
ABSTRACT
Introduction and objectives: The Interventional Cardiology Association of the Spanish Society of Cardiology (ACI-SEC) and the Spanish Society of Pediatric Cardiology Working Group on Interventional Cardiology (GTH-SECPCC) introduce their annual activity report for 2020, the starting year of the pandemic of coronavirus disease (COVID-19).
Methods: All Spanish centers with cath labs and interventional activity in congenital heart diseases were invited to participate. Data were collected online, and analyzed by an external company together with members from the ACI-SEC and the GTH-SECPCC.
Results: A total of 16 centers participated (all of them public) including 30 cath labs experienced in the management of congenital heart diseases, 7 of them (23.3%) dedicated exclusively to pediatric patients. A total of 1046 diagnostic studies, and 1468 interventional cardiac catheterizations were registered. The interventional procedures were considered successful in 93.4% of the cases with rates of major procedural complications and mortality of 2%, and 0.1%, respectively. The most frequent procedures were atrial septal defect closure (377 cases), pulmonary angioplasty (244 cases), and the percutaneous closure of the patent ductus arteriosus (199 cases).
Conclusions: This report is the first publication from the Spanish Cardiac Catheterization in Congenital Heart Diseases Registry. The data recorded are conditioned by the COVID-19 pandemic. Diagnostic cardiac catheterization still plays a key role in this field. Most interventional techniques have reported excellent security and efficacy rates.
Keywords: Congenital heart disease. Cardiac catheterization. Atrial septal defect closure. Coronavirus. COVID-19.
RESUMEN
Introducción y objetivos: La Asociación de Cardiología Intervencionista de la Sociedad Española de Cardiología (ACI-SEC) y el Grupo de Trabajo de Hemodinámica de la Sociedad Española de Cardiología Pediátrica y Cardiopatías Congénitas (GTH-SECPCC) presentan el informe de actividad hemodinámica en cardiopatías congénitas de 2020, año de inicio de la pandemia de la enfermedad coronavírica de 2019 (COVID-19).
Métodos: Se invitó a participar a los centros españoles con laboratorio de hemodinámica y actividad intervencionista en cardiopatías congénitas. La recogida de datos se realizó telemáticamente; una empresa externa, junto con miembros de la ACI-SEC y el GTH-SECPCC, los analizó.
Resultados: Participaron 16 centros (todos públicos), que acumulan 30 salas de hemodinámica con actividad en cardiopatías congénitas, 7 (23,3%) de ellas con dedicación exclusiva a pacientes pediátricos. Se registraron 1.046 estudios diagnósticos y 1.468 cateterismos intervencionistas. Los procedimientos terapéuticos fueron exitosos en el 94,9%, con una tasa de complicaciones mayores del 2% y una mortalidad del 0,1%. Las técnicas más frecuentes fueron el cierre de comunicación interauricular (377 casos), la angioplastia pulmonar (244 casos) y el cierre de ductus arterioso (199 casos).
Conclusiones: El presente trabajo representa la primera publicación del Registro Español de Intervencionismo en Cardiopatías Congénitas. La casuística registrada está condicionada por la pandemia de la COVID-19. Los cateterismos diagnósticos siguen teniendo un papel relevante en esta actividad. Para la mayoría de las técnicas intervencionistas se han reportado excelentes datos de seguridad y eficacia.
Palabras clave: Cardiopatia congenita. Cateterismo cardiaco. Cierre de comunicacion interauricular. Coronavirus. COVID-19
INTRODUCTION
Interventional activity in the management of congenital heart disease in Spain has not been properly evaluated or analyzed to date. The collaboration between the Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology (ACI-SEC) and the Spanish Society of Pediatric Cardiology and Congenital Heart Disease Working Group on Hemodynamics (GTH-SECPCC) has reactivated and updated a registry that includes all procedures performed in patients, of any age, with congenital heart disease since their fetal stage up to their adult age.
The first report resulting from this new stage of the registry included the activity developed in 2019 and was presented in the 31st Annual Congress of ACI-SEC that was held online back in December 3-4 of 2020, and in the online administrative meeting of GT-SECPCC held in December 11, 2020.
The current report presented in this article includes the activity developed in 2020 and is the first one to be published; all the information obtained is extremely useful not only to know the volume and results of this activity, but also for the analysis of the implementation of different interventional techniques in Spain and put them in an international context. The continuity of this work will bring us knowledge of its progress in the coming years.
The provision of data was voluntary and took place through an online database. An external company handled and analyzed all the data collected. Members from the ACI-SEC and the GTH-SECPCC boards of directors were involved in the follow-up and process of revising this database; the involvement of both scientific societies—essential to conduct the registry—initiates a very desirable collaboration that should strengthen synergies among interventional cardiologists who work in adult and pediatric areas.
METHODS
This registry includes diagnostic and interventional procedural data from most Spanish centers with significant interventional activity in the field of congenital heart diseases. The submission of data has not been audited and is voluntary. It was conducted through an online questionnaire that only the person responsible from each center can access through ACI-SEC website.1 An external company (Tride, Spain) handled and analyzed the results from the registry in collaboration with members from ACI-SEC and the GTH-SECPCC boards of directors. In case of conflicting data or outside the routine clinical practice, the lead investigator of each center was contacted to verify the information submitted. Given the methodological characteristics of the study and since it was an activity registry only no approval was necessary from any ethics committees. No informed consent was needed either.
RESULTS
Resources and infrastructure
A total of 16 hospitals participated in this registry, all of them from the public healthcare network (annex 1). A total of 30 cath labs with activity in the management of congenital heart disease were included, 7 of which (23.3%) were for pediatric use only. The regular number of days a month dedicated to performing interventional procedures to treat congenital heart diseases in each hospital had a median of 7.5 (4-15) days. However, in 14 (87.5 %) of these centers, emergency cath lab care has become available on a 24-hour basis for patients of any age with congenital heart diseases.
With regard to the medical personnel, a total of 50 interventional cardiologists are involved in this activity 26 of whom (52%) are trained in adult interventional cardiology and 24 (48%) in pediatric interventional cardiology.
Diagnostic procedures
A total of 1043 diagnostic studies were conducted; 55 (5.3%) in infants < 1 month of age; 111 (10.7%) in patients between 1 month and 1 year, 486 (46.7%) cardiac catheterizations in patients between 1 and 18 years of age, and 399 (37.4%) in patients over 18 years of age.
With regard to the type of studies conducted, only 69 (6.6%) were categorized as emergency studies and the remaining ones as scheduled studies. Only 1 serious complication (cardiac tamponade) and no deaths were reported in this group.
Interventional procedures
A total of 1458 therapeutic cardiac catheterizations grouped into 13 different categories and distributed based on age and frequency were reported: only 1 case (0.1%) during the fetal stage, 141 (9.7%) in infants < 1 month, 257 (17.6%) in patients between 1 month and 1 year, 694 (47.6%) in patients between 1 and 18 years of age, and 367 (25.1%) in patients over 18 years of age (table 1).
Table 1. Number of interventional procedures performed and distribution by age groups
| Variable | Total | Fetal | < 1 month | 1 month through 1 year | 1 through 18 years | > 18 years |
|---|---|---|---|---|---|---|
| Interventional procedures | 1458 | 1 (0.1) | 141 (9.6) | 257 (17.6) | 694 (47.6) | 365 (25.0) |
| Congenital aortic valvuloplasty | 45 | 1 (2.2) | 7 (15.6) | 18 (40.0) | 16 (25.6) | 3 (6.7) |
| Congenital pulmonary valvuloplasty | 97 | 0 | 33 (34.0) | 28 (28.9) | 25 (25.8) | 11 (11.3) |
| Congenital mitral valvuloplasty | 1 | - | 0 | 0 | 1 (100) | 0 |
| Pulmonary angioplasty | 244 | - | 11 (4.5) | 50 (20.5) | 143 (58.6) | 40 (16.4) |
| Aortic angioplasty | 109 | - | 3 (2.8) | 25 (22.9) | 40 (36.7) | 41 (37.6) |
| Other angioplasties | 91 | - | 22 (24.2) | 20 (22.0) | 35 (38.5) | 14 (15.4) |
| Closure of interatrial communication/patent foramen ovale | 377 | - | - | 2 (0.5)a | 155 (41.1) | 220 (58.4) |
| Closure of the patent ductus arteriosus | 189 | - | 7 (3.7) | 42 (22.2) | 132 (69.8) | 8 (4.2) |
| Closure of interventricular communication | 39 | - | - | 3 (7.6)a | 29 (74.3) | 7 (17.9) |
| Other occlusions | 106 | - | 3 (2.8) | 19 (17.9) | 54 (50.9) | 30 (28.3) |
| Removal of foreign body | 34 | - | 2 (5.9) | 3 (8.8) | 23 (67.6) | 6 (17.6) |
| Atrial septostomy and transseptal puncture | 68 | - | 56 (82.4) | 2 (2.9) | 10 (14.7) | 0 |
| Transcatheter aortic valve implantation | 58 | - | - | - | 29 (50.0)b | 29 (50.0) | a In this case, data < 1 month, and from 1 month through 1 year were not reported separately, which is why the value is < 1 year of age. b Data correspond to patients under 18 only, which is why the value is exclusive to this group only. Data are expressed as no. or percentage (%). |
A total of 132 of these procedures (9%) were categorized as emergency procedures. A total of 30 serious events directly associated with cardiac catheterization were reported (table 2) including 2 deaths (a 0.1% mortality rate). Also, 17 cases of device embolization were reported 5 of which required surgery.
Table 2. Distribution of complications and deaths reported for each interventional procedure
| Interventional procedure | N | Major complications and deaths |
|---|---|---|
| Congenital aortic valvuloplasty | 45 | 2 (4.4) 1 severe aortic regurgitation, 1 death |
| Congenital pulmonary valvuloplasty | 97 | 2 (2.1) 1 case of severe arrhythmia, 1 tamponade |
| Congenital mitral valvuloplasty | 1 | 0 |
| Pulmonary angioplasty | 244 | 4 (1.6) 2 embolizations, 1 case of severe arrhythmia, 1 arterial dissection |
| Aortic angioplasty | 109 | 1 (0.9) 1 femoral artery pseudoaneurysm |
| Other angioplasties | 91 | 3 (3.3) 1 arterial dissection, 1 neurological event, 1 death |
| Closure of interatrial communication/patent foramen ovale | 377a (330) | 6 (1.8) 5 embolizations, 1 removal due to massive residual shunt |
| Closure of the patent ductus arteriosus | 189 | 5 (2.6) 5 embolizations |
| Closure of interventricular communication | 39 | 4 (10.2) 3 embolizations, 1 case of severe arrhythmia |
| Other occlusions | 106b (100) | 0 |
| Removal of foreign body | 34 | 0 |
| Atrial septostomy and transseptal puncture | 68 | 1 (1.5) 1 embolization |
| Transcatheter aortic valve implantation | 58c (53) | 2 (2.8) 1 embolization, 1 coronary artery compression |
| Total | 1.458d (1.401) | 30 (2.0) | a Percentages estimated over 330 cases reported. b Percentages estimated over 100 cases reported. c Percentages estimated over 53 cases reported. d Percentages estimated over 1401 cases reported. Data are expressed as no. or percentage (%). |
Percutaneous valvuloplasties
A total of 45 aortic valvuloplasties performed on congenital aortic stenoses were reported including the only case of fetal cardiac intervention in the registry, 25 of these (55.6%) were performed in patients < 1 year 7 of whom (15.6%) were < 1 month, and only 3 (6.7%) were performed in patients > 18 years of age. In 82% of the procedures, the native valves that had not been treated previously were dilated. The procedural success rate was 93.3%, and only 1 death and 1 case of severe aortic regurgitation after dilatation were reported.
A total of 97 pulmonary valvuloplasties were reported. The most numerous age range reported with 61 cases (72.9%) was that of patients < 1 year, 33 of whom (34%) were infants < 1 month, and 11 (11.3%) were patients > 18 years of age. In 95 cases (97.9%) data on the type of valves treated were reported: 80 (84.2%) were native valves, 9 of which (9.4%) were imperforated; only in 3 of these valves ductal stenting was performed to optimize pulmonary output in association with perforation and valvuloplasty. A total of 87 procedures (89.7%) were considered successful. A total of 2 major complications—cardiac tamponade, and arrhythmia with hemodynamic repercussion—were reported. Finally, only 1 case of mitral valvuloplasty was reported on a valve previously treated that turned out a success.
Percutaneous angioplasties
Pulmonary angioplasty is the group with the most cases in this section with 244 cardiac catheterizations; 143 of these (58.6%) were performed in patients between 1 and 18 years of age being this age range the most common one for this procedure. The anatomical substrate of angioplasty was the dilation of branch pulmonary arteries in 176 cases (72.1%), native outflow tract in 38 (15.5%), and the surgical implantation of a pulmonary artery conduit in 30 cases (12.2%). The technical data of 209 procedures were reported (overall percentage, 85.7%): in 55% of these procedures the angioplasty was performed with stenting while in the remaining 45% conventional balloon dilatation was used; no dilatations with cutting balloons were reported. The success rate was 91.4%, and 4 major complications were reported: 2 cases of device embolization, 1 vascular dissection, and 1 case of severe arrhythmia.
A total of 109 aortic angioplasties were reported: in this case the age group with more dilatations was that of patients > 18 years of age with 41 cases (37.6%). A total of 70 procedures (64.2%) were reinterventions while 39 (35.7%) were procedures to treat the native aortic valves. The technical data of 100 cases (overall percentage, 91.7%) were reported with the following distribution: conventional balloon angioplasty, 33%; bare-metal stent implantation, 36%; covered stent implantation, 21%; and redilation of balloon-expandable stent, 10%. A total of 105 procedures (96.3%) were successful. Only 1 case of major complication was reported (1 arterial pseudoaneurysm that required thrombin therapy).
A total of 91 cardiac catheterizations associated with other angioplasties were reported; in this section the anatomical substrate was reported in 63 cases only (69.2%) with special attention to the dilation of the patent ductus arteriosus in 21 cases (33.3%), and surgical fistulae in 5 (7.9%). The success rate reported in this group was 89%; 1 death associated with cardiac catheterization, 1 vascular dissection, and 1 serious neurological event were reported as well.
Shunt closures and other closing procedures
Closure of interatrial communication (CIAC) was the most widely performed interventional procedure in the registry with 377 cases; 220 of these closures (58.4%) were performed in patients > 18 years of age. The type of anatomy of the defect was reported in 374 cases (99.2%): on the one hand, simple CIAC with a single hole, borders > 5 mm, and nonaneurysmal septum in 125 cases (33.4%). On the other hand, complex CIAC and patent foramen ovale in 83 and 166 cases (22.1% and 44.3%, respectively). The most widely used imaging modality to guide the closure was transesophageal ultrasound in 298 procedures (79%) followed by intravascular ultrasound in 56 (14.8%). Angiographic measurement during balloon inflation was used in 79 closures (20.9%). Results were reported in 330 cardiac catheterizations (87.5%) being successful in 97.6% of them; out of the 5 embolizations registered only 1 required surgical bailout.
A total of 199 closures of the patent ductus arteriosus were collected, 132 of which (66.3%) were performed in patients between 1 and 18 years of age, 10 closures (5%) were performed in premature patients, and 8 (4%) in patients > 18 years of age. Occlusion devices were used in 85.2% of the cases reported, and coil-type occlusion devices in the remaining ones. The antegrade venous access was the most widely used of all (69.3%). The success rate reached 96.5% with 5 cases of device embolization, 1 of these eventually requiring surgery.
The third group of shunt closures studied was the closure of interventricular communication (CIVC) including 39 cases, 32 of which (80%) were performed in patients < 18 years of age. This was the distribution of the IVC by anatomical substrate in the 38 closures (97.4%) that included this variable: perimembranous in 26 cases (68.4%), postoperative in 7 (18.4%), and muscular in 5 (13.1%). With regard to the technical data of the procedure, in 56.7% of the cases occluder devices were used while coil-type devices with a controlled release mechanism were used in the remaining ones (40.3%). Only 2 were hybrid procedures. Only 31 cases (79.4%) were considered successful associated with 4 major complications: 3 embolizations (1 of these required surgical bailout), and 1 case of severe arrhythmia as a type of atrioventricular block that prevented the delivery of the occluder device.
Also, data from other occluder devices were collected for a total of 106 cases including the closure of aortopulmonary collaterals in 41 cases (38.6%), the closure of venous collaterals in 18 (16.9%), and the closure of coronary fistulae in 28 cases (26.4%). The materials most widely used were occluder devices (48.5%) followed by coil-type occluder devices (29.1%), and particles (13.5%). The success rate reported reached 99%.
Atrial septostomy
A total of 68 procedures were collected, 56 of which (82.4%) were performed in infants < 1 month. Echocardiography was used as imaging modality guidance in 43 cases (63.3%), and x-ray images in 30 (44.1%). A total of 57 cases (83.8%) were treated with Rashkind balloon atrial septostomy. Also, 8 procedures of septal perforation with radiofrequency, and 7 procedures of septal stenting were reported. The success rate reported reached 100%.
Transcatheter aortic valve implantation
A total of 58 procedures were reported, 29 of which (50%) were performed in patients > 18 years of age. Of these, a total of 55 valves were implanted in the pulmonary position, 2 in the mitral position, and 1 in the tricuspid position. The results of 53 cases (91.4%) were reported with a success rate of 100% and 2 major complications without associated mortality: 1 embolization (that was solved percutaneously) and 1 coronary artery compression.
DISCUSSION
This study is the first one to report on the amount of interventional activity developed in our country for the management of congenital heart disease including pediatric and adult patients. The continuity of this registry and the collaboration between the ACI-SEC and the GTH-SECPCP will improve the quality of this registry in the coming years, and study its evolution in time.
The year 2020 was defined by the COVID-19 pandemic, which also conditioned the way care was provided for the management of cardiovascular disease.2,3 In its annual activity report, the Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology Registry of 20204 revealed that the reduction in the activity reported was actually not as significant as the one described within the first weeks of confinement, which would confirm a rebound in the activity reported after the first wave of the pandemic. In this registry, the volume of structural heart procedures like transcatheter aortic valve implantation did not fall that much while the volume of procedures like patent foramen ovale actually increased. In line with this trend, we also present a comparison of the data available from the Spanish Cardiac Catheterization in Congenital Heart Diseases Registry from 2019 and 2020 (figure 1). This comparison shows a slight increase in the number of all interventional procedures performed compared to the previous year with an overall increase of 4.1%. We should mention that in the 2019 registry the participation of hospitals dropped (2 centers left the registry) compared to 2020, which puts this information into context.
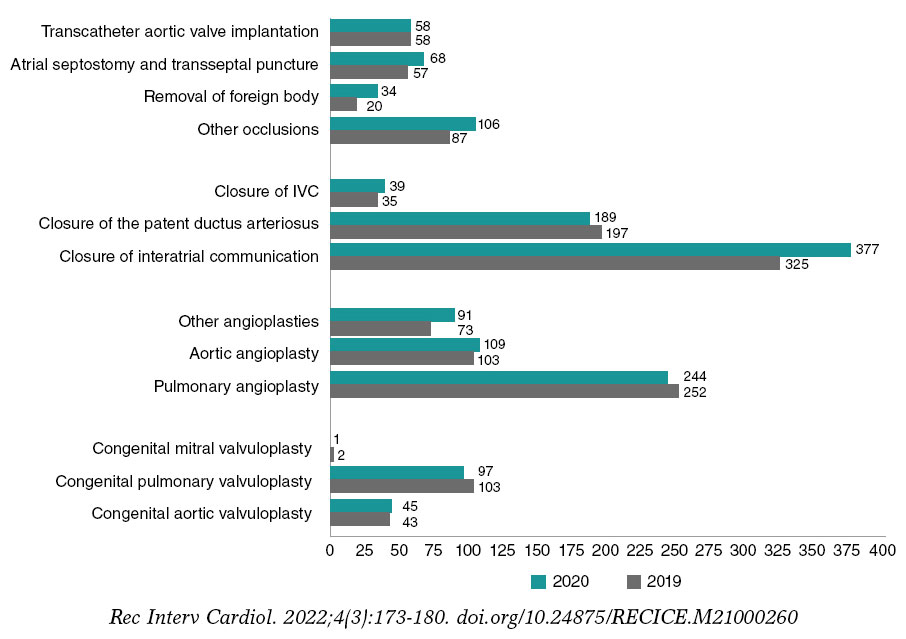
Figure 1. Comparison between the number of interventional procedures performed in 2019 and 2020. IVC, interventricular communication.
Diagnostic cardiac catheterization provides relevant anatomical and hemodynamic information to guide the treatment required by patients with congenital heart disease through different stages of the disease. Despite the continuous development of other diagnostic techniques in this field, its significance can be seen in the volume of diagnostic procedures reported (1401 cases), which represent 41.6% of the overall number of cardiac catheterizations included in the registry.
Data from 1458 interventional procedures were collected of which 1093 cases (74.9%) correspond to patients < 18 years of age meaning that this activity is basically performed in the pediatric setting m. Only in the closure of interatrial communication, age range > 18 years was the one that accumulated more cases (overall percentage, 58.4%). On the other hand, only 1 interventional procedure (aortic valvuloplasty) was reported during the fetal stage, indicative that the number of patients treated with prenatal percutaneous therapy in our country is still limited.5
Over the last few years different studies have analyzed the risk of serious adverse events associated with cardiac catheterizations performed in pediatric and adult patients with congenital heart diseases;6,7,8 given the variability of its methodology, the rate of serious adverse events also varies (from 2.5% to 7%) and for this same reason, the mortality rate reported is between 0.1% and 2%. In this registry, results and complications were reported in 96% of all interventional procedures performed. In addition, the rates of serious adverse events (2%) and mortality (0.1%) are consistent with those reported in previously cited international studies. Device embolizations—that mostly solved percutaneously—are among the complications most widely reported.
On the other hand, the overall effectiveness of interventional procedures is close to 94.9% (table 3). The least effective technique (79.4%) is the CIVC that is also associated with a high rate of complications (10.2%). All this could be interpreted as a demonstration of how difficulty and demanding it is to perform this procedure. Recently, the experience in our country with the CIVC using the Nit-Occlud device (PFM AG, Germany)—a coil-type device with a controlled release mechanism—has been published.9 It includes the experience of 16 national centers in the management of 116 patients with an 89% efficacy and a rate of major complications of 6.9%.
Tabla 3. Summary of the efficacy of interventional procedures reported
| Interventional procedure | N | Success | Infectious |
|---|---|---|---|
| Congenital aortic valvuloplasty | 45 | 42 (93.3) | 3 (6.7) |
| Congenital pulmonary valvuloplasty | 97 | 87 (89.7) | 10 (10.3) |
| Congenital mitral valvuloplasty | 1 | 1 (100) | 0 |
| Pulmonary angioplasty | 244 | 223 (91.4) | 21 (8.6) |
| Aortic angioplasty | 109 | 105 (96.3) | 4 (3.7) |
| Other angioplasties | 91 | 81 (89.0) | 10 (11.0) |
| Closure of interatrial communication/patent foramen ovale | 377a (330) | 322 (97.6) | 8 (2.4) |
| Closure of the patent ductus arteriosus | 189 | 184 (97.4) | 5 (2.6) |
| Closure of interventricular communication | 39 | 31 (79.4) | 8 (20.5) |
| Other occlusions | 106b (100) | 99 (99.0) | 1 (1.0) |
| Removal of foreign body | 34 | 33 (97.1) | 1 (2.9) |
| Atrial septostomy and transseptal puncture | 68 | 68 (100) | 0 |
| Transcatheter aortic valve implantation | 58c (53) | 53 (100) | 0 |
| Total | 1.458d (1401) | 1330 (94.9) | 71 (5.0) | a Percentage estimated over 330 cases reported. b Percentage estimated over 100 cases reported. c Percentage estimated over 53 cases reported. d Percentage estimated over 1401 cases reported. Data are expressed as no. or percentage (%). |
With regard to valvuloplasties, percutaneous dilatation is the most widely accepted technique to treat congenital pulmonary valvular stenosis. Its efficacy reported in this registry (89.7%) may have been conditioned by certain unfavorable anatomical or genetic scenarios disregarded during data duration. In primary care of congenital aortic stenosis there is still an unsolved ongoing debate on whether to go surgical or percutaneous.10 The results reported on the aortic valvuloplasties performed (with a 93.3% efficacy) back up the convenience of using the percutaneous option in our setting. Finally, we should mention that, to this date, mitral valve valvuloplasty is an unusual technique in the congenital heart disease setting.
Within percutaneous angioplasties, the most widely used procedure was the dilation of branch pulmonary arteries that was also the second most widely performed interventional procedure of all in the registry. On the technique used, we should mention that no cutting balloon was used; instead, stent implantation was predominant. The cases reported of aortic angioplasty were mainly reinterventions and only a third treated the native aortic valve. Angioplasty with stenting was the most widely used procedure. Also, bare-metal stent implantation was more common compared to covered stent implantation.
Closure of interatrial communication (CIAC) is the interventional procedure with most cases reported in the registry especially the closure of the patent foramen ovale. The evidence published over the last few years on its utility in the prevention of strokes anticipates its growth in the years ahead.11,12 Transesophageal ultrasound is the most widely used imaging modality to guide the closure of interatrial shunts compared to intravascular ultrasound that is a minority.
Regarding the closure of the patent ductus arteriosus, the use of occluder devices is predominant. In the pediatric setting, the implementation of this technique in premature patients could grow significantly within the next few years after the publication of different studies that support its safety and efficacy profile.13,14
The evolution of both the technique and the indications for transcatheter pulmonary valve implantation, as well as the availability of new valves15,16 widen the number of anatomical scenarios eligible for this procedure. Therefore, it is expected that more patients with right ventricular outflow tract dysfunction will be treated with interventional procedures.
Limitations
The comparison between data collected from this Cardiac Catheterization in Congenital Heart Diseases Registry and data from the Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology Registry (both from 2020)4 reveals a significant underestimate of some interventional procedures performed in patients > 18 years of age. This would undermine the percentual distribution reported for such procedures between children and adults. Future registries should correct this deficiency and open participation to all centers from our country with some kind of interventional activity to patients with congenital heart diseases, especially adults.
From the methodological point of view, the success parameters of some interventional procedures have not been predefined assuming a uniform criterion in all participant centers. On the other hand, grouping certain techniques like the angioplasty of branch pulmonary arteries, the pulmonary artery conduit, and the native outflow tract can be a confounding factor regarding the assessment of its technical peculiarities and results. Finally, extending the information included on the latest techniques available adds a new asset to the registry and should be reevaluated in future editions.
CONCLUSIONS
This study is the first publication of the Spanish Cardiac Catheterization in Congenital Heart Diseases Registry thanks to the collaboration of the ACI-SEC and the GTH-SECPCC.
Diagnostic cardiac catheterization still plays a key role in the management of patients with congenital heart disease. The most widely used interventional procedures are the CIAC, the angioplasty of branch pulmonary arteries, and the closure of the patent ductus arteriosus. The efficacy and safety data reported on the different interventional techniques used are consistent with the medical literature available. The complications most widely described are embolizations. The CIVC is a technique associated with the lowest success rate and the highest rate of complications in our setting.
Future editions of this registry should encourage the participation of hospitals from our country with interventional activity in the management of congenital heart disease and make the resulting information as truthful and honest as possible.
FUNDING
None whatsoever.
AUTHORS’ CONTRIBUTIONS
All authors contributed substantially to data curation and the process of revising this study. F. Ballesteros Tejerizo, F. Coserría Sánchez, and R. Romaguera were also involved in the drafting of this manuscript.
CONFLICT OF INTERESTS
R. Romaguera, and S. Ojeda Pineda are associate editors of REC: Interventional Cardiology; the journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. The remaining authors had no competing interests to declare.
WHAT IS KNOWN ABOUT THE TOPIC?
- Cardiac catheterization is the cornerstone for the management of patients with congenital heart disease.
- Excellent success rates have been reported in the medical literature available on the use of interventional techniques with limited morbidity and mortality rates too.
- In Spain, numerous centers offer interventional procedures to patients with congenital heart diseases both in the pediatric and in the adult settings.
- The national, multicenter studies on the interventional activity developed for the management of congenital heart diseases published to this date are scarce and only include certain techniques or are limited by age segments.
WHAT DOES THIS STUDY ADD?
- This is the first publication that evaluates the interventional activity developed in Spain to treat congenital heart disease in patients of any age.
- Based on the data submitted, diagnostic cardiac catheterization still plays a key role in the management of patients with congenital heart diseases with a significant number of procedures being performed.
- The interventional techniques that comprise a greater number of cases in our setting are the closure of interventricular communication (CIVC), the angioplasty of branch pulmonary arteries, and the closure of the patent ductus arteriosus.
- The efficacy and safety results reported on the different techniques used are consistent with the data previously published in the international medical literature.
- The type of complication most frequently associated with cardiac catheterization is device embolization.
ANNEX 1. List of centers that participated in the Spanish Cardiac Catheterization in Congenital Heart Diseases Registry
| Complexo Hospitalario Universitario, A Coruña |
| Hospital Universitario 12 de Octubre (Instituto Pediátrico del Corazón), Madrid |
| Hospital Universitario Ramón y Cajal, Madrid |
| Hospital Universitario Reina Sofía, Córdoba |
| Hospital Universitario de Cruces, Barakaldo, Bilbao |
| Hospital Universitario La Paz, Madrid |
| Hospital Universitario Son Espases, Palma de Mallorca |
| Hospital Universitario Virgen de la Arrixaca, Murcia |
| Hospital Universitario y Politécnico La Fe, Valencia |
| Hospital Universitario Gregorio Marañón, Madrid |
| Hospital Universitario Virgen de las Nieves, Granada |
| Hospital Universitario Virgen del Rocío, Sevilla |
| Hospital Clínico Universitario de Valladolid, Valladolid |
| Hospital Regional Universitario de Málaga (Materno-Infantil), Málaga |
| Hospital Universitari Vall de Hebrón, Barcelona |
| Hospital Miguel Servet, Zaragoza |
REFERENCES
1. Asociación de Cardiología Intervencionista de la Sociedad Española de Cardiología. Registro de Actividad ACI-SEC. 2020. Available online:http://www.registroactividadacisec.es. Accessed 21 Jun 2021.
2. Romaguera R, Cruz-Gonzalez I, Jurado-Roman A, et al. Considerations on the invasive management of ischemic and structural heart disease during the COVID-19 coronavirus outbr. Consensus statement of the Interventional Cardiology Association and the Ischemic Heart Disease and Acute Cardiac Care Association of the Spanish Society of Cardiology. REC Interv Cardiol. 2020;2:112-117.
3. Moreno R, Diez JL, Diarte JA, et al. Consequences of canceling elective invasive cardiac procedures during Covid-19 outbr. Catheter Cardiovasc Interv. 2021;97:927-937.
4. Romaguera R, et al. Registro Español de Hemodinámica y Cardiología Intervencionista. XXX Informe Oficial de la Asociación de Cardiología Intervencionista de la Sociedad Española de Cardiología (1990-2020) en el año de la pandemia de la COVID-19. Rev Esp Cardiol. 2021;74(12):1095-1105.
5. Galindo A, Gómez-Montes E, Gómez O, et al.Fetal Aortic Valvuloplasty:Experience and Results of Two Tertiary Centers in Spain. Fetal Diagn Ther. 2017;42:262-270.
6. Jayaram N, Spertus JA, Kennedy KF, et al. Modeling major adverse outcomes of pediatric and adult patients with congenital heart disease undergoing cardiac catheterization:Observations From the NCDR IMPACT Registry (National Cardiovascular Data Registry Improving Pediatric and Adult Congenital Treatment). Circulation. 2017;136:2009-2019.
7. Hill KD, Du W, Fleming GA, et al. Validation and refinement of the catheterization RISk score for pediatrics (CRISP score):An analysis from the congenital cardiac interventional study consortium. Catheter Cardiovasc Interv. 2019;93:97-104.
8. Taggart NW, Du W, Forbes TJ, et al. A Model for Assessment of Catheterization Risk in Adults With Congenital Heart Disease. Am J Cardiol 2019;123:1527-1531.
9. Solana-Gracia R, Mendoza Soto A, Carrasco Moreno JI, et al. Registro español de cierre percutáneo de comunicación interventricular con dispositivo NitOcclud LêVSD-Coil. Experiencia tras más de 100 implantes. Rev Esp Cardiol. 2021;74:591-601.
10. Saung MT, McCracken C, Sachdeva R, Petit CJ.Outcomes Following Balloon Aortic Valvuloplasty Versus Surgical Valvotomy in Congenital Aortic Valve Stenosis:A Meta-Analysis. J Invasive Cardiol 2019;31:E133-E142.
11. Saver JL, Carroll JD, Thaler DE, et al. Long-term outcomes of patent foramen ovale closure or medical therapy after stroke. N Engl J Med. 2017;377:1022-1032.
12. Turc G, Calvet D, Guerin P, et al. Closure, anticoagulation, or antiplatelet therapy for cryptogenic stroke with patent foramen ovale:systematic review of randomized trials, sequential meta-analysis, and new insights from the CLOSE study. J Am Heart Assoc. 2018;7:e008356.
13. Rodríguez Ogando A, Planelles Asensio I, de la Blanca ARS, et al. Surgical Ligation Versus Percutaneous Closure of Patent Ductus Arteriosus in Very Low-Weight Preterm Infants:Which are the Real Benefits of the Percutaneous Approach?Pediatr Cardiol. 2018 Feb;39:398-410.
14. Shyam K. Sathanandam, Dan Gutfinger, et al. Amplatzer Piccolo Occluder clinical trial for percutaneous closure of the patent ductus arteriosus in patients ≥700 grams. Catheter Cardiovasc Inerv 2020;96:1266-1276.
15. Stotut KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease:executive summary:a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation. 2019;139:e637-697.
16. Kim GB, Song MK, Bae EJ, et al. Successful feasibility human trial of a new self-expandable percutaneous pulmonary valve (Pulsta valve) implantation using knitted nitinol wire backbone and trileaflet α-gal-free porcine pericardial valve in the native right ventricular outflow atract. Circulation Cardiovasc Interv. 2018;11:e006494.
* Corresponding author:
E-mail address: fernandoballe@gmail.com (F. Ballesteros)










