
Innovation in interventional cardiology
High-definition intravascular ultrasound
30/04/2019

In certain fields, the high quality and excellence of existing materials make continued innovation difficult. Transradial introducer sheaths represent one such field.
In 2020, Cardinal Health (USA) presented the RAIN Sheath vascular introducer. This device has an ultrafine wall that allows it to have an outer diameter that is one French smaller than that of the catheter that will be passed through it. For example, for a 6-French catheter, the outer profile of the introducer is equivalent to that of a 5-French. It is made with a polymer that has elastomeric qualities that provide great flexibility and better resistance to torsion than other similar devices on the market. Thin-walled introducers are prone to torsion and lumen collapse, but this is avoided thanks to the properties of the RAIN Sheath.
One of the key innovations is that it is available in 4, 5, 6 and 7 French, for cases in which the radial artery is very small caliber but radial access is nonetheless required. Other details are its high-performance hydrophilic coating, which facilitates atraumatic entry and withdrawal, as well as a hexacuspid valve that prevents bleedback.
As with other commonly-used introducers, it comes in a kit with a 45 cm, 0.021’’ diameter metal or polymer guidewire and a 21 G bare needle or IV catheter needle.
Palabras clave: intervención coronaria percutánea, introductor vascular, acceso radial. Keywords: percutaneous coronary intervention, vascular sheath, radial access.

A new coronary angioplasty guidewire has been brought to the North American market. This hybrid guidewire combines several technologies. It is produced by the company Asahi Intecc (Japan), which, in my opinion, is a guarantee of success. It is called Minamo and it has a three-piece coaxial core. These pieces are, from proximal to distal: a round stainless steel core, followed by a tapered nitinol core, and most distally, a stainless steel round press core. This end segment is surrounded by a 170 mm coil, with the most distal 30 mm containing braided wires with ACT One technology. As is well known, this section with ACT One technology allows the preshaped curve to retain its shape for a longer time and be reshaped as many times as necessary without breaking the guidewire. It can be preshaped easily with a special needle, and even it this is done several times, it forms a perfect J curve without distortion.
The Minamo guide wire is suitable for everyday use in most interventional procedures. It has a tip load of 0.5 gf. The most distal 25 mm of the tip is silicone-coated, and the remainder is hydrophilic-coated.
Palabras clave: intervención coronaria percutánea, guía de angioplastia coronaria. Keywords: percutaneous coronary intervention, coronary wire.

The practice of working with robots has been incorporated for some time in many surgical specialties. In cardiac catheterization, great advances in the development of devices have allowed us to treat cardiac conditions that would previously have been unthinkable. The way we perform catheterization has not changed much since 1958, when the first angiography was performed, and physicians are still exposed to disease-causing radiation and have to tolerate the weight of lead aprons. Robots allow us to perform an intervention on a patient, not only from a physical distance, but also a geographical distance. This could be a solution to the problem of certain acute patients accessing – in a timely manner – centers with interventional facilities (24 hours a day, 7 days a week, 365 days a year).
A very advanced system, from Corindus (recently acquired by Siemens) has been around for years, undergoing frequent improvements. Another, lesser-known system is also available – Robocath1.
This system has two key components. The first is an articulated arm that holds a device where the guide catheter, angioplasty guidewire, and balloons or stents are placed along with the connections to the infusion pump and saline flush. The second is a mobile control unit, which contains the screens, two joysticks – one to steer the catheter and one for the guidewire – the control for contrast injection and the controls for the table.
The aim of robotic assistance in cardiac catheterization is to perform the procedures safely, comfortably, and accurately, working in the best interests of the patients. It is clear that telemedicine will undergo substantial development in the coming years, as we have seen during 2020 with the COVID-19 pandemic. The problem with robotic assistance in cardiac catheterization is that currently it can be used for simple cases, but a lot of fine tuning is still needed for more complex cases and complications that may arise during procedures. It is a very interesting area of innovation that has a lot of future potential.
BIBLIOGRAFÍA
1. Robocath. 2021. Available at https://www.robocath.com/. Accessed 4 Jan 2021.
Palabras clave: intervención coronaria percutánea, asistencia robótica. Keywords: percutaneous coronary intervention, robotic-assisted.
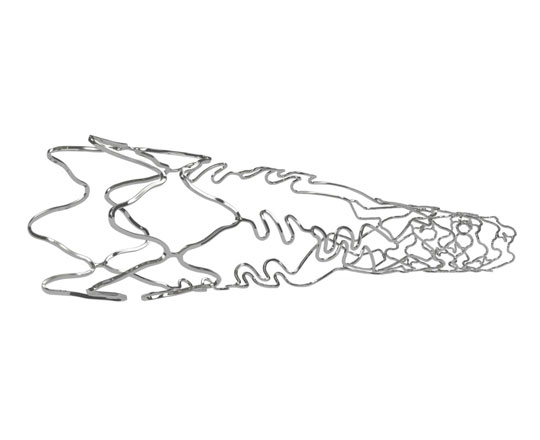
Older devices can be revived with innovative technological improvements. This is the case for the design of a stent specifically for bifurcations, now called Biomime Branch (Meril, India).
This is a chrome-cobalt stent with 65 µm strut thickness. It is covered with a resorbable PLGA-PLLA polymer that elutes sirolimus at a dose of 1.25 µg/mm2. The device’s architecture is interesting because it has a hybrid design, which is very useful for treating 1,1,1 bifurcations in which there is a very high probability of needing more than one stent. It is mounted on a balloon (with four radio-opaque markers) with a tapered design, which allows stent implantation from the main branch into the side branch. The proximal segment (which is positioned in the main branch) has a closed-cell design and the distal segment (for the side branch lesion) has an open-cell design. The distal segment has a variable length, from 6.5 to 13 mm, to ensure coverage of side branch lesions.
Between the two segments there is a transition zone with three panels with highly flexible connectors that leave large open spaces, allowing access to the main branch to implant a further stent without the risk of losing the side branch, and avoiding overexpansion of the stent at post-dilatation. This reduces the risk of losing important branches with severe lesions.
In my opinion, this is a very interesting device, as it simplifies the procedure, reduces the intervention time when it is likely that 2 stents will be implanted, and limits the amount of metal that may be exposed at the carina.
Palabras clave: Intervención coronaria percutánea, bifurcación coronaria, stent coronario para bifurcación, stent coronario liberador de droga. Keywords: Percutaneous coronary intervention, coronary bifurcation, bifurcation dedicated stent, drug eluting stent.
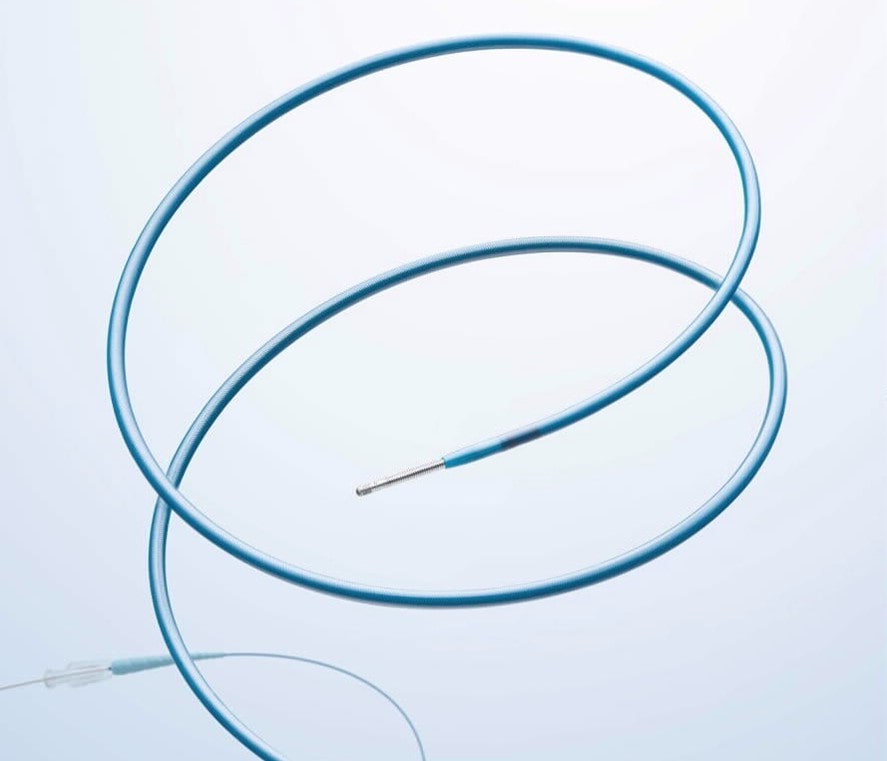
New on the market is a microcatheter bearing the Medtronic stamp (USA). Medtronic, in collaboration with Surmodics Inc. (USA), has released a microcatheter that aspires to become the standard for multiuse microcatheters in percutaneous coronary intervention. Surmodics is a company specialized in the production of hydrophilic coatings that has been collaborating with Medronic for many years on a mission to improve the performance of their devices.
The Telemark microcatheter has three key features:
- It is made of a mixed (flat and round) braided mesh with Xtreme technology, which provides improved push force transmission.
- It has a Pristyne hydrophilic coating, which improves deliverability and lesion crossing.
- It has a very low-profile, tapered design, from 2.6 to 1.4 French.
The crossability, deliverability, and lubricity of this microcatheter are significantly superior to that of other standard microcatheters on the market. Use of this Telemark device will soon become established in everyday clinical practice.
Palabras clave: microcatéter, oclusión coronaria crónica total. Keywords: microcatheter, chronic total occlusion.