
To the Editor,
Coronary re-access continues to be a challenge following transcatheter aortic valve implantation (TAVI). Commissural alignment of the prosthesis facilitates coronary re-access, especially in self-expanding prostheses.1 Additionally, for certain devices, different techniques for coronary cannulation might be necessary if the previously implanted prosthesis has commissural misalignment.2 By analyzing 3-cusp and left-to-right 2-cusp overlap (2-cusp) projections after TAVI, it is possible to estimate the degree of commissural alignment in prostheses with identifiable commissural posts on fluoroscopy.3,4 This study aimed to describe the optimal projections for left and right coronary artery (LCA, RCA) cannulation in patients with previous TAVI.
We analyzed the pre-TAVI computed tomography scans of 105 consecutive patients referred to our center for TAVI implantation. Of these scans, 5 were excluded due to their poor quality or previous aortic valve replacement. The ideal projections for LCA and RCA catheterization were identified by using 3mensio software (Pie Medical Imaging, The Netherlands) and were defined as projections coplanar with the cross-sectional transverse plane of the aorta at the level of each coronary ostium and orthogonal to them, respectively. An en-face projection to the aortic annulus can be established intraprocedurally as a projection where the prosthesis is foreshortened, usually in a cranial (CRA) and right anterior oblique (RAO) angulation. The subsequent projection is useful for guiding clockwise or counterclockwise rotation of the catheter, which is particularly beneficial for determining whether the catheter crosses the stent frame within an aligned cell near the coronary ostium (figure 1).
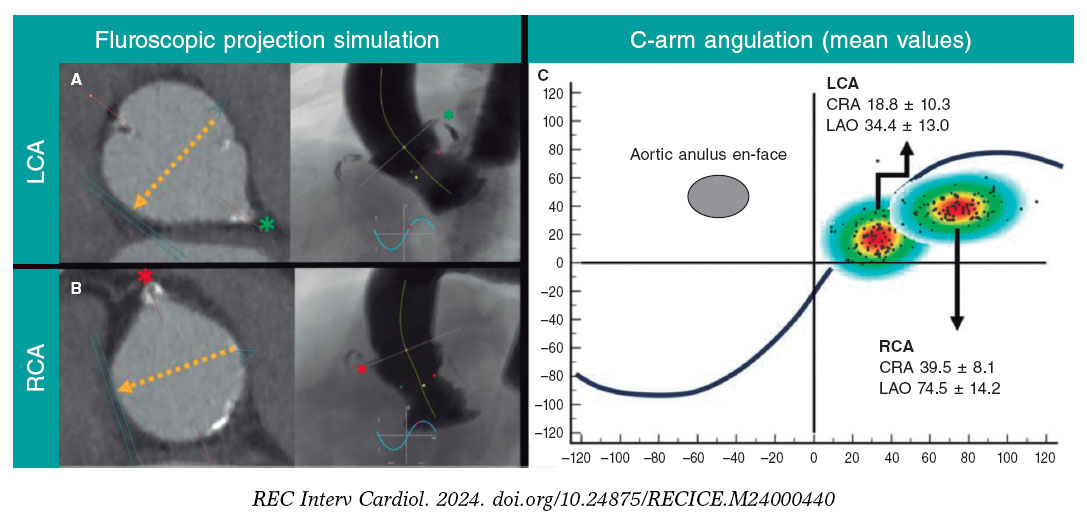
Figure 1. Computed tomography-derived fluoroscopic angulation. A: LCA cannulation (green asterisk; LCA ostia). B: RCA cannulation (red asterisk; RCA ostia). The yellow arrow indicates the direction of the C-arm projection at the en-face aortic root multiplanar reconstruction of the computed tomography scan. C: Scatter plot for LCA and RCA cannulation (grey ellipse; usual en-face projection to the aortic root); CRA, cranial; LAO, left anterior oblique; LCA, left coronary artery; RCA, right coronary artery.
The mean projections for LCA and RCA cannulation were as follows: CRA 18.8º ± 10.3º, LAO (left anterior oblique) 34.4º ± 13.0º, CRA 39.5º ± 8.1º, and LAO 74.5º ± 14.2º, respectively. Figure 2 illustrates the coronary cannulation of the LCA with a Judkins left 4.0 catheter in a patient with a previous Evolut PRO + 24 (Medtronic, United States) prosthesis using the proposed C-arm and en-face angulations.
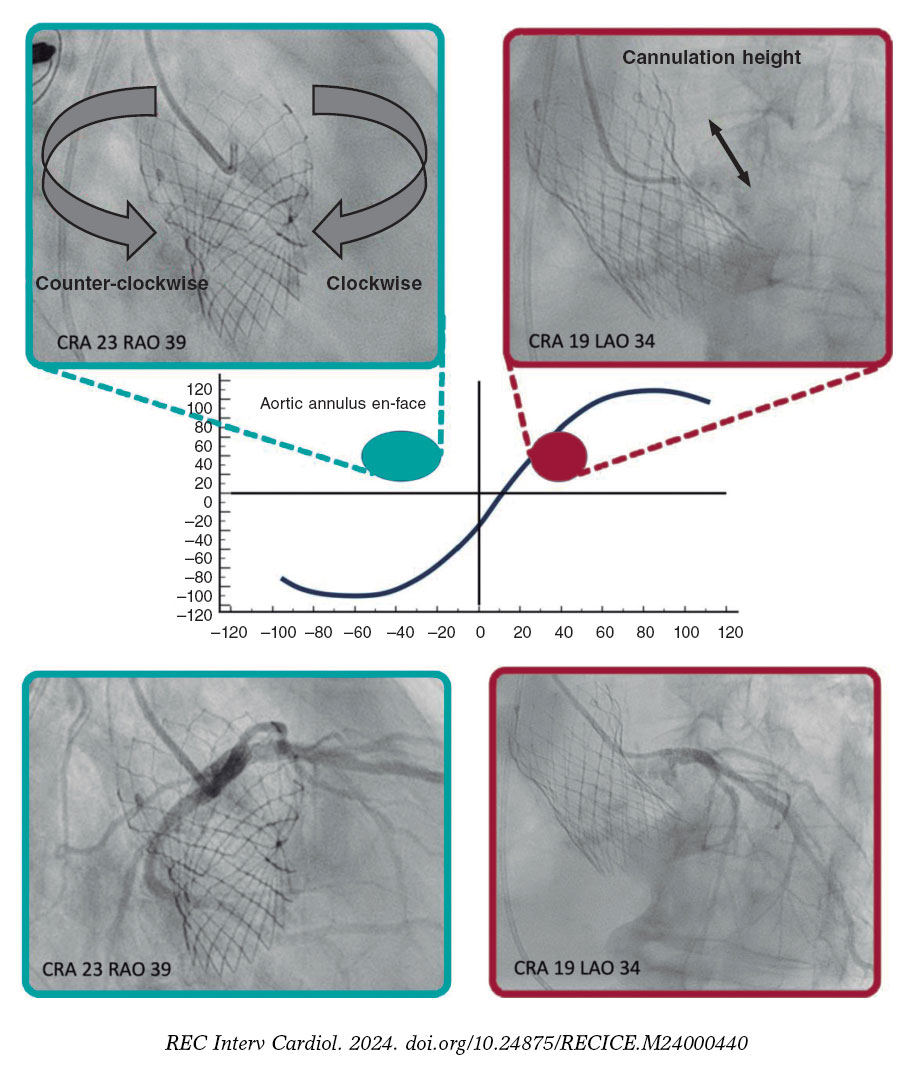
Figure 2. Example of LCA cannulation. CRA 19 LAO 34º projection was used to determine the height (purple arrow) of the cell for crossing in CRA angulation and RAO (blue ellipse) angulation assisted in the rotational orientation of the catheter either clockwise (blue arrow) or counterclockwise (red arrow). CRA, cranial; LAO, left anterior oblique; RAO, right anterior oblique.
As a result, we propose that when a post-TAVI patient is referred for a coronary angiogram, the first step should be to determine the TAVI alignment using previously described methods.3 Coronary cannulation of the LCA might be attempted in CRA 18.8º LAO 34.4º and for RCA cannulation in CRA 39.8º LAO 74.4º, using an en-face projection to rotate the catheter clockwise or counterclockwise (figure 2). Different cannulation techniques should be considered based on the degree of commissural alignment.2
Furthermore, we suggest that after each TAVI procedure, the degree of commissural alignment should be noted. In addition, patient-specific RCA and LCA cannulation projections could be included in the report to facilitate subsequent coronary cannulation.
FUNDING
None.
ETHICAL CONSIDERATIONS
All patients signed the informed consent form, and the study was approved by the ethics committee of the hospital. Possible sex and gender variables were considered according to SAGER guidelines.
STATEMENT ON THE USE OF ARTIFICAL INTELLIGENCE
No artificial intelligence tool has been used in the preparation of this article.
AUTHORS’ CONTRIBUTIONS
A. Redondo Diéguez and X. Irazusta Olloquiegui were involved in data collection. A. Redondo Diéguez drafted the manuscript. B. Cid Álvarez, R. Trillo Nouche, A. García Campos, and J.R González- Juanatey reviewed the manuscript. All authors approved the final version of the manuscript.
CONFLICTS OF INTEREST
R. Trillo Nouche is a proctor for Boston Scientific and Medtronic. None of the other authors have any conflicts of interest to declare.
REFERENCES
1. Tarantini G, Nai Fovino L, Scotti A, et al. Coronary Access After Transcatheter Aortic Valve Replacement With Commissural Alignment:The ALIGN-ACCESS Study. Circ Cardiovasc Interv. 2022;15:e011045.
2. Yudi MB, Sharma SK, Tang GHL, Kini A. Coronary Angiography and Percutaneous Coronary Intervention After Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2018;71:1360-1378.
3. Redondo A, Santos-Martínez S, Delgado-Arana R, Baladrón Zorita C, San Román JA, Amat Santos IJ. Fluoroscopic-based algorithm for commissural alignment assessment after transcatheter aortic valve implantation. Rev Esp Cardiol. 2022;75:184-187.
4. Tang GHL, Amat-Santos IJ, De Backer O, et al. Rationale, Definitions, Techniques, and Outcomes of Commissural Alignment in TAVR:From the ALIGN-TAVR Consortium. JACC Cardiovasc Interv. 2022;15:1497-1518.
* Corresponding author.
E-mail address: (A. Redondo Diéguez).
 @alfredoRedondoD; @belcid7; @ramirotrillo; @josejuanatey; @xabiira
@alfredoRedondoD; @belcid7; @ramirotrillo; @josejuanatey; @xabiira












