
Innovation in interventional cardiology
High-definition intravascular ultrasound
30/04/2019

The OmniWire pressure guide wire (Philips, Netherlands) is the first solid-core pressure guide wire to appear on the market. Normally, pressure guide wires are produced with a hypotube that houses the fibers and leads connected to the intracoronary pressure sensor. This design means the guide wire requires a more delicate handling and is less durable during the procedure.
The OmniWire guide wire has a robust design that is completely new from top to bottom. The composition of its materials is very complex, and a lot has been invested in its industrial design.
From distal to proximal it has 4 sections. The most distal section has a molded band of stainless steel with a rounded platinum-alloy tip. This radiopaque tip is 3 cm long and weighs 0.53 g; it is, therefore, a soft, atraumatic guide wire. The core is made of Nitinol, a very elastic alloy, with high durability and shape memory. Outside, covering the Nitinol core, it has a flexible length polymer coating (which does not include the coil tip). Proximal to these 3 cm, it contains the integrated pressure sensor. The remaining length of the guide wire is integrated in the solid proximal core, made of a cobalt alloy that guarantees torque, pushability, and resistance to torsion.
One of the advantages of this device is the length of its hydrophilic coating, over the distal 39 cm of the guide wire, which ensures navigability in more troublesome areas. The remaining length has a hydrophobic coating (PTFE) from 146 cm up to the most proximal part of the guide wire.
I think it will be a significant improvement in guide wire usage.
Keywords: Pressure guide wire, coronary circulation.

New to the market is the Hi-Torque Infiltrac guide wire (Abbott, United States), a new angioplasty guide wire with high penetration power for the treatment of chronic occlusions.
It is a tapered (0.009'') guide wire made of hydrophilic-coated Durasteel stainless steel, providing better lubricity and facilitating movement within the microcatheter. The distal 3 cm are radio-opaque, and the tip does not have a hydrophilic-coating to offer better control and tactile feedback.
The Hi-Torque Infiltrac guide wire’s special tip technology has great penetration power thanks to its unique microtexture design, which provides greater feedback and safety during procedures. Another key characteristic is the guide wire’s pre-formed 1-mm Micro-J tip with 25° angulation, which provides steerability and facilitates access to the occlusion without causing prolapse.
The guide wire is available in two tip loads and penetration powers to facilitate access to all types of occlusion: Hi-Torque Infiltrac, at 11 g and 167 kg/in2, and Hi-Torque Infiltrac Plus, at 14 g and 224 kg/in².
Given its design, it looks to be a candidate for antegrade wire escalation in cases with a proximal capsule resistant to penetration.
Keywords: percutaneous coronary intervention, coronary guidewire, coronary chronic total occlusion.

The Perclose ProStyle system (Abbott Vascular Inc, United States) is the newest generation of the Perclose vascular closure family, designed to percutaneously apply a suture to close the femoral artery or vein access site in patients undergoing diagnostic or interventional catheterization procedures. We could describe its function as a vascular closure system that, as well as closing the access site, repairs it.
Hemostasis is achieved by approximating the edges of the vessel wall with a biocompatible surgical suture to promote healing by primary intention,1 leaving smaller scars,2 allowing immediate re-access, and reducing the time to ambulation and hospital discharge.3
This new system comprises three elements that help the user to position, approximate, tie off and then cut the remaining ends of the suture:
- A Perclose ProStyle device designed to ensure greater needle resistance and ease of use.
- The device sheath contains a large, white, guide-wire exit port for better visibility and easier guide wire insertion. The proximal, metal part of the guide wire has reference markers that provide a visual estimation of the depth of the subcutaneous tract during suture deployment. The distal, hydrophilic-coated guide wire allows smoother advancement of the device and increases needle resistance, to minimize deviation in thickened tissues. The plunger has an improved spring to ensure better-controlled placement of the needles at the foot without a rebound affect.
- A suture trimmer and a snare-knot pusher, designed to approximate the knot to the top part of the access site. The suture trimmer has a metallic, hydrophilic-coated sheath, depth reference markers that line up with those of the device, and a more rigid cutting lever to reduce the possibilities of accidental cutting. The snare-knot pusher has been included as an additional low-profile accessory to facilitate advancing the knot in cases of deeper access.
BIBLIOGRAFÍA
1. FDA Databases. Perclose™ ProStyle™ SMCR System - Instructions for Use. Available at https://fda.report/GUDID/28717648235188. Accessed 10 Apr 2021.
2. Mercandetti, M. Wound Healing and Repair. Medscape. 02 Apr 2019. Available at: https://emedicine.medscape.com/article/1298129-overview. Accessed 10 Apr 2021.
3. Bhatt DL, Raymond RE, Feldman T, et al. Successful "pre-closure" of 7Fr and 8Fr femoral arteriotomies with a 6Fr suture-based device (the Multicenter Interventional Closer Registry). Am J Cardiol. 2002;89:777-779.
Keywords: percutaneous vascular closure device.
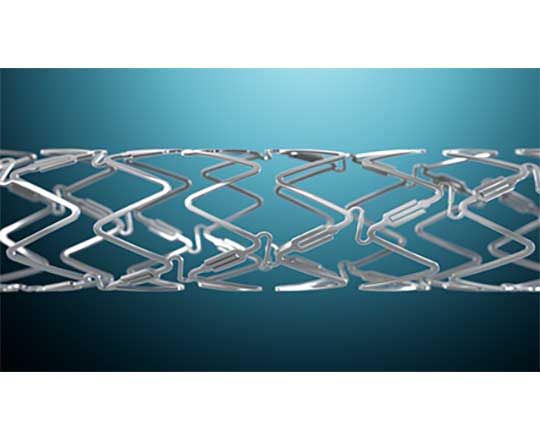
The DynamX Bioadaptor (Elixir Medical Corporation, United States), is a novolimus-eluting stent with a bioresorbable polymer coating. However, the stent has a unique hybrid design, with metallic segments that fit together with resorbable polymer connections.
Once implanted, the stent’s resorbable polymer elutes the drug (novolimus) for the first 3 months, and the polymer and connections between the metallic parts resorb over the next six months. This process uncages some elements of the stent in the artery and the rigid metallic structure is freed, allowing a more physiological positive adaptive remodeling of the vessels. This restores the pulsatile movement of the vessel and the physiological cyclical pressure and returns the artery to its original angulation so that it can move with the natural expansion and contraction, unlike a conventional metallic stent.
The first patient has just been enrolled in the BIOADAPTOR study, a multicenter, single-blind randomized clinical trial that will enroll 444 patients (mainly in Japan and Germany) treated with DynamX Bioadaptor with a 1:1 randomization versus Resolute Onyx (Medtronic, United States). It will be very interesting to see if there is any place for resorbable technology in coronary metallic stents.
Keywords: percutaneous coronary intervention, drug-eluting stent.

PulseCath iVAC2L (Terumo, Japan), is a percutaneous pulsatile pump for use as short-term mechanical circulatory support. It currently has the CE mark for use in high-risk coronary interventions, but is not indicated for use in cardiogenic shock. After transfemoral implantation via an 18-French sheath, this device increases cardiac output up to 2 L/min, maintaining sufficient coronary and vital organ perfusion and reducing the ventricular systolic workload.
Unlike other mechanical devices that use a continuous flow or axial pump, the iVAC2L has the advantage of being suitable to combine with any counterpulsation balloon console. As it does not need a special console, its operation is simplified and its costs are reduced. Another advantage is that it generates a more physiological pulsatile flow that is less deleterious for the patient.
The helium is connected to an external, transparent, flexible-membrane pump and in turn to the catheter. The catheter has a two-way valve 6 cm from the distal tip of the catheter, where there is an inlet. During systole, blood is aspirated from the left ventricle toward the membrane pump, and during diastole it is expelled toward the ascending aorta via a lateral outlet in the catheter. This process is synchronized with the cardiac cycle thanks to the counterpulsation balloon, reducing the systolic load and oxygen demand. Electrocardiography or the pressure waveform trigger the moment at which the helium enters the membrane pump, synchronizing the pump with the heart, and preserving neurohumoral pathways better than other mechanical support systems.
The device causes minimal hemolysis, similar to other devices already on the market.
An important disadvantage is its current requirement for 18-French femoral access, compared with the 12-French, and possibility of single access, offered by the competition.
Keywords: coronary disease, heart failure, high-risk percutaneous coronary intervention, mechanical circulatory support.