Innovation in interventional cardiology
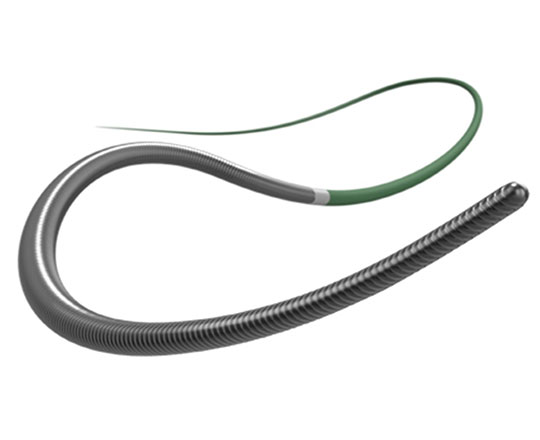
Gladius Ex chronic total occlusion guidewire
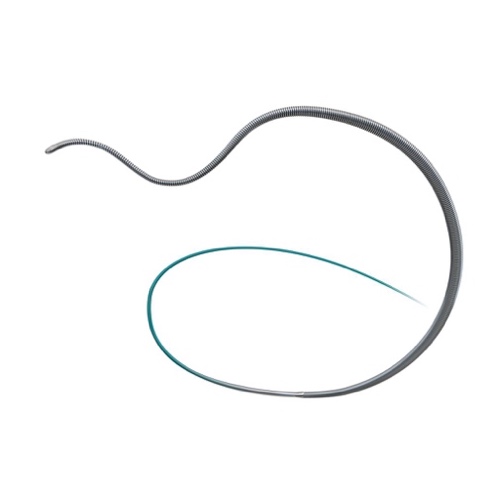
The Gladius guidewire, manufactured by Asahi Intecc (Nagoya, Japan) is designed for peripheral vascular interventions.
It is a polymer guidewire that is used in cases of severely-calcified chronic total occlusion when the vessel architecture is unknown and the guidewire needs to be advanced to bridge the length of the occlusion. The Gladius EX guidewire is exactly the same, but it will have the CE mark for the indication for percutaneous coronary intervention.
Using polymer guidewires for more than 15 minutes in microcatheters designed for use with 0.014’’ guidewires leads to excessive friction that can impede the movement of the guidewire within the catheter and the coronary lesion. The Gladius EX has superior glide to the classic polymeric guidewires within the microcatheter lumen. It allows the tip to be bent into a 1-mm knuckle to pass through the subintimal space if necessary.
The tip weight is 3 g and it is flexible enough to aim it towards the target with a precise torque thanks to its ACT ONE technology – a distal wire surrounding the core all the way to the tip. There is also an exterior 0.014’’ coil all the way to the rounded tip, with a hydrophilic polymer coating. It is very useful in the hybrid strategy for antegrade and retrograde access and dissection re-entry with the Stingray device (Boston Scientific).
Keywords: Chronic Total Occlusion, coronary wire.

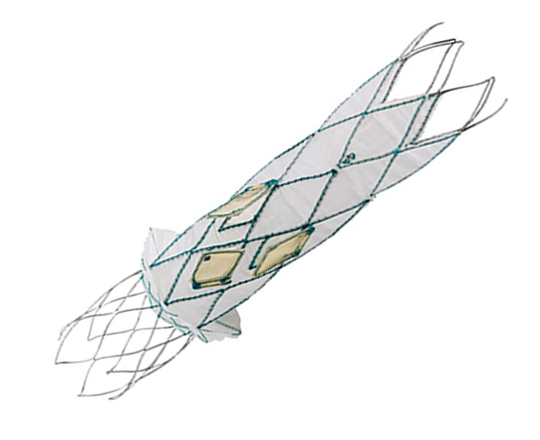
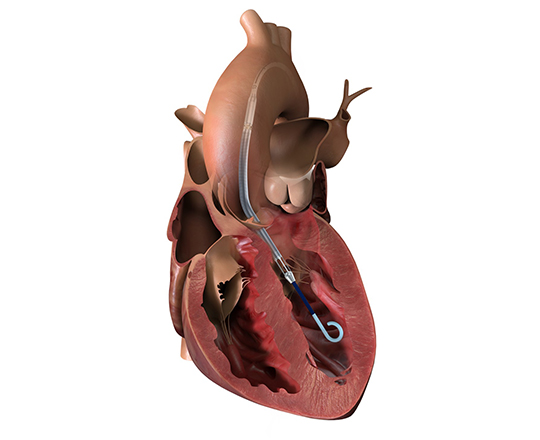
TricValve. Transcatheter bicaval valves
The latest devices under development for the treatment of functional tricuspid regurgitation are transcatheter valves.
In patients with high surgical risk, a system of bicaval valves, such as TricValve, represents an alternative to surgery. The valves consist of a nitinol frame and 3 bovine pericardial leaflets and are available in 25 mm and 29 mm for the superior vena cava and 31 mm and 35 mm for the inferior vena cava.
After implantation of the CAVI system, the caval V wave becomes flattened, while the atrial V wave increases due to the reduced tricuspid regurgitation volume. In the acute phase, the mean caval pressures decrease slightly (2-3 mmHg). In the following weeks, RV remodeling due to the reduced load volume causes a reduction in the vena caval and right atrial pressures1.
The long-term effects on right atrial and right ventricular function are not yet known. However, there are data from 24 months post-implantation that show that the device functions well in patients, with a substantial clinical improvement observed, from NYHA (New York Heart Association) class IV to class II with normalization of previously abnormal liver function.
The CAVI procedure is a clear example of the growing movement towards minimally-invasive devices in structural cardiology.
1.Figulla HR, Kiss K, Lauten A. Transcatheter interventions for tricuspid regurgitation - heterotopic technology: TricValve. EuroIntervention. 2016;12:116-118
Keywords Tricuspid regurgitation, percutaneous prothetic valve.

DFR: a new resting index
Boston Scientific has introduced a new resting index called the diastolic hyperemia-free ratio (DFR) that is comparable to iFR (instantaneous wave-free ratio) values, as demonstrated in the analysis of 893 waveform tracings from 833 patients in the VERIFY 21 and CONTRAST2 studies.
DFR values are equivalent to iFR. In fact, DFR has a diagnostic accuracy of 98%, with a sensitivity of 96% and specificity of 99%.
The main advantages of DFR are that it does not require an ECG signal, it incorporates 5 heartbeats, it is not necessary to identify the dicrotic notch of the pressure wave, and it uses mean arterial pressure, as well as the diastolic wave-free period.
The cutoff value is 0.89, independently of the diastolic period considered (30%, 65%, or 90% of diastole).
Alongside this advance is the new software added to the Polaris multimodality guidance system. The FFR Link system connects to the control panel via Bluetooth connection, to integrate the new DFR values.
Another technological advance that will be included in the Polaris control panel is the smart minimum FFR (smFFR) algorithm: this system excludes all artefacts from the fractional flow reserve (FFR) study. These artefacts commonly occur when the hemostasis valve is opened, when flushing with physiological saline or when the guidewire is withdrawn, affecting the accuracy of the values. The system has been developed based on algorithms validated by the University of Texas.
1. Hennigan B, Olroyd KG, Berry C, et al. Discordance Between Resting and Hyperemic Indices of Coronary Stenosis Severity. The VERIFY 2 Study (A Comparative Study of Resting Coronary Pressure Gradient, Instantaneous Wave-Free Ratio and Fractional Flow Reserve in an Unselected Population Referred for Invasive Angiography). Circ Cardiovasc Interv. 2016;9. pii: e004016.
2. Nishi T, Johnson NP, De Bruyne B, et al. Influence of Contrast Media Dose and Osmolality on the Diagnostic Performance of Contrast Fractional Flow Reserve. Circ Cardiovasc Interv. 2017;10. pii: e004985. doi: 10.1161/CIRCINTERVENTIONS.117.004985.
Keywords: Coronary pressure wire.

Gaia Next chronic total occlusion guidewire
The Gaia guidewires (Asahi Intecc, Nagoya, Japan), designed specifically for recanalization of chronic total coronary occlusion with precise directional control, have some limitations if the plaque is severely calcified and hardened. In fact, they may even fracture if they are rotated excessively over the plaque without advancing.
To improve their performance, a family of guidewires named Gaia Next has been developed, though they are not yet available in Europe. They incorporate a technology termed XTRAND coil, in which the main outer coil of the guidewire is made of 7 wires woven together to form a rope, which prevents potential fracture. The XTRAND coil surrounds the guidewire core and the ACT ONE inner coil of the conventional Gaia family. This design means that the wires press against each other when the guidewire is turned in an anticlockwise direction, significantly increasing torque control.
The Gaia Next guidewires have a 40-cm hydrophilic coating at the distal portion which improves lubricity, as it avoids them getting trapped in the plaque, something that occasionally occurs with the conventional Gaia guidewires.
They have a micro-cone tip that is much more tapered and slimmer than the conventional Gaia guidewires, and they are available in 3 sizes: Gaia Next 1, Gaia Next 2 and Gaia Next 3.
| Tapered tip | Tip load (gf) | Penetration force (kg/in2 | |
|---|---|---|---|
| Gaia Next 1 | 0,011 in | 2 | 70,8 |
| Gaia Next 2 | 0,012 in | 4 | 141,5 |
| Gaia Next 3 | 0,012 in | 6 | 212,3 |
I anticipate that these new guidewires will improve the success rate of percutaneous intervention in these complex lesions.
Keywords: Chronic Total Occlusion, coronary wire.

I recently became aware of a hemostasis valve that is shorter than standard. The conventional hemostatic valves used in coronary interventional procedures generally measure 76 mm or more and are sufficient for almost all interventions.
The FLO40XR valve (MeritMedical, South Jordan, UT, USA) measures 50 mm, has a 7.3 French inner lumen (0.096’’ or 2.44 mm) and withstands a pressure of 400 psi. It is the shortest valve on the market that allows contrast injection, through a 15 cm extension tube.
Such valves are useful in special cases in which the balloon or stent is not long enough to reach the target area. On occasion, they are needed when we have to dilate the native bed of the left anterior descending artery via a mammary artery graft, in some types of telescopic assembly with several catheters, and in some types of retrograde access. A gain of 2 centimeters can be enough to reach the desired site without having to cut the guide catheter.
Key words: hemostasis valve, coronary interventional procedure.
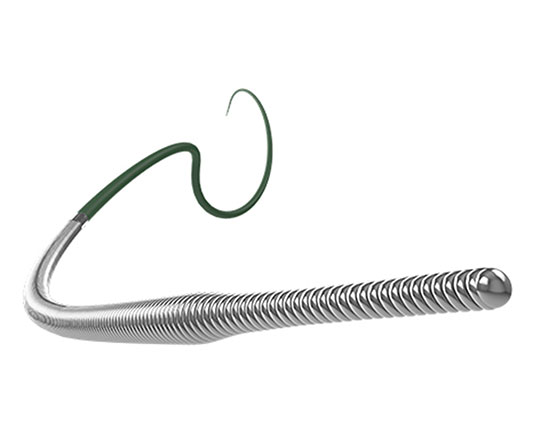
A new guide extension catheter named Telescope (Medtronic) has just been released on the market, and we have already tested it. Its advantage over other available extension catheters is that its structure differs to allow a highly safe and effective catheter release in distal portions of the coronary arteries.
The characteristics of the different parts of the device are as follows:
- Distal segment. The catheter has a coil-based structure, unlike others which contain mesh. The distal portion is more flexible than the proximal portion. The polymer tip measures 2 mm (it has a radiopaque marker) and is produced by extrusion; its flexibility allows deflections that adapt appropriately to the tortuosity of the coronary artery, to calcifications, and to lesions encountered in the coronary lumen, without causing dissection.
- Coating. . The distal segment has a 21 cm hydrophilic-coated jacket that helps safely improve navigation and glide inside the coronary artery. The inner surface of the catheter has a polytetrafluoroethylene coating (PTFE) that reduces friction when devices are passed through it.
- Pushwire. It has a solid, round pushwire that confers greater force and pushability than other types of pushwires or pushtubes (some are flat; others round and hollow), minimizing the risk of kinking.
- On-ramp. Measuring 40 mm and comprising 3 parts: the portion that connects with the catheter, a polymer semi-circular tube and a beveled end. The bevel is long, gradually transitions from the catheter to the pushwire, and has a polymer coating, which reduces potential difficulty with passing and delivering stents. The pushwire also tapers from proximal to distal where it connects with the catheter.
It is available in 6 F (0.056” inner lumen) and 7 F (0.062” inner lumen). This device represents an innovation in the category of guide extension catheters.
Key words: guide extension catheter, coronary interventional procedure.

At EuroPCR 2019, Dr Giovanni Amoroso presented a study on an innovative and distinctive medical device, which uses nanotechnology to monitor and manage potential complications in transradial access. The technology is called ROAM (Radial Occlusion Artery Monitoring). It consists of a monitoring bracelet called IdaFlo Tr (IdaHealth, Florida, USA) that allows continuous assessment of arterial flow, with real-time wireless data transmission on arterial compression.
This device can detect abnormal flow in the radial artery after catheterization and warns the doctor or nurse that the radial compression should be adjusted to avoid complete radial artery occlusion. In fact, it is a telemedicine system that transmits collected data on radial artery blood flow to an iPad application. It is a predictive system that helps improve patient safety and reduces the workload on nursing staff.
Key words: transradial access, radial artery occlusion, coronary interventional procedure.

The JUDO guidewires (Boston Scientific) are designed for complex cases of chronic total coronary occlusion and allow maintained direct tactile feedback of the hardness of the plaque. The combination of an effective penetration force, flexibility and precise torque control make them one of the best crossing guidewires particularly for intraluminal crossing of occlusions.
These guidewires are tapered along the last 60 mm, with a core that is surrounded by coiled filaments and goes all the way to the tip. They are hydrophilic-coated to the tip, which measures 0.008”. They possess an innovative technology, called Micro EMT, which means that the core and coil are tapered to match exactly, to enable intraluminal lesion entry. This design avoids exit into the subintimal space; the flexibility of the distal portion along with the precise torque enables effective intraplaque recanalization. These properties reduce whip effect, an important point when aiming for a 3D (3-dimensional) effect, and minimize the possibility of vessel perforation.
Three guidewires of different specifications are available:
- JUDO 1: Soft intraluminal crossing wire for antegrade microchannels, with 1 gf tip load and a penetration force of 31 gf/mm2.
- JUDO 3: Intermediate intraluminal crossing wire for fibrocalcific lesions, 3 gf tip load and a penetration force of 93 gf/mm2.
- JUDO 6: Extra penetration with excellent control in harder lesions, 6 gf tip load and a penetration force of 185 gf/mm2.
Key words: angioplasty guidewire, total chronic occlusion, coronary interventional procedure.