
To the Editor,
During the first few months of 2020, a severe acute respiratory syndrome outbreak due to coronavirus 2 (SARS-CoV-2) was an- nounced worldwide. The WHO (World Health Organization) declared the global pandemic in March 11, 2020. After the United States, to this day Spain remains as the second country with the highest number of patients infected. Apart from the direct consequences of the coronavirus disease 2019 (COVID-19), the healthcare system overload is negatively impacting the effective management of other severe conditions whose treatment can’t wait.
During the current COVID-19 pandemic, patients with cardiovascular diseases are suffering diagnostic and treatment delays that are probably impacting cardiovascular mortality.1 Scientific societies have issued several warnings on the management of the acute coronary syndrome and ST-segment elevation myocardial infarction.2
Symptomatic severe aortic stenosis (SSAS) has a poor short-term clinical outcome if untreated. As transcatheter aortic valve implantation (TAVI) has been established as the most common treatment option for the management of SSAS,3 recommendations on this therapy during the current pandemic are clinically relevant for physicians who are treating these patients.
In order to clarify how the COVID-19 pandemic may affect patients with SSAS who are eligible for TAVI the Interventional Cardiology Association of the Spanish Society of Cardiology (ACI-SEC) has issued the following 10 recommendations:
– In patients with SSAS > 70 who require treatment during the current COVID-19 pandemic, transfemoral TAVI should be the treatment of choice regardless of their surgical risk because this procedure is less invasive compared to the surgical aortic valve replacement. Also, it is associated with shorter hospital stays and a lower in-hospital COVID-19 infection rates.
– Patients eligible for TAVI are a high-risk population for COVID-19 infection mainly because they are older. For this reason, TAVI should be postponed in clinically stable patients with preserved left ventricular ejection fraction (figure 1).
– Stable patients with postponed TAVIs should be monitored closely (telemedicine can be useful) to detect any clinical destabilizations early and be able to act fast.
– In patients who need to undergo TAVI during the current pandemic, the procedure should be as minimalistic as possible (ie, without intubation or transesophageal monitoring) to shorten the hospital stay and minimize the risk of SARS-CoV-2 contagion.
– To reduce the need for new invasive procedures that could extend the hospital stay and increase the risk of SARS-CoV-2 contagion, devices that require fewer permanent pacemakers are advised.
– Try to minimize the rate of complications that could require additional procedures: vascular access should be assessed carefully and devices with small size sheaths should be considered (to avoid vascular complications). Also, special attention should be paid to prevent acute kidney injury from happening (avoiding the need for renal replacement therapy).
– In-hospital echocardiographic studies after the procedure should not be performed if deemed unnecessary to reduce the risk of COVID-19 infection at the echocardiography laboratory. A handheld echocardiographic device at the patient’s bedside can be used to discard complications such as late pericardial effusion.
– If the procedure cannot be postponed for clinical reasons, always look for COVID-19 infection (polymerase chain reaction) before the procedure. If the polymerase chain reaction tests positive for COVID-19, the procedure should be postponed (figure 1).
– In patients with COVID-19 disease and a clear need for TAVI (asymptomatic COVID-19 disease with highly clinically unstable SSAS), the heart team involved in this procedure should be protected properly.4
– In critically unstable patients with COVID-19 disease in whom treatment for SSAS is contemplated, the percutaneous aortic valvuloplasty can be a valid option as a bridging therapy to TAVI.
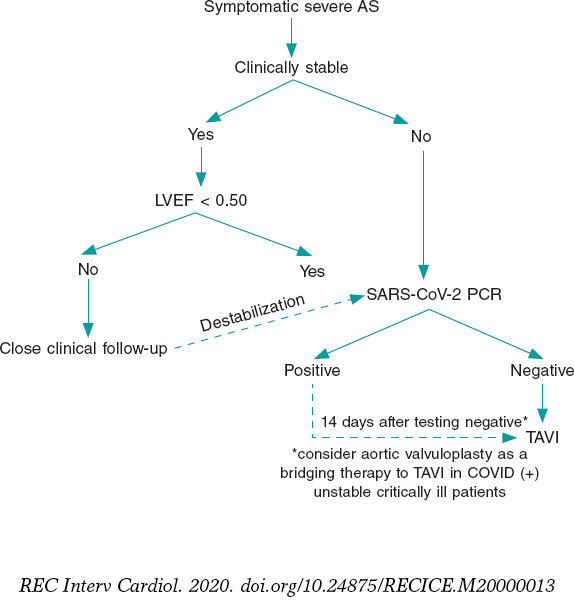
Figure 1. Proposed management of symptomatic severe aortic stenosis with TAVI during the current COVID-19 pandemic (Interventional Cardiology Association of the Spanish Society of Cardiology [ACI-SEC]). AS, aortic stenosis; LVEF, left ventricular ejection fraction; TAVI, transcatheter aortic valve implantation; PCR, polymerase chain reaction.
CONFLICTS OF INTEREST
R. Moreno is associate editor of REC: Interventional Cardiology. The journal’s editorial procedure to ensure impartial handling of the manuscript has been followed. R. Moreno is a proctor for Acurate Neo, Lotus (Boston Scientific), and Allegra (New Vascular Therapy) valve devices. The remaining authors have not declared any conflicts of interest whatsoever.
REFERENCES
1. Rodríguez-Leor O, Cid-Álvarez B, Ojeda S, et al. Impact of COVID-19 pandemic over activity of interventional cardiology in Spain. REC Interv Cardiol. 2020. https://doi.org/10.24875/RECICE.M20000123.
2. Romaguera R, Cruz-Gonzalez I, Jurado-Roman A, et al. Considerations on the invasive management of ischemic and structural heart disease during the COVID-19 coronavirus outbreak. Consensus statement of the Interventional Cardiology Association and the Ischemic Heart Disease and Acute Cardiac Care Association of the Spanish Society of Cardiology. REC Interv Cardiol. 2020. https://doi.org/10.24875/RECICE.M20000121.
3. Otto CM. Informed Shared Decisions for Patients with Aortic Stenosis. N Engl J Med. 2019;380:1769-1770.
4. Romaguera R, Cruz-Gonzalez I, Ojeda O, et al. Consensus document of the Interventional Cardiology and Heart Rhythm Associations of the Spanish Society of Cardiology on the management of invasive cardiac procedure rooms during the COVID-19 coronavirus outbreak. REC Interv Cardiol. 2020. https://doi.org/10.24875/RECICE.M20000116.
Corresponding author: Departamento de Cardiología, Hospital Universitario La Paz, Paseo de la Castellana 261, 28046 Madrid, Spain.
E-mail address: raulmorenog@hotmail.com (R. Moreno).











