
We present the case of a 42-year-old woman admitted due to ST-segment elevation acute coronary syndrome. The coronary angiography revealed the presence of an occluded mid-distal left anterior descending coronary artery (LAD) (figure 1A, asterisk) with an image suggestive of intramural hematoma (IMH) consistent with spontaneous coronary artery dissection (figure 1A, arrow). Guidewires were passed through the distal and diagonal LAD that resulted in flow recovery (figure 1B, line and arrowheads outlining the IMH). The intravascular ultrasound (IVUS) confirmed the presence of a large 25 cm long IMH (figure 2A,D). After dilatation with a 2.0 mm/6 mm cutting balloon (Wolverine, Boston Scientific, United States) (figure 1C, asterisks) flow improved leaving a mild residual stenosis (figure 1D). After a few minutes the retention of contrast in the LAD was confirmed (figure 3A, ellipse) followed by ischemic changes on the electrocardiogram. The angiography revealed the presence of 2 regions of critical stenosis with aggravated distal flow abnormalities (figure 3B, lines outlining the IMH, arrowheads showing the stenotic regions). A 2.25 mm/33 mm drug-eluting stent was implanted (Ultimaster Tansei, Terumo, Japan) (figure 3C, asterisks) and later dilated up to 2.75 mm with excellent angiographic (figure 3D) and IVUS results (figure 2E,F). The entire procedure is summarized on video 1 of the supplementary data.
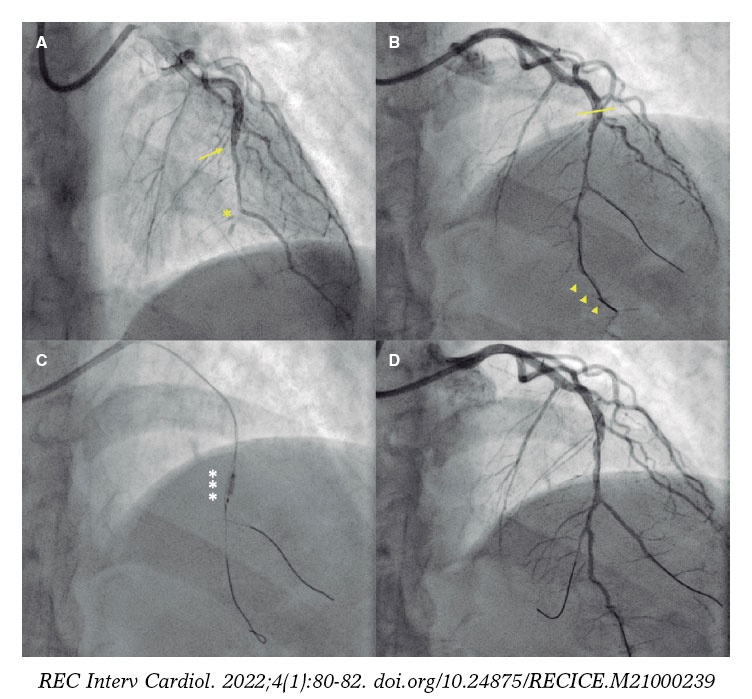
Figure 1.
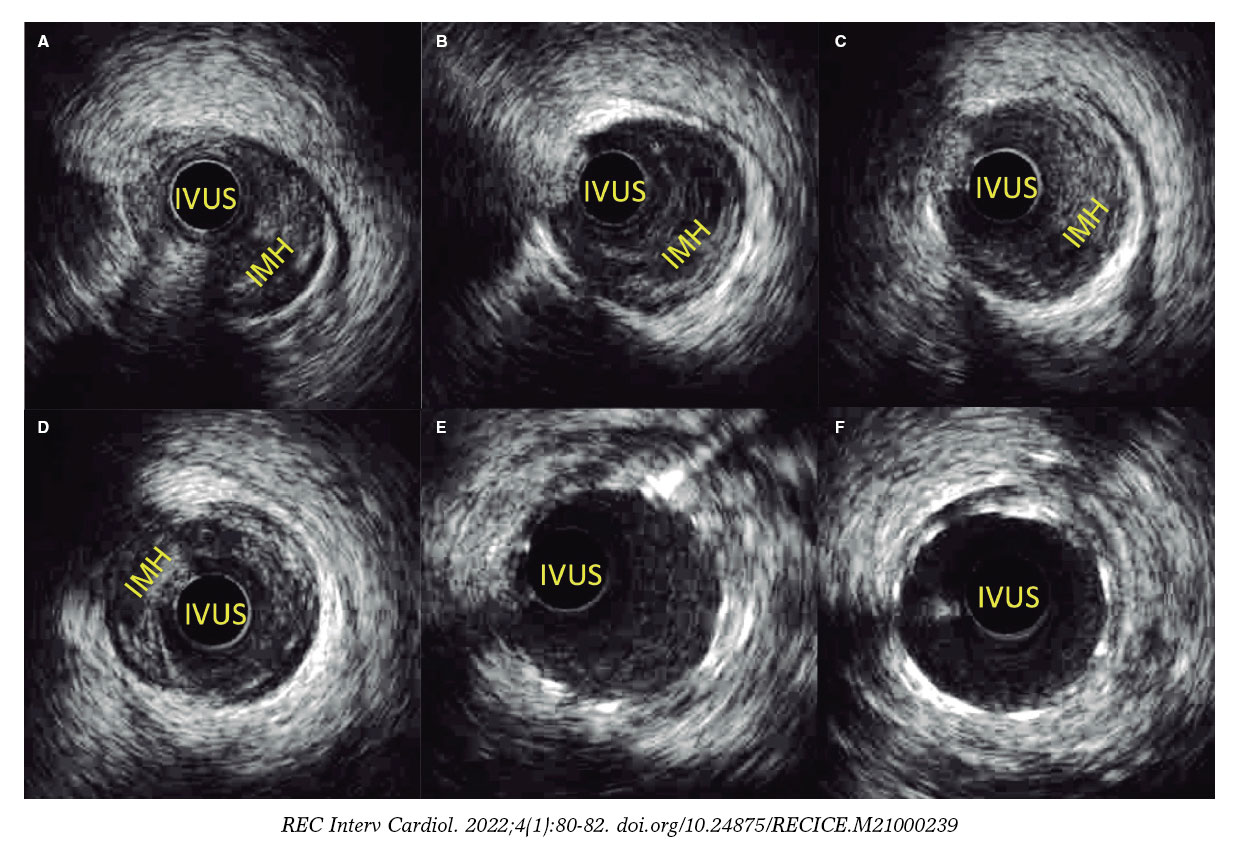
Figure 2.
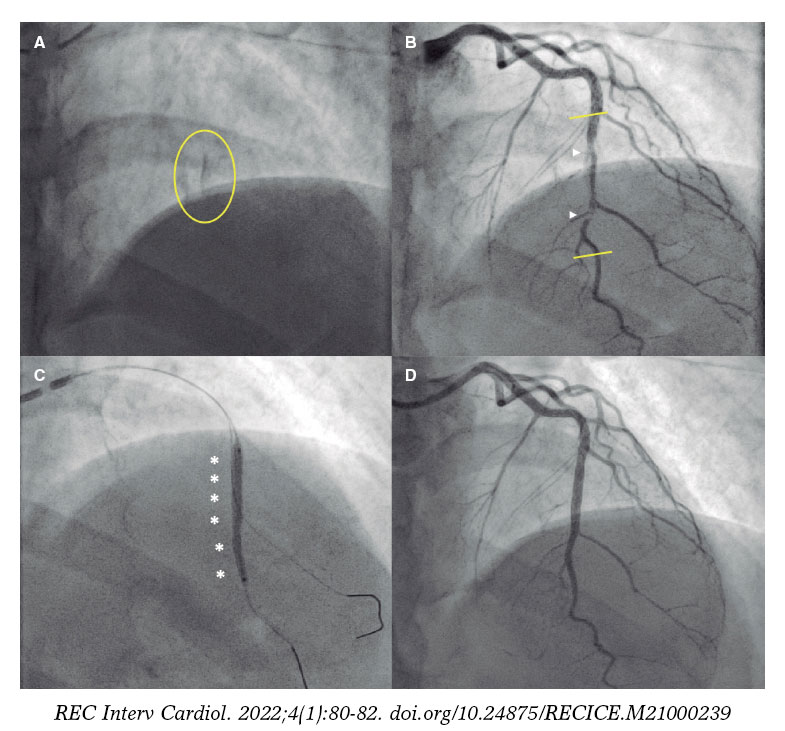
Figure 3.
The patient’s informed consent case was obtained before publishing the case.
We reported our experience on the isolated use of a cutting balloon during percutaneous coronary intervention to treat spontaneous coronary artery dissection to generate the fenestration of the IMH and, eventually, reduce the possible risk of spreading. The use of the cutting balloon before stent implantation can also prevent the spread of IMH after implantation. This case illustrates the fact that, sometimes, the totally unpredictable evolution of the isolated strategy makes stent implantation necessary to guarantee good distal flow and prevent coronary artery re-occlusion.
FUNDING
None.
AUTHORS’ CONTRIBUTIONS
M. Vicente, and García-Guimaraes designed the study and wrote the manuscript. N. Salvatella, A. Aparisi, A. Negrete, and B. Vaquerizo performed the critical review of the manuscript.
CONFLICTS OF INTEREST
The authors declared no conflicts of interest whatsoever.
SUPPLEMENTARY DATA
Vídeo 1. Vicente M. DOI: 10.24875/RECICE.M21000239












