
To the Editor,
We present the case of a 73-year-old woman with arterial hypertension, morbid obesity (122 kg, body mass index = 44), and chronic lower limb swelling with recurrent skin infections due to multi-drug resistant microorganisms. She had a significant degenerative mitral regurgitation with moderate pulmonary hypertension and dyspnea, and NYHA functional class II. Despite the patients’ low surgical risk scores (1.5% and 1.29% in the Society of Thoracic Surgeons and EuroSCORE II scales, respectively) she was considered noneligible for mitral surgery because of her obesity and perioperative infectious risk. The heart team studied the case and decided to treat the mitral regurgitation with percutaneous treatment whose overall risk is lower. The patient’s informed consent was obtained for data publication in observance of the Declaration of Helsinki ethical principles.
While planning the procedure, the presence of degenerative mitral regurgitation was confirmed associated with chord rupture and posterior leaflet eversion (flail) of the P1 scallop (figure 1A,B, asterisks) of 9 mm in height and 14 mm of amplitude. Quantitative parameters suggested a 1.3 cm2 anatomical regurgitant orifice, a 50 mL regurgitant volume, and a 51% regurgitant fraction with hemodynamic repercussion on the right superior pulmonary vein and systolic component reversal. The mitral valve apparatus was preserved with a 7.2 cm2 area according to the 3D planimetry. However, the mean gradient was somehow higher (4 mmHg) probably due to the mitral regurgitation hyperflow and an increased cardiac output (estimated in 11 L/min) in atrial fibrillation at 125 beats per minute.
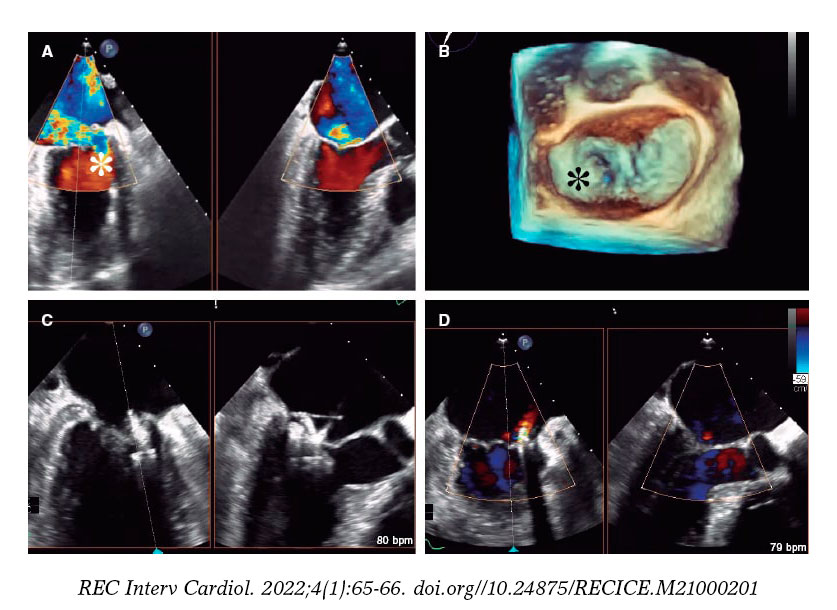
Figure 1. PASCAL Ace device implantation in a patient with complex mitral regurgitation. A: bi-plane color Doppler transesophageal echocardiography imaging. B: 3D reconstruction of the mitral valve showing the P1 eversion (asterisks) accompanied by a significant jet towards the septum. C: final clasping of the leaflets. D: very mild final regurgitant jet.
The defect was repaired using the PASCAL Ace device (Edwards Lifesciences, Irvine, CA, United States). This is a percutaneous mitral valve repair system to correct mitral regurgitation using the edge-to-edge technique via femoral vein and transseptal access to reach the left atrium. The PASCAL device is basically different from the MitraClip (Abbott Laboratories, Abbott Park, IL, United States) in that it has a central spacer to refill the regurgitant orifice and an elongation feature to remove it from the ventricle (at the eversion site) that makes it safer. The PASCAL Ace is a variant of the original design with a lower amplitude compared to the latter (6 mm vs 10 mm), and a smaller central spacer (2 mm vs 5 mm). The objective of these changes was to be able to treat more complex anatomies like our case. Due to the paracommissural anatomy, the original device could easily tangle up in the chordae of the subvalvular apparatus.
The procedure was performed under general anesthesia and continuous echocardiographic monitoring. Access to the left atrium occurred through a transeptal puncture 43 mm from the valvular plane. The clasping of the leaflets was attempted repeatedly for the complete correction of the anatomical defect. An independent clasping system was used to optimize the anterior and posterior leaflet grasping. In 1 of the attempts, the device got trapped into the subvalvular apparatus, but it could be easily retrieved thanks to the device elongation. The eversion was eventually immobilized (figure 1C) with an early clasping maneuver of both leaflets and significant optimization towards the posterior leaflet. This reduced mitral regurgitation significantly (figure 1D), improved the hemodynamic parameters, and returned the patient to a normal sinus rhythm. The final gradient was reduced down to 2 mmHg after the hemodynamic improvement with a final mitral area of 4.4 cm2. Clinical evolution was favorable and without complications. The patient was discharged from the hospital 24 hours after the procedure and functional class improved slightly at the follow-up.
The percutaneous treatment of severe mitral regurgitation is well-established today.1 There are different devices available in the market, although the edge-to-edge therapy that simulates the Alfieri surgical technique, basically with a MitraClip device, is the most popular one. Also, it is the one on which there is more evidence available to this date.2-4 The PASCAL system5,6 has several particular features: the central spacer, the independent clasping of the leaflets, and the possibility of elongating the device inside the ventricle for retrieval purposes. The central spacer seems to generate less tension inside the mitral valve, especially in mitral regurgitations of functional mechanism with significant tension. The independent grasping of the leaflets facilitates maneuvers to optimize the insertion of the leaflets securing a more stable fixation of these. However, to avoid small valvular distortions that may trigger unexpected final regurgitations, the first grasp is performed with a simultaneous reduction of the clasping followed by an independent clasping to optimize results. The possibility of elongating the device when trapped inside the subvalvular apparatus makes its retrieval much easier. The PASCAL Ace system is less voluminous, but it can increase the insertion of the leaflets up to 1 mm. This facilitates treating more complex anatomies when there is a risk of interfering significantly with neighboring structures. This was the very first experience in Spain with the PASCAL Ace system.
FUNDING
This study has received no funding whatsoever.
AUTHORS’ CONTRIBUTION
All the authors have contributed substantially to the concept, design, analysis, and interpretation of this manuscript. They also conducted a critical review of its intellectual content and approved it for publication. Finally, they take full responsibility on the truthfulness of this study.
CONFLICTS OF INTEREST
D. Arzamendi received personal fees from Edwards Lifesciences while conducting this study.
REFERENCES
1. Bonow RO, O'Gara PT, Adams DH, et al. 2019 AATS/ACC/SCAI/STS Expert Consensus Systems of Care Document:Operator and Institutional Recommendations and Requirements for Transcatheter Mitral Valve Intervention. J Am Coll Cardiol. 2020;76:96-117.
2. Mauri L, Foster E, Glower DD, et al. 4-Year results of a randomized controlled trial of percutaneous repair versus surgery for mitral regurgitation. J Am Coll Cardiol. 2013;62:317-328.
3. Stone GW, Lindenfeld J, Abraham WT, et al. Transcatheter Mitral-Valve Repair in Patients with Heart Failure. N Engl J Med. 2018;379:2307-2318.
4. Obadia J-F, Messika-Zeitoun D, Leurent G, et al. Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation. N Engl J Med. 2018;379:2297-2306.
5. Lim DS, Kar S, Spargias K, et al. Transcatheter Valve Repair for Patients With Mitral Regurgitation:30-Day Results of the CLASP Study. JACC Cardiovasc Interv. 2019;12:1369-1378.
6. Fernández Peregrina E, González Salvado V, Asmarats Serra L, Li CH, Serra Peñaranda A, Arzamendi Aizpurua D. Transcatheter mitral valve repair with the PASCAL system:initial experience. Rev Esp Cardiol. 2020;73:594-595.









