
CASE RESOLUTION
The procedure was performed under general anesthesia and with the administration of the standard dose of sodium heparin to prevent thrombosis or systemic embolisms (high risk considering the patient’s condition) via venous femoral access.
This procedure was planned using 3D reconstruction through rotational angiography (figure 1 and video 1 of the supplementyary data). Embolization was guided using the roadmapping technique that merges the 3D reconstruction simultaneously while overlapped to the 2D reconstruction in the x-ray image projection required during multiple occlusion device implantations.
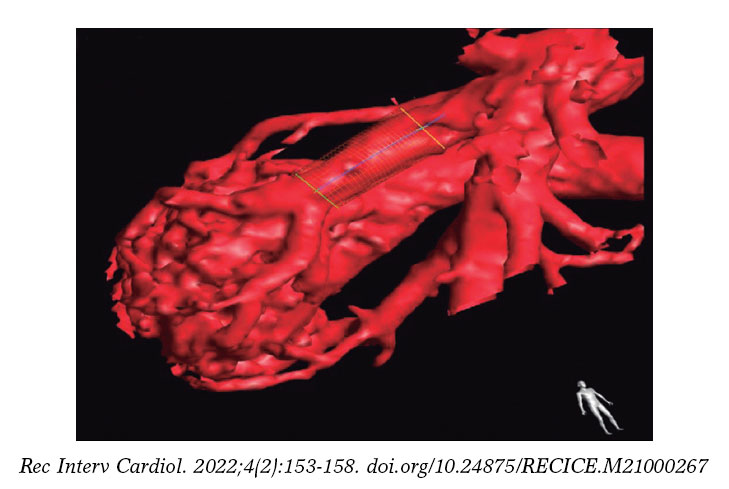
Figure 1. 3D reconstruction of a pulmonary arteriovenous malformation from data obtained from the rotational angiography performed.
The medical equipment used during the procedure included 4-Fr guide-catheters (using JR4 or MP catheters based on the anatomical needs of each patient), coils (Concerto Coil System 5/20 mm; Medtronic, United States), and vascular occluder devices (4 mm to 8 mm Amplatzer Vascular Plug from; Abbott, United States). A staged occlusion strategy was planned that started with the peripheral closure of the arteriovenous malformations (AVMs) using coils followed by the closure of nutrient vessels with coils and vascular plugs. Indeed, according to former studies, both devices combined are associated with a low rate of recanalization after embolization.1 This is the approach that has been systematically used at our center for quite some time to avoid possible spontaneous recanalizations due to collateral circulation towards the nonembolized vascular sac. The AVMs were embolized in a 2-stage procedure, 2 months apart, and without any complications being reported.
The procedure final outcomes were satisfactory with total occlusion criteria for the AVMs (video 2 of the supplementyary data). It was decided to keep the patient on low-molecular weight heparin (40 mg/24 h) for 3 months. Afterwards, anticoagulation was withdrawn. No thromboembolic (vascular or systemic) or hemorrhagic complications or associated with device embolizations were reported in any of the procedures performed. The patient’s current clinical situation (2 years after the procedure) is satisfactory. She remains asymptomatic without clinical signs of cyanosis, and peripheral arterial blood oxygen saturation levels close to 98%.
The patient’s family signed the written informed consent authorizing the use of the girl’s personal data for this article.
Although data among the pediatric population is limited, the medical literature available demonstrates that the presence of AVMs is associated with the occurrence of adverse events.2 Additionally, the use of roadmapping has proven useful for the closure of cerebral AVMs in the adult population.3 Based on our own experience, the addition of rotational angiography with 3D reconstruction and roadmapping to the embolization technique is an added value to plan this technique with greater technical accuracy. Also, it facilitates the staged occlusion strategy, which happens to be a safe technique with low rates of relapse.
FUNDING
All authors declared that no funding of any sort was received to publish this manuscript.
AUTHORS’ CONTRIBUTIONS
I. Martínez Bendayan, J. Salgado Fernández, and F. Rueda Núñez all contributed to the processes of image selection, image acquisition from the rotational angiography, and technical specifications on how to perform the procedure. The authors D. López Vázquez, A. Varela Cancelo, and M. Quintas Guzmán all contributed to the bibliographic search, drafted, and prepared this manuscript.
CONFLICTS OF INTEREST
None whatsoever.
SUPPLEMENTARY DATA
Vídeo 1. López Vázquez D. DOI: 10.24875/RECICE.M21000267
Vídeo 2. López Vázquez D. DOI: 10.24875/RECICE.M21000267
REFERENCES
1. Hundt W, Kalinowski M, Kiessling A, et al. Novel approach to complex pulmonary arteriovenous malformation embolization using detachable coils and Amplatzer vascular plugs. Eur J Radiol. 2012;81:E732-E738.
2. Donaldson JW, McKeever TM, Hall IP, et al. Complications and mortality in hereditary hemorrhagic telangiectasia:A population-based study. Neurology. 2015;84:1886-1893.
3. Rustemi O, Di Clemente L, Raneri F, et al. Utility of 3D rotational angiography road map in flow diverter deployment in a distal dissecting MCA aneurysm. Neurosurg Focus. 2019;46 (Suppl 1):V13.
* Corresponding author: As Xubias 84, 15006 A Coruña, Spain.
E-mail address: Domingo.Jose.Lopez.Vazquez@sergas.es (D. López Vázquez).










