
To the Editor,
Currently, transradial approach is the most widely used access route both in coronary angiographies and percutaneous coronary interventions.1 However, it is not rare to find anatomical difficulties like severe spasm, small-caliber vessel, loops or tortuosities that cannot be overcome with the usual techniques and lead to access route changes eventually.2 In these situations, the advance of the catheter can dissect or perforate the artery and cause hematomas or even compartmental syndrome, although this entity is rare.3
As the main cause of resistance when advancing the catheter, Patel et al.4 identified the so-called razor effect exerted by the catheter distal border on the vessel wall (figure 1A), a mechanism that has been confirmed in optical coherence tomography studies.5 These same authors described the balloon-assisted tracking (BAT) technique4 that consists of inflating an angioplasty balloon that partially protrudes across the catheter distal border to keep its coaxial position with the artery avoiding the razor effect and providing better maneuverability (figure 1B). Therefore, the anatomical difficulty is crossed using a 0.014 in soft tip angioplasty guidewire. Afterwards, a 1.5 mm to 2.0 mm semicompliant balloon is inflated between 6 and 8 atm at the tip of the catheter and advanced en bloc beyond the anatomical problem (figure 2). Once the difficulty has been overcome with the catheter, both the balloon and the guidewire are retrieved to continue the procedure with the usual technique. All of it should be performed under strict fluoroscopic follow-up.
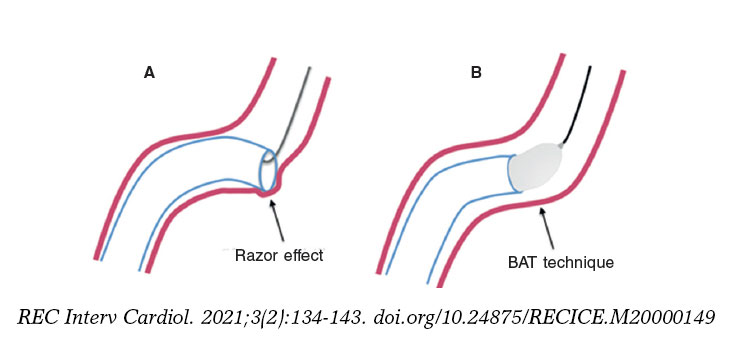
Figure 1. A: Razor effect of the catheter distal border over the vessel wall. B: correction of the razor effect with an angioplasty balloon inflated at the tip of the catheter. BAT, balloon-assisted tracking.
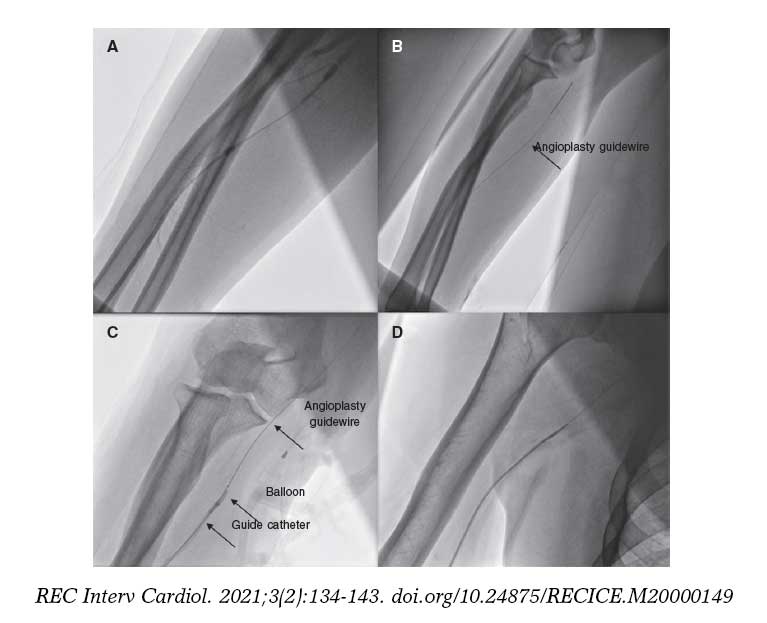
Figure 2. A: diffuse severe spasm of radial artery. B: advance of the angioplasty guidewire. C: catheter with balloon inflated in the distal border. D: crossing of the anatomical difficult.
During the period from January 2019 through January 2020 we used this technique in 28 patients (2.3% of all transradial approaches attempted). In all of them, after the correct canalization of the artery, it was impossible to advance the catheter. Table 1 shows the patients’ clinical characteristics, and reasons why the BAT technique was used. On 2 occasions it was used in the primary percutaneous coronary intervention setting. Informed consent was obtained from patients by telephone for the dissemination of the data included in the study.
Table 1. Clinical profile and reasons to proceed with balloon-assisted tracking (BAT) technique
| Demographic characteristics | N = 28 |
|---|---|
| Age (years) | 67 ± 14 [36-91] |
| Women | 15 (54) |
| Arterial hypertension | 16 (57) |
| Smoking | 10 (36) |
| Diabetes mellitus | 8 (29) |
| Dyslipidemia | 7 (25) |
| Peripheral arteriopathy | 13 (46) |
| Access using the right radial artery | 15 (54) |
| Acute coronary syndrome | 22 (79) |
| Percutaneous coronary intervention | 18 (64) |
| Difficult moment during radial access | |
| Advance of 0.035 in guidewire | 1 (4) |
| Advance of 5-Fr diagnostic catheter | 10 (36) |
| Exchange of 5-Fr diagnostic catheter for 6-Fr therapeutic catheter | 17 (61) |
| Indication for using the BAT technique | |
| Unsolved severe spasm | |
| Small caliber | 7 (25) |
| Severe radial or brachial tortuosity | 3 (11) |
| Radial loop | 3 (11) |
| Subclavian loop | 1 (4) |
|
Data are expressed as no. (%), mean ± standard deviation or median [interquartile range]. |
|
To proceed with the BAT technique, 2 mm × 12 mm semicompliant balloons were used in 6-Fr catheters and 1.5 mm × 12 mm semicompliant balloons in 5-Fr catheters.
The success of the technique, defined as the overcome of the anatomical difficulty to be able to perform the procedure without having to change the access route, was achieved in 93% of the cases. In only 2 patients it was necessary to change the access route: one case of a heavily calcified small-caliber radial artery that made it impossible to advance the 0.014 in guidewire (indispensable step to use the BAT technique) and another case of a subclavian loop plus severe aortic elongation that could not be overcome with the BAT technique. None of the patients had vascular complications associated with the technique.
Therefore, we agree with other authors that the BAT is an easy-to-use technique that can improve the rates of success of radial access.6 Although in our group of patients there were only 2 cases of primary percutaneous coronary intervention, this scenario is especially sensitive to the need for access route change where the BAT technique also proved efficient.7 It is essential that in cases of minimal resistance while advancing the catheter an angiography should be performed to assess the anatomical difficulty and, once the problem has been defined, the BAT should be used early on to reduce the rate of complications.
FUNDING
None.
AUTHORS' CONTRIBUTIONS
All authors have contributed substantially to the idea, design and data acquisition of the study.
CONFLICTS OF INTEREST
None declared.
REFERENCES
1. Cid Álvarez AB, Rodríguez Leor O, Moreno R, Pérez de Prado A. Spanish Cardiac Catheterization and Coronary Intervention Registry. 28th Official Report of the Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology (1990-2018). Rev Esp Cardiol. 2019;72:1043-1053.
2. Azzalini L, Khan R, Al-Hawwas M, et al. Effect of radial-to-femoral access crossover on adverse outcomes in primary percutaneous coronary intervention. Am J Cardiol. 2014;114:1165-1173.
3. Goirigolzarri Artaza J, Casado Álvarez R, Benítez Peyrat J, León Aliz E, Goicolea J, García Touchard A. Síndrome compartimental agudo de la mano tras un cateterismo transradial. Rev Esp Cardiol. 2017;70:672-673.
4. Patel T, Shah S, Pancholy S, Rao S, Bertrand OF, Kwan T. Balloon-assisted tracking:a must-know technique to overcome difficult anatomy during transradial approach. Catheter Cardiovasc Interv. 2014;83:211-220.
5. Merella P, Lorenzoni G, Casu G. Inside the “Razor Effect“:Lessons From Optical Coherence Tomography-What Does Angiography Hide?JACC Cardiovasc Interv. 2019;12:409-410.
6. Wojciuk J, Beijk MA, Goode G, et al. Balloon-assisted tracking technique as 'a way forward'for transradial intervention. Coron Artery Dis. 2019;30:440-447.
7. Obaid D, Hailan A, Chase A, et al. Balloon-Assisted Tracking Use Reduces Radial Artery Access Failure in an Experienced Radial Center and is Feasible During Primary PCI for STEMI. J Invasive Cardiol. 2017;29:219-224.












