
A fifty-five year-old hypertensive and former smoker male admitted with signs of typical chest pain, left bundle brunch block, and normal troponin levels. The angiography revealed 2-vessel, left circumflex and right coronary artery disease. The latter was treated with a stent and for the circumflex coronary artery an instantaneous wave-free ratio (iFR)-guided intervention was decided. Then, a second conventional guidewire was used for stabilization purposes. Figure 1A shows initial angiography (video 1 of the supplementary data), equalization of proximal and distal pressures (figure 1B and figure 2A), plain balloon angioplasty and iFR wedge pressure determination (figure 1C and figure 2D), angiographic result after balloon-angioplasty (figure 1D), iFR determination after balloon angioplasty (figure 1E and figure 2E,F), and final result (figure 1F, figure 2G,H and video 1 of the supplementary data).

Figure 1
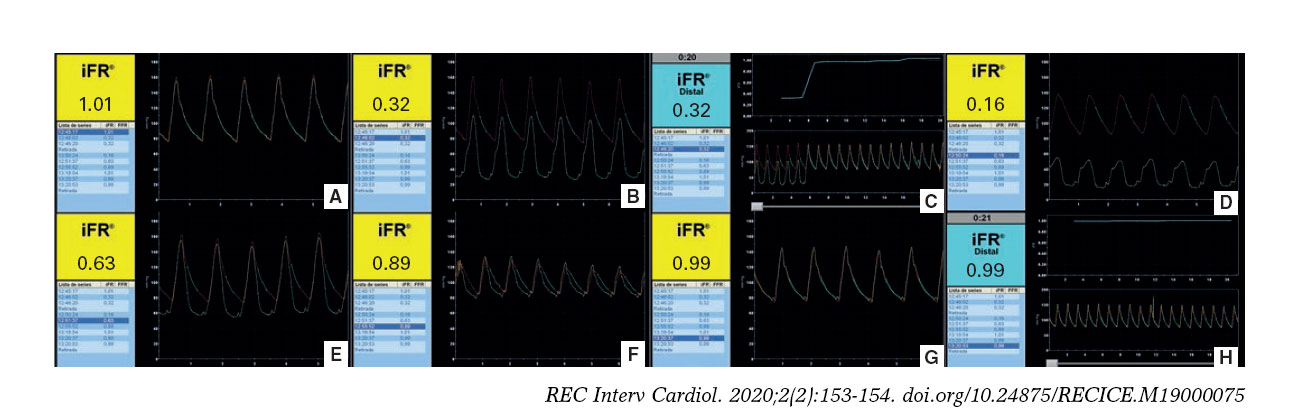
Figure 2
Figure 2A shows equalization, positive iFR after the lesion (figure 2B), sudden iFR change during the pullback suggestive of focal stenosis (figure 2C), iFR during balloon inflation without antegrade flow (iFR wedge pressure) (figure 2D), iFR 1 minute after the angioplasty (figure 2E), 4 minutes later without maneuvers or drugs (figure 2F), final iFR and iFR pullback, respectively, after stenting (figure 2G,H).
The still low iFR (0.63) immediately after balloon angioplasty was probably due to microcirculation and collateral flow. Thus, flow increase after the angioplasty balloon deflation is expected following arteriole compensatory vasodilation. This compensatory increased flow elevates the translesional pressure gradient resulting in lower iFR values than expected after lesion treatment. However, the iFR increased 4 minutes later (from 0.63 to 0.89), a reasonable time to recover the conditions at rest including the baseline vascular arteriolar tone, confirming the good physiological result of balloon-angioplasty.
In conclusion, resting physiological indexes need to be performed carefully and timely to avoid bias and issues when interpreting the results.
SUPPLEMENTARY DATA
Video 1. Núñez-Gil I. DOI:10.24875/RECICE.M19000075
Video 2. Núñez-Gil I. DOI:10.24875/RECICE.M19000075









