
To the Editor,
Aortic pseudoaneurysm is a rare high-risk complication following surgery with aortic manipulation.
This is the case of a 66-year-old male patient with a past medical history of aortic valve replacement 16 years ago. He required a second surgery 3 months later due to prosthetic valve endocarditis with mechanical valve replacement with homograft valve implantation. Since then, the patient has remained asymptomatic until 1 year ago when he developed progressive dyspnea. The echocardiographic study revealed severe aortic regurgitation with heavily calcified valve and ascending aorta. A new surgical intervention was performed to replace the homograft by a bioprosthesis. Surgery was very complex due to the presence of significant calcification. Two months after this last intervention the patient was admitted with clinical signs of thoracic pain and hemoptysis. The computed tomography scan performed revealed the presence of a narrow-necked aortic pseudoaneurysm at the ascending aorta lateral wall, probably at the level of the cannulation performed during the previous surgery with a large periaortic hematoma (figure 1). Although the surgical repairment of the aortic pseudoaneurysm is the routine treatment, in this case it would have been the fourth reintervention. Instead, percutaneous treatment was decided.
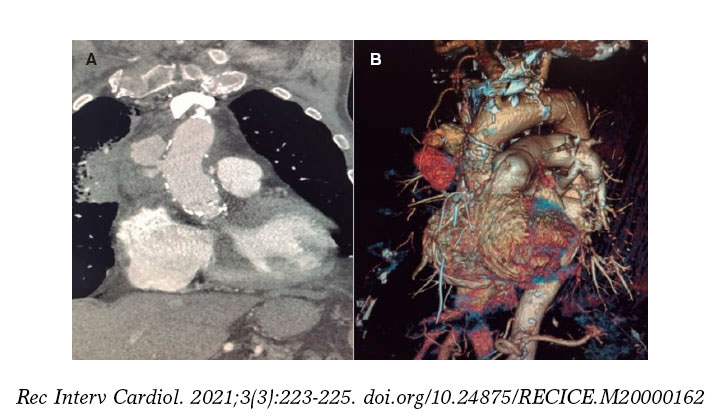
Figure 1. Coronary computed tomography angiography with contrast. Coronal view (A) and 3D reconstruction (B). Extensive atheromatous disease in the ascending aorta with diffuse calcification. Solution of continuity in the ascending aorta lateral wall with contrast extravasation contained by the tunica adventitia or surrounding tissues making up a partially thrombosed narrow-necked saccular pseudoaneurysm.
Numerous articles have been published, most on isolated clinical cases, describing the closure of an aortic pseudoaneurysm with occluder devices different to the ones often used for the closure of septal defects, vascular plugs, etc. or coil embolization.1,2 No comparative studies have ever been conducted on the different treatment options available. We only found an article in the medical literature published by Lyen et al.3 that described a combined strategy in 7 patients with coil release and implantation of an occluder device in the same procedure. We also found a simple strategy with occluder device implantation in 5 patients with better results compared to the combined strategy. In our case, since the aortic pseudoaneurysm was large and the entry neck was small, a stepped combined strategy was decided of coil embolization and if flow was persistent, followed by a second closure of the entry neck with an occluder device.
The procedure of coil embolization was uneventful, but the computed tomography scan with contrast performed 24 hours later showed flow persistence and progression of the size of the pseudoaneurysm (figure 2A), which is why percutaneous closure was decided with an occluder device.
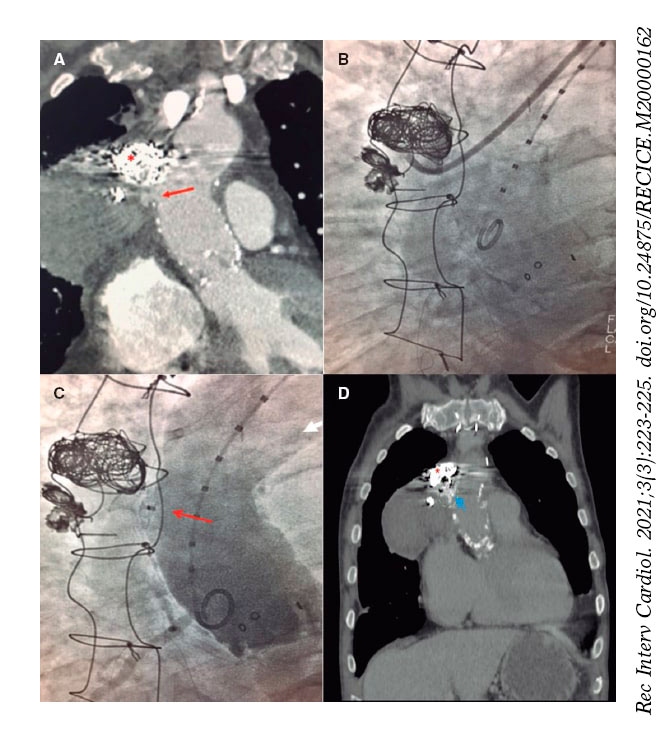
Figure 2. A: Coronary computed tomography angiography after coil release (asterisk) with presence of contrast in the cavity of the pseudoaneurysm indicative of incomplete occlusion. The entry neck (arrow) and larger size compared to the initial study can be seen. B: fluoroscopic imaging showing the distal border of the 8-Fr JR4 delivery catheter inserted into the pseudoaneurysm. C: post-implantation aortography. Occluder device (arrow) delivered inside the neck of the pseudoaneurysm. No significant passage of contrast to the inside is seen. D: thoracic computed tomography scan without contrast performed after 4 weeks. Occluder device (arrow) on the lateral wall of the aorta and coil metal artifact (asterisk) implanted in the main cavity of the pseudoaneurysm.
The estimate size of the neck of the pseudoaneurysm was 8 mm. There are no protocols with criteria on how to choose the most suitable occluder device for the management of aortic pseudoaneurysms. However, it was thought that the ones used for the closure of atrial septal defects are designed to be implanted into low-pressure cavities, which means that the tissue of the device probably cannot stop high-pressure flows. Also, in the devices used to close atrial septal defects both discs are asymmetric in size, which would result in the implantation of the largest disc into the pseudoaneurysm, which could damage the wall of the sac. Therefore an 8 mm Amplatzer VSD Muscular occluder (Abbott, United States) with 2 discs of the same size was used.
The procedure was fluoroscopy and angiography guided. Because of the situation of the aortic pseudoaneurysm—similar to the location of anastomosis of right coronary artery grafts—the delivery sheath used was an 8-Fr Launcher JR4 guide catheter (0.090 in internal lumen) (Medtronic Launcher, United States) as it was the most suitable one to place it as coaxially as possible to the neck of the pseudoaneurysm. Using a standard 0.035 in guidewire via right femoral access the catheter was advanced towards the ascending aorta effortlessly. After a slight clockwise rotation, it entered directly into the pseudoaneurysm through the neck. No support guidewire was required (figure 2B). Afterwards, an Amplatzer VSD Muscular occluder device was implanted, 1 disc was placed inside the pseudoaneurysm and the other inside the aortic wall. The control angiography performed immediately after the implant showed no significant residual shunt (figure 2C). No periprocedural complications were reported and the patient was discharged 48 hours later. The patient remained asymptomatic and the computed tomography scan confirmed that the aortic pseudoaneurysm remained stable at the 4-week follow-up (figure 2D). However, 6 months after remaining asymptomatic, the patient died of severe hemoptysis, probably due to aortic pseudoaneurysm recurrence. The patient expressed his consent for his case to be published, respecting his right to privacy and the protection of personal data.
Although in our case the short-term outcomes were not satisfactory, the percutaneous closure of the aortic pseudoaneurysm with a combined technique of coils plus occluder device can be a valid therapeutic option for patients ineligible for surgery. That is so because it adds the coils prothrombotic effect to the entry flow reduction prompted by the occluder device. Further data are needed to determine whether this combined technique improves long-term survival compared to conservative treatment.
FUNDING
There is no funding.
AUTHORS' CONTRIBUTION
All authors have contributed to the conception, design and revision of the article.
CONFLICTS OF INTEREST
None.
REFERENCES
1. Tang L, Lesser JR, Gössi M, et al. Transcatheter Closure of Complex Ascending Aortic Pseudoaneurysms After Cardiac Surgery. Circ Cardiovasc Interv. 2018;11:e007052.
2. Quevedo HC, Alonso A. Endovascular therapy for ascending aorta pseudoaneurysm. Cardiovasc Revasc Med. 2016;17:586-588.
3. Lyen SM, Rodrigues JC, Manghat NE, Hamilton MC, Turner M. Endovascular closure of thoracic aortic pseudoaneurysms:A combined device occlusion and coil embolization technique in patients unsuitable for surgery or stenting. Catheter Cardiovasc Interv. 2016;88:1155-1169.












