
To the Editor,
Distal transradial access (dTRA) has been postulated as a new alternative to traditional left transradial access for coronary angiography.1 Its main advantages are reduced time to hemostasis, increased comfort during the procedure—both for patient and operator—and preservation of proximal access for future interventions.
Traditionally, hemostasis with the dTRA has been done manually or using conventional radial bands with the limitation of instability causing increased or ineffective compression due to anatomical mismatch. The PreludeSYNC DISTAL2 is the first dTRA hemostatic band with the setback of having multiple devices for a reasonably similar access.
The TR Band is a compression device designed to assist in radial artery hemostasis after performing a transradial procedure. The transparent structure is designed for visual control and selective compression of the radial artery featuring dual compression balloons through air titration. Also, it has a rigid transparent plastic support to guarantee compression. This plastic support avoids the correct apposition in the anatomical snuffbox if used for dTRA compression purposes (figure 1A,B).
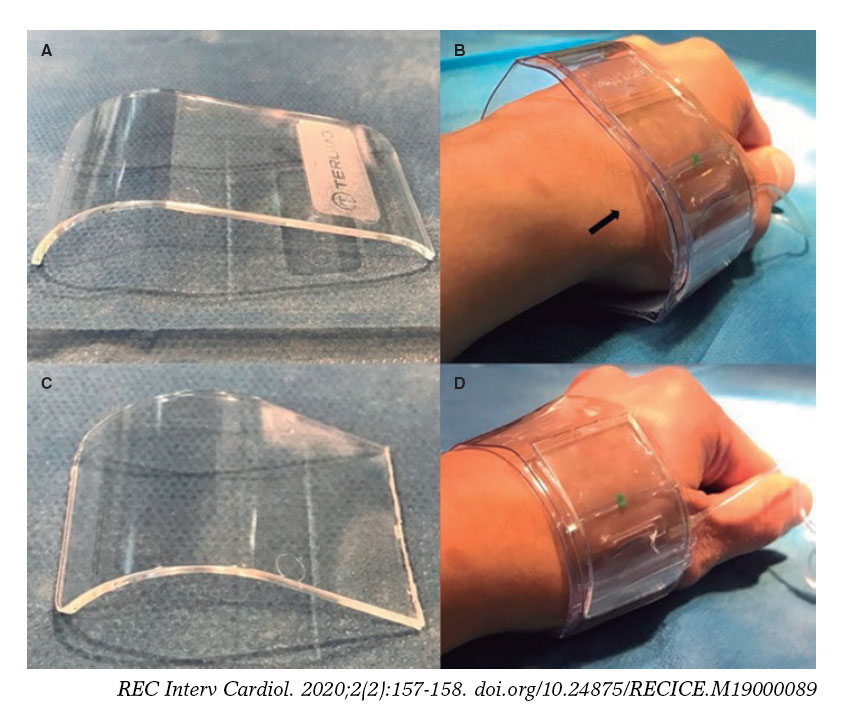
Figure 1. A-B: incomplete apposition in the anatomical snuffbox of the unmodified TR Band. C-D: complete apposition in the anatomical snuffbox after cutting through the middle of this rigid transparent plastic.
Cutting through the middle of this rigid transparent plastic (using surgical scissors, figure 2, video 1 of the supplementary data) facilitates the right apposition of the splint, and maximizes the effectiveness of compression in dTRA. The visibility of the puncture site is guaranteed, allowing the adjustment of the pressure depending on each patient’s individual condition, while distributing the pressure evenly in the compression zone. The local effects of the remaining plastic shards are avoided by covering the plastic structure (figure 1C,D).
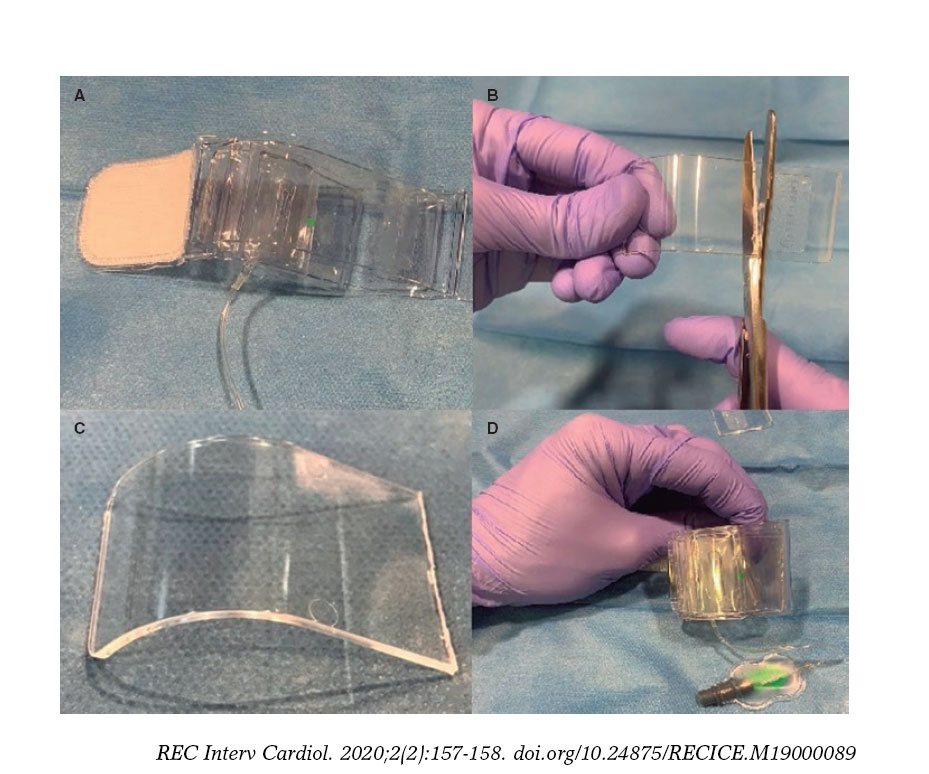
Figure 2. Modification process of the TR Band.
We have performed 96 cases of dTRA to date. In every procedure, punctures were ultrasound-guided3 to minimize damage to the artery during the process. This modification of the TR Band was used as a hemostatis method in 90 out of a total of 96 patients treated with dTRA. The cases where it could not be used were patients with too thick a wrist for the TR Band to fit correctly and safely (6 patients). Thus, it was decided to perform manual compression of the distal radial artery to avoid possible complications associated with any accidental moves of the TR Band. No bleeding, hematomas or vascular complications were reported.
Other authors have suggested3,5 further modifications of the TR Band by completely removing the rigid transparent plastic support with good results. Although it is an equally acceptable alternative worth taking into account, in our own experience we have not seen that the patient’s anatomical characteristics are a limiting factor to apply our modification. The main advantages are a greater stability achieved during device placement and a more homogeneous pressure distribution. The rates of success of the entire removal of the plastic splint are similar compared to our own results (94.9% vs 93.75%).4
This off-label modification allows an effective and secure compression when using the dTRA with the most widely used device today. It can be an alternative to manual compression or dedicated devices. In our own experience it can bring more stability compared to the complete removal of the plastic splint. Puncturing the snuffbox is still not widely used in our routine clinical practice, and safe modifications of devices available can help both logistically and economically generalize the technique.
SUPPLEMENTARY DATA
Video 1. Martínez-Crespo J. DOI: 10.24875/RECICE.M19000089
BIBLIOGRAFÍA
1. Kiemeneij F. Left distal transradial access in the anatomical snuffbox for coronary angiography (ldTRA) and interventions (ldTRI). EuroIntervention. 2017;13:851-857.
2. Merrit medical 2019. PreludeSYNC DISTAL™. Available at: https://www.merit.com/cardiac-intervention/hemostasis/compression-devices/preludesync-distal/ Accessed 9 Dec 2019.
3. Hadjivassiliou A, Kiemeneij F, Nathan S, Klass D. Ultrasound-guided access of the distal radial artery at the anatomical snuffbox for catheter-based vascular interventions:A technical guide. EuroIntervention. 2019;pii:EIJ-D-19-00555, doi:10.4244/EIJ-D-19-00555
4. Oliveira MDP, Navarro EC, Kiemeneij F. Distal transradial access as default approach for coronary angiography and interventions. Cardiovasc Diagn Ther. 2019 Oct;9:513-519.
5. Aoi S, Htun WW, Freeo S, et al. Distal transradial artery access in the anatomical snuffbox for coronary angiography as an alternative access site for faster hemostasis. Catheter Cardiovasc Interv. 2019;94:651-657.












