
CASE PRESENTATION
This is the case of an 82-year-old man with a past medical history of permanent atrial fibrillation, chronic obstructive pulmonary disease, and stable Alzheimer’s disease admitted due to heart failure.
Transthoracic echocardiography revealed the presence of bicuspid aortic valve with severe aortic stenosis (maximum gradient, 76 mmHg; mean gradient, 48 mmHg), and a normal left ventricular ejection fraction (60%). During the examination, the coronary angiography documented the presence of proximal and middle right coronary artery severe stenosis treated with dual drug-eluting stent implantation. The baseline cardiac computer tomography angiography showed a bicuspid aortic valve type 1 with a noncoronary right calcified raphe and a 778.5 mm2 area (figure 1).
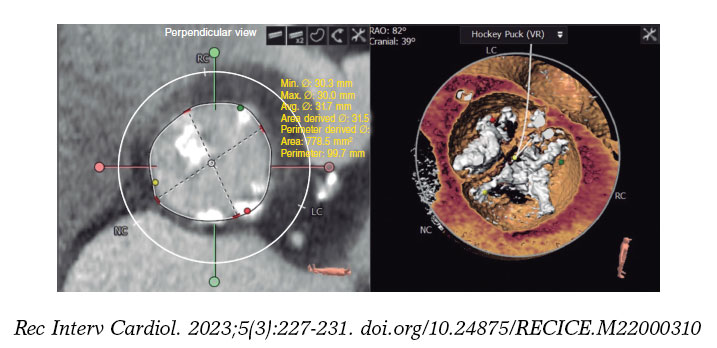
Figure 1. Computed tomography images. Left: valve measurements. Right: valve reconstruction. LC, left coronary; NC, noncoronary; RC, right coronary; VR, volume rendered.
After Heart Team discussion, transcatheter aortic valve implantation (TAVI) with balloon-expandable was decided. A 29 mm SAPIEN 3 Ultra valve (Edwards Lifesciencies; United States) was scheduled. The patient’s informed consent was obtained. A 16-Fr Edward sheath was inserted via right femoral arterial access, a 7-Fr pigtail catheter was placed into the ascending aorta via left femoral arterial access, and 6-Fr left femoral venous access was used for ventricular pacing lead placement.
All attempts to cross the aortic valve proved ineffective following its severe calcification and complex anatomy despite many different catheters and wires were used by 3 different interventional cardiologists with great experience in TAVI in a center with a volume of 125 procedures each year. Given the numerous unsuccessful attempts made, a bailout solution was needed.
FUNDING
None whatsoever.
AUTHORS’ CONTRIBUTIONS
J. Martínez-Sole, S. Lozano-Edo, and J. Sanz-Sánchez designed, drafted the manuscript, and were involved in the manuscript final approval. F. Ten-Morro, L. Andrés-Lalaguna, and J.L. Díez-Gil designed the study, conducted the manuscript critical review, and approved its final version for publication.
CONFLICTS OF INTEREST
None reported.
* Corresponding author.
E-mail address: sjorge4@gmx.com (J. Sanz Sánchez)










