
To the Editor,
This is the case of a 72-year-old male examined due to exertional angina, and severe inferior wall ischemia through a single-photon emission computed tomography with Tc-99. After obtaining the patient’s written informed consent he was referred for a coronary angiography that confirmed the chronic total coronary occlusion (CTO) of the proximal right coronary artery (RCA) (figure 1A) with a J-CTO score of 3 (blunt entry shape, lesion > 20 mm, and calcification), and the presence of septal collaterals from the left anterior descending coronary artery (figure 1B, video 1 of the supplementary data). Initial antegrade approach was planned that quickly had to be changed for the retrograde approach due to the unfavorable characteristics of the lesion.
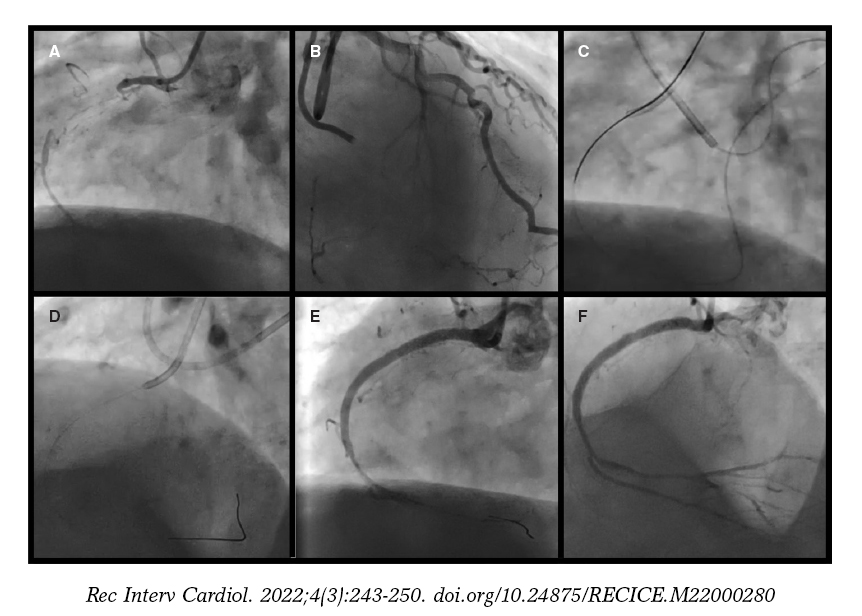
Figure 1. A: total occlusion of proximal RCA. B: septal collaterals from the left anterior descending coronary artery. C: externalized retrograde wire from the septal collateral crossing the right coronary artery occlusion. D: antegrade wiring with the help of a microcatheter placed in the distal right coronary artery. E: angiographic result after occlusion predilatation and stenting with TIMI grade-1 flow. F: after drug-eluting balloon, TIMI grade-3 flow is achieved with a diseased distal vessel.
After surfing across the septal collateral channels, the distal cap of the occlusion was crossed using a Corsair Pro XS microcatheter (Asahi Intecc, Japan) loaded with a Gaia Third wire (Asahi Intecc, Japan). A RG3 wire (figure 1C) was externalized followed by the antegrade advancement of the microcatheter (figure 1D). Finally, predilatation of the mid and proximal segments of the RCA plus 3 SYNERGY drug-eluting stents (DES) (Boston Scientific, United States) were deployed (figure 1D). The severe and diffuse stenosis of the distal RCA provided a poor run-off with a Thrombolysis in Myocardial Infarction (TIMI) grade-1 flow (figure 1E).
The vessel characteristics ruled out further DES implantation to avoid perforation, and minimize the risk of stent thrombosis. For this reason, a decision was made to treat the distal bed with prolonged inflations of drug-eluting balloons (DEB) (SeQuent Please NEO 2.5 mm × 30 mm, and 2 mm × 30 mm, Braun Melsungen, AG Vascular Systems, Germany) to improve the run-off. TIMI grade-3 flow was confirmed at the end of the procedure (figure 1F, video 2 of the supplementary data).
The patient was scheduled for a deferred coronary angiography to see the evolution of the distal bed. After 6 months, the study shows the patency of the stents, and a significant improvement of the distal vessel with TIMI grade-3 flow (figure 2A, video 3 of the supplementary data). An optical coherence tomography (Abbott, United States) confirmed the excellent results of the distal RCA, and the correct apposition and expansion of the DES (figure 2B, video 4 of the supplementary data).
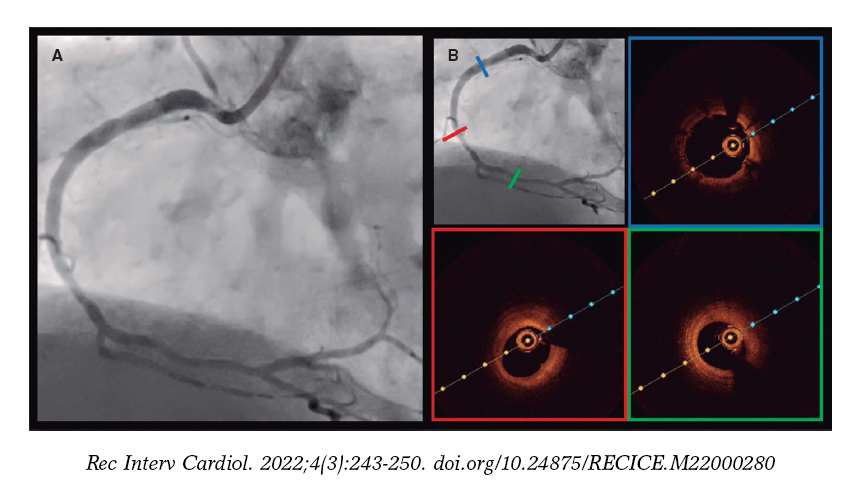
Figure 2. A: excellent angiographic evolution of right coronary artery at the 6-month follow-up. B: excellent stent apposition and distal vessel improvement according to the optical coherence tomography.
Only a few studies and case reports have analyzed DEBs in the CTO and complex PCI setting as an alternative to stent implantation.1-3 Köln et al. used a DEB as the only strategy after successful CTO recanalization with rates of procedural success and re-occlusion of 79.4% and 7.4%, respectively, at the follow-up.1 Our case emphasizes the feasibility of a hybrid approach by treating the occlusion zone with a DES, and the distal bed with a DEB to avoid further stenting. With this approach, the operator can reduce small caliber, and total stent length both associated with restenosis and worse clinical outcomes. The BASKET-SMALL 2 randomized trial showed that the DEB was non-inferior to the DES regarding major adverse cardiovascular events in small-vessel native coronary artery disease. In addition, the PICCOLETO II randomized trial showed lower in-lesion late lumen loss using a novel DEB.4,5
We should mention that in the CTO setting, the distal bed can increase its size just by reestablishing blood flow. Yet, this is another reason to refrain from DES implantation to avoid malapposition by selecting inadequate diameters.
This case confirms the feasibility of treating small-vessel native coronary artery disease in CTO cases with DEBs to improve the distal bed, avoid unnecessary stenting, and minimize the risk of stent thrombosis/restenosis.
FUNDING
None whatsoever.
AUTHORS’ CONTRIBUTIONS
Conceptualization: I. Pascual, and M. Almendarez. Writing: M. Almendarez, and I. Pascual. Image and video editing: A. Alperi, and R. Álvarez-Velasco. Revision and editing of the final draft: C. Moris, P. Avanzas. I. Pascual, and M. Almendarez contributed equally to the first authorship.
CONFLICTS OF INTEREST
None reported.
SUPPLEMENTARY DATA
Vídeo 1. Pascual I. DOI: 10.24875/RECICE.M22000280
Vídeo 2. Pascual I. DOI: 10.24875/RECICE.M22000280
Vídeo 3. Pascual I. DOI: 10.24875/RECICE.M22000280
Vídeo 4. Pascual I. DOI: 10.24875/RECICE.M22000280
REFERENCES
1. Köln PJ, Scheller B, Liew HB, et al. Treatment of chronic total occlusions in native coronary arteries by drug-coated balloons without stenting - A feasibility and safety study. Int J Cardiol. 2016;225:262–267.
2. Onishi T, Onishi Y, Kobayashi I, Umezawa S, Niwa A. Drug-coated balloon angioplasty for de novo small vessel disease including chronic total occlusion and bifurcation in real-world clinical practice. Cardiovasc Interv Ther. 2019;34:139–148.
3. Cortese B, Buccheri D, Piraino D, Silva-Orrego P. Drug-coated balloon angioplasty for coronary chronic total occlusions. An OCT analysis for a “new” intriguing strategy. Int J Cardiol. 2015;189:257–258.
4. Cortese B, Di Palma G, Guimaraes MG, et al. Drug-Coated Balloon Versus Drug-Eluting Stent for Small Coronary Vessel Disease:PICCOLETO II Randomized Clinical Trial. JACC Cardiovasc Interv. 2020;13:2840–2849.
5. Jeger RV, Farah A, Ohlow MA, et al. Drug-coated balloons for small coronary artery disease (BASKET-SMALL 2):an open-label randomised non-inferiority trial. Lancet. 2018;392:849–856.












