
ABSTRACT
Introduction and objectives: The results of the Radcong-21 Registry of the Spanish Society of Pediatric Cardiology and Congenital Heart Disease Working Group on Hemodynamics are described to analyze data, establish updated reference parameters, and compare them to other registries.
Methods: Retrospective, cross-sectional, observational, multicenter registry of patients with congenital heart disease undergoing cardiac catheterization in 2021. Each cath lab sent the last 100 cases performed prior to January 2022. A descriptive analysis was conducted of anthropomorphic variables, procedural (grouped by type and radiation exposure categories [REC]) and technical characteristics, and dosimetric parameters with additional review of all values outside the 95%CI of the median.
Results: A total of 1090 procedures performed in 11 cath lab of 10 hospital centers were analyzed. Age distribution: 22.8% < 1 year, 60.7% between 1-18 years, and 16.4% > 18 years. In dose area product (DAP)/Kg and DAP/Kg/fluoroscopy, the distribution was very similar regardless of the type of cath lab as is the case with most pediatric patients in terms of age, weight, and REC group. The DAP/Kg was higher in the REC I and III groups compared to other countries with registries and improvement programs in this area (78% and 8,3%, respectively).
Conclusions: Representative data of dosimetric parameters by age and procedures in congenital cardiac catheterizations were obtained in Spain back in 2021. DAP/Kg is the parameter with the lowest dispersion in the sample. There is room for improvement compared to other countries with optimization programs in this area.
Keywords: Congenital heart disease. Angiography. Pediatric cardiac cath lab. Radiation dose. Radiation protection.
RESUMEN
Introducción y objetivos: Se describen los resultados del Registro Radcong-21 del Grupo de Trabajo de Hemodinámica de la Sociedad Española de Cardiología Pediátrica y Cardiopatías Congénitas con el objetivo de analizar los datos, establecer parámetros de referencia actualizados y compararlos con otros registros.
Métodos: Registro multicéntrico, observacional, transversal y retrospectivo de pacientes con cardiopatías congénitas tratados con cateterismo cardiaco en 2021. Cada sala de hemodinámica remite los últimos 100 casos realizados hasta enero de 2022. Análisis descriptivo de variables antropomórficas, procedimientos (agrupados por tipo y riesgo estimado de radiación [RER]), características técnicas y parámetros dosimétricos. Revisión adicional de todos los valores fuera del intervalo de confianza del 95% de la mediana.
Resultados: Se analizaron 1.090 procedimientos en 11 salas de hemodinámica de 10 centros hospitalarios. De los pacientes, el 22,8% fueron < 1 año, el 60,7% entre 1 y 18 años, y el 16,4% > 18 años. Los valores del producto dosis-área (PDA)/kg y del PDA/kg/fluoroscopia fueron muy similares independientemente del tipo de sala, al igual que ocurre con la edad, el peso y el grupo RER en la mayor parte de las salas pediátricas. El PDA/kg fue superior en los grupos RER I y III comparado con otros países con registros y programas de mejora activos en este campo (un 78 y un 8,3%, respectivamente).
Conclusiones: Se obtienen datos representativos de los parámetros dosimétricos por edad y procedimientos en los cateterismos cardiacos congénitos en España en el año 2021. El PDA/kg es el que tiene menor dispersión en la muestra total. Existen áreas de mejora en comparación con otros países con programas de optimización.
Palabras clave: Cardiopatía congénita. Angiografía. Sala de hemodinámica pediátrica. Dosis de radiación. Protección radiológica.
Abbreviations
ASD: atrial septal defect. CL: cath lab. DAP: dose-area product. REC: radiation exposure category. SECPCC: Spanish Society of Pediatric Cardiology and Congenital Heart Disease. VSD: ventricular septal defect.
INTRODUCTION
Over the past few years, interventional procedures to treat congenital heart diseases have become an inescapable reality across all age ranges. The use of ionizing radiation is no stranger to health risks for the patients and health professionals involved, which is why the Spanish legislation and the International Commission on Radiological Protection recommend registering the dose of radiation received and establishing and applying reference values for the different fluoroscopy-guided procedures. Doses that should be reviewed on a regular basis.18-20 In this context, it is necessary to register local data to facilitate comparisons and good clinical practice analysis across different centers.
The Spanish Society of Cardiology Working Group on Pediatric Cardiology and Congenital Heart Disease (GTH-SECPCC) presented a communication in its National Meeting held back in 2017 to establish the very first approach to this problem. Previous attempts had been made regarding coronary procedures like the one published by the Interventional Cardiology Association of the Spanish Society of Cardiology Working Group on Dosimetry and Quality Criteria in Interventional Cardiology.21 However, to this date, no similar reports on the pediatric age or patients with congenital heart diseases have been published in our country.
The main objective of this study was to show and analyze current data of representative dosimetric parameters from cardiac catheterizations performed in patients with congenital heart disease in Spain. Also, an attempt was made to establish the reference values for such parameters in our country by age group and type of intervention and compare them with other registries already established in different countries.
METHODS
This was a multicenter, observational, cross-sectional, and retrospective study. It describes the dosimetric parameters of procedures performed in Spain in a large number of patients with congenital heart diseases in 2021. The rules and regulations settled by the different centers involved have been observed at all times to access clinical data. Patients and hospitals have been anonymized and coded with consecutive numerical tags. The study protocol was approved by the reference research unit Ethics Committee (code 2018/491). Informed consent was not deemed necessary due to the retrospective and observational nature of the study with the sole purpose of improving healthcare.
The study population included the last 100 cardiac catheterizations performed in patients with congenital heart diseases in each cath lab (CL) until January 2022. GTH-SECPCC affiliated centers were asked to participate. Case mining was performed consecutively and regardless of the type of procedure performed and the patient’s characteristics. No external auditing was possible. However, to have maximum quality control according to the principle established in the STROBE (Strengthening the reporting of observational studies in epidemiology) checklist22 it was decided that all data received outside the 95% confidence interval (95%CI) values of the median should be submitted to researchers for additional outcome review, confirmation, and justification. Therefore, the exclusion criteria were an n < 50 cases per CL, cardiac catheterizations performed prior to 2021, those performed in patients without congenital heart disease, failure to fill in the registry form with all the variables (except for air kerma), and negative responses (or no response at all) to the review and additional confirmation, if necessary. The foramen ovale was not considered a congenital heart disease, and CLs with > 75% of cases rejected were excluded from the analysis.
The following variables were collected:
- – Anthropomorphic parameters: age, weight (kg), height (cm), and body surface area (m2).
- – Types of procedure grouped into 16 different categories: pulmonary branch angioplasty, right ventricular outflow tract angioplasty, stenting in ductus arteriosus or fistula, coarctation of aorta, other angioplasties, pulmonary valve implantation, closure of atrial septal defect (ASD), closure of ventricular septal defect, closure of ductus arteriosus, closure of collaterals, aortic valvuloplasty, pulmonary valvuloplasty, combined procedure, pulmonary vasodilator test, diagnostic catheterization, and other. Also, to compare them with other series published, the procedures were grouped into radiation exposure categories (REC) based on the criterion used by Quinn et al.23 in 3 different groups of diseases with similar doses of radiation anticipated and arranged in descending order.
- – Technical characteristics: use of biplane or 3D rotational angiography (3DRA), and type of CL.
- – Dosimetric parameters: dose-area product (DAP, µGym2), air kerma (AK, mGy), and fluoroscopy time (min).
Statistical analysis
The descriptive analysis of the variables included in the study was conducted using the statistical software packages SPSS, version 28.0, and R version 4.1.2. Bilateral comparisons were used, and P values < .05 were considered statistically significant. Qualitative variables were expressed as absolute and relative frequencies. The quantitative ones were expressed as median and its 95%IC following the criterion used in former reference studies to facilitate comparison with our results, and read and interpret the tables much easier. Median comparisons were also drawn. The supplementary data includes the mean and interquartile range for each variable in the description of the overall sample (table 1 of the supplementary data), the REC groups (tables 2 to 4 of the supplementary data), and type of CL (tables 5 to 7 of the supplementary data).
A description of the entire sample based on the REC group and type of CL was made. Radiation parameters were described both in general and by participant CL, per type of CL, age group and type of procedure.
The comparison of radiation parameters based on the type of CL was made through median comparison by applying Bonferroni correction. Scatter plots were used among the different exposure parameters DAP/Kg, and DAP/Kg/fluoroscopy (Y axis), and weight (X axis) both in general and by REC gruop.
RESULTS
Sample population
In Spain, interventional activity to treat patients with congenital heart diseases is performed in 3 different types of CLs based on the profile of each patient: preferential dedication to patients < 18 years (pediatric type), preferential dedication to patients > 18 years (adult type), and no age discrimination (hybrid type). A total of 12 hospitals responded to the registry request. In 2 of them, interventional activity takes place in different CLs and with different heart teams depending on whether patients are children or adults. Therefore, the total number of participant CLs was 14: 8 pediatric, 4 hybrid, and 2 adult CLs. After applying the exclusion criteria, data from 3 CLs were excluded: 1 for having an n < 50, and 2 because > 75% of the cases met the exclusion criteria (most of them for not responding to the review petition and additional confirmation request). The total number of procedures submitted by the remaining 11 CLs was 1100, 10 of which were excluded due to negative responses to the additional review. Finally, in this study, data of 1090 procedures from 10 hospitals for a total of 11 CLs (7 pediatric, 3 hybrid, and 1 adult) were analyzed. Flowchart is shown on figure 1. The medians of age and weight were 6 years old (95%CI, 6-7), and 20 Kg (95%CI, 19-22.1). Distribution by age group was 22.8% < 1 year, 60.7% between 1 and 18 years, and 16.4% > 18 years. In the overall sample, the median of dosimetric parameters was 1128.9 µGym2 (95%CI, 975.6-1275) for the DAP (n = 1090), 15.12 min (95%CI, 14.1-16.2) for fluoroscopy time (n = 1090), and 83 mGy (95%CI, 76.5-92.8) for AK (n = 889). We should mention that 2 of the CLs (1 adult and 1 pediatric) just don’t register AK on a routine basis (table 1).
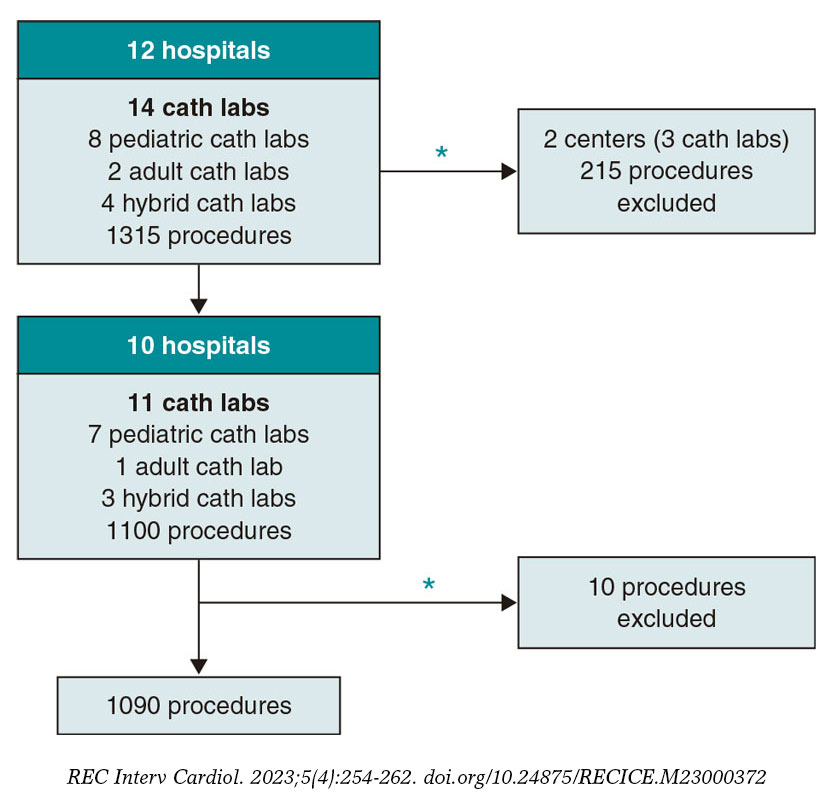
Figure 1. Flowchart of the selection of the procedures analyzed. * Exclusion criteria: n < 50 cases per cath lab, catheterizations performed before 2021, in patients without congenital heart disease, failure to fill in the registry form with all the variables (except for air kerma), and negative responses (or no reponse at all) to review or additional confirmation, if necessary. All cath labs with > 75% of cases rejected were excluded from the analysis.
Table 1. Demographic characteristics and dosimetric parameters of the overall sample
| N | Mean | Median | 95%CI (median) | |
|---|---|---|---|---|
| Age | 1090 | 11.03 | 6 | 6-7 |
| Weight (kg) | 1090 | 29.69 | 20 | 19-22.1 |
| Height (cm) | 1090 | 113.46 | 114 | 109-119 |
| BSA (m2) | 1090 | 0.93 | 0.8 | 0.77-0.87 |
| Air kerma (mGy) | 889 | 286.26 | 83.02 | 76.47-92.8 |
| DAP (µGym2) | 1090 | 3783.27 | 1128.9 | 975.62-1275 |
| Fluoroscopy (min) | 1090 | 21.29 | 15.12 | 14.13-16.2 |
| DAP/fluoroscopy (µGy.m2/kg/min) | 1090 | 216.18 | 77.62 | 70.11-88.89 |
| DAP/kg (µGy.m2/kg) | 1090 | 132.38 | 62.3 | 56.75-69.03 |
| DAP/BSA | 1090 | 3500.87 | 1633.57 | 1480-1811.09 |
| DAP/Kg/fluoroscopy | 1090 | 8.28 | 3.81 | 3.54-4.06 |
| DAP/BSA/fluoroscopy | 1090 | 213.84 | 99.73 | 91.99-107.09 |
|
95%CI, 95% confidence interval; BSA, body surface area; DAP: dose-area product. |
||||
Type of procedures
Table 2 shows the distribution of procedures based on the REC group developed by Quinn et al.,23 and the type of CL. A total of 83.5% of all procedures performed were categorized into some of the REC groups (81.7%, 15.9%, and 2.4% in groups I, II, and III, respectively). A total of 63.4%, 27.4%, and 9.2% of the procedures were performed in pediatric, hybrid, and adult CLs, respectively. The most common procedure in all the CLs is diagnostic catheterization, especially in adult CLs (65% of the total). Closure procedures of ductus arteriosus (14.2%) and ASD (11.7%) followed by pulmonary branch angioplasty (7.4%) or coarctation of aorta (6.1%) are among the most predominant interventional procedures reported.
Table 2. Procedures per REC group and type of cath lab
| Total | REC | Type of cath lab | |||
|---|---|---|---|---|---|
| Pediatric | Adult | Hybrid | |||
| N (%) | N (%)a | N (%) | N (%) | N (%) | |
| Total general | 1090 (100) | 910 (100) | 691 (63.4) | 100 (9.2) | 299 (27.4) |
| Total REC I | 743 (68.2) | 743 (81.7) | 453 (65.6) | 78 (78) | 212 (70.9) |
| Stenting of the ductus arteriosus or fistula | 9 (0.8) | 9 (1) | 5 (0.7) | 0 (0) | 4 (1.3) |
| Coarctation of aorta | 66 (6.1) | 66 (7.3) | 45 (6.5) | 1 (1) | 20 (6.7) |
| Occlusion of ASD | 128 (11.7) | 128 (14.1) | 79 (11.4) | 8 (8) | 41 (13.7) |
| Occlusion of ductus arteriosus | 155 (14.2) | 155 (17) | 98 (14.2) | 1 (1) | 56 (18.7) |
| Aortic valvuloplasty | 29 (2.7) | 29 (3.2) | 19 (2.8) | 1 (1) | 9 (3) |
| Pulmonary valvuloplasty | 67 (6.2) | 67 (7.4) | 48 (7) | 2 (2) | 17 (5.7) |
| Pulmonary vasodilator test | 12 (1.1) | 12 (1.3) | 6 (0.9) | 0 (0) | 6 (2) |
| Diagnostic catheterization | 277 (25.4) | 277 (30.4) | 153 (22.1) | 65 (65) | 59 (19.7) |
| Total REC II | 145 (13.3) | 145 (15.9) | 103 (15) | 10 (10) | 32 (10.7) |
| Pulmonary branch angioplasty | 81 (7.4) | 81 (8.9) | 57 (8.3) | 5 (5) | 19 (6.4) |
| RVOT angioplasty | 21 (1.9) | 21 (2.3) | 14 (2) | 4 (4) | 3 (1) |
| Occlusion of VSD | 24 (2.2) | 24 (2.6) | 19 (2.8) | 0 (0) | 5 (1.7) |
| Collateral closure | 19 (1.7) | 19 (2.1) | 13 (1.9) | 1 (1) | 5 (1.7) |
| Total REC III | 22 (2) | 22 (2.4) | 8 (1.2) | 4 (4) | 10 (3.3) |
| Pulmonary valve implantation | 22 (2) | 22 (2.4) | 8 (1.2) | 4 (4) | 10 (3.3) |
| Total no REC | 180 (16.5) | 0 | 127 (18.3) | 8 (8) | 45 (15.1) |
| Other angioplasties | 32 (2.9) | 0 | 14 (2) | 7 (7) | 11 (3.7) |
| Combined | 90 (8.3) | 0 | 72 (10.4) | 1 (1) | 17 (5.7) |
| Other | 58 (5.3) | 0 | 41 (5.9) | 0 (0) | 17 (5.7) |
|
ASD, atrial septal defect; REC, radiation exposure category; RVOT, right ventricular outflow tract; VSD, ventricular septal defect. |
|||||
Comparison among participant cath labs
Result comparison by age and REC group in the overall sample and per participant CL is shown on table 3. Most pediatric CLs show a very similar distribution by age, weight, and REC group. In all CLs, more patients fall into the REC I group. Compared to the pediatric ones, adult, and hybrid CLs (4% vs 1%) show slightly more REC III group procedures. Regarding DAP/Kg and DAP/Kg/fluoroscopy, distribution is very similar in the 3 types of CL except for CL4 that shows higher values compared to the total (261.3 µGym2/kg vs 62.3 µGym2/kg, and 37.1 µGym2/kg/min vs 3.8 µGym2/kg/min).
Table 3. Demographic characteristics, DAP/kg, and DAP/Kg/fluoroscopy per cath lab and radiation exposure category group
| Total | CL1 | CL2 | CL3 | CL4 | CL5 | CL6 | CL7 | CL8 | CL9 | CL10 | CL11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | 1090 | 100 | 99 | 100 | 100 | 99 | 100 | 100 | 100 | 100 | 92 | 100 |
| Type of cath lab | Adult | Hybrid | Hybrid | Hybrid | Pediatric | Pediatric | Pediatric | Pediatric | Pediatric | Pediatric | Pediatric | |
| Median age (95%CI) | 6 (6-7) | 34 (30-42) | 7 (6-10) | 8 (7-15) | 5.5 (4-8) | 3 (2-5) | 4 (3-9) | 3.7 (2.4-4.9) | 2 (1-3) | 7.5 (6-10) | 4 (4-6) | 5.5 (5-8) |
| < 1 year (%) | 249 (22.8%) | 0 | 21 | 13 | 23 | 40 | 25 | 32 | 36 | 25 | 15 | 19 |
| 1-18 years (%) | 662 (60.8%) | 2 | 59 | 56 | 61 | 59 | 63 | 68 | 64 | 74 | 75 | 81 |
| > 18 years (%) | 179 16.4%) | 98 | 19 | 31 | 16 | 0 | 12 | 0 | 0 | 1 | 2 | 0 |
| Weight, median (95%CI) | 20 (19-22.1) |
66.9 (62.8-71.2) | 26 (21.6-34) |
36 (25-49) |
19.5 (16-26) |
12 (9.1-16.3) | 15.2 (11.8-18.3) | 15 (12-20.3) |
11.4 (9.5-13.4) | 23.5 (20-32) |
16 (14-20) |
21 (18-27) |
| REC | N = 910 | 92 | 86 | 89 | 79 | 79 | 91 | 76 | 96 | 77 | 82 | 63 |
| REC I (%) | 743 (81.6%) | 78 (84.8%) | 69 (80.2%) | 76 (85.4%) | 67 (84.8%) | 54 (68.4%) | 60 (65.9%) | 59 (77.6%) | 85 (88.5%) | 59 (76.6%) | 79 (96.3%) | 57 (90.5%) |
| REC II (%) | 145 (16%) | 10 (10.9%) | 14 (16.3%) | 10 (11.2%) | 8 (10.1%) | 25 (31.6%) | 26 (28.6%) | 17 (22.4%) | 11 (11.5%) | 16 (20.8%) | 3 (3.7%) | 5 (7.9%) |
| REC III (%) | 22 (2.4%) | 4 (4.3%) | 3 (3.5%) | 3 (3.4%) | 4 (5.1%) | 0 (0%) | 5 (5.5%) | 0 (0%) | 0 (0%) | 2 (2.6%) | 0 (0%) | 1 (1.6%) |
| DAP/kg (µGy.m2/kg), median (95%CI) | 62.3 (56.7-69) |
64.0 (52.2-78.7) | 50.1 (37.6-65.8) | 56.2 (45.3-73.5) | 261.3 (213.2-326.9) | 52 (44.5-75.9) | 44.6 (34.3-61.9) | 69.8 (55-93.8) | 33.2 (27.2-38.3) | 95.9 (74.4-136.5) | 37.6 (29.5-44.6) | 80.9 (64.4-97.6) |
| REC I | 48.1 (43.6-53.1) | 53.4 (38.8-69) | 54.4 (37.6-72.9) | 49.1 (39.7-59.8) | 215.7 (180.5-284.4) | 30.3 (23.4-45.2) | 21.5 (18.2-34.7) | 54.3 (47.7-101.2) | 30.5 (25.1-35.7) | 71.2 (59.7-92.2) | 31.8 (23.5-39.8) | 54.3 (38-83.3) |
| REC II | 104.7 (80.7-130) | 116.5 (53-195.9) | 38.9 (21-80.7) | 135.5 (53.1-276.9) | 417.1 (262.7-644.4) | 81 (52-105.8) | 91.7 (57.1-122.4) | 91.9 (78.1-216.1) | 80 (46.5-131.5) | 238.8 (139.8-561.7) | 47.6 (37.5-223.7) | 175.7 (170.8-223.8) |
| REC III | 213.5 (161.9-291.6) | 202.4 (113-351) | 178.3 (65.8-291.7) | 144.7 (105.4-225.9) | 253.4 (145.1-328.6) | 0 | 298.5 (233.8-471.9) | 0 | 0 | 195.8 (176.8-214.8) | 0 | 161.9 |
| DAP/kg/fluoroscopy (µGy.m2/kg/min) | 3.8 (3.5-4.1) |
3.22 (2.81-3.62) | 2.9 (2.2-3.9) |
4.8 (3.7-5.7) |
37.1 (31.2-41.2) | 2.2 (1.8-2.6) |
2.8 (2.4-3.4) |
2.6 (2.3-3) |
3.9 (3.5-4.4) |
6.8 (5.9-7.9) |
2.8 (2.5-3.3) |
5.4 (4.7-7.2) |
| REC I | 3.61 (3.4-3.9) | 2.9 (2.4-3.4) | 3.4 (2.5-4.5) | 4.4 (3.5-5.6) | 39.6 (30.7-46) | 1.8 (1.5-2.5) | 2.7 (2.3-3.2) | 2.5 (2.2-3.2) | 3.8 (3.4-4.3) | 6.3 (5-7) | 2.8 (2.5-3.3) | 5.1 (4.6-7.6) |
| REC II | 3.6 (3-4.4) | 4.3 (3.1-4.8) | 1.7 (1-4.1) | 4.8 (2.6-9.9) | 29.3 (12.5-43.3) | 2.3 (1.8-2.8) | 3 (2.4-4.5) | 2.3 (2.2-3.4) | 4.4 (3.6-7) | 8.6 (5.3-10.1) | 3.5 (2.8-5.4) | 8.1 (7.8-9.1) |
| REC III | 7.03 (5.3-8.9) | 5 (3-6.1) | 7 (1.5-8.5) | 5.3 (4.5-16) | 6.3 (4.4-9.9) | 0 | 7.5 (7.4-9.7) | 0 | 0 | 9.3 (8.9-9.7) | 0 | 11.4 |
|
95%CI, 95% confidence interval; DAP, dose-area product; REC: radiation exposure category. |
||||||||||||
Analysis of dosimetric parameters
In scatter plots of weight vs DAP, weight vs DAP/Kg, and weight vs DAP/Kg/fluoroscopy in the overall sample and per REC group, lowest dispersion is seen in the DAP/kg parameter especially in the overall sample and the REC I group (figure 2 and figure 1 of the supplementary data). Regarding distribution based on the type of CL by age, REC group, and dosimetric parameters, significant differences were reported in all the median comparisons for 2 independent samples except in the DAP/kg, and DAP/kg/fluoroscopy parameters between adult and pediatric CLs (figure 3).
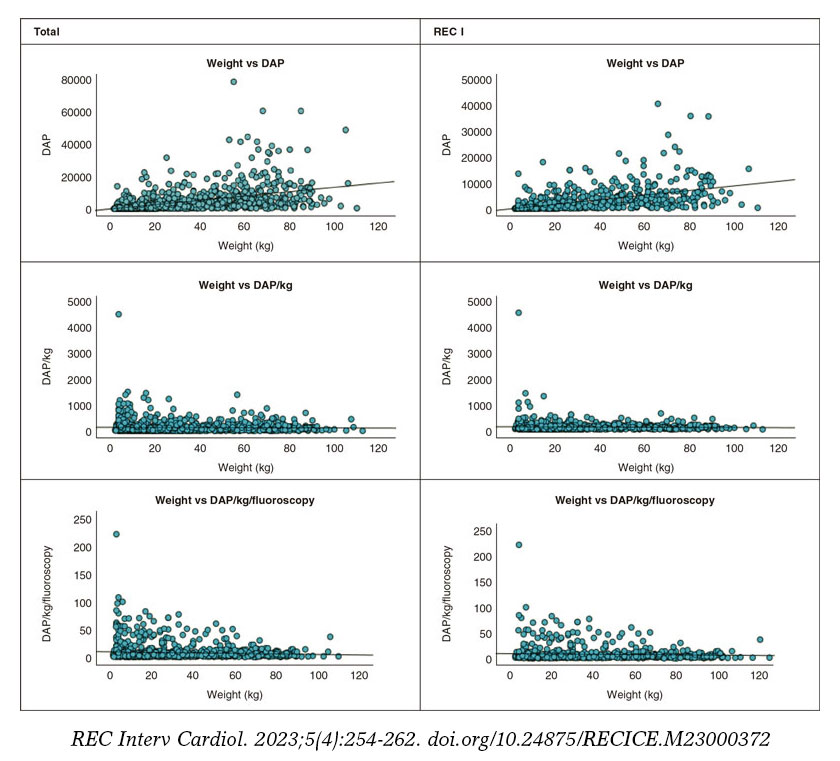
Figure 2. Scatter plots from the overall sample and radiation exposure categories (REC) group for the values of weight (kg) vs dose-area product (DAP) (µGy.m2), weight vs DAP/kg (µGy.m2/kg), and weight vs DAP/Kg/fluoroscopy (µGy.m2/kg/min). All plots from the overall sample and procedures from the REC I group are shown here (the remaining ones from the other groups are shown in the supplementary data). The lowest dispersion is seen in the central column of weight vs DAP/kg, both in the overall sample and in the REC I group.
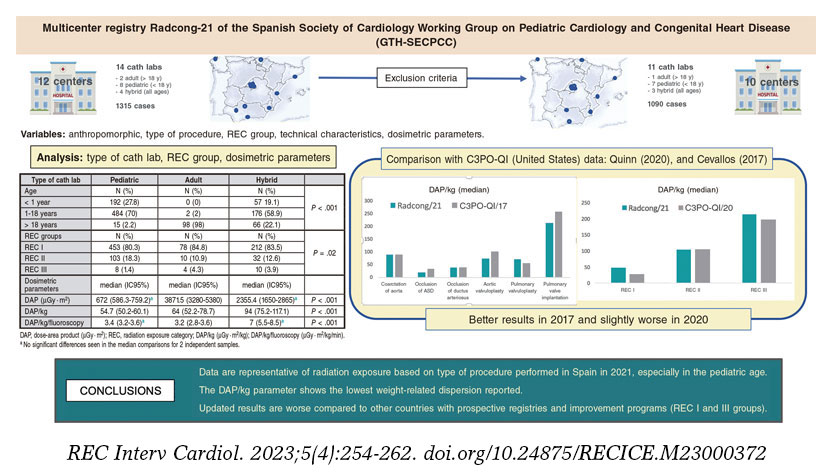
Figure 3. Central illustration. Summary of the design of case selection, results by type of cath lab, age, REC group, DAP/kg, and DAP/Kg/fluoroscopy compared to other registries and study conclusions. 95%CI, 95% confidence interval; ASD, atrial septal defect; DAP, dose-area product; REC: radiation exposure category.
DISCUSSION
As far as we know, the current is the first study ever published on the dose of radiation associated with interventional procedures performed in patients with congenital heart diseases in Spain. Radiation in the cardiac catheterizations of these patients should be the main concern since these are particularly long, complex, and intricate procedures. This problem mainly affects the pediatric population with congenital heart diseases who will undergo multiple cardiac catheterizations throughout their lives.24,25 Also, the dose accumulated by the operator is a relevant issue here, especially with pediatric patients in whom distance to the x-ray tube (which is key in the amount of radiation received26) is much shorter compared to the adult population. Therefore, the imaging modality used for image acquisition should follow the principles established in the «ALARA» concept (As Low As Reasonable Achievable) that includes recommendations like rationing the zoom, using collimation, proper table position, the characteristics of the beam (images per second, voltage, amperage), and image storage since fluoroscopy, instead of cine.27-30 Therefore, using the proper technique can reduce the dose of radiation received without changing the overall fluoroscopy times while observing enough clinical guarantees for the decision-making process and work at the CL.
There is a history of lower doses being received after the implementation of training programs involving machines, and interventional cardiologists,30,31 the development of specific image acquisition protocols,32,33 and the creation of registries on the amount of radiation received. Therefore, in the United States, several reports have been published on this topic drafted by the multicenter Congenital Cardiac Catheterization Outcomes Project Working Group founded back in 2006.34 Using data from this working group, in 2014, Ghelani et al. published the results of a retrospective study conducted from 2009 through 2013 to establish the dosimetric parameters of reference for 6 congenital diseases.35 Parallel to this, the Congenital Cardiac Catheterization Outcomes Project – Quality Improvement (C3PO-QI) for radiation dose optimization was developed. It included training seminars for health professionals on radiologic protection, information exchange between centers and manufacturers, image acquisition optimization protocols, the development of digital tools for registry purposes, and the identification of areas with room for improvement. Then, in 2017, Cevallos et al. published the results of a prospective registry conducted from 2014 through 2015.36 The implementation of such program resulted in lower doses of radiation for all the aforementioned diseases. Finally, in 2020, Quinn et al.37 presented the data prospectively included in the C3PO-QI from 2015 through 2017 on 40 simple or combined procedures grouped into the 3 REC groups previously proposed23 demonstrating a significant reduction in the dose of radiation received.
This study conducted by the GTH-SECPCC can lay the foundations for the development of similar programs in our country. The distribution of patients by age, procedure, and REC group is fairly similar to that of former registries with larger numbers of patients.34,36,37 Although 16.5% of the patients could not be categorized in any REC groups, most correspond to combined procedures or other angioplasties, which would presumably increase the number of patients in REC II or III groups. Maybe the greatest limitation of the Radcong-21 is the scarce participation of centers and CLs with special dedication to the adult population. The 31st Spanish Cardiac Catheterization and Coronary Intervention Registry of the Interventional Cardiology Association of the Spanish Society of Cardiology (ACI-SEC) included 527 interventional procedures performed on congenital heart diseases in adults in 2021.38 Although our series doesn’t cover the entire 2021 (just 100 cases per hospital), a total of 179 procedures are reported in individuals > 18 years, which is far from the numbers mentioned above. Nonetheless, almost all Spanish CLs with special dedication to pediatric congenital heart diseases participated in our registry (12 out of 14 total). Therefore, percentage wise, data from the Radcong-21 are very similar to the distribution per type of procedure in patients < 18 years in the 1st official report from the ACI-SEC and GTH-SECPCC on the 202039 Spanish Cardiac Catheterization and Coronary Intervention Registry including, predominantly, closure procedures of ASD and ductus arteriosus, and pulmonary angioplasty or coarctation of aorta.
Quantifying the dose of radiation received by an individual during cardiac catheterization is extremely challenging. The purpose of using coversion factors is overlooking the discrepancy among the different systems of measurement. However, we should mention that, on many occasions, these are based on artificial models and applied differently.40 To make things harder, there is not such a thing as a homogeneous criterion of units among the different manufacturers, which complicates direct comparisons among hospitals. For several authors, the closest parameter to the dose of radiation received by a patient is the DAP.36,37 Former studies say that fluoroscopy time is not indicative of the dose of radiation received since very different values like air kerma or DAP are associated with the same fluoroscopy times.33-37 Some suggest using weight-based air kerma.34 However, in our setting we, know that this parameter is not collected across centers on a routine basis. Consistent with former studies, our data show that with older age higher doses of radiation received, which can be explained by the patient’s increased weight (table 1). Other factors can significantly impact the dose of radiation received like the difficulty of each procedure and the operators’ experience. To minimize these limitations, DAP can be indexed based on weight (reduces the bias of increased radiation based on the characteristics of each patient) and fluoroscopy (reduces the bias of increased radiation due to the special complexity of the procedure or the operator’s lack of experience). Therefore, some authors suggest that DAP/kg would allow more reliable comparisons between procedures and age ranges.37 Others claim that it would only allow standardization among patients of the same age group with significant weight differences.36 According to our information, DAP/kg is the lowest dispersion value of the entire sample, and in type I REC (figure 2 and figure 1 of the supplementary data), which would recommend its use in comparative studies. According to our data, it is surprising to see that in some CLs with DAP/Kg values higher compared to other CLs, such a relation is inverted in the DAP/Kg/fluoroscopy parameter probably due to differences among operators like we mentioned before. Here we should mention the comparison between CL2, CL5, and CL7 with DAP/kg of 50, 52, 69.8, and DAP/Kg/fluoroscopy of 2.9, 2.2, and 2.6, respectively, and CL6 and CL8 with DAP/kg of 44.6 and 33.2, and DAP/Kg/fluoroscopy of 2.8 and 3.9, respectively. It would be interesting to do more in-depth analyses of these data in future studies to see what the variability is among operators across different centers or CLs.
If we compared our data to those published by C3PO-QI (table 4) we’ll be able to see that the numbers of DAP/kg from our series are better or similar to the ones published in 2017,36 yet unfavorable compared to REC I and III groups in 202037 (dose increases of 78% and 8.3%, respectively). Differences don’t seem to be too significant, especially if we consider the 95%CIs. They don’t relate to all the centers from the registry either. However, reflection should be made on the need for training and awareness policies on the amount of radiation received while performing cardiac catheterizations in our country.
Table 4. Comparison between Radcong-2021 and data from the C3PO-QI from 2017,19 and 202020
| Prevalent diseases | Radcong-2021 | C3PO-QI 201719 | |||
|---|---|---|---|---|---|
| n (% total) | PDA/kga (IC95%) | PDA/kga (P95) | n (% total) | DAP/kg (95thP) | |
| Coarctation of aorta | 66 (6.1%) | 90.2 (56.7-121.1) | 90.2 (413) | 288 (3.3%) | 90 (384) |
| Occlusion of ASD | 128 (11.7%) | 20.5 (18.1-26.1) | 20.5 (358) | 295 (3.4%) | 34 (199) |
| Occlusion of ductus arteriosus | 155 (14.2%) | 37.5 (31.8-44.4) | 37.5 (216) | 443 (5.1%) | 37 (217) |
| Aortic valvuloplasty | 29 (2.7%) | 72.1 (52.7-129.5) | 72.1 (284) | 136 (1.6%) | 99 (383) |
| Pulmonary valvuloplasty | 67 /6.2%) | 71.2 (48.6-90) | 71.2 (450) | 258 (3%) | 53 (335) |
| Pulmonary valve implantation | 22 (2%) | 213.5 (161.9-291.6) | 213.5 (327) | 199 (2.3%) | 257 (671) |
| REC group | Radcong-2021 | C3PO-QI 202020 | |||
| N (% total) | DAP/kga (95%CI) | N (% total) | DAP/kga (95%CI) | ||
| REC I | 743 (81.6%) | 48.1 (43.6-53.1) | 10 649 (70%) | 27 (7-66) | |
| REC II | 145 (16%) | 104.7 (80.7-130) | 2771 (18%) | 106 (50-216) | |
| REC III | 22 (2.4%) | 213.5 (161.9-291.6) | 1837 (12%) | 197 (13-119) | |
|
95%CI, 95% confidence interval; 95thP, 95th percentile of the median; ASD, atrial septal defect; DAP, dose-area product; REC, radiation exposure category. |
|||||
Limitations
This study has some limitations due to its retrospective nature. Data mining was voluntary and unaudited. The participant centers had different volumes of patients, which is why the time interval to meet the goal of procedures set was not constant. This criterion was followed to promote the representativity of the reality nationwide that can be considered appropriate in the pediatric, not in the adult age, where participation dropped. Contribution from the operator’s own experience or the technical quality of the CL to the dose of radiation can be a confounding factor. Still, it is part of the day-to-day reality of a CL. Patients with repeated procedures could not be considered either or those in whom additional imaging modalities plus the scheduled catheterization were performed, which led to increased doses of radiation.
CONCLUSIONS
Representative data from age and procedure-based dosimetric parameters in catheterizations performed in patients with congenital heart disease in Spain in 2021 were obtained. The DAP/Kg parameter has the lowest dispersion from the sample. Results are representative of the pediatric reality in our country since they include almost all centers performing interventional procedures. These results could be used as the reference in this age range, but just as a mere guidance among adults. Overall, the results obtained are worse compared to other countries with prospective registries and training and improvement programs in this area. Figure 3 shows the registry design, overall general results, and final conclusions.
Keeping registries helps control quality of care and identify areas with room for improvement. Training and educational programs in this area should be conducted, and prospective registries with more adult CLs. Therefore, this registry is an important step forward to develop future improvement programs or projects in this area at both local and national level.
FUNDING
This study received no specific funding from public, private or non-profit organizations.
AUTHORS’ CONTRIBUTIONS
F. Rueda Núñez, B. Insa Albert, C. Abelleira Pardeiro, and M. Álvarez-Fuente drafted the manuscript. V. Balboa Barreiro conducted the statistical analysis. All the authors contributed to the study idea and design, data curation, critical review, and final approval of the manuscript.
CONFLICTS OF INTEREST
None whatsoever.
WHAT IS KNOW ABOUT THIS TOPIC?
- On many occasions, cardiac catheterization is needed to treat patients with congenital heart diseases at an early age and, repeatedly, over time across the patient’s lifetime. These are long and complex procedures that increase the risk of radiation exposure for both patients and health professionals.
- Local registries are needed to establish reference values of radiation exposure per type of procedure and patient.
- The implementation of registries and training programs reduces the dose of radiation as seen in prospective studies.
WHAT DOES THIS STUDY ADD?
- This is the first study ever conducted in our country on dosimetric parameters of cardiac catheterizations in patients with congenital heart diseases.
- Representative data on age and procedure-based dosimetric parameters in congenital cardiac catheterizations performed in Spain in 2021 were obtained. Therefore, reference values regarding comparative or prospective studies have been established, especially in the pediatric age.
- Overall, results in our country are worse compared to other countries with prospective registries and training and improvement programs in this area.
SUPPLEMENTARY DATA

REFERENCES
1. International Commission on Radiological Protection. ICRP Publication 103: The 2007 Recommendations of the International Commission on Radiological Protection. Ann ICRP. 2007;37:1-332.
2. Real Decreto 1976/1999, de 23 de diciembre, por el que se establecen los criterios de calidad de radiodiagnóstico. Boletín Oficial del Estado núm. 311, de 29 de diciembre de 1999. Available at: https://www.boe.es/eli/es/rd/1999/12/23/1976. Accessed 1 Oct 2022.
3. Real Decreto 601/2019, de 18 de octubre, sobre justificación y optimización del uso de las radiaciones ionizantes para la protección radiológica de las personas con ocasión de exposiciones médicas. Boletín Oficial del Estado núm. 262, de 31 de octubre de 2019, páginas 120840 a 120856. Available at: https://www.boe.es/eli/es/rd/2019/10/18/601. Accessed 1 Oct 2022.
4. Sánchez RM, Vano E, Fernández JM, Escaned J, Goicolea J, Pifarré X; DOCCACI Group. Initial results from a national follow-up program to monitor radiation doses for patients in interventional cardiology. Rev Esp Cardiol. 2014;67:63-65.
5. Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Epidemiology. 2007;18:805-835.
6. Quinn BP, Armstrong AK, Bauser-Heaton HD, et al. Congenital Cardiac Catheterization Project on Outcomes-Quality Improvement (C3PO-QI). Radiation Risk Categories in Cardiac Catheterization for Congenital Heart Disease: A Tool to Aid in the Evaluation of Radiation Outcomes. Pediatr Cardiol. 2019;40:445-453.
7. Andreassi MG, Ait-Ali L, Botto N, Manfredi S, Mottola G, Picano E. Cardiac catheterization and long-term chromosomal damage in children with congenital heart disease. Eur Heart J. 2006;27:2703-2708.
8. Andreassi MG. Radiation risk from pediatric cardiac catheterization: friendly fire on children with congenital heart disease. Circulation. 2009;120:1847-1849.
9. Ingwersen M, Drabik A, Kulka U, et al. Physicians’ radiation exposure in the catheterization lab: ¿does the type of procedure matter? JACC Cardiovasc Interv. 2013;6:1095-1102.
10. Patel C, Grossman M, Shabanova V, Asnes J. Reducing radiation exposure in cardiac catheterizations for congenital heart disease. Pediatr Cardiol. 2019;40:638-649.
11. Justino H. The ALARA concept in pediatric cardiac catheterization: techniques and tactics for managing radiation dose. Pediatr Radiol. 2006;36(Suppl 2):146-153.
12. Chida K, Kato M, Saito H, et al. Optimizing patient radiation dose in intervention procedures. Acta Radiol. 2010;51:33-39.
13. Hill KD, Frush DP, Han BK, et al. Image Gently Alliance. Radiation Safety in Children with Congenital and Acquired Heart Disease: A Scientific Position Statement on multimodality dose optimization from the Image Gently Alliance. JACC Cardiovasc Imaging. 2017;10:797-818.
14. Verghese GR, McElhinney DB, Strauss KJ, Bergersen L. Characterization of radiation exposure and effect of a radiation monitoring policy in a large volume pediatric cardiac catheterization lab. Catheter Cardiovasc Interv. 2012;79:294-301.
15. Boudjemline Y. Effects of reducing frame rate from 7.5 to 4 frames per second on radiation exposure in transcatheter atrial septal defect closure. Cardiol Young. 2018;28:1323-1328.
16. Glatz AC, Patel A, Zhu X, et al. Patient radiation exposure in a modern, large-volume, pediatric cardiac catheterization laboratory. Pediatr Cardiol. 2014;35:870-878.
17. Kobayashi D, Meadows J, Forbes TJ, et al. Standardizing radiation dose reporting in the pediatric cardiac catheterization laboratory. A multicenter study by the CCISC (Congenital Cardiovascular Interventional Study Consortium). Catheter Cardiovasc Interv. 2014;84:785-793.
18. Ghelani SJ, Glatz AC, David S, et al. Radiation dose benchmarks during cardiac catheterization for congenital heart disease in the United States. JACC Cardiovasc Interv. 2014;7:1060-1069.
19. Cevallos PC, Armstrong AK, Glatz AC, et al. Radiation dose benchmarks in pediatric cardiac catheterization: A prospective multi-center C3PO-QI study. Catheter Cardiovasc Interv. 2017;90:269-280.
20. Quinn BP, Cevallos P, Armstrong A, et al. Longitudinal Improvements in Radiation Exposure in Cardiac Catheterization for Congenital Heart Disease: A Prospective Multicenter C3PO-QI Study. Circ Cardiovasc Interv. 2020;13:e008172.
21. Freixa X, Jurado-Román A, Cid B, Cruz-González I; en representación de la ACI-SEC. Registro español de hemodinámica y cardiología intervencionista. XXXI Informe Oficial de la Asociación de Cardiología Intervencionista de la Sociedad española de Cardiología (1990-2021). Rev Esp Cardiol. 2022;75:1040-1049.
22. Ballesteros F, Coserría F, Romaguera R, et al. Registro español de intervencionismo en cardiopatías congénitas. Primer informe oficial de la ACI-SEC y el GTH-SECPCC (2020). REC Interv Cardiol. 2022;4:173-180.
23. Chida K, Kagaya Y, Saito H, Ishibashi T, Takahashi S, Zuguchi M. Evaluation of patient radiation dose during cardiac interventional procedures: what is the most effective method? Acta Radiol. 2009;50:474-481.












