
CASE PRESENTATION
This is the case of a 61-year-old man with cardiovascular risk factors who presents with a 3-day history of intermittent oppressive pain in the middle of his chest. The electrocardiogram confirmed the presence of an inferior-posterior wall ST-segment elevation. The emergency coronary angiography revealed the acute occlusion of a dominant left circumflex artery (videos 1 and 2 of the supplementary data) that was revascularized with 2 drug-eluting stents in the proximal left circumflex artery (bifurcation with the first obtuse marginal artery) using the TAP technique (T and small protrusion) (figure 1 and video 3 of the supplementary data). No other significant epicardial lesions were found. During the procedure the patient became desaturated, developed progressive hypotension, and eventually required invasive mechanical ventilation and intra-aortic balloon pump implantation. The echocardiogram confirmed the presence of significant mitral regurgitation (MR) with a slightly depressed left ventricular ejection fraction (LVEF) and inferior-lateral and apical akinesis with preserved right ventricular function. The transesophageal echocardiography confirmed the diagnosis of acute mitral regurgitation of ischemic etiology with a predominant jet at medial level, and no organ damage to the valve or the subvalvular apparatus (figure 2 and video 4 of the supplementary data). Within the next few hours, the patient developed refractory hypotension to vasoactive drugs and multi-organ failure. In the successive electrocardiograms performed the inferior wall ST-segment elevation was maintained. After studying disease progression, the intra-aortic balloon pump was exchanged for an Impella CP device (Abiomed; United States) via right femoral artery. A different coronary angiography was performed through the Impella introducer-sheath (figure 3) that discarded the presence of stent thrombosis (figure 4). Within the next few days, mechanical support was maintained with the Impella CP device at a rate of 2.5 L/min, and negative fluid balances were forced through continuous veno-venous hemodiafiltration that allowed extubation 72 hours later. Severe mitral regurgitation with a slightly improved LVEF still persisted on the control echocardiography, which stopped the removal of the Impella CP device. Also, the patient developed hemolysis with significant anemia (Hemoglobin levels of 7.8 g/dL) and thrombocytopenia, and required transfusion support. No significant bleeding event was reported. Since it was necessary to remove the device and LVEF had recently improved with a perspective of recovery of acute valvular heart disease, the implantation of an Impella 5.0 device was decided via right subclavian access. Ten days after days the acute event, do you think of a way to move on with treatment?
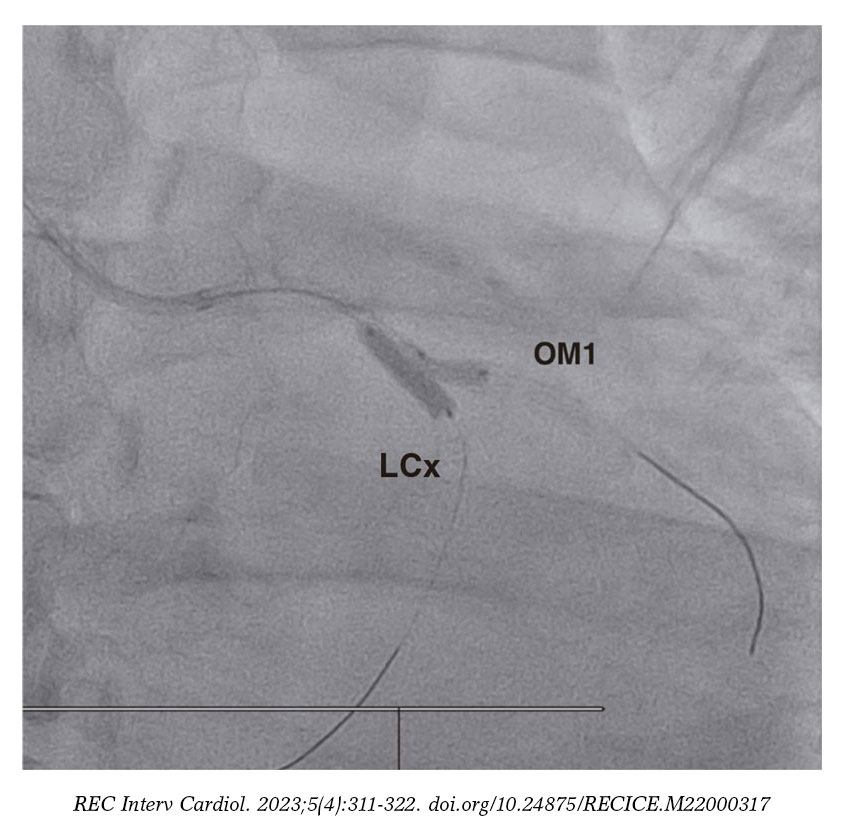
Figure 1. Revascularization using the TAP technique (T and small protrusion). LCx, left circumflex artery; OM1, first obtuse marginal artery.
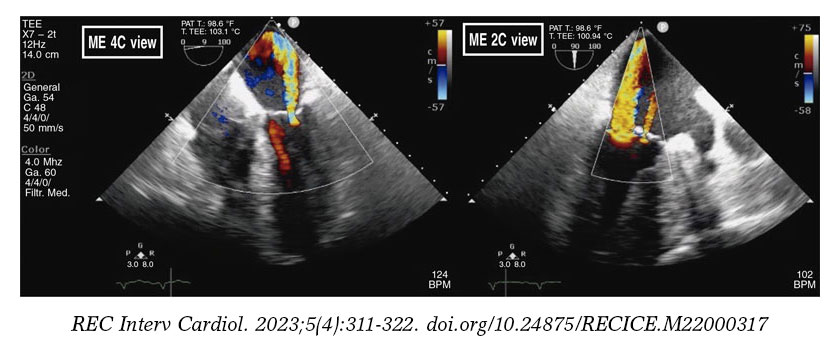
Figure 2. Transesophageal echocardiography showing severe central mitral regurgitation in A3-P3 with another jet in A2-P2.
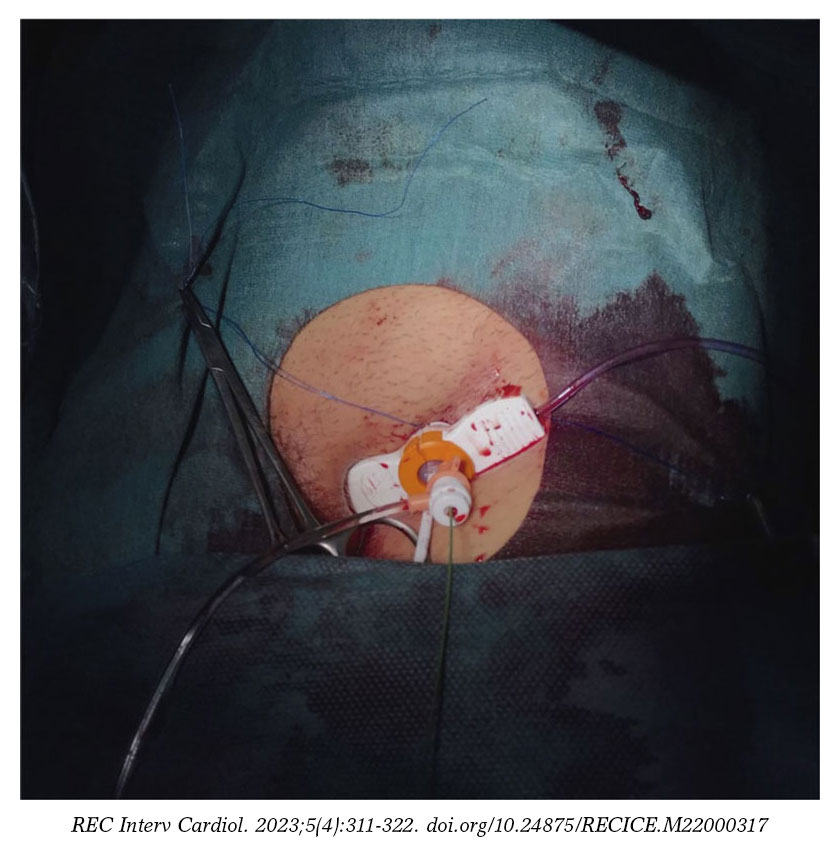
Figure 3. Only access via right femoral artery.
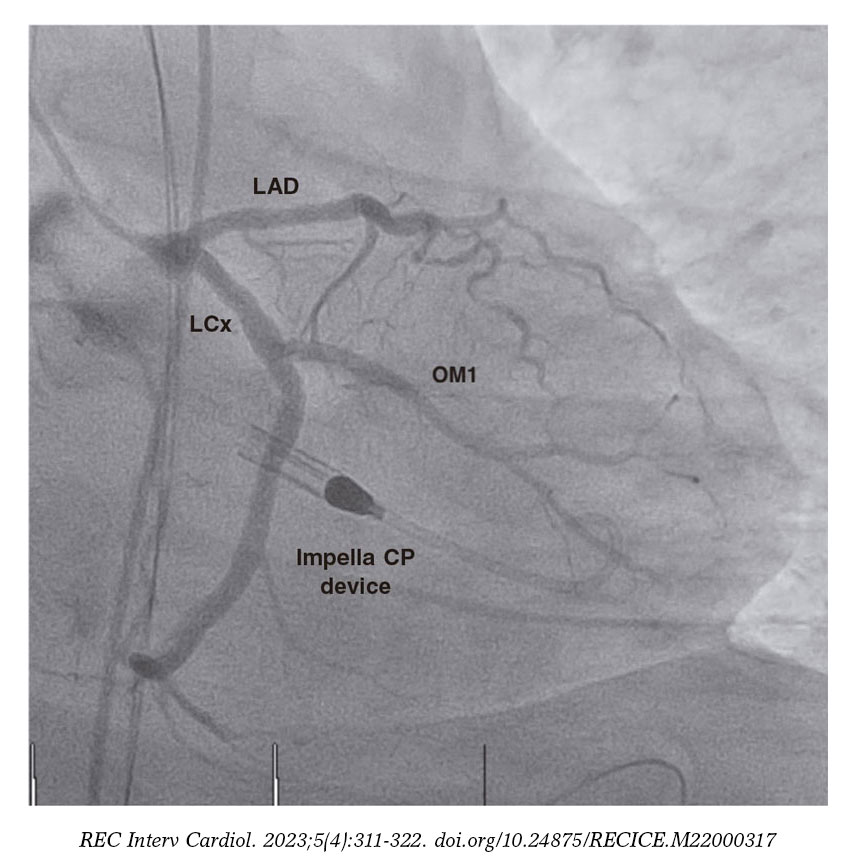
Figure 4. Impella CP device with previous patent stents. LAD, left anterior descending coronary artery; LCx, left circumflex artery; OM1, first obtuse marginal artery.
The case was published after obtaining the patient’s verbal consent.
FUNDING
None whatsoever.
AUTHORS’ CONTRIBUTIONS
All the authors contributed drafting or reviewing the case.
CONFLICTS OF INTEREST
R. Moreno is associate editor of REC: Interventional Cardiology; the journal’s editorial procedure to ensure the impartial handling of the manuscript has been followed. A. Jurado-Román is a member of the editorial team. The remaining authors declared no conflicts of interest whatsoever.
SUPPLEMENTARY DATA
Vídeo 1. Ugueto-Rodrigo C. DOI: 10.24875/RECICE.M22000317
Vídeo 2. Ugueto-Rodrigo C. DOI: 10.24875/RECICE.M22000317
Vídeo 3. Ugueto-Rodrigo C. DOI: 10.24875/RECICE.M22000317
Vídeo 4. Ugueto-Rodrigo C. DOI: 10.24875/RECICE.M22000317











