
A 77-year-old woman was admitted for non–ST-segment elevation acute coronary syndrome, Killip class III. The emergency cardiac catheterization showed a chronic non-occlusive lesion in the mid left anterior descending coronary artery, which was treated. The clinical course, after recovery of left ventricular ejection fraction, suggested the presence of tako-tsubo syndrome (figure 1A,B).
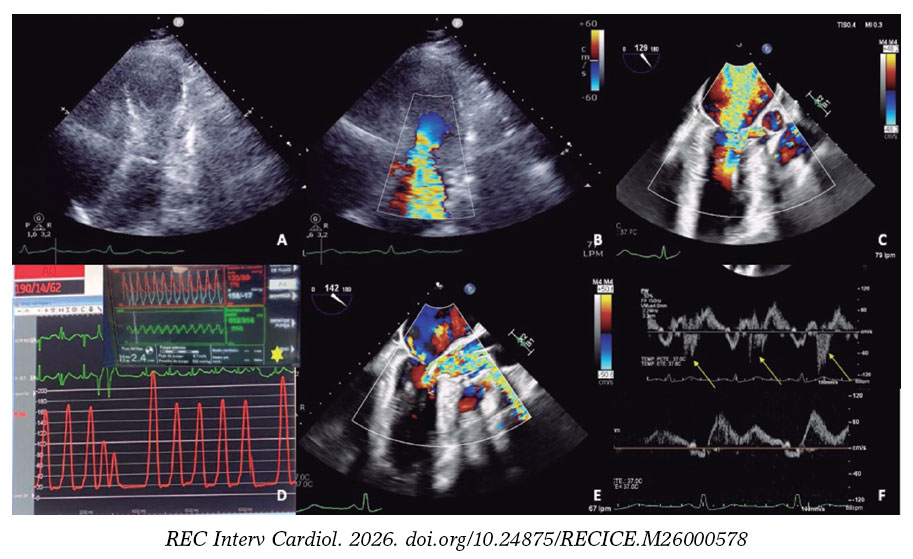
Figure 1.
Despite the administration of fluid therapy and esmolol to reduce dynamic left ventricular outflow tract obstruction (DLVOTO), the patient progressed to SCAI-D cardiogenic shock and required vasopressors, intubation, and intra-aortic balloon pump implantation at a 1:3 ratio to avoid exacerbating DLVOTO. Given the ongoing deterioration, escalation to Impella CP (Abiomed, Inc., United States) as a bridge to recovery was decided. Organic mitral valve disease was ruled out. Since the mitral regurgitation was due to systolic anterior motion (figure 1C; video S1), an emergency septal ablation was planned.
Implantation of the Impella-CP device (figure 1D, asterisk), with flow adjusted to 2.4 L/min (P4) to prevent suction, resulted in immediate hemodynamic and respiratory improvement, as well as a reduction in mitral regurgitation (figure 1E,F; arrows indicate the systolic S wave). A second septal branch (SB) showed extrinsic compression and was selected after confirmation of septal perfusion (figure 2A; arrow indicates second SB; asterisk: first SB). Two coils were deployed (figure 2B) due to potential reversibility, resulting in immediate flow reduction and DLVOTO improvement.
After 24 hours, the patient’s hemodynamic status deteriorated. Due to a slight increase in cardiac enzymes and recurrence of DLVOTO, alcohol ablation of the second SB was performed. Because basal septal contractility persisted (figure 2C, oval), occlusion of the first SB was also undertaken. Due to the impossibility of selective catheterization (figure 2D), a drug-eluting stent was implanted in the proximal left anterior descending coronary artery; thereafter, basal septal akinesia and mild mitral regurgitation were observed (video S2).
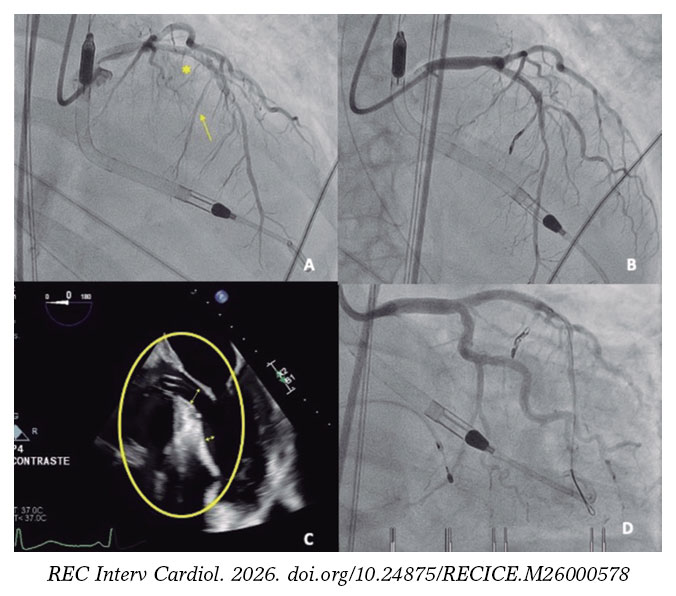
Figure 2.
This case demonstrates that ventricular unloading with an Impella device may be considered in complicated tako-tsubo syndrome and describes for the first time the sequential application of 3 different septal ablation techniques in this context.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
This article fully complies with the recommendations outlined in the Declaration of Helsinki. There are no considerations regarding ethnicity, race, or sex. Informed consent was obtained for the procedures as well as for the dissemination and publication of the case.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence was used in the preparation of this article.
AUTHORS’ CONTRIBUTIONS
R. Martínez-González participated in drafting the initial manuscript and subsequent editing. M.Á. Martín-Arena participated in drafting and editing. A. Jurado-Román, A. Rodríguez-Chaverri, S.O. Rosillo-Rodríguez, and R. Moreno reviewed and corrected the text. Final editing was performed by R. Martínez-González and A. Jurado-Román. All authors approved the final article.
CONFLICTS OF INTEREST
R. Moreno is an associate editor of REC: Interventional Cardiology; the journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. The remaining authors declared no conflicts of interest whatsoever.
SUPPLEMENTARY DATA
Vídeo 1. Martínez-González R. DOI: 10.24875/RECICE.M26000578
Vídeo 2. Martínez-González R. DOI: 10.24875/RECICE.M26000578












