
We present the case of a 16-year-old girl with a prenatal diagnosis of Ebstein’s anomaly and an atrial septal defect with severe tricuspid regurgitation.
In 2020, the patient was referred due to functional deterioration. Surgical repair included the implantation of a 26-mm Contour 3D tricuspid annuloplasty ring (Medtronic, United States) with the cone reconstruction technique and closure of the atrial septal defect. During the postoperative follow-up, the patient developed moderate paravalvular leak lateral to the ring that progressed to severe regurgitation with moderate right ventricular dilatation without dysfunction a year and a half later. The patient experienced no episodes of heart failure until 2 years after surgery.
Cardiac catheterization was performed via transjugular and right femoral access under general anesthesia and transesophageal echocardiography guidance, revealing the presence of a 13 mm × 10 mm leak posterolateral to the tricuspid annuloplasty ring that appeared as a 15 mm leak on ventriculography (figure 1). The first closure attempt with a 14-mm Konar MF device (Lifetech, China) did not achieve complete closure or attachment at the defect. Therefore, a second attempt was made with an 18-mm Amplatzer Muscular VSD device (Abbott, United States), which achieved proper attachment and almost complete occlusion (figure 2). After release, minimal residual regurgitation was confirmed by transesophageal echocardiography (figure 3 and video of the supplementary data). There were no irregular heart rhythms or repolarization abnormalities.
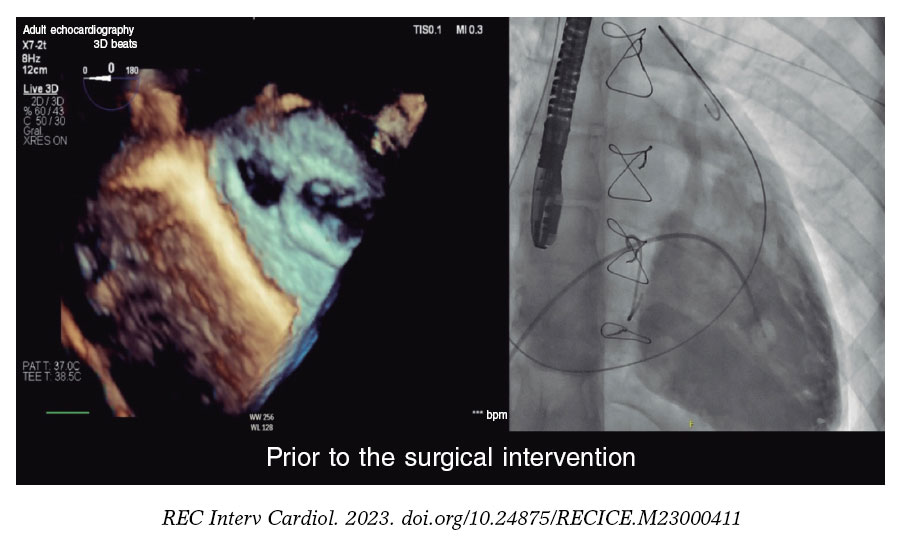
Figure 1.
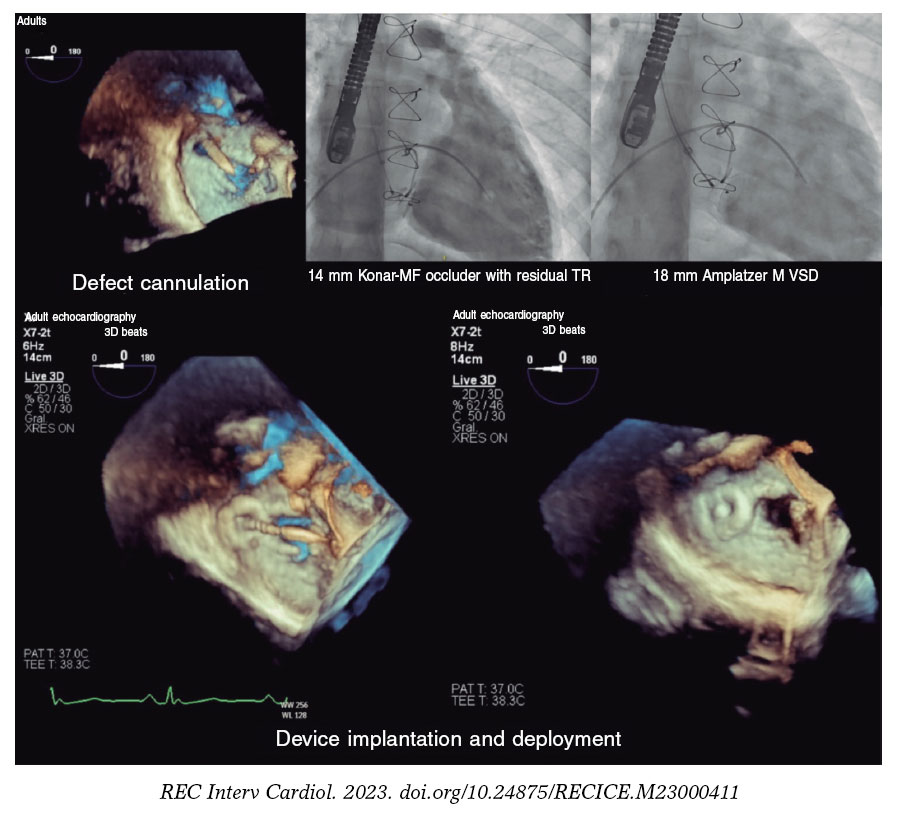
Figure 2.
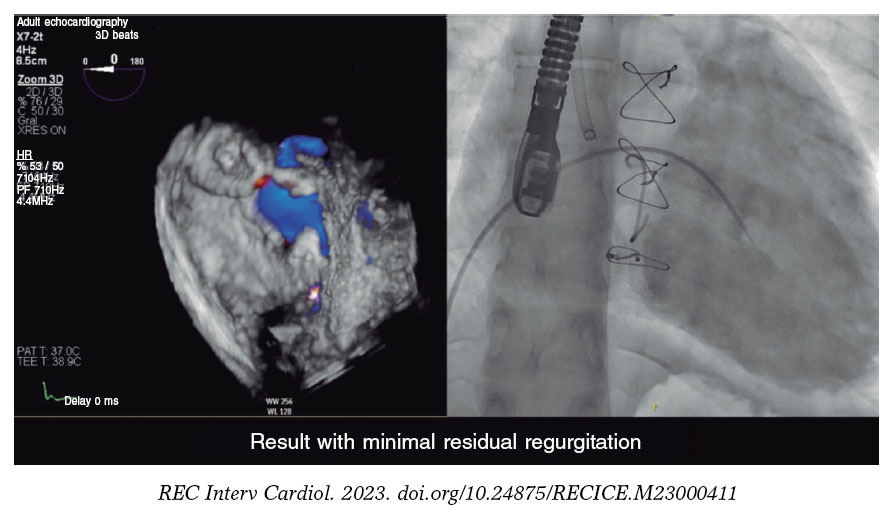
Figure 3.
The patient was discharged 24 hours after the procedure, with the initiation of aspirin therapy. Follow-up revealed a normal electrocardiogram, with minimal residual regurgitation, and no hemolysis. The patient reported improvement during exertion.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
This case was approved for publication by the pediatric cardiology unit, and did not require further evaluations by the research ethics committee. The parents of the minor and the mature minor herself gave their prior written informed consent. Because this is a presentation of an isolated case, the SAGER guidelines did not need to be followed.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
No artificial intelligence tool has been used during the preparation of this work.
AUTHORS’ CONTRIBUTIONS
All authors participated in the procedure, image review, and manuscript drafting.
CONFLICTS OF INTEREST
None declared.
ACKNOWLEDGEMENTS
We wish to thank the pediatric cardiology unit at Hospital Universitario La Paz for their professionalism and attention to publication details. Final results are a direct consequence of their excellent patient care.
SUPPLEMENTARY DATA
Vídeo 1. Guillén Mendoza NB. DOI: 10.24875/RECICE.M23000411









