
We conducted the FOSW functional study with 5-, 6-, or 7-Fr guide catheters without side holes, using an OptoWire (Opsens Medical, Canada). After advancing the wire toward the tip of the guide catheter, we removed the introducer sheath and flushed the system with saline solution to prevent damping of the pressure wire resulting in equal pressure of the wire and the guide catheter at the tip of the catheter. After advancing the pressure wire distally, we administered 200 μg of intracoronary nitroglycerin before taking any measurements. We took the 2 dPR measurements after waiting the necessary time to obtain confirmation of a stable baseline distal-to-aortic coronary pressure ratio (Pd/Pa).
Subsequently, we took 2 different FFR measurements. Hyperemia was induced according to standard practice in each center (through intracoronary or IV adenosine infusion). If intracoronary adenosine was infused, for the second measurement, we waited until the baseline heart rate, blood pressure, and Pd/Pa were regained and then infused the same dose of adenosine. If IV adenosine was infused, the infusion was stopped until baseline heart rate, blood pressure, and Pd/Pa were regained, and then we infused adenosine at the same rate.
We evaluated the presence of drift upon removal of the pressure wire from the guide catheter. Drift was defined as a difference in Pd/Pa of at least ± 0.02 upon removal of the pressure wire from the guide catheter. In the presence of significant drift, measurements were repeated.
Cutoff values
The cutoff value was ≤ 0.80 for FFR and ≤ 0.89 for dPR.10 We categorized all studied vessels based on dPR and FFR values into 4 groups: concordant positive group (FFR ≤ 0.80 and dPR ≤ 0.89), concordant negative group (FFR > 0.80 and dPR > 0.89), discordant FFR+/dPR− group (FFR ≤ 0.80 and dPR > 0.89), and discordant FFR−/dPR+ group (FFR > 0.80 and dPR ≤ 0.89).
Statistical analysis
Continuous variables are expressed as mean and standard deviation, while categorical variables are expressed as percentages. We measured the association between continuous variables using Pearson’s correlation coefficient. To determine differences in variables in the FFR/dPR concordance groups we used ANOVA (for continuous variables) and the chi-square test (for categorical variables). We used the chi-square test to assess how each variable impacted FFR−/dPR+ and FFR+/dPR− discrepancies, and a multiple logistic regression model with backward elimination to determine the factors impacting FFR−/dPR+ and FFR+/dPR− discrepancies. On univariate analysis, we included variables with P < .1 in the logistic regression analysis and excluded those with a total n < 10. The analysis was conducted using SPSS software (version 20.1) and R (version 4.0.4).
RESULTS
We included a total of 428 stenoses in 361 patients. Table 1 and table 2 show the patients’ baseline characteristics, clinical presentation, and procedural characteristics.
Table 1. Patients’ baseline characteristics
| N = 361 | |
|---|---|
| Age (years) | 65.80 ± 10.5 |
| Male sex | 76.9 |
| Hypertension | 63.3 |
| Diabetes mellitus | 31 |
| Hypercholesterolemia | 60.4 |
| Active/former smoker | 19.7/40.5 |
| Previous acute coronary syndrome | 30.5 |
| Atrial fibrillation | 14.7 |
| Heart failure/dysfunction | 15.4 |
| Peripheral artery disease | 10 |
| Valvular heart disease, previous bypass, stroke | < 6 |
|
Data are expressed as No. (%) mean ± standard deviation. |
|
Table 2. Clinical presentation and procedural characteristics
| N = 361 | |
|---|---|
| Clinical presentation | N = 361 |
| Chest pain | 45.8 |
| Acute coronary syndrome | 23.1 |
| Unstable angina | 7.1 |
| Left ventricular dysfunction | 9.9 |
| Others | 14.2 |
| Procedural characteristics | |
| Baseline systolic blood pressure (mmHg) | 132 ± 24 |
| Systolic blood pressure during hyperemia (mmHg) | 125 ± 25 |
| Baseline heart rate (bpm) | 70 ± 12 |
| Heart rate during hyperemia (bpm) | 69 ± 15 |
| Reference luminal diameter (mm) | 3.09 ± 0.53 |
| Stenosis (%) | 54 ± 8 |
| Lesion length (mm) | 17.9 ± 12.2 |
| IV/intracoronary adenosine | 33/67 |
| Catheter size (5-Fr/6-Fr) | 17.5/81 |
| Drift ≥ ± 0.02 | 5.7 |
| dPR | 0.90 ± 0.08 |
| FFR | 0.83 ± 0.08 |
|
dPR, diastolic pressure ratio; FFR, fractional flow reserve. Data are expressed as No. (%) mean ± standard deviation. |
|
Sixty-seven percent of the patients received intracoronary adenosine; the mean doses of intracoronary adenosine administered were 324 μg (standard deviation [SD] ± 152) via the right coronary artery and 442 μg (SD ± 234) via the left coronary artery.
The medians of dPR measurements were 0.90 and 0.90 (SD ± 0.08) for the first and second measurements, with positivity rates of 27.4% and 27.9%, respectively. For FFR, the medians were 0.83 and 0.83 (SD ± 0.08) for the first and second measurements, with positivity rates of 28.1% and 30%, respectively.
The most widely studied vessel was the left anterior descending coronary artery (63%), followed by the left circumflex (20%) and right coronary arteries (16%).
The left anterior descending coronary artery showed a higher positivity rate (dPR+, 35.3%; FFR, 34%) than the left circumflex (dPR, 11.9%; FFR, 20.5%) and right coronary arteries (dPR, 15.9%; FFR, 17.4%).
Diagnostic reproducibility was 95.8% for dPR, with a correlation coefficient between the 2 measurements (dPR1 and dPR2) of 0.974 (P < .0001) and a mean difference of 0.019 (max, 0.12; min, −0.17). For dPR values < 0.86 or > 0.92, diagnostic reproducibility was 99.6%, decreasing to 90.7% when values were ≥ 0.86 or ≤ 0.92. For FFR, diagnostic reproducibility was 94.9%, with a correlation coefficient (FFR1 and FFR2) of 0.942 (P < .0001) and a mean difference of 0.029 (max, 0.14; min, −0.18) (figure 1). Values < 0.77 or > 0.83 showed a diagnostic reproducibility of 98.6%, decreasing to 86.4% when these values were ≥ 0.77 or ≤ 0.83.
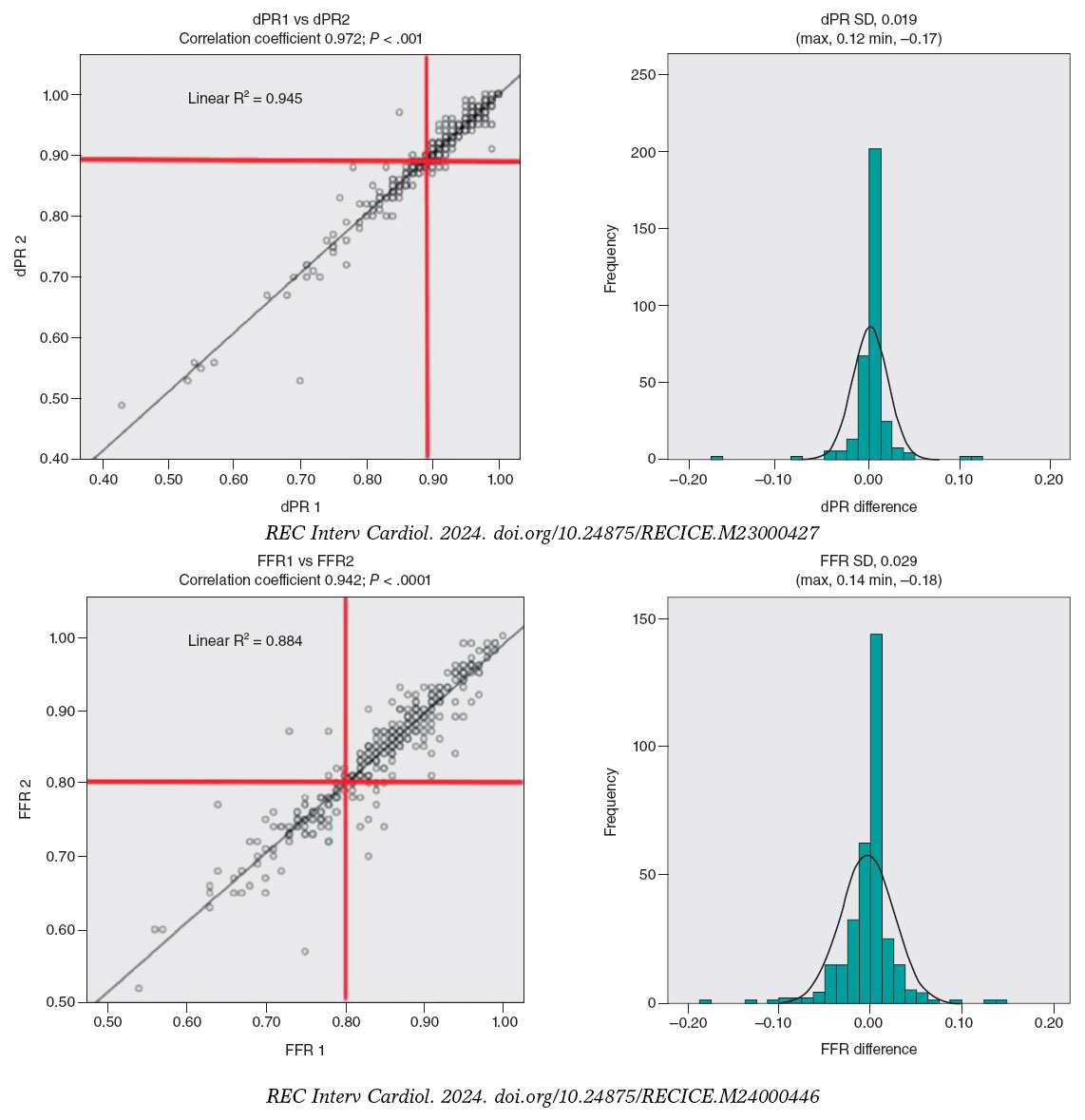
Figure 1. Correlation coefficient and histogram of the differences between the 2 dPR and FFR measurements. dPR, diastolic pressure ratio; FFR, fractional flow reserve; SD, standard deviation.
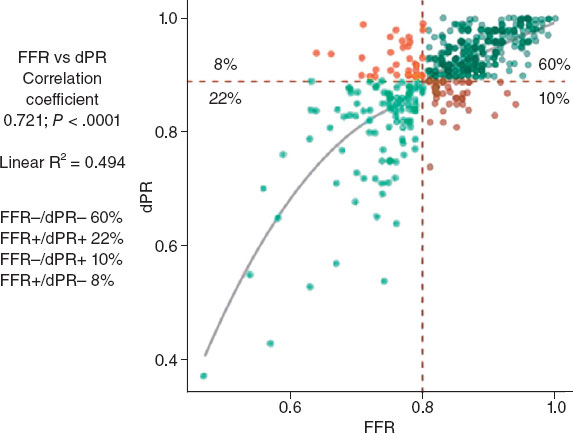
The diagnostic concordance (figure 2) between FFR and dPR was 82%, with a correlation coefficient of 0.721 (P < .0001), while diagnostic discordance was 18.2% (FFR+/dPR–, 8.2% and FFR–/dPR+, 10.0%). In the FFR+/dPR– discordant group, FFR was 0.76 ± 0.04 and dPR, 0.93 ± 0.03. In the FFR–/dPR+ discordant group, FFR was 0.84 ± 0.03 and dPR, 0.86 ± 0.03.
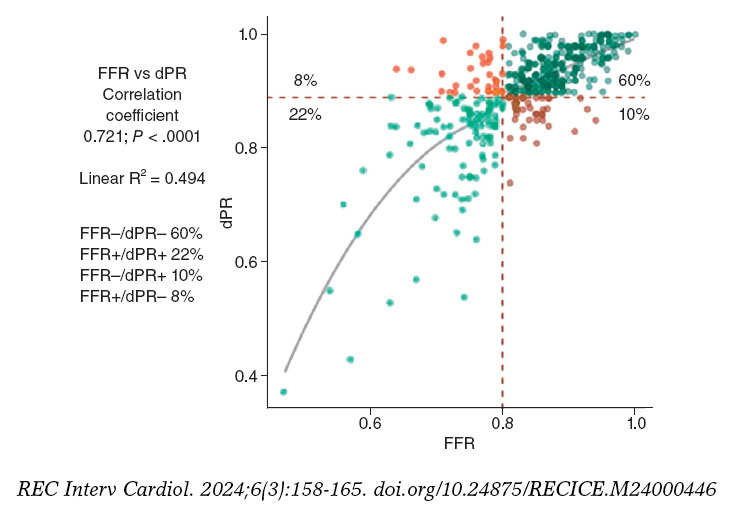
Figure 2. Distribution of lesions according to FFR and dPR, with the rate of concordant and discordant measurements. dPR, diastolic pressure ratio; FFR, fractional flow reserve.
Out of the 75 discordant results reported, the measurements at the cutoff value (7 stenoses with FFR 0.80 and 18 stenoses with dPR 0.89) showed a discordance rate of 72%, which decreased as it moved away from the cutoff value (figure 3).
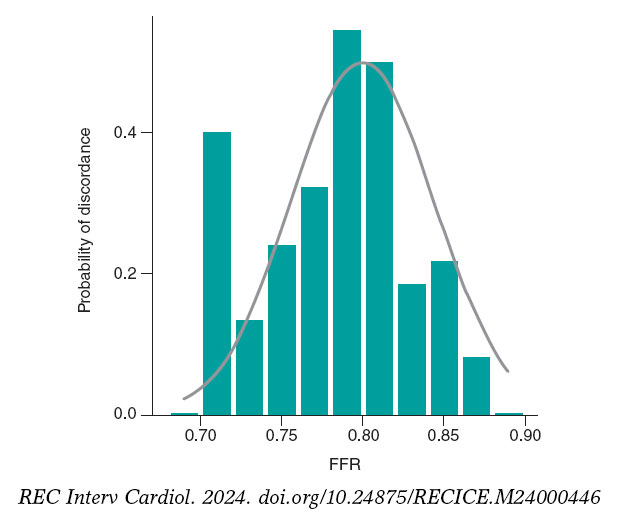
Figure 3. Probability of diagnostic discordance between FFR and dPR. The probability of discordance is close to 50% around the FFR cutoff point of 0.80 and decreases as it moves away from this point. Empirical model (bar chart) and model proposed by Petraco et al.11 (in grey). dPR, diastolic pressure ratio; FFR, fractional flow reserve.
Table 1 of the supplementary data illustrates the association between clinical and anatomical characteristics and the extent of agreement between FFR and dPR.
Out of all the variables analyzed in the multivariate analysis, hypertension (odds ratio [OR], 3.48, 95% confidence interval [95%CI], 1.01-11.98; P = .043) and intracoronary adenosine (OR, 7.04; 95%CI, 1.63-30.3; P = .001) were significantly associated with FFR–/dPR+ discordance. Age younger than 75 years (OR, 4.52; 95%CI, 1.03-20; P = .016) and percent diameter stenosis > 60% (OR, 6.69; 95%CI, 2.79-16; P < .001) were significantly associated with FFR+/dPR– discordance (table 3).
Table 3. Univariate analysis and multivariate logistic regression of variables associated with discordance
| Variables | FFR+/dPR− | FFR−/dPR+ | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate analysis | Multivariate logistic regression | Univariate analysis | Multivariate logistic regression | |||||
| OR (95%CI) | P | OR (95%CI) | P | OR (95%CI) | P | OR (95%CI) | P | |
| Age < 75 years | 9.5 vs 3.3 | .039 | 4.52 (1.03-20) | .016 | 7.1 vs 8.9 | .347 | ||
| Female sex | 5.7 vs 8.9 | .231 | 11.4 vs 6.2 | .079 | ||||
| Hypertension | 7.2 vs 10.4 | .178 | 10 vs 2.2 | .002 | 3.48 (1.01-11.98) | .043 | ||
| Diabetes mellitus | 7.3 vs 8.6 | .406 | 11.7 vs 5.3 | .018 | 2.11 (0.95-4.69) | .064 | ||
| Dyslipidemia | 7.5 vs 9.5 | .304 | 7.1 vs 6.7 | .525 | ||||
| HF/LV dysfunction | 4.4 vs 9.0 | .154 | 11.8 vs 6.7 | .118 | ||||
| Valvular heart disease | 7.7 vs 8.3 | .635 | 19.2 vs 6.8 | .037 | ||||
| Coronary calcification | 6.7 vs 8.6 | .387 | 5.3 vs 8 | .302 | ||||
| Moderate/severe tortuosity | 7.8 vs 8.3 | .516 | 10.6 vs 5.7 | .054 | ||||
| Left main coronary artery | 0 vs 7.9 | .612 | 50 vs 6.9 | .007 | ||||
| Left anterior descending coronary artery | 7.9 vs 7.6 | .531 | 9.4 vs 4.4 | .041 | ||||
| Right coronary artery | 10.8 vs 7.1 | .176 | 2.4 vs 8.8 | .029 | ||||
| Left circumflex artery | 4.3 vs 8.5 | .179 | 2.9 vs 8.4 | .081 | ||||
| RLD > 3 mm | 6.6 vs 13.3 | .049 | 7.5 vs 8 | .518 | ||||
| Length > 20 mm | 12.5 vs 5.4 | .010 | 7.8 vs 7.3 | .492 | ||||
| Stenosis > 60% | 16 vs 3 | < .001 | 6.69 (2.79-16) | < .001 | 5.8 vs 8.3 | .227 | ||
| Heart rate > 80 bpm | 8.4 vs 8 | .527 | 10.8 vs 6.8 | .155 | ||||
| Intracoronary adenosine | 7.4 vs 8.5 | .713 | 13 vs 3.8 | .004 | 7.04 (1.63-30.3) | .001 | ||
|
95%CI, 95% confidence interval; dPR, diastolic pressure ratio; FFR, fractional flow reserve; HF, heart failure; LV, left ventricle; OR, odds ratio; RLD, reference luminal diameter. Data are expresed in %. |
||||||||
The drift rate was 5.7%.
DISCUSSION
We present the results of the first study conducted with a FOSW capable of measuring the diagnostic variability of 2 consecutive determinations of nonhyperemic and hyperemic indices, as well as the diagnostic discordance between the 2 techniques.
Previous discordance studies between the 2 indices with PPSW revealed discordance rates ranging from 12% to 22%,12,13 largely depending on the proximity of the values to the cutoff point. In a study by Lee et al.,12 the mean iFR and FFR values were 0.95 ± 0.10 and 0.87 ± 0.11, respectively, with a discordance rate of 12%, while in a study by Warisawa et al.,13 the mean iFR and FFR values were 0.89 ± 0.05 and 0.80 ± 0.03, respectively, with a discordance rate of 22%. In our study, the discordance rate was 18.2%, with a mean dPR of 0.90 (SD ± 0.08) and a mean FFR of 0.83 (SD ± 0.08), which is a slightly lower discordance rate than that reported by previous studies on PPSW and mean iFR and FFR values close to the cutoff point, which may be indicative of the accuracy of measurements obtained with FOSW.
The main findings of this study were the excellent diagnostic reproducibility of the FOSW, the clinical and anatomical variables related to FFR/dPR discordance, and the low drift rate reported in the measurements.
Diagnostic reproducibility with the fiber-optic sensor wire
Diagnostic reproducibility with the FOSW was excellent, with a variation between 2 consecutive measurements < 0.02 for dPR and < 0.03 for FFR. This accuracy in measurement confers excellent diagnostic reproducibility. These data are better than those previously reported with PPSW.11
Clinical and anatomical variables associated with FFR/dPR discordance
For FFR+/dPR− discordance, in the multivariate analysis, only age younger than 75 years and percent diameter stenosis > 60% were significantly associated with FFR+/dPR− discordance. This discordance in participants younger than 75 years could be explained by a slower baseline flow and a greater coronary flow reserve in younger patients with preserved microvascular function.14,15 Although discordance due to a higher percent diameter stenosis has already been described in previous studies,15,16 such discordance requires a preserved coronary flow reserve.6 When arterial flow velocity significantly increases during hyperemia, the pressure gradient does so too, decreasing distal coronary pressure during hyperemia substantially compared with baseline values, resulting in a low FFR value.
For FFR−/dPR+ discordance, in the multivariate analysis, the associated variables were hypertension and the administration of intracoronary adenosine. Although hypertension has not been associated with FFR−/dPR+ discordance in previous studies, it is known that patients with hypertension and left ventricular hypertrophy have a reduced coronary flow reserve17 and a possible lack of vasodilatory response to adenosine due to an increased left ventricular end-diastolic pressure. These 2 factors could play a key role in the association between hypertension and FFR−/dPR+ discordance.
Although IV adenosine is the most widely studied route of administration to achieve maximum hyperemia, intracoronary adenosine at doses > 300 μg may be equally or more effective in achieving maximum hyperemia18 and with fewer adverse events.19 In our study, the FFR−/dPR+ discordance reported when intracoronary adenosine was used could be a result of a failure to achieve adequate hyperemia.
These variables related to discordance demonstrate that dPR and FFR measure different aspects of coronary circulation, which may be affected differently in distinct patients or myocardial territories, leading to discordant FFR values and nonhyperemic indices.20
Drift in the fiber-optic pressure wire
The incidence of drift in clinical studies of pressure wires is not well known, and the drift considered acceptable has varied over the years. Previously, FFR measurement was repeated when drift was > 5 mmHg,21 while in more recent studies, drift > 3 mmHg has been considered significant. When FFR is between 0.77 and 0.82, drift ≤ 3 mmHg can reclassify 18.7% of stenoses,22 and this reclassification may be higher when a nonhyperemic diastolic or whole-cycle index is used.23 In the CONTRAST trial analysis of the PPSW, the drift rate (Pd/Pa ± 0.03) was 17.5%,24 while a more recent study comparing drift between FOSW and PPSW revealed a significantly lower rate with the FOSW (4.8% vs 26.7%; P = .02).9 In our study, the drift rate was 5.7%, which is consistent with other studies on FOSW, and much lower than that reported with PPSW, facilitating the use of pressure wire in routine clinical practice.
Limitations
Our study has several limitations. Both the severity and length of coronary lesions were quantified by the operator’s visual estimation at the time of the procedure, and since this was a study without a core laboratory, we cannot rule out the possibility that some of the discrepancies found were due to technical problems in determining the indices. Since the study was based on our routine clinical practice, most patients received intracoronary adenosine, and the protocol did not specify the intracoronary infusion comprehensively, which may have resulted in the lower hyperemia reported in some patients.
Target lesion revascularization was based on dPR or FFR values according to the operators’ decision. Patient selection for pressure guidance evaluation was also left to the treating physician’s discretion, which may have resulted in biases. However, our intention was to study dPR and FFR indices under real-world conditions.
CONCLUSIONS
Although FFR and dPR measurements with FOSW have excellent reproducibility and a low incidence of drift, the discordance rate remains similar to that reported by previous studies with PPSW, and largely depends on the proximity of values to the cutoff point. Intracoronary adenosine and hypertension, which imply a lack of hyperemia or increased microvascular resistance, are associated with FFR−/dPR+ discordance. Age younger than 75 years and the severity of stenosis, which may be associated with a preserved coronary flow reserve, are related to FFR+/dPR− discordance.
FUNDING
This study received no funding.
ETHICAL CONSIDERATIONS
This study was approved by the Drugs Research Ethics Committee of the Basque Country (internal code PS 2019039) for its implementation. All patients received a patient information sheet about the study and signed an informed consent form before enrollment. The study took into consideration sex and gender variables before drafting this article.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence has been used.
AUTHORS’ CONTRIBUTIONS
M. Sádaba Sagredo drafted the protocol, included patients as the lead investigator of his center, and drafted the manuscript. A. Subinas Elorriaga and A. Quirós contributed to the statistical analysis and drafting of the manuscript. The remaining authors are lead investigators of the READI EPIC-14 trial in their respective centers and contributed to patient inclusion and article review.
CONFLICTS OF INTEREST
None declared.
WHAT IS KNOWN ABOUT THE TOPIC?
- Determination of fractional flow reserve (FFR) is a widely used technique to establish the functional significance of coronary stenoses. In recent years, resting indices have been developed to assess the functional significance of coronary stenoses without the need for adenosine administration. The optimal cutoff value—equivalent to 0.80 in FFR—has been established at 0.89. Despite its validation in clinical trials and endorsement in clinical practice guidelines, discordant results are obtained in up to 20% of the cases between the 2 techniques.
WHAT DOES THIS STUDY ADD?
- Studies on discordance between hyperemic and nonhyperemic indices are conducted with piezoelectric pressure sensor wires. Fiber-optic sensor wires are not sensitive to temperature or humidity changes, making measurements more reproducible and drift rates very low.
- No previous studies have compared the concordance between hyperemic and nonhyperemic indices with the use of a fiber-optic sensor wire. –Despite the low diagnostic variability of diastolic pressure ratio (dPR) and FFR (4.2% for dPR and 5.1% for FFR) in 2 consecutive measurements, and a similarly low drift rate (5.7%), the discrepancy between the 2 indices remains similar to that reported by previous studies (18.2%), indicating that discrepancies are more related to clinical and anatomical variables and proximity to the cutoff value than to the pressure wire used.
SUPPLEMENTARY DATA
Supplementary data associated with this article can be found in the online version available at https://doi.org/10.24875/ RECIC.M24000448.
ACKNOWLEDGEMENTS
We wish to thank M.ª Ángeles Carmona for her support in data collection and patient inclusion.
REFERENCES
1. Escaned J, Echavarría-Pinto M, Garcia-Garcia HM, et al. Prospective Assessment of the Diagnostic Accuracy of Instantaneous Wave-Free Ratio to Assess Coronary Stenosis Relevance:Results of ADVISE II International, Multicenter Study (ADenosine Vasodilator Independent Stenosis Evaluation II). JACC Cardiovasc Interv. 2015;8:824-833.
2. Davies JE, Sen S, Dehbi HM, et al. Use of the Instantaneous Wave-free Ratio or Fractional Flow Reserve in PCI. N Engl J Med. 2017;376:1824-1834.
3. Götberg M, Christiansen EH, Gudmundsdottir IJ, et al. Instantaneous Wave-free Ratio versus Fractional Flow Reserve to Guide PCI. N Engl J Med. 2017;376:1813-1823.
4. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40:87-165.
5. Jeremias A, Maehara A, Généreux P, et al. Multicenter Core Laboratory Comparison of the Instantaneous Wave-Free Ratio and Resting Pd/Pa With Fractional Flow Reserve. The RESOLVE Study. J Am Coll Cardiol. 2014;63:1253-1261.
6. Cook CM, Jeremias A, Petraco R, et al. Fractional Flow Reserve/Instantaneous Wave-Free Ratio Discordance in Angiographically Intermediate Coronary Stenoses:An Analysis Using Doppler-Derived Coronary Flow Measurements. JACC Cardiovasc Interv. 2017;10:2514-2524.
7. Kobayashi Y, Johnson NP, Berry C, et al. The Influence of Lesion Location on the Diagnostic Accuracy of Adenosine-Free Coronary Pressure Wire Measurements. JACC Cardiovasc Interv. 2016;9:2390-2399.
8. Van't Veer M, Pijls N, Hennigan B, et al. Comparison of Different Diastolic Resting Indexes to iFR. Are They All Equal?J Am Coll Cardiol. 2017;70:3088-3096.
9. Haddad K, Potter B, Matteau A, et al. Assessing the Accuracy of a Second-Generation Optical Sensor Pressure Wire in a Wire-to-Wire Comparison (The ACCURACY Study). Cardiovasc Revasc Med. 2022;35:51-56.
10. Kern M. Comparing FFR Tools:New Wires and a Pressure Microcatheter. Cath Lab Digest. 2016;24(5).
11. Petraco R, Sen S, Echavarria-Pinto M, et al. Fractional Flow Reserve-Guided Revascularization. Practical Implications of a Diagnostic Gray Zone and Measurements Variability on Clinical Decisions. JACC Cardiovasc Interv. 2013;6:222-225.
12. Lee JM, Shin E-S, Nam C-W, et al. Discrepancy Between Fractional Flow Reserve and Instantaneous Wave-free Ratio:Clinical and Angiographic Characteristics. Int J Cardiol. 2017;245:63-68.
13. Warisawa T, Cook C, Howard JP, et al. Physiological Pattern of Disease Assessed by Pressure-Wire Pullback Has an Influence on Fractional Flow Reserve/Instantaneous Wave-Free Ratio Discordance. Insights From the Multicenter AJIP Registry. Circ Cardiovasc Interv. 2019;12:e007494.
14. Lim HS, Pim AL, De Bruyne B, et al. The impact of age on fractional flow reserve-guided percutaneous coronary intervention:A FAME (Fractional Flow Reserve versus Angiography for Multivessel Evaluation) trial substudy. Int J Cardiol. 2014;177:66-70.
15. Dérimay F, Johnson NP, Zimmermann FM, et al. Predictive factors of discordance between the instantaneous wave-free ratio and fractional flow reserve. Catheter Cardiovasc Interv. 2019;94:356-363.
16. Wienemann H, Meyer A, Mauri V, et al. Comparison of Resting Full-Cycle Ratio and Fractional Flow Reserve in a German Real-World Cohort. Front Cardiovasc Med. 2021;8:744181.
17. Schäfer S, Kelm, Mingers S, Strauer BE. Left ventricular remodeling impairs coronary flow reserve in hypertensive patients. J Hypertens. 2002;20:1431-1437.
18. Lopez-Palop R, Carrillo P, Frutos A, et al. Comparison of effectiveness of high-dose intracoronary adenosine versus intravenous administration on the assessment of fractional flow reserve in patients with coronary heart disease. Am J Cardiol. 2013;111:1277-1283.
19. Abo-Aly M, Lolay G, Adams C, et al. Comparison of Intracoronary versus Intravenous Adenosine-induced Maximal Hyperemia for Fractional Flow Reserve Measurement:A Systematic Review and Meta-analysis. Catheter Cardiovasc Interv. 2019;94:714-721.
20. Nijjer SS, De Waard GA, Sen S, et al. Coronary pressure and flow relationships in humans:phasic analysis of normal and pathological vessels and the implications for stenosis assessment:a report from the Iberian–Dutch–English (IDEAL) collaborators. Eur Heart J. 2016;37:2069-2080.
21. Vranckx P, Cutlip DE, McFadden EP, Kern MJ, Mehran R, Muller O. Coronary Pressure–Derived Fractional Flow Reserve Measurements. Recommendations for Standardization, Recording, and Reporting as a Core Laboratory Technique. Proposals for Integration in Clinical Trials. Circ Cardiovasc Interv. 2012;5:312-317.
22. Wakasa N, Kuromochi T, Mihashi N, et al. Impact of Pressure Signal Drift on Fractional Flow Reserve-Based Decision-Making for Patients With Intermediate Coronary Artery Stenosis. Circ J. 2016;80:1812-1819.
23. Cook C, Ahmad Y, Shun-Shin MJ, et al. Quantification of the Effect of Pressure Wire Drift on the Diagnostic Performance of Fractional Flow Reserve, Instantaneous Wave-Free Ratio, and Whole-Cycle Pd/Pa. Circ Cardiovasc Interv. 2016;9:e002988.
24. Matsumura M, Johnson N, Fearon WF, et al. Accuracy of Fractional Flow Reserve Measurements in Clinical Practice:Observations From a Core Laboratory Analysis. JACC Cardiovasc Interv. 2017;10:1392-1401.
ABSTRACT
Introduction and objectives: Although drug-eluting stents are the main treatment in percutaneous coronary interventions (PCI), drug-coated balloons (DCB) represent an appealing alternative as they eliminate the risk of stent thrombosis and avoid leaving any metal structure in the vessel wall. However, limited evidence has been published to date on the vessel wall healing processes, plaque remodeling, plaque composition, and the impact on the coronary microcirculation after percutaneous coronary intervention with DCB (DCB-PCI).
Methods: This is investigator-initiated, single-center, single-arm, open-label, pilot study of 30 patients with native vessel disease undergoing DCB-PCI. Intravascular ultrasound and angiography-derived index of microvascular resistance (IMRangio) will be performed before and immediately after PCI, and at 3 months of follow-up.
Conclusions: The study aims to provide new evidence on the modification of atherosclerotic plaque in patients with de novo lesions undergoing PCI with DCB. This will be assessed by examining the change in the percentage of atheroma volume and late lumen enlargement using intravascular ultrasound and by evaluating changes in the microcirculation using IMRangio.
Registered at Clinicaltrials.gov (NCT06080919).
Keywords: Drug-coated balloon. Intravascular ultrasound. Angiography-derived index of microvascular resistance.
RESUMEN
Introducción y objetivos: Pese a que los stents farmacoactivos son el tratamiento principal en las angioplastias coronarias, los balones farmacoactivos representan una alternativa interesante dado que eliminan el riesgo de trombosis del stent sin dejar ningún tipo de estructura metálica en la pared del vaso. No obstante, la evidencia en cuanto a los procesos de cicatrización de la pared del vaso, el remodelado, los cambios en la composición de la placa ateroesclerótica y el impacto en la microcirculación coronaria tras el intervencionismo coronario percutáneo (ICP) con balón farmacoactivo aún no se ha esclarecido.
Métodos: Estudio piloto abierto, de un solo grupo, iniciado por el investigador, de 30 pacientes con enfermedad de vaso nativo sometidos a ICP con balón farmacoactivo. Se realizará ecografía intravascular y se determinará el índice de resistencia microvascular derivado de la angiografía (angio-IRM) antes, inmediatamente después y a los 3 meses de seguimiento de la angioplastia.
Conclusiones: Se aportará nueva evidencia sobre la modificación de la placa en pacientes con enfermedad de vaso nativo tratados con balón farmacoactivo, evaluando el cambio en el porcentaje del volumen de ateroma y el aumento luminal tardío, así como los cambios en la microcirculación mediante angio-IRM.
Registrado en Clinicaltrials.gov (NCT06080919).
Palabras clave: Balón farmacoactivo. Ecografía intravascular. Índice de resistencia microvascular derivado de la angiografía.
Abbreviations
DCB: drug-coated balloon. EEM: external elastic membrane. IMRangio: angiography-derived index of microcirculatory resistance. IVUS: intravascular ultrasound. PCI: Percutaneous coronary intervention.
INTRODUCTION
Coronary artery disease is the leading single cause of mortality worldwide, accounting for more than 7 million deaths annually1 and its prevalence has been increasing in the last 20 years.2 Percutaneous coronary intervention (PCI) has been crucial in the treatment of coronary artery disease.3,4 The advent of drug-eluting stents (DES) has substantially reduced restenosis rates through the deposition of antiproliferative drugs in the vessel wall. DES have evolved over the years and have become the gold standard in PCI.5 Drug-coated balloons (DCB) represent an alternative in the setting of PCI. DCB consist of a balloon coated with antiproliferative agents encapsulated in a polymer matrix.6 Upon inflation, the balloon brings the antiproliferative drug into contact with the vessel wall. The main goal of DCB is to eliminate the risk of stent thrombosis and achieve lower restenosis rates by not leaving any type of metal structure in the treated segment.6
The safety and efficacy of DCB have been extensively studied in de novo coronary artery disease.6 In small vessel disease, DCB have demonstrated noninferiority to DES in several randomized clinical trials.7 A recent meta-analysis has shown that the use of DCB, compared with that of DES, is associated with a lower risk of vessel thrombosis and a trend toward a lower risk of acute myocardial infarction.8 In large vessel de novo lesions, current data do not support the widespread use of DCB over DES, although DCB appear to be safe and effective.9,10 Nevertheless, there is a need to elucidate the elution on the vessel wall, healing processes, plaque remodeling, plaque composition and the impact on the coronary microcirculation following PCI with DCB.
The present report describes the design and rationale for a study of plaque modification and impact on the microcirculation after PCI with DCB (the PLAMI study).
METHODS
The study will be an investigator-initiated, single-center, single-arm, open-label, pilot study in patients undergoing PCI with DCB for de novo lesions. The study has been approved by the hospital ethics committee on research involving medical products. The study has been registered in ClinicalTrials.gov (NCT06080919).
Procedure
Eligible patients will be informed about the study and will be required to provide signed informed consent prior to inclusion. Patients will undergo DCB-PCI under intravascular ultrasound (IVUS) guidance. Angiography-derived coronary physiology will be assessed after the procedure using Angio Plus software (Pulse Medical Imaging Technology, China). The angiography images will be used to obtain the angiography-derived index of microcirculatory resistance (IMRangio) values, before and after DCB-PCI. All procedures will be performed according to current European guidelines5: the target lesion will be predilated with semicompliant balloons or noncompliant balloons, with a diameter equal to the reference vessel diameter and with an appropriate length. Multiple predilations will be accepted. The DCB will be the paclitaxel-coated balloon Pantera Lux (BIOTRONIK AG, Switzerland).
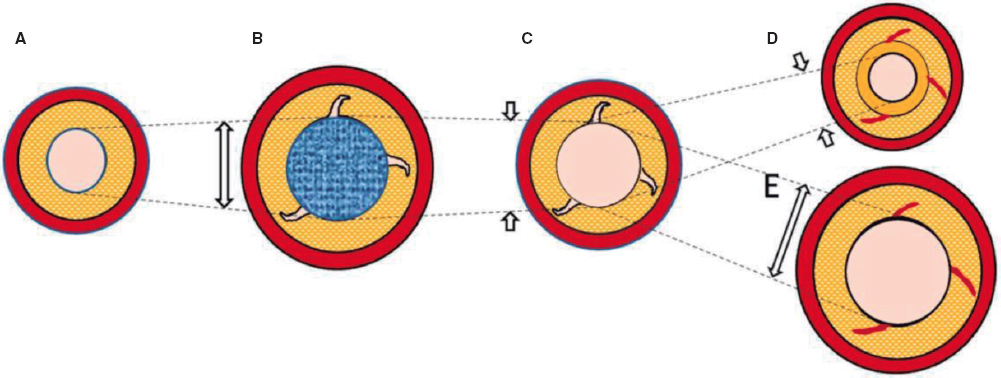
The lesion will then be treated with a DCB with a reference vessel diameter/balloon diameter ratio of 1:1. DCB length will be equal to lesion length + 5 mm. DCB inflation time will be set at 45 to 60 seconds to guarantee correct and complete drug elution. The prespecified reasons for DES implantation after DCB-PCI will be residual stenosis > 30%, dissections > type B and TIMI flow < 3.6 Angiographic follow-up with IVUS and IMRangio evaluation will be performed 3 months after the index procedure. The study timeline is summarized in figure 1.
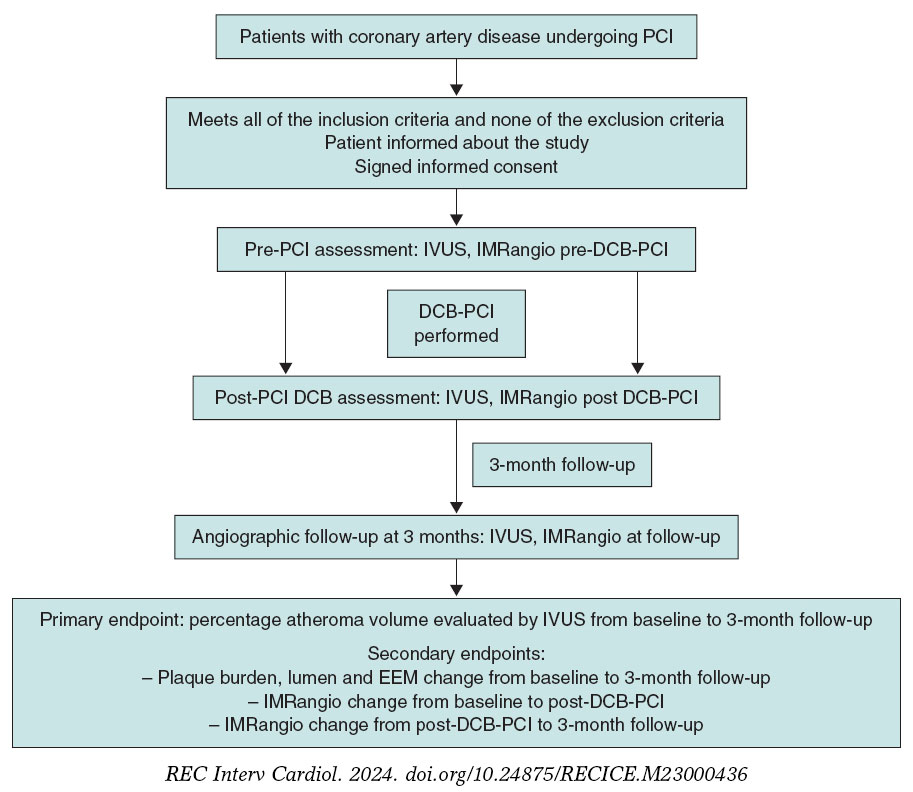
Figure 1. Timeline of the PLAMI study. DCB, drug-coated balloon; IMRangio, angiography-based index of microcirculatory resistance; IVUS, intravascular ultrasound; PCI, percutaneous coronary intervention.
IVUS images will be taken before the DCB-PCI, immediately after, and at 3 months of follow-up using the Opticross HD 60 MHz (Boston Scientific Corp, United States) system. All IVUS studies will be performed after intracoronary administration of 200 μg of nitroglycerin. The IVUS images will be acquired at 30 frames per second with an automatic transducer pull back (at 0.5 mm/second) to the proximal reference vessel lesion. As there will be no stents to take as a reference, the proximal and distal side branches adjacent to the treated lesion will serve as references, matching the coronary angiographic images (figure 2). All IVUS images will be analyzed by an independent core lab.
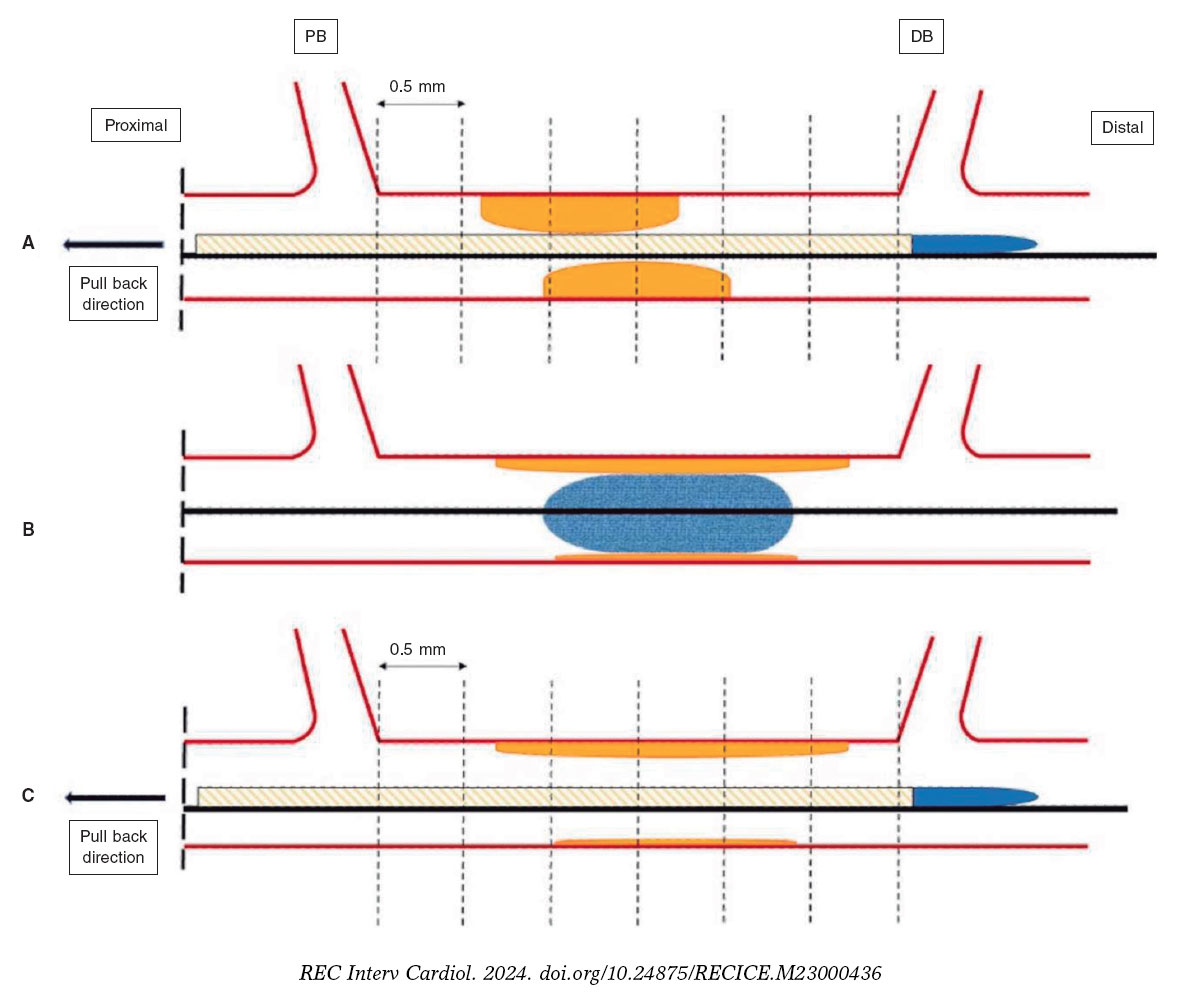
Figure 2. Schematic representation of IVUS acquisition. The IVUS images will be acquired before (A) and after (C) DCB-PCI (B) at 30 frames per second with an automatic transducer pull back (at 0.5 mm/second) to the proximal reference vessel lesion. The same anatomic slice will be analyzed before, after, and at 3 months of follow-up after the PCI by using reproducible landmarks (side branches). The first frame analyzed will be the distal point of the treated vessel before the exit of the DB (represented by the rightmost dotted line), and the last frame analyzed will be the proximal point of the vessel before the split of the proximal branch. DB, distal branch; DCB-PCI, drug-coated balloon percutaneous coronary intervention; IVUS, intravascular ultrasound; PB, proximal branch.
Angiography-derived assessment of coronary physiology will be performed with Angio Plus software (Pulse Medical Imaging Technology, China). For the evaluation of each lesion, at least 2 projections with a difference of > 25° will be selected. The operator will manually mark the points proximal and distal to the lesion, and the system automatically outlines the contours of the detected vessel. If the traced vessel trajectory deviates from the normal lumen, the necessary manual modifications will be performed. The artificial intelligence-assisted software combines the intravascular imaging information with the estimated vessel flow to obtain the IMRangio. All the angiography images will be analyzed by an independent core lab to obtain the IMRangio.
Study population and enrolment criteria
Patients will be screened to ensure they meet the inclusion criteria and none of the exclusion criteria prior to study enrolment. Inclusion criteria consist of an indication to undergo PCI for a de novo lesion according to current guidelines (with no restrictions regarding vessel size).5 Inclusion and exclusion criteria are summarized in table 1.
Table 1. Inclusion and exclusion criteria
| Inclusion criteria | Exclusion criteria |
|---|---|
| Patient with CAD undergoing PCI with DCB with no limitation to vessel size | Age < 18 years |
| Cardiogenic shock | |
| ST-segment elevation myocardial infarction | |
| Use of mechanical circulatory support | |
| Complex coronary lesions* including chronic total occlusions, bifurcation lesions, left main coronary artery disease, severe calcified lesions, graft interventions and in-stent restenosis | |
| Inability to provide informed consent | |
| Unable to understand and follow study-related instructions or unable to comply with study protocol | |
| Currently participating in another trial | |
| Pregnant women | |
|
CAD, coronary artery disease; DCB, drug-coated balloon; PCI, percutaneous coronary intervention. |
|
Sample size
Because of the exploratory nature of this study, no formal sample size calculation is required. Based on previous pilot studies with similar designs,12 a sample of 30 lesions is planned to evaluate the impact of DCB on coronary healing and the microcirculatory territory.
Study endpoints
The primary endpoint is the change in percentage atheroma volume evaluated by IVUS from baseline to 3 months of follow-up. Secondary endpoints will include a) lumen change from baseline to 3 months of follow-up (minimum, maximum, average areas), b) the percentage of progressors and percentage of regressors, c) external elastic membrane (EEM) change from baseline to post DCB-PCI (average), d) EEM change post-DCB-PCI to the 3-month follow-up (average), e) the percentage of remodeling types (neutral, negative, and positive), f) IMRangio change from baseline to post- DCB-PCI, g) IMRangio change from post-DCB-PCI to the 3-month follow-up.
An independent clinical event committee, consisting of cardiologists not participating in the trial, will review and adjudicate all major adverse cardiac events according to the study protocol.
Considering the luminal area as the area delimited by the luminal border, the minimal luminal area is defined as the smallest lumen area within the length of the treated lesion.13,14 The atheroma or plaque burden is defined as the ratio of atheroma area to the vessel EEM and is calculated by dividing the sum of plaque and media cross-sectional area (CSA) by the EEM CSA.13,14 As the atheroma area can be calculated in each frame, the total atheroma volume is obtained by taking the sum of the differences between the EEM CSA area and the luminal CSA for all available images.15 The percent of the volume of the EEM occupied by atheroma is called the percentage atheroma volume.15,16
Serial arterial remodeling types will be classified as usual: neutral if there is no change in EEM, negative if there is a decrease in the EEM and positive if vice versa.
Statistical considerations
Continuous variables will be described as mean ± standard deviation or median [interquartile range]. Categorical variables will be described as percentages. The paired t-test will be used to compare continuous variables measured before and after treatment in the same patient, and differences in proportions will be tested with the chi-square or Fisher exact test. A P value less than .05 (typically ≤ .05) will be considered statistically significant. Statistical analyses will be performed using Stata software version 13.1 (StataCorp LP, United States).
DISCUSSION
Although the use of DES remains predominant in the performance of PCI, complications such as stent thrombosis and in-stent restenosis led to the development of DCB. DCB have the theoretical benefit of not leaving metallic material in the vascular lumen, thereby reducing the possibility of mechanical complications such as malapposition, stent fracture, and stent thrombosis. This could potentially reduce neointimal proliferation and shorten the duration of dual antiplatelet therapy.6 Current guidelines assign a level IA recommendation to the treatment of in-stent restenosis.5 While the use of DCB in de novo lesions seems promising, it is not yet widespread. In addition, PCI is not without risks, as it involves a certain degree of injury to the artery wall from balloon inflations and stent struts.17,19 The vascular response to endothelial cell and smooth muscle cell injury represents a complex network of biochemical responses that involve the immune system. All these factors regulate the processes of neointimal hyperplasia, vascular remodeling, and normal reendothelialization of the arterial wall.17
The pathophysiology of restenosis and lumen loss after angioplasty is a complex process involving various factors and is not limited to neointimal hyperplasia.19 Acutely, plain old balloon angioplasty (POBA) generates an increase in luminal area that is mainly due to an expansion of the EEM, mainly attributed to the elastic properties of the vessel rather than to plaque compression or removal.20 Subsequently, within the first few minutes after PCI, there is an “acute recoil” due to the elastic properties of the arterial wall. In the chronic phase, IVUS data indicate that luminal loss is mainly due to a progressive reduction in EEM rather than an increase in atherosclerotic plaque volume. Unlike the acute phase where loss of area is solely due to elastic properties, “chronic recoil” leading to the loss of area also involves a combination factors such as fibrosis, apoptosis, and changes in the extracellular matrix.19,21 Interestingly, not all patients show negative remodeling with a decrease in EEM; around 25% show a persistent increase in EEM, which is correlated with a reduced restenosis rate. Consequently, restenosis appears to be primarily due to the direction and magnitude of changes in arterial remodeling,19 although neointimal hyperplasia also plays a role .
Nevertheless, the existing evidence is based on analysis after the use of traditional balloons. With DCB-PCI, late lumen enlargement has been observed compared with POBA.20 Although this finding has been partly attributed to the inhibition of neointimal proliferation by antiproliferative drugs,22 the role of plaque modification or vessel healing phenomena in influencing this process cannot be excluded. A previous study showed that late lumen enlargement was higher in areas with the highest plaque burden; however, that study was a retrospective assessment and used a quantitative coronary angiography protocol.23 It could be hypothesized that, by inducing controlled damage to the artery wall, together with the antiproliferative effect of DCB, positive vessel remodeling might be achieved, reducing restenosis rates without the need for DES. Therefore, with DCB-PCI, we are able to treat coronary stenosis not only from a mechanical point of view, but can also change the natural history of the disease and restenosis. In this regard, IVUS analysis will be essential to evaluate the reasons behind the gain or loss of luminal area. The dynamic changes produced after PCI are depicted in figure 3.
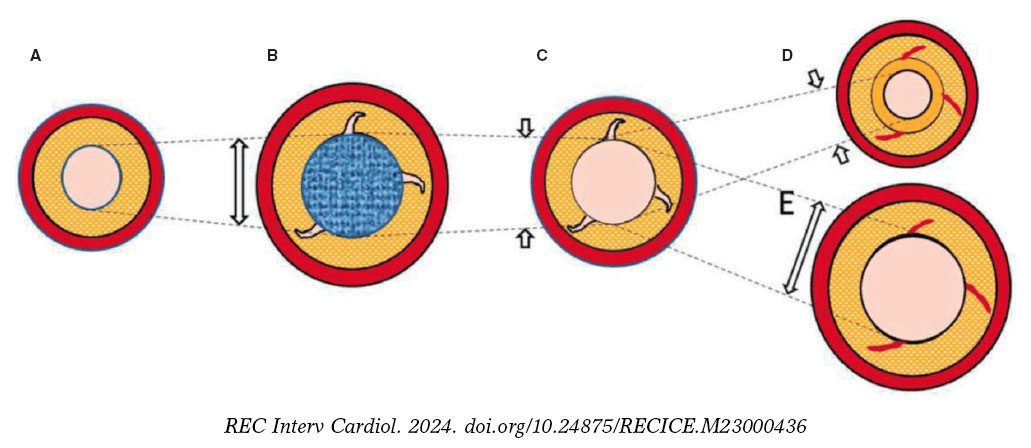
Figure 3. Central illustration. Schematic representation of timeline of DCB-PCI and lumen variation. A: pre-DCB-PCI de novo lesion. B: DCB-PCI (blue), generating injury to the vessel wall and an increase in lumen and EEM CSA. C: acute recoil. D, chronic recoil with decrease in EEM and neointimal hyperplasia. E. LLE due to maintenance of EEM area and no neointimal hyperplasia. The dotted lines represent the variations of the luminal area throughout the process. The image exemplifies how changes in luminal area, as well as plaque burden, are mainly due to variations in EEM rather than plaque compression. CSA, cross-sectional area; DCB-PCI, drug-coated balloon percutaneous coronary intervention; EEM, external elastic membrane; LLE, late lumen enlargement.
The DCB that will be used in our study, paclitaxel, has been extensively analyzed as a balloon-coating drug due to its lipophilic properties and its ability to elute into the vessel wall.24 Moreover, the available paclitaxel-DCB have shown good results in patients undergoing PCI for native vessel disease.25 In contrast, because of the hydrophobic characteristics of sirolimus, maintaining an adequate percentage in the wall over the mid-term poses technical challenges. However, advances in the formulation of the new generation of sirolimus DCB are anticipated to address this issue by facilitating adequate drug release into the vessel wall.24
As previously mentioned, the coronary microcirculation is closely related to proper coronary functioning and the pathophysiology of coronary artery disease. While it is believed that the performance of PCI, as well as the injury and healing of the coronary artery, may affect the coronary microcirculation, the evidence regarding DCB-PCI is scarce. Moreover, the plaque rupture, intimal dissections and thrombus formation that occur during balloon angioplasty are a potential source of embolism to the microvascular bed.
Since direct visualization of the microcirculation is not feasible in clinical practice,26 its assessment relies on parameters reflecting its functional status, usually coronary flow reserve and the IMR. Coronary flow reserve is defined as the ratio between hyperemic flow in response to nonendothelial vasodilation and resting blood flow. It is crucial to exclude epicardial stenosis before using coronary flow reserve, as it provides an integrated measurement of both epicardial and coronary microcirculation.26 IMR is calculated as the product of distal coronary pressure at maximal hyperemia multiplied by the hyperemic mean transit time.
In our study, we will perform a noninvasive, nonhyperemic assessment of the coronary microcirculation using IMRangio. This approach aims to characterize the baseline status of the microcirculation and assess the microvasculature changes induced by PCI and their variation over a 3-month period.
By monitoring IMRangio before and after treating the stenotic epicardial lesion, we will be able to assess the effects of acute fracture of the atherosclerotic plaque and injury to the arterial wall in the microvascular bed. We also aim to investigate whether these collateral harmful changes provoked during angioplasty remain consistent or vary significantly at 3 months of follow-up. In this same context, the analysis of IVUS during follow-up will allow us to correlate the changes in the arterial wall and atherosclerotic plaque after DCB-PCI with microcirculation physiology. To date, no insights into the anatomical and physiological process of healing of the injured arterial wall after DCB-PCI have been available in the published literature.
CONCLUSIONS
The PLAMI study is a first-in-man pilot study that aims to provide new information on the modification of atherosclerotic plaque assessed by intracoronary imaging in patients with de novo lesions undergoing PCI with DCB.
FUNDING
None reported.
ETHICAL CONSIDERATIONS
The study has been approved by the hospital ethics committee on research involving medical products. Eligible patients will be informed about the study and must provide written informed consent prior to inclusion in the study. Possible gender/sex biases have been considered.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence has been used in the preparation of this article.
AUTHORS’ CONTRIBUTIONS
J.A Sorolla Romero, A.Teira Calderón, J. Sanz Sánchez and H.M. Garcia-Garcia contributed to the conception, design, drafting and revision of the article. J.P. Vílchez Tschischke, P. Aguar Carrascosa, F.Ten Morro, L. Andrés Lalaguna, L. Martínez Dolz and J.L. Díez Gil contributed to the critical revision of the intellectual content.
CONFLICTS OF INTEREST
None declared.
WHAT IS KNOWN ABOUT THE TOPIC?
- DCB have proven clinical effectiveness in cases of in-stent restenosis and de novo lesions involving small vessel coronary artery disease.
- Several studies in small vessel coronary artery disease have shown a benefit of DCB in the vessel wall, with late lumen enlargement during follow-up.
- However, there is little evidence of their use in larger vessels.
- In addition, the impact of DCB on the coronary microcirculation has not been evaluated to date.
WHAT DOES THIS STUDY ADD?
- The PLAMI study aims to characterize vessel healing using IVUS after DCB-PCI in patients with native vessel disease and to correlate these findings with the impact on microcirculation.
REFERENCES
1. Ralapanawa U, Sivakanesan R. Epidemiology and the Magnitude of Coronary Artery Disease and Acute Coronary Syndrome:A Narrative Review. J Epidemiol Glob Health. 2021;11:169-177.
2. Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease:A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140:e596-e646.
3. Canfield J, Totary-Jain H. 40 Years of Percutaneous Coronary Intervention:History and Future Directions. J Pers Med. 2018;8:33.
4. Stefanini GG, Alfonso F, Barbato E, et al. Management of myocardial revascularisation failure:an expert consensus document of the EAPCI. EuroIntervention. 2020;16:e875-e890.
5. Neumann F, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40:87-165.
6. Jeger RV, Eccleshall S, Wan Ahmad WA, et al. Drug-Coated Balloons for Coronary Artery Disease:Third Report of the International DCB Consensus Group. JACC Cardiovasc Interv. 2020;13:1391-1402.
7. Tang Y, Qiao S, Su X, et al. Drug-Coated Balloon Versus Drug-Eluting Stent for Small-Vessel Disease:The RESTORE SVD China Randomized Trial. JACC Cardiovasc Interv. 2018;11:2381-2392.
8. Sanz Sánchez J, Chiarito M, Cortese B, et al. Drug-Coated balloons vs drug-eluting stents for the treatment of small coronary artery disease:A meta-analysis of randomized trials. Catheter Cardiovasc Interv. 2021;98:66-75.
9. Yerasi C, Case BC, Forrestal BJ, et al. Drug-Coated Balloon for de Novo Coronary Artery Disease:JACC State-of-the-Art Review. J Am Coll Cardiol. 2020;75:1061-1073.
10. Nishiyama N, Komatsu T, Kuroyanagi T, et al. Clinical value of drug-coated balloon angioplasty for de novo lesions in patients with coronary artery disease. Int J Cardiol. 2016;222:113-118.
11. Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization. J Am Coll Cardiol. 2022;79:e21-e129.
12. Joner M, Finn AV, Farb A, et al. Pathology of drug-eluting stents in humans:delayed healing and late thrombotic risk. J Am Coll Cardiol. 2006;48:193-202.
13. Xu J, Lo S. Fundamentals and role of intravascular ultrasound in percutaneous coronary intervention. Cardiovasc Diagn Ther. 2020;10:1358-1370.
14. Mintz GS, Nissen SE, Anderson WD, et al. American College of Cardiology Clinical Expert Consensus Document on Standards for Acquisition, Measurement and Reporting of Intravascular Ultrasound Studies (IVUS). A report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol. 2001;37:1478-1492.
15. Gogas BD, Farooq V, Serruys PW, Garcia-Garcia HM. Assessment of coronary atherosclerosis by IVUS and IVUS-based imaging modalities:progression and regression studies, tissue composition and beyond. Int J Cardiovasc Imaging. 2011;27:225-237.
16. Tobis JM, Perlowski A. Atheroma Volume by Intravascular Ultrasound as a Surrogate for Clinical End Points. J Am Coll Cardiol. 2009;53:1116-1118.
17. Feinberg MW. Healing the injured vessel wall using microRNA-facilitated gene delivery. J Clin Invest. 2014;124:3694-3697.
18. Inoue T, Croce K, Morooka T, Sakuma M, Node K, Simon DI. Vascular Inflammation and Repair:Implications for Reendothelialization, Restenosis, and Stent Thrombosis. JACC Cardiovasc Interv. 2011;4:1057-1066.
19. Mintz GS, Popma JJ, Pichard AD, et al. Arterial Remodeling After Coronary Angioplasty. Circulation. 1996;94:35-43.
20. Her AY, Ann SH, Singh GB, et al. Comparison of Paclitaxel-Coated Balloon Treatment and Plain Old Balloon Angioplasty for De Novo Coronary Lesions. Yonsei Med J. 2016;57:337-341.
21. Geary RL, Nikkari ST, Wagner WD, Williams JK, Adams MR, Dean RH. Wound healing:A paradigm for lumen narrowing after arterial reconstruction. J Vasc Surg. 1998;27:96-108.
22. Sogabe K, Koide M, Fukui K, et al. Optical coherence tomography analysis of late lumen enlargement after paclitaxel-coated balloon angioplasty for de-novo coronary artery disease. Catheter Cardiovasc Interv. 2021;98:E35-E42.
23. Kleber FX, Schulz A, Waliszewski M, et al. Local paclitaxel induces late lumen enlargement in coronary arteries after balloon angioplasty. Clin Res Cardiol. 2015;104:217-225.
24. Yerasi C, Case BC, Forrestal BJ, et al. Drug-Coated Balloon for De Novo Coronary Artery Disease:JACC State-of-the-Art Review. J Am Coll Cardiol. 2020;75:1061-1073.
25. Venetsanos D, Omerovic E, Sarno G, et al. Long term outcome after treatment of de novo coronary artery lesions using three different drug coated balloons. Int J Cardiol. 2021;325:30-36.
26. Kunadian V, Chieffo A, Camici PG, et al. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology &Microcirculation Endorsed by Coronary Vasomotor Disorders International Study Group. Eur Heart J. 2020;41:3504-3520.
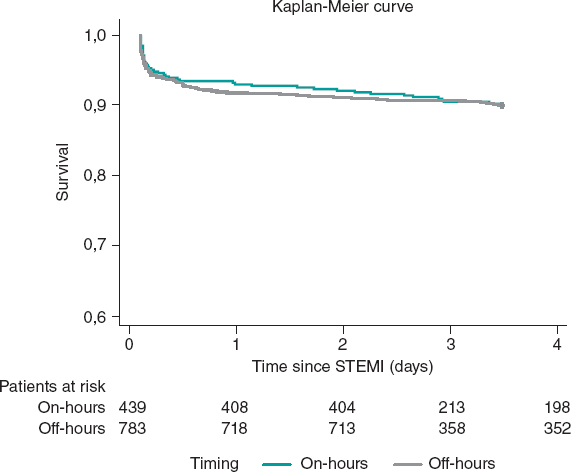
ABSTRACT
Introduction and objectives: In patients with ST-segment elevation myocardial infarction (STEMI) treatment delay significantly affects outcomes. The effect of admission time in STEMI patients is unknown when percutaneous coronary intervention (PCI) is the preferred reperfusion strategy. This study aimed to determine the association between STEMI outcomes and the timing of admission in a PCI center in south-western Europe.
Methods: This retrospective cohort study analyzed the local electronic data from 1222 consecutive STEMI patients treated with PCI. On-hours were defined as admission from Monday to Friday between 8:00 AM and 6:00 PM on non-national holidays.
Results: A total of 439 patients (36%) were admitted on-hours and 783 patients (64%) were admitted off-hours. Baseline characteristics were well-balanced between the 2 groups, including the percentage of patients admitted in cardiogenic shock (on-hours 5% vs off-hours 4%; P = .62). The median time from first medical contact to reperfusion did not differ between the 2 groups (on-hours 120 minutes vs off-hours 123 minutes, P = .54) and no association was observed between admission time and in-hospital mortality (on-hours 5% vs off-hours 5%, P = .90) or 1-year mortality (on-hours 10% vs off-hours 10%, P = .97). Survival analysis showed no differences in on-hours PCI vs off-hours PCI (HR, 1.1; 95%CI, 0.74-1.64; P = .64).
Conclusions: In a contemporary emergency network, the timing of STEMI patients’ admission to the PCI center was not associated with reperfusion delays or increased mortality.
Keywords: ST-segment elevation myocardial infarction. Admisison time. Percutaneous coronary intervention. Emergency medical services. Mortality.
RESUMEN
Introducción y objetivos: En pacientes con infarto agudo de miocardio con elevación del segmento ST (IAMCEST), el retraso en el tratamiento afecta de manera importante los resultados. El efecto del horario de atención en los pacientes con IAMCEST es dudoso cuando la intervención coronaria percutánea (ICP) es la estrategia de reperfusión preferida. Este estudio tuvo como objetivo determinar la asociación entre los resultados del IAMCEST y el momento de la admisión en un centro con ICP del suroeste de Europa.
Métodos: Estudio de cohorte retrospectivo en el que se analizaron los datos electrónicos locales de 1.222 pacientes consecutivos con IAMCEST tratados con ICP. El horario de atención laboral se definió como la admisión de lunes a viernes de 8 a 18 horas, en días no festivos.
Resultados: Un total de 439 pacientes (36%) ingresaron en horario laboral y 783 (64%) se admitieron fuera del horario. Las características iniciales estaban bien equilibradas entre los grupos, incluyendo el porcentaje de pacientes ingresados en shock cardiogénico (en horario laboral el 5% y fuera del horario laboral el 4%; p = 0,62). La mediana de tiempo desde el primer contacto médico hasta la reperfusión no fue diferente entre los 2 grupos (dentro del horario laboral 120 min y fuera del horario laboral 123 min; p = 0,54). No se observó asociación entre el tiempo de admisión y la mortalidad hospitalaria (dentro del horario laboral el 5% y fuera del horario laboral el 5%; p = 0,90) ni la mortalidad a 1 año (en horario laboral el 10% y fuera del horario el 10%; p = 0,97). El análisis de supervivencia no mostró diferencias entre la admisión dentro del horario laboral y la admisión fuera del horario laboral (HR = 1,1; IC95%, 0,74-1,64; p = 0,64).
Conclusiones: En una red de código infarto contemporáneo, el horario de admisión de pacientes con IAMCEST no se asoció con retrasos en la reperfusión ni con un aumento de la mortalidad.
Palabras clave: Infarto agudo de miocardio con elevación del segmento ST. Horario de ingreso. Intervención coronaria percutánea. Emergencia médica. Mortalidad.
Abbreviations
PCI: percutaneous coronary intervention. STEMI: ST-segment elevation myocardial infarction.
INTRODUCTION
Ischemic heart disease is the leading cause of death worldwide. In Europe, despite the decline in incidence and mortality between 1990 and 2009, these trends have slowed in recent years. Moreover, Mediterranean countries showed lower rate of decline during this period.1
ST-segment elevation myocardial infarction (STEMI) is a particularly important presentation, associated with high mortality in young individuals.2,3 Primary percutaneous coronary intervention (PCI) is recommended as the first-line therapy to lower mortality and morbidity in STEMI patients.4-6 The timing of treatment is crucial for positive outcomes, and minimization of the time from symptom onset to revascularization is essencial.7,8 While several factors affect treatment timing, emergency system delays play a crucial role as they can be more easily altered by organizational measures and are often used as a quality measurement in STEMI networks.4,9-13
To ensure timely treatment, primary PCI centers included in STEMI networks are recommended to have a 24/7 service.4 However, the impact of admission time (on- vs off-hours) on treatment delay and patient outcomes remains a matter of debate. Some studies and a large meta-analysis have shown that off-hours admission is associated with worse outcomes, partially explained by longer system delays, less guideline-directed management, and less revascularization.14-16 Conversely, studies in high-volume PCI centers integrated in STEMI networks, demonstrated no differences in outcomes according to admission time.17-20 Overall, these results are heterogeneous and include populations from different health care systems.
In Europe, efforts have been made to improve STEMI care through public awareness, emergency medical system operations, and the implementation of a full national coverage 24/7 PCI network.21
The aim of this study was to determine the association between timing of admission in a PCI center and STEMI patients’ outcomes, within a STEMI network in south-western Europe.
METHODS
Study design and population
This retrospective observational cohort study identified 1369 consecutive patients treated with primary PCI at the catheterization laboratory of the Hospital de Braga (Portugal) between June 2011 and May 2016, through the local database that systematically includes all patients undergoing invasive coronary procedures. After an initial analysis, 115 patients were found to have evolved STEMI (> 12 hours since symptom onset) and were therefore excluded. To avoid duplication of results, we excluded 12 records of a repeat episode of STEMI in a patient previously identified in the selected time frame. Lastly, clinical follow-up data were not available for 20 patients, resulting in a final sample of 1222 patients (figure 1). These patients were divided into 2 groups according to admission time (on-hours and off-hours admission), and the main outcome measures evaluated were time delays, in-hospital mortality, and 1-year mortality.
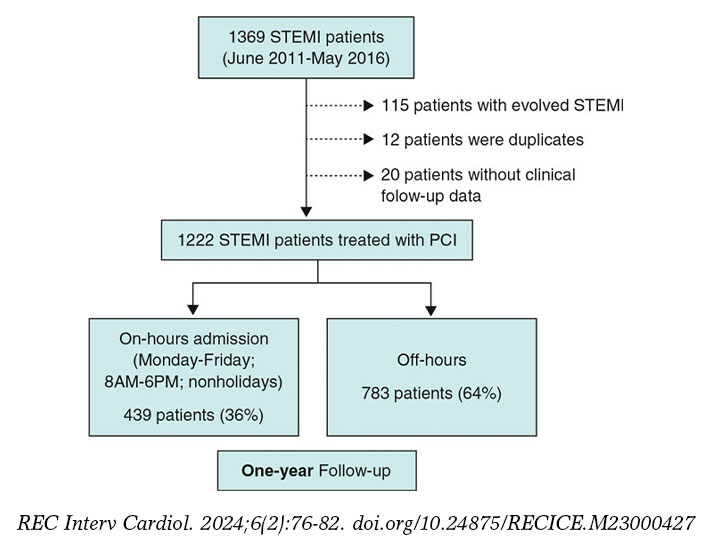
Figure 1. Study flow-chart. PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction.
Definitions
STEMI was defined as the presence of symptoms of myocardial ischemia, associated with electrocardiographic criteria for ST-segment elevation.4
Admission time was based on arrival at the catheterization laboratory. On-hours were defined as admission from Monday to Friday between 8:00 AM and 6:00 PM on non-national holidays.
The first medical contact was defined as the first contact with a health service (hospital or primary care clinic). In patients primarily attended by the emergency medical system, the moment when the emergency vehicle carrying a trained physician arrived at the location of the patient was recorded. The reperfusion time was considered as the moment when the angioplasty guidewire crossed the culprit lesion. Time delays from symptom onset to first medical contact (patient-dependent time), from first medical contact to reperfusion (system-dependent time) and from symptom onset to reperfusion (total ischemic time) were characterized.
Patient stratification according to the Killip classification was based on physical examination and the development of heart failure. A Killip class IV classification was assigned to patients in cardiogenic shock.22
STEMI network organization
Hospital de Braga has a 24/7 catheterization laboratory service for primary PCI, performed by senior interventional cardiologists (on-call during off-hours). The hospital is the only primary PCI-capable hospital in the Minho region in the north of Portugal and serves approximately 1.1 million people (figure 2). First medical contact can be made by the emergency medical system or in non-PCI-capable hospitals and clinics, which decide whether to transfer the patient to the PCI-center after consulting the on-call clinical cardiologist. First medical contact can also be made in Hospital de Braga, with rapid triage to primary PCI.
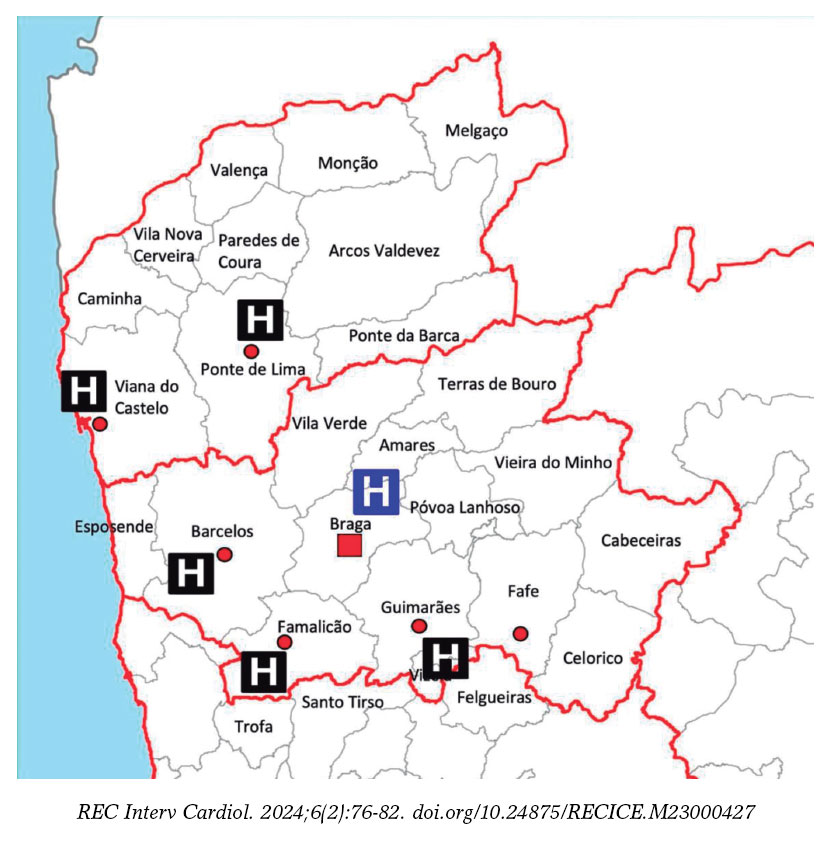
Figure 2. Referral network of the catheterization laboratory of Hospital de Braga.
Data collection and statistical analysis
The data for the present study were obtained from the local database of the patient undergoing PCI, the patient’s clinical record, and the electronic health registry of Portugal. Clinical and demographic variables were collected.
The IBM Statistical Package for the Social Sciences (IBM SPSS) version 28.0 was used for data treatment. The variables studied to characterize the patients were divided into continuous variables and categorical variables. For the analysis of continuous variables, the distribution was first evaluated. If the variables showed symmetrical normal distribution, the results are presented as mean ± standard deviation, while for variables without normal distribution, the results are reported as median [interquartile range]. To compare continuous variables between the 2 groups of patients, parametric tests were applied for variables with normal distribution and nonparametric tests for the remainder. The Student t test for independent samples was used as the parametric test, after evaluation of the homogeneity of variances using the Levene test. The Mann-Whitney U test was the nonparametric test applied. For the description of categorical variables, absolute (No.) and relative (%) frequencies were calculated. The comparison of proportions between the study groups was made using the chi-square test or Fisher exact test when the percentage of cells in the table with an expected frequency less than 5 was greater than 20%. The 1-year survival analysis was performed using the Kaplan-Meier method, comparing the groups using the log-rank test. A multivariate analysis with Cox regression was performed, and was adjusted for confounding variables that were statistically significant in the univariate analysis (age, sex, smoking, diabetes mellitus, hypertension, cardiogenic shock, and total ischemia time), to determine if the timing of patient admission was an independent predictor of 1-year mortality. The adjusted hazard ratio (HR) and 95% confidence interval (95%CI) were analyzed to determine the significance of the predictor. In all analyses, results with probability values of P < .05 were considered statistically significant.
Confidentiality and ethical considerations
Informed consent for the procedure was obtained in all patients. The confidentiality and anonymity of all collected data were ensured during all phases of the study. This study was approved by the local ethics committee and complies with the provisions of the Helsinki Declaration. Informed consent for the present analysis was waived by the ethics committee due to the retrospective nature of the study.
RESULTS
Baseline characteristics
Between June 2011 and May 2016, of 1222 consecutive patients with confirmed STEMI, a total of 439 (36%) were admitted on-hours and 783 (64%) were admitted off-hours. Baseline characteristics were well-balanced between groups, including the percentage of patients admitted in cardiogenic shock (on-hours 5% vs off-hours 4%; P = .62) (table 1).
Table 1. Baseline characteristics
| Total (N = 1222) | On-hours (N = 439) | Off-hours (N = 783) | P | |
|---|---|---|---|---|
| Clinical characteristics | ||||
| Age, y | 61 ± 13 | 62 ± 13 | 61 ± 14 | .40 |
| Female | 269 (22) | 102 (23) | 167 (21) | .44 |
| Smoking (active or previous) | 625 (54) | 218 (51) | 407 (55) | .18 |
| Dyslipidemia | 553 (46) | 201 (46) | 352 (45) | .72 |
| Diabetes | 250 (22) | 104 (25) | 146 (20) | .04 |
| Hypertension | 622 (51) | 224 (52) | 398 (51) | .89 |
| Previous history | ||||
| ACS | 84 (7) | 28 (6) | 56 (7) | .63 |
| PCI | 62 (5) | 43 (4) | 19 (6) | .38 |
| CABG | 11 (1) | 5 (1) | 6 (1) | .50 |
| Presentation | ||||
| Direct admission | 452 (36) | 159 (37) | 293 (37) | .68 |
| Anterior MI | 642 (53) | 229 (52) | 413 (53) | .85 |
| Cardiogenic shock | 51 (4) | 20 (5) | 31 (4) | .62 |
| Angiography | ||||
| Multivessel disease | 583 (48) | 215 (49) | 368 (47) | .51 |
| Echocardiography | ||||
| LVEF | 44 ± 10 | 45 ± 10 | 44 ± 10 | .41 |
|
ACS, acute coronary syndrome; CABG, coronary artery bypass graft; LVEF, left ventricular ejection fraction; MI, myocardial infarction; PCI, percutaneous coronary intervention. Data are expressed as No. (%) or mean ± standard deviation. |
||||
Comparison of treatment delays
The statistical analysis revealed no significant differences between groups for system-related, patient-related, and total ischemia time (table 2). Similarly, when examining patients directly admitted to the PCI-center, no significant differences were observed in terms of system-related, patient-related, and total ischemia time (table 2).
| Irrespective of place of FMC | Total (N = 1222) | On-hours (N = 439) | Off-hours (N = 783) | P |
|---|---|---|---|---|
| Patient-related SO-FMC, min | 87 [45-165] | 82 [45-160] | 89 [48-166] | .30 |
| Emergency system-related FMC-reperfusion, min | 123 [92-172] | 120 [91-169] | 123 [92-173] | .54 |
| Total ischemic time SO-reperfusion | 225 [164-354] | 220 [159-343] | 228 [165-360] | .39 |
| Admitted directly to the PCI-center | Subtotal (N1 = 452) | On-hours (N1 = 159) | Off-hours (N1 = 293) | P |
| Patient-related SO-FMC, min | 77 [40-150] | 75 [45-155] | 78 [40-150] | .96 |
| Emergency system-related FMC-reperfusion, min | 88 [68-115] | 87 [68-115] | 88 [70-115] | .54 |
| Total ischemic time SO-revascularization, min | 177 [125-265] | 175 [127-254] | 177 [124-267] | .92 |
|
FMC, first medical contact; PCI, percutaneous coronary intervention; SO, symptom onset. Values are expressed as median [interquartile range]. |
||||
Association between admission time and outcomes
A 1-year follow-up was completed for all patients included in the analysis. There was no association between on- and off-hours admission time and in-hospital (5% vs 5%; P = .90) or 1-year mortality (10% vs 10%; P = .97). Equally, in patients admitted on- and off-hours directly to the PCI center, in-hospital (4% vs 7%; P = .30) and 1-year mortality (9% vs 13%; P = .27) was similar.
Patients who experienced cardiogenic shock had significantly higher rates of both in-hospital (55% vs 3%; P < .01) and 1-year mortality (71% vs 7%; P < .01) compared with stable patients. However, the time of admission to the hospital did not show a significant impact on the in-hospital (on-hours 50% vs off-hours 58%; P = .57) or 1-year mortality (on-hours 65% vs off-hours 74%; P = .48) for those with cardiogenic shock.
Hospital admissions for heart failure did not differ in patients admitted on- and off-hours (3% vs 3%; P = .60).
Kaplan-Meier curves showed no differences between timings in survival terms (log-rank P = .95) (figure 3). The timing of admission was not a predictor of 1-year mortality after adjustment (HR, 1.1; 95%CI, 0.74-1.64; P = .64). Independent predictors of mortality at 1-year are depicted in table 3, with cardiogenic shock emerging as the only strong predictor of 1-year mortality.
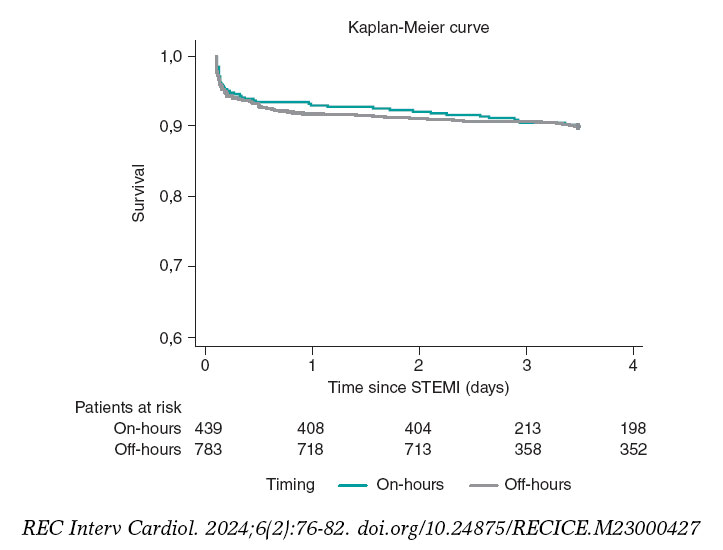
Figure 3. Kaplan-Meier curves for 1-year survival. STEMI, ST-segment elevation myocardial infarction.
Table 3. Predictive factors of 1-year mortality
| Adjusted HR* | 95%CI | P | |
|---|---|---|---|
| Age | 1.08 | 1.06-1.10 | < .01 |
| Cardiogenic shock | 12.64 | 7.60-19.47 | < .01 |
| Diabetes mellitus | 1.49 | 0.98-2.26 | .06 |
| Hypertension | 1.11 | 0.72-1.73 | .63 |
| Sex | 1.29 | 0.78-1.88 | .43 |
| Smoking | 1.06 | 0.65-1.74 | .81 |
| Total ischemic time | 1.00 | 1.00-1.01 | .06 |
|
95%CI, 95% confidence interval; HR, hazard ratio. * Multivariate analysis with Cox regression adjusted for confounding variables that were statistically significant in the univariate analysis (age, cardiogenic shock, diabetes mellitus, hypertension, sex, smoking, and total ischemia time). Admission time was not associated with 1-year mortality in univariate analysis (P = .95). |
|||
DISCUSSION
This study suggests that there is no association between the timing of admission in the PCI center and adverse outcomes, in a structured STEMI network that offers PCI as the standard of care 24/7. Patients admitted off-hours had the same characteristics and were offered the same quality of care as those admitted on-hours, reflected by the similarity in treatment delays. Previous studies, in networks that provided the same quality of care whatever the admission time, reported no differences in outcomes.17-20
On the other hand, studies that report worst outcomes in patients admitted off-hours, mainly reflect differences in care during this period, with increased delay before revascularization, lower delivery of primary PCI, different procedural characteristics, and fewer available staff during off-hours.16,23-25 Additionally, several studies found that patients tended to have worse clinical status on admission during off-hours, which adversely impacted outcomes.16,26 A finding that supports the outmost importance of presentation status is the fact that cardiogenic shock at admission was found to be an independent predictor of 1-year mortality in this study. However, we did not find significant differences in presentation status according to admission time.
This analysis emphasizes that good organization of STEMI networks, with fast-track 24/7 primary PCI, is key to improve patient outcomes and to obviate the adverse impact of off-hours. However, time delays can still be optimized. Public awareness is key to reduce patient-dependent delays, and efforts should be made to improve recognition of symptoms and activation of emergency medical systems. System delays are quality of care indexes, and in this study, they are in the upper margin for benefit of PCI over fibrinolysis (120 minutes).4,27 This group previously analyzed the impact of interhospital transfer in time from first medical contact to reperfusion, and suggested improvements in chest pain work-up in emergency rooms and prompt transfer protocols after STEMI detection.28
Mortality rates in STEMI differ widely among analyses according to the geographical area, time frame analyzed, patient inclusion criteria, and patient management protocols.29,30 Nonetheless, in this analysis, mortality rates (5% in-hospital and 10% 1-year mortality) were in line with those reported in contemporary registries.2,31
To the best of our knowledge, this is the first study in a STEMI network in south-western Europe ensuring the feasibility and safety of on-call off-hours primary PCI in a contemporary STEMI network. This provides substantial reassurance to the usual organization of cath labs with on-call professionals, essential for workload management and organization of the laboratory workforce.
Study limitations
First, this is a single-center study and may not reflect regional differences in STEMI network organization. Moreover, the results of this study reflect those of a high-volume PC center with a long-standing 24/7 primary PCI program, which may differ from others due to diverse organizational features and available resources. This could be tackled by a future study analyzing national registry data.
Second, the retrospective nature of this study has the limitations inherent to this type of design.
Third, the definition of off-hours admission time is heterogeneous across the literature. In this study, it was defined according to the organizational features of the cath lab, which may not reflect off-hours in other centers/networks.
Additionally, overall mortality in this study may be underestimated, as the group of patients diagnosed in hospitals other than the PCI center and who died before or during transfer were not included in this analysis.
Another limitation of this study is the focus on the management of the patient exclusively until the performance of the primary PCI. Other factors that affect outcomes in these patients, most importantly the delivery of guideline directed medical therapies immediately after revascularization, were not analyzed.
Our findings, based on procedures conducted between 2011 and 2016, may not fully reflect the most current health care trends, given the continuous development of clinical guidelines and treatment approaches. For instance, the reduced use of thrombus aspiration, in line with updated guidelines, highlights the imperative for ongoing research to capture the latest developments in the field.
CONCLUSIONS
In a contemporary emergency network, STEMI patients’ admission time in the PCI-center was not associated with reperfusion delays or increased in-hospital and 1-year mortality. Mortality in efficient STEMI networks is primarily affected by the severity of clinical presentation.
FUNDING
None.
ETHICAL CONSIDERATIONS
Informed consent for the procedure was obtained in all cases. The confidentiality and anonymity of all collected data were ensured during all phases of the study. This study was approved by the local ethics committee and complied with the provisions of the Helsinki Declaration. Informed consent for the present analysis was waived by the ethics committee due to the retrospective nature of the study.
Possible sex/gender biases were taken into account and avoided.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
The authors did not use artificial intelligence tools during the preparation of this study.
AUTHORS’ CONTRIBUTIONS
All the authors contributed to the study design, performed a critical review of the manuscript, gave their final approval, and are fully responsible for all aspects of the study guaranteeing both its integrity and accuracy.
CONFLICTS OF INTEREST
None.
WHAT IS KNOWN ABOUT THE TOPIC?
- The impact of admission time (on- vs off-hours) on treatment delay and patient outcomes remains a matter of debate. Some studies have shown that off-hours admission is associated with worse outcomes, while others disprove these findings.
- Previous analyses are heterogeneous and include populations from different health care systems.
WHAT DOES THIS STUDY ADD?
- Real-world clinical evidence that STEMI patients’ admission time to the PCI-center is not associated with reperfusion delays or increased in-hospital and 1-year mortality.
- Mortality in a STEMI network is primarily affected by the severity of clinical presentation.
REFERENCES
1. Vancheri F, Tate AR, Henein M, et al. Time trends in ischaemic heart disease incidence and mortality over three decades (1990–2019) in 20 Western European countries:systematic analysis of the Global Burden of Disease Study 2019. Eur J Prev Cardiol. 2022;29:396-403.
2. Zeymer U, Ludman P, Danchin N, et al. Reperfusion therapies and in-hospital outcomes for ST-elevation myocardial infarction in Europe:the ACVC-EAPCI EORP STEMI Registry of the European Society of Cardiology. Eur Heart J. 2021;42:4536-4549.
3. Fokkema ML, James SK, Albertsson P, et al. Population Trends in Percutaneous Coronary Intervention:20-Year Results From the SCAAR (Swedish Coronary Angiography and Angioplasty Registry). J Am Coll Cardiol. 2013;61:1222-1230.
4. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2018;39:119-177.
5. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction:A quantitative review of 23 randomised trials. Lancet. 2003;361:13-20.
6. Nielsen PH, Maeng M, Busk M, et al. Primary angioplasty versus fibrinolysis in acute myocardial infarction:Long-term follow-up in the danish acute myocardial infarction 2 trial. Circulation. 2010;121:1484-1491.
7. Cannon CP, Gibson CM, Lambrew CT, et al. Relationship of Symptom-Onset-to-Balloon Time and Door-to-Balloon Time With Mortality in Patients Undergoing Angioplasty for Acute Myocardial Infarction. JAMA. 2000;283:2941-2947.
8. Koul S, Andell P, Martinsson A, et al. Delay from first medical contact to primary PCI and all-cause mortality:a nationwide study of patients with ST-elevation myocardial infarction. J Am Heart Assoc. 2014;3:e000486.
9. Terkelsen CJ, Sørensen JT, Maeng M, et al. System Delay and Mortality Among Patients With STEMI Treated With Primary Percutaneous Coronary Intervention. JAMA. 2010;304:763-771.
10. Peterson MC, Syndergaard T, Bowler J, Doxey R. A systematic review of factors predicting door to balloon time in ST-segment elevation myocardial infarction treated with percutaneous intervention. Int J Cardiol. 2012;157:8-23.
11. Pereira H, CaléR, Pinto FJ, et al. Factors influencing patient delay before primary percutaneous coronary intervention in ST-segment elevation myocardial infarction:The Stent for life initiative in Portugal. Rev Port Cardiol. 2018;37:409-421.
12. Pereira H, CaléR, Pereira E, et al. Five years of Stent for Life in Portugal. Rev Port Cardiol. 2021;40:81-90.
13. Wein B, Bashkireva A, Au-Yeung A, et al. Systematic investment in the delivery of guideline-coherent therapy reduces mortality and overall costs in patients with ST-elevation myocardial infarction:Results from the Stent for Life economic model for Romania, Portugal, Basque Country and Kemerovo region. Eur Heart J Acute Cardiovasc Care. 2020;9:902-910.
14. Kostis WJ, Demissie K, Marcella SW, Shao YH, Wilson AC, Moreyra AE. Weekend versus weekday admission and mortality from myocardial infarction. N Engl J Med. 2007;356:1099-1109.
15. Magid DJ, Wang Y, Herrin J, et al. Relationship Between Time of Day, Day of Week, Timeliness of Reperfusion, and In-Hospital Mortality for Patients With Acute ST-Segment Elevation Myocardial Infarction. JAMA. 2005;294:803-812.
16. Sorita A, Ahmed A, Starr SR, et al. Off-hour presentation and outcomes in patients with acute myocardial infarction:systematic review and meta-analysis. BMJ. 2014;348:f7393.
17. de Boer SPM, Oemrawsingh RM, Lenzen MJ, et al. Primary PCI during off-hours is not related to increased mortality. Eur Heart J Acute Cardiovasc Care. 2012;1:33-39.
18. Rathod KS, Jones DA, Gallagher SM, et al. Out-of-hours primary percutaneous coronary intervention for ST-elevation myocardial infarction is not associated with excess mortality:a study of 3347 patients treated in an integrated cardiac network. BMJ Open. 2013;3:e003063.
19. Lattuca B, Kerneis M, Saib A, et al. On- Versus Off-Hours Presentation and Mortality of ST-Segment Elevation Myocardial Infarction Patients Treated With Primary Percutaneous Coronary Intervention. Cardiovascular Interventions. 2019;12:2260-2268.
20. Casella G, Ottani F, Ortolani P, et al. Off-hour primary percutaneous coronary angioplasty does not affect outcome of patients with ST-segment elevation acute myocardial infarction treated within a regional network for reperfusion:The REAL (Registro Regionale Angioplastiche dell'Emilia-Romagna) registry. JACC Cardiovasc Interv. 2011;4:270-278.
21. Wein B, Bashkireva A, Au-Yeung A, et al. Systematic investment in the delivery of guideline-coherent therapy reduces mortality and overall costs in patients with ST-elevation myocardial infarction:Results from the Stent for Life economic model for Romania, Portugal, Basque Country and Kemerovo region. Eur Heart J Acute Cardiovasc Care. 2020;9:902-910.
22. Killip T, Kimball JT. Treatment of myocardial infarction in a coronary care unit:A Two year experience with 250 patients. Am J Cardiol. 1967;20:457-464.
23. Magid DJ, Wang Y, Herrin J, et al. Relationship Between Time of Day, Day of Week, Timeliness of Reperfusion, and In-Hospital Mortality for Patients With Acute ST-Segment Elevation Myocardial Infarction. JAMA. 2005;294:803-812.
24. Barnett Pathak E, Strom JA. Disparities in Use of Same-Day Percutaneous Coronary Intervention for Patients With ST-Elevation Myocardial Infarction in Florida, 2001–2005. Am J Cardiol. 2008;102:802-808.
25. Cavallazzi R, Marik PE, Hirani A, Pachinburavan M, Vasu TS, Leiby BE. Association Between Time of Admission to the ICU and Mortality:A Systematic Review and Metaanalysis. Chest. 2010;138:68-75.
26. Glaser R, Naidu SS, Selzer F, et al. Factors Associated With Poorer Prognosis for Patients Undergoing Primary Percutaneous Coronary Intervention During Off-Hours. Biology or Systems Failure?JACC Cardiovasc Interv. 2008;1:681-688.
27. Pinto DS, Frederick PD, Chakrabarti AK, et al. Benefit of transferring ST-segment-elevation myocardial infarction patients for percutaneous coronary intervention compared with administration of onsite fibrinolytic declines as delays increase. Circulation. 2011;124:2512-2521.
28. Ferreira AS, Costa J, Braga CG, Marques J. Impacto na mortalidade da admissão direta versus transferência inter?hospitalar nos doentes com enfarte agudo do miocárdio com elevação do segmento ST submetidos a intervenção coronária percutânea primária. Rev Port Cardiol. 2019;38:621-631.
29. Williams C, Fordyce CB, Cairns JA, et al. Temporal Trends in Reperfusion Delivery and Clinical Outcomes Following Implementation of a Regional STEMI Protocol:A 12-Year Perspective. CJC Open. 2023;5:181-190.
30. Landon BE, Hatfield LA, Bakx P, et al. Differences in Treatment Patterns and Outcomes of Acute Myocardial Infarction for Low- and High-Income Patients in 6 Countries. JAMA. 2023;329:1088-1097.
31. Szummer K, Wallentin L, Lindhagen L, et al. Improved outcomes in patients with ST-elevation myocardial infarction during the last 20?years are related to implementation of evidence-based treatments:experiences from the SWEDEHEART registry 1995–2014. Eur Heart J. 2017;38:3056-3065.
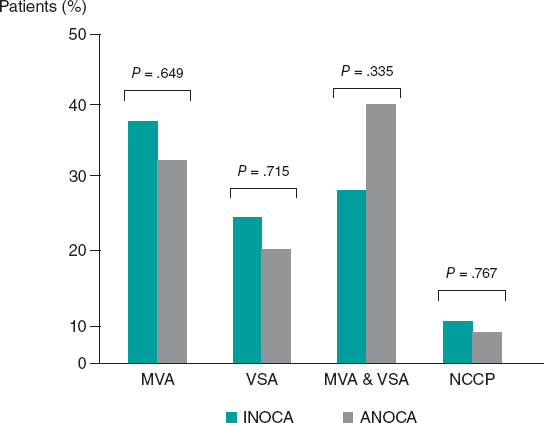
ABSTRACT
Introduction and objectives: A systematic approach to patients with angina with no obstructed coronary arteries (ANOCA) or ischemia with no obstructed coronary arteries (INOCA) patients is not routinely implemented.
Methods: All consecutive patients diagnosed with ANOCA/INOCA were referred to a designated outpatient clinic for a screening visit to assess their eligibility for a NOCA program. If eligible, patients underwent scheduled coronary angiograms with coronary function testing and intracoronary acetylcholine provocation testing. Medical therapy was optimized accordingly. All patients were then followed up at 1, 3, 6, and 12 months. Baseline and 3-month follow-up assessments included the Seattle Angina Questionnaire (SAQ) and EuroQol-5D questionnaire.
Results: Of 77 patients screened, 23 (29.9%) were excluded and 54 (70.1%) were included (29 [53.7%] with INOCA and 25 [46.3%] with ANOCA). Microvascular angina was diagnosed in 19 (35.2%) patients, vasospastic angina in 12 (22.2%), both microvascular angina and vasospastic angina in 18 (33.3%), and noncoronary chest pain in 5 (9.3%). There was a notable increase in the use of beta-blockers, calcium channel blockers and nitrates. Complications occurred in 3 (5.5%) patients. Compared with baseline, there was no difference in the mean EQ-5D score at the 3-month follow-up, but there was a significant improvement in the SAQ score related to physical limitations, angina stability, and disease perception, with no differences in angina frequency or treatment satisfaction. No events were recorded at the 1-year follow-up.
Conclusions: A specific diagnostic and therapeutic protocol can be easily and safely implemented in routine clinical practice, leading to improvement in patients’ quality of life.
Keywords: INOCA. ANOCA. Diagnosis. Therapy. Protocol.
RESUMEN
Introducción y objetivos: El abordaje sistemático en pacientes con angina con arterias coronarias no obstruidas (ANOCA) o con isquemia con arterias coronarias no obstruidas (INOCA) no está bien protocolizado.
Métodos: Todos los pacientes con diagnóstico de INOCA o ANOCA se trasladaron a una clínica ambulatoria específica para evaluar su elegibilidad para el programa NOCA. Si eran elegibles, se sometían a una angiografía coronaria programada con pruebas de función coronaria y provocación intracoronaria con acetilcolina. La terapia médica se optimizó en consecuencia. Todos los pacientes tuvieron un seguimiento a 1, 3, 6 y 12 meses. Al inicio y a los 3 meses se aplicaron los cuestionarios SAQ y EuroQol-5D.
Resultados: De 77 pacientes se excluyeron 23 (29,9%) y se incluyeron 54 (70,1%) (29 [53,7%] con INOCA y 25 [46,3%] con ANOCA). Se diagnosticó angina microvascular a 19 (35,2 %) pacientes, angina vasoespástica a 12 (22,2 %), angina microvascular y angina vasoespástica a 18 (33,3 %), y dolor torácico no coronario a 5 (9,3 %). Hubo un aumento significativo en el uso de bloqueadores beta, bloqueadores del calcio y nitratos. Se presentaron complicaciones en 3 (5,5%) pacientes. No hubo diferencias en la puntuación media del EQ-5D a los 3 meses y se observó una mejora significativa en la puntuación SAQ respecto a la limitación física, la estabilidad de la angina y la percepción de enfermedad, sin diferencias en la frecuencia de angina y la satisfacción con el tratamiento. No se registraron eventos al año.
Conclusiones: Un protocolo diagnóstico y terapéutico específico podría implementarse de manera fácil y segura en la práctica clínica diaria, y con ello mejoraría la calidad de vida de los pacientes.
Palabras clave: INOCA. ANOCA. Diagnóstico. Terapia. Protocolo.
Abbreviations
ANOCA: angina with no obstructed coronary arteries. INOCA: ischemia with no obstructed coronary arteries.
INTRODUCTION
Ischemic heart disease is the leading cause of disability and mortality worldwide and is commonly characterized by the presence of obstructive coronary artery disease (CAD) (defined as any coronary artery stenosis ≥ 50% in diameter).1 However, up to 60% to 70% of patients with angina and/or documented myocardial ischemia do not have angiographic evidence of CAD.2 This condition is defined as angina with no obstructed coronary arteries (ANOCA) or ischemia with no obstructed coronary arteries (INOCA) when associated with evidence of myocardial ischemia.3 Of note, despite the absence of CAD, these patients are at an increased risk of future cardiovascular events such as acute coronary syndrome, heart failure hospitalization, stroke, and repeat cardiovascular procedures compared with healthy individuals.4,5 Therefore, appropriate management in terms of diagnosis and treatment is of the utmost importance to improve patients’ prognosis and outcomes.6 The Coronary Microvascular Angina (CorMicA) trial demonstrated that a strategy of adjunctive invasive testing for disorders of coronary function together with stratified medical therapy can improve outcomes (ie, reduction in angina severity and enhanced quality of life).7,8 However, there are still concerns about the implementation in real-world practice of a systematic diagnostic and therapeutic approach in INOCA and ANOCA patients, potentially impacting outcomes and quality of life.
We report our single-center experience of the implementation in clinical practice of a specific diagnostic and therapeutic protocol (no obstructed coronary arteries [NOCA] program) in INOCA and ANOCA patients.
METHODS
Eligibility criteria for the NOCA program
All consecutive patients diagnosed either at our hospital or at our referral centers with angina or ischemia with nonobstructive CAD on coronary angiography were referred to a specific outpatient clinic (the NOCA clinic at Hospital Clínic, Barcelona, Spain) for a screening visit. Nonobstructive CAD was defined as angiographic evidence of normal coronary arteries or diffuse atherosclerosis with stenosis < 50% and/or fractional flow reserve (FFR) > 0.80 if there was stenosis between 50% and 70%. During the screening visit, a team of expert cardiologists confirmed patients’ eligibility for the NOCA program based on the following criteria: a) diagnosis of ANOCA, defined as stable, chronic typical angina symptoms (eg, chest pain precipitated by physical exertion or emotional stress and relieved by rest or nitroglycerine); b) diagnosis of INOCA, defined as the demonstration of myocardial ischemia identified by a noninvasive test with pharmacologic or exercise stress tests such as cardiac single photon emission computed tomography, cardiac magnetic resonance, stress electrocardiography, or echocardiography.3 The exclusion criteria were: a) atypical angina symptoms, and b) clearly identifiable noncoronary causes of chest pain (figure 1). The study protocol adhered to the Declaration of Helsinki and the study was approved by our institutional review committee. All patients provided written informed consent to be included in this program and study. The clinical ethics committee gave their approval for a retrospective analysis of the collected data.

Figure 1. Central illustration. Flowchart for the inclusion of patients in the NOCA program. Cath lab, catheterization laboratory; INOCA: ischemia with no obstructed coronary arteries; NOCA, no obstructed coronary arteries; NOCAD, nonobstructive coronary artery disease.
NOCA program: diagnostic approach
After patient inclusion in the NOCA program, specialized counseling was provided by expert cardiologists and nurses. All patients were thoroughly informed about their disease, the importance of reaching a specific diagnosis, and the importance implementing tailored therapy. During the counseling sessions, the predicted benefits and low associated risks of an invasive procedure to specifically study coronary microcirculation and vasospasm were explained in detail. All patients provided written informed consent to undergo coronary angiography and intracoronary provocation testing with acetylcholine (ACh).
Subsequently, all patients underwent a scheduled coronary angiogram with a comprehensive diagnostic work-up consisting of the following: a) coronary function testing to assess coronary flow reserve (CFR) and the index of microvascular resistance (IMR); b) intracoronary ACh provocation testing to assess the presence of coronary vasomotion disorders (eg, epicardial or microvascular spasm).
Coronary function testing was performed using a pressure-temperature sensor guidewire (PressureWire X Guidewire and Coroventis CoroFlow Cardiovascular System, Abbott Vascular, United States) placed in the left anterior descending artery (LAD) as the prespecified target vessel, reflecting its subtended myocardial mass and coronary dominance. Steady-state hyperemia was induced using intravenous adenosine (140 µg/kg/min). If there was severe tortuosity of the LAD or evidence of myocardial ischemia in a region other than the territory of the LAD, the wire was placed in the right coronary artery or the left circumflex, as per the operator’s decision. CFR was calculated using thermodilution, defined as resting mean transit time divided by hyperemic mean transit time (abnormal CFR was defined as ≤ 2.5). IMR was calculated as the product of distal coronary pressure at maximal hyperemia multiplied by the hyperemic mean transit time (normal value < 25).6,9
Intracoronary ACh provocation testing was performed with a standardized protocol involving serial ACh infusions for 20 seconds at increasing concentrations (2-20-100 µg in the left coronary artery with an interval of 2-3 minutes between each injection) with concomitant assessment of the patient’s symptoms, electrocardiogram documentation, and angiographic scans. Patients taking vasoactive drugs (eg, calcium channel blockers and nitrates) underwent a wash-out period of at least 48 hours before the provocative test.10,11,12 Epicardial coronary spasm was defined as the reproduction of chest pain and ischemic electrocardiogram changes in association with a reduction in coronary diameter ≥ 90% from baseline in any epicardial coronary artery segment.13 Microvascular spasm was diagnosed when typical ischemic ST-segment changes (deviation ≥ 1 mm) and angina developed in the absence of epicardial coronary constriction (< 90% diameter reduction).14
Subsequently, patients were stratified into 4 endotypes: a) microvascular angina (MVA) (evidence of coronary microvascular dysfunction [CMD] defined as any abnormal CFR [< 2.5], IMR [≥ 25], or microvascular spasm); b) vasospastic angina (VSA) (CFR ≥ 2.5, IMR < 25 and epicardial spasm); c) both MVA and VSA (evidence of CMD and epicardial spasm); and d) noncoronary chest pain (CFR ≥ 2.5 and IMR < 25, with neither microvascular nor epicardial spasm).6
Any complications occurring during the invasive diagnostic work-up were documented, including bradyarrhythmias, atrial fibrillation, ventricular tachycardia or fibrillation, coronary perforations, death from any cause, and any other complications.
NOCA program: pharmacological and psychological therapeutic approach
Once the endotype was identified, medical treatment for each patient was optimized accordingly (table 1). In patients with MVA, treatment with beta-blockers and calcium channel blockers (CCBs) was started or up-titrated. Ranolazine was added if angina symptoms were not fully controlled by beta-blockers and CCBs. In patients with VSA, treatment with nondihydropyridine CCBs and long-acting nitrates was started or up-titrated. In patients with both MVA and VSA, treatment with nondihydropyridine CCBs or beta-blockers was started or up-titrated. In patients with noncoronary chest pain, vasoactive drugs were discontinued unless clinically indicated for other reasons. Additionally, treatment with angiotensin-converting enzyme inhibitors/angiotensin receptor blockers and statins was started or up-titrated in all patients. If a patient showed intolerance or had contraindications to a specific medication (eg, asthma for beta-blockers, perimalleolar edema for CCBs, severe bradycardia for both beta-blockers and CCBs), the treatment was tailored and modified accordingly.
Because stress is an important trigger factor for angina symptoms, all patients were also referred to a team of expert psychologists for psychological support.15
NOCA program: clinical outcome and quality of life evaluation
All patients were followed up at 1, 3, 6, and 12-months for treatment titration and assessment of clinical outcomes. At the time of coronary angiography (ie, baseline) and at the 3-month follow-up, all patients were administered the Seattle Angina Questionnaire (SAQ) and quality of life questionnaire (EuroQol-5D [EQ-5D]). The SAQ is a validated 19-item self-administered questionnaire that measures 5 dimensions of CAD: physical limitation, angina stability, angina frequency, treatment satisfaction, and disease perception.16 The EQ-5D is a standardized, nondisease-specific questionnaire used to describe and evaluate patients’ health status and was intended to complement other quality-of life measures.17 Figure 2 provides a visual representation of all the steps involved for patients included in the NOCA program.

Figure 2. Visual representation of the NOCA program. EQ-5D, EuroQol-5D; NOCA, no obstructed coronary arteries; SAQ, Seattle Angina Questionnaire. * See text for more details.
Statistical analysis
Data distribution was assessed according to the Kolgormonov-Smirnov test. Continuous variables were compared using the unpaired Student t-test or the Mann–Whitney U test, as appropriate. The data are expressed as mean ± standard deviation (SD) or as median and interquartile range [IQR]. Categorical data are expressed as numbers and percentages and were evaluated using the chi-square test or Fisher exact test, as appropriate. A 2-sided P value < .05 was considered significant. All analyses were performed using SPSS version 21 (SPSS, United States).
RESULTS
Baseline characteristics of the study population
From January 2021 to December 2021, a total of 77 patients were screened at the NOCA clinic for inclusion in the NOCA program. Following the screening visit, 23 (29.9%) patients were excluded from the NOCA program: 12 due to atypical angina symptoms and 11 due to a clearly identifiable noncoronary cause. Consequently, 54 patients were included in the NOCA program (mean age 64.4 ± 9.4 years, 39 [63.9%] women). A total of 29 (53.7%) patients had INOCA and 25 (46.3%) had ANOCA. All clinical and angiographic characteristics of the study population are shown in table 1.
Table 1. Medical therapy according to the specific endotype of ANOCA/INOCA
| Pathogenic mechanism of MINOCA | Therapeutic implications |
|---|---|
| MVA | Beta-blockers (Nebivolol 2.5–10 mg daily) |
| CCBs (amlodipine 10 mg daily, or verapamil 240 mg daily, or diltiazem 90 mg twice daily) | |
| Ranolazine (375-750 mg twice daily) | |
| VSA | Nondihydropyridine CCBs (verapamil 240 mg, or ciltiazem 90 mg twice daily) |
| Long-acting nitrates (isosorbide mononitrate 30 mg) | |
| MVA and VSA | CCBs (verapamil or diltiazem) or beta-blockers |
| Noncoronary chest pain | Beta-blockers or dihydropyridine CCBs if clinically indicated (eg, hypertension) |
| ACEi or ARB if clinically indicated | |
| Statins if clinically indicated | |
|
ACEi, angiotensin-converting enzyme inhibitors; ANOCA, angina with no obstructed coronary arteries; ARB, angiotensin receptor blockers; CCBs, calcium channel blockers; INOCA, ischemia with no obstructed coronary arteries; MINOCA, myocardial infarction with non-obstructive coronary artery disease; MVA, microvascular angina; VSA, vasospastic angina. |
|
NOCA program: diagnosis of the specific endotype and complications
The results of the invasive functional assessment are presented in table 2. The mean IMR and CFR values were 21.2 ± 10.6 and 2.3 ± 1.4, respectively. MVA was diagnosed in 19 (35.2%) patients, VSA in 12 (22.2%), and both MVA and VSA in 18 (33.3%). Finally, 5 (9.3%) patients were diagnosed with noncoronary chest pain.
Table 2. Clinical and angiographic characteristics of patients included in the NOCA program
| Characteristics | Study population (n = 54) |
|---|---|
| Clinical characteristics | |
| Age | 64.4 ± 9.4 |
| Female sex | 39 (72.2) |
| Clinical presentation | |
| ANOCA | 25 (46.3) |
| INOCA | 29 (53.7) |
| Diabetes mellitus | 12 (22.2) |
| Hypertension | 35 (64.8) |
| Dyslipidaemia | 28 (51.9) |
| Former smokers | 3 (5.7) |
| Current smoker | 14 (25.9) |
| Familiar history of CV disease | 5 (9.3) |
| Previous CV history | |
| Prior MI | 7 (13.0) |
| Prior PCI | 8 (14.8) |
| Prior CABG | 0 (0.0) |
| COPD | 1 (1.9) |
| CKD (eGFR < 60 mL/min/m2) | 4 (7.4) |
| Depression | 15 (27.8) |
| Anxiety | 19 (35.2) |
| Invasive functional evaluation | |
| Vessel explored | |
| LDA | 48 (88.9) |
| LCx | 3 (5.6) |
| RCA | 3 (5.6) |
| IMR | 21.2 ± 10.6 |
| Increased IMR (≥ 25) | 18 (33.3) |
| CFR | 2.3 ± 1.4 |
| Reduced CFR (< 2.5) | 33 (61.1) |
| Increased IMR (≥ 25) and reduced CFR (< 2.5) | 13 (24.1) |
| Diagnosis (endotype) | |
| MVA | 19 (35.2) |
| VSA | 12 (22.2) |
| MVA and VSA | 18 (33.3) |
| Noncoronary chest pain | 5 (9.3) |
|
ANOCA, angina with no obstructed coronary arteries; CABG, coronary artery bypass graft surgery; CFR, coronary flow reserve; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CV, cardiovascular; eGFR, estimated glomerular filtration rate; IMR, index of microcirculatory resistance; INOCA, ischemia with no obstructed coronary arteries; MI, myocardial infarction; MVA, microvascular angina; LAD, left anterior descending; LCx, left circumflex; PCI, percutaneous coronary intervention; RCA, right coronary artery; VSA, vasospastic angina. Values are expressed as No. (%), mean ± standard deviation or median [interquartile range]. |
|
Among INOCA patients, MVA was diagnosed in 11 (37.9%) patients, VSA in 7 (24.1%), both MVA and VSA in 8 (27.6%), and noncoronary chest pain in 3 (10.3%). Among ANOCA patients, MVA was diagnosed in 8 (32.0%) patients, VSA in 5 (20.0%), both MVA and VSA in 10 (40.0%), and noncoronary chest pain in 2 (8.0%). There were no statistically significant differences in the prevalence of any endotype between INOCA and ANOCA patients (all P > .05, figure 3).

Figure 3. Prevalence of the different endotypes among INOCA and ANOCA patients. ANOCA, angina with no obstructed coronary arteries; INOCA, ischemia with no obstructed coronary arteries; MVA, microvascular angina; NCCP, noncoronary chest pain; VSA, vasospastic angina.
Complications occurred in 3 (5.5%) patients during intracoronary ACh provocation testing: 2 (3.7%) patients had transient bradyarrhythmias and 1 (1.8%) patient had paroxysmal atrial fibrillation that spontaneously reverted to sinus rhythm.
NOCA program: treatment optimization according to the specific endotype
Inclusion in the NOCA program led to statistically significant changes in medications after diagnosis of the specific endotype. There was a significant increase in the use of beta-blockers (33.3% before vs 57.4% after, P = .008), nondihydropyridine CCBs (9.3% before vs 37.0% after, P < .001), and long-acting nitrates (46.3% before vs 63.0% after, P = .012). There were no statistically significant differences in any other medications before and after the invasive assessment (all P > .05, figure 4). All changes in medications according to the specific endotype of ANOCA/INOCA are shown in figure 5.

Figure 4. Differences in medical treatment before and after patient inclusion in the NOCA program. ACEi, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; DP-CCBs, dihydropyridine calcium channel blockers; LA, long-acting; ND-CCBs, nondihydropyridine calcium channel blockers.

Figure 5. Changes in medications according to the specific endotype of ANOCA/INOCA. A: patients with MVA. B: patients with VSA. C: Patients with MVA and VSA. D: patients with noncoronary chest pain. DP-CCBs, dihydropyridine calcium channel blockers; LA, long-acting; MVA, microvascular angina; ND-CCBs, nondihydropyridine calcium channel blockers; VSA, vasospastic angina.
NOCA program: clinical outcome evaluation
At 3 months of follow-up, there was no statistically significant difference in the mean EQ-5D score compared with baseline (64.8 ± 18.1 at baseline vs 66.1 ± 17.1 at 3 months of follow-up, P = .302) (figure 6). However, there was a statistically significant improvement in the SAQ score in terms of physical limitations (59.7 ± 19.3 at baseline vs 66.2 ± 16.9 at 3 months of follow-up, P = .037), angina stability (57.1 ± 28.1 at baseline vs 75.8 ± 22.3 at 3 months of follow-up, P = .010), and disease perception (42.5 ± 13.9 at baseline vs 50.8 ± 16.3 at 3 months follow-up, P = .015). No statistically significant difference was found in angina frequency (74.3 ± 20.4 at baseline vs 80.7 ± 19.8 at 3 months of follow-up, P = .193) or treatment satisfaction (68.1 ± 12.6 at baseline vs 70.5 ± 12.5 at 3 months of follow-up, P = .950) (figure 7). No events were recorded at the 1-year follow-up.

Figure 6. Differences in EuroQol-5D (EQ-5D) score at baseline and at 3 months of follow-up.

Figure 7. Differences in SAQ score at baseline and at 3 months of follow-up. AF, angina frequency; AS, angina stability; DP, disease perception; EQ-5D, EuroQol-5D; PL, physical limitations; SAQ, Seattle Angina Questionnaire; TS, treatment satisfaction.
DISCUSSION
The main results of our experience can be summarized as follows: a) the implementation of a specific diagnostic and therapeutic protocol (NOCA program) in patients with diagnosed with nonobstructive CAD is feasible and allowed a parsimonious use of medical resources; b) a comprehensive diagnostic work-up in INOCA and ANOCA patients is safe, with a low rate of mild and transient complications (5.5%); c) the inclusion of patients in the NOCA program led to significant changes in medications and a significant improvement in their angina symptoms at the 3-month follow-up with no adverse events at 1 year.
Although accumulating evidence has demonstrated that an approach consisting of a comprehensive diagnostic assessment and stratified medical therapy in INOCA and ANOCA is crucial to improve patients’ prognosis, such an approach is far from routinely implemented in clinical practice.7,8 There are still concerns mainly related to the cost-benefit ratio, the associated prolonged procedural time, increased costs, and the risk of possible associated complications. Furthermore, in the most recent European Society of Cardiology guidelines, invasive coronary function testing is assigned a class IIa (“should be considered”) recommendation, while ACh provocation testing is supported by a class IIb recommendation (“may be considered”) to assess microvascular spasm and class IIa in patients under consideration for VSA.3 As a result, the management of these patients is commonly left to physicians’ discretion or relies on the experience of each center. Consequently, diagnosis of a specific NOCA endotype is frequently missed, and medical therapy is not optimized. This, in turn, has a significant negative impact on patients’ quality of life and clinical outcomes, as well as on health care costs, due to the need for repeat hospitalization or invasive procedures.18
In reporting our experience, we demonstrate that a specific diagnostic and therapeutic protocol (ie, the NOCA program) in patients with a previous diagnosis of nonobstructive CAD can be easily implemented in clinical practice. A key innovation of our study, compared with prior publications, is the creation and implementation of a specific protocol for the INOCA/ANOCA population. Additionally, our approach involves a screening visit with assessment by a team of expert cardiologists for patients with a suspected diagnosis of INOCA/ANOCA. This approach improves identification of such patients, and, in our experience, led to the exclusion of almost one third of patients (29.9%) due to atypical angina symptoms or no clearly identifiable coronary causes of chest pain. This is another novelty of our study that could be extremely relevant in the management of these patients. Indeed, the selection of patients to be included in the program may allow clinical resources to be directed to patients who are most likely to benefit, while avoiding repeat invasive procedures and related risks in patients with unclear indications. Additionally, the specialized counseling provided by cardiologists and nurses during the screening visit, together with psychological support, are likely to be vital components of the management of INOCA/ANOCA patients. Indeed, recent studies have demonstrated how psychological factors, such as chronic stress, anxiety, depression, and social stressors are involved in the pathogenesis of MVA and VSA.19-23 Mental stress has been demonstrated to determine CMD mainly through endothelium-dependent mechanisms and endothelial dysfunction.24 Similarly, by activating brain areas involved in regulation of neuroendocrine and autonomic nervous systems, mental stress can lead to hyperreactivity of vascular smooth muscle cells, autonomic nervous system dysfunction, oxidative stress, vascular inflammation, and endothelial dysfunction, resulting in an increased propensity to coronary vasospasm.25-27
Furthermore, in line with previous studies,28-30 our experience demonstrates that performing a comprehensive invasive diagnostic assessment for the diagnosis of the specific endotype in INOCA and ANOCA patients is safe and is associated with a low rate of mild and transient complications. For all these reasons, patients and clinicians should be reassured about the lack of serious complications and cardiologists should be strongly encouraged to implement a specific diagnostic and therapeutic program in these patients. Indeed, the availability of such a program for INOCA and ANOCA patients may have significant clinical and therapeutic implications, as, in our experience, it resulted in substantial changes in medications and a marked improvement at the 3-month follow-up of the SAQ questionnaire regarding physical limitations, angina frequency, and disease perception. The lower and nonsignificant improvement in the other parameters (eg, angina frequency and treatment satisfaction) could be attributed to the already high baseline values (74.5 ± 19.9 and 69.6 ± 11.9, respectively). Similarly, the absence of a significant improvement in the EQ-5D questionnaire at 3 months might be due to the short follow-up period or the fact that it is a nondisease-specific questionnaire designed to describe and assess patients’ health status and is intended to complement other quality-of-life measures.31
Study limitations
Some limitations of this study should be acknowledged. First, this is a single-center study with a relatively small sample size and short follow-up. Second, we did not perform a cost-analysis and therefore we cannot speculate on the impact of the NOCA program on health care-related costs. Further studies in larger ANOCA and INOCA populations are warranted. Finally, the absence of a control group precluded a thorough assessment of the improvement in the quality of life among these patients.
CONCLUSIONS
Our experience demonstrates that a specific diagnostic and therapeutic protocol (NOCA program) can be easily and safely implemented in routine clinical practice. Such a protocol could ensure the best care for INOCA and ANOCA patients, as well as improve their quality of life and avoid inappropriate treatments and incomplete investigations. Future evidence from randomized clinical trials or recommendations from international clinical guidelines supporting the implementation of a specific protocol in these patients are strongly warranted.
FUNDING
This study received no funding.
ETHICAL CONSIDERATIONS
The study protocol complied with the Declaration of Helsinki and the study was approved by our Institutional Review Committee. All patients gave written informed consent to be included in this program and study. The clinical ethics committee gave their approval for a retrospective analysis of the data collected. In this work, the possible variables of sex and gender have been taken into account.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence tools were used during the preparation of this work.
AUTHORS’ CONTRIBUTIONS
R. Rinaldi, F. Spione, F.M. Verardi: data extraction and analysis and manuscript drafting; R. Rinaldi, F. Spione, S. Brugaletta: design and manuscript revision; P. Vidal Calés, V. Arévalos, R. Gabani, D. Cánovas, M. Gutiérrez, M. Pardo, R. Domínguez, L. Pintor, X. Torres, X. Freixa, A. Regueiro, O. Abdul-Jawad Altisent, M. Sabaté: manuscript revision. All authors have read and agreed to the published version of the manuscript.
CONFLICTS OF INTEREST
The authors have nothing to disclose.
ACKNOWLEDGMENTS
F. Spione has been supported by a research grant provided by the Cardiopath PhD program.z
WHAT IS KNOWN ABOUT THE TOPIC?
- Up to 60% to 70% of patients with angina and/or documented myocardial ischemia do not have angiographic evidence of obstructive coronary artery disease. This condition is defined as angina with no obstructed coronary arteries (ANOCA) or ischemia with no obstructed coronary arteries (INOCA) when associated with evidence of myocardial ischaemia. There are still concerns about the implementation in real practice of a systematic diagnostic and therapeutic approach in INOCA and ANOCA patients, potentially impacting outcomes and quality of life.
WHAT DOES THIS STUDY ADD?
- The implementation of a specific protocol (NOCA program) in patients with a diagnosis of nonobstructive CAD is feasible and allowed parsimonious use of medical resources. A comprehensive invasive diagnostic assessment in INOCA or ANOCA patients is safe and is associated with a low rate of mild and transient complications. The availability of a specific diagnostic and therapeutic program for INOCA and ANOCA patients may have important clinical and therapeutic implications, as, in our experience, it led to significant changes in medications and a notable improvement at 3 months of follow-up in the SAQ questionnaire regarding physical limitations, angina frequency, and perception of the disease.
REFERENCES
1. Roth GA, Mensah GA, Johnson CO, et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019:Update From the GBD 2019 Study. J Am Coll Cardiol. 2020;76:2982-3021.
2. Patel MR, Peterson ED, Dai D, et al. Low diagnostic yield of elective coronary angiography. N Engl J Med. 2010;362:886-895.
3. Neumann FJ, Sechtem U, Banning AP, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41:407-477.
4. Jespersen L, Hvelplund A, Abildstrøm SZ, et al. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2012;33:734-744.
5. Taqueti VR, Solomon SD, Shah AM, et al. Coronary microvascular dysfunction and future risk of heart failure with preserved ejection fraction. Eur Heart J. 2018;39:840-849.
6. Kunadian V, Chieffo A, Camici PG, et al. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology &Microcirculation Endorsed by Coronary Vasomotor Disorders International Study Group. Eur Heart J. 2020;41:3504-3520.
7. Ford TJ, Stanley B, Good R, et al. Stratified Medical Therapy Using Invasive Coronary Function Testing in Angina:The CorMicA Trial. J Am Coll Cardiol. 2018;72:2841-2855.
8. Ford TJ, Stanley B, Sidik N, et al. 1-Year Outcomes of Angina Management Guided by Invasive Coronary Function Testing (CorMicA). JACC Cardiovasc Interv. 2020;13:33-45.
9. Candreva A, Gallinoro E, van 't Veer M, et al. Basics of Coronary Thermodilution. JACC Cardiovasc Interv. 2021;14:595-605.
10. Montone RA, Meucci MC, De Vita A, Lanza GA, Niccoli G. Coronary provocative tests in the catheterization laboratory:Pathophysiological bases, methodological considerations and clinical implications. Atherosclerosis. 2021;318:14-21.
11. Ford TJ, Ong P, Sechtem U, et al. Assessment of Vascular Dysfunction in Patients Without Obstructive Coronary Artery Disease:Why, How, and When. JACC Cardiovasc Interv. 2020;13:1847-1864.
12. Gutiérrez E, Gómez-Lara J, Escaned J, et al. Assessment of the endothelial function and spasm provocation test performed by intracoronary infusion of acetylcholine. Technical report from the ACI-SEC;REC Interv Cardiol. 2021;3:286-296.
13. Beltrame JF, Crea F, Kaski JC, et al. International standardization of diagnostic criteria for vasospastic angina. Eur Heart J. 2017;38:2565-2568.
14. Ong P, Camici PG, Beltrame JF, et al. International standardization of diagnostic criteria for microvascular angina. Int J Cardiol. 2018;250:16-20.
15. Jespersen L, Abildstrøm SZ, Hvelplund A, Prescott E. Persistent angina:highly prevalent and associated with long-term anxiety, depression, low physical functioning, and quality of life in stable angina pectoris. Clin Res Cardiol. 2013;102:571-581.
16. Chan PS, Jones PG, Arnold SA, Spertus JA. Development and validation of a short version of the Seattle angina questionnaire. Circ Cardiovasc Qual Outcomes. 2014;7:640-647.
17. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20:1727-1736.
18. Jespersen L, Abildstrom SZ, Hvelplund A, et al. Burden of hospital admission and repeat angiography in angina pectoris patients with and without coronary artery disease:a registry-based cohort study. PLoS One. 2014;9:e93170.
19. Smaardijk VR, Lodder P, Kop WJ, van Gennep B, Maas AHEM, Mommersteeg PMC. Sex- and Gender-Stratified Risks of Psychological Factors for Incident Ischemic Heart Disease:Systematic Review and Meta-Analysis. J Am Heart Assoc. 2019;8:e010859.
20. Mehta PK, Hermel M, Nelson MD, et al. Mental stress peripheral vascular reactivity is elevated in women with coronary vascular dysfunction:Results from the NHLBI-sponsored Cardiac Autonomic Nervous System (CANS) study. Int J Cardiol. 2018;251:8-13.
21. Konst RE, Elias-Smale SE, Lier A, Bode C, Maas AHEM. Different cardiovascular risk factors and psychosocial burden in symptomatic women with and without obstructive coronary artery disease. Eur J Prev Cardiol. 2019;26:657-659.
22. Gomez MA, Merz NB, Eastwood JA, et al. Psychological stress, cardiac symptoms, and cardiovascular risk in women with suspected ischaemia but no obstructive coronary disease. Stress Health. 2020;36:264-273.
23. Bekendam MT, Vermeltfoort IAC, Kop WJ, Widdershoven JW, Mommersteeg PMC. Psychological factors of suspect coronary microvascular dysfunction in patients undergoing SPECT imaging. J Nucl Cardiol. 2022;29:768-778.
24. Hammadah M, Kim JH, Al Mheid I, et al. Coronary and Peripheral Vasomotor Responses to Mental Stress. J Am Heart Assoc. 2018;7:e008532.
25. Shah A, Chen C, Campanella C, et al. Brain correlates of stress-induced peripheral vasoconstriction in patients with cardiovascular disease. Psychophysiology. 2019;56:e13291.
26. Hung MY, Mao CT, Hung MJ, et al. Coronary Artery Spasm as Related to Anxiety and Depression:A Nationwide Population-Based Study. Psychosom Med. 2019;81:237-245.
27. Crea F, Montone RA, Rinaldi R. Pathophysiology of Coronary Microvascular Dysfunction. Circ J. 2022;86:1319-1328.
28. Probst S, Seitz A, Martínez Pereyra V, et al. Safety assessment and results of coronary spasm provocation testing in patients with myocardial infarction with unobstructed coronary arteries compared with patients with stable angina and unobstructed coronary arteries. Eur Heart J Acute Cardiovasc Care.2020:2048∖20932422.
29. Montone RA, Rinaldi R, Del Buono MG, et al. Safety and prognostic relevance of acetylcholine testing in patients with stable myocardial ischaemia or myocardial infarction and nonobstructive coronary arteries. EuroIntervention 2022;18:e666-e676.
30. Rinaldi R, Salzillo C, CaffèA, Montone RA. Invasive Functional Coronary Assessment in Myocardial Ischemia with Non-Obstructive Coronary Arteries:from Pathophysiological Mechanisms to Clinical Implications. Rev Cardiovasc Med. 2022;23:371.
31. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16:199-208.
- Excimer laser coronary atherectomy in severely calcified lesions: time to bust the myth
- Effectiveness of the DyeVert Power XT system during percutaneous coronary interventions
- Thermodilution assessment of vasoreactivity and microvascular function in the absence of obstructive coronary artery disease
- Design of the ROLLERCOASTR trial: rotational atherectomy, lithotripsy or laser for the management of calcified coronary stenosis







Interviews

An interview with Bruno Scheller
aServicio de Cardiología, Hospital Universitario de La Princesa, Instituto de Investigación Sanitaria de La Princesa (IIS-IP), Universidad Autónoma de Madrid, Spain
bCentro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain




