
CASE RESOLUTION
A scheduled procedure was decided. An 8-Fr 45 cm long Flexor Shuttle-SL introducer guiding sheath (Cook, United States) was inserted via femoral access again. An 8-Fr AL2 guide catheter was inserted into the ostium of the aortocoronary graft with a valve with a body shorter than usual, the FLO40XR hemostasis valve (Merit, United States). Afterwards, a 120 cm straight tip 5-Fr Heartrail ST01 guide catheter was inserted (Terumo, Japan) that was connected to a different FLO40XR valve. The SION blue Extra Support guidewire (Asahi Intecc, Japan) was advanced towards the left circumflex artery, and mounted over it, a 5-Fr GuideLiner guide extension catheter (Teleflex, United States) was advanced. The goal of this telescoping catheter system was to increase support to be able to move the stent forward (figure 1 and figure 2).
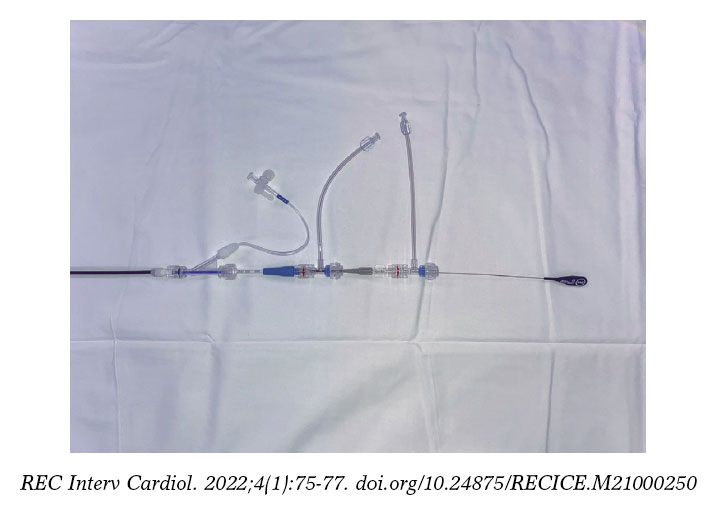
Figure 1. Arrangement of the catheters with their special valves to allow a longer usable length. The valves with the shortest bodies allow longer effective catheter lengths to reach the target lesion.
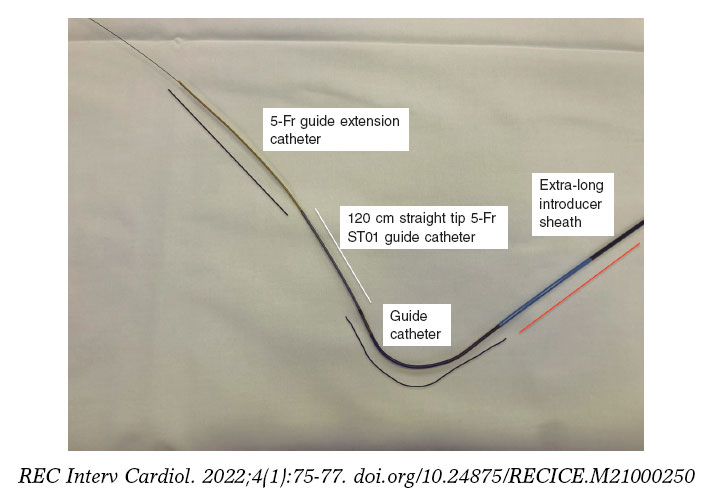
Figure 2. Quadruple telescoping catheter system mounted over the SION blue ES guidewire. The compatibility between the 5-Fr guide extension catheter and the 5-Fr ST01 guide catheter is seen here.
The tip of the GuideLiner catheter was placed in the most proximal region of the lesion. However, when the new 3 mm × 8 mm Resolute Onyx zotarolimus-eluting stent (mounted once again over the GuideLiner) was advanced it failed to cross the lesion (figure 3). The entire telescoping catheter system lost its position with all these crossing attempts, which is why the whole procedure had to start all over again. In the second attempt, the guidewire was advanced spontaneously towards the most distal region of the marginal branch, and when the GuideLiner was advanced it almost passed distal to the lesion (figure 4). This situation occurred because the guidewire lost the steep angulation it had as it moved proximally to the proximal left circumflex artery.
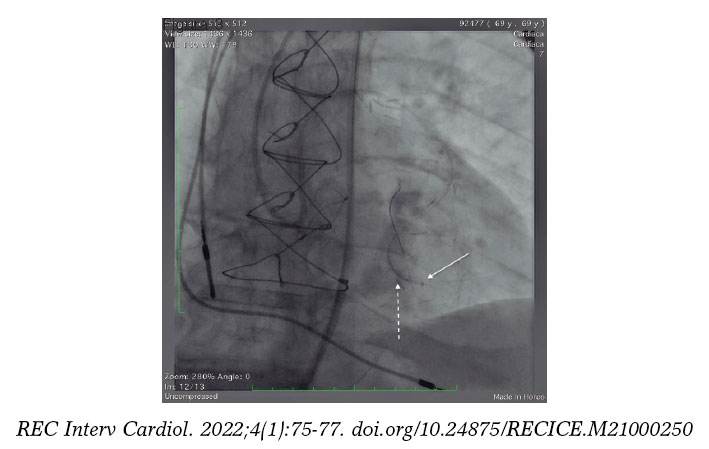
Figure 3. Note the tip of the guide catheter on the lesion proximal zone (dotted arrow), and the stent about to cross the lesion (dotted arrow).
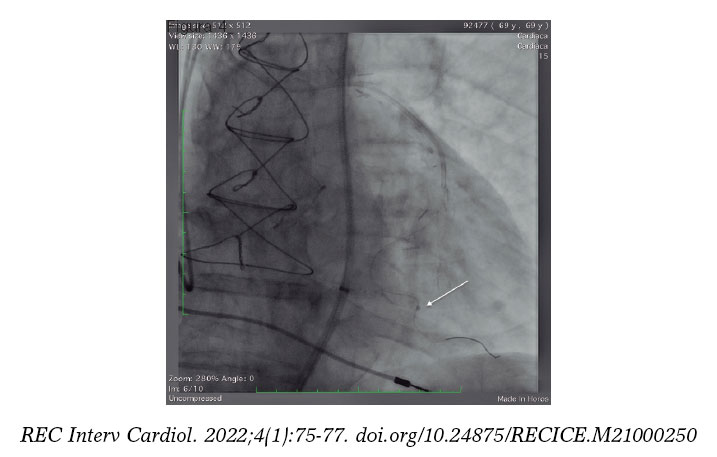
Figure 4. The guidewire advances towards the marginal branch while its more favorable position facilitates the easier advancement of the GuideLiner to cross the lesion (arrow).
Despite of this, the same stent used before was now crossing the lesion with too many difficulties (video 1 of the supplementary data). However, it was eventually implanted in the lesion with excellent results and without causing proximal lesions (video 2 of the supplementary data and figure 5). Prior to cardiac catheterization, the patient’s informed consent was obtained for the possible publication of his case for teaching purposes.
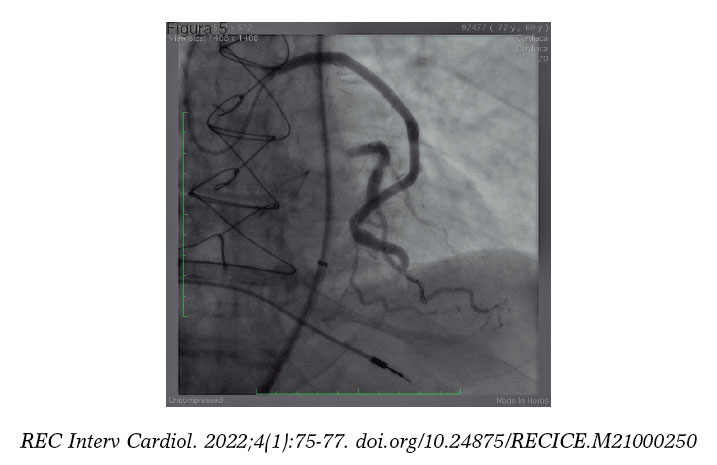
Figure 5. Result after stenting.
Several methods to increase support and facilitate the arrival of devices and stents into the target lesions have been described.1 There is no doubt that long introducer sheaths, 8-Fr guide catheters, high-support guidewires, and guide extension catheters are key to perform the most complex procedures. In some cases, triple telescoping catheter systems with 2 guide extension catheters (8-Fr and 5.5-Fr GuideLiner) have been described inside an 8-Fr guide catheter with good results.2
In this patient, the key to success was to place a quadruple telescoping catheter system never described before to achieve the maximum passive (long introducer sheath, and 8-Fr AL2 guide catheter) and active support possible (ST01 catheter, and 5-Fr GuideLiner). Also, the better orientation of an angioplasty high-support guidewire to guarantee a more favorable access to cross the lesion without excessive angulations.
FUNDING
None whatsoever.
AUTHORS’ CONTRIBUTIONS
J.R. Rumoroso Cuevas wrote, edited the text of this manuscript, and provided direct medical assistance to the patient. M. Sádaba Sagredo, and A. Subinas Elorriaga supervised the manuscript and contributed to its iconography.
CONFLICTS OF INTEREST
None reported.
SUPPLEMENTARY DATA
Vídeo 1. Rumoroso Cuevas J.R. DOI: 10.24875/RECICE.M21000250
Vídeo 2. Rumoroso Cuevas J.R. DOI: 10.24875/RECICE.M21000250












