
To the Editor,
The infection caused by the SARS-CoV-2 virus (COVID-19) has impacted significantly the management of other conditions. In particular, the data from surveys conducted in coronary1 and interventional cardiology units2 show fewer admissions due to myocardial infarctions and coronary interventions, respectively.
Although these are observational and retrospective data that cannot be used to establish causal relations, they are valuable information, actually they may be the only information available to this day. Different hypotheses have been proposed to explain this 40% to 50% drop in the number of acute coronary syndromes (ACS) managed at the hospital setting. The first hypothesis is that a true reduction of new cases of ACS (health epidemic) would have been due to the population physical rest and reduction of air pollution.3 The second one is that it was due to the patients’ lower attendance rate on fears of acquiring COVID-19 in the hospital setting and to avoid saturating health services. The third hypothesis is that it was due to the worse quality of care of the healthcare system due to saturated ERs and diagnostic biases from ACS towards COVID-19.
We conducted a study to analyze the impact of SARS-CoV-2 on the new cases of ACS that were managed invasively. Our interventional cardiology database included prospective data until hospital discharge and covered an area of approximately 1 million people (Hospital Príncipe de Asturias, Hospital Severo Ochoa, Hospital de Fuenlabrada, and Hospital Clínico San Carlos de Madrid). The data provided here go from March 1 until April 30, 2020 and include a total of 118 patients with ACS and cardiac arrest who underwent a coronary angiography. Table 1 shows the clinical characteristics (similar) and angiographic findings (fewer culprit lesions in the group of COVID-19 positive patients).
Table 1. Clinical characteristics and angiographic findings
| Total (n = 118) | COVID-19 negative (n = 105) | COVID-19 positive (n = 13) | P | |
|---|---|---|---|---|
| Clinical characteristics | ||||
| Ae | 66 (56-77) | 65 (55-76) | 75 (62-77.5) | .158 |
| Feminine sex | 35 (29.7%) | 33 (31.4%) | 2 (15.4%) | .34 |
| Hypertension | 76 (64.4%) | 68 (66%) | 8 (66.7%) | .964 |
| Dyslipidemia | 57 (48.3%) | 53 (51.5%) | 4 (33.33%) | .235 |
| Diabetes | 35 (29.7%) | 33 (32%) | 2 (16.7%) | .273 |
| Former smoker | 62 (52.5%) | 56 (54.4%) | 6 (50%) | .774 |
| Peripheral vascular disease | 6 (5.1%) | 5 (5%) | 1 (8.3%) | .628 |
| Previous stroke | 12 (10.2%) | 11 (10.9%) | 1 (8.3%) | .786 |
| Previous infarction | 27 (22.9%) | 22 (21%) | 5 (38.5%) | .156 |
| Kidney damage | 16 (13.6%) | 15 (14.9) | 1 (8.3%) | .54 |
| Type of ACS | .849 | |||
| Unstable angina | 35 (29.7%) | 31 (29.5%) | 4 (30.8%) | |
| Non-ST-segment elevation ACS | 48 (40.7%) | 42 (40%) | 6 (46.2%) | |
| ST-segment elevation ACS | 35 (29.7%) | 32 (30.5%) | 3 (23.1%) | |
| Primary angioplasty | 25 (21.2%) | 23 (21.9%) | 2 (15.4%) | .587 |
| Left ventricular function (%) | 57 (44.3-60) | 56 (45-60) | 60 (37-61) | .497 |
| Angiographic findings | ||||
| Normal coronary arteries | 24 (20.3%) | 21 (20%) | 3 (23.1%) | .795 |
| Number of vessels with serious disease | 1 (0-2) | 1 (0-2) | 1 (0-2.5) | .844 |
| Culprit angiographic lesion | 69 (58.5%) | 65 (61.9%) | 4 (30.8%) | .032 |
| Revascularization | 72 (61%) | 67 (63.8%) | 5 (35.8%) | .077 |
| Number of vessels treated | 1 (0-1) | 1 (0-1) | 0 (0-1) | .107 |
| Total number of stents | 0 (0-1) | 1 (0-1) | 0 (0-1) | .256 |
|
ACS, acute coronary syndrome. Data are expressed as count (percentage) and median (interquartile range). |
||||
In the first place, the new cases of ACS were examined in patients in whom a coronary angiography was performed, this number was compared to the same period from 2019, and a significant 40.4% reduction was seen (chi-square goodness of fit test, P < .001) in the new diagnoses of ACS (figure 1). These data are similar to the ones obtained in the national surveys conducted in Spain and Italy.1,2
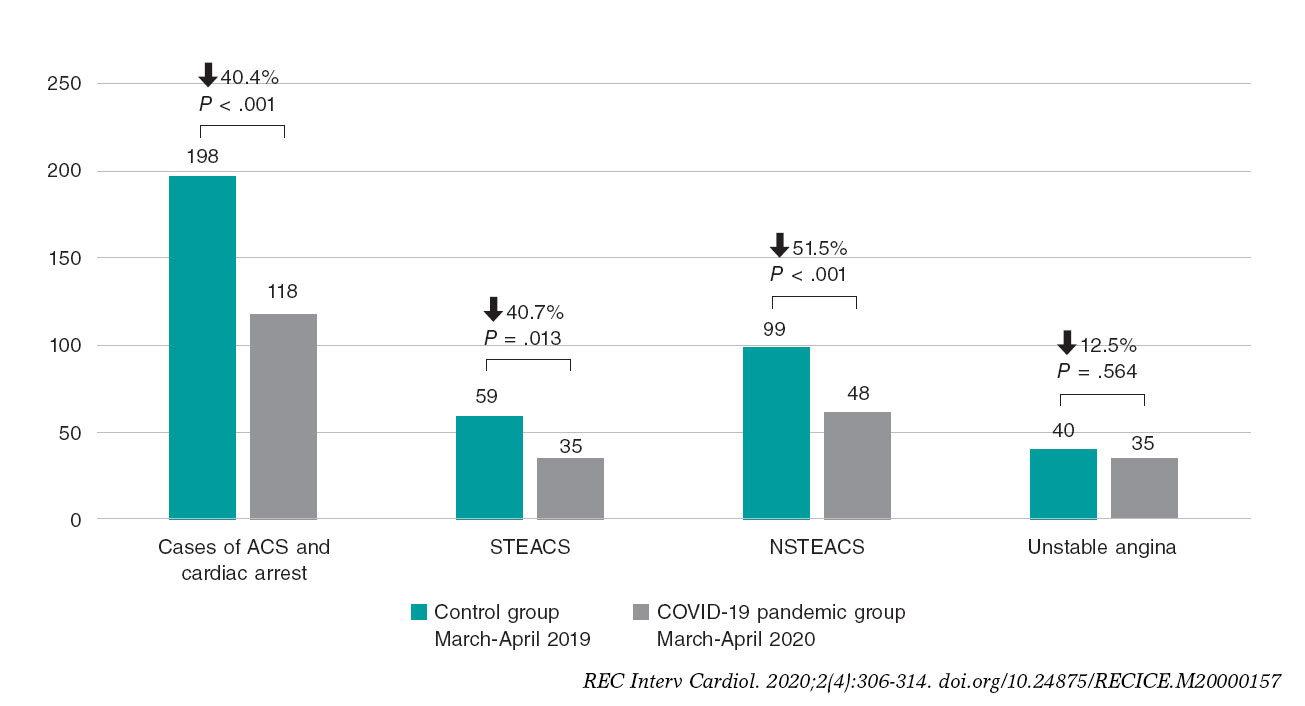
Figure 1. Count of cases of acute coronary syndrome in 2019 and 2020 during the months of March and April. P value obtained using the chi-square goodness of fit test. ACS, acute coronary syndrome; NSTEACS: non-ST-segment elevation acute coronary syndrome; STEACS, ST-segment elevation acute coronary syndrome.
When an in-depth temporal analysis was conducted (with data only from 2020 this time), we compared the new cases of ACS that were managed invasively on a weekly basis to the new cases of COVID-19 from our regional registry (figure 2). A negative correlation was seen with the number of new cases of COVID-19 diagnosed in Madrid (official data from the Spanish Ministry of Health dated March 15, 20204) as well as an obvious impact of the mandatory confinement declared in Spain back in March 15, 2020. Afterwards, the cases recovered gradually as the incidence of new cases of COVID-19 decreased. This means that, during confinement, it is possible that these cases changed the normal provision of healthcare and the patients’ attendance rate to their doctor’s office. By the way, the reduction in the number of cases is not associated with the incidence of COVID-19 in other regions.2 If there was actually a «health epidemic» with a real reduction in the number of ACSs, this reduction of cases should have been maintained in time since the degree of confinement was exactly the same at the end of the study.
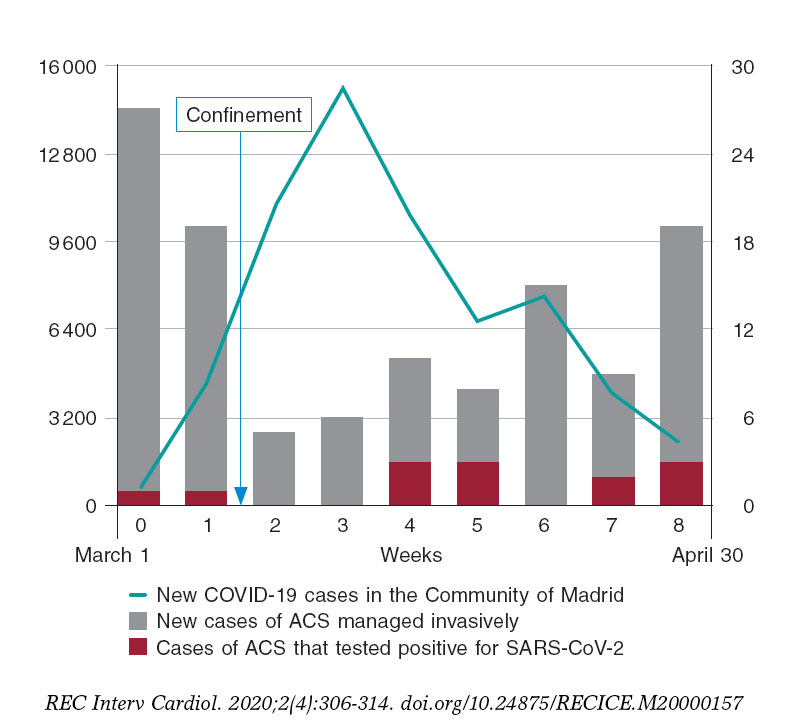
Figure 2. New weekly cases of COVID-19 in the Community of Madrid vs new admissions due to acute coronary syndrome (ACS) between March 1 and April 30, 2020. The left vertical axis shows the number of new cases of COVID-19 found in the province (green line). The right vertical axis shows the count of new cases of ACS that were managed invasively (gray bars) and those cases of ACS with a polymerase chain reaction (PCR) positive test for SARS-CoV-2 (red bars). Week 8 only included 5 days from April 26 to April 30.
Figure 2 (red bars) shows the cases that tested positive as confirmed by the polymerase chain reaction test during admission due to ACS (13 out of the 118 patients, 11.02%). There were some sporadic cases seen during weeks 4 and 5 (30% and 27% COVID-19 positive, respectively). This rate is consistent with the seroprevalence seen in a pilot study conducted by the Spanish Ministry of Health in our region that revealed that 11.3% (95% confidence interval, 9.8-13.0) of the population of Madrid already has IgG antibodies to SARS-CoV-2 (preliminary results from the ENE-COVID study19 from March 13, 20205).
This study has the limitations of an observational and retrospective study and does not provide information on patients with ACS who did not undergo a coronary angiography. However, the protocols for the management of ACS did not change substantially.6
In conclusion, the temporal analysis on the reduction of new cases of ACS that were managed invasively keeps a negative correlation with the official data of new cases of COVID-19 and a direct correlation with the declaration of confinement. The number of patients who tested positive for SARS-CoV-2 on the polymerase chain reaction test is similar to the seroprevalence estimated in the region.
REFERENCES
1. De Rosa S, Spaccarotella C, Basso C, et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur Heart J. 2020;41:2083-2088.
2. Rodríguez-Leor O, Cid-Álvarez B, Ojeda S, et al. Impacto de la pandemia de COVID-19 sobre la actividad asistencial en cardiología intervencionista en España. REC:Interv Cardiol. 2020;2:82-89.
3. Anjum NA. Good in The Worst:COVID-19 Restrictions and Ease in Global Air Pollution. Preprints. 2020. https://doi.org/10.20944/preprints202004.0069.v1.
4. Ministerio de Sanidad, Consumo y Bienestar Social. Situación actual Coronavirus. Available online: https://www.mscbs.gob.es/en/profesionales/saludPublica/ccayes/alertasActual/nCov-China/situacionActual.html. Accessed 14 Jul 2020.
5. Ministerio de Sanidad, Consumo y Bienestar Social. Estudio Nacional de Sero-Epidemiología de la Infección por SARS-CoV-2 en España (ENE-Covid). Available online:https://www.mscbs.gob.es/ciudadanos/ene-covid/home.htm. Accessed 14 Jul 2020.
6. Romaguera R, Cruz-González I, Jurado-Román A, et al. Consideraciones sobre el abordaje invasivo de la cardiopatía isquémica y estructural durante el brote de coronavirus COVID-19. REC:Interv Cardiol. 2020;2:112-117.












