
To the Editor,
Acute myocardial injury in young adults may be a challenging finding. Although coronary artery disease associated with traditional cardiovascular risk factors is possible, other etiologies like the use of recreational drugs, myocarditis, coronary embolism, spontaneous coronary artery dissection or coronary vasospasm should be considered as well.1 Intracoronary imaging modalities provide diagnostic information added to invasive coronary angiography on coronary lesion features, and are useful to guide percutaneous coronary interventions.2
This is the case of a 29-year-old male patient with a history of smoking. His family history included coronary artery disease, but not at a young age. The patient presented to the emergency room with signs of acute chest pain radiating down his left arm the morning following a night of heavy alcohol and cannabis consumption.
The 12-lead electrocardiogram revealed sinus rhythm, heart rate of 60 beats per minute, and slight and diffuse ST-segment elevation (figure 1A). Blood biochemistry analysis revealed elevated troponin I levels (37.6 ng/mL; normal values < 0.045 ng/mL). The transthoracic echocardiogram revealed the presence of preserved left ventricular systolic function with normal heart wall motion kinetics, and no evidence of structural heart disease.
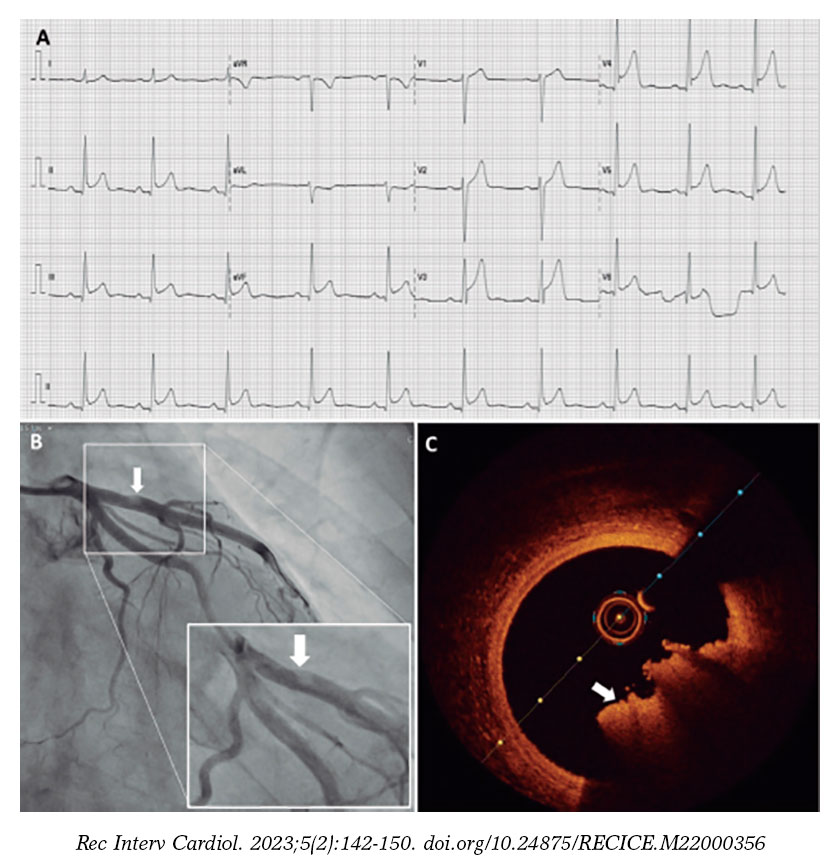
Figure 1. A: first 12-lead electrocardiogram. B: invasive coronary angiography of left main coronary artery with zoomed-in image of the filling defect. C: optical coherence tomography imaging of the same lesion showing a red thrombus.
Although the early suspected diagnosis was myopericarditis, and the patient was already pain-free, he was referred for elective invasive coronary angiography—via right radial artery—24 hours after hospital admission. We first visualized a dominant right coronary artery with no significant disease. Afterwards, the left main coronary artery angiography showed no significant disease on either the left main or circumflex arteries, but a small filling defect in the proximal segment of the left anterior descending coronary artery causing no flow restriction (figure 1B). To better characterize the lesion, an intracoronary imaging modality—optical coherence tomography—was prescribed (video 1 of the supplementary data). In the corresponding area of the filling defect, we observed a red thrombus that prevented the evaluation of a possible underlying atherosclerotic plaque (figure 1C; minimum lumen area of 9.5 mm2 (reference, 12.6 mm2).
After these findings, the diagnosis of acute coronary syndrome was assumed. Therefore, since no percutaneous coronary intervention was ever performed, the patient remained on triple antithrombotic therapy (acetylsalicylic acid, 100 mg; ticagrelor, 90 mg twice a day, and enoxaparin 1 mg/Kg twice a day). Reassessment with invasive coronary angiography was scheduled in a 7-day interval.
By the time of the second left main coronary artery angiography, no filling defect was seen on the proximal segment of the left anterior descending coronary artery (figure 2A). To confirm the improved status of the lesion, reassessment with optical coherence tomography was also performed (video 2 of the supplementary data). This time, we observed a fibroadipose atherosclerotic plaque with no signs of instability with some reminiscent thrombus on the surface of the plaque (figure 2B). The lesion mechanism was thought to be definite plaque erosion (according to the classification by Kolte et al.3). The patient was successfully discharged on dual antiplatelet therapy and behavioral restriction regarding drug consumption.
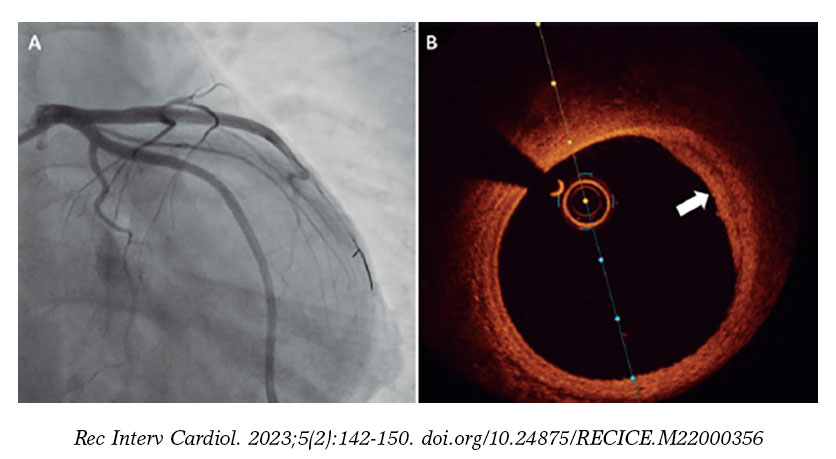
Figure 2. A: reassessment with invasive coronary angiography no longer showing the previous filling defect on the proximal segment of the left anterior descending coronary artery. B: optical coherence tomography of this region revealing a fibroadipose atherosclerotic plaque without signs of instability.
It has been established that cannabis exerts pathophysiological effects on the cardiovascular system.4 There is a growing number of case reports describing adverse cardiovascular events, specifically, cannabis-induced myocardial infarction. As this situation is most frequently reported in young individuals, it may go unnoticed and, consequently, untreated. Intracoronary imaging modalities play a key role in the definition of the mechanism behind coronary lesions—whether atherosclerotic or not—in patients with suspected acute coronary syndrome/myocardial infarction with non-obstructive coronary arteries.2 Reassessment after some time of triple antithrombotic therapy may also contribute to clarify the mechanism as the artery lumen may be thrombus-free.
Informed consent and authorization to publish these figures and videos were obtained from the patient.
FUNDING
None whatsoever.
AUTHORS’ CONTRIBUTIONS
All authors contributed to the genesis of this manuscript, were involved and approved its submission.
CONFLICTS OF INTEREST
None reported.
SUPPLEMENTARY DATA
Vídeo 1. Duarte P. DOI: 10.24875/RECICE.M22000356
Vídeo 2. Duarte P. DOI: 10.24875/RECICE.M22000356
REFERENCES
1. Gulati R, Behfar A, Narula J, et al. Acute Myocardial Infarction in Young Individuals. Mayo Clin Proc. 2020;95:136-156.
2. Aparisi Á, Cubero-Gallego H, Tizón-Marcos H. Intracoronary imaging: review and clinical use. REC Interv Cardiol. 2022;4:228-237.
3. Kolte D, Yonetsu T, Ye JC, et al. Optical Coherence Tomography of Plaque Erosion: JACC Focus Seminar Part 2/3. J Am Coll Cardiol. 2021;78:1266-1274.
4. Chetty K, Lavoie A, Deghani P. A Literature Review of Cannabis and Myocardial Infarction-What Clinicians May Not Be Aware Of. CJC Open. 2021;3:12-21.












