
A 53-year-old man was treated with extracorporeal cardiopulmonary resuscitation with the controlled automated reperfusion of the whole body (CARL) system (Resuscitec, Germany) after a refractory in-hospital cardiac arrest following an arrhythmic storm in the setting of an episode of inflammatory cardiomyopathy. The patient required Impella-CP device implantation (Abiomed, United States) via femoral access due to insufficient unloading with the intra-aortic balloon pump. Catheter malapposition was suspected after several suction alarms were triggered. Despite repeated attempts at repositioning, flow rates remained < 1 L/min. Transesophageal echocardiography and thoracic x-ray (figure 1) confirmed that the catheter had bent in upon itself (asterisk in the figure), and the pigtail had been caught in the outlet (figure 2) following the multiple attempts at repositioning. The catheter migrated toward the descending aorta and urgent removed was decided. An attempt to unscrew the pigtail through femoral manipulation proved unsuccessful (figure 3A and video 1 of the supplementary data). A 7-Fr Amplatz Super-Stiff guidewire (Boston Scientific, United States) was advanced through the Impella loop via left radial access, and traction on the catheter from the femoral access successfully disengaged the pigtail from the outlet (figure 3B). Concurrently, a 12 mm × 20 mm EN-Snare loop (Merit Medical, United States) was inserted to capture the tip of the pigtail (figure 3C). The guidewire was removed and traction was applied simultaneously to the Impella device and the pigtail tip, which extended the Impella (figure 3D and video 2 of the supplementary data) and allowed its extraction through its introducer. We decided not to restart the device due to the risk of thrombosis in its interior, and chose to remove it using a 14-Fr transaortic pigtail catheter through the Impella access.
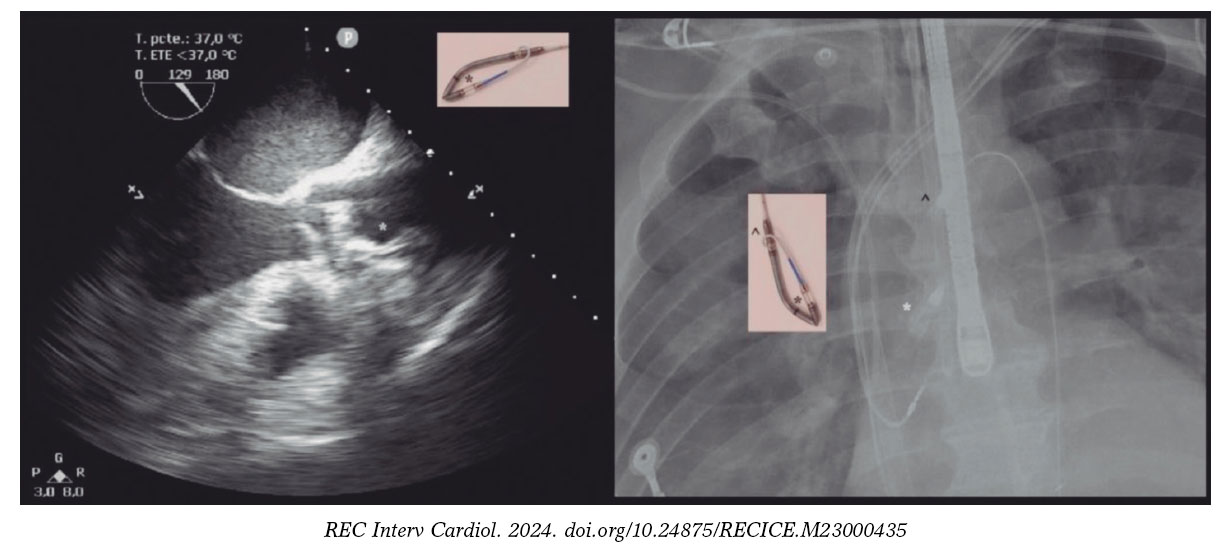
Figure 1.
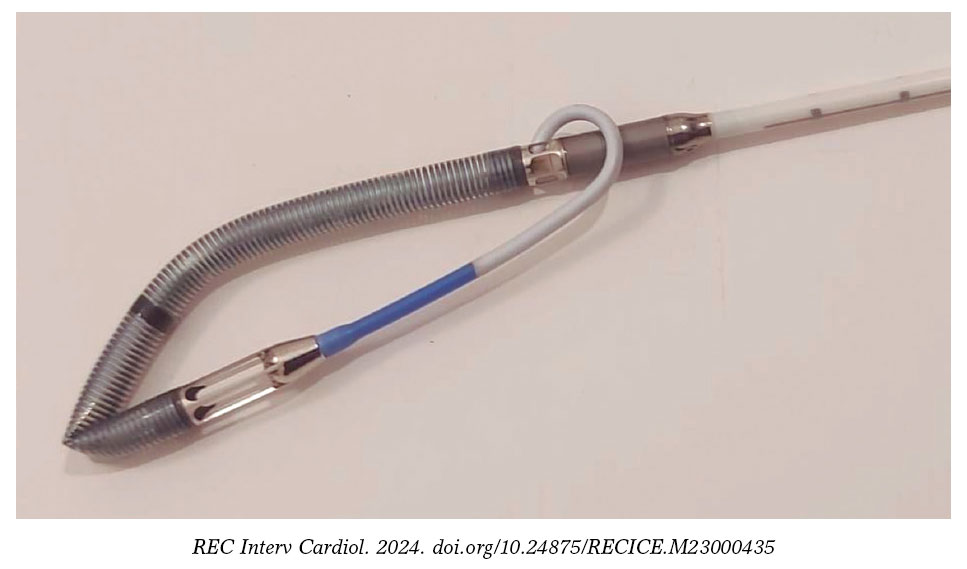
Figure 2.
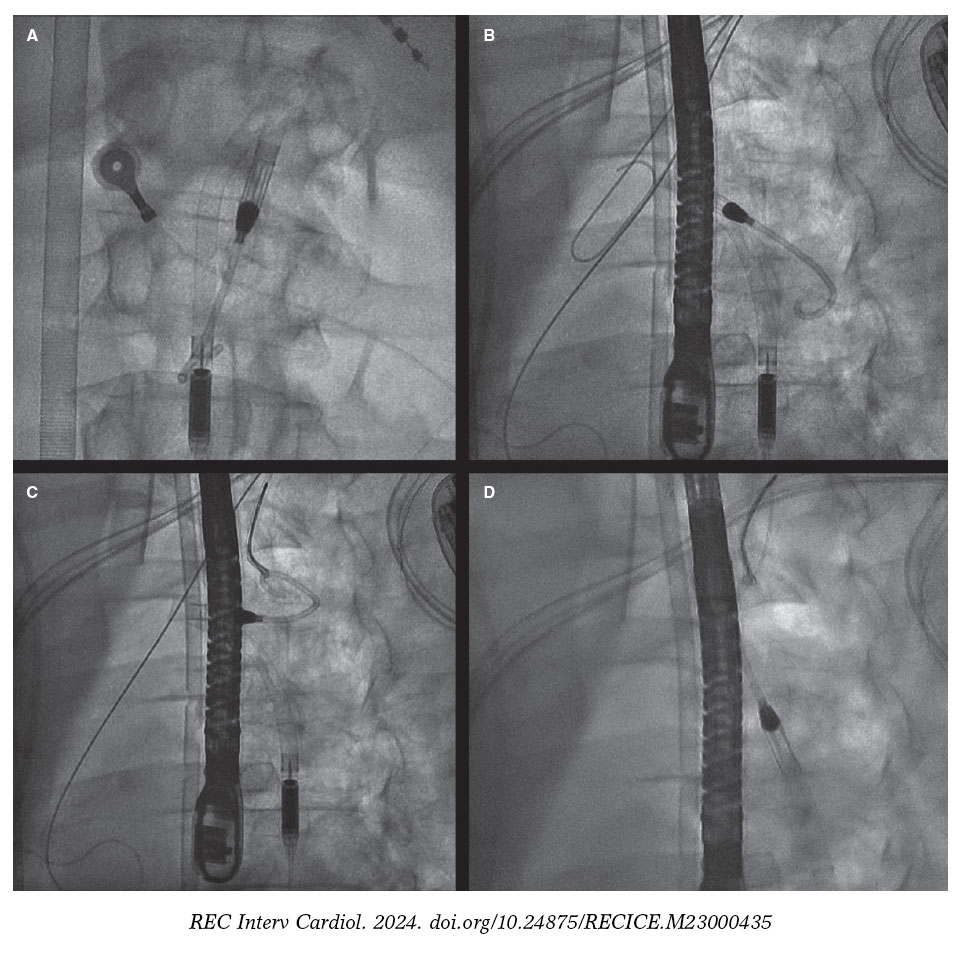
Figure 3.
A deep understanding of medical devices is of paramount importance to recognize rare complications and optimize outcomes.
FUNDING
None declared.
ETHICAL CONSIDERATIONS
The authors declared to have obtained the prior written informed consent the patient for publication, reproduction, and disclosure in print and online through REC Interventional Cardiology. The work was conducted in full compliance with the international recommendations on clinical research set forth in the Declaration of Helsinki.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
The authors declare they did not use artificial intelligence in the preparation of this article.
AUTHORS’ CONTRIBUTIONS
All authors contributed equally to the preparation of the article.
CONFLICTS OF INTEREST
None declared.
SUPPLEMENTARY DATA
Vídeo 1. Plaza Martín M. DOI: 10.24875/RECICE.M23000435
Vídeo 2. Plaza Martín M. DOI: 10.24875/RECICE.M23000435












